Sports Doc Talk is dedicated to providing a format for all its followers. We are happy to introduce complete transcripts of our shows which can be found below.
Staying on the Court: Elite Joint Care and NBA Medicine with Dr. Travis Maak

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthoped- orthopedic surgeon and sports medicine specialist, Dr. Garcia. Man, your background is snazzy. How you doing today?
Dr. Grant Garcia: Yeah, it's super snazzy. You're... This is gonna be a good one.
Will Sanchez: Yeah, we're
Dr. Grant Garcia: really excited. I went all out on this one. AI is-- AI had some extra time for me.
Will Sanchez: Yeah, we're really excited. I know you're excited about this next guest, but before we get to our guest, as we always like to do, we give a little shout-out to the folks at Mike B and The Recovery Shop. Tell us once again why you love them.
Dr. Grant Garcia: Yeah. So again, big shout-out to our sponsors. Again, uh, they're awesome.
They're really good for especially us surgeons that do a lot of the complex knee stuff. Um, but ability to have all aftermarket products for patients that really want [00:01:00] extra, they constantly are asking for it. I've had a number of surgeons even come up to me during some of these courses that we teach and ask about this.
They say, "Hey, I got my patients asking for stuff, but I don't really know where to send them. I'm kinda tired of going to Amazon, et cetera." So this is a great option, so reach out to Mike B. Uh, they're very accommodating, and this is a, a great thing for us as surgeons to have at our fingertips
Will Sanchez: Yeah. And, uh, personal experience, uh, just utilizing the recovery shop and the, the, the great equipment that they have there to help recover throughout my Achilles injuries and things like that.
But, uh, let's get to our guest. You know, today on Sports Doc Talk, we're joined by Dr. Travis Mack, the orthopedic sports medicine specialist at the University of Utah, the Utes. Head orthopedic team physician for the Utah Jazz. Maybe we'll talk a little bit NBA, because I'm a big sports fan and I have some questions there.
You know, all you guys, Stanford, Yale, and obviously Hospital for Special- Pretty, pretty
Dr. Grant Garcia: poor upbringing. I know. He's, it's
Will Sanchez: really, really struggling ... Uh, yeah. Again, look, how do you guys all end up at s- at, uh, Special Surgery? Uh, it's- ... [00:02:00] it's great. But, uh, selected by the president, eh, he was selected as the president of the NBA Physicians Association, eh, for the 2004-2005 s- uh, '25 season, and he's helping shape how we think about keeping high level athletes performing without sacrificing long-term joint health.
Enough with introductions because we have so much to talk about. He's got some cool gear, bunch of stuff. You're gonna be all nerded out. We're talking about- ... elbows, knees, and hips. So let's bring him on. Dr. Mack, how are you? Listen, thank you for being here. We really appreciate you being here and taking time to, to join us today.
Dr. Travis Maak: No, it's my pleasure. Thanks for having me. Grant, thanks for having me as well. This is a wonderful opportunity.
Dr. Grant Garcia: Awesome. Uh, so Travis, will you tell us, everybody, I mean, the listeners already know some of your stuff. They've, you know, they've probably seen your work online for all the things you do. Um, but will you tell the listeners kind of how you got started?
I mean, obviously Stanford, uh, Yale, and then HSS, but sort of what kind of spurred you even to go into the field of sports medicine [00:03:00] and where you're at now?
Dr. Travis Maak: Yeah, it's a good question. I, I didn't actually even think I wanted to become a doctor, to be totally honest with you, when I was growing up. I grew up on a farm in Utah, in re- really, really r- rural Utah, and candidly, I, I, I thought I wanted to be a vet, but then I realized animals couldn't talk back to me, and that irritated me, so-
that had kind of a theme, to be honest. Um, at, at the end of the day, when things irritate me, I try to fix them, uh, which will be a theme through this whole process. So, uh, you know, ultimately, you know, when I was in, uh, in high school, I thought it might be fun to be a ski patroller. I wasn't a particularly good skier and I wanted to get better at that, and I'd heard lots of glory, glory stories about ski patrollers, so I thought this would be a good idea.
So back in the day before lots of regulations, they let volunteer people be ski patrollers on Saturday and Sunday. So I did ski patroller, I was a ski patroller, volunteer ski patrol at Park City, um, which is right near where I grew up. Not where I live, mind you. Um, so I'd go there on Sundays and, and do ski patrol, and it was a crazy experience.
It was... I'd done it for about a year and a half, and I got called, [00:04:00] um, to the top of one, it, a place called McConkey's Bowl, which is in Park City. They now have a lift there. Before you had to hike there. And I got called to go check out, uh, an injury that had been reported, and I went down there, and a guy had, uh, jumped off this cornice, uh, which was about a 30-foot drop, and he had not...
Y- you know the, the baskets you have on your poles, Grant, s- the, the bottom... You, you're a skier, aren't you? A little
Dr. Grant Garcia: bit? A little bit, but not,
Dr. Travis Maak: I'm, I'm
Dr. Grant Garcia: decent. Yeah,
Dr. Travis Maak: you're... All right. What are these? Yeah, all good. All good. So there's some baskets on the bottom of your poles that kind of stop your ski poles from going too deep in the snow.
Yes. And, uh, so this guy somehow had managed to lose his baskets, and he didn't care. He was still gonna get after it. So he, he hucked this cornice, jumped off it, and somehow in the process of him jumping off this cornice, his ski... He lost his ski pole, 'cause he didn't have it on his hand, and he impaled himself on his ski pole.
Will Sanchez: Oh.
Dr. Travis Maak: It went all, literally all the way through Um, so he ... I didn't know what to do, and I, I, you know, kind of freaked out a little bit, to be honest with you, and [00:05:00] just kind of got on my radio and said, "I don't know what I'm doing. Please help me."
Will Sanchez: Are, are you, are you on skis or a snowmobile? Like, how is this all happening? Skis.
Dr. Travis Maak: Skis. Okay. So I'm coming in on skis, trying to ski. And, and usually you get called for, like, you know, somebody gets a little over their skis literally, and then you gotta kind of pick up their stuff, put them back on skis, and get them down. And this was a whole different ballgame. So keep in mind, I'm s- 17 years old, and, and I come down, and this guy's impaled through it, w- like, through his lung, um, with his ski pole.
Wow. So I totally freaked out, which by the way, you're not supposed to do. And, uh, a- you know, I, I call up, and they came down and helped me, and all I remember is being totally helpless. So I never wanted to f- feel that again, and so at that point, I decided I thought I wanted to learn more and know how to actually help this guy versus feel totally helpless.
So then I went to college, kind of bounced around, and s- never kind of got that I don't want to feel helpless feeling away from me. So that's how I ended up in medicine. And then how'd I end up in orthopedics? Simple. Ultimately, I like fixing things, and in orthopedics, we fix stuff. And, and I like fixing people who like to fix themselves, and, and that's sports medicine.
So as young, [00:06:00] or in my case, old athletes that think we're athletes- ... even if we're not. Um, and then people want to get back to doing stuff that makes them healthy, healthy and have really amazing lifestyles. And so that's how I ended up doing what I'm doing, and I, I really love all the patients that I treat 'cause I empathize with them.
'Cause at the end of the day, if I can't be active and do sports and do the things I wanna do, I, I'd rather not be around too longer.
Dr. Grant Garcia: Um, that's awesome. Yeah. Do ... So one thing that you're really known for, I mean, we've talked about this at courses together, et cetera, is your preservation. I mean, you do knee, and we haven't worked together with the hip stuff.
But what kind of drew you to that? I mean, it's obviously pretty hot space. We'll talk about some of the stuff you're doing there. Um, but w- why, why preservation? You could have chosen anything. You could be the multi-lig guy, right? You could be- Sure ... you know, hip... You could do other things. ACLs all the time.
Like, what, what's the reasoning?
Dr. Travis Maak: Yeah, 100%. So you, you and I of- oftentimes commiserate, I, I think because we share our s- a similar view on the world, and, uh, which is w- we like- we're sort of masochists, honestly, um, in the sense that I, I told Brian Kelly, who's one of my mentors on the hip side, uh, he said, "What do you want to [00:07:00] do with your life?"
I said, "Well, I really love cartilage and I really, really love hip preservation. So I want to do hip scopes and cartilage preservation." He said, "You are gonna have a lonely, miserable life." Um, and, and I, and I said, verbatim. I'm Brian, Brian's a man of few words. But he's very stately. And I said, "Why is that, BK?"
Uh, 'cause I called him BK at the time. He said, "Well, cartilage is this unknown black box. We don't know why people get injuries. We don't know what to do with them. We have no idea why stuff works and what, why it doesn't. And we know everyone has it and it's a big problem, but we don't know how to fix it.
And that's pretty much the hip in a nutshell, too. So if you want to marry those two, good luck." Um, and, and I, in my head, I thought to myself... He goes, "But I took the charge 'cause I have the same perspective." And so I said, "You know what? I really like that because there's a lot of opportunity there. We can make it better."
Dr. Grant Garcia: I, I think that's really interesting for p- the viewers here. Actually, Will, this reminds me of the podcast we had a month ago. The doctor said the exact same thing about cartilage and no one could regenerate it, and there's nothing- Yeah ... we could do about it, and it's the, the same [00:08:00] scenario in the sense of what Travis is mentioning, right?
It's like there's a lot more opportunity. The... We've alr- you know, know, you know this, but as like, you know, we can all do good ACLs, but the ACLs have changed a little bit. We have some cool new techniques and little things here. But the cartilage is just exploding. Um, from the, from... How do you feel like this, you know, what do you think of in the last, you know, five, 10 years, you think from the cartilage standpoint, either, you know, maybe just on the hip or the knee, you've seen sort of as a more progression, like that black box is no longer a black box- Sure
in your opinion?
Dr. Travis Maak: Sure. So a- again, I use my own folly to, to, to lead my wisdom, which I'm not sure I have yet, but I'm working on it. Um, and that is, uh, about 12 years ago, I had a patient who, classic Utah, he was snowboarding, totally true story by the way, um, off his roof, um- ... because there'd been a lot of snow Yeah, this is real, okay?
So there's a ton of snow that year. So the dude lives in the middle of nowhere, awesome dude, incredible snowboarder. He goes, "I'm gonna huck my roof." So [00:09:00] he s- he, and he has his buddy videoing it, of course. So I have the total video, all right? I've shown it a ton of times. So he's snowboarding off his roof and literally c- drills a tree.
Like, m- c- like right- ... off his roof. Like, completely drills it. He dislocates his hip, posterior dislocation.
Will Sanchez: Oh.
Dr. Travis Maak: Big cam deformity, so hip stuff. Um, FAI, but that wasn't his problem. They reduce him- Oh ... in the ER and then call me because he has a loose body, a retained loose body. Uh, so they say, "You know, you gotta scope his hip, get the loose body out, you're good to go."
Uh, "Okay, fine." So
Will Sanchez: I- So for the... I'm sorry to interrupt No, you're good For those that don't know what loose body means, right, are we talking about just loose cartilage? What, can you explain that to-
Dr. Travis Maak: Yeah, it's all
Will Sanchez: of the above ... the listeners that really don't understand it? Go ahead.
Dr. Travis Maak: No, a heck of a good question.
So what's a loose body? The answer is exactly what it says. It's anything that's loose floating around in a joint. In a joint. So it is a body, i.e. something. It's a j- kind of a catch-all term, to be honest with you. Yeah. In this case, it was a, what I thought anyway, [00:10:00] was a piece of cartilage, um, effectively, and a little tiny piece, a fleck of bone on it, that had kinda cracked off during his dislocation.
So you don't want a piece of bone. It's like a rock in your shoe, you know? Yeah. It kinda bothers you, so you move around your shoe till
Will Sanchez: at some point- That's a good explanation. I like that.
Dr. Travis Maak: Yeah, you gotta take your shoe off- Yeah ... get the rock out.
Will Sanchez: Yeah.
Dr. Travis Maak: So that was the game plan. I was gonna, you know, put my scope in, take the rock out.
That was my plan. So, and that was all I was planning on doing. So I scope the guy, I pop the scope in, I'm gonna be a hero, right? This is literally the story of every disaster I've ever had. So I put the scope in, I'm gonna be a hero, in and out case, and then I look in there, and the guy, he's effectively sheared off, meaning completely taken off, like two-thirds of his, this, the cartilage on the top of his hip socket called the acetabulum.
It peeled off into the joint. And, and once again, it's one of those holy crap moments. I kinda felt like I felt back when I was, you know, watching the guy getting impaled by that ski pole, except at this point I'm the attending trying to do his surgery and hip re- fix him. But I didn't know what to do, uh, 'cause I, it was all of his cartilage, basically.
And it was right where he needs it on the t- uh, top of his socket, where the ball [00:11:00] kinda connects to the socket, right? You gotta walk on that. Mm-hmm. So in my head, I'm thinking, "Well, maybe I'll take it out." Well, that didn't seem like a good idea, 'cause it was literally all of his cartilage and the k- guy's 22, so that's dooming him to a hip replacement at an early age.
Then the other option is, well, I, what, I sew it down, glue it down? That doesn't work. So I didn't have any good options, so basically I said, "I have no options, therefore I'm gonna pretend I didn't do anything and go f- down, go down the ostrich mentality," which is stick my head in the sand and pretend it didn't happen.
So that's what I did. So I repaired the labrum, uh, took out the loose body, said, "We're good. I really hope you're doing well." Of course, I told him about it like you always do and say, "We're gonna follow you." So- Four years later, uh, he comes back and says he has hip pain, and I'm like, "Oh, my goodness gracious, what could possibly be going on?"
But at that point, I'd kinda thought about the process, 'cause I told you this is a theme in this conversation, which is I really hate stuff that I can't fix. Mm-hmm. It bothers me. And so during that time, I had asked the question that you asked, Grant, which is what can you do? What things can we change? How can we help this black box?
And the answer is [00:12:00] taking people's cartilage that they have already, 'cause frankly in the hip, we cut away tons of cartilage. My knee replace- my knee replacement, hip replacement colleagues are like, "Yeah, great, you're just accelerating them to come let me replace their hip." Not true, but we do cut out good cartilage sometimes in an area that they don't actually need it, and we call it an ephemeral osteochondroplasty.
So I thought, what if we don't have to cut that cartilage out? What if we can save it, and collect it, and then use that healthy cartilage and put it back where the not healthy cartilage is missing? So at that point, because of him, I'd done a bunch of research on this actually, and developed a technique called AMEC, which is autologous minced ex- uh- M- m- excuse me, autologous matrix enhanced cartilage transplantation, or...
It's a terrible name, by the way. That's why no one used
Dr. Grant Garcia: it.
Dr. Travis Maak: Um, and it-
Dr. Grant Garcia: I mean, we, we should get to four letters. The fifth letter just screws
Dr. Travis Maak: you. I mean, it's- Yeah, it's just absolutely terrible. Yeah. You would've had something better, I know you would've. So, uh, th- so back- so at that point, I did a ton of research to prove that that cartilage is alive on the [00:13:00] femoral head-neck junction, which is where the CAM is, and turns out it has a, a time of harvest about 60% viability.
And if you combine it with basically co- extracellular matrix, um, and then, uh, allow it to culture either in vitro or in vivo, and that means out of the body or in the body- Hmm ... it gets up to over 99% chondrocyte viability within five to nine days. So- Wow ... since that time, we proved in our lab with multiple patients who I've harvested from, we can take that cartilage and transplant it at the same time, and at that point, we can actually heal their own cartilage with their own cartilage.
So now it's called- Wow ... it's a technique called AutoCART, uh, that Grant knows, and that was the origin of it actually. Um, it was a lot harder to harvest back then. There was something called Grafnet that was popularized by a company called Arthrex at the time, and they, they kinda used it for a different tech- different reason, right?
They were just gonna suck this stuff out with this Grafnet, and I'll just kinda do it on the back table. So we did it and showed that it worked, and that's been a black box that, in many cases, we've [00:14:00] solved, not with stem cells actually, uh, but rather with the patient's own cartilage and combined with extracellular matrix and growth factors.
So that part- Is the- ... has
Dr. Grant Garcia: helped ... is the technique you do similar to the current AutoCART, or is this- this was the beginning of this s- scenario?
Dr. Travis Maak: Yeah, so this was the beginning actually. So since then, um, combining it with a l- some cellular matrix, so bio-cartilage or extracellular matrix, also some biologic factors, so you can combine it with PRP, you can com- combine it with BMAC, which increases the cellular regenerative capacity.
So we've advanced this since then. Again, this was 12 years ago. Uh, so now the technique has gotten much better. I told you it was really, really clunky initially when I first did it 'cause I didn't have any technique to tell me how to do it, but now we've got it dialed in, and now we've used it in the knee, we've used it in the hip, and it's a single stage of, uh, transplantation using the patient's own cartilage.
So that's something super nice that I- we've done actually, um, and it, it's really opened up a lot of opportunity I think. [00:15:00]
Dr. Grant Garcia: And obviously for the listeners to hear this, I think we'll go to the knee in a second 'cause, you know, you and I, I, I know the knee better even than the hip stuff. But from the hip standpoint, you know, there really isn't many good options, so to have something that you can use for your own patient, you can do it easily, 'cause again, it's also harder to do things through the hip 'cause of the access points, right?
Mm-hmm. Versus the knee, and you, you don't wanna... If you go, you know, we can always open the knee, and obviously we don't wanna do that if we don't have to, but it's not as hard in my opinion. Right. But you go open a hip, it's a much different animal. So you're, you're not like, it's not like you can just go and open the hip to do these procedures, right?
I mean, it's much more morbid.
Dr. Travis Maak: That's exactly right.
Dr. Grant Garcia: So that's just something for, and also for listeners to know, I mean, really your options right now, right? You, the main one you're... Is that one of your main cartilage uses, cartilage things you do for the hip?
Dr. Travis Maak: Yeah, for the same reason you just described, Grant.
In order to do anything like, for instance, a bulk cartilage transplant, like an osteochondral allograft, which is using cartilage and bone from another person, transplanting it into the hip, that's not just a simple little arthrotomy, which is a little [00:16:00] cut you make to open up the hip. You have to completely dislocate the hip.
You have to cut bone. You gotta do- Hmm ... There's a, it's a really, really rough procedure with a hard recovery and a lot of complications. So most of us don't do that very often. This you can do with a scope. You can do at the same time as treating other stuff. So I would say 98% of my cartilage work in the hip is now done with AutoCart or AMEC.
Dr. Grant Garcia: How long would you tell the patients this would take you now with the, you know, the new systems, right? Because it sounds, initially it sounds very tedious. Like, you do it. Right You harvest it. You make it. How long, how long would this take someone like you, once you get in there and you realize you have this, to actually do the, the procedure to implant it?
Dr. Travis Maak: So a standard hip scope usually takes me, and that's using a camera to treat the other stuff in a hip, uh, other than the cartilage, usually takes me somewhere between an hour and 15, an hour and 45 minutes. This adds 15 minutes
Dr. Grant Garcia: Oh, that's awesome.
Will Sanchez: Can you describe, uh- So you, I was gonna ask
Dr. Travis Maak: that ...
Will Sanchez: no, I was just gonna say, can you describe a specific type of his- hip surgery that normally would take X amount of time, and now with this new [00:17:00] procedure, uh, you could compare that?
I'm talking about recovery time. Sure. And then also, whether it's not just the, the short-term recovery, but the long-term recovery, uh, differences.
Dr. Travis Maak: Sure. So prior to this, I had done a few bulk osteochondral allograft transplants to the socket. Uh, I did it with my open hips preservation colleagues. I work with some amazing p- uh, partners.
One of them in particular is a guy named Chris Peters, who's very well known in the open hip space. So we did it together. It's, you have, it, it, the approach is called a surgical hip dislocation, uh, which is a big morbid procedure. You have to cut one part of the bone, dislocate the hip. Uh, it took me about three hours to do it with him.
Yeah. Um, and then you have to let the bone heal, 'cause you just cut it with a saw. Uh, so the recovery, you have to keep them in a brace, you have to keep them on crutches, you have to... It takes about three, three months or so, just for them to recover from the open surgery. And again, he's a wizard surgeon, okay?
So I'm pretty sure- Yeah ... with other people, it'd take a lot longer. And now, with the AMEC or AutoCart [00:18:00] technique, it's done through the same three poke holes that are about that big that we use a camera to, to treat the hip anyway. Uh, the whole procedure takes me about an hour and 45 minutes. With the cartilage, if it's an hour and h- half, normally.
Um, they s- we start them toe touch weight bearing. They're still using crutches, but almost no pain for about four weeks. They transition. By six weeks, they're hiking, biking, and swimming. Um, and then we get them back to effectively jogging and running in about three months, rather than getting off the crutches.
So,
Dr. Grant Garcia: so the activity- What do
Will Sanchez: you tell them
Dr. Grant Garcia: for how long it takes to grow back?
Will Sanchez: Yeah.
Dr. Travis Maak: The cartilage?
Dr. Grant Garcia: Yes.
Dr. Travis Maak: Yeah, so typically speaking, with AutoCart or AMEC in the past, we, we've MRIs these, actually, and generally speaking, you have perfect fill and hyaline-like cartilage that's effectively full by six months.
Realistically, in the lab, though, we have mature cartilage that happens within weeks.
Dr. Grant Garcia: Got it. '
Dr. Travis Maak: Cause again- Well, and that's- ... you're already working with their cartilage ...
Dr. Grant Garcia: well, and also, it's autographed. I mean, the, for the patients listening, the, your own tissue always heals faster, in many cases, than tissue from somebody else.[00:19:00]
Dr. Travis Maak: Correct. Right, so- The other component of this, um, that you mentioned, uh, Grant, and I'll just highlight this, when you're using cartilage from someone else, which is your point, you gotta wait, and you have to wait for someone to have a unfortunate accident. You have to time it. It's really hard. This, you can do any time, 'cause you're using that- Mm-hmm
patient's own cartilage.
Dr. Grant Garcia: Yes, Will.
Will Sanchez: No, I was just gonna say that it's, uh, that's life-changing. You know, this is... The recovery and it's getting back to your family, it's getting back to work, it's getting back to your normal day. It's you not sitting around and your testosterone is shooting down. It ju- there just s- there's...
I, I mean, I could go on and on-
Dr. Grant Garcia: Yeah ...
Will Sanchez: just by, you know, this procedure and the recovery time and the quality of life. Uh, that itself, just thinking about it is, um, is just, like I said, is game-changing. So it's great, great to hear.
Dr. Grant Garcia: I wanna stay on the hip for a few more minutes, and then we are gonna do probably a fair amount of knee conversation with you, 'cause I know you got a lot.
This is just the tip of the iceberg with all the stuff that you do. Um- Yeah,
Will Sanchez: Garcia just wants to talk about knee. He just loves the knee.
Dr. Grant Garcia: I'm trying [00:20:00] not to talk about, I'm trying not to talk about knee 'cause Travis and I will never get off the conversation. So, um, obviously you have a lot of experience with the NBA, right?
You're head team doctor for the Jazz. The... Where do you s- like, from your, again, cartilage and hip stuff, is that part of the algorithm at all with the NBA players? 'Cause it's already ju- it's just barely on the iceberg or tip of the iceberg right now for knee. And so for the hip, is it a different animal or is it, is it...
Are things treated differently in the hip in the NBA?
Dr. Travis Maak: So i- interestingly, hip in the NBA, and frankly hip in all elite athletes, really de- determines on what position they play. Yeah. So a lot of cartilage damage, at least for impingement or FAI, which stands for femoral acetabular impingement, as I know you guys know that already, it's basically the ball banging into the socket when it's not supposed to.
Mm-hmm. That's all that means. That's usually in a deep flexion position. So we see that a lot in y- guards, not as much in centers, not as much in forwards, and when it happens, a lot of it can be alleviated frankly by just changing [00:21:00] their strength training routine. So the nice thing about elite athletes, we have a really close access to them, and when they have pain, we can modify stuff really quickly.
So the first thing I would say is most of this stuff is preventable frankly, by just activity modification, changing the way you strength train, that kind of stuff. So ca- candidly, we can avoid a lot of this surgery in elite athletes, and frankly could probably avoid it in a lot of athletes period. Hockey goalies are an exception.
That's kind of a unfortunately- Yeah ... necessary evil. Um, but having said that, to your point, has it gotten people back sooner? Absolutely. Hip preservation, we used to do all this open actually. Um, any sort of hip preservation was done open, and the recoveries were abysmal. They got back, but holy smokes, you're talking one year.
You're talking nine to 12 months. It, it's... Now we get them back to, uh, elite athletes, a lot of my US speed skaters that I, which is, they get a lot of impingement because the positions they're in.
Dr. Grant Garcia: Yes.
Dr. Travis Maak: Uh, we get them back on the ice within six weeks. We get them back in full competition at four months, and they're skating at levels they weren't skating before surgery at around six [00:22:00] months.
So with, that's even without the cartilage. With the cartilage really doesn't change that. If anything, it, it gets them back feeling better, but does not change the timeline.
Dr. Grant Garcia: Well, that's important for the listeners to hear, right? Because you're talking about additional surgeries you do during the time, but it doesn't add more time to your recovery.
So it's like it's synergistic, it, it almost. And would you say almost in the sense of like if they need it and you're doing it, it might actually improve the overall recovery process? Because now they're not having this defect that's causing pain, and you've already addressed now all the issues. You know, less pain during the recovery always makes things easier.
Will can attest to this.
Will Sanchez: Yeah, I'm just thinking about, you know, the, one of the famous athletes- Hmm ... and, you know, uh, Ken Griffey Jr. also had some hip issues. You know, the, the big one is Bo, uh, Bo Jackson. Um, and you know, the things that he, he never recovered w- on that tackle, uh, on back in '91, and I think- Right
what was that? A vascular, right, uh, necrosis and some other hip issues. That's not a
Dr. Grant Garcia: good one.
Will Sanchez: I mean- That's a tough one ... so it, it ruined his career. He could've been a, who knows, Hall of Famer in football and baseball. I [00:23:00] mean, he was on that trajectory. So it's just, uh, it's amazing. So you talked about the guards.
What are the positions that you're seeing some of these hip issues? Because as we mentioned at the top of the show, you're working with the Utes of the Utah football team. What are some of the concerns or some of the positions that you're seeing? And then how are you getting in front of that with the strength ta- training and being a part of those conversations?
Dr. Travis Maak: Yeah, so really any sport that requires deep flexion positions and rotation in those flexion s- positions. Rotation. So the worst possible scenario, and it's highlighted 'cause everyone's seen it, is the hockey goalie hockey stop that stops- Yeah ... the shot on goal, where they do that flare of their legs. They go out deep.
The butterfly. Yeah, the butterfly. Yeah. Exactly. The butterfly. So that is the hyperflexion internal rotation, squatting down deeply. Holy smokes, that's a tough spot, and the hip does not like to do that. So any position that sort of mimics that position, either that extreme or to some degree similar. So, and other examples would be baseball catchers as an [00:24:00] example.
Mm-hmm. That deep position. Lacrosse players, soccer players when they're kicking, not on their kicking leg, but on their non-kicking leg that they rotate on as they follow through. Are, are you seeing
Will Sanchez: it in bodybuilders that are squatting heavy? Are you, are you seeing it in that kind of area? So
Dr. Travis Maak: it's interestingly sometimes, but not as often, because- Oh
elite bodybuilders, builders do not typically squat with their knees together. They wide squat. So because it gives them a s- a wider base and a s- more stable base, and what that- Or sumo
Will Sanchez: squat ...
Dr. Travis Maak: yeah, so they do a sumo squat- Yeah ... to rotate their legs out to, so they can weight bear more, and frankly, that's protective.
Yeah, yeah. So guards are in that deep rotational position. I, I told you speed skaters, our Olympic speed skaters on their inside leg when they're down in crouch and curving around, that gets 'em. So anything, imagine the sports, you talked about football. So in that case, you're talking about your linemen.
You're talking about your running backs. Not so much your wide receivers 'cause they're standing up and out. So that, that's kinda what we're [00:25:00] talking about.
Will Sanchez: That's
Dr. Grant Garcia: cool.
Dr. Travis Maak: You, you asked how we stop it. I- A quick, a quick little comment there. The answer is modifying your strength training regimen. So the amazing thing when I talk to all of my NBA players, the first thing they come in when we draft them and they come out of high school or college is, "Hey, my hip's been hurting, Doc.
What's going on?" Mm. "I, I stretch it and it makes it worse." And I go, "How do you stretch it?" They're like, "Well, I gotta stretch my external glutes, and I pull it like that. And I bring my knee up and I shove it in my chest and I push really hard." That's awkward. And I'm like, "How's that feel?" They're like, "Not good at, at all, actually."
"But they tell me I gotta stretch my external rotators." I'm like, "Okay, please don't ever do that again." A- and then turns out their pain actually goes away. So just commenting and coaching people on positions to avoid can largely eliminate some of these symptoms.
Dr. Grant Garcia: Well, I think the point you made, and we've had this many times in this, this, uh, podcast, is that these elite athletes, you're able to get to them faster and more focused, and they get to have doctors like you that sees them right away, you know, and says, "This is what you're doing incorrectly."
And it's amazing some of the non-operative treatments that we can perform or we can do for the patients, or that [00:26:00] how much PT helps when it's done correctly and effectively and more frequently.
Dr. Travis Maak: Yeah. And you and I have talked a lot, Grant. Like, the, the... You know, it's interesting because- Mm-hmm ... a lot of people think surgeons wanna do surgery.
A- and I would argue that not if they're good ones. Uh, because at the end of the day, surgery makes you different. It may not make you better, and it certainly can make you worse. Uh, s- it can make you better for sure, but I will tell you, the people it makes the best are the ones that absolutely need it. Uh, and what I mean by that is- Mm
you try non-surgical management first. You try PT, you try activity modification, you try injections if you need them. A- and you and I have talked a lot about this. At the end of the day, your best outcomes are in the patients that have absolutely certain indications for the surgery, and I think good surgeons make sure that's the case.
Dr. Grant Garcia: Yeah. I mean, and, and as what you do, I mean, I think we'll... I wanna talk... Obviously, you guys can already hear who's listening. You know, we're, we're talking about someone that not just takes care of NBA, but is used to, you know, hockey, elite athletes in the, um, in the cold weather sports, you know, skiing. I've [00:27:00] seen some of your, you know, your presentations on speed skaters, downhill skating, you name it.
So you have a lot of experience with different athletes. How... I, I know this, I don't wanna load this question, but how d- does treating them different than your average recreational athletes, not from how you care for them in terms of the care you give them or the- Sure ... options you give them, but it, there is a perspective that's important when you're doing team level or high-level professional level athletics.
You know, there's seasons that matter, et cetera. Can you maybe listen to the audience who wanna hear, you know, they always come in like, "I wanna be treated like a pro athlete." I'm like, "Maybe you don't always want to. Depends on how you treat things." Right? Everything's a little bit different. But so how would you, how do you approach those situations where, yeah, maybe they actually need surgery or it's a borderline scenario?
Dr. Travis Maak: So two things I would say. The first is timing is everything, and elite athletes, the only thing for me that they change is the importance of timing. So you identified it a little bit. So Olympics are actually the hardest, to be honest, because they train for four years-
Will Sanchez: Mm.
Dr. Travis Maak: Yeah ... for [00:28:00] one month of glory.
Really, like a week of glory. So for them, if they get injured nine months before their Olympic trial and they've already qualified or they're qualifying, it is a much higher bar because that's four years of your life and it's one shot. Whereas, not to say that elite professional athletes aren't elite and important, but th- they miss a season Not an entire four-year training period.
Interesting. So at some point, it's a risk-benefit analysis, and that's what I tell all of my patients, whether elite athletes or not. Surgery and timing is a risk-benefit analysis, and I'll give you an example. Even today, I had a high school kid who wants to go, they have a trip planned to Hawaii with their family.
He's graduating, he's a senior. He's done playing sports, actually, and he tore his ACL, and they wanna know, and he has a meniscus tear. And you know this as well as anyone, Grant. He's already a month and a half out from his meniscus tear, 'cause it took him that long to figure out he wanted surgery. Now he's coming to see me, and you know as well as I do, he's a young kid with a meniscus tear that needs surgery, [00:29:00] and likely you're gonna sew it back together.
And outcomes are better between six and eight weeks of repair. So this guy needs to get in basically yesterday- Right. Mm-hmm ... to get his meniscus repaired to have the best outcome for the rest of his life. And I would argue that's way more important than a c- next year's career, or next year's season, if you will.
It's for his life. So he asks the question, "Can I go to my trip in Hawaii in a month and have my surgery after?" And his mom's sitting there saying the same thing. Of course, they don't know any better, and what I have to tell him is, "Well, it's a risk-benefit analysis. You have your, your ha- your Hawaii trip, I totally get it, but the chance of your meniscus healing when you come back six weeks from now is gonna be less than it is if I fix it in a week."
Mm. "And but I, if I did fix it in a week with your ACL, it's probably not gonna be a great Hawaii trip for you, honestly." Yeah. So that's a similar balance. Everyone has to make these decisions. The difference with professional athletes, though, is they have a huge armamentarium of resources behind them that maybe sometimes we don't, and that can be both good and bad.[00:30:00]
So to your point, Grant, do you wanna be like them? Well, it depends. So with the resources, sure, count me in. However, they also have a lot of pulls on their n- their requirements to get back sooner. They have a lot of people kind of chirping in their ear, telling them lots of different things. Some good, some bad.
So sorting through that milieu of confusion can be difficult. I-
Will Sanchez: is it a contract year? You know, are you, are you t- you know, like, you know- Yeah ... three years out of four years, you know, you have a player that needs a surgery and, you know, they rush him back because they, you know, they, they wanna average X amount of money because this might be their last contract and last time to...
So I, I can imagine, that's just one scenario. I can imagine all the different scenarios- J- ... at, at, at that professional level.
Dr. Grant Garcia: For the listeners, and this is just diving into the, uh, the professional athlete level. Who, who do you usually have chirping in the ear? I think they probably were curious. You know, I know you have the agents, you have other doc- you know, is it, you're the, you're a very good doctor, but I'm sure a lot of the pros get extra opinions.
I know how it works. They fly all over the place, and you [00:31:00] gotta either deal with that conversation or whatever. Um, so what do, what do you see as the outside sources for these pro athletes that cause this situation to be more challenging?
Dr. Travis Maak: Well, I'll give you an example. Uh, a very recent one actually, and this is in the media, so you can Google it.
I'm not telling you anything that's not already out there. But, um, patients of mine, elite athletes that you evaluate, f- you find things sometimes. And then there have to be press releases about them by, by regulation through the NBA. Mm. The second that press re- release goes out, everybody has an opinion.
You have people w- uh, that want to weigh in. They want to be the experts. They want to market themselves. And I get a l- there's a lot of them are critics. Honestly, it's really easy to be a critic, I've learned. Super easy to throw stones if you have no responsibility for the consequences of the stones. Mm.
But I've also learned we all live in glass houses, so I never throw stones at the end of the day, uh, at anyone. So I will tell you that a lot of these people will write things. They'll, they'll, they'll chirp on Twitter. They'll [00:32:00] say- Mm-hmm ... you know, "Shouldn't have ever happened," or, "This was intentional," or, "For the Jazz, they're trying to tank, so they found this one thing that isn't true."
Mm. And you can imagine as a professional athlete, you go, "D- dude, my knee hurts. Like, I don't want it to hurt. I never asked for this. I don't want surgery." These guys don't want surgery. They're not trying to make these things up. It's just frankly not true. Mm. Uh, but unfortunately, they have to deal with the perception that they are trying to make this up, that they're getting unnecessary surgery just to not play.
And I will tell you, if you sit back for a second, none of you would do that. No one would do that. And they don't either. It's crazy. But the problem is they have to listen to this stuff, right? And they have to get multiple opinions. And of course, when you get multiple opinions, as you know, Grant, 'cause you're a third opinion doc, everyone comes to you for second opinions, and you give them a good one, thankfully.
Um, but I will tell you, there are a lot of people that feel the need as a second opinion doc to say something different.
Will Sanchez: Yeah.
Dr. Travis Maak: Uh, because if you're an elite athlete and someone's like, "Well, that guy didn't talk to you about this, but..." or, "That lady didn't talk to you about this, but I, look at what I found," all [00:33:00] of a sudden you sound smarter.
But here's the thing. The goal is not to do that. The goal is to deliver the best care you can period, irrespective of what other people have said. And that's what I try to do with all my athletes i- is let them sort through the process. And frankly, I, I don't have any interest in operating on them or not operating on them.
I don't care. I tell all of my elite players of teams that I cover, "Look, I'm an opinion. I'm happy to take care of you. But I'm also happy to have someone else take care of you and, uh, and help you sort through the process. Ultimately, my goal is for you to have the best outcome, whatever that looks like for you."
Dr. Grant Garcia: Well, I think it's important for the audience to hear what you just said because that's a challenge, your second or third opinion. You wanna be respectful of the first opinion, second opinion, because if you start, first off, it, you think it may feel, make you feel better, but the people are gonna come back and they're gonna talk to the other doctor sometimes and be like, "This guy said this, that you were crazy."
Like, it's just not a good idea, as you keep saying. Like, it, there's no... You don't get away with that. We have that... I know of many people I can talk off the top of my head and from the city that I have heard about those scenarios. So you just wanna be careful, right? And [00:34:00] the other thing is it's really, it does a disservice to the patient, as you're saying, whether it's an elite athlete or a regular athlete or anybody off the street, 'cause then they confuse them.
And when you confuse them, then they can't make an, uh, the regular decision. You know, your whole goal is not to make yourself smarter than the person that saw them previously or pretend that you're smarter. It's to give them the opinion, like you said, completely unbiased. And many times, and I tell them that actually the best opinions are when, like, three people say the same thing.
Like, I ca- I sent someone for another opinion today and I was like- Mm-hmm ... "We're doing a big knee surgery," and I say, "Why don't you get another opinion? And I hope it's similar, 'cause that way at least you won't feel like we're totally out of line." 'Cause this becomes really challenging to make the right decision, right?
If you're a patient.
Dr. Travis Maak: Uh, you know, it's fascinating. The, the other flip side of the coin is also equally good, I will tell you. And the reason I say that, so when I was first starting in the NBA, and it was 12 years ago, uh, I've done this for a long time now. So my... The first guy I operated on, um, I saw, I'd literally barely started taking care of the team, and he had an injury in his shoulder, and I, I told him [00:35:00] what I thought was going on, and then he flew around and got four other opinions, okay?
In addition. Which, uh, they're totally fine. That's pretty standard, actually, um, for the NBA. The fascinating thing, every single one of those opinions, and these are all well-known, very good doctors that I respect highly, said something different. Every single one of them. So by the time we were done, he had five opinions from five doctors, all that said something similar but also different.
So at the end of the day, the good news was I could do whatever I wanted because someone had said it was right. Like, w- pick your poison. It was right. I'm like, "Well, you know, that's good news." So that's what I do. Well,
Dr. Grant Garcia: that's, that's a very rarity that you got to have a dealer's choice jokers.
Dr. Travis Maak: Yeah, yeah. It was fascinating.
Dr. Grant Garcia: Oh,
Will Sanchez: my God ... Can you talk about that a little bit? Um, g- how did you become the NBA Physician Association, like the president? Like, how, how did that come about? I'm just curious.
Dr. Travis Maak: That was dumb luck, to be totally honest with you. I, I mean, honestly- So- He's
Dr. Grant Garcia: so... He's humble ... you guys can see it already.
Everyone's listening, they're like, "No way that guy was lucky to get it." [00:36:00]
Dr. Travis Maak: No, it's true. I, so the, the truth is, I, I'd done it for a long time. I was the old, one of the old guys in the room. And I, I think for better or for worse, when I get irritated by stuff, I usually raise my hand and say something. Um, a- and that's both good and bad, okay?
'Cause sometimes it's not anything anyone wants to hear. So I, I think in the room there were a few things that really bothered me. Um, and, and- So in the process of having conversations and asking questions, I think the questions that were a- that I asked echoed what a lot of people in the room, the other NBA physicians were thinking.
Mm-hmm. Um, and so I think that's really what kind of made it, made them... And I also was involved. I d- I chaired the, the NBA Research Committee for a while, so I kind of understood how the inner workings of the NBA with the NBA teams worked. So it was a combination of those things a- and frankly, just asking the questions that I think everyone else maybe was thinking but didn't wanna ask, 'cause they were a little irritating.
Will Sanchez: Yeah.
Dr. Grant Garcia: Um, [00:37:00] on the NBA, I know obviously you're pretty involved, do you know, I mean, obviously there's w- there's a trend right now, I mean, what's your trend or how do you guys work on injury prevention and working on athletes' health? I mean, obviously it's important. We talk about this all the time, you know, nutrition, recovery systems, things like that.
Yeah. But what are you guys doing to advance that? 'Cause obviously every time some player gets injured, it's a lot of money lost for the Utah Jazz-
Dr. Travis Maak: Yeah ...
Dr. Grant Garcia: to, or any of those players you take care of. It's a player for the m- the player can lose money from their contract or not get re-signed, or, and as you guys, you don't get the output, right?
You don't get a playoff or you don't get a championship.
Dr. Travis Maak: Right. Right. High risk. So here's what I'll tell you. W- when I'm asked, and the, the Jazz organization's phenomenal. I'm, I'm blessed to be able to take care of such an incredibly confident and honestly supportive organization. Some d- I, I think some docs aren't quite so lucky.
Yeah. Um, but I, I do consider myself very lucky. So in that capacity, they, they really do listen to me. Uh, but sometimes they'll say, "Hey Doc, uh, how do we make it so our players never get hurt?" A- and I say, "That's, that's..." Like, I have a total understanding. That's a
Dr. Grant Garcia: very good, that's a [00:38:00] legitimate question, though.
Dr. Travis Maak: Yeah. 100%. Uh, it's like, it's a business. And I have a, I have an absolute certain answer for them every time, and the answer is, "Set them on the bench." Like, 100%.
Will Sanchez: Yeah.
Dr. Travis Maak: Like, uh, don't ever play them, and they will never get hurt. The, the problem is that's not reality. So I harken back to one of our elite s- uh, alpine skiers who was an Olympic gold medalist, and she sat in a meeting.
It was a huge conference, and she was the keynote speaker. It really hit me hard. This was years ago. Um, and she said, "You know, this is called the inj- the Consortium for Injury, I- Illness and Injury Prevention for the USOPC," which is U- U- United States Olympic and Paralympic Committee. She said, "The first thing I'm gonna tell you is that term, injury prevention, is offensive."
Ooh. And I said, "Wow." Uh, and e- it was like a pin drop. You could hear a pin drop in this place, 'cause it was literally the conference title, okay, for the whole thing. And the
Dr. Grant Garcia: c- conference title is this-
Dr. Travis Maak: And everyone's looking at each other like, "Oh, boy. Where are we going from here?" And she said, "It's not that, [00:39:00] it's not that y- you're not wrong," uh, or, or, "It's not that you're wrong.
It's just that injury prevention is a fallacy, because any athlete that puts skis on, that straps on shoes, and goes out and plays a sport is going to get hurt." It is fundamental to what we do, because you put your body and you push it to the brink, and sometimes you cross the brink and you get hurt. So when you say there's something like injury prevention, then the athlete feels like somehow it's our fault we got hurt, and we should have been able to prevent it.
She said, "Here's what I'd suggest. You should call it the consortium of an, of illness and injury mitigation, because that's really all we're doing, is trying to reduce but not eliminate the risk." And it was really interesting to hear her phrase it that way, 'cause she's totally right. At the end of the day, that's what we do.
So how do I apply that to the NBA? The answer is, [00:40:00] lots and lots of biomechanical engineers that are way smarter than I am. We do force plate analyses, we do 3D motion capture. We, we watch them move all the time. We, we check their electrolytes. We make sure their labs, vitamin D, calcium, s- all of this stuff is constantly monitored to really push their bodies safely to the brink without crossing it.
Because at that level, just like Olympics when you're talking about a split second or even a millisecond difference, that push is the difference between winning and losing. Uh, but you push too far, and we've seen it in the last Winter Olympics, then you get injured, and that brink is the end. Hmm. Yeah. So th- that is a really narrow gap, but there are lots of things that we explore to try to push them safely.
All, the other thing- That's awesome ... is a huge credit to the NBA league. They have developed a huge database that's a curated database. So any time an athlete gets hurt, it's very specifically inputted into the NBA EMR. It's curated. We have an incredible stat [00:41:00] system called IQVIA that constantly evaluates it, and we get updates quarterly on, here are the injuries.
We see an uptick in here. This last one was Achilles tendon tears. The second Achilles- Yeah ... there were a lot of guys that tore their Achilles. Yeah. Everyone heard about it. Holy crap. Like, what's going on, right? So I can tell you, the first thing that happened, we all sat down, and within a week, developed an elite expert consortium on Achilles tendon tears to say, we l- we had Bob Anderson, we had Marty O'Malley.
We had a lot of folks in the room, myself included, although they was the ex- they were the experts, not me. Um, to kind of talk about this, to say- Yeah ... "Look, let's look at the data. Let's look at the analytics. Let's take the video motion capture of every game, analyzing loads. Is it overloading them?" And people talk about load management.
It's real, okay? It's not like trying to stop- Right ... players from playing. You push them to the brink, and you don't want to push them past the brink, 'cause then they tear something. I know everyone wants to watch their, their favorite player, but d- you don't want to watch them get hurt. So pushing to that brink is the game.
Dr. Grant Garcia: Got it. Well, Will, this is super interesting. Th- like, sorry, Will, [00:42:00] ask your question. I want to make sure we talk
Will Sanchez: about as
Dr. Grant Garcia: much-
Will Sanchez: No, I, I, I kind of wanted to stay with the NBA a little bit. Uh, obviously on, uh, February 3rd, the Jazz traded for Jaren Jackson. Two weeks later, you're working on him and operating on him.
So it's two questions, really, is- He's,
Dr. Grant Garcia: he, I don't even know if he wants
Dr. Travis Maak: I, I'll say what I can. I'll say what
Will Sanchez: I can Yeah, yeah. So whatever you can-
Dr. Grant Garcia: Well, no, he actually, we read the news article. It's in the published news article
Will Sanchez: Yeah,
Dr. Grant Garcia: so he wants- What were you saying? What do you want to ask him, Will? Ask him
Will Sanchez: to- Well, one, the, the surgery, right?
Because this, you know, Jaren Jackson is a big-time NBA player, right? So g- just the type of surgery, and then also I'm curious, and you answer whatever you can, is do you, uh, is management and general managers having these conversations knowing that maybe a player's already injured before they're making a trade, this huge investment- That's a good question
coming over, and then you're saying, "Yes, you know, I've looked at his, uh, whatever it is, and I recommend this trade. I think we're gonna get him going. He's gonna be an incredible part of this Utah Jazz in the 2026-2027 seve- uh, season."
Dr. Travis Maak: So I will, [00:43:00] I'll answer this in a somewhat of a vague, nebulous answer without- Sure
directly applying it to Jaren Jackson Jr. Sure. So, um, in general, this is how it works. Yeah. So i- if a player's getting drafted, or in this case traded- Mm-hmm ... especially a high-value player, but I will tell you any player by definition is high value. Yeah. Uh, he's really expensive though, 'cause he's an incredible player, obviously, as you know.
Will Sanchez: One of the top players in the NBA.
Dr. Travis Maak: Yeah. 100%, and an amazing human too, by the way. Yes. So what I will say, the way it works, the, the draft gets made, uh, the teams agree, a- and then they say, and this is true for all dra- all trades, okay? Yeah. So the trades get made. They say, "Okay, fine." Both teams agree, and then they fly the players in and, and we evaluate them, and they give us- Right
all the information. The team doctors and the teams are very open about what injuries they've had. We review and get access to their EMR, and it's very selective. So, um, I only get granted access for 24 hours or 48 hours, depending on the time- That's fantastic ... to, to his, to his EMR. And at that [00:44:00] point, I get to review all of his injury, uh, history, all of the notes, everything.
Just like you're, you're seeing a pl- patient, right? So you review previous r- Yeah ... it's the same story. So I see the i- images. I see, read, read the reviews. I see the doctor's notes, et cetera. Then they fly him in and I examine him, and the players are really open about everything. People think they hide stuff.
They don't hide stuff. It, they, they, it's not in their best interest to do so. They, they wanna be healthy too. So they actually like the process, I think. I've never actually asked them, but they s- I think they do, uh, in the sense that they get lots of doctors always taking care of them. I mean, I'm sure it gets onerous at times, but for the most part, they like the new opinions and new views.
So they, they're very open. They say, "Look, I've had this surgery or I've had that surgery. Yeah. I have this thing that's kinda sore, that thing that's sore. This is how I treat it." Same like a patient when you go into the doctor's office, right? Same story. So at that point, we evaluate them, and if they've had stuff that we wanna make sure looks okay or if they're having soreness, then we get a full battery workup, just like you would, would a patient.
Mm-hmm. So we get x-rays, we get MRIs, we evaluate all of them, and then once that's [00:45:00] done, then we say, "Yes, they can..." They pass the medical physical or they fail the medical physical. Mm-hmm. So it's very rare to fail a medical physical, okay? So that is something where, uh, to be honest with you, I don't think I've ever failed anyone, honestly.
Um, in a, in a trade. Now I've failed people in the draft, but I have not failed people in trade.
Will Sanchez: Interesting.
Dr. Travis Maak: So failing means you physically, you're, you like from a physician's standpoint believe that their participation in the sport of basketball or a sport is dangerous to their health.
Dr. Grant Garcia: Got
Dr. Travis Maak: it. They cannot practice or play safely Okay?
So that, that's kind of where this ... And that came into the, the conver- conversation the last Olympics, as you probably know. So, so with Jaren Jackson Jr., that was the conversation. We knew everything in advance. Yeah. Um, for, a- a- and you know, and, and then you have a conversation, and that includes the patient or the player, and they're the same thing here.
And then you have a conversation about what's best for them and what they wanna do.
Will Sanchez: [00:46:00] Mm-hmm.
Dr. Travis Maak: And then y- you get with the team, and ultimately it's the same principles, and this is what people don't understand, that it's not any different for a trade than it is a patient, which is can you play with this? In his case, do we have to take this thing out?
What are the risks with taking it out? What are the benefits with taking it out? Like, does it hurt you? Does it not? It's just, it's literally the same thing as taking care of a patient, it's just the stakes are maybe a little bit higher. But I would argue not that much higher- Yeah ... 'cause I mean, I don't want, I don't want my knee to get messed up either.
Yeah.
Dr. Grant Garcia: Yeah. Great. No, that's perfect. Um, on a new note, 'cause I wanna show this part, can we pull up the slides? So one, you, we talked a lot about hip. I'm not gonna get as much time with you on the knee, which is sad for me, but we'll figure it out. That's okay. Uh, but- A
Will Sanchez: little bit.
Dr. Grant Garcia: Also, you talked about cartilage from somebody else.
Obviously- That's a knee ... you have a wait list. That is a knee, yes. We finally got there. Uh, but you know, cartilage transplants, I do a lot of them. You do a ton of them. I've seen your stuff on it. But one thing that's really cool is, like, you talk about you've already done a lot of innovations. I mean, you talked about the one, the thing that, you know, that I- [00:47:00] AMSET?
AMSET? I can't even say it right. Yeah, AMIC, dude. I told you- AMIC. AMIC ... it's terrible. Just call it AutoCart.
Dr. Travis Maak: That's really what it's called now. AutoCart.
Dr. Grant Garcia: Yeah. Right? Like a huge jump, right, forward with cartilage. You're now trying to do another cutting edge technology for cartilage transplants, right?
Because while AutoCart's great for many scenarios, especially hip or some smaller lesions in the knee, um, the cartilage transplants is still a high work course for us, some of us cartilage surgeons. So review this, you know, briefly obviously. What, what jumped you to this? And maybe go to the next slide, Will.
And so for the sake of time he can kind of go over some stuff that he's, uh, discussed.
Dr. Travis Maak: Yeah,
Dr. Grant Garcia: so- So, like, tell us a little bit about this.
Dr. Travis Maak: Yeah, so bottom line, as you know, Grant, 'cause you and I do a lot, a lot of this, bulk osteochondral allograft transplant, so that's taking cartilage from a donor, um, and living cartilage, just like a transplant, and transplanting into a person who we talked about before have a h- has a hole in their cartilage and pain from it, is an amazing thing.
So it's a true living pl- transplant. And cartilage, for the listeners that may not know, is something [00:48:00] we call immunoprivileged. Meaning we talked about AutoCart. That's taking the patient's own cartilage. That's fine 'cause it's your own. But this is taking someone else's cartilage and their bone and transplanting it into a person who needs it.
So interestingly, the cartilage, I can take my cartilage, Grant, and put it in you. Although you're younger and healthier, so I want yours instead. Um, and that's totally fine. But the problem is, a- and bone actually heals really well. So taking cartilage and bone and transplanting that is incredible. Now, you can't trans- transplant, transplant the bone marrow, so we gotta be a little careful with that, and there are ways to get around it.
But one of the downsides of osteochondral allograft transplant is that the curvature has to fit. So what does that mean? Well, you can't put a car tire on a truck. It doesn't work because they're different sizes. They're both tires, but it doesn't fit. So this is not like a transplant where you have to match the heart and all the cells and all that fancy stuff that I'm not smart enough to understand, but instead, you have to match the curve.
So you [00:49:00] have to get a person's own bone and cartilage and match it with someone else's own bone and cartilage. Now, there are places that that's easier, but there are places that's really hard. So one of the examples, as shown here, is the trochlea. So that's the groove that the kneecap or patella runs in.
It's got a unique curvature that's really hard to match, and then you get your, do your best effort, and then surgically it's really hard because if you transplant it incorrectly and you pop it in, you gotta-- it's a one-shot deal. If you get it wrong, that chip is cooked. So that's it. You don't have another chance, and you say, "Ah, I'll get it better next time.
Nothing else I can do." So what-- I found it very complicated and hard. I told you, I'm not very good at stuff, and I find problems, and I like to fix them. So I wanted something that, instrumentation that could make me a better surgeon, which is not that hard to do. Um, that's the first thing. The second thing is I had a patient, I told you I don't like things that make me angry that I can't fix, and this was one of them.
I had a patient with a cartilage defect on the top of their shin bone called the tibial plateau, and that's what's shown- That's there on
Dr. Grant Garcia: the right, [00:50:00] guys, for
Dr. Travis Maak: anybody listening ... yeah. So it's crazy because there it looks easy to transplant the-- but the problem is the femur's in the way, so the other side of the knee.
So you can't get there, and you literally cannot, or at least it's really hard, arguably almost impossible, to put a cartilage and bone transplant into that place. But I really wanted to do it because they do so well, especially when the bone is bad. You gotta fix the bone, too. So I got really frustrated watching these patients come through my clinic and, and saying, "There's nothing I can do for you."
An orthopedic surgeon in classic fashion, when we don't have an option, then we t- say to ourselves, "Ostrich, put your head in the sand. It doesn't exist." And we say, "Ah, you don't have to treat it anyways. It's gonna be fine." But I would argue if it's not fine on the femur, why is it fine on the tibia? The, the, the answer is 'cause you can't get to it, so you just convince yourself it's okay.
So good news, we can get there now because I got really angry, and some people much smarter than I am helped me. Biomechanic engineer Zach Evans, Wade Fallin, they helped me out w- at the University of Utah to develop instruments that allow us to [00:51:00] get there now. So this is the ChondroMatch family. It's a comprehensive osteochondral repair transplant system.
ChondroMatch Standard allows you to do a very fast and easy transplantation technique using this amazing little guide here. Um, it-
Dr. Grant Garcia: Oh, he's gonna show it.
Dr. Travis Maak: Oh, yeah. It's got little four feet. Um, it can transplant directly on it. I would even say, you see this? This is an ankle. It's a talus. It's super hard.
But look at that thing. It lines up perfectly All you have to do is take the four feet, you pop it on. No matter where you pop it, it finds its spot. And the same thing in the knee, it's the same story. In the trochlea, it can find its spot. But holy smokes, this is small. What if it's a really big defect? So this is the trochlea, right?
There's a big hole here, and if you wanna match that hole, that is tough. So if you come in with a circular piece, look at that. It doesn't fit. Yeah. You gotta kinda guess, right? And this is what you and I do right now, Grant. We guess. We put this in here. And thankfully for you, you're a really [00:52:00] good surgeon, so your guess is as good as anybody's, is very educated.
But for me, I'm not so good at guessing. So what do I do? Well, I come up with something that makes me better, and that's this guy. It's, it was designed, and we came up- This is the
Dr. Grant Garcia: coolest thing I've ever seen, by the
Dr. Travis Maak: way. Yeah. So this is- This part is sick ... it came up from our, a game I used to play when I was a kid.
My parents got me this hand- ... where you could stick your hand on the nails, and it made an imprint of your hand. All good, uh, good things have already been invented for kids, just so you know. Uh, so at the end of the day, Better Nails was the idea for this. So I said, "Well, if it can take an imprint of my hand, it can take an imprint of the trochlea."
So good news, that's exactly what this does. These little Better Nails push down, they're little spring-loaded, and no matter what I do, they stay right where they're supposed to be. And then you kinda take the imprint of the patient, in this case we'll drop it down here, and then you screw this thing down like that, and next thing you know, you've got-
Dr. Grant Garcia: That's awesome
Dr. Travis Maak: Better Nails. And look at this. You put it here, it doesn't fit. But look at this, you just screw it home, and it sits right where- Right ... it's supposed to be. Sits right where it ... And then
Dr. Grant Garcia: you can- We'll put all of us up on the screen while he's talking. So for e- for [00:53:00] all the viewers that understand that this, you know, they don't...
If you're an orthopedic surgeon watching this, which is what a lot of people are that watch this show, they're gonna geek out when they see this because they don't understand how hard this can be. Yeah. So he just basically used a simple toy and figured out a way to make a very hard portion of the surgery.
This is the, the trochleas, in my opinion, are the hardest- Yes ... of all the major transplants. And then he also found a way to fix the plateau, and you guys may or may not, the reason I had him talk about some of this, and we can talk about it now, is there was a press release 'cause you were the first one in the country to d- use that technique, um, on the reversed tibial plateau- Yeah
which is really good. So I think what's interesting for the listeners is that not only are you talking about all the cool stuff you're doing, and giving the updates, and helping out the NBA players with non-surgical treatments, you're finding ways to innovate already complicated procedures, or you're taking things to the next level so that us, so the surgeons, the regular population of surgeons, can take care of patients better, which is really awesome.
Dr. Travis Maak: I'm gonna geek out one more, Grant. The reason this all came back, it came full [00:54:00] circle, and the person, the genius behind all this is not me, actually. In addition to the two people I mentioned before, it's Charlie Saltzman. So he's a mentor to me. He was my chairman before. He's a foot and ankle surgeon that since retired.
He and I did a lot of osteochondral allograft transplants to the talus, and holy smokes, those are hard. Uh, the reason is they sit right here on the corner. So now, Grant, you'll get this 'cause you do this a lot. Now imagine getting tran- taking a transplant like this, okay? You have to come at it through a malleolar osteotomy like that.
So now you have an angle like this. You also have a translation this way and a translation that way. So you have an X, Y, and Z axis that you have to match, and then you put your graft in this way 'cause you can't come perken- perpendicular because the- So
Dr. Grant Garcia: you got it. You're putting it in with an edge, and so it's not a contained.
Correct. You're basically trying to put a plug that's cur- Oh my gosh. So that's why- On the- ... that new thing is gonna be better ...
Dr. Travis Maak: on the shoulder, okay? Right here.
Dr. Grant Garcia: Will, this is like, this is like shooting a bullseye from, like, 1,000 [00:55:00] yards out.
Dr. Travis Maak: So check this out, man. So here we come in. You get your angle right, right here.
You don't know what it is, but guess what? That's your answer, and then you come into the donor. You lock it in. You have your angle. It's dummy-proof, and I like to call it Mack-proof. So you come in like this, pop it in. You've got your graft. No longer do I have to sweat bullets 'cause Charlie would sit over me with his glasses like this
Is it gonna be perfect? I'm like, "I don't know, sir. H- I mean, I sure am gonna try." And that's how it went. So that was the design.
Dr. Grant Garcia: So he scared you into doing this. I like that.
Dr. Travis Maak: Oh my
Dr. Grant Garcia: goodness.
Dr. Travis Maak: That- Terrified. 'Cause he was my chairman, and I, I was al- like, I was like three years into practice. I was terrified. Uh, so we got pretty good at it.
He's actually been subsequently an incredible mentor to me and helped me design this whole thing. Um, and the impetus behind it, he was super supportive the whole... He's like, "We, you gotta do b- this is better. Yeah, give yourself stress for this, Travis. We, we [00:56:00] gotta do better than this." So he in concert with the Orthopedic Innovation Center, the OIC, was, was the genius behind this.
Awesome. So we're super excited about have... getting it out there to everybody. And I, Grant, you're on the list, buddy. We're gonna send you some sets pretty soon.
Dr. Grant Garcia: Dude, I am so excited. Yes. Um, Travis, as I said, we were gonna try to go 45. We're at 56 minutes. We have to cut off at one hour or social media will be mad with us.
Oh, you're good. So we're gonna let you go. Um, Will, I know you got a billion questions for Travis. I,
Will Sanchez: w- uh, we're just... Yeah, we need two
Dr. Grant Garcia: more
Will Sanchez: hours.
Dr. Grant Garcia: You're overwhelmed.
Will Sanchez: I wanna keep talking to
Dr. Grant Garcia: you. You're
Will Sanchez: overwhelmed. NHL, hockey,
Dr. Grant Garcia: wres- This is a six-part series, everyone.
Will Sanchez: Yeah, yeah, yeah. Let's talk... I want... I'm getting to Lindsey Vonn and the injuries and the, and the mindset-
of the pro athlete and ev- we got too much
Dr. Grant Garcia: stuff. Oh
Will Sanchez: my God. We just wanna thank you- Travis,
Dr. Grant Garcia: where do you... Well, one second. Where do you see the future for some of these things? And I mean, you already showed the future right there. I mean, this isn't even out. Like, or you're the only one. That's the first time I've ever seen this.
This is incredible.
Dr. Travis Maak: Yep.
Dr. Grant Garcia: So where do you see the future for some of the cartilage stuff that you're doing? Again, briefly as possible, and then Will, [00:57:00] uh, Will finish up any questions.
Dr. Travis Maak: The, the future is in biologics in my opinion. So ultimately, it's gonna be taking stem cells, and I do this in my lab as well.
We can cr- take stem cells from juvenile chondrocytes from that little tiny finger, the sixth finger that we throw away. You may remember, Grant, kids that are born with six fingers. You cut the third, the sixth finger off. That has great cartilage. I can take it to my lab right now. I can ca- take juvenile chondrocyte implantation sheet, stem cell sheets and put them down.
That's where it's gonna come. So at the end of the day, a lot of this stuff is, I mean, maybe in my lifetime, I don't know. Hopefully. Uh, but down the road, a lot of this stuff is not available in Europe. It's not available in the Asian countries, the osteochondral allograft transplants. We can fut- in the future, we're gonna be able to create this stuff.
Not from people- Yeah ... who had unfortunate accidents, but synthesize it in our lab in bulk fashion and have it ready to go in the OR. That's the future.
Dr. Grant Garcia: Awesome.
Dr. Travis Maak: We're almost there.
Dr. Grant Garcia: Will, anything closing?
Will Sanchez: No, we're just gonna thank you, Dr. Mac. Thank you [00:58:00] so much for spending time with us. Check us out, sportsdoctalk.com for great interviews, uh, transcripts, and so much more.
Uh, once again, Dr. Garcia, another great one. Say goodbye, Dr. Garcia.
Dr. Travis Maak: Appreciate you both. Thank you so much.
Will Sanchez: Take care. Bye.
Audio Transcript
Dr. Marc Pietropaoli: Knee Repair, Not Replacement

Today on Sports Doc Talk, we’re excited to welcome Marc Pietropaoli, MD, founder of Victory in Motion and the visionary behind Knee Repair, NOT Replacement®.
Sports Doc Talk Podcast – Guest Introduction
Today on Sports Doc Talk, we’re excited to welcome Marc Pietropaoli, MD, founder of Victory in Motion and the visionary behind Knee Repair, NOT Replacement®.
Some good topics to talk about based on the slides:
-The book and the $1 vs $1 million challenge are good to talk about.
-The “cycle of insanity”
-DataBiologics Registry Results
-Dr. Hernigou’s study data
-My introduction to orthopedics where I was told there was “No way to cure arthritis, no way to grow back new cartilage and no way to repair a knee and not replace it” in the first day of my orthopedic rotation as a 3rd year medical student.
-Being the first surgeon in the world to perform an FDA indicated non-research study BEAR (Bridge Enhanced ACL Restoration) surgery on 10/29/21
Sports Doc Talk Podcast – Guest Introduction
Today on Sports Doc Talk, we’re excited to welcome Marc Pietropaoli, MD, founder of Victory in Motion and the visionary behind Knee Repair, NOT Replacement®.
Dr. Pietropaoli—often known as Dr. P—is the #1 Amazon bestselling author of Repair, Not Replace: Natural Joint Relief Without Surgery or Pills. His mission was born in 1994 during his third year of medical school, after witnessing his first orthopedic surgery and being told a knee “could not be repaired.” That moment sparked a lifelong commitment to finding a better way.
With over 27 years in practice and more than 30,000 patients treated, Dr. P specializes in regenerative and movement-based care for active adults whose knee, hip, shoulder, or joint pain threatens the life they’ve worked hard to build. He travels internationally teaching on regenerative medicine, joint health, longevity, and restoring mobility—challenging the traditional “wait until it’s bad enough” mindset.
Perhaps most boldly, Dr. P has set a mission to end the need for joint replacement surgery by 2043.
Today, we’re diving into the biggest misconceptions about arthritis, the dark side of knee replacement surgery, and what it really means to repair—not replace—the human joint.
20 Sports Doc Talk Podcast Questions for Dr. Marc Pietropaoli
Origin & Philosophy
1.Take us back to that moment in medical school in 1994—what did you see in the OR that fundamentally changed your career path?
2.You built your entire philosophy around repair, not replace. What do you think medicine got wrong early on when it comes to joint degeneration?
Arthritis & Aging Myths
3.What are the biggest misconceptions patients—and even physicians—have about arthritis as we age?
4.Is “bone-on-bone” really the end of the road, or is that an outdated narrative?
5.How much of joint degeneration is truly “wear and tear,” versus movement patterns, loading, and lifestyle?
The Dark Side of Knee Replacement
6.You’re outspoken about the downsides of knee replacement—what don’t patients hear during the consent discussion?
7.In your experience, which patients are least likely to be satisfied after a knee replacement—and why?
8.How do revision rates, persistent pain, and functional limitations factor into your concern about overuse of joint replacement?
Regenerative & Movement-Based Care
9.When you say “regenerative medicine,” what does that mean in real-world practice—not marketing terms?
10.Where do biologics, injectables, and movement retraining fit together in a successful joint repair strategy?
11.What role does the nervous system and motor control play in joint pain that imaging alone misses?
Active Adults & Longevity
12.Many of your patients are active, driven people—what mistakes do high-performing adults commonly make with joint health?
13.How should athletes and weekend warriors think differently about pain versus damage?
14.What does joint longevity actually look like in your 40s, 50s, and 60s?
Evidence, Skepticism & Collaboration
15.Skeptics argue regenerative care lacks strong evidence—how do you respond to that criticism?
16.Where do you see traditional orthopedics and regenerative medicine overlapping rather than competing?
17.How should patients evaluate clinics offering “regenerative” treatments that may overpromise?
The Future of Joint Care
18.Your goal is to end the need for joint replacements by 2043—what has to change in medicine for that to happen?
19.If you could redesign the musculoskeletal care pathway from scratch, what would it look like?
20.For listeners dealing with joint pain right now, what is the single most important step
they can take before accepting surgery as inevitable?
Audio Transcript
NIL_ Health & the Making of a Student Athlete With Scott Laigo

[00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez. You know who this guy is. This is our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia, the busiest man that I know. I don't know how you do it. Um, you've got... Let me see. You got people in your office. You've got surgeries. Every time I looked up on LinkedIn, you're at Arthrex, you're in Denver, you're in Florida, you're in California.
By the way, you went on vacation with your family. You're in Costa Rica. You're surfing. You're... How do you have the time? I think I'm busy. You're putting me to shame. You get-- you have time to work out. You eat right. Uh, listen, uh, do you... Are you time traveling? What, what's going on, and how [00:01:00] are you doing? I'm good.
Uh, well, you know what? I think it's, uh, maybe it's a lack of sleep. Who knows? Uh, trying to do too many things at once, but, uh, unfortunately there's lots of different parties involved and, uh, wanna get as much done as I can, so we gotta maximize. Gotta be efficient. Man, I don't know how you do it. I don't know how you recover, but somebody that knows about recovery, that's Mike B and the Recovery Shop folks.
You like that little segue? Shout out to Mike B and the Recovery Shop. Beautiful. Folks, give us a little insight on why you love the Recovery Shop. Yeah, I mean, just a couple days ago I had a surgeon I chatted with. You know, they, they really, their patients keep asking me like, "I want something extra." You know, like, "I'm, I'm happy with the surgical eval- evaluation, post-surgical discussion, but I just don't...
I need the nutrition. I wanna talk about other options for, you know, ice options, et cetera." And so this allows my patients to get the next level in care. It's essentially, you know, a higher [00:02:00] level pre-evaluated sort of Amazon for recovery items. Mm-hmm. And so the patients can go this way with, after their, you know, when they're deciding their surgeries, and it's a really great option for them.
It makes the patients, you know, allow to have more options and feel like they're getting everything they ask for, right? It just answers all their questions. There's a lot less, "Well, I read about this, I thought this, I wanna do this after surgery," and it's there. So it's awesome. So reach out to Mike B if you're an interested surgeon.
If you're a patient and you're about to get surgery, reach out to Mike B too. Mike B'll tell you who works with him, and they can work with you. Yeah. And, um, you know, we talked about it before. I've had experience working and, uh, and experiencing the Recovery Shop and, and the great items that they've had to help me recovery.
So, uh, from a patient's point of view, I'm giving it two thumbs up. That is my approval. And, uh, for those that are on the show, looking at the show, as you can see from the title, NIL Health and the Making of Student Athlete with Scott Ligo. Scott Ligo is a former [00:03:00] coach. He is in the coaching life. The family's in the coaching life.
I mean, this guy is the real deal. He's the president of the Student Athlete Advocate. Let's welcome Scott Ligo to the show. Scott, thank you so much. We're so happy that you can be a part of this and have discussions not only about NIL, but also the safety of the college students. Uh, we're thankful for you, uh, being on the show.
Man, how are you? I'm good. Uh, thank you for having me on, and, uh, you guys already made me tired by just listening to both of your schedules. So I think I'm just gonna go and get myself some recovery just listening to your schedule. So, but that, that's awesome. Thank you, Scott. Uh, listen, um, listen, let's start there, right?
We talked about, uh, the student athlete advocates. Explain, uh, explain what you're doing with them. You've been doing this for quite a while now. So as we... before we get into some of the other details, tell us a little bit about that type of work and why you got into it. Well, I used to be the head football coach at Garfield High [00:04:00] School here in Seattle, Washington, which is a really well-known high school.
Brandon Roy is from here. Unfortunately, he's made the paper here locally today, but, uh, not for good reasons, but, uh, he had made it. And my point is that, uh, good school, very academic, uh, but then I realized some issues that were going on there. A lot of people don't know this across the country, but the, uh, student, uh, to c- counselor ratio is 408 to one in the United States.
Uh, so there's a chance you wouldn't even see your counselor, even if you're just a regular matriculated student, let alone a student athlete who really just needs a lot of guidance. And if you follow college athletics right now, it is a, a quagmire is probably the nice way of putting it. Uh, it's a, it's a mess.
Uh, there's, you know, probably, I think I read yesterday, like 89 court filings right now, uh, with appeals and things going on and no direction and no sense of direction from the NCAA. Um, I think there's some things that are happening that we'll maybe talk about a little bit later at the end about the legislative stuff.
But the bottom line was a [00:05:00] lot of kids aren't, uh... what a lot of par- You know, when I first started it, it was about GPA, the sliding scale, making sure kids were gonna be academically qualified. Well, there's no longer an SAT, ACT requirement for Division I or Division II anymore, only really Division III.
But I would recommend that most parents get, uh, an SAT, ACT score if they can, especially if they have to go the Division III route. Uh, having said that, and what it's morphed into today, uh, with the change with the transfer portal with NIL, um, there's about 525 to 550 less high school football players being taken out the, out the Power Four level.
So if you start thinking about how that trickles down and matriculates, there's just, you know, 525 to 550 less kids that are taken high school-wise. Uh, the portal has really changed. Um, you know, they say now, uh, when it comes to recruiting, it really starts with, uh, the coach is re-recruiting his, his college team.
That's number one. And then they go in and they go... and they, you know, figure all that out. [00:06:00] Then they figure out who they've have asked to leave, and they go out and they go to the portal. They figure that piece out. Then they go to the JUCO if they have to fill out some more of their... And then the high school kid comes in and, you know.
So he's number four on the list, really where they're at. And what par- what parents really need to really understand and realize that college coaches, you know, unfortunately, Coach Signetti's success at, at, uh- Indiana has put the pressure on everybody else a little bit more than everybody realizes. Um, there's no-- You-- I would not come in with a PowerPoint with a five-year plan.
Coach Mike McNeely shows you can do it in two years at Indiana, and if you have the right situation and everything works out well, and you have a plan, you can make it happen. So bottom line is college coaches have to win, and they have to win quickly, and so they make decisions based upon how their roster fits, do those things, and To, to convolute it even more, the NCAA decided they're gonna give more roster spots, okay?
So let's use baseball as a great example. They went from 11.7, which I [00:07:00] never have understood. Will and I talked about this for years, how you have to make a, you know, baseball team, and you can't with 11 players, you know, um, you know, making it happen and, and d- doing that. And now they've upped it to 34.
Well, that's great, but all universities don't have to fully fund 34 players, and a lot of them are choosing to fund only 11.7. And so, um, although it looks good on paper, what's the reality of where you're gonna go and how you're gonna fit, you have to figure that out. And then comes the, what used to be, whatever term it at the beginning was NIL, which is how they were gonna pay the players.
It's now called rev share. So whatever you, your c- your college makes through all their media deals, that's the, the, really the cut that's gonna pay the players. NIL traditionally is now going back to what the old model was. The original model was your name, your image, and likeness was how you can make some money.
And so from that piece, um, you know, it just, it just changed considerably, and so a lot of parents just don't know how to, how to deal with all this stuff. And, [00:08:00] and unfortunately, NIL now is even trickling down into the high school ranks. So, uh, a lot, a lot to be out there. So Scott, a lot, a lot you to, um, pack in, which is awesome, all the information.
Uh, but for the players out there, right, I mean, there's obviously we can talk about the injuries and how that affects things and everything else that I do on my daily basis. But what I'm hearing from you is not only has there been already an upgrade from what we call NIL to now rev share, and it makes sense, right?
I think probably your likeness, you make some money, but if the school is making... The school has more power, they can make more money off you, right? 'Cause they know people, and it's sort of like it's the next tier, and so they wanna be a part of that as well. Yes. Um, and understanding, again, everybody's following the money, unfortunately, uh, as you say.
But the other thing is, you know, how is that, how is that affecting? I mean, that just keeps growing in terms of money, so that probably makes it more complicated, but also probably adds more pressure to the scenario, right? 'Cause as we keep getting these wallets deeper and deeper, it becomes more challenging.
It's [00:09:00] like, you know, you're not just going there for five fifty, you're going there for two hundred thousand now, or a million or something. Yeah. Well, I, I think you hit it right on the nose, Doc. I think there's, there's two pieces to that piece, and one is what you're saying, and I don't know if it's sustainable.
I don't know if these boosters are gonna be, be able to, you know, keep rolling this, this bankroll to make this happen, and we can use a couple examples. But, um, to be honest with you, I, I'm helping a player right now who's from the Seattle area who had played at a D3 good school, wants to go up and play at a D2, maybe a, a, a D1 school, m- mainly academic.
His issue is exactly what you just said. He was, uh, one of the better players in his conference, uh, in California, and then he came down with a, a broken ankle three weeks, uh, two weeks before the end of the season, and now he wants to enter the portal. Well, now we've got injury Now we've got how are we gonna have-- handle the NIL?
Uh, you know, is it really about academics? Is it you wanna go to the best schools? You wanna go to a place that's gonna fit you? So those are questions that, you know... [00:10:00] Basically, you, you've got a damaged athlete, and so not damaged, but an injured athlete. So how do you-- how does that look like in the process of, of a transfer portal in NIL and the deal that's gonna happen?
And to your point, um, I-- what concerns me is, you know, uh, Cody Campbell is the big eight, uh, the big booster down in Texas Tech, and he's, uh, if you saw the movie, you know, the show called "Landman," that's how he kind of literally made his money. That's-- he made it through the oil field. Well, he's got $6.8 billion, and that's great, and but when you're talking, you're going against, you know, Phil Knights and all those other guys, and they've got $100 billion, how do you compare it?
And I don't, I don't know if the s- the system is sustainable, and The way that, the way that- Can you explain that more to the, the listeners? Sure. You mentioned two big places. So how does the booster have to do with the big corporate? At least, again, I'm being more layman 'cause this is, this is nice. I don't always get to ask questions on a show- Sure
where I don't know what you're asking. Sure. So the way... And, and that's kind of the third piece that we [00:11:00] haven't even talked about. That's when the actual, um, you know, you, you... The school can put together a group of people, boosters basically, and they become a, an entity, and then they funnel money through there, besides what they have through the rev share, and they can add to that piece, and then that's gonna, can increase the amount of money that they give per student athlete.
You know, like right now they're saying Arch Manning is about $6.8 million for, to play quarterback at Texas. Um, top tier quarter... You know, uh, the best basketball player, the young kid from BYU, Will probably knows his name, I can't pronounce it very well. But, um, you know, the s- supposedly the word on the street was $4.8 million for a true freshman.
Um, so you're talking about big money and, but is this sustainable and how does this work? And, um, I've seen figures where, you know, the equity's out there and it's, it looks all good and everybody's kinda getting a piece and the basketball program's getting a good amount. But g- good example, um, the SEC, I just saw, [00:12:00] um, the offensive coordinator from Oregon, who my son works with, just took the head coaching job at, um, Kentucky.
Well, I just saw yesterday, uh, Kentucky's NIL, uh, budget for their basketball program was $22 million. And I'm pretty sure I think, um, only teams play with, uh, 13 guys on their team. So 22 million divided by 13 is not a bad number. And if you're the b- the football coach, you're tr- you're, you're... I mean, you know, the apparently not a good football program, all of a sudden the basketball program's, you know, like got everybody's making 2 million bucks and his left guard's making 50 bucks and how is he gonna compete in the SEC?
And you gotta win at the highest level. So again, it's a combination of all those things. Um, and, and there's been a call to, to maybe end the, the, the booster piece, but I don't know if that... I don't, I don't think that's gonna go either. The, I mean, there's always a way to funnel. There's always a way. The one thing, doctor, you'll learn in the, with the NCAA and especially with college football coaches, um, uh, I know that you have a certain, uh, [00:13:00] decorum that you have to work with from a legal standpoint.
College football coaches, and you gotta think about there's some pretty smart ones like Mike Leach and Rick Neuheisel are former attorneys. Uh, they see that big old book about that thick, um, in front of them, and what they always do is they look for what it doesn't say. Where's, where's the gray matter?
Where can I- Yes ... figure out this other piece? And that becomes the issue. And, you know, there's a new governing board supposedly that they said they were gonna put, um, push down on tampering. Well- Everybody knows that tampering has been going on all day long, and there's nobody's been-- no program has yet or no coach has been hit with any fines.
So what do you think every college coach in the country's gonna do? 'Cause he's gotta win. He's gonna say, "Well, if they're not tampering and they're not gonna hit us with it, we're gonna continue to go down this road and we're gonna do whatever we gotta do." So it's the NCAA level and everything, and, um, it's, it's, it's quite a mess, to be quite frank and honest with you.
It-- and it's been my thing, and Will knows this, I've been saying for five [00:14:00] years, I don't care what we do, I don't care how we get here, I think kids deserve a little bit of the pie. I, I think, I, that not, that's not my thing. What's bothered me from the beginning is there was just no guidelines, there was no rules, there was no- Yes
no sense of this is, we're gonna do it this way. And, and to be quite frank and honest with you, in the back right corner of the, of the stove percolating is, is the Title IX. The girls are, are gonna get some of this money. It's illegal, it's a law. Yes. I mean, and they're just sitting there waiting, and they're waiting for it to all settle, and they're gonna go, "Hey, remember us over here?
You guys forgot about us, and now we're here, and they're all getting the money. We need to get our piece, too." So, uh, there's a lot more to be fixed than there is to be, you know, solved and re- and, and resolved, so. And do you think, uh, this model right now is also throwing things off 'cause it's no longer, like there's, the strategy's changed for the coaches, right?
Like if you show up to a program and they have 22 million, like your s- your skill set as a coach doesn't really, isn't really... No [00:15:00] offense to that scenario, but you know, you show up with like nothing. You gotta kinda work for it to get these recruits. Start looking for high school, looking for people that slip through the cracks, gray zones, whatever you wanna call it.
Uh, the coaching, it's another element that you didn't have before, right? Oh, absolutely. It just, it just changes everything. Absolutely. I, I, you know, I'll, I'll be honest with you, you know, um, you know, I've heard a lot of coaches, college coaches say, you know, "I, I was hired to be an X and O guy. I wasn't hired here to figure out contracts and how much, who gets what, and how this is working and who."
Because I, I mean, most of those guys, I mean, they're not contract law guys. They don't understand those things. They just go to the budget and they see the dollar bottom line. Yes. And, as you said, and, and, and to what you guys do, what you guys talk about, but what's kind of, I mean, the stress that they put on these student athletes and d- for them to...
If Division I is a go, it does not stop. It's 24/7, 365. And it, you know, I would argue that a lot of the, you know, I think a lot of teams would probably show, if you, if you listen to Coach Cignetti talk [00:16:00] on how he approaches it, he is less is more for him. He practices about 45 minutes. Mm-hmm. And he just, and he, and he tones it down farther as he goes into the season.
He just feels like he doesn't have to. And I think it paid off with his program. I think there's a lot of programs- Yes ... where, you know, 'cause they're trying to win, they're just m- you know, pushing these kids really, really hard. I know for a fact that, uh, you know, Oregon, when they went into the semifinal game, they, the, so the, the game the week before against Texas Tech quarterfinal game, they had a seven-man, um, rot- uh, seven-man in the running back room.
By the next Friday night when they were playing Indiana, they had two running backs. Four went into the portal. One got injured, uh, broke his, uh, clavicle. The, um, the, the starter, and actually only won the game with one, to be honest with you. The starter got injured during the week, pulled his hamstring, so they're down to really one running back, and they, they brought one of the portal guys back in, I think a couple bucks, asked him to stay for one more week, and he stayed for the game.[00:17:00]
So it just shows you w-what, how fast this can happen. And then you're putting that much stress on student athletes to, to, to play in a semifinal game with basically two running backs. Yeah, there's so much to, uh, to kind of get into. I, I'll stick with what's happening here, and I know it's something that, uh, you talked about before, um, as far as, um, the recruiting deadlines.
Should there be some deadlines? Uh, it, it seems like, you know, you're, you're going out and recruiting these kids in December, and you have to make these commitments, but you're still in the playoffs and the timeline, and all of that's now being affected with money and who's going into the portal. Like you said, you're still playing the season.
You're, you're hopping into the portal. So what would you like to see, and, and this kind of goes a little bit away from the NIL, but still keeping that in mind as far as the timeline. How would you adjust the timeline so seasons end, recruiting from high school to college, opening up the portal, so everyone kind of [00:18:00] knows what's happening at the right time at the right place, so you know what you're working with?
And especially for these kids that say, "I'm going to the portal," when you have four thousand kids going into the portal, and there's only three hundred jobs available. Yeah. Well, I, I think you, you started... The number one thing that you just said, Will, is, is the most important thing. They have to fix the calendar, and I think they even have to maybe go to a pro style.
I mean, there's been talk about OTAs, uh, organized team activities, and changing, not having really a spring ball, pushing that down the road, uh, moving the portal more into the springtime, because let's be honest, what's gonna happen here, and they, they've come up with a new rule that if a kid, let's just argue, um, realizes he's not gonna play at a school and he- gets injured and he goes into the, he goes out of the school and enters through the backdoor way of the let me just argument of a portal.
If a coach took him on, supposedly the NCAA's now saying that you'll be, you're gonna, you're gonna face a fine. If you take [00:19:00] him, uh, you could be su- suspended for a couple games. Well, I, I think that would be challenged in court, to be honest with you. And if you know anything about the Supreme Court with the Alston case from the beginning, uh, you know, Judge Kavanaugh has basically said that he thought that the players, athletes deserve even more than what they were gonna give them in the, in the suit.
So it would, it would go for the, for them, uh, in, in, in that, in that regard. Going back to what you were saying, so let's use Oregon as a good example. Both the coordinators became head coaches during, during the playoffs. So now they're playing a playoff game. The running backs are down to two running backs.
Both coaches After they get done with practice, go behind the screen when nobody's watching when the, in the press conferences, and they're calling their prospective schools, Cal and, and Kentucky, and calling their recruits, while try- still coaching the semifinal game, while trying to figure out their roster, which they're not at their school, so they're not even at the pro- on the [00:20:00] school.
So when they beat, uh, Texas Tech, you know, they had two days to go back to Kentucky, two days to go to Cal, figure those things out, rush back to Oregon, coach the game. I mean, we, we just created this bad mess, and that's what we seem to do. Yeah, with Arkansas and then we saw that disaster. I mean, Oregon, I, I mean, you're, you're pointing it out, but it was almost quiet compared to the mess that was happening at Ole Miss, Lane Kiffin, coaches leaving, coaches coming back, recruiting, everything else that was going on.
Just- Yeah ... let's not even... Just trying to- No, no, they, they, they, you, you hit it right on the nose. They, they really just need to, you know, sit down and have a, a real heart-to-heart with this. And I know that, you know, uh, President Trump just had the, what they call the roundtable. I honestly didn't feel like the people at the table were the right people.
Um, i.e., some student athletes. I felt like there was some p-people like Tiger Woods. I mean, really, I mean, golf is so different from the rest of the sports. His son is, right now they say his, his NIL value is 2.5 million at Florida State, so I don't... [00:21:00] What, what's really, what's he gonna argue for at the table, right?
Right? My point being is that we need to have the student athletes, and I really think that they just need to have some common sense people in there, some former coaches. Chris Peterson I think would be a great choice. I think Nick Saban. Uh, these guys that are, they've seen it, done it, they know what's out there.
Uh, get the, the, the true major sports, basketball and football. The, let's be perfectly blunt, those are the ones that finance this whole thing. Get them on the table, figure it out, bring the media guys in and say, "Can you... Is this a workable, you know, segment that we can w- look at?" If that can work, then bring the student athletes in and say, "Okay, you're gonna be part of the next process of in-initiating it and doing all these things."
But we have to have some type of leadership. And, you know, uh, for argument's sakes, I would honestly probably say that the NCAA is null and void. I don't th- they don't do anything. They don't govern anymore. I think they really should just manage the f- the, you know, the greatest tournament we all like to do, and we're all about to fill our brackets out [00:22:00] and make it happen and, you know, you know, try to win, trying to win the basketball thing.
So let them be the manager of the basketball. It's a billion-dollar industry for them. They make a ton of money, and just let them become the managers of that, and then let the Power Four do whatever they're gonna do. And, and that's really the sad part to me is the lower levels have been hit so hard on this.
Oregon States, Washington States, they're not the programs they used to be, and it's really sad what it's come to. And it's, and that's basically because the, the bigger ones get even more money. It's like the rich get richer, and then everyone else is just screwed So are they getting, are they getting pulled away?
You know, like if they even get his top player, it's no longer like, "Well, I'm gonna stay there for three or four years and play because I'm like, there's more money and I gotta get my money before I get hurt or something else." You're right. And, and, and to be honest with you, doctor, like for example, my stepson, he's the special teams coordinator at Oregon.
He took the, the, the kicker and the punter from Nevada this year 28, and he's t- that, uh, Will will love this. He's a 28-year-old Australian [00:23:00] punter, Will. Um, so, you know, think about that. I don't know if he's bringing his family and kids and everybody else with him, but I mean, just it's crazy. But my point being, Coach Choate literally got on f- on, on, um, social media and says, "Great, we develop them.
We do great, and then Oregon comes in and gives them a million bucks, and they, they take off." And so that's the hard part for the lower guys. You know, they, they're, they're really doing development. And to be honest with you, that's how I like to tell kids nowadays. It's like, "Guys, you basically have to go to a lower level, do well, compete."
The kid from the, the, the best lineman from, uh, Montana State last year, a Bozeman kid- Yeah ... um, ends up getting a, a big-time, you know, Division I scholarship. I mean, it's just, just kind of the model we're at. You have to go out and prove the tape, things like that, and then once you can do that, then you can go in off the portal and do those things.
It's kinda crazy, though, 'cause it used to be... Again, maybe I'm not as well-versed as you guys are, but it used to be like, you know, you do well in high school, you could go to junior college. You go do well in junior college, then you go get your big thing or you jump right in. Now it's like you gotta go to a good [00:24:00] school and then you get pulled again to another school, right?
Yeah. It's another layer, as you keep saying because it's, because they don't need as many athletes, right? Like you don't need to... If you've got all these extra schools to pick from, then you don't really need, like you don't need to worry about the development as much. You just let the other schools do it for you and then you pick 'em off.
Yep, that's exactly it and it's, it's, it's- Wow ... hard, uh, it's a hard pill to swallow for parents. They don't really understand it and, you know, i- if you really think about it from the big perspective of recruiting, um, I've already mentioned it, you know, the Australian punter. If you ever looked at the u- uh, the university, uh, golf programs, it's not, not Tim Johnson.
It's kids from Korea , from the, the, Europe. I mean, they're coming from all over the world to take American golf scholarships. Um, you know, basketball, a lot of European players coming over here taking jobs. Are they, are they subject to the same money or is it different? International kids do have a little bit of a, a, a weird thing they have to get past and once they do it they, they, they will [00:25:00] get money.
But they have to kinda go through like a basically a little timeframe period where they don't get anything and then once they've hit this threshold then they can get some money. But it's, it's the way they- Can you recruit them though? Like can you recruit, let's say have a good Eur- I mean European, you know, especially like Eastern European, some of the players are these super tall athletic basketball players.
Can you, can you NIL them to come over and then tell them, "Hey, when you get your thing you're gonna get paid," or is that, we're not happening? Oh yeah, that's definitely happening. That's definitely happening. It's, it's just a new model. So it's not just local. No. It's not just US, this is all around the world we're doing this.
Yeah. I mean, it's, it's, it's, it is what it is. And I, you know, I, and I'd be lying to you if I was telling you that the, you know, golf kid from Korea is making a lot of money like the big timers in, in, in the football. That's not the same kind of money, but they are making some money. They're making some dollars.
And, and, you know, so it's... But to your point, yes, it's, it's worldwide. It's all those athletes from any place. And [00:26:00] you can go get 28-year-old Australian punters. You can go get a good golfer from Korea, and you can go get a basketball player from Lithuania. Wow. And that's, you know- You brought up a really good point.
One of my surgeon friends, like with all these talks I do, I get to see the guys that do team doctors for most of the different professional, uh, and, um, college level. And he was saying that the problem he's having now is like high school kids with NIL money. It's not much money. I mean, again, it's m- money for the average population think is a lot, but you know, $25,000, $50,000 and he has players saying, "I don't wanna get this surgery," even though in their high school, 'cause they're like, "It's gonna hurt my $50,000 NIL money."
Yeah. Because now you have like even a little bit of money in these high school kids is like so much. It's like we're talking about one, two, $3 million contracts, and we're talking about like, this kid's gonna jeopardize his entire career for $25,000 because he's not used to getting anything, right? And so now they're just dangling even smaller and smaller carrots at these kids, and they're willing to do things.
And because you go to a certain [00:27:00] socioeconomic area, it's even more desperate. So it's like even those bottom scenarios are bad with the money sometimes, or it can be stressful. You, it's hard to navigate. So like you're talking about student athletes, but what about the guy that's a D3 barely making it, but he got offered $25,000 and he gets hurt, and he's like, "I don't wanna do...
I need to push through this 'cause I'm blah, blah, blah." You know? It's like it, that's even more scary, right? Okay. At least if you get hurt, you've made $20 million, you can at least do something. You get hurt and you have $25,000, you're definitely gone quickly. Well, I mean, y- y- you're exactly right, Doc. I mean, I mean, you look at quarterbacks are probably the best example.
I mean, if you're, if you're, uh, Arch Manning, you go and go get a, a rookie contract next year, you're taking a pay cut. Yeah. Oh, yeah. I mean, you take a pay cut. I mean, y- I mean, it doesn't, I mean- Yep ... stay in college. I mean, they're gonna keep paying you. I mean, you know what I mean? Got a lot of co-eds walking around.
I mean, it's not a rough life. I mean, you have a pretty good, pretty good day there. I mean- And Carson Beck stayed for what, six years, seven years I think ... two years and didn't go to school, his last two. I mean, you know, it doesn't- Yeah. Yep ... I mean, it's, [00:28:00] it's, the, the system is what they have to change, and they have to figure this piece out.
And it, I've always said that, you know, I feel like it all should be tied into a trust. And going back to what you're talking about, I think that there's another piece that's really frustrating. I know that UDub last week announced or show, put on social media they are doing some financial literacy, uh, type course on the campus.
I'm not saying it's mandate- mandated to all the athletes, they have to do it, but at least they're offering it. I think that they, th- this could be a invaluable thing if it was done right. I think all of us is, you, you running your business, learning about an LLC, learning about, um, you know, incorporations, all the things, tax write-offs, how you do those things, would be important for all these kids to do it.
And, um, you know, I just, the way that most of the colleges and universities handled it was that they said, "We, we're not gonna give any advice because if we give advice, then we can come back and sue us." Well, I'm pretty sure that in every college campus there's a law school and a accounting school I think they [00:29:00] could have an open house with both of those schools and to say, "We're not telling you you have to use any of these services or any of these people in this room.
We're telling you this is a mixer. You can just meet each other, pass cards to each other, figure this thing out if you wanna use it. But I would advise you to probably talk to somebody about what you're doing with your finances." I, I, I guarantee you right now there is a 30 for 30 for sure being made about the financial issues that are going on with all these kids.
And, and we're talking- Oh, absolutely ... we're talking about, you know, um, you know, we, we, we literally at Georgia they, they can, they can make an all 22 team at the University of Georgia with kids that have been, have, have a, a, you know, felony against them for driving too fast or whatever down there in, in, in Georgia.
I mean, the, you know, when we give kids that kind of money on a college campus, we're asking for, you know, accidents. And so I just think that then we need to have some guidelines, and once we do that, I think we'll, we'd be good. And, you know, I used this [00:30:00] example a couple years ago. University of Utah gave away 85 trucks.
Well, that was great. I mean, it's, you know, super. But nobody realizes there's a 1099 attached to that truck. There's probably a mileage attached to that truck like a lease. So you got a young man who's got a new truck, 80-- you know, new, new truck, and his girlfriend lives 250 miles away, and he's driving back and forth seeing her.
And a year from now he comes rolling in, the, the place hands him a $8,000 1099 taxes and said, "Oh, yeah, and you're over the mileage by 30,000 miles, and here's your second, you know, bill." And the kid's like, "What? I, I thought I just got a truck," you know? And again, it's the education of these things. And, um, you know, it's, it even happened here locally, Dr.,
uh, there's a program that was gonna be called Tips, uh, that this person was in the outskirts of Seattle, and Bellevue was trying to put together. Basically, you can go to a high school basketball game or a high school game, any game, and you could give a kid a tip. [00:31:00] I don't know, if you went back to your, your high school that you went to and you noticed a good kid, maybe send him 20 bucks and he goes down to the local corner burger joint and has a burger after the game on you.
I'm all for it. Now we're talking about another guy comes to the game, his name is Guido, and he's not re- you know, there to, you know, hang out with your family. He's there to give you $1,000 with a wink when he hands it to you and says, "I'll see you in a couple years, and then we'll, you know, have a discussion about where you go to next."
And if people don't realize, if you've done any of the research like I have, online gambling with young men is scary. There's a lot of people gambling and, you know, the, the NFL rule is you cannot have a, um, gambling app on you, on, on your phone while in the facility. Doesn't mean a kid can't go down 100 yards away from the facility, pull over the side, put that back app on the thing, and pl- place a bet 'cause he just happened to be in the training room and noticed that the left guard was not looking really good and probably not gonna be starting the game, and he knew [00:32:00] that he could make himself a couple bucks.
And I know that's being nefarious when I say those things, but it's the reality and the truth of what we're dealing with. It's-- I mean, anything you're talking about is probably worse even behind the scenes. So, you know, whatever we can you say in line is there's, we've seen it all. And, um, it's a, it's a perfect example too, just, you know, how even these injuries are just an important part of it too, right?
Because like you said, like someone gets injured, but it's not announced. We don't know what's going on. It's a, we always, and Will and I always joke, they call it a knee strain, shoulder strain, right? But it's more than that. And so now you have inside information, and all of a sudden now, you know, this player's not gonna be at the performance level, and you know that, and they're a starter, right?
Yeah. A quarterback's injured, and they're not really playing as well as you think they are. Yep. So. Well, and, and I think- Sorry, I was gonna, I was gonna ask a quick question, and it's really the question's for both of you, especially since you had an affiliation with colleges and, you know, in Oregon and in some other places as well.
Um, going back to [00:33:00] the injuries, right? So what is the responsibility of the university, the team doctors when you have a player that's been on your team but is possibly transferring and already has an injury? You know, are, are doctors taking care of this kid or are they saying, "Well, you're leaving, we're not taking care of you"?
Like I, I'm not sure, Dr. S, if you heard it on your end, but it seems like it's that kind of like, "Are you with us or you're not? And if you're leaving and you're injured, are we no longer talking to you? Is it an insurance thing?" So I'm, I'm curious, uh, Dr. S, I'll start with you first, and then Scott, if you have any insight, I'd love to hear from you as well.
Yeah. So I'll add to that. I mean, so the good news is that physicians generally are employed who work in those places, so they're employed at a contract rate. So they're... They get a salary, or if they're at a college, they're usually just employed in general at the facility, right? So like, you know, the University of Washington surgeons are employed by University of Washington.
So they're not [00:34:00] incentivized to do anything that's outside of the norm, which is good. And I would assume most doctors would not be incentivized regardless of the money. But you never know. Everyone's different as soon as money starts coming out. But the-- there's a reason for that, right? Like, if you're a team physician for the Seahawks, you don't get paid more or less by clearing or not clearing.
There's pressure, right? Like, but we know Ed Khalaf at the Seahawks is not feeling obligated to go and clear someone because he's been there for twen- you know, almost 20 years or more, and he doesn't-- he's not... His job's not in jeopardy. He wants to make sure that the player gets the best thing. Now, if you're a new surgeon, things might change a little bit because you just, you just got the team program and you wanna look good.
But for the most part, that's probably not happening, um, because of the fact that they're not in-- there's no incentive for a surgeon to do that. Now, like if the, you know, the coach, you know, as you and Scott saying, that's a different animal because there may be a coach sitting behind your ear yelling at you, telling you what to do, and that may feel, [00:35:00] you may feel pressure that direction, but it's not generally gonna be the doctor.
There's gonna be another influence in that. Uh, but for the most part, the good news is that there are a lot of like anti-tampering things. And you saw Brian Daboll get slapped with a huge fine when he showed up to the New York Giants tent and interrupted Scott Rodeo as he was evaluating for a concussion, right?
Like, they're smart about this because they know that like it's not the doctor that's gonna do it, but it's a person that's sitting behind, behind their shoulders that you don't see. Uh, and that may push them to feel uncomfortable in the scenario. Now, it depends on the surgeon, right? And if you have someone that's been there for a number of years, there's job security.
First year, second year, maybe you don't feel that way, so But if there's a gap in handoff, like, like I said, you know, you've got Jimmy that is going to go into the portal in two weeks, and then so essentially that player's no longer your responsibility. What, what happens to that player once he goes into the portal, still has an injury and is trying to find a home?
At that point is, is the player on his own to find his own doctor to take care of [00:36:00] himself, even though he got injured with your team on your field, uh, with his teammates? So Scott, why don't you chime in, and then, uh, Garcia, if you have something to add on that, I'd love to hear it. Yeah, I, I, you know, well, I, I mean, I, I wouldn't wanna get into the legality of figuring that piece out.
I mean, I'm really giving you a clear answer. I would probably assume to think that it's probably a little bit of in between there. It feels like... But we both know there's not COBRA for, for student athletes, unless you can have this little coverage going with you on that deal. I think they would feel their...
The, the university would feel their obligation to whatever they needed to do to, for that student athlete. But once that portal opens, man, I'm just telling you right now, it's, it's pretty much you're out the door and, you know, they're, and they're, they, they've moved on from you. And, um, so from that point, that's, you know, I think that the student athlete is kinda like out on his own.
But, uh, to your point, I think that they have a legal obligation to fulfill whatever his, the injury was up until he, he [00:37:00] leaves. And so that in between time, that's, that's, I, I wouldn't, I wouldn't know the answer. Doc would probably have a better answer for that one. I mean, I think it depends on if they have an agent, right?
You know, in some of these cases of agents, they get independent evaluations. So when we affiliated some of the pro athletes, the agent gets you because you're not affiliated with any team, and then they'll say, "Hey, I want independent ex- examination. How bad is this scenario?" Right? Um, so that's usually what they'll do if they're in between scenarios.
But also, you gotta pay for that. You're gonna hope your agent does that. But again, it depends on the amount of money, right? If they have, if it's, they're, they're going there for other reasons, it's different. But if they've got a, if they've got money involved and you know there's agents now for everything 'cause everybody's gotta get a cut of this, um, nowadays, then, then they're usually, they're probably gonna handle that.
They'll probably handle to cover the cost, um, of it. But obviously it depends. Like if you're the player I told you about, like $25,000, like no one's helping you. Yeah. You know? You need to be, you know, you're, you're $2.4 or $5.6 million, then [00:38:00] yeah, you're gonna have a lot of people offering to help you with transfer portal and get injured yesterday.
Well, we, we just kinda saw it in the pros with Max Crosby Yep. With the situation, you know? And so, I mean, and to Doc's point, the, the dollar amount's a lot different in that deal, so, you know, there was a lot more to, you know, to, to, to risk and, or not to, you know, make the deal ha- happen and stuff like that.
But it's an interesting piece, you know? Well, also this is in... it's influenced by the, by the lawsuits recently. I mean, you had the Philadelphia Eagles one where Rothman and Jim Bradley got na- nasty, almost $4 million or plus thing. So do you wanna be the team doctor saying, "I think this player's great to play with us.
It's worth it," or are you saying, "You know what? Screw this, you know? I've played this game too long. I've done this too long in this group. I'm not gonna get sued by this athlete coming in and having a bad year on his contract, and they're gonna protect themselves." So unfortunately, the, you know, these lawsuits, they swing both directions for these different team doctors.
But it may be a scenario now where you have d- you know, doctors who can say, "I'm gonna be more stringent with this injury. I'm gonna tell the coach, like, 'I'm not gonna sign off on this. This may not [00:39:00] last. It's not worth your money.'" And the players are gonna have to sit there and just either sit on the other team and do what they have to do.
But again, it's not that common, and there's still a lot of people pushing the envelope on what they think is possible. But there's players also, as we talked about this with Will, that play with some awful-looking injuries or chronic injuries, right? That they're able to do things that normal athletes can't do, you know, these super athletes.
Again, pros are different than we're talking about here in college. It's a different animal, and the injuries are different. They're not the same attritional injuries of the 30-year-old, 40-year-old quarterback or running back Yeah, it's just another concerning area. And that, that's why I bring it up. You know, talking about NIL deals, talking about the transfer portal, you know, and, and that can be another gray area, and maybe the player's not sharing that information.
Is there allegation from the teammates coming from to share that information? Is there patient confidentiality? So I'm just curious about all of that stuff just to add a- another [00:40:00] wrinkle into all this. I know we're almost 40 minute... We're 40 minutes into the show. Uh, we wanted to talk some of the, the stuff, revenue share, NIL deals.
Scott, was there something that you really kind of wanted to, to share with the audience that I can, uh, pull up here, uh, that you wanted to, uh, you know, make people aware, whether it's the legislative efforts or the- Well, yeah, just, just bring one up. We have the PASS Act or whatever you want, um, however you want to do it.
Sure. It kind of, it, it kind of goes in line with what we were talking about earlier with, uh, President Trump's roundtable. Uh, there are some, four different segments of some legislative things out there, uh, that are being looked at when it comes to, um, you know, chances maybe to right the ship is the best way to put it.
Um, I would be honestly, you know, all of them have their pros and their cons to what's good and what's not good about them. At least there's some type of structure they're trying to make from this [00:41:00] deal. Um, but again, I, it's, I would argue that the people that should be at the table aren't at the table and really understanding it.
The coaches need to be there. I mean, they need to s-reset the calendar. They re- need to reset, um, you know, the financial stipulations. They need to think about how the real, the real market is out there. They need to bring the TV guys in because they're, eventually they're the ones gonna pay a lot of this money and how that can happen.
Um, so I think that all those players need to be at the table, but it may be at different segments and the time that they bring them in. Uh, but they need to have some people that, you know, I always like to use the, you know, they know where the bodies are buried. Uh, Coach Saban and Coach Peterson, um, you know, Jeff McGrath from Notre Dame basketball.
I mean, there's a lot of people out there. Lynn Dunn, basketball coach, uh, longtime person, you know, another one that they could bring in and at least talk about this and, and say, "Hey, what, what are we doing good? What are we doing bad? How can we improve this? Where, what should we do? What, where are the guidelines, the stipulations that we should make happen?
And then we can work from there." [00:42:00] The bottom line is, you know, then I think that there would be some things could happen the, at the, for the lower levels that could be a, a good thing. Maybe there'd be better streaming, you know, contracts for the smaller schools, and they can get a little bit of the, you know, cut of the money.
I'm not-- I don't know those things. I don't know if those could be true. But if you think about the Pac-12 now, we're, uh, you know, whatever the new Pac-12 is, you wanna look at it, but you're still deal- dealing with the same problems when it comes to streaming and the, and the issues of audience. And Will, you know this well so much is, you know, San Jose's not the greatest market.
San Diego's not the greatest market. Obviously, you know, Spokane's not a great market, market when you talk about Gonzaga, you know, as a, as, as a market, uh, per se for TV, you know, uh, being watched every night, even though Gonzaga's a well-known entity. And so they're still gonna have the same problem in the, in the new Pac-12 with Logan, Utah, another school, uh, with a low, you know, small, um, TV market.
And so we've gotta [00:43:00] look at those things, and that's gotta be a piece of the whole puzzle to figure it all out to make it work right. At least that, that, that's my opinion of the deal. Um, but I'm way low on the totem pole when it comes to those. That's just my opinion. Um, you know, the guys that make all the big money, they can...
They're, they're the ones that can go figure that out, but they've gotta figure something out sooner than later
Um, we saw with, um, Texas Tech We've seen with a couple other schools that they have a GM in place. Um, very professional feel, right? They have all the elements in play, um, like a, like a professional team. Do you foresee that schools are going that direction? Or, you know, besides foresee that, but also think that it is necessary that way the money is moving, keeping track of everything, taking, um, all of this extra work off the plate of the coach and having the general manager in place for these [00:44:00] colleges.
Do you think that that's the way to go? Because obviously the genie's out of the bottle, that's never gonna go back in. We're just trying to now curtail it a little bit and try to have some, some control. So if you are running a program right now, would that be one of the ways that you go to say, "Let me get this off the coaches, let them focus on football.
I'm gonna manage the money. I'm gonna keep my eye out on recruiting," and so on and so forth. What are your thoughts on that model going forward for the college landscape? I- it, it, it is the model now. It's going to be the model from here going forward. Um, it's p- be honestly, well, it's, it's now being run like an NFL program.
There is a player personnel guy, there is a recruiting coordinator, only guy, there's a GM, there's a money person who's just working on, you know, all the, the dollars. Um, there's rumor now that, uh, college coaches will, it'll, it'll be like an NFL model in regards to recruiting, that the college coaches will stay home now and not go on the road, and the recruiting department will go out, and [00:45:00] they'll go out and talk to the coach, the high school coaches and figure this out, and then come back and do it the exact same way the NFL model works.
These guys come in the room, they start arguing about these are the best players. This, this, like a recruit- like they do in the NFL and the scouting things, and they'll do all the reports and things like that. Uh, it is definitely going that model in the hence why somebody like a Bill Belichick and Mike Lombardi are at University of North Carolina.
Um, that is really the model to go out. Because, you know, like I said in the beginning, college coaches, they weren't hired to... They were coach- they're hired to coach. They weren't hired to figure out contracts and, you know, budgets and, you know, you know, thing. And until they figure out, you know, really a true cap, then, and they're gonna need a cap person to figure that whole piece out and how that's gonna work out and things like that.
Um, but they also need to figure out the, the, you know, the NCAA needs to figure out this, um, eligibility thing too. I mean, we've got guys like playing eight, nine, ten years. I mean, what are we doing out here? I mean, this is crazy the amount of time that these guys... So they gotta figure that piece out. If they wanna play 'em five for [00:46:00] five, that's it, and it's once the clock starts, you got only five years to play five years and then you're done and you're out.
Yeah. So I mean, I think we're gonna kind of wrap it up. Obviously, we don't wanna keep you too long and, uh, you know, go beyond the time. Uh, but, you know, where do you see the kind of future of this? How does this all integrate in? You know, is this sort of like you said, everyone's gonna go to a professional model?
Do you see, uh, reform where we get less? I mean, I, it sounds like athletes getting more money Which is good because I think as we all say that, you know, they were getting taken advantage of, at least that's some way some people feel before where they were getting nothing. But now we've got this whole other problem, right?
That I don't think-- I think we could have anticipated it from the pro athletes, but these guys are even younger and gals are even younger and even more immature than these professional athletes. So where do you see the like regulation curtailing with all this other stuff happening? Like how are they gonna get this all...
Because at some point it makes it get so out of hand, like they're gonna have 10 players arrested on a team for all driving their Lamborghinis 200 miles an hour. So like we have to find some scenario [00:47:00] where this doesn't, doesn't stop because you're gonna, you can't give an 18-year-old a million dollars with no other obligations or costs and tell them to be good, to do a good job and be nice.
Yeah, I I'd be remiss to say that I, I think there's a couple unfortunate ways this can go. I think this either is going to implode itself. Uh, I think that they will either have, um, I think the, the-- I, I've heard heavily there's already donor, you know, frustration with this deal and burnout, and, uh, they're gotten to a point where like, you know...
I mean, Texas A&M is a great example. They spent a lot of money down there. They got rid of a coach for $87 million. They bought a new coach in for $100 million. They've, you know, supposedly paid $25 million for the last four years every year for programs. That's $300 million, and they don't have a national championship.
So after a while, that's gonna-- You know, those guys are gonna say, "I'm, I'm done. I'm not gonna do this anymore." And then you have facilities and things like that. Are those things gonna take a, [00:48:00] uh, you know, back, you know, s- to the back porch and not be upgraded and things like that? And for you and for what you do, um, those services, I mean, are we doing a good job of making sure that the docs and the, and the medical staff are taken care of, and they're doing a good job with these student-athletes?
And if we're bringing on more student-athletes, are we bringing on more staff to help those kids and those things like that? You know. So to answer your question, what I would like to see is a true reform. Uh, people honestly just, you know, shut the door, don't let anybody in, and just say we, w- like Will said, the tube-- the, the paste is out of the tubes.
I'm not-- We're not going backwards. That-- We're not gonna do that. We have to say, "These are the guidelines. These are the, what stipulations we have to work from, and this is how we're gonna do it. We have to get the kids in line. They're gonna have five for five," whatever the deal is. And then, uh, I think that, you know, they have a chance to make, make this thing happen.
It's a great-- It's-- The sport is a good sport. Everybody loves to watch it. We all like to, to enjoy it. But at the present state, I just don't know if [00:49:00] it's sustainable. I just don't know if the am- the amount of money... Um, you know, I, I, I know Will's heard me say this probably 10,000 times, but I use Oregon, Oregon State as a prime example.
Oregon is... You know, I'm not sure what you guys are wearing, but, you know, I mean, some- one of us probably has some type of Nike thing on. Could have, right? Shoes, whatever. And that's the machine that helps the Oregon football program. And then there's Oregon State, which is 62 miles away. My granddaughter is a, a, you know, freshman there this year, and they sell potato and macaroni salad And that's how they make their money from the Reser family.
And it's, this is unfair market. I mean, the three of us could go out tonight and buy a tub of Reser's macaroni and potato salad and help the student athletes at Oregon State, but it's probably not gonna do the amount of, you know, money that, uh, N- Nike products bring in year round and s- make that thing happen.
So that is where you start to where the, where, where's this market? And I think a lot of programs like Oregon State and I think Washington State, they would [00:50:00] love to get off the train and just be a regular program and just do their thing and make their thing happen. Um, but to answer your question, I think, I, I do really do think whether it be legislatively or with the, the college, you know, whoever you wanna s- the commissioner or whatever you wanna call it, they know that they, they've got to right the ship sooner than later.
Right. If they don't, they're, they're not gonna... Th- this, this thing can't last. And, um, you know, sooner or later the, you know, the, even the media guys are gonna be like, "We can't... We, we, we don't, we can only do, charge so many much for, for a commercial," and stuff like that. "So we can't do this either." So I mean, uh, you know, in the meantime, I hope those kids are making some money and I hope they have a good financial advisor.
That's what I'm hoping. Yes. Good. Scott Ligo, Student Athletes Advocates. Check out studentathletesadvocates.com. Um, Scott is well-versed in all of this information. He's there to help, uh, not only the student athlete, but [00:51:00] the parents to navigate these really choppy waters, so please go check him out. Uh, Scott, thank you so much for your time.
I feel like we can talk on and on about all this subject, an ever-changing subject. We can have another conversation a month from now and God knows where it'll be. So I just wanna thank you for your time and I appreciate you being with us. Well, thanks, guys. Thank you, Scott. For what you guys do, guys, I really appreciate it.
It's always bringing light to the injuries and the athletes, and that's, it's awesome work you guys do. Thank you, Scott. Dr. Garcia, Scott Ligo. I mean, we could have gone on and on. I had questions about Cinderellas. Will we ever see a Cinde- will we ever see a Kawhi Leonard stay at a New Mexico State?
Today's money, probably not. He's gonna get recruited by Duke or Kentucky or something like that. So, um, we m- still may see it in football, but I think for basketball, those Cinderella great stories, uh, th- they may be long gone, but that's a story for another day. Uh, Dr. [00:52:00] Garcia, what are your final thoughts as we say adieu?
Well, it was great having him on. It's an interesting topic, which we talk, we dabble about all the time when we talk on this show, uh, but to have a real expert on has been great. So looking forward to more fun guests. Stay tuned. We got a whole good lineup. Submit if you're interested. We get a lot of requests recently, so this is great.
So anyhow, thank you again, Scott, for being on, and we look forward to this coming out This is Sports Doc Talk. Will Sanchez, our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia. Stop making us look bad by doing so many different things. And if you need to recovery, to recover, check out our boy Mike B at The Recovery Shot, Shop.
Dr. Garcia, once again, it's, uh, great spending time with you. And, uh, till next time, we've got a lot of shows lined up, a lot of great guests, so we're really excited. Excited. Thank you so much, guys.
Audio Transcript
Minimally Invasive Surgery with Dr. Anthony Yi

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon in sports medicine specialist Dr. Greg Garcia. Dr. Garcia, I'm fired up. I love our guest today. We have a lot in common, but Dr. Garcia, first and foremost, how are you doing?
Dr. Grant Garcia: I'm good. I'm fired up too. You can see we got, our backgrounds are stepping it up. We got this next level. AI even will change background. That's how excited he's for the guests.
Will Sanchez: I had to step up, man. You, you, you, you and your AI backgrounds have been making me look like a fool, so I was like, man, I'm gonna step up my game if now I'm not gonna hear the end of it, but you know, it's, uh, it's good to see you.
It's great to have our guest. As always, let's give a shout out to Mike B and the folks at the Recovery Shop. [00:01:00]
Dr. Grant Garcia: So, yeah, so big shout out again to them and they just keep trying to step it up. I mean, the thing is, it's really great for our patients, and actually I know Dr. Use recovery shop as well. Uh, but patients, you know, I had multiple today saying, Hey, I, I, I like what your surgery is.
I like some of the biologic things, but what's the next level I can go to? I really wanna get the best outcome. And whether or not, you know, always the data is always there for some of these things that patients really wanna know and have an option, and they're gonna go aftermarket, or they're gonna go through someplace that's more reputable if you can have it So.
It's really great to have it. They need nutrition, braces, machines, anything you need and things that we want, it all can be there for them. So it's a really nice option. So thanks again guys.
Will Sanchez: Hundred percent. And as we, uh, get ready to introduce our, uh, our guest, Dr. Anthony Yee, uh, just quick background footing ankle specialist at the orthopedic specialist of Seattle.
Trained at USC. Went to ub, went to Harvard. I eventually, I wanna find out what's going on. Where is his? You know, alle allegiance to, you know, is he a [00:02:00] Trojan? Is he a husky? You know, in fact, maybe we can ask that question. Now let's bring on Dr. Yee. Dr. Yee, welcome back to the show. It's been a while. It's great to see you.
And just a little quick background, Dr. Y performed surgery on my Achilles rupture. So I have a love hate relationship because I went to go see Dr. Yee in a very bad state, but he put me all together. Dr. Yee, welcome to the show.
Dr. Anthony Yi: Thanks for having me. Uh, good to see you Will, um, really excited to be here tonight.
Will Sanchez: That's great. Um, hey, let's get, just let everybody know a little bit about your background. I kind of teased it in the segue, uh, you know, with your background with USC and Harvard and UDub. But let everyone else know a little bit about your background and, and what you do and, uh, and really why you specialize in this specific area.
Dr. Anthony Yi: Uh, so I'm an orthopedic surgeon here in Seattle, Washington, and, uh, I [00:03:00] subspecialize within orthopedics within foot and ankle. So that's probably about 90, 95% of the care that I provide. With regards to foot and ankle issues? Um, I think that the biggest draws to me for foot and ankle, uh, were during training.
Um, the mentors that I had, uh, uh, some of the most, uh, generous, uh, wise folks that I've come across. Um, and then in terms of the actual work itself, uh, the things that really turned me on foot and ankle were, uh, the. And, um, meat help patients of all different types of backgrounds, whether it's, uh, younger, uh, children, um, you know, young adults, middle aged folks, older patients that get to run the whole gambit.
And that's, um, I, I like that having a little bit of different flavor from each part of different walks of life, uh, different, uh, issues. And it keeps me on my toes, so to speak. I like to have that [00:04:00] variety. I like to, uh, go to the, or. You know, jump from, you know, fixing an ankle to repairing an achilles, to replacing an ankle joint, uh, to doing something, uh, altogether different each step of the way.
That's fun for me.
Dr. Grant Garcia: Balance, like, I mean, one thing you really focus on is minimally invasive techniques. Can you kind of go through a little bit more of that in terms of what your focus has been? I mean, I know that that's all, a lot of, that's new. I mean, I trained doing some foot and ankle at HSS and we didn't really do a lot of minimally invasive options are good to see them.
Right. And then in practice I don't do that. So I'm just curious as to what your focus has been because that was, that's been a really big deal for foot and ankle because foot and ankle has always gotten a bad rap about the healing ability of the foot and the ankle because it's so far away from the heart.
So can you kind of go through that and what the benefit is to patients and what's, what's your thoughts on that?
Dr. Anthony Yi: Absolutely. You know, I think that's one of the things I'm most passionate about is minimally invasive surgery when it comes to foot and ankle. And also similar to you, I had. Exposure to it at all during residency.
I, I didn't even know what it was, [00:05:00] um, until fellowship And, um, learning those techniques and seeing what it does for patients was, was really eyeopening experience. I'll be honest, sometimes the first time I saw some of those techniques, I would say, there's no way I'm doing that. That's crazy. Uh, but you know, again, going back to that, um, you know, humbleness and, and thirst to, to always be better and find the best, best techniques and methods for patients, I think, um, you know, uh, one of my mentors always said, you know.
Sort of change your, the way you ask the question, you know, it says, don't ask what, um, what you, you can through do through a minimally invasive techniques, but what you can't do, um, but you know, all the while. Being cognizant of, you know, putting patient safety and outcome outcomes first. But, um, I think that, you know, it's, it's been a journey so far.
You know, it, it means, you know, spending time in the lab, uh, [00:06:00] practicing the technique, uh, learning from other people and talking about what works and what doesn't work. But in a nutshell, I think it's the idea behind it's try to get a really good outcome for your patient, um, but minimizing that soft tissue injury, keeping the incision small and.
Uh, with all the purpose of, um, less scarring, less pain, less inflammation, and, and getting the patient, um, back, uh, at least a bit of their life back as soon as possible. You know, so, um, for example, some, with some of the techniques,
you start getting patients weight bearing right away, as opposed to some of the more traditional techniques where we've.
Historically them off entirely for, you know, four to six weeks at a time. Um, and so, uh, yeah, that's, that's been a, a major game changer. And, um, I think we'll, we'll probably see that much more and more
coming [00:07:00] years.
Dr. Grant Garcia: Awesome. Do you wanna bring that up? Will, can you bring up that bunion correction situation and show the people that. Anthony, you talked about kind of like some wildness you first saw and then now you were kind of a mainstream. Will you go over this a little bit and kind of describe the situation here?
Dr. Anthony Yi: Yes. So this was exactly what I was talking about earlier. The first time I saw an x-ray of this, there was, um, you know, I was like, you know, this, that looks crazy and I don't know that I'm gonna do that. But after seeing time and time again, how well patients were doing, um, fellowship, you know, this is something that I couldn't deny, um, but.
Basically we can, I can do all this work, uh, for the bunion correction through four small incisions, so four total stitches. Um, so using a special instrument, uh, called the minimally invasive Shannon Burr. And relative to, um, some of the other instruments that we use in orthopedics, uh, this spins at a much lower.
Revolution per minute. [00:08:00] So the idea being it doesn't generate as much heat, it doesn't damage the soft tissue as much, but when applied correctly, due to the design of the bur itself, how it's engineered, you can still, uh, if again, use correctly cut bone. So perform what's called an osteotomy or a controlled cut of the bone to move and shift and correct the position.
Of, for example, something like a bunion here. Um, so on the left side, you know, you can clearly see, uh, this patient had a bunion, which is a, you know, not necessarily extra bone, but. If you look at the right side of that left photo, um, the long skinny bone in the middle is pointed towards the right side. Um, and so effectively the foot widens and that area gets quite irritated and rubs.
And then if you see on the right hand, x-ray. I've made [00:09:00] a bony cut and I've actually shifted the round portion of that long skinny bone, the metatarsal over to a corrected position, and it's being held in two place with two screws. Um, and then there's a little bit of fine tuning of that correction with the bone above it.
You see a third screw up there. Um, and, and, and I think this has been a game changer. You know, I, I let patients actually walk out of the surgery center in a flat postoperative shoe. Immediately after surgery. Um, and, and you know, I ask them to take it relatively easy. I'm not having them go run laps around immediately, but, you know, they get at least a part of their life back pretty quickly, uh, with this technique, uh, which has, which has been been an awesome experience for me and, and the patients more importantly.
Dr. Grant Garcia: And then will you show that other slide Will, so can you, what kind of was the old way of doing this? I mean, this is obviously pretty new stuff and it's been really impressive some of the results.
Dr. Anthony Yi: Yeah. Um, so some of [00:10:00] the more traditional, you know, techniques which, you know, I'll, uh, you know, you'll, I'll use in the right setting for example.
And one popular, especially here in the northwest is the, well you'll probably heard here as the lapidus procedure or there's also lipoplasty that's pretty con, you know. A specific company's, um, instrumentation that's very popular and it's been advertised fairly heavily. Um, but with that it's, you know, generally a bigger incision and you're trying to shift and move bones and fuse them to other bones.
And so traditionally, you know, often times, you know, staying off of it, the foot completely for six.
Surge around the foot and ankle that, you know, that is, that's quite limiting. You know, that's, that's hard. You know, will, will knows about staying off of the, of the foot and that, that's challenging. Crutches are nobody's friends, you know, I, you know, I've seen all levels of athletes including professional, you know, struggle on [00:11:00] crutches.
That's, that's no fun. So, um. I think that's been the, the, the major game changer and, and that, um, and you can see on that series of x-rays there. So the, the leftmost side is, is before surgery. The middle is, um, six weeks after surgery. And so looking still a bit crazy there 'cause we're not seeing bony healing quite yet.
And then, but you can see how much bone fills in, uh, at that six month mark. Um, so, uh, to the point where that's the leftmost screw along, that first metatarsal is completely surrounded by, with new bone at that point. So, um,
Dr. Grant Garcia: is there a faster weight bearing with this than the regular?
Dr. Anthony Yi: Yeah. Yeah. I'll let them wait there right away in a flat post-op shoe.
So they'll walk out of the surgery center. Um, as long as the bone felt good, there are some caveats. So, you know, if, if subjective, it is a bit subjective. If I'm worried about the bone quality as I'm putting the screws in, just like when you're putting the screw into a piece of wood, you get a sense of how, how [00:12:00] good that bite of screw is.
Now, I'll, I'll, I might, I might just have them put weight through their heel only, uh, through a special shoe, but still getting them at least part of their life back immediately.
Dr. Grant Garcia: Do you? Um, and then from these MIS things. What other, what other things you really like? I mean, we can show some syn, some scope things.
What other things have you brought in the last, like couple years? Are you really excited about? From
Dr. Anthony Yi: standpoint, actually, um, you talked about his Achilles injury and was. He was smart about his injury and got medical attention right away, but, you know, um, some people un uh, unfortunately, um, might not get, have the diagnosis early on or right away or in a timely fashion.
And, and in some cases. Um, rupture goes untreated, you know, you know, whether it's surgical or non-surgical. It's important to really, um, identify it first and, and [00:13:00] have it treated. Um, then, and in those situations, if it goes untreated, unfortunately that tendon can, you know, heal in a stretched out position.
So you see that, uh, image, uh, on the left. That's a nice job of showing what an Achilles tendon sort of look like. You know, it's never a clean tear. It's like Mopp ends, uh, on both ends that have, uh, torn away from each other and, um, if not properly treated, ill heal in that stretched out position. So sort of like that rubber band you've used.
One too many times, uh, it's not gonna, you're not gonna be able to generate power through that. And, and in those situations, um, you know, the sort of, um, uh, more traditional technique, make a huge incision along the back of the Achilles, open it up. Clean it up and then maybe do things like a tendon transfer and then get those two tendon ends together and the proper tension.
[00:14:00] Um, but one of the things that I've come to really enjoy is fun is doing it actually, um, doing it through a minimally invasive technique. So doing it all arthroscopically. Um, so two small incisions each needing a single stitch, um, on both sides of the Achilles tendon. And then. The ArtScope or the camera in there, cleaning it out.
And then, um, uh, finding, um, the FHL tendon, which is one of the two tendons that helps to bend the big toe down and then we can actually reroute that. Plug it in front of the achilles tendon, all arthroscopically. Um, which, you know, I'll admit, I'll admit that first started doing this. It was incredibly frustrating from a technical standpoint.
I was in the lab a bunch practicing this and just trying to figure out how to, how to get it to work properly, but. At this point, it's become something that's really fun and I actually look forward to doing now because it's, um, uh, amazing for, you know, for the patient to not have to have [00:15:00] this huge incision along the back of their heel.
And especially, like you were saying earlier, in an area that can be really tough to heal because the blood supply is just not as good as some other parts of the body.
Dr. Grant Garcia: Do you know, is this something, so the viewers already heard about Achilles, and we can go back to that in a minute from an athlete standpoint, but with this transfer option, do you, are you willing to do it more frequently now that you can do it through the scope or does that not change your indications for doing this procedure?
Dr. Anthony Yi: Yeah, I think, you know, definitely, um, you know, there are some patients that are higher risk, uh, like you suggested earlier, and, um, I worry a lot less. Uh, being able to do it through an arthroscopic approach. You know, for example, some patients might have some risk factors that have a higher chance of things like infection, but I sleep a lot easier at night knowing that this can be done through the scope, uh, scope now.
Um, and not, while not all of these injuries [00:16:00] require, um, uh, an FH shell transfer, you know, I found it interesting there, you know, relatively recently there was a, uh, a decent study. Foot and ankle international. Were very, very high level soccer players, um, across seas. Uh, were having their achilles ruptures treated like this primarily.
So instead of, um, you know, repairing the tendon end to end, sort of using that tendon as an internal, um, uh, sort of, uh, way to hold the proper tension. Uh, and to get that achilles to hold. So it's kind of like splinting it internally. Um, and, and those patients were able to return to very high levels of soccer though.
Dr. Grant Garcia: Do you think That's an interesting topic. Uh, that's, I never heard of that. So you're doing. They would get the repair of the Achilles like a lot of these athletes do. And then they would also get the FHL transfer or they don't, they don't repair the Achilles at all. [00:17:00]
Dr. Anthony Yi: The latter. So no repair of the Achilles at all.
And just using that to set the tension, not too different, I guess, from the concept of the mid substance SP speed bridge. So with the mid substance speed bridge, as you know, is, um, you're running some suture along the, the top. Portion of the, so when there's two ends, like the top and then the bottom of the rupture, locking in sutures at the top, and then you're bringing it down to meet the, the bottom end of the rupture, like this
Dr. Grant Garcia: one.
Dr. Anthony Yi: Exactly. And then you're anchoring it down into the heel bone in that correct tension. So you're, you're simply setting the tension, but there's not an end to end repair of the tendon. So, um, just a different way of achieving that. So,
Will Sanchez: okay. I'm sorry.
Dr. Anthony Yi: No, go. Well, no go.
Will Sanchez: No, I was gonna say, um, just kind of bringing the, some of the sports into this conversation, um, you know, we saw Deante Murray and [00:18:00] Jason Tatum.
We've seen upticks in the NBA, uh, I believe as of. We've had 16, uh, uh, Achilles ruptures in the NFL. We've seen Daniel Jones and George Kittle in the playoffs for the 49 ERs. Um, is there, is there any reason or trend that's been happening that, of why this is going on? Some people are saying, well, you know, maybe these guys are just training less.
Right. You know, because they're playing more games, they're not practicing as much. Maybe they're not in, you know, the shape that they used to be when football was doing two aday, or maybe we just don't have the data back then. But is there any correlation, uh, you know, or reason why this is happening or it's just like, Hey, this just what's happening right now for whatever it is. And, uh, we're not exactly sure, but it's something to monitor,
Dr. Anthony Yi: I think. We're not entirely sure, but there's some. Reasonable speculation. [00:19:00] Um, I think in terms of, I think sports sciences come a long ways in terms of nutrition and exercise and, and monitoring minutes and. We're, I think we're getting to a point that, you know, much, much improved and back with, back with data.
Um, and that's always good. Um, but some of, I think some of the spec, uh, speculation, um, you know, I think, uh, shoe wear has changed a lot. Playing surfaces have changed a lot.
I think that there's some speculation with regards to two, both of those two, I don't think anybody can outright prove it. Um, but I think that's where a lot of the conversation is right now and probably where a lot of the attention will be spent in terms of, you know, seeing if there's any, any correlation.
Um, but, you know, I think from a, you know, nutrition and, and strength and, um, uh, [00:20:00] you know, um, athletic, um. Uh, shape wise, you know, I think, I think the modern athlete is, is, is pretty good.
Will Sanchez: Does it matter that they all have their own personal trainers and everyone's kind of doing their own thing? When you looking at Christian McCaffrey and the way he's training and, you know, maybe emphasis more plyometrics and this, uh, you know, these bursts, he trains pretty much as a track athlete, as a football player compared to someone that is just, you know.
Lifting heavy, going hard with certain things that it seems like all of these players have their own trainer, right? LeBron James is famously known for spending millions of dollars on his own trainers. Could, could that be also, uh, something to consider if they're not getting the proper training for their body type, for their age, um, for anything else that plays along with that.
Dr. Anthony Yi: I think you have a really good point there and I think it makes it that much harder to, you know, study and look at when, [00:21:00] you know, there's not a standard protocol and not that there should should't necessarily be one, but yeah, I think that's, that's a great point. You know, it's hard. I think it's hard to, when there's a lot of, uh, different variables in the mix.
Uh, certainly hard to, hard to say. Um, but I think that you might be onto something there too.
Dr. Grant Garcia: Anthony, can you tell the viewers, like you deal with an athlete with tendinopathy, obviously the acute rupture's pretty obvious, right? That's surgery. It's pretty straightforward. But how do you deal with that spectrum, right, because it's a little bit harder.
Because we know that occasionally these tendinopathies from induced from maybe injections induced from over training can go under ruptures. So do you have a threshold ever that you change your management or how does that work for you with that athlete? With the tendinopathy?
Dr. Anthony Yi: Yeah, that's a great question.
You know, it's, you know, you want, you want these athletes to stay, you know, on the field. Um, and then, you know, not necessarily, and [00:22:00] do, you don't want, we don't want to do unnecessary surgery. But on, on the flip side, we don't want it to become an urgent issue where, where an unhealthy tendon that's been stressed constantly.
Suddenly goes and ruptures, you know, we definitely see that happen, uh, unfortunately. And then also, uh, in, in those scenarios, uh, sometimes it can be a more rare variant, you know, in that picture that we had up earlier of the, what we call the mid substance Achilles ruptures, where there's a tear along the center of the tendon itself, you know, that's a lot easier to, to treat.
Um, and. From, you know, a, a technical standpoint in terms of, uh, how we repair that. Uh, that's a fairly straightforward, you know, surgery overall, uh, that generally doesn't take so long. Uh, but there is a rare variant of like, you know, Achilles tendon sleeve avulsion. Uh, rupture where the tendon tears directly off of the heel bone.
And so there's [00:23:00] no, there's no tendon to tendon to tendon attached.
Will Sanchez: No thank you. No, thank you.
Dr. Anthony Yi: And so in those scenarios, it gets a little more complicated and, and, and quite frankly, much more technically challenging to, to repair that back down onto the heel. And, and I see that. Happen, unfortunately, usually in the setting of a patient have, having had chronic or long-term pain along the Achilles, they've had this tendinosis, they've been struggling with, um.
And, um, yeah, in terms of, you know, to more directly answer your question, you know, how do, how do we balance that? You know, I think, um, it, I think it just takes regular, you know, check-ins and, and, and education, uh, with regards to, to what to look out for. Uh, you know, we wanna stay active, but we don't wanna push it to a point where it's really flared up because that we're, we're probably teetering on the edge of, of potentially, uh, resulting, resulting in a rupture.
You know, I recently had a patient who, [00:24:00] um, was in that situation. She was diligently working through pt, uh, but just had had this unhealthy tendon for. Many, many, many years. And unfortunately, you know, she was doing her stretches at home and then it, and then she had the injury, the sleeve avulsion. So, uh, we went and got that taken care of pretty quickly.
But, um, but yeah, that, that was one of the cases where, um, you know, it, it makes you wonder sometimes, you know, when, you know how, how do we balance it? And I think part of it is just having a, uh, edu the education, uh, talking with the patient and having regular check-ins. Um, going over safe exercises and, um, you know, signs and to look for.
Will Sanchez: Uh, Dr. Yee, can you, uh, talk about, you know, I, I mentioned it to a couple people after I had my Achilles rupture, and, um, how antibiotics are the type of antibiotics, uh, weaken your tendon? Can you explain that to the audience? Because I think a lot of people don't [00:25:00] realize that there is a correlation.
Correlation and what specifically that does, and what's the timeline if you are on medication? Before you ramp up to explosive activity?
Dr. Anthony Yi: Hmm. Yeah, that's a great question. So. Uh, we don't entirely understand it, but there is a type of antibiotic that falls under the class of, of what's called a fluoroquinolone.
And so it can be used for a variety of different infections, including things like, uh, upper respiratory tract infections. Um, and, but there is a black box warning label on it, meaning it's, um, you know, when it's prescribed. Basically in huge letters is a warning that, um. That, that it can cause tendon to weaken and in some situations tend to rupture.
Um, it's something we always look out for, uh, and talk to patients about. Fairly rare, to be honest with you. [00:26:00] It's probably, you know, one of those things that, I mean, it, you know, it is, um, you know, certainly, you know, we, we need to talk about with patients, but, uh, still pretty rare. I think the percentage is percent of patients who are on that, on antibiotic, who ultimately have a rupture is, is pretty low.
To the point that, you know, would not lose sleep over it, but something to keep an eye out for, especially if you were starting to have some symptoms like pain along a tendon, those types of things. Um, but yeah, that's, that's the black box warning label for those, you know, I, um, have seen one patient. Um, who unfortunately was on an antibiotic that, that fluoroquinolone antibiotic and, and ultimately had had a rupture, um, and got it taken care of.
But fortunately overall. Rare.
Will Sanchez: Do you have a timeline if, if when somebody wanted to be safe that you're on this type of antibiotics? Uh, and I don't know if the data shows that anywhere to say, well, you know, once you're, [00:27:00] if you started it last week, you're on for seven days.
Dr. Anthony Yi: Yeah.
Will Sanchez: If you're prone to injury, you know, I would be mindful for the next eight weeks.
Or is there something there that you can kind of give some guidance if anyone wanted to be extra safe, especially for your. Older weekend warriors Yes. That are going out there and being active, but not consistently where they're a little bit more prone to injuries.
Dr. Anthony Yi: I'll be honest with you, I don't know entirely.
Um, but my suspicion would be that, um, you know, I if that, and I don't have proof for this, but, and I, I'm happy to look this up, but if, if. Um, you know, if it's, once it's cleared the system, I think that it's probably okay to start, you know, easing back into the swing of things. Um, but I think just thinking about it from a, you know, pragmatic standpoint, you know, if you're, if you're sick and on an antibiotic, you're probably not gonna be running around, uh, too soon.
So, but once you're recovered, I think it's is [00:28:00] probably a safe time to, to get back. So, so, because I would suggest to you. Completed the antibiotic treatment and then you're, you've cleared whatever infection you've been, you've been dealing with is probably out of your system at that point. Thanks
Dr. Grant Garcia: Anthony.
Will you go into, so we've got obviously things that can increase the chances of rupture. How about things that decrease? You talk about biologic therapies both in for Achilles or tendon ruptures or, or pre ruptures, like, so how you deal with the chronic one, and then do you do any biologics ever or is there any consideration for the future?
Dr. Anthony Yi: Future? Yeah, great question. Um, so for the chronic situations, you know, biologics, like things like PRP. Um, like the platelet rich plasma, as you know, getting a sample of blood from the arm, putting in that special machine that spins around super fast and then it layers out the components of the blood and we can isolate the healing portions and then inject it into specific, uh, body parts.
Um, that does, uh, fairly well, I'm not gonna say a grand slam, but fairly [00:29:00] well for things like chronic tendinopathy. Um, and you know, I usually reserve that. For situations where we've tried the really basic things like the home exercises, the, some physical therapy, and then if we're not in a good spot, I'll bring that up as, as an option because I think it's reasonable at that point for the more the chronic tend tendinopathies or tendinosis.
Um, and then in terms of, you know, the role within, you know, like at the time of surgery or at the time of injury wise, um, probably the biggest application that I use it is for, uh, cartilage injuries. And so like around the ankle joint itself, you know, once people, um, might have a twist or turn of the ankle, um, and then we get really.
Um, honed in on, on the, the ligament sprain or the ligament tear, but sometimes the, um, you know, we don't pay as a much attention as we should to the actual joint itself, where there might be a little pothole or a little divot that's formed where the cartilage was. And so kind of like when you [00:30:00] drive a car over the pothole, that can be uncomfortable in the ankle joint and sometimes that can feel unstable.
And over time, the rest of the road might start to crumble a bit, meaning the rest of the joint. And, uh, in these situations, um, you know, oftentimes when I'm
treating these types of cartilage injury for the ankle itself, uh, unfortunately we don't have. I don't think as many options as like the knee. Uh, I know, uh, Dr.
Garcia has, has the amazing, um, tool in his toolbox of, of Macy, for example. Um, uh, that, that's not FDA proven the ankle quite yet. Um, uh, but, uh, and, but what, what I have in my toolbox is, um, some forms of cartilage repair, kind of like repairing or patching up that pothole on the road. So, you know, filling it in with gravel and then sealing it off and that gravel might be a little bit of bone graft and then sealing it off with a substance called bio [00:31:00] cartilage or, uh, sim.
Something similar to that. But basically fancy way is, it's a extracellular matrix. So basically a scaffolding upon which new collagen can can grow. And it's not the exact same type of cartilage that you're born with, but it's a pretty good reasonable substitute and there's pretty good data showing that it's gonna last you 10, 15 years and, you know, eight outta 10 people, even at that time point, are doing pretty well.
And, um, there's even a recent study that came out for, for the, for the Foot and Ankle was saying that maybe even last 20 years. I'll be honest, I'm a little skeptical of that one, but I think probably 10 to 15 years sounds about right.
Um, uh, and then, uh, for the bi biologic portion of it, so I, I'll generally get some stem cells or, or PRP and I'll mix it with that.
So sealant, so to speak, the, the bio cartilage. And that's been, that's been shown to that, that that can improve results for patients in terms of, um, you [00:32:00] know, pain relief, uh, and, um, filling in that pothole, so to speak a little better. So that's probably the main, do
Dr. Grant Garcia: you do this arthroscopically or open?
Dr. Anthony Yi: Yeah. Um, I try my best to do it arthroscopically. Um, but if it's in a really challenging, tough spot on the back of the ankle or, or, um, I'm not confident that I'm gonna be able to do the best job of it, just through the scope, I'll, I'll make a, a slightly bigger incision, but. Generally my approach is to at least start off arthroscopically because, you know, with a little bit of positioning in the ankle and the correct positioning, it's, it's pretty cool where you can, you can, uh, you can reach some far places in the back of the ankle sometimes.
Dr. Grant Garcia: Talking about, I think arthroscopy. Will I, will you talk a little bit about how, you know, we talk about, we do knee, you know, do knee scopes, shoulder elbow, but the ankles, you know, a different animal. There's some other things you can do, um, from the [00:33:00] perineal tendons, et cetera. Will you go into kind of your gamut of arthroscopic options?
I mean, it's definitely expanded, I feel like, over the last five, 10 years.
Dr. Anthony Yi: Yeah. So, you know, arthroscopy a really good tool. Um. Uh, so as you know, making small incisions, uh, either front or back of the ankle, you can, um, take a good look around, um, using a small couple millimeter camera or arthroscope, uh, going into the ankle joint and getting a really, really good look at it.
Um, some of the ways that Ive. Used it more and more my practice, or for example, uh, trauma, uh, that you see athletes, you know, breaking their ankles or, uh, you know, having, uh, high ankle sprains or, you know, syndesmosis tear. Um, I think the scope is a really useful tool, uh, because it allows us to take a really good direct look.
Structures such as ligaments that are torn the rest of the joints, and then [00:34:00] also gives us the ability to do something called a, you know, like a dynamic evaluation. So in real, in, in real life, you know, I can move the fibula bone and, you know, and right here, for example, you know, I'm putting, um, an instrument called the shaver on, so the, this is someone's left ankle as if they're laying down on a table.
And so I'm putting this, um, instrument in. From the front of the ankle. And so to the left of this picture is the shin bone, the bottom is the Alis, and to the right is the fibula bone. And so those three bones are the main bones that come together that make your ankle joint and with the high ankle sprain.
The ligaments that connect, you can think about them like ropes, connecting two bones, connecting the fibula and the tibia. So the shin bone and that side skinny bone on the little toe side of your ankle. Uh, those tear. And if I press on this bone from front to back or side to side, sometimes I can [00:35:00] see that fibula shifting and the tibia staying still.
And so that's a nice sort of dynamic way to evaluate. You know, not only is the ligament torn, but is it also unstable? Because there are a lot of things that can tear but are not unstable, that we don't necessarily have to repair or address sort of surgery, and our bodies can do a reasonable job of repairing.
Uh, but this is. There's been a nice way, really nice way to, to evaluate and without causing significant trauma. You know, there, there are ways to, you know, make a big incision and look directly at the syndesmosis or the relationship between the tibia and fib, but this is a really nice way of doing it to really small in a, in a minimally invasive fashion.
Dr. Grant Garcia: Do you, do you think this is something, is this something that you've already made the decision to do it or this sometimes helps you make your decision on what to do?
Dr. Anthony Yi: A little bit of both. I think, uh, most of the time I'll probably go in there, um, if I'm suspicious enough based on their pattern of injury that they've also [00:36:00] had a high ankle sprain on top of everything else.
Um, I'll, I'll talk to them about the pros and cons of just going ahead and doing the, the scope, uh, to begin with. Uh, but sometimes, um, you know, if you're on the edge or. I'm not entirely sure that that can be a nice tool tool as well to, to help you, help you decide what you need to do.
Dr. Grant Garcia: Um, I wanna come back to the high ankle sprain 'cause that's a really common thing.
We see it a lot in sports. I know Will, I'm sure Will, has tons of players have top his head. He can think of that. He's had to do, seen that before. But this ankle fracture idea, obviously we're both Giants fans. So Cam getting the ankle fracture, do you think like. How has the role of this ankle scope evolved?
Because I know you started doing those at our practice. That was pretty cool because I had not seen that as well in my training. Um, what percentage now are you doing ankle scopes with the F or the fixation of the ankle?
Dr. Anthony Yi: Yeah, so any higher energy ankle [00:37:00] fracture. Um, and I'll define that a little better, but I'm scoping and, and the rationale is that, um, higher the energy, uh, there's gonna be almost certainly something in the joint that's going on, whether it's a loose piece of bone, loose piece of cartilage, or, um, like an osteochondral injury.
So like a divot in, in the cartilage slash bone. Um, high percentage I'd say have an injury like that. And the high energies that I consider are, if there was a dislocation. I am for sure doing that because it's almost certain that there's something that's happened. Um, or, um, you, there are, you know, the three sides to the ankle.
So bi mular, ankle facia be two sides that are broken. Try Malia be three. Any try Malia or all three sides are broken. That that generally, uh, suggests a higher mechanism of injury as well. I'll put a scope in, in that ankle as well. Um, and then also other things. If there are [00:38:00] clear evidence of ligamentous injury that looks unstable, uh, for example, let's say there's a fibula fracture plus the syn osmosis looks awfully wide, that tells me as well that allot of energy went through that ankle.
So I'm, I'll put the scope in there as well.
Dr. Grant Garcia: Do you think so? But when you put the scope in, so that's good for the listeners, obviously they're gonna get an ankle RIF for somebody and they don't get the scope, which obviously is not something that, you know, if I'm on call and doing ankle fracture, I probably don't feel as comfortable scoping an ankle if I haven't done that many.
Is that a reason to consider someone like you as a specialist to do it? Like what is the benefit of having the scope? You can treat it there, or is it just information?
Dr. Anthony Yi: I'd say both. You know, if there's an, there's an injury there, you can treat it. You know, I never don't wanna leave anything loose in the ankle joints 'cause that can cause problems later down the road.
So addressing it then and there, um, and then if there is a tailless injury. Um, uh, you can also consider, uh, treat treating it, but I, I, I have a conversation [00:39:00] be before with the patient with regards to the pros and cons with that, um, uh, before going in and so that we're ready to go. If, if I do notice that.
But I think, um, you know, at a minimum it also gives us information about sort of what you can expect into the future. You know, so I think, you know, the best case scenario I say, Hey, your ankle actually looked great. It looked clean. I'm not too worried about the cartilage. It, you know, it actually looked really nice in there.
So I'm really optimistic that, you know, we're not gonna have to, we're hopefully not gonna have to deal with a much in the way of arthritis down the road, or wear and tear the ankle. Um, and then, and then let's say that there is a cartilage injury, then I can say, Hey, you know, we'll have to, you know, unfortunately, see how the ankle does.
Uh, there was a pretty big cartilage injury there. Um, I cleaned it up, I treated it, but, you know, uh, um, you know, history, you know, suggests that your, your ankle might wear out. Faster than [00:40:00] we hope for. And, and you know, if that time comes we can, you know, talk about treatment options. But, you know, I think good, good for the patient to have in the back of their head so they, uh, so they know, um, sort of they can sort of plan, plan their life accordingly and keep that, and keep that in mind moving forward.
Will Sanchez: I think my ankle. That's good point. No, I was just gonna say, I think my ankle and calf has tightened up, uh, since we've had this conversation. I'm feeling every little nook and cranny. Um, I, with all the evaluation and all the, all the conversations of Achilles and, and dislocations and everything else, I'm just, I just wanna throw it out there.
I'm checking myself here. But all jokes aside, he
Dr. Grant Garcia: might be going under, going to scope soon. Who knows to
Will Sanchez: get his evaluation, I'm going in, I'm gonna make an office appointment right now. Check everything out. Um, for Cam that had this injury, we saw Fred Warner had this injury. He looked like he was ready to come back for the playoffs.
Just amazingly freak athletes. But when you're evaluating somebody, uh, [00:41:00] with such a serious injury, what are the steps to not only get back to, you know, everyday normal, but performance normal? Uh, and, and, you know, where do you go? Hey, thumbs up, you, you're clear, and what's that process look like?
Dr. Anthony Yi: Yeah, absolutely.
Will Sanchez: With that type of injury.
Dr. Anthony Yi: I think at time zero, making sure you don't miss any other injuries. So you know the big, you see the big obvious one in front of you would always take the time. Um, you know, as a provider to check them from head to toe, make sure there's nothing else going on. So the last thing we want is we, we fix the ob exactly.
Fix the obvious issue, but there's something else lingering that, that causes problems down the road. Um, and then, um, the next part I think is coming up with a thoughtful plan on how to, how to best, uh, tackle it, you know, um, managing the soft tissue portion of it. So, you know, you know, one of my mentors always said, you know.
A fracture is only. Um, an injury beneath, [00:42:00] uh, a bigger soft tissue injury. So making sure that, you know, we're not missing something else there as well. And we're handling that with care so the patient will recover as well. Um, and then thoughtful surgical planning. You know, if, if you're concerned that you know you're not, or if something looks off and you're not quite convinced that this is looking straightforward, don't be afraid to, you know, get more imaging.
Sometimes things like a CT scan can really. Uh, open your eyes to things that you might have otherwise missed. X-rays are a good screening tool, but don't show the full picture. Um, and then I think game planning for, for the, or having a plan A, B, and C and having those backups available to you, um, you know.
You know, just, just like a game plan going into a game doesn't always, they're not always going with game plan A, you know? Um, but having plan B may not be bad. Plan C might not be bad, but, you know, having those options to, uh, to, to make sure, you know, for example, [00:43:00] like instrumentation, uh, you may be set on using a certain implant.
But being aware that maybe that doesn't work out and you have to use something else to, to get the job done. Um, and then, and then, you know, just not leaving the operating room until you're completely happy with, with how it's, how everything is looking. And so, um, just, just really, really taking your time and, and knowing that.
Maybe even if you had to redo a step that might add 10 minutes with that, that may be the difference between getting this thing perfect and not, um, and just, just being humble enough to acknowledge that. This is what
Will Sanchez: every patient wants to hear. By the way. I, I mean, you're, you're, you're, every patient that comes in wants to hear that from their doctor.
I'm gonna go in, I'm gonna check it out. You know, it's almost like checking the list, checking it twice, seeing if you're an audio nice. And that's what you're doing. You're being extra nice by doing that stuff. So, as a patient. That's hearing what you're saying. That's exactly what I want to hear. You're going in, you're doing the job, [00:44:00] but you're checking everything and making sure that when you're done, if you are happy, then I know most likely the.
Dr. Anthony Yi: Yeah, absolutely. I completely agree. And I've actually written down a list with it. If the case is getting really complicated and I always say, Hey, can someone check that box right there as we're going, going through? And just to, just to make sure you can never be too careful. And then, um, and I think the other, on the other side of surgery, I think the, the rehab.
Uh, is super important, so making sure you've got a good team and, and folks that you trust, like, good. I think we're lucky here in Seattle. We have some awesome physical therapists all throughout that do a really nice job and, and one of the things I most appreciate is the communication sort of back and forth, whether it's a text or a quick call or an email saying, Hey, so and so is doing great, or.
Hey, what do you think we should do at this point? You know, I think that goes a really long way. Um, and, and to your, to your question. I think that, that, that's what makes, makes [00:45:00] or breaks, I think the, the, the rehab and getting someone, uh, the, the, all the way there, not just halfway there.
Dr. Grant Garcia: So I wanna do one more question then we can start wrapping up, because I know that Dr.
Y's gotta get. Still with the, the monsters that were running around upstairs, uh, that we all heard. Uh, but anyhow, we got a lot going on and obviously we wanna be careful of your time. So this is a big deal, right? The mental aspect of the surgeries that we do is no joke, right? The, my regular surgeries, cleanups, things like that, those are pretty quick to get back.
But some of these foot ankle surgeries are not a joke. I mean, you gotta see the, a different, Achilles is a different animal obviously than an ankle fracture. How do you deal with the athletes in talking about foot and ankle surgery? I mean, they're, most of the surgery you're doing, they're not quick recovery.
Dr. Anthony Yi: Yeah, it's a great question and, uh, will, knows this better than almost anybody, but, you know, I just, I, I just try to have a very real conversation from the first time we meet. So you come into my [00:46:00] office with an Achilles rupture. I'm not gonna sugarcoat it. I'm just gonna play and say, this is going to suck.
This is gonna test you, it's gonna test the people you live with. It's gonna mm-hmm. Gonna test the people that you love and that we're gonna be taking care of you. Um, this is probably gonna be the hardest injury you recover from, you
know, and, but the good news is that we'll get you there, you know, and, you know, my goal is that, um, know it may not be 100% of what you used to have.
But by and large, the average person at this injury is, is gonna get there, is gonna be able to do the things that you, they wanna do and they love doing. And so we'll get there. But you, it's, it's, it's really tough and probably something we don't talk about enough. But I'll say there's a lot of people that get really down and depressed, uh, especially in that first six to 12 weeks.
Uh, when you're, you just feel like everything was taken from you, right? You're just, you can't [00:47:00] even, you can't even really walk. Um, and so it was just the basics of day-to-day life are extremely challenging. And, and, and, um, so I just, I, I, at first once just try to, uh, have that conversation and then each check in, just check in to see how, see how they're doing.
You know, um, surprising how many, you know, uh, just even small things, you know. Um, I had a patient who came in and, you know, out of all things, he's a great athlete, had an Achilles rupture, uh, came in. He is like, Hey, doc, like. You know, my sex drive is just completely gone. Mm-hmm. At first I was like, why is he talking to me about this?
Then, you know, I realized, you know, it's like this, these are, these are the real life things. Right. And then we talk a little further and, and we find out, you know. He took the advice of friends and family and saying, Hey, you need to cut back on calories when you're, because you're not working out. And so he is like almost starving [00:48:00] himself and you know, so, um,
Dr. Grant Garcia: which is not good for wound healing. We can go into that another topic.
Dr. Anthony Yi: So like, so just the whole process. So there's a lot to it, you know, I think things we don't always think about, simple things that we don't cover, like nutrition. Um, mental health, all those things, super, super important. Um, but I think just spending a few minutes to make sure that your patient's good and that they have the support, I think can go a long ways.
Will Sanchez: Yeah. That, that's a good, that's a good point. I just wanna jump in real quick. I, I'll just spend 30 seconds on it. You make a excellent point, and, and I think that listeners to really, uh, focus on that, it's, it's really difficult and you need to talk to someone. I did get depressed. It was hard on my family.
Thankfully, I had the nice machine, you know, a little shameless plug for the recovery shop where my wife could just fill in a little bit of water and I can manage everything from my chair, and she didn't have to run for ice every 20 minutes, so that that was really helpful. [00:49:00] But carrying the burden of taking care of myself.
Taking care of the kids, taking care of the household, you know, and dealing with all that. And you're sitting around. So when I went to the doctor, my testosterone levels dropped down because I'm not working out, I'm not being active. And you're feeling a certain way about your manhood, whether it's men or woman, but.
It's really important to realize that there's not just you're healing from the injury, but you're healing from so much physically, mentally, and you know you need to check yourself. So for anyone out there, we've talked about mental health on the show in the past, and you're going through this. Talk to someone, whether it's your doctor, your therapist, or anything like that, because that's gonna help you get through this.
The healing part and the surgery, Dr. Yid took care of that eventually. You gotta get to get into physical therapy because every single doctor that we've talked to says the same thing, I'm gonna fix it, but if you don't go to therapy, all my beautiful work that I've done, you just thrown it out the window and you're not doing what you need to do.
So just a [00:50:00] reminder to our listeners there. Go ahead. Just wanna chime in.
Dr. Grant Garcia: No, it's good. I mean, I think the important part too is you hear that. That's, there's doctors that care about the other side of things, right? We talked about the recovery shop, we've talked about the mental aspect. We've had mental health coaches on here. Professional athletes pay a lot of money for a mental health coach.
Dr. Anthony Yi: Mm-hmm.
Dr. Grant Garcia: We've talked to the people, we talked to, the guy that he's the Seahawks and Russell Wilson, et cetera. Like there's a mental aspect that's huge and a lot of us don't have the opportunity to have a coach like that. So you gotta find another ways.
Um, but what's, what the really good part is having a surgeon. Uh, Dr. Yee who thinks about those things and things that are coming to our practice in the future is the nutrition focus, right? Because that's kind of the lost art, is do we do the whole thing? Because as surgeons we're not good at the, like other things we're really good at, like the surgery part.
That's what we went to school for. That's what we were all the grueling hours before. But the part that's really important is like, how do we get to the next level? Like how do we dial up our indicate, dial up our success? And like y said, it's really important. So anyhow, I, we go on and on. [00:51:00] This is a whole nother show topic.
Maybe we'll have Dr. Y on again to talk about nutrition. Mm-hmm. And how he can get all of his, how he gets all of his ankles and surgeries back faster. But for now, I think this is probably the, the end of this nutrition conversation.
Will Sanchez: Dr. Yee, thank you so much for your time. We really appreciate it. Uh, a lot of great learnings, a lot of great information.
I hope that our listeners and viewers can really benefit, uh, from it. Uh, Dr. Anthony Yee with Orthopedic Specialists of Seattle. Uh, he's my doctor of choice, so I highly recommend. Uh, going to talk him out, talk to him and check him out, uh, because he is on the cutting edge of technology and has a great team to make sure that everyone gets back on their feet.
So, Dr. Yee, thank you for your time today.
Dr. Anthony Yi: Thanks for having me. And, and it's, it's easy to look good when you got good patients like you will. So,
Will Sanchez: yeah. Okay. Stop it. All right. Say goodbye to Dr. E, Dr. Garcia. [00:52:00]
Dr. Anthony Yi: Good to see you guys.
Will Sanchez: That's Dr. Anthony Yee. Um, you know, just to reiterate, I know we're running outta time here, but it's so important, uh, there, there's so many key things that he talked about, about making sure getting it right, right, doing the things that he needs to do to make sure that his patient, if he feels good, that that stood out for me.
If he feels good about the surgery, most likely the patient's gonna feel good about the surgery. Talking about doing the rehab, taking care of your mentors. Uh, so it's really important. And just like Dr. Yee and all of our other guests, we have transcripts shows. If you wanna be a guest on the show, check us out at sports talk com.
We're listening on every platform that you can think of. We're on YouTube, we're everywhere. Dr. Garcia, um, we're really happy for, uh, Dr. You to be on there. Your closing statements as we wrap it up.
Dr. Grant Garcia: Well, again, it's always great to have, you know, Dr. E does amazing job going over everything, and we are able to get a really long gamut because again, foot and ankle injuries [00:53:00] and athletes are huge.
We've seen so many of them this year. It's really al literally almost as common as some of the knee and sports injuries I deal with, if not more. Um, so it's been great to have an expert on here, and again, more to come, I think, on this. Uh, and we have a lot more topics to talk about, but again, if you're, if you're interested in being a guest, let us know.
We've had a lot of quests, had a lot of guests over the last few months, and we're gonna have some more coming up. And you never know who we're gonna have on. So it changes. We've had F1 drivers who orthopedic surgeons will maybe coming up soon. We've had really high level cartilage surgeons. We've had people that aren't doctors.
We've had different levels. You never know. So thanks again for everyone listening,
Will Sanchez: thank to Dr. Dr. Garcia. Appreciate your time as well.
Audio Transcript
From Disc Pain to Game Ready

Will Sanchez:[00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez with our favorite orthopedic surgeon in sports medicine specialist Dr. Garcia. Dr.Garcia, can you believe we did not win the Golden Globe for Best podcast? So they gave it to Amy. Unbelievable. I was like, wait a minute, we got robbed. I mean, this is this injustice, this podcast we have a great guest on, but we are gonna, we're gonna rant and rave. We demand a recount. What are you, what are your thoughts and how are you doing?
Dr. Grant Garcia: I, I'm good. Yeah, I totally agree with you. Uh, we got some, we got good backgrounds, so there's really no excuse for what happened, but nonetheless, um, yeah, no, I'm excited for our next guest. This will be a good, uh, change of pace from some of the other ones we've had on here, so this is great.
But first we [00:01:00] gotta talk about our sponsors.
Will Sanchez: Let's talk about Mike B. There you go. There's our guest there. But Mike B at the Recovery Shop. We love them. Mike B is great. Member to contact Mike and Mike b@shoprecovery.com. Dr. Garcia, why do you love Mike b?
Dr. Grant Garcia: I mean, they just work well for us as surgeons.
Surgeons, we have patients that get complicated surgeries or they want something extra after surgery, and it's really nice. Even as we modify our protocols, they can adapt pretty easily, which is really nice. So, you know, a nice machine, we're trying something new with different things every day. Uh, and those are there for the patients.
And, and I talked to patients today before surgery and they're like, Hey, I really liked using this. I felt, I felt really good about getting all this stuff that I needed before surgery, or if there's an issue. They can take care of it after surgery, so it's great. So thank you to our sponsors. Uh, but now moving on to our guests.
Will Sanchez: All right, everyone. Uh, today we have Dr. Bridget Rosenberg. She's joining us. She's an LA based spine specialist with over 30 years of experience, and she's the [00:02:00] creator of Advanced Spinal Restoration Therapy. Don't worry about it. Dr. Garcia and Dr. Rosenberg explain all that. That's not my job, that's theirs.
We just wanna let everybody know she's worked with high level athletes across every sport you can imagine. Lectures nationally on spine mechanics collaborates with orthopedic surgeons like Dr. Garcia to help figure out who can avoid the operating room. Bridget, welcome to Sports Doc Talk. We are really glad to have you.
Thank you for joining us.
Dr. Brigitte Rozenberg: Thank you for having me. I'm excited to be here.
Will Sanchez: We're excited to have you. Uh, we'll just kick it off real quick. Dr. Rosenberg, uh, 30 years in spine care, uh, thousands of patients, Olympic level athletes. I'm curious, what's the most rewarding text message or phone call, uh, you've ever gotten from a patient that made you think, yeah, this is why I do it.
This is why I love it.
Dr. Brigitte Rozenberg: I love it. Yeah. I mean, every time they, when they feel better, when they're back in their normal realm, when they're back in their normal lifestyle, [00:03:00] um, of course if it's an athlete and he is back in the court or back playing or doing whatever it is that they're doing, it's extremely rewarding, very rewarding to be in this, uh, position, day in and day out.
Um, and to even know that there's just so many things out there that we can do to help them. 'cause it's never like a one, one thing. It's never like one answer. Um, it, it's just, that's. Someone told me once you don't choose the profession, the profession chooses you.
Dr. Grant Garcia: Mm-hmm.
Dr. Brigitte Rozenberg: I really truly feel that. So it's just rewarding to be in this place.
I love it.
Dr. Grant Garcia: So, and I think this is really interesting, as Will mentioned, and I was saying this, you know, you're a different bit of guests that we have, sometimes many of the guests we've had are surgical intervention, right? And so it's nice to have someone who does no surgery to talk about that side of things, especially when it comes to spine surgery.
'cause as we know, spine surgery is a different animal than some of the other surgeries in terms of outcomes and choosing the right patient and really the non- operative stuff is something that we really like to. Do a lot of, or at least focus on, but many of the surgeons are not as good at that. That's right.
We're called [00:04:00] surgeons. We're do a little more of the surgery part, a little less of the non-surgical, so it's good to have someone like you on there. We've touted this sort of advanced spine restoration therapy. You talk a little bit about kind of what brought you to design this and a little bit about the program itself.
Dr. Brigitte Rozenberg: So, you know, I've been, I've been a chiropractor for many years and I always in, in my field, just like in your field, you can sometimes specialize in like doing surgeries on knees or shoulders or hips or spine. You know, everybody kind of finds their niche of what they like to do. I always treated patients after some kind of trauma, whether it was an accident, work-related accident, sports injuries.
Uh, car accident, you know, people that are really like in pain, not, you know, of course we can all do regular wellness, but that was always the kind of work that I was drawn to and the patient was drawn to me. Um, and so over the years there's just so much you can do with your hands or so much you can do with rehab and.
As, as we progress, we have so many, so many new technologies [00:05:00] and with the advancements of medical technologies, we can achieve so many great things. And when I start noticing and seeing it, we, I always use different modalities in my practice, but you know, as things advance, I see that. Putting them together in a very specific manner got so much more results for a lot of these patients.
A lot more than you can achieve with just doing your hands or just doing rehab. And definitely just by taking medication. And I think that's what kind of led me to put that program together that encompasses all these different modalities in a very specific, you know, formalized manner. Uh, and, and that's how we get the result.
It's not one thing, it's a combination of multiple things.
Dr. Grant Garcia: Will you give the audience a little bit about your background? I mean, obviously you've been in practice for a long time, but kind of where you started and then I know you mentioned how the patients you have, but how did you kind of. Get in this direction of doing all this.
Dr. Brigitte Rozenberg: So when I started 30 years ago, you know, chiropractic was a little bit out of the mainstream. It kind of had its own little world. Uh, but I, uh, my [00:06:00] first job was in a medical group that actually, funny enough, it serviced the studios where you had the Golden Globes yesterday. So it was very, it was here in the ally area and, and the, the medical group I was part of was servicing.
Those people that were either getting ready to, uh, shoot a movie or were very active while shooting a movie. So we had to go on set, um, along with seeing all those laborers that worked on the set. And so those are the kind of people that we saw. So it was either. They had some injury or they had to, they needed to prevent injury to some point, or, you know, they, they fell at work or they were lifting something extremely heavy.
And within that realm of working in that medical group, I also saw a lot of patients that were injured after car accidents and they were severely injured, like severe end severe concussion, like different things that they were looking for additional. Form of therapy. So that was my early, you know, career.
I was there [00:07:00] working alongside physical therapists. It was like within the physical therapy department. They had chiropractic and physical therapy, uh, and working closely with medical doctors and orthopedists that were coming in. So this was kind of like where my career started and I, you know, was drawn to this.
I always liked it. My mother was a physician. Um, and so. Medicine was always in my life, but when I chose to become a chiropractor, I, I just really liked this whole interaction with a patient. I, myself was treated by a chiropractor and I really liked that work, but I always, you know, what can I do within that profession?
That was a little bit more than just adjusting patients and working in the medical. You know, and, and a medical group working alongside the physical therapist, working closely with orthopedic surgeon. It's kind of like led me to that line of work I always done. I've always done that. Uh, and then six years
ago, or seven years ago, it was before COVID, I was, um, introduced to this, um, concept, which I knew.[00:08:00]
I just did not have the latest technology called a non-surgical spinal decompression. And what really attracted me to that was non-surgical spinal decompression is a great treatment for patients with herniated disc. Or, I was thinking, well, I see so many patients with herniated disc. You know, I can help them, but I always, I get stuck.
Like I, there's a certain, well, I'll
Dr. Grant Garcia: pop that slide.
Dr. Brigitte Rozenberg: Yeah, exactly. So, you know, you help them, but then like you can't achieve a full result of, of the treatment. Like you can't adjust them with when it's too hard of a disc, you can manipulate on that. Um, when, when the patient is in severe pain and they have sciatica, you can't put 'em through any rehab because they can barely do anything.
Like there is so much pain. So I constantly felt like, well, you know, there's not much that we can do. And when I was. When I, uh, not was introduced, but when I realized the new technology that's in the realm of non-surgical spinal decompression, and I took many classes and got certified, I was like, wow, this is, this is amazing.
This is almost like the missing [00:09:00] link of what I needed to have in my practice. But I didn't have, because, you know, over the years, 30 years, I have machine, I have ultrasounds and I have low level light therapies and different tables and different flexion distraction. You know, things are evolving. I always say the cell phone you have today is not the one we had 10 years ago.
So I was exposed and introduced to the new technology, which I thought was amazing and that's why I decided to bring it to my practice. And you know, I have three locations, so everything you do, you have to kind of do for three offices. It's a little bit complicated. But you know, the more I did and the more I treated the patients with this, the, these technologies, the more results I saw and the results were incredible because.
You know, I have, LA is very diverse. We have patients from, you know, many different diverse cultures and there are some people that for religious reason, will not want to have surgery. There are some people that, for cultural reasons,
don't [00:10:00] believe that the hospital is gonna help them or the doctors are gonna help them.
So, you know, I see all those different patients from all those different walks of life. And then I see patients that, whatever the doctor will tell me to do, I'm never gonna change that. So you see it all and you. Basically treat them no matter where they are in their life. And then you start seeing those results and then you bring another equipment in and then you, you know, kind of see better results and then you, you develop a better technique, you know, just like in anything, it, it takes time and skill.
It, it takes time and repetition to sharpen the skill. And so. I've done it so many times and I've added so many different tools that are so beneficial that when I decided to put it together, because I'm like, okay, so when are we gonna use the laser versus when are we gonna use the software versus when are we gonna use the, the non-surgical spinal decompression table?
And, and then I really. You know, thought about it a lot and seen so many patients, I decided to formalize a [00:11:00] treatment plan, uh, and give it a name and a method so we can have a little bit better structure and, you know, not kind of do things just for the sake of doing things. And that, that was my story.
Dr. Grant Garcia: I like this.
Yeah. We had, um. Uh, we had a physical therapist on that kind of talked about a method. He used a similar thing just to, for, in order to make it more structured. Um, will you talk a little bit about the devices that you use? I think we might show one. Is this one of those that you wanna talk about? Yeah, we'd love to hear a little bit about this.
We've got a few. I think these are things that I've, I don't get to see as often 'cause we don't do a lot of the non-surgical things. So it's really cool to hear this and kind of hear your thoughts on this and the combination,
Dr. Brigitte Rozenberg: right. So, you know. I always say, because the way that I practice all my, all my careers, I always practice alongside surgeons and pain management and neurologists.
And I always say, you know, it's all about collaboration. It's not, instead off, it's in addition to, there's many things that I do that you guys don't, many things you do that there, there's nothing that, it's not even close to [00:12:00] what I do. So
I think the collaboration always works. And I worked with a neurosurgeon once who told me, you know, 80% of my cases don't end up in a surgical table because if I can avoid.
Spine surgery. I will try to do that, but it's just, the problem is sometimes conservative care fails and so they need something a little bit more, you know? Um. Better inter, I mean, different intervention and, and that's where the surgery comes in. But those, those devices that I am gonna show you and I'll talk about, they're used by some, you know, this particular device is used by a neurosurgeon and I've met and I work very closely with, so this is called the Sculp Neo.
This is a very interesting device and it's just the latest addition to my. You know, mix here. It used to be used for many years for aesthetic purposes because this is the only device in the market that builds muscle, burns fat, and tighten skin. So you would think, okay, well what does it have anything to do with you treating patients with pain?
[00:13:00] But as you know, a lot of people with back injuries and, and disc injuries, which what, what I see a lot, you know, they develop muscle weakness and fatigue and atrophy and so weak muscle. You know, weak muscles cannot support weak joints. Like in order to support a joint, you need to have strong muscles, whether you have surgery or you don't have surgery, like you have to strengthen the muscles.
Some of these people are having a very hard time rehabilitate. Themselves back to normal just with pt, they're just too weak all around. So this device causes in 30 minutes of treatment, it causes 20,000 muscle contractions. So when you apply it on the abdomen, yes, of course. Initially it was introduced as a sculpting device, more aesthetic, but patients with weak core muscles.
I mean, they'll always have back pain patients with weak glutes, they can, they can, you know, recover either with surgery or without. They need to strengthen those muscles. So the MCO [00:14:00] Neo is a brand new device that was recently FDA cleared to strengthen muscle and to reverse sarcoidosis, which is basically, you know, muscle, no atrophy.
And it is a great add-on to patients, whether they had surgery or they, um. They didn't have surgery or they're in between, they had epidurals. It didn't work.
They, you know, they didn't have it. Any and all in between can benefit from, this is one of those modalities. So I recently added that to my advanced spinal restoration as the rehab component because once you strengthen their.
Abdominal muscles, the, you know, they call it like the protocol is core to floor. Like you need to strengthen the pelvic floor muscles, the abdominal muscles, the glue, the hamstring. Then you can go and rehabilitate back and do whatever you need to do. 'cause you can't just live on using these devices. So.
You know, when you, when you incorporate something so powerful, the results are unbelievable. And, you know, they submitted a study and FDA cleared it for functional wellness and [00:15:00] this is now the, the greatest thing in the market almost.
Will Sanchez: Is this something that you can only get at your office or is this something that someone a patient can take home and use?
What, what? Uh, you know, we. We started the show talking about the recovery shop, um, and how to get equipment to help with your recovery. So I just want to know if someone's interested in, in a device like this, what's the process? Do they need to see you first or do they have, do they have the option to do something else to get their hands on this?
Dr. Brigitte Rozenberg: So this device is not something you can buy. I. Clearly you can buy anything if you have the money for it. It's very expensive. But this is not a home use device. This is a device that's used that's primarily used in a clinical setting, so it has to be an office that carries it. A lot of doctors now carry it.
Um, like I said, one of my close friends who was a neurosurgeon, he carries this device in his office. I have it in my clinic here in LA and there are other doctors that carry it, but you normally cannot. Buy it and use it at home.
Will Sanchez: What, what's the [00:16:00] treatment like? Is that once a week or, it depends on the severity of the injury or twice a week.
I, I'm just curious for anyone that's interested and want to come in and say, Hey, this is, this is kind of what, what's recommended or is it all dependent on the patient?
Dr. Brigitte Rozenberg: So we have a treatment protocol for this device. Each treatment is about 30 minutes only, and we can, we can basically use two areas per treatment or per day.
So let's say you come in for just using this device, right? So let's say you come in and we do 30 minutes in the AB and 30 minutes on the glute, that would be one treatment. So 30 and 30, it's one hour. So minimum 30 minutes, maximum one hour. And it can be used in each area. For rehabilitative purposes, you need to do minimum four times.
So if you wanna strengthen the abdomen, the core, you need to do minimum four visits on the stomach. So, or the abdominal muscles. So at least once a week, it's the minimum twice a week. You know, we don't do that more than once a twice a week. So that's the [00:17:00] frequency.
Dr. Grant Garcia: Well, and it's, it's good to have this.
It's really interesting you kept saying that. 'cause you know, even today I had patients in the office postoperatively or preoperatively in there. You know, you're not bad. They're not, they're upset about whether they're, you know, they're, some of them are happy or some are saying, Hey, I'm not where I want to be.
But a lot of it is the recovery. Right. And as a surgeon. My PTs that I send people to, they don't have some of these options. You know, they have e-stim, they have blood flow restriction. Those are kinda what we do. But again, it's an extremity scenario. But having something like this is really cool. From the post- surgical recovery side, obviously I'm thinking like a surgeon, but I'm also thinking about the patient I saw today that didn't need surgery and I don't have the solution for it 'cause I don't have all these tools.
You know, it's nice to have that, especially as a spine surgeon, if you see patients like you said. If a good spine surgeon only does surgery on 20 or less percentage of patients that they see, but we know that's not always accurate and that's because we run out of things to do and we don't have the right people to contact.
And so it's really interesting that that, you know, something like this, the ability to, with around surrounding the joint [00:18:00] and getting the strength up there is really important. So I really like the idea of that. Um, and
Dr. Brigitte Rozenberg: this is one of many, we use many modalities, but this is a really strong one that is really, I think it's, it's a lot more, it's starting to be more common, but, you know, I would consider our office being more on the cutting edge.
So we, we buy those machines and offer it to patients, but you know, clearly you need to have an office that would, that would buy those equipment to apply to the patient when they come in for rehab. And there
Dr. Grant Garcia: Well, and you need the right patients, right? You're in la I'm in Seattle. Right. If you're in the middle of the country and there's different focus on different things or it's different injuries or different aesthetics or things like that, right?
You have a, you're in an aesthetic city within a machine that's works on focusing on abs and lower back, you can see that it'd be easier to get than it would be in a less aesthetic place too, as well. I
Will Sanchez: wanted to use, ready for South Beach
Dr. Grant Garcia: i's gonna
Will Sanchez: order. I was like, I could get ready for the summer.
Right now we're ready for the beach, but no, I, you know, it's, it's for physical therapy. It's for healing. Okay.
Dr. Brigitte Rozenberg: You can use it. We can, we can, we can [00:19:00] sculpt you.
Dr. Grant Garcia: Yeah. He doesn't need any sculpting. Look at him. So anyhow, the, uh, let's show, let's show another modality. This is a really interesting one. We'll put the laser.
Yeah. This is something that some point we'll have another episode on, but this laser therapy is a humongous topic in orthopedics right now.
Dr. Brigitte Rozenberg: Right.
Dr. Grant Garcia: Um, and there's been some a OS and orthopedic things, but I, I don't wanna take away from your thunder. So why don't you talk a little bit about this edition and what does this do?
Dr. Brigitte Rozenberg: Well, this is, this is a laser device. It's a class four robotic laser. The reason why I added that machine into that specific laser into my practice and add a different laser, because, you know, class four laser can
be, if it's used inappropriately, it can hurt someone. 'cause it, it can be hot and it can, it can, it can, it can injure someone.
This particular device has a robotic head and it's a cold class for laser, so it's not gonna hurt anyone, meaning it's not gonna burn you. Hmm. Now the Class four laser, normally the way it works is that, you know, it's called photo biomodulation and it stimulates, it reduces inflammation, it accelerates cellular, [00:20:00] uh, repair and cellular healing, and it will increase blood flow.
So when you use this now in conjunction, and you'll show some other slides with other machines, so I see patients. You know, with disc injuries, big disc, smaller disc, whatever. And so they have a lot of pain and a lot of inflammation. There's always inflammation has to go with along. Inflammation always goes along with all these injuries.
So you need to reduce the inflammation, the internal inflammation, and you need to increase the cellular healing. And there are thousands of. Peer-reviewed study showing how laser therapy is so effective, just like you said in orthopedics. So when you use that in conjunction with other modalities, you are able to reduce inflammation one way, increase cellular healing another way, strengthen muscle a third way.
So you, you, you know, you work. How should I say? It's like a very comprehensive approach to the, to the injury. And when you comprehensively attack the problem, you fix it much faster. It's a, it's a really great pain management device. It's not dangerous. It's not painful. They feel nothing. [00:21:00] It's very limited, like not a lot of time.
It's 10 minutes max. It, it works well.
Dr. Grant Garcia: Do you, was it something you'd mix in in the same day with that other machine or is this something different? Modality.
Dr. Brigitte Rozenberg: Yes, I mix. I have a formula that I mix in the laser therapy, software therapy, electrical specific electrical stimulation outta tens unit. And then the last piece of the, you know, the, the three faceted approach is the rehab that I incorporate, the sculp neo that you saw.
Dr. Grant Garcia: And do you think, again, I know this is multifaceted, but do you think the idea of what you're doing by calming the disc. Not only are you working to comet, but you're working to strengthen everything around it. Right?
And that becomes really difficult. If you've ever had a disc herniation, which I've had, it's terrible.
And the pain is unbearable. And even if you feel like you can push through it, it's very difficult. And I didn't even have the hottest disc of any of my friends that I know. So, you know, you get a really hot disc, it's very hard to do anything. Um, so you can imagine finding a way to [00:22:00] drop that, the heat of the disc, but also to strengthen around is really important, especially when you can't move.
Dr. Brigitte Rozenberg: Absolutely. That's what we do all day, every day. A lot of our patients, they have, you know, we see patients that either. We're told, well try everything you can and if it doesn't work, come back and we'll do surgery. We saw, we see those patients. Mm-hmm. We see patients that had discectomies minor, you know, minor, minimally invasive surgeries, and they have a recurrence and they're like, I don't wanna have another surgery.
I wanna try to avoid it. We see those people and we see those that say, I don't wanna have any surgery because I'm too scared and my, my neighbor had it. My cousin had it. The results were whatever. So I was, I'm trying to avoid and try to do whatever I can. So our approach is, well first of all, when we, we use the
non-surgical spinal decompression, so we decompress the disc.
And I'm thinking now that I'm thinking, I'm looking at all the slides, you don't have the picture of the main component, which is the acus. That's a different machine, you know, but I, I was, I'm gonna show
Dr. Grant Garcia: this. Is this, is [00:23:00] this the table you're doing or we take away your thunder?
Dr. Brigitte Rozenberg: Okay. Yes, this is it. So this, this is a decompression table, so if you can see closely, there is a computer next to the table.
So this is a computer generated axial decompression, meaning we input the data into the computer that's based on your MRI results. So if you have a, if a patient has a herniated disc of L four L five, which is the most common, we will then input the data into the computer of that. System. It's called the acute spina System.
It's made in the United States, and then what happens is we adjust the decompression. So we adjust an angle, we pull the spine, right targeting the L four and L five disc, which is about. 15, 20 degrees of pool. And so if you see on the table, it has a big tower in front of it, and the way the patient lays down, we harness them.
And then we will adjust the angle of the pool targeting that particular disc. And the way that this system works, it's kind of like in a progression, regression kind of a manner. Think about it [00:24:00] like a pumping mechanism. It pumps it and it, it, it. Decompresses the spine, and by doing that you create a negative pressure in the disc.
So I always give an example, it's like a plunger, and you basically allow the body to suck the disc material back in place. So when you do that treatment. Very gently and a very like, you know, 'cause we adjust the, the weight based on the patient weight. We adjust the pool, we adjust the time. And when you do that very gently, and then after that treatment you apply other modalities to reduce the inflammation and the pain, then you apply the laser therapy, then you apply, then patients feel better slowly and slowly and slowly and you baby step it into the, into the full recovery.
But that's how they feel better. Uh, they need some medication. You know, and they go to their doctor, or maybe they had an epidural and they feel a little better, but not a hundred percent. Then we add that in. But if you use it in such a formulated manner, the right cadence and frequency, you really are able to [00:25:00] get the result.
And that's, that's how we get the results with these DISC patients.
Will Sanchez: Dr. Roseberg, this is
Dr. Grant Garcia: really interesting.
Will Sanchez: Uh, just real quick here, um, you're pretty much in a, in a field of pain and relief, right? Uh, I mean, for everyone that's had back pain and Dr.
Garcia referenced it, whether it's arthritis or perforance or like you said, a a slip disc, a herniated disc.
You, you're having patients coming in at all ages with different, uh, pain thresholds. How do you, how do you manage that and, and what are some of the, the key, um. The communications that you have with your team, when you're dealing with patients that are in constant pain and you're trying to find relief, what, what is that thought process that goes into it?
Dr. Brigitte Rozenberg: So, you know, first of all, you have to be very compassionate with these people because they're coming in, they're in a lot of pain. So these are people that tried everything. Most of the time they've been everywhere. Like we have patients that go to the emergency room and they're being sent back home with some kind of pain pill or whatever.
'cause, you know, and they're, they're [00:26:00] upset. And I'm like, well, the emergency room has to deal with emergency. You know, they have to deal with a stroke and a heart attack. I mean, you have back pain, which is bad for you, but back pain is not an emergency. It's a disability. So of course it, it's really understanding the patient that's in front of you, having a lot of compassion and training the team.
Everybody on my team, whether it's the doctor or the clinical staff, they all go through rigorous certification program and training. Like we don't just bring people. And just jump them onto the like, okay, here's a patient. Go treat them. Like they need to be properly onboarded. They need to understand the technology that we use.
They need to know how it's being used, what it's used for, and they need to follow the protocol. So. Communication and relationship that we build with a patient is a very important piece. You know, people that come in in pain, pain affects your mind. It doesn't matter if you are, you know how long you've been in pain.
It doesn't matter who you are, whether you're an athlete that affects your like livelihood and your career. And if you're just [00:27:00] a, a patient that's. You know, cannot function, cannot lift your kids, cannot play golf. Whatever it is, it starts affecting your mind. So having that understanding with a patient is very important.
Giving them that comfort that we are here and we are gonna walk with you through this every step of the way. That's almost half of the recovery. Because if they feel comfortable where they're going and they feel com, they feel, they feel heard. They feel like we pay attention to them. They feel like we're gonna, you know, be there for them every step of the way.
They can come see us. Sometimes, I tell you can come every day if you need to for the first few weeks so we can control the pain. But the ideal situation is three days a week. We're not gonna do the same treatment every single day. But just the thought that I'm telling a PA when I'm telling a patient, you can come here.
Come here every day, four days a week, just, just, if you're in pain, just come here. We'll try to do something. That comfort level is really easing the patient. It's like, okay, I feel at least I feel like you'll take care of me, whether it's gonna work a hundred [00:28:00] percent or not, we'll see, but at least I know that you'll take care of me.
And so I think that is the differentiating factor between us and just, just doing things to do things. That's just not how we do it here at Spin Anatomy. Does that make sense?
Dr. Grant Garcia: That's great. I, I want to go one back to this table one more time because I think it's really cool. So I think for the, for the, the viewers, if you show the picture, and we can just do this really quickly here, which is kind of cool.
So you can see how the way the, the lumbar spine is curved, so she's talking about the angle that they're gonna pull it at. So if you just pull straight up, that's great, but that's axial tr that's a straight traction and that doesn't always work for everybody. Do you have, um, does this table go, uh, canter this way or that way based off of what side the disc is on?
Dr. Brigitte Rozenberg: No
Dr. Grant Garcia: as well, or is it most up and down?
Dr. Brigitte Rozenberg: So the way it works is the table will stand up in this position where the patient is actually going to lean against the, the table. It's gonna stand up because patients cannot just jump on a table and sometimes they have a hard [00:29:00] time laying down. So we're they're standing, and then the table kind of goes down into that horizontal position.
And then we harness them before they even get on the table. And so we kind of do all of it. And the table just pulls in, in just this direction. However, the way that it pulls in a, in a horizontal direction, the angle, if you see that big tower in front of it, the angle of the pool, that will be determined of us.
The doctor kind of programming the pool. So if I work on L one L two, that pool will be about 30, 35 degrees. But if I work on L five S one or L four L five, which is lower part of the lumbar, and that pool will be about 10 to 15 degrees. So the pool will determine, you know, where. You know what we target, but the patient does not move.
The table does not move. They're very comfortable. 99.9% of the patients fall asleep on the table and they, this is the position that they have the least amount of pain when they have a [00:30:00] hot disc. Because they're very comfortable. They have a booster under their knees. They have something underneath their arms, like everything is very ergonomically made for them to be comfortable.
So just a table and the system creates that pool, that event to decompress the spine that really leaves the pressure from from that disc.
Dr. Grant Garcia: Yeah. And well, and also it's the decompression of the muscles around it, right? They're really hot as well. So the whole thing just relaxes. And you can, ima I can imagine those patients coming in, I mean, we, I don't, I deal with patients in pain, but they're in chronic pain and they're in a different, it's not the same as, as nerve pain like you deal with.
Um, but it's, you know, all that stuff you mentioned about compassion, it's really important, right? Because the, and you probably see this too, but when you make the patient better, they are a different person. Correct.
Will Sanchez: It's
Dr. Grant Garcia: very frequent, the personality of the person that coming in. They could be abrupt, they could be angry, they could be upset, they could be disruptive almost.
Yeah. Um, and then you fix them and they are like a different person. So it's, that's the, that's kind of a rewarding part, but it's, you have to [00:31:00] work to get to that. Right? Because you don't know that at the beginning.
Dr. Brigitte Rozenberg: True. I wanna mention one more thing about this particular system, the acusa. The reason why I chose this system than others is because this has ave, this system has a very gentle motor, so it's very gentle on the spine and it has a patent.
Within the me, uh, mechanics, it's called oscillation. So in the process of decompression, it oscillates the tissue. Micro oscillation, you don't really feel it, but it prevents the muscles from going into spasms. So when you use it, it's very, when the patient is on it, it's very comfortable and it's very, you know, soothing.
And so when they get off, if they have pain, we ice it, and then we kind of go through other forms of therapy to reduce the inflammation. And it's very comfortable. It's just a matter of repetition.
Will Sanchez: What's the biggest myth that you're dealing with when you know people hear about spinal decompression? You know, is there something that, you know, people walk in and they say, when I hear spinal decompression, I think you're cracking my back, or something like that.
What, what, what do you tend to hear that you're [00:32:00] like, no, that's not true. This is what's happening. What's your biggest myth?
Dr. Brigitte Rozenberg: So, uh, interesting few. So one thing, few. Okay. I, you know, they say, I don't believe. I don't believe in this. I'm like, well, you know, okay, I respect that, but this is not. Religion you don't believe.
It's not about believing. This is, this is scientifically proven to work. Uh, it's a mechanical fix. You know, it fixes the spine mechanically. And a herniated bulging disc is a mechanical issue. So it either works or it doesn't, doesn't hurt you. So I hear that and I kind of, you know, that's my. Explanation.
Um, and second thing that they say, well, I don't believe this can really, how can this really fix the disc? And so then we go and we say, well, the disc is a, um, dynamic structure, you know, kind of like, it's like a sponge. I, I always have those little models and it's like a sponge full of water, or I say it's like a donut with jelly.
And so when you press on it too hard, the water leaks out or the jelly comes out [00:33:00] and this treatment with this me mechanics can actually suck this.
Disc material back in the jelly, back into the donut. So the myth is like, well, well, is it gonna work for me or, or it only works on some people, I'm too heavy or I'm too old, or I'm too this.
And the reality it, it's, it works on anybody and everybody, of course, you have to have certain parameters and we go through the examination and evaluation to see if you are a candidate, but. Doesn't matter if you're young or old. If you are heavy or skinny, it doesn't really matter if you're athletic or you're not athletic.
It can work on anyone. So it's either works or it doesn't, but 90% of our patients feel 90% better. So these are kind of like the the, the things that I hear when I talk to patients.
Dr. Grant Garcia: Great. Let's go over this. Uh, neuro me. Can you talk about this device?
Dr. Brigitte Rozenberg: Yeah. This is a great stimulator. It's called en Neuro, so it's electro analgesia.
Basically this is a pain management device using electrical current, [00:34:00] um, and it, the way that it works it, so it feels like an electrical stimulation. But just to give you a little bit of understanding, you know what a TENS unit, TENS unit works up to 250 pulses per second, and you can buy it on Amazon and use it all the time.
Then a regular electrical stimulation in a rehab facility works up to 800 pulses. Per second, this device works up to 10,000 pulses per second. It doesn't, it doesn't mean it electrocutes you, but it means that the Nutanix is so deep and it's so strong. I always tell this like, is it gonna electrocute me?
I'm like, no, it's not. But
Will Sanchez: take a cup of water at the same time. But
Dr. Brigitte Rozenberg: yeah, exactly. No, for sure. But it, what it does, it basically interrupts the pain signals and it reduces the nerve irritation by the mechanics and how it works. So it reduces muscle spasm and it kind of stimulates the nerve. And the way we use it is, for example, we put a patient on the decompression system, we get 'em off the system, we use a [00:35:00] lot of ice, and then we use this device to reduce inflammation.
And after we're done with this device, and it works about. You know, 25 minutes different, you know, reduces the pain. Then we'll use laser therapy to stimulate the healing. So when you follow those patterns, then you really see the result in patient leaves like, wow, I feel so much better. I couldn't, I can't even believe that.
Basically numbs the pain without lidocaine. It's really cool. And
Dr. Grant Garcia: then this, I mean this is sort of, you time talked about the ultrasound. Is this ultrasound or soft wave? You mentioned this I think.
Dr. Brigitte Rozenberg: Yeah. Soft wave is not, yeah. Soft wave is not an ultrasound. It's a form of a, it's not really like a shockwave therapy.
'cause shockwave is very like radial. It's very direct and it's very painful. This has a much bigger circumference, so it's an acoustic sound waves. They actually use it on many different sports team. Uh, that, uh, stimulates more cellular healing. So. Well, we, we call it like a stem cell stimulation device because it stimulates your own basically tissue [00:36:00] regeneration.
So again, all of them almost do similar things in different ways, but if you use them together, not at the same time, then you achieve a much better outcome. So I have many patients that come in and their pain level, for example, is like nine out of 10, and we would use one visit of soft wave and the pain level can drop to.
Sometimes five out of 10, sometimes six out of 10, sometimes four out of 10, but it always drops, so they're like, wow. I feel like the intensity reduced significantly. So that's another.
Dr. Grant Garcia: And then, and then the I, the idea is by you, you don't wanna hit 'em with one modality, right? Then you switch it up, so therefore you're not doing the same.
They each work with dif different mechanisms. Correct. So therefore, you're not overdoing one thing. You know, you can't do so much traction. You can't do so much of the neuroma, or you can't do so much of the muscle stem, or it could damage something. So you kind of mix it up. You keep the body guess.
Dr. Brigitte Rozenberg: Correct. We mix it up. We can mix two of them sometimes [00:37:00] together, but we don't mix all of them at the same time. They may get, so for example, if they come in 24 times or 30 times, they may be on the decompression table, all of those 24 or 30 times, but they will not get the same modalities in addition to the decompression.
So sometimes they'll, they'll, we'll use the soft wave and sometimes we'll use the laser and the neuro me and you know, we kind of, and then at the end, the last phase of our. To rehab because my advanced spinal restoration treatment has like three different phases. Then the last phase, which is, uh, basically rebuild and rehab.
Then we'll use the M scope. So I'm not, we're not gonna use the M scope when the patient comes in in severe pain. We always gonna use it at the end.
Dr. Grant Garcia: Got it.
Will Sanchez: I wanted to get talk about, uh, because we do like to talk about sports on this show as well, and we wanted to bring up the 70-year-old gymnast that, you know, the, the buzz that people were talking about and, and what she was dealing with when she first walked into your clinic.
So, can you tell her story a little bit and, and what that process was to, you know, helping her and to getting her back [00:38:00] to, uh, where she needed to be as an athlete?
Dr. Brigitte Rozenberg: Yeah, so interesting that she was my last case. That's why I, I wanted to talk about her because she's, wow. She's training, um, hopefully for the Olympics.
We'll see how that works. But she's very young and her parents, um, brought her because she developed low back pain that really. Prevented her from doing all her routines. And so of course they sent her for an MRI and she did not have a full herniated disc. But what she did have is that she had disc degenerate.
She had like disc desiccation, which is like the disc is starting to dehydrate and then the facet. Became a little bit too jammed. So it, it sounded like, you know, that when she was doing her routines, either they didn't work on some muscle groups, but the pounding and the axial pressure was so strong that it kind of jammed the facets and it was almost the MRI showed that she was, it was almost will develop the spondylolysis and they, you know.
At that time, you know, they were afraid for this to happen. So when they brought her
Dr. Grant Garcia: and will, that's a common thing in gymnast, what she's [00:39:00] trying to bring up. That's common. They can break the actual area where the facet is. So, but she, that's what she's trying to talk about. Sorry. Keep going.
Dr. Brigitte Rozenberg: Yeah, no, that's good.
So, you know, with her, because she didn't have a full disc, but you know, we wanted to kind of rehydrate the disc back and decompression, uh, therapy can rehydrate the disc back. That's part of the, uh, physiological effects and responses of the decompression therapy. So, you know, I put her on a 16 session, right?
I'm like, okay, she doesn't need 30. 'cause we have.
Will Sanchez: How does she walk into your office? Just so, so the listeners or viewers can understand the severity of her walking into your office and, and what you were dealing with. It just, I'm just backtracking you up a little bit.
Dr. Brigitte Rozenberg: Yeah. So. I mean, I, her parents, uh, researched and they found, they found our office.
Uh, she walked in. She, she was in pain and she was off training. Okay. I think she was two months of off training. Uh, so she walked in the office. She. [00:40:00] Normal, but she was just in a lot of pain and she could not work out. She couldn't train, she couldn't work out, she couldn't do anything. Uh, and this is a, this is a person, this is a, a, a gymnast that started training when she was, or like doing gymnastics when she was three years old.
So that, that's her life. Uh, and of course. Um, she was doing national competitions and she's training for the Olympics. So they were extremely concerned because she just couldn't do any of the routines. Uh, so that was, that was how she walked in, like in terms of limitation. And then when I did the m, when we did the MRI, and then I did an exam, then we saw exactly where the problem was and I'm, okay, well, she doesn't have.
A herniated or bulging disc, but she has the disc desiccation, so, and she's 16, so the reason or 17 there, and she was almost 17. So the reason why I'm bringing up the age is because, you know, young adults, when their growth plates are not completely formed, we, there are certain modalities, there are contraindicated.
We don't wanna do that. But you know, again, you have to kind of evaluate the [00:41:00] case, the case that's in front of you. And she's an athlete. And you know, I think. If I'm not mistaken, someone wanted to put her on steroids 'cause she was in pain and I think that the parents were like, I, I think it's a little too much to put her on steroids.
Uh, so they were trying to find something else. So I, I can't remember if that was the case, but I said, okay, so we're gonna do, instead of doing 30 visits because she does have a herniated disc, we're gonna do 16. The reason why I'm giving you a number, because there was some research that was done on decompression and it shows that you need at least 20 visits for discs to kind of regenerate.
Given the fact that she's so young and it wasn't really bulging. I'm like, let's do 16 sessions of that and let's really monitor. We'll do the soft wave. I'm not
gonna do it directly on the spine, but I'll do it on the paraspinal muscles and then we'll do a little laser, but I'm not gonna do it directly on the bone.
We'll do on the muscles. So we did that. And the interesting thing, I then put her on the M scope only on the abs, to strengthen the core, even though she's a strong. You know, [00:42:00] athlete, but that combination really allowed her disc to kind of rehydrate a bit and regenerate. And then I referred her to a, um, you know, like an athletic, like Olympic athlete trainer, because I, I asked her, I said, who is training you?
And, and the parents said nobody. I mean, she kind of trains in the, in the whatever national gymnastic. Whatever that gym is, but nobody specifically. And I said, well, you know, that level of, um, of exercise and training really requires a little bit more of a one-on-one attention because one wrong move. I mean, if someone is not gonna watch what she's doing or not gonna really work on maybe her form or correctly on the muscles that, that she needs to work on, then she can really injure herself and that can be very detrimental for her career.
So. We really followed the protocol, but with her specifically, like I didn't use, like, I didn't use the nommed [00:43:00] because it's electrical stimulation. We don't wanna use it on the growth plate, but I used the decompression very gently. Um, and then I used the, you know, the soft wave and we used the laser and.
She rehabilitate back to normal and the, the, the actual exercise that she's, the routines that she's able to do right now are just amazing because she's very strong and very capable. But that, that little injury really put her out.
Will Sanchez: Well,
Dr. Grant Garcia: I think it's Will, if I talk to the viewers listening this, the, the problem you have with that MRI findings that she's talking about are.
For a surgeon, there's really nothing we can do, right? That's not a surgical situation. There's not a growth plate arrest, there's not a actual fracture of the facets. So this is like the perfect non-surgical treatment regimen because you don't wanna hurt her, you don't wanna damage your growth plates, uh, you don't want to damage your disc more.
And this situation, as you mentioned, as many of these modalities, while they're effective, they don't do harm. Uh, and so that's really the key [00:44:00] here is like, what can we do to make her better? And the fact that, you know, helping
rehydrate, that's a really weird concept that most people don't understand unless you've either had your own disc herniate or you do disc herniation work, but the idea that the disc will go back in is really true or it will disappear, but generally resorb.
Um, and so the idea behind this is you're, what you're basically trying to do is trying to suck it back in, right? Give it a good environment, have it come back in. Um, so that it can not have to be herniated anymore. The, the challenge, right, as you mentioned before, is how long can patients make it before they pull the trigger on surgery?
'cause it's absolutely miserable. So if you can find a way to get them more time, they've, they've done studies right that show the longer you can do a non- surgical treatment for a disc, the higher chances you don't need surgery. But most people can't make it that long. Right. It's just, they just too, unless they go to someone like you, right?
They have all the modalities. But it's an interesting concept that, you know, you gotta get the disc calm down as soon as possible to try to buy someone more time to see if that'll get better. [00:45:00]
Dr. Brigitte Rozenberg: And you know, that takes me now to the whole concept of spin anatomy. We have three location. We, we, we really would like to, you know, working on being in more locations because, you know, we feel, I feel, and I'm sure you feel the same way, that the, the general public is more educated and more open-minded to all the alternatives that are out there and would.
I refer them for surgery all the time. There's certain things that there's, I'm not gonna touch because it's too much. There's other thing going on in the spine that they need surgeries. There's cer certain things that I cannot, that we cannot fix, but the general public is a lot more educated and they're a lot more open- minded, and they're looking for different solutions because they don't want just to accept.
You know, the medication and, you know, the, the healthcare system, I think you can agree with me, is inundated with so much. Doctors are so busy, they're so, like, they're overloaded with patients and people are just looking for different solutions and different options that are available, available for them.
And, you know, they'll, they'll hopefully they can find them
Dr. Grant Garcia: [00:46:00] well and lower back pain is one of the most common diagnosis we have. And if I think it's, of all the things we have, it's the most likely diagnosis that any of us will get. Um, is lower back pain with disc issues. So it's really cool. Well, I, again, in the, in the sake of time, we don't wanna keep you on much longer, but we really appreciate you coming on.
I dunno if Will has any final questions.
Will Sanchez: Yeah,
Dr. Grant Garcia: but this has been great
Will Sanchez: so far. Like, we always do, we always wanna finish up and, and ask that question, what's next? Right? So what is next when it comes down to technology? Obviously you, your office is full of technology. But is there something out there that you're excited, whether it's coming out now or, or you could see it in horizon to advance medicine, to advance the relief of back pain that, uh, you can, uh, focus on.
Dr. Brigitte Rozenberg: I mean, I think that for right now we have pretty much everything. The mco neo, which is the most, um, advanced form of rehab and advanced form of modality. We just recently introduced it into our practice and, uh, we have an Sela, which is a. Basically works on the [00:47:00] pelvic floor. And I think that if we can rehabilitate the whole chain core to floor and you basically revive the disc or give it the right environment to heal itself and you reduce the inflammation and regenerate a tissue, the patient can recover and they can feel much better.
Um, whether they're just before surgery, sometimes even after the surgery. 'cause sometimes they had surgery and they still have some discomfort. So wherever you need to meet them where they're at and try to help them and the whole. Recovery process. And I mean, I think, I think the, the technology, you know, like look AI and look with everything that's going on, I mean, it just evolving so fast, who knows what's the next machine that's gonna come up to the market, um, and how it's gonna help.
But I feel, I feel like, I feel the, what's next is for me, my mission is educating people. Really to give them an option. You know, I always say, you are the patient, you'll make the final decision. I'm here just to give you another option, another perspective, and if you think this is for you, then you know we [00:48:00] can visit this.
And if you think something else is for you, then that's okay too. But I think that if I will educate you on what's available for you, then whenever you make a decision, it's an educated decision and not. 'cause someone just told you, um, to do certain things or not to do certain things. Um, so that, that is my mission, that's my next, and I think sending the message across to as many people as possible, um, of the advancements of technology and to have as many spinatus as possible to work alongside great surgeons like yourself.
'cause I think collaboration is the key
Dr. Grant Garcia: a hundred percent.
Will Sanchez: All right, Dr. Rosenberg, thank you so much for your time. Creator of Advanced Spinal Restoration Therapy. That's so much fun to say. Uh, non-surgical protocol that combines decompression, regenerative biologics and neuromuscular retraining to get athletes and.
People back healthy to feel. But, uh, Dr. Garcia, I don't know about you. My back's feeling a little stiff with all this conversation. I've been [00:49:00] stretching. I'm talking, I'm trying, Tom trying to
Dr. Grant Garcia: get good posture.
Will Sanchez: She put the on us. I'm like, I feel like I need to stretch
Dr. Brigitte Rozenberg: anatomy in Seattle.
Will Sanchez: Yeah,
Dr. Grant Garcia: we need to, I wanna, I wanna fall asleep in that unit. That looks amazing. So anyhow, I don't wanna digress.
Will Sanchez: Thank you
Dr. Brigitte Rozenberg: so much. If I open up an office in Seattle, I'll let you know.
Dr. Grant Garcia: Thank you. You perfect.
Will Sanchez: We're we're, we're coming. Thank you so much Dr. Rosenberg.
Dr. Brigitte Rozenberg: Thank you for having me. I appreciate the time.
Will Sanchez: Thank you.
Dr. Grant Garcia: Thank you,
Will Sanchez: Dr. Garcia. I mean, that was, uh, that's, that's phenomenal and no joke, man.
I, I was, I was feeling a certain way, man. But we wanna remind all our listeners and viewers check it out@sports.talk.com. With this show and so many others, we'll have transcripts, we'll have previous shows. We have recommendations.
The website's great. You can watch us on YouTube, listen to us on your favorite streaming platform, and as always, we appreciate you the viewer, you the listener, and our guests.
We [00:50:00] have phenomenal guests. We're always learning stuff. I'm telling you, I'm, I need a. I, I don't know. I, I need a, a Phoenix, uh, university of Phoenix, uh, doctorate at this point with everything that we, it was great. Well,
Dr. Grant Garcia: thank you.
Will Sanchez: Yeah. Um, Dr. Garcia, thank you for your time. We really appreciate you. We appreciate all our guests.
Any last words for you?
Dr. Grant Garcia: Thanks to the listeners. Keep checking us out. Request as you do guest requests, you know, we're not gonna be able to pick everybody, but. We wanna make sure we have a good plethora of people on here. So it's been great so far. And stay tuned.
Will Sanchez: We were robbed. We should have got best podcasts. That's all I'm saying.
Audio Transcript
What F1 Racing Taught Me About Saving Knees with Dr. Nicholas Colyvas

[00:00:00] I am Will Sanchez, along with our orthopedic surgeon in sports medicine specialist Dr. Grant Garcia. Uh, Dr. Garcia man, how you doing today? I'm good. I'm good. I'm excited. We had a really awesome topic and just in time for, we'll go from F1 over here. And then we got a little bit of surgery over here, so it's gonna be exciting to talk about.
I do not have this many mics in front of me. Somehow the AI decided to make all these mics plus of the mic on the green screen hidden, so who knows what's going on. Yeah, so, uh, obviously we don't know how to use technology, but we try our best. So this is great. I'll try not to get distracted. It'd be like the dot thing that's happening with the microphone, but you know who we make sure we never get distracted by.
It's the good folks over at the recovery [00:01:00] shop. We remind everybody. Visit them@shoprecovery.net. Dr. Garcia talk about our friends at the recovery shop there. Again, thanks to our sponsors, you've heard this ad nauseum, but these guys are awesome for especially those sort of like, what extra can I do after surgery?
These complex surgeries, we're gonna get into some complex knee surgeries, uh, with our guests as well, uh, but they allow people to have these sort of aftermarket options, which is great, uh, for the patients and, uh, it actually appeases them quite well, especially after surgery when they're looking for something a little different.
So, thanks guys. Yeah. All right. So without ado, let's bring in our guests, uh, Dr. Nick, uh, kavas. Thank you so much for taking some time and joining us this evening. We really appreciate it. Thanks, will. Thanks, grant. I really appreciate, uh, uh, getting the invitation to chat with you guys. Uh, Dr. Kavas, before we get into everything that, before you guys geek out on meniscus and shoulders and everything [00:02:00] else, you know, why don't you let our listeners or our viewers know a little about, about your childhood.
It's very interesting coming from a Greek family and South Africa. So just describe the childhood, how you got to the United States and, and fill in the blanks a little bit, leading you to the pathway of where you're at right now. Sure. It's a, it's a fairly long story, but to sort of, uh, summarize it to some degree, I'm gonna, uh, you know, start by saying I'm, I was, I'm a second generation African.
My parents were born in Africa, and their parents were born in Greece. Um, and they, so my grandparents essentially came from, uh, Greece to the United States, sorry, to Africa. And both the, um, both the, uh, the families grew up there. My parents met in Africa, and, and we grew up there. And then it was in my, after, right after high school that I basically came to the us.
Uh, [00:03:00] Bri Well, my parents came to the us uh, immigrated. I stayed behind in Africa and I went to medical school in South Africa. And there, uh, after I finished, uh, came to the us, joined my parents, that's when I did my residency at UCSF, um, following which I went into, uh, private practice for 20 years, which was great, but felt the need, uh, now, so seven to eight years ago.
Um, to change things around a little bit and just opportunities and timing and everything, um, opened up that I essentially returned back to my, uh, trading spot at UCSF. So that's sort of the, the broad summary. That's awesome. And we don't wanna, we're gonna, we're gonna save your fun after school activities, uh, for the more the end of the show.
'cause it's every, it's too exciting and we're gonna distract from the rest of it. Uh, everyone knows what we're getting in a minute, but, uh, can [00:04:00] you walk us through kind of orthopedic surgery? Why sports medicine? I mean UCS F's a great program. Uh, tell us a little bit more about your decision to go into sports.
Yeah, I had a bit of a tough time, uh, deciding that, to be honest. Um, it wasn't a slam dunk for me. Um, I really liked trauma. I, I liked, uh, I liked sports, um, and, uh, I had some really good, you know, this is, I think a fairly common story, right? You, you, if you have good mentors, you have mentors who teach you things that you really.
I mean, if you, I think you've, you admire them, uh, you kind of want to be like them to some degree. And I had some, you know, really great guys teaching me arthroscopy and I, I say this to the residents, you know, I was where you are fumbling around in the subacromial space trying to find your instruments.
Um, and I remember it very clearly and I was re just thinking, boy, that attending, you know, my attending that I had was [00:05:00] really patient because. I probably would've taken over by now if I had, uh, you know, if I, if I had to watch this guy fumbling for so long. But it's just part of the process. So I had, I had great mentors and I found arthroscopy challenging and something I wanted to really master.
Um, and you know, that sort of drove me to sports medicine to arthroscopy at least. Um. And that's sort of what I, uh, felt like, okay, if I'm gonna do something, uh, going forward, I want it, I want it, I want it to be in essentially the arthroscopy field. You guys are hysterical. You, you're the few breed that love to say, I love trauma.
Trauma is my friend. You, you have to be built a certain way. Um, who can you talk about your mentors and, and, and who, who these folks were that to, to help propel you to where you're at. Yeah, so, so Gene Wolf is a name. I think, uh, grant will recognize very well, you know, sort of a, a real giant in [00:06:00] shoulder surgery.
Um, invented the ROM massage, which is one of my favorite, uh, surgeries. It's the LET of the shoulder, as far as I'm concerned. Um, I love it just added to every, every, every shoulder, 'cause it's only gonna do good and not gonna do bad. Just the same, same with an LET in the knee. Um, and, you know, he was, um. He was patient with me and he really, you know, I, I obviously wanted to learn and he, you know, said, okay, look, you know, you come with me and we'll just do shoulder scopes.
And, and at that time I'm talking about, now this is in the nineties, right? Um. Uh, not that many people were doing shoulder scopes, you know, it was, it was pretty, pretty rare. In fact, when I graduated, I, I, I, I was one of the sort of few people in the community that did it now, that after that point it kind of exploded.
It was the next joint deaf knee. But, um, um, you know, he really, he really did that for me. Kevin Louis was another guy that taught me all about knee surgery. He was [00:07:00] a private practice doctor, just recently retired, actually, uh, outta San Francisco. He was the kind of person who really sort of spent the time with you and just showed you what to do and all of these guys, it wasn't just what they did in the or, it was also how they, how they sort of carried themselves, both with patients in clinic and in the OR and the kind of things that, you know, I try and do as well as I can at this point in time.
Uh, and I try and teach to the residents as well. Well. Great. Can you, um, go more into kind of talking about the residents and your work? I know you did the private practice stuff for a while, but now you're more on the, you know, UCSF doing, you know, you see tons of research, lots of other things we can go into as well.
We kind of talk about your clinical role right now. Like, what do you do? What's your, your day-to-day like? Absolutely. So when, when I was in private practice, you know, I found it and I was solo for a lot of that time, and then [00:08:00] joined, basically grew a gr, a big group out of it. But, um, um, I found it that, um, a sort of a little isolated, you know, private practice, you do your own thing, you discuss your case with your pa.
Um, there's not a lot of sort of. A collegiate discussion around surgery and what you're doing, et cetera. And so even while I was in private practice, I was actually taking time, um, and again, fortunate that I had the connection and, and um, uh, the ability to do this, but to go spend one day a week, uh, at UCSF teaching residents, um, and that was seeing patients and doing surgery.
So when, seven years ago I joined basically full time and I gave up the private practice. It wasn't a difficult transition, uh, it just meant that I, what I was doing on my Fridays now I did for the rest of my time. Um, and I'm generally sometimes with medical students, it's mostly residents and fellows and [00:09:00] most of that time it's either seeing patients in the in clinic, but um, the majority is really in the or and we're focusing on, you know, what we do surgical indications.
Different ways people approach it. You know, I'm always trying to make them think about, okay, this, you know, you, you've been shown this way. What about doing it this way? You know, why am I choosing this graft? Why do I add this to that, et cetera, et cetera. Um, and that I think is sort of the major part of the training I'm doing, um, as you know, as part of the academic surgeon, uh, position.
Uh, but there's also a bunch of didactic teaching as well, but. Yeah, by far the fun stuff is just in the or. I mean, you know, everybody, everybody likes that. We always, the fellows are always making excuses to not be in clinic and find us back in the or, you know, I think that's a doctor, it's a surgeon thing, just like we did.
Right. Um, will you, you, you do a ton of LinkedIn, uh, [00:10:00] social media stuff, talking about meniscus work. Obviously it's a big deal. I want to get into it. Why meniscus preservation. Obviously people, I keep pointing the wrong direction, so save the meniscus. We'll get into that in a minute, but talk to you about why, what's this meniscus preservation, what's your, like, how did you spur this?
What's the reasoning for this? Maybe describe it a bit more. Yeah, sure. You know, I mean, one of the things I. You know, going back to the resident, one thing I tell tell them a lot is, you know, so much of life is all about timing. It may not be, this was your original plan from the beginning, but I was always interested in innovation.
And around 2012, 2013, uh, the inventor of the CXX device, the Nova Stitch device, um, through one of my partners, uh, was actually looking for people to sort of help. Developed a prototype and tested in cadavers and stuff like that. And so I was like, yeah, this looks interesting. It's new. We don't have anything like this that, you know, we, [00:11:00] we, we, we have inside out and we have all inside.
And that's pretty much the only ways we repaired men. 'cause we never had circumferential suturing devices. Um, will, can you pull that slide up while he is talking? Yeah. And, and so that really sort of piqued my interest. Um. And when I started doing more of these, um, I started enjoying doing more of them.
And, you know, again, it was a challenge and it was, uh, interesting. And this is a picture of, you know, sort of, this is, this is one of the bigger ones, right? So this is a, this is a lateral meniscus tear that has, um, uh, essentially a horizontal cleavage component and with a circumferential suture. And this is actually this, this.
Slide's kind of interesting 'cause there's three different techniques here. You can't quite tell. But the posterior horn is all circumferential technique with, uh, with um, uh, a nova stitch type device. Then the mid body is actually all inside. And then when we come [00:12:00] to the anterior side, which is difficult to get the instruments.
Uh, to get either the circumferential or the all inside techniques, you do an inside out technique here to, to repair the anterior ho. And this was a, a full round the clock horizontal cleavage tear, which you know, is, is unusual.
Normally it's a section and you just put in maybe four or five, but I think we put in about 11 here.
Um, so this is one, this is one of the bigger ones I'm happy to say is patient's doing great and, uh, all is good. But this is sort of the thing that I think, um, you know, certainly when I started training, we would never do anything like this.
And I think over the course of the last 10 years. You see more and more of this, um, rather than just take out this lateral meniscus and, you know, partial menisectomy on the lateral side is, is really, really tough.
Yeah. It's not a great result. Um, so saving this meniscus, I think becomes quite [00:13:00] critical. And we have the tools to do it now, but you have to. Kind of commit to it, right? It's so much easier to do a menisectomy. I can, you know, I can save myself an hour in the OR by just chomping this thing away. Um, but I think that we are getting to the point where many people are looking at this and saying, no, it's repairable, and let's give it a try.
I think this is interesting topic. I mean, one, the thing that's interesting too here is this, we see this a lot in discoid meniscus. I think I and, and those are ones that are kind of nasty. They end up with transplants. They see them for the.
Transplant. I see them for the discoid initial conversation. Do you have any, I don't want to, we're not sidetracked the conversation, but do you have any specific thing you talk to discoid, like I, in my office, a disco comes in, I'm like, listen, and this is not just a, a normal meniscus, this is gonna be a different animal.
And these things you'd showed, maybe employed, how do you have that conversation with them initially and then kind of what's the, how do [00:14:00] you talk about the outcomes to them? Right. Because this is, so they sometimes these people have seen four docs and all of them said removal and you're the only person that said, we're gonna try to save it.
Yeah, look, I mean, I, I spend with any meniscus patient, but with Discords particularly, I spend a fair amount of time and I like to draw it out. I like to show them the C shape and the D shape of the meniscus. And I explain to them, you know, what it involves when we ize it, you know, and I give them the terms so they understand it.
Um. Then I tell them, you know, when you source right, it almost always you're gonna have a horizontal cleavage tear all the way around and that should be repaired. It shouldn't be, uh, removed. And I think the outcomes there obviously are gonna be better if you do, if you do a repair than if you do a resection.
But I do tell 'em, look, you know, your cartilage on that lateral side has never really seen normal forces. You know, and, and, okay, most of these patient patients are still sort of in the younger group, but I've even got older discos that come in, you know, and it's been [00:15:00] unrecognized for a while, and then your cartilage has never seen that, the, the normal forces that a normal cartilage would see.
So when we do all of this, or you know, as a result of the tear, it may not respond like normal and we may be talking about early arthritis, et cetera, et cetera. So I do, you know, I don't give them the, um. The, oh, we are gonna do surgery and everything's gonna be perfect. You know, that is, I think with Discord, it's all bets are off.
Um, many of them do. Many of them do great. I mean, I've, I, over the last 10 years, I've done quite a few now with repairs, and I've been very, very happy with it. I think it's 10 times better than, you know, try just taking it out. Hmm. I I have a question for you too. I've seen your LinkedIn posts, they're pretty awesome.
You do a, I do complicated mixes ones, but you've take on some things that even I think I look at and I'd say, I'm not even sure I could fix this. Um, which is really great. Uh, it's nice to see. It's refreshing that you show your stuff.
Thank you. I appreciate, I appreciate that com comment coming [00:16:00] from an expert surgeon like yourself.
Uh, but anyhow, so yeah, so I, I am, how do you, how does that go for you? I mean, obviously. Right. You're with the residents and the fellows, and they're seeing you fix a meniscus, and they're like, this is really cool. I'm excited to be here. Right? But you're posting that stuff online that's already a little out there, and you're showing pretty awesome results and pretty cool things.
You're really pushing the envelope on this. What encouraged you to get to this level? Right? Because it's, like I said before, you're, you're showing people that even the people that do a lot of these, that they're still not even enough. Um, I think that it's a, it is a evolutionary process. I think 10 years ago I wasn't pushing as hard as I do now, um, in terms of what I, what I'm going to, what I'm gonna repair versus resect.
I, I think, you know, obviously we show. The ones that are interesting and they tend to be the ones that look difficult and that we're still able to repair. I will [00:17:00] say behind the scenes, you know, there are some, when I just look at and I say, I just cannot do that one, or I can do it. I mean, you know what I tell patients oftentimes, look, most times.
I can technically repair your meniscus. I can, you know, put it back together if, if, you know, if it's just a technical exercise, but it's a decision between whether or not you can technically do it and whether or not there's a high likelihood of it healing, right? So some of those meniscus is a pretty beat up, but either there's, you know, the arthritis or the alignment's not right, or the patient's overweight or all the other factors.
It's not just the meniscus, it's everything around the meniscus. If those factors aren't. Correct. Or, you know, favorable. Um, I think you've just gotta, it's a judgment call, but what I found is that as I've done more and I've done things that, you know, I've said, nah, maybe this one's on the gray in the gray area and I fix it, and the patient does well, that encourages you to push forward more.[00:18:00]
It's a slow process. And how have, do you think these techniques improved over this, 'cause you mentioned this 10 year period, right? But what, what's different over the last 10 years? I mean, I know you've gotten more experience, right?
That's great. Yeah. But what's, what do you think's evolved? You mentioned something about, you know, one of the, the Nova such device, and that's just one part of it.
What do you think's gotten to this point where now you're like, okay, maybe I can fix these now. Maybe they're gonna do better, right? Just research and things like that, but there's more to it. Yeah, so I, I think the biggest advance we've made in the 10, in the last 10 years, and everyone. Everyone kinda laughs at this a little bit because it's not like some fancy new device.
It's, uh, MC Lpy, crusting. Um, I think that that has allowed us to take on. Um, repairs because we have access, because we have the ability to actually get to the tears and get to the posterior horn and really get, um, the sutures where they [00:19:00] need to go. Um, I think that's given us the ability to take the existing techniques inside out, outside in, um.
And, and really, you know, sort of leveraging, leveraging, leverage them to the maximum. I think the other thing is that we've, we we're better at, and there's still lots of, lots of room for improvement here, but we're better at using biologics. Whether that's marrow venting, whether that's, you know, fibrin clot, whether it's PRP.
Will, can you bring that fibrin clot thing while he is talking? Sorry. Keep going. All of those things that are the, um, you know, the sort of second. Part of this, which is. It's obviously when you're talking about repair. So when you're talking about preservation, it's okay, first of all, which ones do you repair?
Which ones don't you repair? If you're gonna repair, then you have to get the mechanically best repair you can possibly get. And then the last piece to it is definitely the biology. You're gonna maximize the biological environment, [00:20:00] um, to really sort of. Uh, improve your outcomes basically. And so this picture's a fibrin clot.
I like fibrin clot di canon taught me how to use it. 30 years ago. Will you describe it for the patients? 'cause I don't even know, you know, some of us don't even use it, some people use it more than others and it's a, there's a little trick to it. So maybe you could describe it a little bit better. Sure. So Fibroin clo, like I said, it's not a new technique.
When people started me repairing meniscus, uh, arthroscopically, I'm not sure. I think Henning is really the first person who did it. And essentially it's taking the patient's own blood. Um, and then using, um. Using the, that blood once it's clotted and you clotted on a glass rod, because that's how it clots better.
Um, it forms this fairly robust. I mean, people think of a, as a blood clot as as, as quite unstable and difficult to work with, but actually it's more robust than you think it is. You can tie sutures into it. [00:21:00] Um, and that allows you then to shuttle it into a position. So what I do, this is an horizontal cleavage.
Tear, for example, um, you pass a shuttle suture on one side through the middle of the horizontal cleavage tear, and then one on the other side. And you shuttle this clot in, you've, you've sewn it now with the, with the suture and you attach it to the shuttles and then you shuttle it into place there, and then you place your sutures on top and bottom and you kind of zipper it closed with that fibrin clot in there.
And I, I, the, the, there's a description out of some Australian surgeons as, as the, the, the jam sandwich. So basically it's, you know, your two leaves with some jam, with some strawberry jam in the middle there. And that jam sandwich, I think. Provides the mechanical strength that I'm talking about. And you know, there's, there, there's tricks about putting in as many sutures as you need, not just one or two.
You know, you've gotta put, for a tear like this, I think you'd put in four or five at least. Um, and then [00:22:00] maximizing your biological environment as much as possible to get that to heal. And how are you deciding, is that all your horizontal tears? Like who's getting the fibrin clot? What's your decision making process?
Yeah, that's a great question. It adds more time and more adds more complexity, right? So I, I think the horizontal cleavage tears is a good choice. And I, I do the fibrin clot now, I would say more and more, is it most of my horizontal phage tears? No. But it's, it's, it's more and more, and I'm doing it more, uh, actively.
I'll also do it for any radial tear. At this point, a radial tear I think is a really difficult clinical problem. You know, they, they're, they're. Born trying to die. Uh, they, uh, they're uh, they're constantly feeling the, the, uh, axial load on the hoop stress to pull them apart. You know, horizontal cleavage tear actually works the other way around.
And, you know, your axial load is actually pushing those leaves together. Uh, the radial tear is the [00:23:00] opposite, so I will use fibrin clot for that. Um. And um, you know, I think things that don't need it is like a root tear. I've done it just to show that it's clinic, you're clinically able to do it, but I think a root tear, you've got a tunnel, you've got enough blood in there.
I don't think you need a five o'clock for that. Is there a, a specific age group that you kind of focus on or a range for, for you to do this procedure or does it not matter? I, I don't think it matters. I don't think there's any specific, um, age, um, cutoffs except that there's, you know, certain types of tear.
Like the root tears are all older patients, right? The medial root tears are all older patients. Um, but any patient you, I have a concern about, maybe it's an older tear or the tissue quality doesn't look great. Um, once you get your anesthesiologist and your, your, your surgical staff to sort of know your.
That's, this could be a potential thing. It's not suddenly, oh gosh, now we have to draw blood. Now we have to [00:24:00] stir it for a 15 minute it, you know, it is, there is a process and it does add time to your surgery, but the more you do, the more everyone becomes familiar with it, the easier it is to just say, Hey, this is what I want to do it on.
I mean, there are many that I'll just decide beforehand and everyone knows, but sometimes I'll be in there and I'll say, ah, I just want to add a fibrin clot. So the, so the age might come into play if it's, you know, depending on time, under anesthesia or some other factors, right? That's where you, you made a decision, whether it's yourself or you and the team, if you're gonna do a procedure like that.
Yeah, I think all of those, all of those factors come into it. You know, I, time under anesthesia is probably not one that I would, I would focus on heavily. Uh,
but really it's the, it's the nature of the tear. I mean, you could see like this tear, the cartilage surface is excellent here, but that meniscus is, is awful.
And I would wanna do everything I can. To try and preserve that meniscus. 'cause that's the whole goal here. The [00:25:00] meniscus is there simply to serve the cartilage. You know? It is, it is the cartilage protector. We're, the whole goal here is cartilage protection. Meniscus preservation is all about protecting cartilage.
Perfect. And what do you, this is a good concept. We just, uh, recently inter, we had coal on and we kind of talked about the same thing, but talk about sort of the idea of preservation, right?
I mean, you're preserving the cus you keep saying, but there's other factors at play, right? Age is one of them, but they're talking about, you know, you're looking at all these things, right?
Alignment, how good the cartilage is, and that all has to be. Part of it. Right? What's your kind of algorithm that you look for? What do you, what do you, you know, when you have a care like this, right? You're not just looking at that tear. Absolutely. You have a discoid, you're not just looking at the discoid.
Absolutely. So every patient, um, you know, I think this is a little different maybe to some of my partners or whatever, but every knee patient I get gets an alignment film. I think that's critical. I think you have to know what that alignment is. I think if you are trying to repair a tear and the patient has, you know, seven degrees of various alignment.[00:26:00]
You're just doomed to failure. Um, on that side, you know, you gotta think about doing an osteotomy and, you know, there's lots of arguments back and forth, but, um, I'm looking at the, the, the, the important things are alignment. Cartilage quality and stability. Right? And you've gotta have a, if you don't have an ACL that's working on that side, don't fix the meniscus and leave the ACL unfixed.
You gotta do both the, you know, the ACL and the meniscus, particularly the medial meniscus. Do an intricate. An intimate dance together, you know, they need to both be fixed and, and that sometimes is not meniscal preservation, but meniscal replacement. Right. Putting in a transplant, uh, I just did one today.
Um, I, you know, I, I see these, I like you do, I see a lot of use, you know, we see revision acls and time after time I see this failed ACL in someone who's had. More than [00:27:00] one menisectomy. Well, after you start taking out one meniscus, you know, bit of meniscus here, bit of meniscus there, you really
gotta think about a meniscus replacement and you really gotta get, you know, meniscus replacement, I think can be a difficult surgery and people's.
Kind of shy away for it because of that, but you can't just go back in there and put a new ACL. So stability, cartilage quality and alignment are sort of my three big ones and lesser ones. I mean, they're more important to me than B, MI and H. I think those two, you know, certainly come into play, but they're, you know, if I have someone who's older and heavier, but all those other things are perfect, I'm more likely to say, yeah, you, you know, we we're gonna go for it.
We're gonna give you a meniscus repair. Got it. Do you, and do you, how do you, this is an interesting for, you know, we have similar practices in terms of the complex knee stuff. How do you, so a patient comes into your office, right? You're maybe second or third opinion, I mean, you're UCSF, so they're probably coming in that situation [00:28:00] and they come in, they're told they need this, a small meniscus repair, and all of a sudden now you're telling 'em they need an HTO.
And then they need to have this as well. Like how does that conversation go? I mean, usually it's, you know, there's a little deer in the headlights. Uh, 'cause you know, you're, if you're the, you listen, you're doing limb lengthening films, you know that you're not one of the, you're one of the few guys that probably does it, uh, in that area.
Yeah. Routinely. And you're catching way more things than you think. So how does that conversation go? Like, how does your, right, because they're like, I came to you from a menisectomy, and now you're like, well, you need to have your meniscus replaced or. ACL or something else. I mean, there, there you can, you're smiling.
I can tell 'cause you've had it before. Oh yeah. So I'm curious how's your, how your approach goes. It ha Well, so two things happens a lot that I see a patient and they've not had, you know, they've seen two or three other surgeons who've not had alignment films. And then we catch a significant amount of various, you know, on the medial side if we're looking at medial meniscus.
Um, and I would say that most of my patients come to me because. They know that I'm [00:29:00] likely to be more aggressive about repairing a meniscus. 'cause patients, you know, this is another, um, there's a bit of a sidebar here, but, you know, patients are typically well read, well educated, well sort of. Uh, researched and they are the ones who drive the idea that I don't want a men mastectomy, I want a meniscus repair.
And so they naturally seek out people who, you know, have some kind of a reputation for being more aggressive with repairs. So. I don't get those many, the many that say, well, you know, I don't need, um, I, I just came to you for a menisectomy. But you know, when we do have those that I say, you know, I think we're gonna have to realign you.
You just, you know, otherwise your transplant or your mace or your meniscus, you know, repair is not likely to work. And then I explain what an osteotomy takes and, and how it's, you know, it's not the world's most fun [00:30:00] surgery. Um, that's when you get the sort of, wow. Um, are you sure you know that? Is that, are you sure I need that?
Well, I was like, look, I think that's. The recommended path I would take, I don't, you know, say I'm not gonna do surgery on you unless, uh, but I would say it's the recommended path I would take, and I just worry that if we don't do that, anything else we do is gonna have a high failure rate. And, you know, patients get it.
Do you find, yeah. Do you find, what I find interesting is that conversation you just had. Sometimes they're like, I don't know. And then about two months later they come back and then they're ready to do it because they've done the research now and they're like, wait a second. That's actually the right answer.
Yeah, I just haven't heard that before. They may have seen someone else in the interim as well. Not only have they done the research, they've gone and had a one or two more opinions and they've, they've, you know, they've sort of figured out. Either that that guy didn't even get a film or somebody got the film and said exactly [00:31:00] the same thing and that's it.
So I, I, I mean, I think the alignment's the one big thing that probably needs, you know, that's kind of thing I'm drilling into the residents and the, and the fellows now is be comprehensive in your evaluation. It's not just what the MRI looks like. Um, s speaking of, uh, the meniscus stuff, I want to talk, uh, you had mentioned something previously, you were talking about some meniscus transplant stuff.
Do you have any memorable cases or things you can talk about, like, you know, what's your experience with meniscus transplant? I know you do a lot of them, you know, is there Yeah, I, I, what's your thoughts on. I enjoy meniscus transplants. I think they do well. I think the data continues to get better. I think we were quite pessimistic about them in the past.
Um, I know when I first, you know, 20 years ago, it was always more like a salvage procedure, right? You know, it wasn't like we're gonna return you to sports. I think that some of the latest [00:32:00] data I'm seeing where 50% of patients are getting back to high level sports, I mean that's, you know, I mean it means 50% aren't, but 50%, you know, many of the other ones that aren't are getting back to recreational sports.
Um, I think the results are getting better. I think that, and this is now sort of a personal, um, feeling of mine, um, moving to all soft tissue technique rather than, you know, dovetails or bone plugs or whatever makes the surgery easier. Um, there's data around extrusion that shows that you still get higher levels of extrusion, but the outcome data for patients with meniscus transplants shows no difference really for.
Either bony procedures, plugs, or dovetails versus soft tissue. So if you, you know, so if you do. Think about doing an a, uh, meniscus transplant surgery. If you're a, you know, a surgeon who's thinking about it and you're put off [00:33:00] because the ones you saw in residency all took four hours and there was lots of swearing in the or, and you do them and you do them sort of in a simpler, easier technique, you're gonna start doing more of them, and I think that's gonna serve patients well.
The other side of meniscus transplant is, I think. There's a tendency to get to it too late, right? There's data to show that it's probably better getting earlier before the cartilage changes have happened. Um, you're gonna get that chondro protective effect and probably more longevity outta your graft.
Um, and so that's my sort of philosophy around the, uh, the, the meniscus allograft. I, I think that once you do, the more you do, the more likely. You're gonna find those indications, um, that you will, you will say, this is, this is gonna benefit my patient. Is it from a teaching perspective for transplant? This is really interesting.
So I taught, was trained by coal, uh, started off doing meniscus [00:34:00] transplants and, you know, first couple were couple hours, three hours, two and a half hours. And he, he did it in 45 minutes and I couldn't figure out how, and then eventually got, do you teach them anything? Like the point you made is really interesting, right?
Because. I'm still a dovetail bone plug. Yeah. I've leaned toward a little soft tissue in the anterior horn with acls. 'cause I'm so tired of getting anywhere near that tunnel. Um, do you teach your res, I mean, the point you just made there is like, if you're gonna do nothing, it's better to do this right.
Right to do this option. And the other thing is like if you're the first few years out of, out of residency or fellowship and you start doing meniscus with ACLS and cartilage, like you're gonna, you're gonna never leave the or. Right? So yeah, I think, I think that How do you teach them that that stuff that's in that part's really interesting.
'cause that's not something like I would've never tackled, I remember my first one took like six hours. I did one last week and it took under three with three different things. So it's like, yeah. But I would never have tackled that first week or two in fellowship or in, um, practice. Well, I think some of it's [00:35:00] obviously your training, right?
Um, if you, you know, you said you train, you train with doing, doing bone plugs and dovetails and the person you trained with does them really well, does them really slick. You learn that technique, I think that's great. And I, what I'm trying to do is teach the residents a technique that they can get comfortable with as quick as possible.
And. You know, I mean, I don't ex, you know, they, their first ones are also gonna take longer, but I think that they're gonna say, oh, this is something I trained. You know, our, our fellows come out having done, I don't know how many, but enough that I think they would tackle it in their first job, you know, quite without too much difficulty.
So I think it's partly. The technique, but it's also partly, um, getting the exposure when you're in training, they, they need, they need to see a good number of these done well, you know, whatever the technique is that [00:36:00] particular technique done well, I think the fellows need to see a good number of those be involved in a good number of those, uh, and then they will be able to basically take that to their practice.
I think it's an excellent point you brought up in terms of they need to see it done well and they need to see good outcomes because, you know, it, it, we're up here too. You get the same one. The patient comes back, they said, meniscus transplants don't work. I'm like, we have testimonials. Look it online. You can see people do well.
You just have to do a good job. Uh, but it, it's, it's a, it's an interesting one 'cause that. It's still definitely one of the more stressful cases when you add a bunch of stuff with it. Um, but the results have done properly are impressive. Um, but that's really important point you brought up there. Uh, they just, it's again, it's anything we do right?
Will we train and if we don't see it done well or we don't see good outcomes, then we're probably gonna be nervous to do it for a while. Yeah. The, you know, they shy away from it, which is, uh, which is a bit sad, but, uh, you know, that's, that's brings in the whole sort of concept of, uh, how do you make a really good fellowship?[00:37:00]
Um, on a, on a personal question, not to be a Debbie Downey here, but I, I'm always curious, like these, you do so many cases, so many surgeries, you work with so many people. What are, what are the most difficult cases for you? Is it a. Maybe a single parent that has kids that have to get back to work, they're struggling with an injury, or maybe someone at at a certain age, you know, that's gonna affect their quality of life.
You know, with all of your experience you've seen so much, uh, um. A, you know, an, an athlete, a professional athlete or a collegiate athlete that was ready to go pro, but had an injury that now has curtailed that dream. What are some of the difficult things that you have to deal with and how you manage that and how you communicate that to your students and, and how to, um, go about their, you know, how, how they go forward?
Yeah, I think, I think a lot of that is [00:38:00] how much, um. Energy and time you allocate right from the beginning, right from the first moment you meet the patient. So I mean, grant and I, I think at this point, the minute we walk in the door, we, we can already see usually the patient who has. A complex problem. You know, we, we, we kind of can get that first sense.
And then, uh, and again, most of this happens outside of the, or, you know, most of what you are asking about, you know, how do you assess that, et cetera, et cetera. And what's gonna be difficult and what's not happens. In your clinical visit, in your clinical time, which is why of course we try and get the fellows in clinic as much as possible.
Um, but because they need to see the stuff. Because what you need to do is then as you're engaging with that patient, you're determining, Hey, look, this person's come in. They've got [00:39:00] all the support they need. They've got all, all their social determinants of health are great. Um, they've got a problem that's relatively easy to take care of.
I know I can do this. I, you know, they trust me. I can tell already that relationship's, building, et cetera, et cetera, those ones need a lot less time than other ones that are, you know, have difficulty and have issues, and you just need to allocate the time. The thing is. Your clinic setup is, you know, you've got however, x, X many minutes per slot, right?
Mm-hmm. And you can't just say, well, everyone's gonna get the same amount of time. For example, you have to allocate the amount of time, and then if you can't, you have more follow-up visits before you do surgery or whatever. I think there's just a lot of things that you need to sort of. Do to really be sure that your patients are number one, trust you, and number two, have their expectations realistic.[00:40:00]
Okay. I think that that's where we run into a fair amount of problems. You know, some patients come in and say, look, I've got this ACL tear. You know, and, um, uh, and I see that all these patients are doing well after ACL reconstruction, and, and that's their expectation. You're gonna sit down, well, look, actually, you have some arthritis.
Your meniscus is trashed. We can probably do a few things here, but I want you to expect that, you know, you're gonna have. This outcome, not something that you've heard from someone else? In my experience, this is what it's likely, well, it is likely to happen, and sometimes that's a difficult conversation, but it is.
It is one I think where you have to make that assessment, and I can say most of it, or all of that happens before you go to the or, and then you have to perform a technically excellent surgery and most times not always, you'll get. The result that the patient expected and you expected, and then you gotta throw in the, uh, wild card of complications, [00:41:00] which always gets you.
So I'm assuming that's a part of that, the conversation that you're having with your fellows, not just the technique and everything that you've learned, but also how to manage because it's, it's a stress, right? And how to manage that in order for you to have a successful career. Absolutely. And we'll do debriefs after clinic.
You know, we do debriefs after surgery. We do debriefs after clinic, and I'll pick out the tough ones and I'll say, look, you know, did you notice during that conversation the patient's eyes glossed over and they didn't understand A word I said is, did you see why I went back to something else? And that, or I'll, or I'll say, you know, um.
What else could we have done for that patient? What, you know, what, what other choices do we have? And, and sort of just try and break all of that stuff down. I think, you know, I mean, fellows get it. We, we all got it. It just was like, you just need the exposure to it to see how are the people do it and, and actually.
You know, talking [00:42:00] about training, you know, you have to see how some people do it badly too, so that you know, okay, that's not the person I want to be, or I'm never gonna do that with a patient. That's also part of training.
That's great. Yeah. Yeah. Um, I do wanna make sure in the essence of time we get to a couple more things that are really interesting.
So, uh, I know you got, we could talk about meniscus saving for probably like three or four more hours, but I would love. At least. So, uh, can you talk about your work? Can we pull up his thing on, uh, convergence Medical? I'd love to know more actually. We, we get, we don't have time for this. We'll go to the next slide.
You're gonna, you're gonna, we're gonna be on more meniscus if I, if I, if I know my meniscus. That's a meniscus topic. Yeah. Will, could we do the convergence medical, uh, to learn more about that? So why don't you tell us, you, you've served as chief medical officer for this, this is sort of, it is a really interesting company, et cetera.
Will you give us a little bit background? Yeah. I mean, I'm not gonna, I'm not gonna. I mean, I'm happy to plug the company as well, as long as you want as well. I'm happy to, uh, talk about it. But, [00:43:00] you know, I think the interesting topic here is robotics in arthroscopy, right? We are behind the eight ball compared to our, uh, our orthoplastic colleagues who've been using robots for a long time and we're way behind the, um, our general surgery and our urology colleagues who now, if you.
You know, um, if you need your prostate out, you're gonna get it out by a robot. I mean, that's basically the way, that's the way it works in the US today. Um, so there has not actually been very much, if any, um, sort of work done around using robots for arthroscopy, using, uh, robots for essentially. Two major components.
One is the navigation side, kind of like our arthroplasty, uh, um mm-hmm. Surgeon's work. And where we would do that in the, in, in arthroscopy, you know, pretty. Pretty much the, the, the use [00:44:00] case, I mean, it's not the only case, but sort of the most obvious is acls, right? So acls, everyone says 40% or so, you know, you and I see a lot of revisions.
A lot of that is tunnel. Tunnel Mel position. So we can get an arthroscopic robot that will show us. Where the ideal tunnel placement is not actually, you know, we will, we will control that, but basically gives us a tunnel assist. Um, I think is one place where robots could really help. And, uh, convergence is not the only company that's working on that You're aware of Smith and Nephews tester system?
Yes. And there's a company out of France called RA that already has a robot. Um, so. Kska. Um, and so this is a, this is a kind of a hot topic and that's the navigation side, but what is a da Vinci machine? You know, da Vinci is now an absolutely massive company, and all our general [00:45:00] surgery residents cannot graduate without being robot certified by da vin.
Um, so it is, you know, it is, it's a big deal. They're a massive company. Robots are huge in general surgery and, and urology. Um, but what they do is they give you dexterity, right? With 3D Vision. Have you, if you've ever looked down a Da Vinci screen and seen what you see compared to what we see with our 2D vision in an arthroscopy, it's a bit of an eye-opener, literally.
Um, so they have. Dexterity and vision that we don't have, and that would really significantly, in fact, it's probably even more important for us in the joint because we working in very tight spaces, trying to move an instrument around. We're essentially one handed, if you think of an arthroscopist, one hand is always on the scope, right?
Yes. Or more or less all the time. Unless you, unless you're doing something a bit strange and you've got a fellow helping you, whatever. But the bottom line is we've got one hand on the. Scope. So we are [00:46:00] one handed surgeons and we really should be two handed surgeons. So there's all, this is just the sort of basic outline of potential for what robots could do, but it's very hard.
It's really, really hard. The, you know, it's a figuring out how to make the robots do what you want to do and figuring out the best use of that. The robotics, um, is really difficult. We've got, like I say, da Vinci's been at it for a long time, and so there's a sort of path. We can follow. Uh, but there are, I think, um, some significant opportunities for us in arthroscopy to use robots.
That's awesome. I mean, people ask that. We had this conversation, we had an AI topic front, the podcast, and people were interested in, you know, we're,
you're saying, oh, doctors are gonna be robots, and like, no. The idea is cys, like you keep saying, it's like, you know, better vision, better dexterity, navigation.
I mean, maybe the future. Uh, but at least for now, we want, we want things to be more accurate, right? Because then [00:47:00] we're review avoids revisions situations. Yeah. Yeah, that's exactly right. So there's a, there's a, you, I mean, I think the acls sort of the poster child for. Yeah, this is a place we could really use it well, but like every other technology, once we start using it, we're gonna find all the other places.
I mean, there's, there's, there's a, there's lots and lots of different things robots could do. Um, you know, I think that question about whether or not they'll actually take over completely from surgeon surgeons is interesting. You know, Elon Musk posted something about that recently. Um, that, you know, they're gonna, they're gonna do all the surgery.
I personally don't think that, but, you know, look at, you don't have Waymo yet in Seattle. Right. But, you know, well, my, my, one of my best friends is a, was a designer for them, so I know a little bit about it. Yeah, yeah. They're in California. You see 'em all over the place. They, they're, I mean, you, you'll see like at area, at an intersection for of them, you know, I mean, it's a, it is like, that's how people get around here and they just release their statistics showing that.[00:48:00]
They are the safest, um, you know, drivers out there. They are better, they're better by leaps and bounds of human beings. So, I don't know, maybe, maybe you'll just press a button and you'll get your meniscus repair. But, uh, I think that's gonna take a long while. Yeah. Will, let's show the fun stuff. So again, you know everyone Yeah.
That's not saying it was a segue. You're talking about these drivers, the Dr Speaking of drivers and safety. Yeah. Look at this guy. Tell us a little bit about this. So this was, so, so I've, I've been crazy about race cars all my life. And it wasn't until I finished residency, went into private practice, actually started making a bit of money that I could actually indulge in this.
Hobby slash passion sport. Um, and you know, I've been doing it for 25 years now. Um, I've raced tons and tons of different types of cars. I've done a lot of racing. This [00:49:00] particular picture was 2019. I did a year with imsa, um, which is, this is an LMP car. So Lamar prototype style car. This is a modern car, a modern race car.
It has. All the electronic aids, everything is uh, push button essentially. You know, you've got a steering wheel, you've got paddle, paddle flips, you've got steering assists. You've got. All kinds of different, uh, you know, there's seven pages of data on the steering wheel that you can, you can scroll through to see what everything is.
So this is a sort of a modern race car. And, you know, this was a, this was a fun year. Um, it did reinforce that I'm not a pro race car driver, but on my, on my team, you'll see there's a big, I had there was, we had two cars and these are endurance cars, so you get a driver change as well. Um, and on my team we had two pros and two amateurs.
We'll show that picture. One, be myself. [00:50:00] Um, and the bottom line is, you know, the pros always. We're always just that, that bit faster, you know, they always, they were always able to do, we put it this way, we benchmarked our performance against what the pros are doing and everything. You know, all the data is logged, all the, everything you can see exactly when, um, and then this is, so this is kind of what I do more of, which is, uh, single seater racing, so that, mm-hmm.
Close. The last car was a closed cock. This is single recede racing. This is a Formula One car from the seventies, and this is at Monaco. And, and we raced there, um, every two years or so. I've done it like five times now. And this is, this is opposite, right? This is. A lot of power, a lot of tire, and all analog, so there's no steering assist.
Your brakes are not power assisted. Your gear shifting is, you know, HPA h pattern, gear shifter. Um, you've got a clutch. All of these different things, real [00:51:00] driving real, that real seat of the pants driving. Yeah. And so I can, can you, um, can you talk about the Monaco race itself? I mean it obviously it's different depending on the.
Format. But why do you like this particularly, or, I know this is a cool picture, everyone knows Monaco, but can you describe it a bit more? Yeah. So I think, you know, I mean, Monaco has its own sort of, um, you know, really, uh, um, it is got a, it is got a very different feel, right? There's no other races like Monaco, you're going through the streets of the principality.
Mm-hmm. Uh. From a race car driver point of view, many street circuits are a bit bit, um, they, they feel, uh, they don't have a lot of good rhythm or a good style to them because they're basically streets that have been squared off. And the other thing about streets, street car races is there's no runoff room, right?
And you make a small mistake. And I've done this unfortunately, um, you know, you can be. Four inches off the line, and you'll get a [00:52:00] steel barrier that you hit on a regular racetrack. You know, you, you, you'll have, you'll have a boom, you'll have a, you'll have a, uh, you'll have a barrier like, you know, about six feet or sometimes 50 feet away.
You've got room for runoff. If there's a mistake at Monaco, you don't, but what's interesting is, even though it's a street circuit. It has a really great rhythm. It's almost, I mean, they, they did it in 1929. I'm sure they didn't have so many professional designer do it. They just closed off a bunch of roads.
But it has a fantastic rhythm to it that really just you, you know, you just, once you get in the zone and it's all racing's all about getting in the zone. Once you get in the zone, that thing just flows. It's just such an awesome track. But you can't make a mistake. Well, what's on the bucket list? Have you been to the 24 Lamonts?
Have you No. You know, gone to Bubi or any of these amazing racetracks? Go ahead. I haven't done Lamont, but I've done a, most of the other tracks. I mean, I've been, you know, [00:53:00] we, we, we get invited to do some of the, um. Uh, pre races for some of the F1 stuff. Nice. Um, so in the us you know, in the US that, that's, uh, that'll be like Coda, um, there.
Um, and then, you know, I've done Montreal, I've done Suzuka in Japan. Um, a bunch of, a bunch of European races. Yeah. Um, so I, I would like to do Lamar, but you know, Lamar doesn't do single seaters. It's all, uh, it's all Lamar cars.
Yeah. Um, and I'm really, my preference is single seaters and, and all of my cars are single seaters right now.
Who, who's your favorite driver right now? Uh, who do I think is the best driver? Who is my favorite driver? We're talking about, I, I think we're gonna say Tappin, right? I mean, he's pretty much has dominated, but who, who's your favorite driver? So, I like Ptri. Huh? Okay. Ptri. I, I think that he is. Cool, [00:54:00] calm, collected and gets on with the job.
A little disappointed with his second half of the season. Yeah. Um, he was heading there and then some, I don't know, he just kind of fell off a little bit. But, um, you know, I think overall, I mean, you watch some of the things he does and he is obviously knows what he is doing. He is got the talent. Um, but right now, I think in F1 it's just hard to say that anyone other than Max Mis Steppen has.
That level, you know, he is just, he is just a force of his own. Yeah. That whole Red Bull team, they, they've got it. They've been dialed in. The last few years with their cars and technology? Well, I, I, I don't know about recently. Huh? I mean, I think that they have been in the past, no question. Um, there were always one two, right?
Yeah. But now it's the pure force of Maxin that's keeping at least one of those cars up front. Yeah. The other one's not always there. Yeah. [00:55:00] Or, or in fact, not a lot there. These, this last year is, you know, there's a massive differential there. Yeah. Yeah. Um, again, we did this, we did it again. We're close to the end of time.
No worries. Uh, I don't want to sidetrack, but before we let you go the, the next five, 10 years, what do you think holds for joint preservation and meniscus repair, et cetera? So I think biologics are gonna get a lot better, right? We're gonna figure out what really works. Uh, you know, is fibrin clot as good as I think it is?
Are there gonna be some other magic things that we can first of all, either inject. Before, or, you know, and basically never do surgery and just use injections, you know, maybe intra meniscal injections. We've been doing a few of those.
Um, there's some data out of Europe that's pretty good for PRP intra meniscal.
Um, but you know, I think all of that's gonna develop with, with more time for sure. And so again, again, I think we're gonna do [00:56:00] less meniscectomies. Uh, and then when we do repair, I think we're gonna do better. Um, with some of the techniques we have now, but with biologic augmentation as well. Um, and then I think there's, you know, there's always innovation that's coming.
It's always interesting to see. I think meniscus transplants will continue to get better. And there's three companies out now that are working on synthetic meniscus transplants. Yeah. None of them are proven. None of them. They're still all, you know, probably three or four years away from. FDA approval, but they're all working on it.
It's all coming. It's all gonna be, you know, down the line here. Cool. Well, thank you so much. Thank you, Nick. We really appreciate your time. Dr. Garcia. Man, we, we needed more racing talk. You just come. I didn't want it. I knew it was gonna happen if I kept going. We were gonna be way over the hour. I was trying to be nice.
Don't get me started. We'll have to have a whole separate podcast on it. [00:57:00] Oh, I love it. Do you have a race simulator at home? I don't, so what I use is a go-kart, A racing go-kart. Okay. Okay. That is, that is as physically demanding as any F1 car, I'll tell you that. Uh, it's better than a race simulator, but I, I know that lots of people do, but I'm not a, i, I can't sit in, sit in my bedroom and do racing.
I have to be on the track. I love it. That is so, Nick, thank you so much for your time. We appreciate it. Thank you so much. Thanks Will. Thank you. Thanks Grant. Dr. Garcia, man, we've, we've done it again. I mean, we we're so thankful for, for the doctor to, to join us. As we wrap it up, just remind everybody, check us out, sports docs hall.com, check out our episodes, transcript of the show.
You wanna be a guest, you have questions, um, pertaining to patients questions through, uh, other shows, anything like that. We really want to thank everyone, including our guests [00:58:00] so much. Garcia, I'm racing through it so we can manage it. Say goodbye, say something. Thanks guys. Really appreciate it. Check us out.
We get guest requests. This is awesome. You never know what we're gonna show. Never know who's gonna be on. So this has been a really good year for guests. This is, uh, it's exciting. So thanks so much for Dr. Corvallis, uh, coming on. This was great. Room room.
Audio Transcript
X-ray in Motion: How DDR is changing sports and surgery with Dr. Gregory Kolovich

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon and sports medicine specialist. Dr. Garcia always blaming me for some kind of technical difficulties we have, but we'll get into that later on. Dr. Garcia, how are you? What's going on? How was your trip to, uh, Brazil? It
Dr. Grant Garcia: is good.
It's a long, uh, but I got to see my roots. That was my first time in Brazil, so that was pretty fun. And the race was awesome. Uh, but I'm, now we're covered, so I'm back onto Seattle time zone, so that's the most important thing.
Will Sanchez: All right. Well, we're glad to have you back. And before we bring on our guests, we will like to handle our business because you know, Mike b likes when we talk about him.
Let's give a little, uh, talk about Mike b in the recovery [00:01:00] shop there.
Dr. Grant Garcia: Yeah. So just again, a shout out to them. Thanks to our sponsors. Again, I just, you know, patient today, same experience. So post-surgical recovery, looking for, you know, solutions and what could they can do after surgery. So the ability to have these sort of aftermarket products all in one spot works really nicely, uh, for the patients as sort of a menu, Hey, do you want to enhance it with this, this, or this?
And they've been great. So contact Mike b, they're awesome. If you're a surgeon, you can use them, uh, to your benefit in this sort of recovery process. And the patient satisfaction level's been very high. So thanks guys.
Will Sanchez: Yeah. Thank you Mike. B we, uh, we appreciate all the love. Let's get right to it because this man I believe is on the East coast.
We're keeping him up late. Let's, uh, bring in Dr. Greg Kovich. Dr. Kovich. Um, hey, first off, thank you for taking time to join us. We really appreciate you being here. Uh, how are you this evening?
Dr. Greg Kolovich: Good. Thanks for having me, guys. Yeah, I'm on East Coast time, but everybody's asleep, so it's a nice quiet evening for me.
[00:02:00] Oh, nice.
Will Sanchez: That's great.
Dr. Grant Garcia: So again, to introduce, you know, again, you went to, looks like med school, Ohio State, uh, and then hand fellowship in a, a, a low level place called Harvard. Uh, you know, um, and then, you know, you did your residency training there in Ohio State. Um, and then now you work in, uh, Savannah, Georgia.
Is that correct?
Dr. Greg Kolovich: Yes, sir. Yep. I'm in private practice in Savannah, Georgia. We have a. 25 surgeon group and, um, we cover pretty much all southeast from Georgia and, and then, uh, up in the Hil head all the way down in the Florida, and then as east to Macon and the southern outskirts of Atlanta. So we cover a wide variety, but multi specialty orthopedics.
Dr. Grant Garcia: Awesome. And then, you know, you also, one of the reasons we're gonna talk about tonight is you co-founded, uh, micro C, which is now, I don't you say That's right. Yeah. I got the background. I got the background. Yeah, yeah, yeah. Uh, nonetheless. So we want to get into that, but I think before we start with that, um, will you [00:03:00] kind of talk about, you know, you're engineer by background.
: Mm-hmm. So
Dr. Grant Garcia: how did this sort of engineering student to orthopedic surgeon cross over? And kind of what was your, what was your reasoning for that?
Dr. Greg Kolovich: Well, so engineering, uh, I was, I went to Georgia Tech and I was an electrical engineer and, um, now I'm an orthopedic surgeon like you. So you, you can attest to the fact that orthopedics is, is very much engineering and practice.
It's, it's not always algorithmic. You have to sort of, um, ad lib and use, um, creativity and engineering has always taught me how to think outside the box, how to use different techniques and tools to get the job done. 'cause it doesn't always go the way you draw it up. And, um, I think that really, uh, led me to a career in orthopedic surgery because it's, uh, you know, orthopedic surgery is, is really engineering and practice.
Um, but there was, there was that sentinel moment, um. Uh, I was actually, I, I was an engineer and I started dating a girl who was pre-med. Uh, it's always has to be about a girl. There it is, right there. [00:04:00] It's so, um, to get in her good graces, uh, she and I, I was always struggling to pay, you know, rent and dues and tuition, so.
We got this job doing Oregon procurement for a company called Lifelink. Um, I'm sure you guys have out on the west coast, but, uh, they do all the MTF tissue, uh, stuff that we Oh,
Dr. Grant Garcia: I know who it is. Yep.
Dr. Greg Kolovich: So you get called in the middle of the night and you'd have to go out and just harvest tissue and bone and.
It was kind of gruesome, but it paid a lot of bills. It paid well and um, it got me really interested in anatomy. So then I started taking, um, as part of my engineering, cre engineering, uh, credits. I also started taking organic and inorganic, and then I took my mcat. Um. But I was an engineer, so I scored really well on the, uh, the, the math and physics part of, of the memca, who was the biology part that I struggled with.
But, but yeah, it was always about a girl. And then, um, I really, uh, I was doing what's called co-op. And so you work a semester and then you go to, [00:05:00] uh, school and I was working for a company and, uh, we, we, we started this cool idea, um, and couldn't really patent it because we. We were just co-ops and, um, basically that, that idea went and sold for a bunch of money and we didn't get anything.
So at that point I was kinda like, I wanna work for myself, um, and not get screwed by sort of the big company. So I really wanted to do something that was, um, that I, I had more autonomy and, and I was already doing medicine, so, so those kind of converged and then I, I, I switched paths from engineering to medicine.
Dr. Grant Garcia: And then in your background, I know you do hand surgery, I mean microvascular. Tell us about your specialty that you do, what you specialize in, and kind of the stuff that you see on a day to basis.
Dr. Greg Kolovich: Sure. So, um, I, I do hand surgery, but I also do, um, you know, free tissue transfer and microsurgery. I do a lot of peripheral nerve.
Um, you know, I'm sure in your practice you find everybody does trigger fingers and carpal [00:06:00] tunnels. Cubital tunnels and, and, and those kind of things. Um, I really wanted to separate myself from, from everybody and do something that no one really wanted to do. Peripheral nerve is, is something that not a lot of people have interest in.
It's, it can be difficult. Um, I do a lot of nerve transfers, uh, nerve reconstructions, so I'll do anything from like a brachial plexus to Oberlin, transfer to elli, transfers in the hand. Basically anything that is like iatrogenically. A problem, um, axillary nerves that are injured during total shoulders. Um, I, I do nerve transfers and I'll do tendon transfers.
So I do a really, a lot of complex stuff. So I, I get a lot of second, third, fourth opinions, um, desperate, uh, cases, cases where, uh, a lot of people, uh, so there was really nothing left and I, I usually come up with a plan for it. So that's actually another part of using engineering. Um. You know, basically if someone comes in with a horrific injury, you gotta find out what they have and then sacrifice what they have to give them something that they need.
And really at that point, it's about adding [00:07:00] functionality to their life. Um, I'll give you an example. I did a, I did a reverse Pelli uh, transfer. Where you take, this is for an ulnar nerve palsy. Um, we try to add, pinch this, this is Elli two, where you take the deep branch of the opponents and transfer it to the deep branch of the ulnar nerve to give them more, um, first horse neurosis and um, adductor pinch.
And that can be a big game changer for someone who has, um, an ulnar nerve palsy or, you know, someone with, uh, who needs to get elbow flexion. You can do an Oberlin transfer, stuff like that. Axially nerve injuries are big. Um, there's all kind of transfers, uh, that you can do to sort of give them that forward elevation.
And then I've actually, my peripheral nerve, uh, interest has really gotten me into the leg. So I do a lot of common peral nerve stuff. Uh, satic nerve. Piriformis releases any, I, I can go anywhere and anywhere with, with nerve.
Dr. Grant Garcia: That's awesome. Well, I mean, those are big things. I mean, we, in orthopedics, I, you know, and I like the point you made.
It's interesting, right? 'cause you said you're private [00:08:00] practice, but you do complicated second, third, fourth opinions. Uh, so I, I like that because obviously in my practice I'm private as well. Uh, and do complicated stuff like the osteotomies and meniscus and cartilage transplants and things like that, that not as many of the people in the area want to do.
So the idea behind that's interesting. I mean, it probably took you a little while to build that practice, I would imagine, um, in that area. Or maybe, maybe it was easy 'cause no one wanted to do it. I don't know. Uh,
Dr. Greg Kolovich: nobody wanted to do it. So I mean, when you're, you gotta be affable available and able, right?
Able is probably the least important. Uh, just be available. Um, you know, private practice is a different animal. Uh, a lot of my friends and colleagues work in academics. Um, I feel in private practice, you, you really, um, it can be extremely rewarding, uh, but it can also be very challenging because you don't have a big, um, you don't have a big organization with deep pockets supporting you.
So, um,
Will Sanchez: so going into that safety net, right? It, you know, with the private practice, you're missing that safety net from [00:09:00] maybe if you were in a private practice.
Dr. Greg Kolovich: Yeah, well, you can't really say no. I remember one of the first, uh, things I did was some, I got a call randomly on like a, a Saturday and it was an infected from another doc.
Um, but the primary care surgeon, the primary care doc actually called me and said, would you be willing to take over care? And I was like, maybe six weeks into my practice. So I just took it right. Complicated osteomyelitis of an elbow in a young person. Okay. I took it, uh, you know, went in, grafted it, put antibiotic beads in it, got it to heal.
That, that doc has sent me patients for 10 years, like, like nonstop. I mean, just so thankful. And then of course, taking self pay Medicaid, you know, you just, you don't put up barriers, so you just send it. No one, no one ever asks what insurance I take. I don't, I take all come, because in the end, like. You know, I always find it frustrating when my partners sit there and nitpick about what insurance the patient has, because in the end, you're gonna have some workers' comp that are gonna pay really well, and you're gonna have some people who are not gonna pay well.[00:10:00]
In the end, it's all gonna, if you just keep the ball moving, it all works out in the end. And the, and the idea is, it is just too good patient care in the, in the end, the outcome really matters. So I, I stopped nitpicking about insurance or about this or that. Um, my phone, everybody has it. My cell, I give my cell phone all the time.
I'm happy to do second opinions. I know some of my partners don't see second opinions, and I, I, I, I find that you're, you're, you're never too advanced. You're never too comfortable to do second opinions. 'cause some of these patients really need help and sometimes they just need a second set of eyes to see whether they're falling down the, the right path or not.
And just, just, you know, give them 10 minutes of your time. It's not super difficult thing to do. You can always say no if they can't help. Can't help.
: Yeah.
Dr. Greg Kolovich: So, yeah, just being available and, and, and, and, and, and being able to, uh, be a resource for people to go to. It has really helped me because I don't have a, a steady, you know, some of these hospital systems have hundreds of primary care doctors and ERs that are flooding their, their referral.
I, I don't have that. So I had to go out and give, you know, go door to door, knock on doors, you know, send Christmas [00:11:00] cards, um, do people favors, um. In the end, you get this point where you're established and it, and it just kind of flows steadily.
Dr. Grant Garcia: Do you wanna, um, will, can you pull up that slide? I wanna know more about this, 'cause that might have to do with sort of the giving back and stuff that you do.
Will you just talk about this a little bit more, this slide? Sure. So,
Dr. Greg Kolovich: uh, these are couple film, uh, pictures. Uh, some of, one of these is from a comp, uh, a couple missions that I did. Part of that is in a country called Sini, formerly Swaziland. Mm-hmm. Um, we've been to Kenya, we've been to, uh, Ethiopia, we've been to India.
One of my partners has an orphanage in Central India, in a place called Salem, which is in the middle of nowhere. So we used to go there. Um. We, we do a lot of mission work. I went to, um, Honduras every year in residency with a, a place, uh, a program called Podemos. So mission work has been really, really important, uh, for me and my family.
You can see that central picture right there is my, [00:12:00] my oldest son now, he, God, he was young back then. He's 13 now. He's a lot tall. He's actually taller than me. There's my wife. Uh, he comes too. Um, but on the left, that's us doing microsurgery. Uh, there was a machete injury. On the right. I believe we're doing, uh, something up in brachial plexus.
Looks like it's a, it's an upper arm. Looks complicated. There's, there's the clinics, right? You can see these patients come from far and wide. We would have five, 600 people just show up randomly. And, uh, you know, you work. It's exhausting. Anyone's done mission work. I hope you guys have, it's exhausting. You work 18, 19 hour days.
Sometimes you work by candlelight, literally. And, uh, it's probably the most rewarding thing you ever do. You, you realize that, um. You realize the, the incredible power that you have, uh, to help people. Um, oftentimes we, we don't see that in our day-to-day clinics. Um, people can become very entitled in our world.
But, but in, uh, in the dark part of Africa where they, some, some of these places don't even have electricity. Uh, you can see our [00:13:00] handheld battery powered x-ray right there. There's no electricity in that building. So we brought our x-rays. It was really helpful. Of course there's one in the locker room that, so that's a, that's our Oxo machine.
But
Will Sanchez: Dr. Kovich, uh, you know, we talk about mentorship. Uh, a lot of times on this show, uh, usually there's been an inspiration and it could come from different areas, different people, um, with your, uh, diverse background and, and everything else that you're kind of doing with, um. Within your organization, what has been inspiring or who has inspired you to kind of take the baton and keep, uh, setting, setting the ground rules for the way you go about your business?
Dr. Greg Kolovich: Oh, uh, wow. Too many. Uh, I could name names. Um, Jesse Jupiter was, uh, was my, I mean, he's one of the most, yeah. Uh, published surgeons in not just orthopedics, probably in all medicine. Uh. He, he would just give me advice all the time, and he would let, he, [00:14:00] sometimes he never lets the fellows scrub in and he would let me do the case, which I was really happy about.
And, you know, he is not one to give easy compliments. And at the end of my fellowship he said, Kovich, you don't annoy me. And that's, that's the best compliment I ever got from him. But, um, you know, at, at that time it was a big deal because like, you know, he, he would never give easy compliments. And then later I was the president of Georgia Hand Society and he was one of my first speakers.
I still see him, uh, at, at meetings. A guy named Dr. Michael Ruff, uh, was the head of hand surgery at Ohio State, really took me under his wing back when I was, uh, I think I was probably a first or second year med student. I would basically, uh, come in on Sunday mornings. Just kind of like sneak in and scrub in and do these, he would do these like latissimous flaps and these, these complex things.
I mean, all the stuff that that would take nine, 10 hours, we'd be in there with like plastic surgery fellows and orthopedics, those big cases. And I remember him saying to me, he goes, I go you, these are orthopedics. And I asked him why we were doing these micro cases. He goes, you know, I mean this is just.[00:15:00]
We, we, we were in the Midwest, so it was a farmer who got sort of a, a horrific injury. He was upper extremity and we were just covering him up and, and doing some tendon and, and free flaps. And, um, I felt like he was this X-Men, like he was just doing stuff that no one wanted to do. And he was kind of the doctor's doctor.
And he walked around with like such a sophistication and like, he wasn't like pompous or anything, he was just like the man. And I remember thinking like, this guy's coming out on a Sunday, not on call, just loving his job, loving his family. He was a, he was a big mentor to me. I mean, there's, there's so many.
Um, you know, God, I mean, I remember, um, I, I, I really appreciated people that, um, were good, but you didn't have to, they didn't have to sell it. You know what I mean? I, I'm sure you guys have come across people like that. Everybody knows who the best surgeon is in their group or in in town. And oftentimes it's really, it's really exciting when that person is not the one who's, um, you know.
Broadcasting it. You just, they just walk around with [00:16:00] confidence and, and, and they tend to be really good, not only in their practice, but also in their life. They love their family. They, they spend time in the community. They do other things. Those are the people that have always, and I can name about a hundred names of people I would've spoke.
Those are the two people that really sort of, uh, steered me in the hand surgery.
Dr. Grant Garcia: That's awesome. You will you tell us a little bit more about kind of your day-to-day practice, like your day in the life. I mean, you're doing these kind of crazier cases, you're taking on hard things. I mean, are you kind of.
Situated one office. Do you move around? Like how does it work for you in your practice? And we'll kind of get into your aspirations outside of medicine.
Dr. Greg Kolovich: Sure. Um, well I started like everybody taking level one trauma call. Um, there weren't a lot of hand surgeons who were doing replants. I started doing that and actually upset some of the people in my, my town for doing that because I just came from Mass General.
We were doing a replant every night. I mean, every night, um, every night you would do some sort of replant or reattachment or reask. We got so used to it when I went into private practice, I would just accept everything. And when I started doing that, [00:17:00] my town in Savannah was getting sort of known for accepting this thing because of me and some of my, uh, colleagues, not, not, not so much in my group, but other people were getting upset with me and I realized I was sort of upsetting the herd.
So I sort of backed off on that and kind of, um, did it sort of more word of mouth because I still wanted to do that stuff. But in private practice you have to go where the patients are. So our group is, is, is pretty big. We own two surgery centers and a hospital, and then we own about 17 satellites. So, um, I like to spend one day traveling 'cause I think it's.
It's nice, it's funny. So one, so like Toma on Wednesday, I go from Hilton Head. I have a clinic in Hilton Head, Bluffton area, which is a lot of retired golfers, lot of well to do people. And then I, I immediately go down to Statesboro, which is a, you know, a college town. And then I get into Reedsville, which is a, which is a really rural country town.
And you'll see these really like, you know, salt to the earth farmers. And then these really like, like super end, like Wall Street [00:18:00] vc, just on the same day, you know, and, and to see everyone in between. It's kind of, it, it's a spice of life. Variety is a spice of life. So see, seeing patients from all different backgrounds is sort of fun for me.
Um, I don't stay put in Savannah just because, uh, you know, patients are getting more sophisticated. They're, they're, they want access. They don't always wanna drive two, three hours. So I, I, I do meet them halfway in many cases. So, um, yeah, I, I, I stay in Savannah. Um, probably three outta five days. I travel on one day and then, uh, we go, we have a rural hospital in, in a place called Reedsville, which I do a lot of complex cases.
The, the big stay overnight, Braco Plexus, TMR cases, and, and then I do most of my cases as the outpatient in our ASCs.
Dr. Grant Garcia: Awesome. Can you, so obviously you, you know, you. Do a lot of really great hand surgery, microvascular, really complicated stuff. Um, but you also, that's engineering background. You've had, you talked about the company that you were initially with that just, obviously you [00:19:00] did a lot of work for them and didn't get the same recognition that you wanted to.
Um, and then you came up with some ideas, right? So you co-founded this company called Micro C, that's now Oxo w uh, will you, will you bring up that slide? Will you kind of go through that background of like how that started? What was your reasoning for that? I mean, there's some, we can make some aspirations of this, but I'd love to hear it from you.
Dr. Greg Kolovich: Well, um, there's actually two, two stories that come to mind. The first, I was in Honduras as probably a fourth or fifth year, and we're in the middle of the jungle and we're seeing, you know, four or 500 patients a day, and we never had x-ray. I know that one of our, we, we used to go down there with the dental students and it had this small dental thing that you could probably take a picture of, the tip of a finger, but that's about it.
It was built for taking a picture of a tooth and it was battery power. And I remember thinking then as a fourth year med or a fourth year resident, like how cool would it be if we could expand this to a larger field of view, uh, make it battery powered and portable? So that was really the first time I thought about it.
And then when I got in fellowship, um, in, in Boston, um, I was doing a hand [00:20:00] replant, literally like replanting a hand one night by myself with an intern. Um. The hand literally kept falling off the radius like I was trying to plate it and I had the intern who didn't wanna be there, and I'm trying to turn a screw First, first step.
Any replay is get bony stability, right? So I'm turning, I'm trying to hold this dorsal plate spanning plate. On the carpas and the metacarpal, and I'm like, hold it. And I'm putting the screw in and the thing just kept falling off and I'm trying to bring in this 800 pound x-ray. We had the big C-arm and I kept knocking the nurse over.
I mean, it was, it was three in the morning. I was tired. I was up all night. I was like, man, it would be really cool to have something. I could just literally like a camera, just shoot a picture and not have to bring this 800 pounds to the Armin and my light bulb went off. I'm a little bit engineered in A-D-H-D-I guess.
So then I finished the case and then immediately went to a lab and started thinking about how I can miniaturize a c-arm. And, um, then I, I took that 800 pound c-arm and built this, this is like an eight pound battery powered. [00:21:00] Now, this, this will do, uh, I mean this, this as a nine inch tech, this will do everything that Big C-Arm does.
It's, it, it is fantastic. So we were able to miniaturize that and we, we realized is that. You know, miniaturization is not all that. It's all that it seems. It, it is a, it is a giant and if you guys want to dork out with me and get the engineering of how we had to do that, I'm happy to do that, but, but it becomes a giant heat transfer problem because you can get bolt of lightning.
I mean, imagine 90,000 volts, that thing will go up to 88,000 volt. 90,000 volts of electricity are going through that thing. So it's a bolt of lightning.
Dr. Grant Garcia: So is that in, is that the same thing that happens in a large crm? It just doesn't take the same amount of heat. So like how is that different than, yeah.
Dr. Greg Kolovich: Uh, so, so that's a, okay, so this, I, I'm glad you've gone on that. I didn't want to be that guy that, that, that totally dorks on you. But, um, okay. So let me give you an example. Okay. So let's take, let's say you take a frying pan. It's with burning [00:22:00] oil. You could throw that into a bath of water and cool. That frying pan off pretty quickly.
Right? That's a good way to, to cool off a frying pan that's hot and it's gonna hurt somebody. So that's a cool way to dissipate heat quickly. You can't, that's kind of what a big C-arm does. They pot the, uh, x-ray tube in what's called dielectric oil. And dielectric oil is extremely heavy. So that's why those things are extremely heavy.
So they're essentially throwing a boiling, like a, a, a hot frying pan into a a, a pot of dielectric oil. Ours is a little bit more sophisticated. We had to be really creative 'cause we don't have, ours can't be really heavy, so we had to be, ours is eight pounds. So we had to use really sophisticated heat sink transfers and what's called phase change heat sink.
Which I, you know, I can really nerd out with that one. But, but essentially we had to come up with a really unique way to spit off heat quickly. Because when you shoot an x-ray, 99% of the energy is given off as heat. And when you've got 90,000 volts going through your hand, you've got to shield [00:23:00] that high voltage electricity from the low voltage, like the PCB board, your motherboard, all the stuff that runs your electronics is, is low voltage.
Right? And that's probably two, three centimeters away from a high voltage too. So when you shoot high voltage, all these ed currents are given off and they can really shock and like basically blow up your low voltage PCB board or your motherboard. So we had to do potting shielding, heat transfer, all these really like material science things to make it safe and then also to give off heat.
And then we had to do all the other things about like focusing the, the, so the FDA, there's. So the first step is you gotta make it safe. You can't kill anybody. You, you gotta basically harness a, a bolt of lightning in your hand and not fry everything that's low volt. That is a conversation for another day.
I'm happy to have that conversation, but it, that's a lot of material science that we had to figure out. But then second, you gotta focus the x-ray. So when you shoot an x-ray, you can't just shoot in the space. The FDA won't allow that. [00:24:00] You can't just shoot free, uh, photonic energy. It's unsafe. Yeah. The ener, the photons have to be focused on the detector.
So we have a collimator, which basically conforms like a lens. It focuses the beam. So think about it when you're far away and you can see my hands. Yeah, you're far away. The beam is real narrow. When you're close, the beam is flat when you're kind of off to the side, the beam kind of skews this way. So we have a collator that's contorting the shape of the photonic beam in 3D.
So the detector always has to know where the emitter is. So they talk through lidar.
Dr. Grant Garcia: Do you have a detector on that device or how does that work?
Dr. Greg Kolovich: Yeah, yeah. Oh, no. You, some of, some of the ones that you'll get from Japan or the ones, the cheaper ones, uh, they don't have a detector, so they sell you this emitter and then you gotta go buy a hundred thousand dollars detector.
And if they don't always, like, I mean, I don't know. I, we didn't wanna do that. We wanted to do a whole focus system, so the detector will talk to the emitter and they always talk [00:25:00] and, and. We to satisfy the, the rules and regulations of the FDA. We had to create all of this new technology that we've patented, similar to driving car, like when you drive a car, it, it's using lidar to, to tell you where you, where you are in space.
Our detector and our emitter always know where they are. So you're, you're not spilling radiation off the detector and they have a stop out. So if I take the detector and point it at your face, it'll lock me out. I can't shoot it at you. Got it. It knows, it knows it's not coordinated with the detector. So these two.
So you need that
Dr. Grant Garcia: detector to, you need a detector to show where it's going.
Dr. Greg Kolovich: Yeah. They always that the talk and if they're not focused on it, if it's in a position where it can't focus, it'll lock out. And that's how we were able to satisfy having it, um, move in space. And that was a really, that was a really, at the time we didn't have a lot of technology.
I mean, back in 20 16, 20 18, we started that. The technology had to sort of catch up to our innovation. So we were [00:26:00] able, I mean, I went, I had these brilliant Georgia Tech engineers, my, my, my friend Evan, who's our CEO now. He and I were really, really kind of going outside the box on this because the FDA put up such a high fence, like a high, I mean, they were like, okay, the only way you're gonna be able to get a handheld device is if they talk and move and it's locked out.
And then, you know, it's extremely safe where it doesn't blow up and hurt anybody. So they. They put, they made it extremely challenging for good, for good reason. I mean, it's, you want everything to be safe. So it was an extremely challenging feat of engineering to get this thing approved.
Dr. Grant Garcia: And how did you test it?
It's like you, are you, are you testing this like in a room? Like how do you test it for the radiation dosage, et cetera?
Dr. Greg Kolovich: Oh, well, we built a radiation room, uh, that we just, I mean, some of the tests, uh, so they do drop testing, you gotta drop it from a certain height. Uh, you gotta fatigue it. You gotta shoot millions of x-rays.
Just keep pop, pop, pop. So we have these lead line rooms where we just keep shooting x-rays and it's all, we have these, like, we have these, like, [00:27:00] you know, these meters that just literally, um, they, they add up all the dose, they add up all the fatigue, stress on everything. So like, so yeah, we beat the heck out of it, um, to satisfy the FDA.
And, uh, there's a place called, there's a company called Intertech, which helps us with the imaging, I'm sorry, with the, the testing. So hats off to the fda. A they make it challenging for, for a good reason. But yeah, it was really difficult to pass their test. So, I mean, the thing is extremely safe. Um, and this was, this was your, was not,
Dr. Grant Garcia: and this was your first version, right?
This was the initial one. You know, you got that new one coming out?
Dr. Greg Kolovich: No, we're at, we're at mc two. The first version was, uh, was actually our al our Alpha version, which, you know, one thing that we harp on in, in any company is customer discovery. Call that up. Well.
Dr. Grant Garcia: Yep.
Dr. Greg Kolovich: Yeah, that's our second version. So that's completely battery powered.
Um, it's got a, it is got a pretty long battery life. Uh, we use that thing on, in for pro sports teams. Uh, I [00:28:00] cover a hockey team. We use that, uh, in a hockey, uh, locker room. Um, we use it obviously in our rural clinics. We take, I'm take, I think one of 'em is gonna Bangladesh next week. Um, it goes all over the world.
We've taken it. I've taken the first version Africa twice. Um, but yeah, you can, it was funny 'cause my first version, I took it to, uh, Mombasa and I was going through TSA, I was going through security and the lady thought it was a bomb. So she actually, I mean, there, there was a language there, there was a, I'm serious.
They brought guys with like loaded rifles, like, and me and my wife were like, it's not, it's not a bomb, it's an x-ray. And there was a language barrier there. So I actually had to. Plug it in and show that I could take an X-ray to, to prove to them that it was safe. They didn't know what it was. So, um, it's really cool to be able to take a, um, you know, an x-ray unit, uh, abroad on a plane because you can take it on these mission trips, which was really, really helpful.
We couldn't have done any of the surgery that we did, uh, without that. So it was really helpful. But, [00:29:00] um, yeah, we use it in rural clinics. We use it. I use one in my office 'cause it just, it helps. We have an x-ray suite as well, but having it in the office allows me to do x-rays and, and streamline the things.
Yeah. And then I can do, uh, DR and fluoro and all that other stuff too, as well.
Dr. Grant Garcia: Yeah. So explain, uh, so explain how this, so explain the DR to the patients, the dynamic digital radiography, and versus explain that, how the differences and what you use it for.
Dr. Greg Kolovich: Yeah. Okay. So, um, you guys have all, you guys probably all have a 4K td.
It's really clear you're watching movies like never before. But, uh, some of us, uh, are old enough to remember the analog TVs, the ones where like, um, the big old heavy ones with the cathode on the back. The ones where like the quarterback would throw the football and there'd be a streak behind the ball.
You remember those old TVs? Um, so those were the analog TVs. Um, Floris fluoroscopy is kind of like analog. The X-ray is just on, so that's why when you move the shoulder or the wrist, you see this, uh, blurred. We call it motion artifact. So that's kinda like the old analog [00:30:00] tv. It's basically the x-ray tube is just on and whatever sort of vibratory or motion effect you get, you get kind of a blurry image.
You guys have all used a a a C-arm or fluoroscope to know that with, that's called motion effect. That really bothered me. Um, particularly in small joints when you're trying to look at like a skate fluid or where the. Where the screw is or where your K wires. So we, um, there's been this big push for DRDR is like a 4K tv.
So a 4K TV is basically a bunch of still images stitched together at a high frame rate. So the reason why a 4K TV is crystal clear is because in some cases it's taking 60 images or more per second, and it's stitching 'em together like a flip book. You guys have all, remember the flip book from grade school, the little stick figures that they move and you're flipping it through.
So DDR is basically pulsing shooting x-rays at a frame rate, and then it's stitching them together for a video. So you get a crystal clear image without any motion artifact. And the only, there's, there's two reasons why DDR R is is better than floral Number one, you [00:31:00] pulse the x-ray so you don't just leave it on so you're not just, is
Dr. Grant Garcia: that less radiation?
Dr. Greg Kolovich: Uh oh, a hundred percent. A hundred percent. So the dose is the area under the curve. So if you look at the dose, if you think of like if, and I'm using my hands here. Uh, if you, if you look at like the radiation dose from Time Zero, it's just on. So you're getting all this dose underneath the curve. Yep. DR you're pulsing it, pulsing it, pulsing it.
So they're, you're basically taking a bunch of line and sticking 'em together. So the area under your pulse, DDR, is far less than, than fluoro. So, um, DDR is, is, is sort of a way to get a clearer image with less radiation. And there's a lot, there's some companies, uh, I know Conica Minolta is big into DR you.
That's gonna be a big, you're gonna see a lot of companies coming out with DDR. It is. You, you, you get a far clearer image with safer radiation. Uh, plus you can stop it. What I like about that is you can actually, I mean, if you see our device, you can roll through the images and just stop that, whatever image.
I mean, you guys have, you guys have iPhone. Oh, I
Dr. Grant Garcia: see what you're saying. So you're like, you're not before you do live fluoroscopy. You can't stop at a [00:32:00] certain point. You're like, okay, stop right there. And then they stop. But it doesn't always stop in the spot. Yeah. You can go through your old, like pictures.
Yeah. It's like basically taking is like the iPhone where you like take like 20 photos and then you can skim through and stop at the one you want. Yep,
Dr. Greg Kolovich: a hundred percent. So if you took a video from your iPhone, you can just scroll and stop at that picture and then like splice that picture and print it.
You're taking a bunch of still pictures and stitching it together as a video. So Yeah, it is. Um, it is, it is, it is the difference between an old analog TV from the 1980s and a 4K tv. Yeah. So if you see it now, hopefully guys, uh, if you on a website, there's a bunch of like crystal clear video. It is literally like looking at a movie of a skeleton.
It is crystal clear imaging. And, and one thing that, I don't wanna oversell it, of course, because no one ever believes that, but you just have to see it to believe it. And I think one of the comments that we always get. Is I, I, I can't believe how crystal clear the DDR is, so I mean, I, I, I hope hopefully you guys will see it.
Dr. Grant Garcia: Do you, um, with this product, do you, uh, from a, from a [00:33:00] patient or from a standpoint of like, obviously clinic efficiency, right? Like if we got four providers in clinic and you have one x-ray machine, that's pretty slow, right? Yeah. And there's certain aspects. Is there different? Like when we looked at new machines in our office, there were certain specialties that it was more beneficial for, like hand Yeah.
Uh, the smaller machines we're better for, but like I do shoulders and knees. Mm-hmm. Is that, do you have, is that the capabilities of this device or is this mainly for the hand extremities?
Dr. Greg Kolovich: So we we're submitting a new, um, a new clearance for larger anatomy. Um, everything needs to be cleared by the FDA, so shoulder and, and, uh, hip and shoulder and knee are on that.
Interesting. Um, but you know, it, it has the same power to, to to do that. Now we have to convince the FDA of that of course. But, uh, um, that, that is, that is on horizon. So. So right
Dr. Grant Garcia: now in your clinic, foot and ankle, and can foot and ankle use it or is it mainly hand,
Dr. Greg Kolovich: foot and ankle and elbow down? Yep. And I, so, so what, what, what I like it for is the fact that, okay, so, you know, um, I want to get a quick, so let, let, let me give you an example.
[00:34:00] Um, instability is a big part of my practice. Anybody that does revision stuff or second opinion is gonna get an SL tear, right? Just like you're gonna get a label tear, right? Anterior lab, you want to, you wanna see dynamic stability, so you wanna stress the arm and see if it kind of comes out. And we, we
Dr. Grant Garcia: can't do that right now 'cause it's too much radiation for somebody.
Dr. Greg Kolovich: Yeah, so our, ours is, well, I mean, we have all kinds of, well, we
Dr. Grant Garcia: can't go in the office and do a fluoroscopy of somebody. It's just, it's just not like, versus being able to bring it into your office like that, you know what I mean?
Dr. Greg Kolovich: Sure, sure, sure. Um, well, so we, I mean, we, we have remote triggers, so there's a footpath, so you don't have to be right next to 'em.
Now, I, I, we can argue about, you know, the radiation exposure and everything, but like for me, getting like when someone feels a pop in their wrist and they're a young guy or young athlete, particularly like a hockey player or like, you know, football player. I worry about SL tear 'cause you don't catch that early.
Then you get, start getting DC and SL diastasis and then you miss the opportunity to fix it. And we, you, you probably remember from, from residencies that SL, chronic SL tear do terrible. Probably like a chronic, you [00:35:00] know, a bank heart that was missed probably will do terrible. You're gonna get glenoid wear and, and all kind of problems.
So, um, if I can catch an SL tear the week of and go fix it with like an internal brace or something, they're gonna do great. So the problem are you saying
Dr. Grant Garcia: Will's favorite word? Be careful.
Dr. Greg Kolovich: Oh, sorry. Internal brace. Oh, I love, oh, okay. I won't, I won't.
Dr. Grant Garcia: He loves that. He gets too excited. He starts. Oh,
Dr. Greg Kolovich: no. Well, I mean, I'm, I'm, I'm very fond of Arthrex, obviously, but, um, the, um, my, my point is, uh, if you catch it early, like it's a difference between salvage procedure like A PRC and having your risk back to normal within a couple months.
Right. I mean, it, it is really like, and the problem is they, they, the x-rays are normal. So you get a still image and it's normal. So you
Dr. Grant Garcia: need dynamic. You need, yeah. Yeah.
Dr. Greg Kolovich: So what I do is I go in there, so I don't even bother taking em over to, I mean, I don't even bother taking 'em over to my x-ray and get a still image because it's not gonna tell me anything.
I could do a clench fist view, but even that can be, so what I do is I just say, look, I want you to do this back and forth, [00:36:00] and then I'll just, I'll, I'll hit the pedal and they'll just go in like this. I'll be, you know. Across the room, and I'm staring at that big screen and I'm looking boom, that the, the skateboard is flexing and the, the lunate is extending and they got clear DC and you see the diastasis and the DDR R is so clear.
I can literally stop on that image and show what a diastasis. So that's a big, that's a big plus for me. And there's all kind of billing parts for that, right? For like DR versus static, but. My, my point is that's a big, and then you, you probably work, uh, with elbow. Um, I, I, I look for Tommy John, uh, ulnar later ligaments.
The other thing I like to look for is MCP and P, particularly MCP instability. That's one that's often missed. Or, um, fracture dislocations of the PIP joint to see where it's stable. You know, I mean, some of those are real stable. If you just, you know, do an extension block, uh, pin or even like a, a splint, you can get away without doing surgery.
But to know where they're unstable is really helpful when you're doing ddr R 'cause you could just [00:37:00] sort of take a freer or even your finger and just, just do that. And you'll see when they come out. And then elbow dislocations, that's another one. I put 'em flat on there after they come with an elbow dislocation.
If they're not super swollen enough for, for me to test them, I kind of look where they just come out and if they're coming out like 30 degrees, I'll put 'em a dynamic splint, say full flexion to like just at 30 or maybe a little bit before then. And then, so I can get 'em, get a DDR of their elbow and find out right where they're coming out and I can sort of brace 'em and, and, and, and I can, um, harbor conservative treatment.
By just watching 'em to see where they come out become unstable. So Ddr r has really changed my practice because it's giving me all kind of things to know where, where their actually dynamic instability is. I think shoulder is a, I don't do a lot of shoulder, but a shoulder would be extremely helpful for, particularly for, for laxity, posterior, anterior, um, I think it would be extremely ddr r DDRs would really help a, a shoulder surgeon.
Dr. Grant Garcia: Well, we don't have that. I mean, most of the time, I mean, I think I have a question for you. I mean, this is something that. I, [00:38:00] in fellowship, I did work. I went to HSS for, uh, residency. We had a lot of good hand surgeons who did some of the crazy surgeries you're talking about brachial plexus, et cetera. Um, but to dynamically see it in the office is very uncommon.
We just don't, we just didn't have that diagnostic tool set. So you're basically allowing, this is allowing you to do, diagnose, a whole nother set of things faster. Than you would've been able to do before that? I mean, 'cause before what were you doing? You weren't, you weren't checking that or were you even doing anything if you didn't have it?
Dr. Greg Kolovich: Well, so I, I don't know about MRIs are disappointing in many cases. I can't tell you how many times I've gone in, uh, and scope the wrist or an elbow thinking I'm gonna see X when I really see y I'm sure in shoulder you go to, you go to a scope of shoulder and the rotator cuff's completely fine and you think it's torn.
Um, that happens a lot. Um. For, for DDR, uh, particularly with fractures, I, I, I, you really kind of find the point of dislocation, which actually really helps me, um, with my pre-op plan. Um, and the, the one thing that [00:39:00] I've always, uh. So, so I, I get a lot of like high energy, uh, TFCC and DREJ dislocations, you know, you're gonna find out where to even splint them.
And the, I swear, I, I, I've done hand surgery for 10 years and sometimes I even get confused. I'm like, do I splint 'em in supination or pronation? You know, which ligament is torn and you kind of know the textbook stuff, but like, you just want to see it pop in and become stable. So what's really nice about this for A-D-R-E-J dislocation.
Or TFTC injury, I can actually find out where they become unstable. It gives me an idea of whether the vol or dorsal complex is, is torn, and I don't, can't tell you how many times I've gone in and, um, I had an MRI, which said that this was torn. And then the DR literally like, blew that outta water. Like the DR completely, uh, did not match.
The dynamic stability did not match up with the MRI. So if I would've treated the MR, I would've got the wrong outcome. So DDR is really, if you can do it and you can fit that in your practice, it will sometimes, [00:40:00] it will sometimes, um, contradict, uh, an MR MRI result. I think MRIs sometimes are, we over rely on 'em.
Dr. Grant Garcia: Yeah.
Dr. Greg Kolovich: Um, seeing a joint where it wants to be, particularly in a hand and wrist, um, it's so easy to do, especially if you've got this in your clinic. Uh, it's really, it's really made me not go down the wrong path in some cases.
Dr. Grant Garcia: Well, I think it's also like you keep saying it's better for the patients, better for the clinicians.
'cause I, I find that, and I think we'll, we'll attest to this, that if you can have a better preoperative expectation for your patients, that's a big deal. Right? Like, if you're like, I'm gonna go in and do this, and you, they wake up and they get that. Sure. That's usually the people that are very satisfied with their outcome.
Even in comparison to people. You know, these, I get second opinions, thirds like yours and they're, or they come back after surgery and they're like, A doc said, I was just gonna figure out what happened inside. Right. That doesn't usually, that outcome's not usually the same. Or it's not as frequently as good as if someone's like, my doc said I was gonna get this and I got this and I feel really good about the thing.
Right. You're basically [00:41:00] giving them more information ahead of time and they're feeling more confident diagnosis, not only from the patient interaction, but also now the interaction between the doctor and the patient.
Dr. Greg Kolovich: Well, I mean, think of it like, think about when, so we always say you could teach a monkey to operate.
You can't teach a monkey when not to operate. Right. And that's, that's really the, the hardest part of our job. Once you, once you learn all the surgeries and you're at that point in your career. Um, the hardest part is learning when not to operate. And I think, um, for me, like if I have someone like, like say MDI like a young girl with, with, you know, a high.
You know, high maintenance family, you don't wanna operate on someone with MDI, you just gotta kind of coach 'em through it, right? So if I can show them safely that you know, their elbow's popping or it's hyperextending and it's clicking, or their shoulder's sort of the sulcus sign, if I can show them that and they can actually see the glen, I mean, they can see the head popping back in and that it's not hurting her 'cause she's not wincing that that does a lot of good for the patient and her family.
You can say, look, they're popping out. [00:42:00] Like without me hurting her. And this is just who they are. And I think that's really, that's really help bailed me out of some typical situations where you've got a patient who's complaining to their mom that they hurt, they don't need surgery, but you gotta convince the family that they don't need surgery.
So DDR is really helpful in that case. And I think ultimately like for the, for the, I had a young patient with an elbow dislocation and um, the mom, the mom was really asking me why I don't do surgery. I was like, well, you not, the body can fix. I mean the ligament's torn, but it's, it's not, it's gonna heal.
The LU C's gonna heal. Let me show you. And I was literally showing this lady, I blocked her a little bit to make her comfortable and I could show how the elbow would sort of come out and pop back in. And I said, this is why we're gonna split you to here. And in two weeks we'll go a little bit further and we'll just, every time you come in, we're gonna go a little bit further.
That ligament heals. And this avoids surgery. It's, it's, it's not gonna create a scar tissue and you'll get to where you wanna be with extension. That really. Because the MR MRI looks, the MR MRI is always terrible, [00:43:00] right? The MR MRI says a million things are torn. They look, they come with you the report and like you need to fix this.
You, your L UCL L is torn. There's a non-displaced OID fracture and they, the MR MRI just shows all these things and you're like, none of that stuff needs surgery that will heal. And a young patient, um, lemme show you. So DDR can be a really nice tool to sort of walk them back. From insanity, right? Like, why are we operating on this poor kid that's gonna do well if we just treat it not, not
Will Sanchez: you?
You mentioned, um, that you've worked with, uh, sports teams. How has DDR been, uh, helpful and impactful with teams and how can you see the future of DDR supporting teams, whether it's, whether it's professional or yeah, you know, college or local. Did, does it become like almost like a on the field triage type?
Can you explain a little bit about that?
Dr. Greg Kolovich: Uh, well, so, so hockey players are animals. Hopefully anybody, hopefully you get a chance to take care of a hockey team. Those guys are the toughest, [00:44:00] I take care of minor league hockey too. So these guys are so tough, they're super nice. They just wanna get back on the ice and hit somebody and, and in some cases you have to be like, I'm using DDR R to like pull these people back.
In some cases I'm like, look, you're unstable. We gotta stop 'cause these guys will literally go back. You know, if you give them any green light. So for me, um, you know, hockey, you'd be surprised how many hand and wrist injuries they get. Um, I see a lot of, uh, forearm fractures, finger dislocations. I don't know how they dislocate their finger.
They're wearing gloves, but they do. I see a lot of rib fractures. Um, I think as we get more advanced with DDR, like looking at like, uh, shoulder instability, uh, cervical spine, I think it could be extremely helpful. Um. Uh, in, in the cervical spine. Lumbar spine, uh, as we, as we get, uh, you know, more sophisticated DR techniques, would,
Will Sanchez: would someone like you need to be a, as skilled as you would need to be that person that's operating this machine, or would it be something as far as like just the team doctor?
Like what's the level?
Dr. Greg Kolovich: Oh, no, no. [00:45:00] I, I, I don't shoot the, the at does it the athletic trainer? Yeah. Um, uh, I'm usually like. Uh, you know, sometimes I'll be i'll, sometimes there'll be, he'll be down there shooting it, and then they'll, we have this little walkie talkie. He'll be like, come in the room. We want, I want you to look at this.
Or sometimes we have a, we have a platform where we can see the x-rays live, or, you know, I mean, we, we have all, oh, that's pretty cool. We made it extremely easy. I mean, we can remotely see the x-ray. Um, so, and we can see the DDR R remotely. So even if I'm, you're not at the game, like those images can be shared securely, uh, to the team doctor.
So we, we really try to make it. Extremely easy for the team doctor because sometimes you're not, you're on the road, you're not on the road with the team and you need to know what's going on. So we, we, we definitely take, um, you know, remote, uh, access and portability to another level, of course. 'cause you can put it in a suitcase and take it with you, right?
Um, so, so that's pretty
Dr. Grant Garcia: cool. So you can be, they, the team can be getting on a way, on a game. They injure themselves. They call you and say, Hey Doc, I want you to take a look at this. And you can literally watch [00:46:00] them do the DDR R.
Dr. Greg Kolovich: Oh yeah, we have a secured access. Yeah, we can log in and look at it. That's pretty cool.
Yep. That's really cool. Um, middle night doesn't matter, especially if they're on the west coast. Yeah.
Dr. Grant Garcia: Uh, chu we want, in the sake of your time, I know it's getting late, we want to kind of know for you what's the roadmap for this technology in the next five, 10 years? Sure. What are you guys thinking?
Dr. Greg Kolovich: Um, well, um, our goal is to make it, uh, more powerful.
Um, we definitely, uh, we know there's a lot of need in, uh, larger anatomy, so, um, we need to get a more powerful x-ray. So we've had a lot of patents around the monoblock. We need, we need to make it more powerful. We need, we, we want to get a bigger detector to cover more anatomy. Those, those are the next goals.
We have a lot of, um, we have a lot of, uh, special vendors. Um. I, I can't really say who they are, but they, they have certain needs, uh, particularly for, um. Department of Defense, um, uh, you could imagine how important it's to be able to get, you know, uh, a, [00:47:00] a chest tube or a central line in the right spot. Um,
Dr. Grant Garcia: yeah.
Dr. Greg Kolovich: You know, I mean, beginning, oh, you
Dr. Grant Garcia: can't do that. You have to have, you can't have a c-arm dragging in there with power.
Dr. Greg Kolovich: Well, I'm talking about putting one on a flight on a helicopter or like a Well, my point is that you couldn't do that
Dr. Grant Garcia: with
Dr. Greg Kolovich: any of the current devices. So, so we have a lot of aspirations for home care.
We, we hope one day that, um, we can, um. I dunno if you guys have children, but I have four. And if you've ever been to the ER on a Sunday, uh, with a kid with a presumed broken wrist, it's a miserable experience. Yeah. It's also very costly. So, uh, we hope to, because it's so portable and safe, we hope to be able to, to dial up an x-ray where you can have a, one of our technicians or one of our, one of our, um, associate, uh, portable companies come and, and shoot the x-ray and then not only get you diagnosis.
Like at the point of care, like in your home or on the sideline, but then also triage you with someone, uh, like you, uh, Dr. Garcia, and then some or someone like me who can, who can then get you an appointment that day. Right? So, um, you might be [00:48:00] sitting, you know, at home on Sunday, you might get a text and say, Hey, there's a patient in your area that, that would like to see you for, you know, a proximal humerus fracture.
And, you know, you can just. Use our, our user interface to go and say, make that person appointment. So, you know, using technology will be able to help you as a surgeon work smarter, not harder, where you don't necessarily have to take these calls and, you know, put yourself out there and cover all these ERs where you can just use a technology that's out there doing it for you.
And just being an early adopter, you can, you can increase your referral basis, uh, and you can start triaging people because it's gonna be cheaper and safer. Right. I mean, I had a $4,000 bill, uh, from a both Bone parum fracture. And one of my children, it was also four, six hours, four to six hours of waiting.
Not a great experience on a Sunday. Ruined my weekend actually. But I mean, it is what it is, uh, especially when your kid is in pain and you trying to helpless. I mean, really, like for me, like she wasn't even that much pain. So like, I just need to get her in a splint and I need to get an x-ray, you know, so I know like, what's going on, so, and I need to get an [00:49:00] appointment.
I mean, you know, so I want to get one of my partners, but um, I was out of town, right? So you needed, you had to do what you had to do. But, um, so we, we hope to, to sort of streamline the process by making it safer and faster, but basically bringing access, portable X-ray to the point of care.
Dr. Grant Garcia: Yes. Yeah. And do you, and right now you bring up, you're bringing up kids and I wanna want to take a time, wrap it up for you and then make sure you can go home and, I mean, go, go to sleep and relax.
Uh, but the, uh, is this, is this approved? Can you use it in children right now or you, is that next step for you with FDA?
Dr. Greg Kolovich: Um, I believe that is on the, uh, this application.
Dr. Grant Garcia: Cool.
Will Sanchez: Great. Uh, as we wrap it up, first off, you know, once again, thank you for your time. I wanna know where your allegiance lies on Saturday.
Are you, uh, you know, John, the farmer? Are you, are you pilgrim? Are your yellow jacket are your buck? It's very confusing. Well, we need to know where, where, where's your allegiance?
Dr. Greg Kolovich: Well, my Georgia Tech yellow jackets are 9 0 1. We [00:50:00] barely beat Boston College. Our defense has got some work to do. I, I, but everyone, I live on an island off the coast of Savannah.
Everybody's a Georgia fan. So, um, but I also grew up in Ohio, so I, I, I'm a big Ohio State fan, and, and Ohio State's a big, uh, they're actually a big proponent of our technology, so they've been great to us. Oh, yeah. Yeah. I, I, I would probably, Ohio State is, has always been, uh, you know, I've always bled scarlet and gray, but, um, is nice to see Georgia Tech, which is not traditionally a great football powerhouse, although we have a great history to be nine one.
I just hope we can hang in there with Georgia. We beat Georgia. That will be my national championship. Are you gonna be okay with your, with your friends there? If, uh, no. I'll wave my flag. I'll wave my wine and go. I, my, my white and gold flag will be out there all year if we beat Georgia.
Will Sanchez: That's great. Uh, Dr.
Kovich, uh, thank you so much for your time. We really appreciate it. It's really informative. It's exciting to hear where the technology is going and it seems like, um, there's a lot of possibilities. [00:51:00] Someone that has done work in Dominican Republic, my wife is in Nigeria right now. Uh, just hearing that you're traveling and helping out these communities, I, I know how difficult it is.
You usually work in conjunction, not only with the locals, but also their, their politicians. And sometimes you don't even have, uh, you know, you're not even able to go into certain. Places without telling someone where it can get pretty hectic and scary if you don't abide by their rules. So just hearing the work that you're doing out there, it's uh, it's, it's heartwarming.
So I, I personally wanna say I, I appreciate hearing that from you.
Dr. Greg Kolovich: Thank you. I really appreciate that. And I, I, you know that in the end, I, I create an x-ray for the purpose of, of, of helping people really, it's really what it's about. And, and we stick to that mission every time and we, we really do enjoy doing mission work.
Is, is, is the icing on the cake for us? Awesome. That's great. Thank you,
Will Sanchez: Dr. Garcia. Uh, it was great having Dr. Kovich. Um, I mean the, the possibilities are [00:52:00] endless, right? I, I was even thinking about the, uh, wilderness first responders, right? They're coming in their helicopters.
Dr. Grant Garcia: There is so many options for this.
Yeah. You
Will Sanchez: have people training. They could, maybe, could do some of these, uh, these, these imaging beforehand. So then by the time they get to the hospital, they already kind of know what's going on. They identify, especially when you have an injury out there in the woods. That can be, you know, extremely dangerous.
Every second counts, especially if you have a tour or anything. Right. So just hearing about stuff like that, that was one of the things I started thinking about, uh, along those lines. Um, uh, I, let's do it. Hey, for. Check us out, sports talk, catch every episode, transcripts. We'll have a transcript of this show.
Um, you wanna be our next guest? Reach out to us. We're, we're extremely thankful for all of our viewers on YouTube, for everyone listening on different platforms, whether it's Apple and Spotify and iHeart and everything else. Uh, we just want to thank everyone, uh, for joining. We hope that [00:53:00] you're learning something That's really the reason that we kind of got into all this.
Uh, besides us talking about the giants and what kind of miserable fans we are, but be, besides that, we're really happy to, uh, provide great information, great guests, uh, last words, Dr. Garcia.
Dr. Grant Garcia: Well, I know great guests, really cool technology. Really gonna be next level for us. Just showing doctors we still have a void in.
Diagnostics, right? MRIs are great. Cts are great. This is a new pattern of things we haven't really got into and easier to use than something that's like ultrasound machines, easier access faster. So all these things are gonna improve for patients. But really the key here is as you keep hearing it's patient first.
Yeah, fix the problem, find a problem, find a solution. So anyhow, thank you. Thank you so much, uh, Dr. Povich for coming on, and um, thanks viewers. Appreciate it. All right.
Audio Transcript
The Power of Play: Preventing Injuries and Promoting Health at Every Age

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez. You know who I am. This is Dr. Grant Garcia, our orthopedic surgeon in Sports Medicine specialist Dr. Garcia. How are you? Let's just start off. We're really excited about our guests, but I won't always wanna say, how are you doing? What's going on? And our giants, once again, are we?
We won't talk about the Johns. We'll just move on. How are you? Let's talk about that.
Dr. Grant Garcia: I was hoping you weren't gonna say anything. It's always one of us that brings it up. But you know what we're, I'm good outside of that. Life's good. We got some great guests coming on. Super excited about this, so this will be really good.
Will Sanchez: Yeah, we have two incredible guests, but as we always do, we wanna make sure that we take care of the folks that take care of [00:01:00] us, that take care of our patients, or more importantly, your patients, the recovery shop, and just talk about Mike B at the Recovery Shop and how good they are.
Dr. Grant Garcia: I think that's our new slogan, takes care of us.
That takes care of them. That takes care of the patients. I like that. I'm gonna tell those guys. Uh, so yeah, so big shout out to them, Mike b uh, for sponsoring us. Uh, they're great. They're really, it's really nice for the surgeons to have these sort of aftermarket options for patients. It's, it's literally today I had.
Probably five people ask about it. So, uh, it's really nice and concise. The patients really like it. We love the nice machine. We're really loving some of the other products. This nutrition is huge. We're gonna talk about some other things today that are really important for the postoperative and preoperative portion of surgery.
So they do a good job. But without further delay, we wanna, we wanna announce our really nice, great guests.
Will Sanchez: You know, today we're talking about something that, you know, every parent coach athlete thinks about, you know, what are we doing, what's right for our kids? Uh, also, you know, how can we keep playing as we get older [00:02:00] without breaking down?
We've had this discussion many a times because I am an older weekend warrior that have broken down, and we're always trying to make sure that we could get things legit. Let's bring on some folks that know what they're talking about and can help us in these areas, like to welcome Dr. Starman and Dr.
Winter. Uh, thank you so much for being here. I'm very excited that we have four people. We have this Hollywood Squares thing kind of going on. We had a center, uh, square. We'll be good to go. But welcome to the show. Thank you for being here.
Dr. James Starman: Uh, great to be with you guys tonight. Yeah, thanks for having me.
Dr. Grant Garcia: Yeah, so you guys both come from Ortho Carolinas and for the, the listeners, it's a really, really prominent orthopedic institute, orthopedic, uh, you know, conglomerate down over there in uh, Carolina. And so it's really great to have you guys on. And I know you guys have a strong emphasis on a bunch of different things, but I think kind of to start, and we'll kinda jump around just to make sure that everybody gets the chat.
Um, but, uh, [00:03:00] Jim, why don't you tell us a little bit about, I know you said you, you know, you emphasize in a bunch of different things, right? The shoulder, knee, and some cartilage. Um, but kind of talk about your background and what brought you over to Ortho Carolinas. I know you trained with Freddie Fu rest in peace, uh, but very prominent orthopedic surgeon.
Um, maybe talk about how that influenced you and et cetera.
Dr. James Starman: Sure. Yeah. So I'm originally from Pittsburgh, which, uh, as fate would have it led me to Dr. Fu. And so he was a big influence in my early career and, and honestly in my, uh, choice to pursue sports medicine. Um, so I, um, I had a chance as a medical student at the University of Pittsburgh to work with him, uh, take actually a whole year off of my, um, medical training to work with him.
So I got a chance to sort of see how he treats athletes from all over the world. Which really influenced me, uh, significantly in, in choosing orthopedics and choosing sports medicine specifically. Uh, so feel really blessed to have known him and obviously it's a great loss that he's no longer with us, but, [00:04:00] um, his legacy certainly has lived on in a lot of other people, so we're really fortunate for that.
Dr. Grant Garcia: Awesome. And what do you do current? Will you talk a little bit more about your practice at, uh, ortho Carolinas for the listeners, especially some of the focuses.
Dr. James Starman: Sure. So I focus on, um, a lot of sports injuries, of course, and also, uh, the weekend warrior population makes up a big part of the people I take care of.
So it's really kind of cradle to grave as far as the knee is concerned. Uh, so I do anything from cartilage restoration, micro fracture, oats procedures, uh, all the way up through knee replacement, and, um, uh, similar kind of profile for the shoulders, uh, from cradle to grave for the shoulders.
Dr. Grant Garcia: Awesome.
Mm-hmm. And, uh, Dr. Winter, can you give us a, can you give us kind of your background too? I know you're kind of in your same, are you guys in the same, I know that Ortho Carolinas is actually quite large. Are you guys in the same sort of subgroup or you guys work on different areas, different offices, and then we'll give us sort of your background too.
I know you did a little more of a shoulder focus.
Dr. Bradley Winter: Yeah. [00:05:00] Dr. Shaman and I are both work in the Winston-Salem office. Uh mm-hmm. Or in like the triad area, which is Winston-Salem, Greensboro, Kernersville. So we worked together fairly, fairly regularly. Um, in my, my journey to sports medicine came from playing soccer.
I grew up playing competitive soccer and then played in college at Vanderbilt and got a chance to hang out with, uh, with the sports medicine guys there at Vanderbilt during my time. Just really enjoyed the. The time learning from them and getting to see what taking care of athletes looks like. Not only from folks they took care of high, local, high schools around Nashville, but taking care of us, um, as athletes at Vanderbilt and just kind of spurred my interest to, to keep pursuing that and moving on.
I. Um, to med school and, and then fortunately, um, had the opportunity to train at Steadman Hawkins with Dr. Hawkins. And, um, really learned a lot about the shoulder from him and, and really spurned my interest in, in shoulder surgery and, and, uh, move forward to where we are today. [00:06:00]
Dr. Grant Garcia: And for shoulder, do you have a, a specific thing you, you know, you like to focus on or you do more, uh, arthroscopy, combination of that replacements or kind of a, are you more sports shoulder focused?
How does it work for you?
Dr. Bradley Winter: A little of both. Um, I, I, I do some traditional sports medicine, knee, knee and shoulder, um, arthroscopy and then open shoulder as well with shoulder arthroplasty and fractures.
Dr. Grant Garcia: And, uh, I think you guys probably can each answer this separately, but kind of what drew you to Ortho Carolinas, obviously big name.
I looked at that for a number of different things from fellowship to residency, et cetera. What, what drew you guys, and we could start off, you know, from right to left, but, but you know what drew you guys to Ortho Carolinas?
Dr. James Starman: Uh, so from my perspective, I, uh, actually did my residency in Charlotte, Carolina and Atrium Health, uh, this partnership with them.
Uh, so I actually got to know a lot of the partners in this group as a resident and they kind of brought me along and, and helped train me and. I did my [00:07:00] fellowship at University of Virginia and then I went into private practice initially in Florida. Uh, but after a few years, we decided that we wanted to come back to the Carolinas.
And so, uh, thankfully I had some contacts up here and was able to, uh, you know, come at the time when there was a, an opening in, in the Winston-Salem market. So that's where we ended up. But um, we've been real fortunate to come back.
Dr. Grant Garcia: Awesome.
Will Sanchez: Yeah. Um, Dr. Witter, uh, what kind of drew you to the specialization?
You, you mentioned that you had a soccer background, but for you to fi, uh, focus on shoulder and elbow, what drew you in that field? Because I don't equate soccer with the shoulder and the upper body with the arms. So what was the correlation there?
Dr. Bradley Winter: I really didn't grow out of, out of my interest in soccer.
Soccer, kind of pushed me into sports medicine in general. And then the exposure to it during training. Just the, the variety of, of things that you see in the shoulder, the complexity of it, um, and some of the challenge, um, that I, that I've just found [00:08:00] very interesting as it relates to taking care of, of the, you know, even.
Young kids with throwing injuries to, to older folks with rotator cuff injuries, to, to, uh, you know, shoulder replacements. Just really get to see the gamut of population. And, um, I just, I found it very interesting and fascinating that the different types of surgeries and, and rehab that you could to do within the shoulder.
Will Sanchez: Uh, did, go ahead. Go ahead, doctor. Keep going. Well, no, what I was gonna say was, did you have an experience, you know, with seeing the shoulder injuries? I, you know, when I think about sports, uh, injuries, uh, especially for youth, it's either football or baseball when it comes to shoulder injuries. So it was this, there was an uptick or there's something there that kind of drew you.
Um, where you wanted to help, because I know Ortho Carol Carolina has an emphasis on serving the community and being a part of it. How does that all kind of intertwine with [00:09:00] what you do with youth sports and, uh, ortho Carolina commitment to, uh, youth sports?
Dr. Bradley Winter: I think probably the biggest thing we see for, for youth sports with throwers is, is throwing shoulder and throwing elbow pain.
There's a, there's a huge number of kids who are, are playing baseball and throwing on a regular basis that, especially during the middle school years, when you start to play middle school ball and travel ball and little league and a lot of those overlap, you, you end up throwing a lot of pitches or, or throwing a lot of bullpens and warm up and, and cool down and, uh, and your pitch counts start to rise.
And so you see a, a big uptick in, in kids that have either throwing shoulder pain or throwing elbow pain. Just being able to, to kind of walk those families through the process of this. Yeah, this isn't the end of your career. This isn't, you know, this isn't something you need to retire from, from, uh, from baseball at 13 or 14.
Now we can, we can get you through this. We can rehab you and we can get you [00:10:00] back thrown again safely and effectively, um, without, you know, really being high risk for long-term injuries. Um.
Dr. Grant Garcia: I, I think it's a, I want to, I want to follow up on that. I like this. This is good. So we're gonna, this is not always going the right direction, the directions we're thinking, which is good.
So can you fill in the listeners, this is a big thing. We have a lot of people actually listen to the podcasts and their families that come in. Not just in salary, but you know, they'll come in, maybe your office and they'll have heard this, but they're really concerned about their kids' throwing ability.
It's less football, much more baseball. I'm assuming that's the same way in your situation where you've got like two parents, a coach and a trainer, and they're all in the same room, and you come in to talk to the player. Right. And they've got a high interest in this. Like how do you, how does that conversation start with you?
Right. Maybe you're lucky and you've had the MRI, you know, it's something that they need surgery or maybe they don't have anything, or maybe you have information, you know, it's not that bad. Like how do you kind of start that conversation with the players and let's say mostly baseball, right? The parents think they're pro, [00:11:00] they're probably not pro, but you gotta figure out a way to navigate that.
How would you, how do you deal with that situation? It's just probably interesting for the, for the parents to hear this as well.
Dr. Bradley Winter: I like to just hear where they're at right now. I like to hear what they've been doing, you know, where they're playing, what teams they're playing on, what coaches they're working with, and just try and get a sense of the overall amount of work that they're doing, the amount of throwing they're doing, and, and try and weave into that, who's really keeping track of the pitch counts.
Um, because oftentimes you can see. Nobody's really taking care of the pitch counts. You know, coaches may be watching them for their particular game with the travel team, and then high school or middle school may be watching that team, but nobody's really counting up all of the pitch counts. So trying to assimilate that and get them to see what we're seeing, which is that this tends to be overuse and not a specific event that their thrower [00:12:00] had, uh, and, and kind of walking them through.
Seeing how much they're throwing and how much they're working outside of practices and how much they're not really keeping track of their pitch counts, tends to lead to these overuse types of injuries. And then let them, you know, let them kind of sort through. How do we move forward from that without overwhelming the, you know, the, the risk of, uh, you know, everybody wants to get to Tommy John immediately, right.
Um, yes, not overwhelming that discussion and, and just, you know, trying to walk them through that if, if we're not convinced that there's something bigger. Obviously if there's something bigger than we go to imaging and, and have those discussions.
Dr. Grant Garcia: Awesome. I
Dr. James Starman: think, I think that's a great point that Brad makes.
And I would, um, add to that as well, that I think it's really important that you understand kind of the goals of the athlete and not necessarily just the goals of the parents or the coaches for that athlete, because that can also inform a lot. Of kind of how we counsel, um, these [00:13:00] types of conversations and, um, trying to allow them to continue to enjoy the sport that they're participating in and not just doing it for the wrong reasons or with this pursuit of perfection that they may never achieve.
Um, and just trying to help, um, you know, guide those conversations and, and maintain the focus on letting these athletes enjoy their sport and, and enjoy their, their participation.
Dr. Grant Garcia: I think that's a really good point. Will, we've talked about this is the focus is on. Player first, then everything else around them.
Right. And what do they, what do they think? And sometimes, like we were making the kind of, I don't wanna say a joke, but when they come in and they, you know, one person thinks they're pro and the other one's just like, I like
playing baseball 'cause it's fun. I put my friends, the conversation changes a little bit different.
Yeah. And also how, what their caliber is, right? I mean, there's, you have to kind of modify your conversation, your thoughts. Right.
Will Sanchez: Yeah, a quick follow up there, um, for, have you seen uptick, right? You're in, you're in [00:14:00] the south warm weather, right? You, you know, if you're the Pacific Northwest, east Coast, northeast coast, you have the changes, but you're not playing baseball all year long or you're not.
Playing football all year long compared to, uh, a warmer climate states. Do you see any differences when you treat a patient that's maybe coming from warmer states where they can play the same sport all year long compared to, uh, colder states where sometimes they have no choice but to play multiple sports?
Any, any data on that?
Dr. James Starman: Um, I, I don't have any specific studies to cite to you on that topic, but I would tell you that I think that, um, most of us would probably agree that there's been a, a general trend nationally and, and elsewhere, um, towards year-round participation at a younger age for most of our athletes.
And that goes across multiple sports, not just. Baseball, we're throwing sports. Mm-hmm.
Dr. Grant Garcia: So I
Dr. James Starman: think that, I think that that's a problem. I, I understand the reasons for it are multifactorial and there's a lot of people [00:15:00] chasing college scholarships and, and dreams of participating at the next level. And it actually creates, I think, sort of a.
Perverse motive that kind of forces everybody to follow suit as you continue to see this decline in sort of truly recreational youth sports. And it becomes this hyper specialized, uh, thing where if you're not playing baseball year round, you really just can't compete against the other kids who are, and so it then becomes less enjoyable for kids to participate in sports unless they're doing it year round.
So I think that that's a problem. That we have not solved. And if anything, I think that's probably getting worse and probably driving some of the, the trends in overuse injuries in this, in this population.
Dr. Grant Garcia: And that's kind of this slide you guys had up here, right? The kind of the risk of, I think this is really interesting because like you said, ev I mean, I'm my kids, I'm not a baseball family.
We're a swim family, right? My kids yesterday, were having a conversation. They're eight and 10, and my wife's telling me [00:16:00] how the other kids are doing like 500 lessons a day. They're gonna hurt themselves, but that's the way it is. Everybody, everybody's trying to one up each other in these scenarios. And it's the same way with baseball, football, you name it.
So obviously there's, it's a balanced conversation. So how do you guys, how does you or Arthur Carolinas, et cetera, like how do you, how do you get involved in this type of conversation? Right, because it's hard. It's almost like preventative, which is more challenging. As a surgeons, that's not really our. We don't really do as good a job in that, at least maybe it's just me, but, uh, the, the preventative stuff is important, but we don't talk about it a lot.
Dr. James Starman: Yeah, I would, I would agree with you. I think that we were more, I
Dr. Bradley Winter: seems to have lost the audio from Jim, but I'll, I'll chime in here. Um, I think getting, getting involved with, with some of the local sports organizations where, you know, your, either your kids are involved or you have patients involved and just like you said, trying to get on the early side of this.
Um, and, and. Even the, the soccer club that my [00:17:00] kids grew up playing for, I got in with the coaches early on and, and talked to them about overuse injuries and, you know, what does it look like to have time off throughout the year for, for some of the kids. Just to see if you can build that into the program, like you said, on the preventative side.
'cause it's much harder to, to work backwards after the kids are injured or they have these obese injuries. 'cause then they're sitting time out and families are unhappy. They want to be playing. Get back as soon as you can. So, yeah, I think it's very much a, a preventative thing, which like you said, is not easy.
'cause that's not our forte. Our forte is taking care of people after they're injured and figuring out how to get them back to sport rather than, than keeping them healthy.
Dr. Grant Garcia: And Jim, I think your audio is working on our side. Do you wanna try it again?
Dr. James Starman: Uh, yeah, as long as you can hear me okay, we, yeah, you're good.
Yep. Yeah, I just can't hear him for some reason. I'm
Dr. Grant Garcia: not sure. He's doing a good job of talking. I can tell you he's doing a great job. Perfect. Yeah. Jim, why don't you continue with your conversation. On. The idea of the sports specialization, like how, how would you intervene? I mean, you're, you're [00:18:00] doing a lot of ACL tears and you're dealing with this.
I mean, we can go to that in a second. Um, but like, what do you think the, how do you think these interventions work? Right? Like, we know that in ACLS you can reduce significantly with neuromuscular training, et cetera, which we'll jump to in a second. But from this sports participation, it's a really challenging thing to deal with because it's like, it's really hard to tell people to like, stop doing that, right?
Because that's what everybody's doing. So like when you do the outreach programs, are they effective? What do you guys think?
Dr. James Starman: I mean, I think that, um, for the people who walk in the door to the clinic, they're coming in with a specific problem and they're looking for a specific solution to that problem.
And so I think our, our job is, is too faceted. The first part is to address the reason they're there, um, and to, you know, accurately diagnose and come up with a plan that's going to resolve that issue. And then the bigger question is, is how do you prevent these issues from continuing to come up? And I think that if you can.
Um, if you have the right parent or the right coach or the right athlete, [00:19:00] that you can kind of have that, that conversation about, um, you know, athlete burnout and, and overuse injuries from over participation and, um, and get that concept of cross training and, and sort of multi. You know, multi-sport participation.
I think that some people can be receptive to that and other people just aren't going to hear what you're saying. And I think that that's just, uh, the reality of, of trying to have that conversation. But I do think it's worth it to try to broach that topic when you're seeing people for these overuse injuries in particular.
Will Sanchez: How much responsibility does, uh, the coach have when it comes down to taking care of taking care of our kids? Uh, Dr. Winston mentioned before that, you know, not everyone's being diligent. About, uh, the pitch count. You know, normally, like if you throw over, uh, I guess literal league rules are if you throw over 66 pitches, you're supposed to be off for four, four days.
There's different rules or regulations. So [00:20:00] staying with that, you know, preventative, uh, outlook, does some of this need to fall? The parents, the coaches, or just everyone needs to kind of, you know, come together to make sure that we're taking care, we're taking care of our kids and athletes.
Dr. Bradley Winter: Ideally, I think it's an everybody approach, but, uh, I think especially in the throwers that I see it, it's, it's kids who are playing for multiple teams.
So you can't, you can't ask the coaches to necessarily be entirely responsible because if they're playing for two and three different teams and they're working with a pitching, pitching coach. Nobody's, nobody's talking to each other for the most part, so nobody's keeping track of how many pitches you threw Tuesday night for your middle school when you're playing Thursday night for your travel team, and then you got three games on the weekend.
Um, or working with your coach in between. So ultimately I think the parents are the ones who are, are gonna hold a lot of that responsibility, but they're also the ones who are probably feeling the most pressure to keep up with the neighbor down the street who's doing the [00:21:00] same thing and the kid who's beating 'em out for the spot on the team.
And so it just, it just gets caught in this really vicious cycle of, of trying to keep up with everyone else who they are perceiving to do all of the things that they. Want their kids to do, but that kid's not getting injured. So why is my kid getting injured? And, um, it's, it's a, it's a tough conversation that takes often a couple of visits to kind of get the parents on board with you to understand that, that a lot of this is not related to a specific moment in time or a specific injury, but it's all of the things that you're doing cumulatively that, that are where you are now.
Dr. Grant Garcia: Do, do you guys maybe I'll, uh, Dr. Starman, do you guys find that, obviously, I mean, I brought this up probably multiple times in the last year on these podcasts regarding baseball, but I know there's other sports. Are there other sports that you see this in that, and I don't, I mean, baseball's just a very particular one for me, for the players, but do you see other sports that you see this in?[00:22:00]
What sports are those and how is, is it different? Is it the same? Like how, how is that conversation different, Dr. Starman?
Dr. James Starman: So the, the best example I can think of on, on that would be gymnastics, which, uh, hits close to home for me. 'cause I have two competitive gymnasts in my house. Um, one who's 10 and one who's 12.
And so. You know, I certainly, um, understand the idea of, of year round participation in a single sport because that's essentially the nature of gymnastics. There's really no other option for them to be competitive gymnasts other than to do it year round. And so, you know, we've dealt with our own set of.
You know, minor overuse injuries just from the repetitive pounding of landing, various flip maneuvers on the floor. And, um, you know, thankfully in my house at least, we've not had to deal with any of the, um, spine issues that can sometimes come up, uh, related to spondylosis and gymnasts, uh, with all these repetitive hyperextension movements in the spine.
But I think that, uh, you know, those are [00:23:00] definitely concerns and, and things that we have to constantly be on the lookout for. Great.
Dr. Grant Garcia: Um, will, do you wanna bring that up? I don't wanna jump into the acls. I mean, that's a big topic, right? So I don't wanna put you on the spot with the Freddie food stuff, but have you, do you, are you, um.
Are you still a proponent of, do you do double bundles ever or do you ev mostly do single bundle acls?
Dr. James Starman: So I do 100% single bundle acls. Um, always have, and I think that, um, obviously Dr. F's legacy is, is double bundle and it always will be tied to that. But I think that, um, he would probably. Argue that, that his legacy should really be more about anatomic ACL reconstruction more so than double bundle as a technique.
And I think that that, that is probably the greatest thing that, that he helped me learn with respect to that surgery is how to place an anatomically correct graft. Um, and so I think that, um. You know, that's really been my focus is, is trying to [00:24:00] make sure that I'm getting a, as accurate graft placement as I can.
Um, and I go so far in, in my cases to actually use fluoroscopy on every case to make sure that I know exactly where my tunnel, um, pin is gonna be placed before I drill my tunnel. Um, and that's based on, on some of the techniques that he had made use of when I was with, um, you know, with him observing him.
Um, and so I think that, uh. You know, that's, that's really to me the, the best lesson that, that he taught me, um, as it relates to ACL surgery. But I think that, you know, the double bundle, the literature is out there. I, I certainly don't think that anyone is obligated to use two bundles to recreate the anatomy.
Um, but I think at this point, I would hope at least that we can all agree that there are two bundles. Um, yes. How that was something of a debate for some people, but. But yeah, there's, you definitely did quite a bit to stimulate the, uh, the discussion on that topic.
Dr. Grant Garcia: Well, and I, again, the goal was not to be a controversial one.
I love that con, I like actually where you went with that. I think that we're gonna [00:25:00] jump to this in one second, but the idea you brought up of the Good done, the well done ACL anatomic right. If you do acls, you sports, you probably do revision acls and a lot of times you do it for non anatomic acls, probably the most common reason.
And so the idea that you're focusing on that is really great for the athletes. 'cause like obviously we wanna reduce ACL risk, which we can talk about. Um, but we also wanna make sure when we do it, we do it correctly. So that's a really important point you brought up. And the idea of maximizing anatomic, you know, there's some companies coming out with CT guidance for some surgeons to do ACL tunnels.
And so it's just a really interesting topic that we could bring up at some other point. Will, uh, to talk about how you get so precise, right? Because it matters. Would you agree? I mean, you really want to do a good job, like you get one shot?
Dr. James Starman: Oh, absolutely. Yeah. I think, um, you know, there's, there's no way to recreate a hundred percent of the footprint with a single bundle graph, but if you have it in the right spot, you're gonna get just the right amount of pl and to, to give you that, that anterior translation control in [00:26:00] addition to the rotational component.
I think that absolutely 100% impacts people's results and their ability to recover and, and probably the risk of re-injury as well. For sure.
Dr. Grant Garcia: Um, I don't wanna leave out, uh, Dr. Winter. He's just, he's always been adding good conversations here. Would you, would you help us out with this slide to talk just a little bit about this?
I think that I get this a lot like. My friends who have young female athletes always are like, why do you do more acls and females than males in certain age groups? And they, you know, they hear about it, but they don't know enough about it. And I have to try to explain it to 'em. So it's good that we have this slide.
Dr. Bradley Winter: Sure. Yeah. Happy to, happy to chime in. Um, yeah, I think like you, we see a lot of, a lot of, uh, female ACL injuries. I see a lot of soccer players with, uh, with ACL injuries and, and basketball as well seem to be the two, two big ones around, uh, around, for me anyway. Um, but yeah, you know, female has a little bit wider pelvis, so increased Q angle.
Um, so more, more valgus stress at the knee. [00:27:00] Um, you know, a lot of, a lot of, uh, people looking into ligamentous laxity and whether there may be some component of, um, hormonal cycle changes that increases ligamentous laxity during certain times of, of a female cycle that may put them at increased risk for injury.
Uh, you know, certainly, um, you know. Changes in intercon or notch, um, somewhat narrowed notch, uh, in females, seems to be higher risk for ACL injuries and then changes in in muscle strength and activation. You know, certainly somewhat more. Um, hamstring, hamstring tight seems to be, uh, somewhat of a risk, uh, for folks.
Dr. Grant Garcia: Um, a question for you guys, both of you on the notch thing, 'cause this just came up. Someone was asking about this when they, I saw doing surgery. Do you guys always, I'm a routine notch Platy guy. I like to see the back, the lateral wall. I know we're getting into the, the weeds here, but do you guys find.
Like, I feel like in females, I try to improve that notch. So if I'm gonna do a ACL as [00:28:00] an impend, is that common for you guys? Or you guys are fine with not doing that? How does it work for you?
Dr. James Starman: Um, for me, I'm, I'm not a notch Platy guy. I've, I've never done them. Um, and, uh, yeah, I, I'm not really a big proponent for that.
Dr. Grant Garcia: Okay.
Dr. Bradley Winter: I do it probably 20% of the time, depending on what I see during the operation. If I think it looks fairly narrowed or I can't see back to the back corner, then I'm probably doing an otoplasty.
Dr. Grant Garcia: Right. Cool. Um, let's go to that next slide. I want to know the, um, this one, so these landing issues, obviously you can see them so that, so in, in some of the places, like, uh, in your institution, do they have you guys measure this for the players?
Like obviously you can see here that somebody did these measurements and stuff. Explain this to the, the listeners or viewers.
We will go with Dr. Starman.
Dr. James Starman: Yeah. So for, um, you know, the landing in valgus, it's, it's gonna increase your load on the [00:29:00] ACL. Uh, this is, uh, you know, not one that in my practice that we routinely monitor or measure. Just with the setup that I have in my office, we're just not really equipped for this, you know, particular type of measurement.
So it's not something that I normally routinely use, but I'm not sure, Brad, if you do that at all in, in your practice.
Dr. Grant Garcia: Go ahead, Dr. Winter, he wants to know if you do the same in your practice or do you guys have physical therapists that you work with that do this or trainers?
Dr. Bradley Winter: Um, I have a conversation about. This often with patients in the office, but, but really having the, the, um, the therapist working with folks on this when we, when we start the, the kind of more sports specific, um, phase of, of ACL rehab.
So kind of the six month plus phase for me is when we're working on a lot of this stuff, but. Yeah, I haven't paid less attention to, to valgus knee, knee landing or valgus, uh, valgus positioning. [00:30:00] And, um, you know, certainly the hyper extension at, at uh, at landing as well. Um, I think these videos are probably from the Charlotte, um, Charlotte Rehab group.
I think they have a little bit, uh, little more video technology than we have in our therapy office to do some of this.
Dr. Grant Garcia: Do you guys focus though? I mean, do you ever talk to the players, like, I have this a lot where the, the ACL's done and then they're worry about the other knee, right? Mm-hmm. They come in, they ask about that.
I think since Dr. Winter you're speaking, do you ever have that conversation with them? Like, you know the, in theory, right? There's higher chance of retear on the other side. Uh, so is that the preventative conversation than you? You, you get to chime in 'cause right, you're not really, if they don't, if they haven't turned their ACL yet, you're probably not seeing them at the beginning before they have that.
Right.
Dr. Bradley Winter: So every once in a while you get a sibling in the room and you're like, Hey, do these, you know, do these exercises so you don't have the same injury. But most of the time you're right, you're talking about the other neat. Um. I have a big, big group of, of soccer players somewhat. 'cause I'm plugged in with that [00:31:00] community.
My kids play competitive soccer and so I get more of those kids just being around the fields and things. So, you know, a a lot of the, the female soccer players, I'm having conversations about how do we, how do we decrease the risk on the other knee, you know, some of the FIFA 11 warmup and, and cool down exercises.
And then specifically some of these. These, uh, preventative type, uh, uh, situations of preventing the valgus when you're landing primarily, is what I'm discussing with them.
Dr. Grant Garcia: Got it. And Dr. Starman, how about you? What kind of conversations do you have with this sort of. The, the, you, you get the athlete in, you've done the ACL surgery or it's a, maybe it's a partial ACL and you're gonna try non-op.
Uh, but that conversation, how, what's that conversation like for you about this sort of the landing methods or ways that, you know, can you make they say, Hey, can I, how can I reduce my chance of ACL tear on the other side, or how can my sister not get it?
Dr. James Starman: Yeah, I mean, for me it's, um, when I'm kind of.
Reaching the one year point with, uh, somebody who's been [00:32:00] reconstructed. I'm, I'm focusing most of my conversation on, on the operative knee and the concept of graft maturation. Um, and how that, how that relates to risks moving forward for, for, mostly for the surgical knee. Um, and trying to put that in terms relative to the contralateral side.
So. Uh, they understand that at, at one year their risk of re-injury is roughly equal to their contralateral knee. And at two years that, uh, as you point out, that the risk of injury is actually less on the reconstructed knee than it is on the non reconstructed knee. Uh, which I think is, is helpful for some athletes in terms of the mental hurdle of getting back into participation and trusting that need that's been reconstructed.
Dr. Grant Garcia: That's a great point. Will you explain that to the listeners and Will and everybody else? What do you mean by the maturation of the graft?
Dr. James Starman: Sure. So when we are reconstructing the ACL with, uh, whichever type of graft you're selecting, whether it's uh, auto graft or allograft tissue, uh, the graft tissue that you put in has to go through a process of [00:33:00] integrating with the body and turning into.
Uh, what would be, you know, equivalent to a ligament, um, histology wise. And so that takes time. And that's something that is really not a function of how hard someone is working at their rehab process, but it's just a biological process that takes a defined amount of time, and that's directly correlated with the risk of re-injury.
We know that around three or four months post-surgical that the, the load to failure for the graft tissue that we've placed is actually less than at the time of of which the surgery is completed. And by, you know, roughly six to nine months, uh, that it's starting to get stronger, but still not as strong as the native ligament.
And then by one year it's typically equivalent to the, the normal load to failure strength of the ACL. But not until two years is it actually at its maximum, uh, which actually becomes less, uh, less likely to reinjure than the contralateral native ligament. So I think that's, that's a concept that I think it's important to note for [00:34:00] people that, that have this kind of.
Idea that they're a fast healer and if we can just work hard enough, we can get them back to sports faster. And you have to kind of debunk that idea and, and tell them that this is not something that they're in control of as much as they would love to be.
Will Sanchez: Awesome. Dr. Winter. Um, there are a lot, I, I'm assuming there's a lot of difficult questions, right.
That you have to have with the patient, with the family for all of you, right? But directing it to you, Dr. Winter, well, how difficult is it to tell an athlete maybe right before an injury or they've had a small injury that they need to back down? Right. We, we started off the show with. Everyone wants to be at the next level.
Now, NIL has added an extra element, just like the cherry on top with the whipped cream where everybody wants to be a pro athlete. That's so much money to make, not even at the pro level, but at the college level. But what are some of those difficult conversations you have when you have to tell an athlete that someone, I need you to back off, [00:35:00] and that might be in their senior season and having those conversations.
Dr. Bradley Winter: Yeah, those, those are tough conversations. Having, having played. I think helps, uh, having an understanding of what that feels like to, to be in that moment in time in life and, and have an injury to kind of have, have some understanding of where they're coming from is helpful. I think one of the bigger challenges we have is a lot of these people, we don't have a relationship.
The first time you see 'em, they may come in with a new injury and, and you may never have seen them before. You may not know the family, you may not know the athlete, and kind of establishing the trust and the rapport to say like, this is important that. You take this time off and you understand what your injury is, and this is what the rehab timeline looks like, and, and getting the buy- in from them and understanding, especially if you don't have advanced imaging yet and you don't have like real data to say, this is the injury and this is the time we need to spend out.
Just we like we need, we need to. To start from scratch. We [00:36:00] need to kind of build that trust to say like, you know, we're, we're gonna be out for a certain amount of time. We're gonna get you through this. This is the, this is the approach we're gonna take. This is the timeline I think we're looking at to get you back.
'cause you're right. Nobody wants to hear you're out. But everybody wants to hear what's the timeline? That's always the next question, when a hundred percent, when when can I return? When can I start practice? When, when can I look at playing? And so trying to get that timeline as quickly as possible for folks, I think starts to establish that trust again.
And starts to get you to the point where you can have those more realistic conversations of. What does this look like? How long is my rehab process? And, and when do you see me getting back to play?
Dr. Grant Garcia: So this is an interesting, uh, maybe side question, um, for, we'll go with Dr. Starman first with your return to play criteria for particular surgeries.
Do you ever change it? For a different athlete? Or do you keep it the same for the kind of the procedure like an ACL or, you know, meniscus repair or something else? Like how, how does that approach for you [00:37:00] work or how do you feel about that?
Dr. James Starman: Yeah, so I think that's, um, that's a great question. I, I think that as we evolve as orthopedists, um, we're seeing more and more of this sort of notion of personalized medicine that's not just cookie cutter, not just following a, a protocol written on a piece of paper.
Looking at the goal of the athlete, uh, the specific injury, um, the, the quality of the repair or fixation that you feel that you have, um, and sort of the risk tolerance for that, that patient and kind of what's at stake. And so I, I always talk with people about, um. In particular with overuse injuries when people are trying to get back for the end of their sports season, and kind of what are the stakes of that season for that athlete and what are the stakes of that injury for that athlete?
And so there's, there's definitely situations where I'll allow somebody to try to, to go and participate. That may end up not being able to kind of perform at their desired level or even, you know, fully participate. [00:38:00] Um, but for them it's really important to get that, that last. One or two games in of senior year of high school in, in football or basketball.
And as long as it's not something that's going to put them at a, an undue risk long-term, I think that's a reasonable conversation to have and, and kinda let that athlete make that decision, uh, with their parents or with you, uh, as the, as the treating doctor, but. I do think that we're gonna see more of that moving forward and, and as we, um, you know, have more insights into these rehab processes, I think that that becomes a more achievable thing to do.
Dr. Grant Garcia: Excellent. Uh, Dr. Winter, do you feel like for, so this may be me again, just talking out loud and there's no data on this, but this, uh, for shoulder, I tend to see that shoulder return to sport in my practice is a lot more variable than the. Then the knee return to sport for some reason, like I'll have lab repair patients that are like, you're ready to rock at like four and a half months.
And maybe I'm crazy for letting 'em go back, but [00:39:00] like, or four months. And they're like, beg, they're begging them football players. And some guys take like six, seven months. Do you notice a little more of, I mean, you do both knee and shoulder, so do you notice any variability in that? Am I crazy for seeing that or is that something you've seen in your practice?
Dr. Bradley Winter: Oh, I, I definitely see the same. I, I have some, some instability patients who. I mean, at two and a half months you're like, I can throw, and I'm like, oh, let's, let's hold on. Um, I'm not, I'm not sure we're ready for that yet. Or I, you know, I, I'm, I'm ready to play football. I'm like, well, you may feel that way, but you know, the biology isn't there yet.
Right. The, the biologic phase of healing isn't, isn't quite there. Um, but yeah, I, I totally see the same, I mean, interesting, interesting story to the, you know, to the point of do you change your rehab. I had an instability case in a soccer player, which is not very common, but I felt like we could get him playing again relatively quickly with pretty low risk.
And, and, uh, you know, parents were ecstatic. She's like, oh my gosh, we're playing at three months. That's incredible. But, [00:40:00] um, yeah, I, I definitely see a lot more variability, I think, in shoulder than knee. And some of it may be my own. Bias about ACL graft maturation. To Jim's point earlier of like not really wanting to stress that graft too earlier in the rehab program and just probably sitting on some of those a little longer because you're waiting for really the biologic healing, you know, more so than is, than he rehabbed or not.
Dr. Grant Garcia: Well, it's also probably, it might also be too of the weight- bearing status, right? Like you're just constantly stressing that graft versus like, you know, they're playing football, right? One big hit, maybe the one that's gonna stress it, but they're not always getting constant stress on the shoulder. It's just a little different.
Baseball, baseball is different, obviously. Um, I, I wanna make sure we have time 'cause we do we're, we are wanna make sure we have time on This always happens with these conversations. Uh. For, to switch topics. 'cause I know that the aging athlete is a really interesting one. This is actually the one that gets a lot more hits 'cause the people talk a little bit less about the aging athlete.
And now with like regenerative medicine, people aging, [00:41:00] everyone's, you know, the forties, the new, the new thirties. Thirties, the new 2060s, the new 40. Who knows? So, uh, we have a slide on that. I wanna bring it up and maybe have each one of you com uh, talk about it. Will you wanna pull that up for me? Sure. So I don't accidentally delete it.
So can you guys talk about this? Let's say I just talked to, let's say Dr. Starman, can you kind of go after this and talk about this? What happens? And you know, we won't doom and gloom this 'cause we have the next slide on how we can keep people strong.
Dr. James Starman: Sure. So just kind of taking it from the top here. So, uh, obviously as we age a lot of things change and, uh, that is.
Certainly, uh, true of our muscles as well. So, uh, physiologically we see a decrease in muscle mass, which, uh, you know, generally accelerates as you age. Um, the, uh, overall strength, uh, comes along with that and the ability to recover. So as we age, we, we lose muscle mass more easily. And we struggle to build it as quickly as when we're younger.[00:42:00]
Um, going along with that is a decrease in bone density and our joint cartilage integrity. So we see, um, kind of irreversible changes to the cartilage surfaces, which, uh, open them up to more cracking and fissure development and, and flaking off of the cartilage in general Thinning. Um, and then obviously we see osteopenia and that continuum towards osteoporosis.
Uh, we see decreases in the elasticity of tendons, uh, which makes them, uh, less able to adjust to kind of sudden loads and, and changes in length, which obviously can lead to a higher rate of, of strains and tears. Um, slower recovery and tissue repair, which I think anyone over the age of 40 needs, no explanation of that.
Uh, myself included. And, um, a gradual decline in the VO two max and endurance, uh, capabilities. Um, so a lot of these injuries that we see are overuse injuries, tendinopathies stress fractures. Bursitis or inflammation. Uh, related [00:43:00] changes, uh, degenerative changes, um, which, uh, the big one of course is osteoarthritis of the knee or, or other major joints.
Uh, meniscal labral tears, which is, uh, kind of a breakdown in some of the, uh, surrounding structures that, that provide cushioning to these joints and, uh, other tendinopathy changes including the rotator cuff achilles tendon. Which relates to, you know, decreases in some of the blood flow to, uh, the watershed zones of some of these tendons, uh, hamstring injuries with, uh, decreased flexibility and, and tissue resilience.
Dr. Grant Garcia: Awesome. And
Will Sanchez: I think, can I keep going? Yeah, yeah. I just wanted, so can you give us a Adam Cliff note version for things for us to, um, look out for? Right. Because you mentioned es, you mentioned the hamstring. Obviously, you know, as we get older, a lot of us don't do a good job of elasticity, stretching besides the strength training.[00:44:00]
So if there's something there that you could say, Hey, you're gonna, you're gonna go out, you're gonna play ball on the weekends, you're gonna do certain things, make sure you should be doing at least these 3, 4, 5 things. Um, Dr. Starman, I, I'll start with you. Um, in case, uh, Dr. Just not here in here. Good.
Dr. James Starman: Uh, so yeah, the things that I always emphasize are, um, the ones that I also don't like doing, which is stretching and warming up.
Um, because I think, uh, our tendency, especially, uh, when you're pressed for time, which many of us are at that point in life, is to just go out that front door and, and start moving. And, um, you know, it really makes a difference to take that extra five or 10 minutes just to warm your body up properly. Also to, you know, focus on cooling down when you're done, uh, with your activity.
Um, so I think that's, that's one that we all probably could do better with. Uh, are we
Will Sanchez: talking dynamic, A dynamic warmup?
Dr. James Starman: Yeah, I mean, uh, just static stretching and, and some dynamic warmup [00:45:00] stuff I think is both important. And, um, you know, some people, you know, do some heat on their muscles before they're, you know, getting started.
Um, and so I, I emphasize a lot with, you know, heat before activity and ice when you're done with activity, um, as a way to kind of get the blood flowing to the muscle tissue before you're asking it to perform and then to limit inflammation at the end of whatever activity you're doing.
Will Sanchez: Yeah. Uh, Dr. Winter, you know, we, you, you, um, we talked about a couple different things here, but what are some of the things that you have to be concerned about?
Because unfortunately, we don't have a cure for arthritis. Right. And we're getting older. We're still being active. You know how not yet
Dr. Grant Garcia: will, not yet.
Will Sanchez: How do we play within the constraints of having arthritis and trying to be safe, but the same time still participating and living our lives? Do you have any, any, uh.
Any recommendations there?
Dr. Bradley Winter: Yeah, I mean, the old adage is, is motion is lotion. So you get, you know, you gotta keep moving, uh, you know, you got, [00:46:00] gotta keep flexibility. Um, you know, certainly I think, I didn't hear everything Jim was saying, but, you know, warming up, cooling down, flexibility is, is gonna be important.
Uh, and I think, I think managing symptoms kind of over time, understanding what drives your symptoms. Is it, is it playing three games instead of two that's gonna gonna make you more sore and have more trouble getting around the next day? Or, um, you know, can you manage, uh, with, with icing after you play with, with periodic NSAIDs and then of, of course to the, you know, to the explosion of these new biologic treatments.
How does that help manage? Yeah. You know, some of, some of your more long-term symptoms and can you. Mitigate some of the six month, you know, return issues of cycling through injections and, and things with some of these biologic treatments. That, that I would say we don't entirely know, um, what the answer to that is, but certainly some promising, uh, some promising outlook there.
Dr. Grant Garcia: Uh. Winter, will you, will you [00:47:00] elaborate on the biologic thing? That's a really good one, and especially like how in your practice does it, you integrate it in both the non-operative as well as the operative side of things? Because I mean, today I got two people on, on non-op and two people on the op side asking about biologics.
Dr. Bradley Winter: Sure. Yeah. I think for, for my practice, I'm using it mostly in knee arthritis from a front end, non-operative side. I think that's where evidence is probably the strongest other than some tendinopathy stuff. So some tennis elbow. Um, and this is, are
Dr. Grant Garcia: you talking mostly about PRP or other biologics? Yeah. Yeah.
Dr. Bradley Winter: PRP for me is pretty much all I'm doing at this point. Um, but, but. Managing, managing knee arthritis symptoms and folks who are either not at the point where they need a knee replacement or ready for a knee replacement or, or want to do activities that the folks who do knee replacements are telling 'em they shouldn't do.
Um, and are trying to find other ways to, you know, keep playing basketball and, and whatever else. Um. And, and I think we've had a pretty good success with that. It certainly isn't a perfect science and not everyone gets as much relief as we'd [00:48:00] hope, but it is another, another option that we have, another tool that we have to manage some of the symptoms to keep people playing, to keep people exercising and, and doing the things they enjoy.
And I think. You know, as, as we have those discussions with, with patients, really trying to understand what is it that they want to get back to and, and how can we help maintain their level of independence and, and ideas about exercise that are, are keeping them either healthy or active or, or enjoying the, the activities that they're doing so they're not coming home hurting and, you know, trying to manage their symptoms for the next six days so they can play basketball on Saturday again.
Dr. Grant Garcia: hundred percent. Uh, Dr. Starman, will you chime in? Oh, sorry. Will keep going.
Will Sanchez: No, I'm, I'm asking the same question. Go ahead.
Dr. Grant Garcia: Yeah. Dr. Starman, chime in on yours. What biologic options do you think about, or anything, some of the sports stuff as well?
Dr. James Starman: I'm pretty similar to Brad in the sense that, um, you know, I, I'm mostly just PRP and, and in fairly limited amounts, uh, for my population.
The biggest barrier is [00:49:00] cost, um, and, and lack of insurance coverage, which I think. Um, you know, unfortunately that kinda limits, uh, for a lot of my patients who can get that treatment. Um, but I agree with Brad. I see that as an option for people with mild arthritis and certain tendinopathies, but, uh, not a whole lot beyond that, that I'm recommending that for, uh, for most of my patients.
Um, and I think, uh, you know, to Brad's point about, um, trying to understand the goals of your patients with respect to, you know, maintaining that aging athlete in, in whatever sport they're participating in, some of that is coaching them on how to participate differently in a sport that they've done for a long time.
And, you know, the example that comes to mind for me is with skiing. You know, as a downhill skier, you know, I've done plenty of moguls in my day and, and as I age and get a little bit older and you realize how hard that is on your knees, I think, you know, looking for other ways you can still enjoy and participate by maybe doing some of the different runs that maybe don't have quite the same level of, uh, intensity and, and still getting the enjoyment outta that.
So I think [00:50:00] having those conversations and trying to help understand what, um, you know, a specific person's goals are for participating and. Trying to guide that conversation, guide that thought process for them to help them, you know, discover what they can do and, and do with enjoyment is, is important to have that.
Dr. Grant Garcia: I think probably we'll bounce on both of you guys, but uh, maybe I'll start Dr. Winter. Do you guys have anything you guys to do? I mean, at the beginning of the show we talked about one of the companies we work with, but they talk, we talk a lot about, but we've had people on here for nutrition, sleep. Other active recovery options.
Is that something you guys ever think about, uh, in your practice, or do you ever, I mean the nutrition now is hot, like you could see it everywhere online and people talking about it. Do you have any thoughts on that or what are your thoughts on that sort of future of that stuff?
Dr. Bradley Winter: We don't have, we don't have a really robust, uh, program to, to walk patients through post-surgical nutrition and, and supplements and things.
I mean, that, that's a question we get all the time is what supplements gonna take that are gonna help me heal faster, you know? You [00:51:00] know. What do you think about, insert your favorite supplement that is, you know, new on social media of the, the last one I BP
Dr. Grant Garcia: 1 57 literally every week.
Dr. Bradley Winter: Yeah. Yeah. That's the hot one right now, I think for sure.
But, uh. It, it morphs over time. I mean, two years ago it was CB, D, now it's, you know, BP 1 57. Yep. Yeah. Who knows what it'll be six months or a year from now. But, uh, yeah, trying to keep up with that, trying to understand, you know, what does it look like to, to coach people through eating, eating the right foods.
So, you know, eating clean. Healthy foods, healthy fresh greens, you know, lean proteins during, you know, during healing and post-surgical phases and, and then managing other symptoms like, you know, use, we use magnesium a lot for folks who can't sleep, um, from shoulder pain after shoulder surgery. Studies that show it can be helpful.
Um, and just how do we, how do we coach them through that without having. A dietician on staff are really a lot of formal training and, and [00:52:00] dietary, you know, kind of questions. Um, so learning as we go, I think, I guess is my, my take.
Dr. James Starman: And I would, I would echo that and, and also say that, um, I think it's important to make sure patients understand what is, um, what is being promoted on some of these social media nutritional supplements.
Um, I know one I just saw in the news recently had to do with a lot of these protein supplements that were found to have high levels of lead. And, and you know, obviously that's not something anybody wants to put in their body if they know about it. Um, but I think people don't always understand that stuff.
That's not, uh, regulated by the FDA. You really just don't exactly know what you're getting with any of these products. And so it really truly is buyer beware, which I think some people are comfortable with that and other people maybe aren't. But I think it's important that we educate our patients on those risks.
Dr. Grant Garcia: Dr. Star and conversation's challenging sometimes. I mean, when we've had nutritionists on there, certain thi certain things we can't talk about on the show from a perspective of doctor, because [00:53:00] it's not really considered something you should be having a conversation with as a medical, with a medical professional.
So it's important. You're right, like on social media, you can say whatever you want, but it doesn't mean it's accurate.
Will Sanchez: Yeah. I was just gonna chime in. Uh, you know, we're, we're talking about all the different things. What about, um, specifically what, is there wearable technology or anything like that, that you're recommending, uh, perhaps with a patient, whether it's post-surgery or anything like that?
Is it something that you guys do in your office with that, you know, kind of biotech and things like that?
Dr. Bradley Winter: I wouldn't say I have a lot of experience with patients, but one of my sons wears one, uh, for soccer that we monitor his load, uh, based on how much he's training, how many practices he's got, how many games he's got on the weekend.
Um, and we're watching how many miles he's running. We're we're looking. He likes to look at his top speed. Which I tell 'em it's not that fast, but, uh,
Dr. Grant Garcia: classic kid. Classic
Dr. Bradley Winter: kid,
Dr. Grant Garcia: that's okay. Yeah,
Dr. Bradley Winter: [00:54:00] exactly. But, uh, I, I mean, I think it, it does give you a lot of information. I think especially in folks who have muscle injuries.
It, it probably is a valuable tool to understand how much load you're, you're putting on those folks. You know, people with hamstring injuries, um, quad injuries, that you're, you're trying to ramp them back up slowly without overwhelming, um, overwhelming the system.
Dr. Grant Garcia: I wanna chime in real for Starman. I had a patient today you'd like the second order.
He said he had his ring, his aura ring, and he says, I know I need my rotator cuff fixed. 'cause I woke up 12 times last night. That was what he told me was the indication for the surgery. He hadn't gotten the MRI back. He's like, I have had woke up 12 times. 'cause my ring told me was he right? I need to have.
Yes, he was right. But that nonetheless, it doesn't matter. Sorry, Dr. Tarman, keep going. You just answer that question for us please.
Dr. James Starman: Uh, yeah, I mean, I, I, I don't really have a whole lot more to add to what Brad, um, you know, said on that one. I'm not really using that routinely in my patients, but I, I do think it's a very interesting technology and I think it's.
Kind of fascinating as a spectator, uh, at the, uh, professional level to see some of [00:55:00] the, you know, monitoring from a performance standpoint. Then all the mountain of data that's able to be collected on these athletes at the really elite levels and, and how they're able to apply that back to improve performance and, and probably also to drive some of the, the training.
Dr. Grant Garcia: Um, so as we always do, we are very close to running outta time. Maybe will, I know you always have fun questions, but I wanted to ask one more for each of you. Go ahead. Uh, maybe since Dr. Starman started, what do you think kind of the, you know, both sports, so what do you think the future of stuff that you like is going?
Dr. James Starman: Yeah, so as far as, uh, sports medicine, I think to me the most exciting thing that's coming down the road. Uh, is, is kind of related to personalized medicine and, and what, uh, artificial intelligence may influence in that realm. So, I know AI is kind of like a hot topic in all realms of life at the moment, but I think as it relates to sports medicine, the, the potential upsides of being able to [00:56:00] integrate the vast amounts of research data that have now been generated.
Um, and to kind of integrate that in a way that we can benefit individual patients. Um, really AI is I think one of the more exciting options that we can use to achieve that. And I think that we need to, um, you know, kind of do our best to, to find ways to integrate that technology and to how we practice and to not see it as a threat.
To, you know, what we do and, and to see it more as an opportunity. But I think that that's really the only reliable way that we could potentially integrate all of the, the data that's been generated with research over the last 20, 30 plus years in this, uh, in this realm in a way that can become useful for individual patients and, and for us as clinicians to make those decisions about treatment and, and rehab and, and specific surgical techniques for specific patients.
Dr. Grant Garcia: Awesome. Dr. Winter, how about you? Yeah,
Dr. Bradley Winter: I think Grant you brought up, uh, you know, navigated surgery and patient specific, uh, uh, imaging integrating into [00:57:00] surgery. I think there's a. There's a huge opportunity there, especially with wearable devices like glasses and things that you may be able to wear during surgery that could reference imaging.
And, and can you overlay that to like real life anatomy, um, and, and actually see the imaging overlying what you're looking at in surgery, that that could be revolutionary in terms of really getting patients specific to like the millimeter detail. Which in theory should, should give us really, really good anatomic outcomes, um, from surgeries.
Um, I think the other is the ability to put a camera on a needle at this point and potentially start to do even less invasive operations, maybe even requiring less significant anesthetics, you know, could that, could that push us to even more, more rapid outcomes. And then combine that with the biologics.
Can we get even faster healing? Can we get more [00:58:00] rapid in-growth of implants and grafts and, and faster biologic healing so that we can rehab folks even faster and get them back quicker?
Dr. Grant Garcia: I love it. That's great. Excellent.
Will Sanchez: All right, let's, uh, let's wrap it up. You know, we, uh, that's a great, great way to end the show.
Um, really excited, especially as a patient to hear that you're gonna cut me less and find ways to kind of advance technology and embrace an ai. Um. For, I, I'm always, uh, I'm always wondering how a pick guy that went to Virginia is now in Tar Hill country. I don't know how that all works out and how the fandom does with all the colleges, but I'm pretty sure that it all gets worked out Big thanks to Dr.Starman and Dr. Winter from Ortho Carolina for joining us. Thank you so much. Dr. Garcia, um, any last words as we say goodbye?
Dr. Grant Garcia: No, thank you guys. It was great. We, this is our first two guests out of time. You guys did awesome. It was, I really appreciate it. So thank you. Thank you. [00:59:00]
Dr. Bradley Winter: Yeah. Thanks for having us.
Will Sanchez: All right. Take care. Bye-bye.
Audio Transcript
Bracing Pioneer to Global Leader – Michael Mcbrayer

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, everyone, do not adjust your dials. That's our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia, Dr. Garcia. We're excited today we have Michael McBrayer here, senior VP of Global Business and Professional Relations at Say IT Invus. Are we saying it correctly here?
Dr. Grant Garcia: We see we're gonna get in trouble regardless.
Will Sanchez: It doesn't matter. I know, I know. Michael, listen, Michael's been at the forefront of innovation, em embracing in sports, uh, medicine for decades from his early work at Don Joy to his leadership role today. We're gonna bring him on in second, but first and foremost, Dr.
Garcia, how are you? [00:01:00]
Dr. Grant Garcia: I'm in a much, well, some sadness with the neighbor's diagnosis of the ACL tear. But the positives of Dart finally wins a game, and we actually look like a legitimate team. So otherwise, yes,
Will Sanchez: and we're not, we're not here to talk about neighbors. Okay. So we're gonna kind of go through all that stuff, but when we're talking about recovery, we're talking about Mike B at the Recovery Shop.
Let's give a shout out to the recovery shot. Dr. Garcia. Tell us why the Recovery Shop works for you.
Dr. Grant Garcia: So big thanks to our sponsors. You guys have seen this time and time again. Um, and as our show grows, it's been great having them as sponsors. So again, for surgeons, postoperative recovery is important.
People are always asking like, what's the next level? Like, what can I do better? And they have the opportunities to have pretty much anything you want. That's sort of something that's out there. And we may even get into that today. We're getting to see some maybe new innovative things and hear about the future of recovery.
From bracing, biologics, et cetera. I don't wanna give away too much, um, but you may see some of this, some of the recovery shop in the near future as well. So this is pretty exciting. And [00:02:00] again, you never know who we're gonna have a guest on here. This started off as a sports surgery podcast. We have had some cool requests, um, and uh, just really been excited to have some awesome guests.
And I think this one is gonna be very exciting for every.
Will Sanchez: And I, I don't, I thought Michael was gonna cancel on us es especially after the results on Sunday when the Giants, the lowly giants got a win over his chargers. Uh, he was still kind enough to come on. Let's see if he's still there. He may have left.
Michael, thank you for joining us. Thank you for being a good sport. We appreciate the win because we, we get very few wins the last five years when it comes to New York Giants, but welcome to Sports Talk. Thank you for your time.
Michael McBrayer: Well, well, thanks for having me. Uh, number one, it is really hard to be a. San Diego fan of sports.
So, you know, we just take that into, you know, into account. Now they move. So I don't even really care anymore. That's, that's okay. Um, I did, I [00:03:00] wanna let your listeners know and, uh, I really appreciate you guys letting me. Off last Monday, uh, for you. Uh, I was really sick last Monday and, and still sound a little nasally.
So, so bear with me. But, uh, I did want to thank you guys for letting me, um, get a week to get healthy and, and try to do the show. So appreciate that.
Dr. Grant Garcia: No problem. We're looking forward to having you on. This will be great for our listeners. Um, I wanted, before we jump into this, uh, I think we wanna make sure that we understand, can you explain the difference?
Obviously you can see on both sides of me, I got Don Joy or what if you, anything Orthopedic knows about John Joy, it's Don Joy. And then pronounce the name for the listeners because I know we're gonna mess it up again
Michael McBrayer: in
Dr. Grant Garcia: it's,
Michael McBrayer: yeah, so the new, the, so our. Corporate entity and how we are traded on the New York Stock Exchange.
The company is Enova Enova. And um, yeah, so we went, I'll take you guys through some history, but the public entity, [00:04:00] so we went public again, um, in April of basically two and a half years ago. So, um, but in Novus is the umbrella entity that. Like I said, it is our New York Stock Exchange way of trading our, our stock, but then the brands of DonJoy and Aircast, uh, live underneath that, uh, umbrella.
Dr. Grant Garcia: Okay. And then of those, did you tell us about kind of what you started off with, where you came from and your background there and how that kind of comes in full circle to now?
Michael McBrayer: Yeah. Thank you. So I, I can kind of tell the history of the company because I am. Part of the history of the company. I've been, um, in December, it'll be 38 years.
Congratulations that I've been with the company. Yeah. Well, I don't know if it's congratulations, but it's, um, it's been a great ride. The company DonJoy has a wonderful beginning. Um, it started in 1978, [00:05:00] so. Mark Norquist was the offensive line captain for the Philadelphia Eagles, and that picture that you're seeing there was from basically from 1978.
So he would come back to Carlsbad, California in the off season to play basketball, so was as good a football player as he was. He was a wonderful basketball player as well, and he came back with inner tube rubber on his knees and his elbows. The athletic trainer for the Philadelphia Eagles at that time was Moose Dead.
And Moose is the first individual to ever put inner tube rubber on people to warm their joints and keep, you know, keep the joint moving. Um, so when he came back to play basketball, there just happened to be another little company here in Carlsbad called Body Glove. So make your wetsuits. Um, Ken Reed, who was an attorney in town, and Mark thought that was a better material than the inner tube rubber.[00:06:00]
And we literally started cutting up wetsuits, um, to make the products make knee sleeves and elbow sleeves. They, they thought it was a good enough idea to create a company and needed to get some money to launch the company, and they leveraged their homes. So wow. New loans on their homes, and in order to get their wives to sign on the new loans, they named the company after their wives, Donna Reed and Joy Norquist.
Dr. Grant Garcia: Smart, smart Men. That was the smartest thing they could have done
Michael McBrayer: that. That's the first thing they could have done.
Oh, wills.
Maybe it's better that Will's muted. I don't know.
Will Sanchez: No, I was just saying that, you know, it's smarter them to, you know, we're gonna put the house up as collateral, but we'll name the product after you, so everything will be fine. So that must have went over quite well. But so did Moose kind of is the [00:07:00] inventor of what we know as the sleeve by him doing that back way back when.
Michael McBrayer: Correct. So they ended up creating a company called Pro. So, you know, Dr. Garcia, I don't know if you know the company Pro,
Dr. Grant Garcia: I haven't heard of the company Pro, but I'm sure it's prob Is it still, I mean, is it still around? So
Michael McBrayer: it's sold mostly to athletic trainers and to training rooms. Okay. Um, and pro and pro is still around.
Um, but the, it's just not as big as, as DonJoy.
Dr. Grant Garcia: It's
Michael McBrayer: interesting. Yeah. Well, the reason DonJoy, the original products were sold to tennis shops. So it was not orthopedically driven to begin with. In fact, they signed, uh, rod Laver to a, um, to an endorsement deal, kind of, and, and Rod Laver. It wasn't a great endorsement deal because Rod would not wear the elbow sleeve in competition.[00:08:00]
He would wear it in practice. He loved the product, but he didn't want the competitor to think they were at an advantage. So we wouldn't wear it in competition.
Dr. Grant Garcia: What, and we have that now with some other products we just interviewed. We have another podcast coming out with a product that some of the NBA players, they won't wear it during the game.
'cause of sponsorships too. Some of those things. Right, exactly. I mean, obviously braces are a different animal. Um, do you, will, can you pull that other timeline? Can you describe to us, kind of like dondre, what was the, the, you're talking about a lot about elbow. I think obviously a lot of things here are the knee braces.
Why the knee? Why? What was the kind of talk about the history again, we don't have to go too crazy on each version of that. Yeah, yeah, yeah. Why, why start with that? I mean, I can talk a lot about the knee stuff, but I think that you're obviously more important here. So,
Michael McBrayer: oh, I, not more important. It's just the fact that when these, when they were trying to sell products into the tennis shops.
At the end of a season, the tennis shops would send back the products [00:09:00] because the season's over. So like in the Northeast, right now in New York and places those tennis shops are done. And so the only reason the company took a turn towards orthopedic is that they did have some accounts that physicians were buying these sleeves.
And it was, it's like, well, why don't we sell? We don't get product back from an orthopedic surgeon. And we get all these broken packages coming back from, from tennis shops. So it, it wasn't by like, Hey, we need to be in orthopedics. It was just the fact that broken boxes were not coming back. And at this point in time in sports medicine, you had individuals like John Fagan and, you know, Dr.
Berg fell from the Cleveland Clinic and Jack Houston down in, in, in Georgia. They didn't even know what A ACL was back then. They would reference it as a trick knee. And, and it was only about this time that they started understanding what the ACL did [00:10:00] and that they, they should try to do something about that, ACL.
And that's why bracing got, got started. Um, the company actually really took off on that. Um, if, if you can see it where it says the, the super sport and ah, yeah. Yeah. I was at a point in my career where. Sports medicine was so new, and these physicians that are, are now, you know, part of the A-O-S-S-M, that's the Sports Medicine Society's Hall of Fame.
Um, they were really looking for, you know, what can we do, what can we do for these patients? What, you know, they, they want to get back to their sport. They wanna, you know, get back to the same level they were. And, and there were some pretty archaic procedures going on back then. Extra articular reconstructions and things that Dr.
Houston used to do. Um, so as, as the fortunate thing for me was the timing [00:11:00] because these people would see me, they would take time, effort, and consideration to actually teach me things and, and have me be involved in the discussion about how they were gonna try to rehabilitate these individuals. And it was a very, very open.
Conversation. Um, it, it, it's a lot more difficult to, to get into, to see you today, right? As a single individual rep. It's like, how do I go in to, you know, get to see Dr. Garcia? It's not easy. And, and it was just very fortunate at my time, and you had Dr. Curlin and Dr. Job up in Los Angeles and they were starting these fellowship programs.
Um, so there were a handful of these fellowship programs. I got to be involved in and, and meet those individuals that then created their own fellowship programs. So as you went to Rush and spent time with Dr. Cole, you know, yes. These become [00:12:00] mentors and, and people that you will engage with, you know, for the rest of your career.
And that's how my career started, just because of the engagement with these individuals looking to try to help patients.
Dr. Grant Garcia: Yeah, and we, I mean, we don't wanna jump ahead with other episodes coming up, but we're gonna talk to people like that that have been branching. It's amazing when you work with someone and we have, we get experience as fellows.
I think Will can hear this from people that I've talked to, some of my mentors you've even had on the show, right? When you show them something that you like it, it spreads like wildfire. Especially at the top places. I mean, will, I've told you this before, the job procedure is the UCL reconstruction. He invented it.
Right? He's talking about a guy that invented the Curl and Job Institute is one of the top fellowships in the country. Right. And these are the two guys curl and job. So, you know, we have, and they treated me
Michael McBrayer: like I was somebody, they, they actually welcomed me in to their clinic and, you know, and, and that's what's sports medicine physicians on [00:13:00] whole.
I may, you know, get, uh, Dr. Garcia's head a little too big. But the sports medicine's, physicians in whole in orthopedics are quite open to suggestion and quite open to saying, okay, what, what else can I do? What else can I learn from others? Whereas, and I don't, you know, I'm gonna profile some things with a broad brush.
Spine surgeons, total joint surgeons. You know, they don't have the same kind of approach to these patients. They have a hammer and nail and they're gonna use the hammer and nail. Whereas a sports medicine surgeon, you really tries to understand what that patient's trying to to do and the the approach. So I think sports medicine surgeons are.
You know the animal that you want taking care of these, these kids.
Dr. Grant Garcia: Yeah. Well, it's also, I think the point you're bringing up is important because I think will sees it on these podcasts. Like we talk about my patients. I had a patients today and I said, if you come to me in 10 years and I'm [00:14:00] doing the same surgery, you should leave my office and go to somebody else 'cause I'm not doing the right thing.
Yeah. So that's the way sports is. Like, we're always, look, we talk about this. Will and I are always looking about futuristic. We're gonna get into futuristic questions here. This timeline doesn't exist unless you try to get better and our patients expect that. I mean. As much as we talk about trying to be on the forefront.
If you're in sports and you're in a big city, like I'm in Seattle, you cannot be behind. You just won't be able to be a busy physician. And patients want that. The internet now chat, GPT, it tells you what, what you want people, patients want to hear. They come in already knowing what they want. You just gotta hope that you're in the same page as them, uh, in in these cases.
Yeah, it's just, it's just the way everything you say is accurate.
Michael McBrayer: I do find, you know, the, the lay population though. In some cases doesn't understand the specialty. I, I even get it in my company, you know, somebody goes, Hey, hey, I, I, I'm getting my shoulder done by so and so. Mm-hmm. It's like, wow. I, I don't know [00:15:00] that name.
Who, where, you know, where are they in practice? Yeah. Well he did my C'S fine. Operation and I'm gonna let him do my shoulder. I said, no, you're not.
Dr. Grant Garcia: Listen, Will's, Will's Will, is a doctor by this show. So he has his MD four. Exactly. He knows that that's, that seems unusual. Yeah.
Will Sanchez: I, I could do the spine surgery if you want, you know, if, if, if that's the case, if you're just gonna say, well, you know, you fix my toe, so now fix my neck.
So that's, uh, yeah. Why, why not? So that it sounds like it's great advice that you're telling them. Yeah. I don't think that's the correct route for you to go.
Dr. Grant Garcia: So, so I guess let's go. So we talked about some of the bracing. Sure. So can you, I know we talked about this, AO S Sm, you got selected to the circle of honor.
This is a big deal. I mean, it was on the internet. If you look up stuff, it's like the first thing comes up. It's a huge deal for any of those listeners. Aos, SM, I'm a member of it. It's got a huge membership. It's probably now. I actually would say it's better than AO s In terms of meetings, it's probably one of the top, it's probably the top sports meeting.
They work with [00:16:00] A JSM, which is one of the top papers, you know, this is, this is the creme de la creme for sports medicine. So can you explain that a little bit more to the listeners to understand what this means? Well, for you to be recognized for this?
Michael McBrayer: Yeah. Well, thank you for bringing it up and, and yes, they, A-O-S-S-M is.
I think the heartbeat of sports, it, it, it's the way that, um, again, the meetings, this is where all these physicians learn and et cetera. So to give, um, recognition to individuals that are not physicians. So that's what the circle of honor, uh, was created for. Now, they probably should have given it to the company, not to me, my, in my name personally, because, you know, sports medicine's a team sport.
And, you know, my team is my company's, so at the time it was DJO. So we probably should have given the circle of honor to DJO and I could have accepted it. Um, Michael Ti and Jim Bradley. Jim Bradley was the president in 2020. Yeah. Uh, when they came up with [00:17:00] the idea to give the awards. So they, they introduced and recognized four people in 2020.
Um, the, the four people were Ken Langone. Yeah. Stanley Drunken Miller, Reinhold Schmidlin and myself. Will you know that? That's CEO Arthrex? Yeah. Yes. And so Reinhold is the owner and operator of of Arthrex, which is a huge company. Uh, those other two names, and he himself, all three of those are billionaires.
I am not, I don't know how I missed out on that, but
Dr. Grant Garcia: I thought that came with the award. You got that
Michael McBrayer: with the award,
Dr. Grant Garcia: right? It wasn.
Michael McBrayer: Well, I'm going back to O SSM and escort then, if that's the case, we'll back you up
Will Sanchez: on
Michael McBrayer: that.
Will Sanchez: Okay. I appreciate that. You're being really humble here, but I, I think what Dr.
Garcia is like. What, what, what does it mean for you personally, professionally, for, for you to have this [00:18:00] award with this distinction that comes from the people that you've worked with for so many years? I, I mean, this is, I mean, you may not be the billionaire, but this is, this is an amazing award. So let, let's, let's, I know you're giving kudos to your team and everyone else, but just personally, what does this mean to you as far as impactful?
And, you know, you go home to the wife and going, I, I can't believe I got recognized like this.
Michael McBrayer: Yeah, that's, uh, so it wa the distinction is, is it was a very impactful piece to me. So it, like, like I said, in 2020 we did it, doing it via Zoom and, and, and Dr. Bradley, I've known chief maybe since he did his, started his fellowship.
Maybe just a Michael TI was a curl and job. Both of those are Curl and job fellows. Um, so not only do I have a personal and professional relationship. These individuals, they, we've become friends and, and friendships, [00:19:00] you know, kind of go deeper than just a, a transaction in business. And, and for, I, I, I feel that they understood what my impact has been related to helping and creating opportunities for education because the, the sports society is really dedicated to, to education.
And I've been. Very engaged in the traveling fellowship program for A-O-S-S-M. I've helped establish other traveling fellowship programs for Foot and Ankle Society, for the American Medical Society, for Sports Medicine, for Sports vt, because I know the interactions that happen with these. So a traveling fellow, there's three that are chosen, and they choose a senior individual that go to Europe.
South America or Asia, in fact, uh, the last traveling fellowship for A-O-S-S-M just got back from Asia.
Dr. Grant Garcia: Yeah.
Michael McBrayer: But these are [00:20:00] life-changing experiences and we as a company support those programs because we know what the benefit is. Um, I mentioned a name earlier, John Fagan who, um, was at Duke. Um, he's the one who came up with this idea of a traveling fellowship, uh, years ago.
And. Aircast company at the time was funding it and we made the acquisition of Aircast. And, and John was, uh, concerned whether or not we were gonna continue to fund it. And, and Dr. Fagan was a, is West Point guy. Uh, he's deceased, but he, he, he was a West Point guy. And I knew when this conversation was gonna have to be serious with Dr.
Fagan because he would call me Mc Brayer. Hmm. Says, Hey, mc Brayer. I, I need to talk to you, um, about, you know, this traveling fellowship. And I knew the, the, the conversation was gonna be casual if he called me [00:21:00] Michael. So he goes, McBrayer, Hey, what are we gonna be doing without this traveling fellowship? I said, well, you know, not only did we acquire a wonderful company called Aircast, but one of the nice pieces that added to that is that we will continue and be a part of the traveling fellowship.
And he says, Michael, that's a good idea.
Dr. Grant Garcia: I. So then see you got on this good side. See, I'm gonna call Sanchez and Garcia, or it's Will and Grant. So we'll now know how we can talk to each other differently. Now we Exactly. Mood.
Michael McBrayer: Now whether it's,
Dr. Grant Garcia: or you, you also see that that's gonna be the new hint on the podcast.
Everyone's gonna be expecting to see how, how are them, how are their, how's their mood today? Um, this is great. So can you talk? So again, one of the big things, we want to go into the larger company, but I think the DonJoy is important. Sure. Can you kind of talk about, some of you know briefly about the science, about how the bracing has shifted over the last, you know, 10, 15 years.
Again, history's great by our listeners. They obviously like cutting edge stuff, right? They're gonna want to know like, where are we going with this? The [00:22:00] orthopedic surgeons listening, they've heard your name, right? They've heard DonJoy, they know all this stuff. True. But for the listeners who are looking at these products, what, what does it, what does it mean for you guys?
How have you guys shifted your mentality for the bracing that you're doing?
Michael McBrayer: Yeah. And, and so knee bracing is just a portion of it now, right? I mean, so when early on we wanted to prove that braces were actually doing something for these ACL reconstructions. We did research at the University of Vermont and it was very cutting edge at the time.
It's been a few years ago now, but we were putting strain gauges on the intact ACL. So we did cadaver work. Initially, we were showing that we were strain relieving, getting strain off of that ACL with our brace. And then somehow we got some volunteers. To have a strain gauge put on their ACL intact ACL [00:23:00] and then put loads on their and Wow.
And show that we can Yeah, exactly. I I still, you wouldn't be able to get that IRB
Dr. Grant Garcia: approval anymore. That's impressive
Michael McBrayer: that IRB would never get approved again. Ever. And I don't know if you wanna explain what an IB is, but it's will, it means that the institution would
Dr. Grant Garcia: approve someone to put an implant in someone's knee without actually needing the surgery.
Michael McBrayer: Exactly. Um, so as a portion of how we've looked at and tried to, um, confirm that our products are doing what they say we do these pieces of research. Uh, we've also done economic studies. So like when you see the college football teams, um, we only have one division, one school that's not in our knee braces.
Um, the rest of 'em are in DonJoy and we've done some, there it is right there. And so the down linemen that are looking to be protected because they get their own player to roll up on them. Um, so they're not, these are contact [00:24:00] injuries, not non-contact injuries, uh, which a brace can be very, very effective for.
And we did a study at University of South Carolina looking at just the economics. Of, okay, you've purchased these braces. How many acls did you have, and what was the cost of that ACL? Um, it's devastating to the player. But from an economic standpoint, we, you know, we, we wanted to prove what the benefit was.
Um, it's important.
Dr. Grant Garcia: Can you tell, um, I mean, it's important Will, I think that that brings this point up. We talked about the cost of injuries. You brought it up on the last show, uh, that we just had. We've talked about it before. It's devastating. Right? And we talked about this, which we will hope, you know, I think the po.
Podcast just came out, you know, on how long does it take to get back and what is the benefit of doing these things. It's really important. As much as everyone says you don't, we don't wanna talk about the cost of something, it's, that actually is really important. Like, is it worth spending the money to get a brace?
Correct. If it's not gonna help you. Right. If it looks nice, that's great. But so for your guys' [00:25:00] bracing, you guys have looked at ACL, um, I'm assuming, you know, MCL and other ligaments is the ACL, the big one you guys are focused on. It's obviously the biggest one. We just talked about a player of ours that, uh, we're dealing with the ACL tear situation.
Mm-hmm. But the, in general, is that your major one you look at, or what other things have you guys looked at or thought about in terms of the bracelet, what you guys do from that?
Michael McBrayer: So, I'm gonna, and I'm gonna shift gears a little bit because ACL's is a big segment of our business, but when you talk about the sheer number of injuries, foot and ankle, total number of injuries is significantly higher.
The total of, you know, sprained ankles and, and et cetera, et cetera. So when you start looking at the, the total number of joints and injuries, ankle is the number one joint for some kind of injury. And, and so these same thing, whether or not we're trying to as a company in Novus is quite different than any other [00:26:00] orthopedic company because we look at the patient from trying to prevent injury.
To post injury, to operative care and postoperative care. And there's no other orthopedic company that does that. You know, the big, big companies, Stryker and Zirin and big companies like that only are working on that patient when they're asleep, um, you know, in the or. And, and so we think we have a unique approach to trying to, this what we call a continuum of care.
So any joint in the body. So foot and ankle is a huge one because we, you, you know, there was a player on the Dallas Cowboys last night. I won't name his name, but he had our walker on, he's on the sideline. Um, I noticed it probably no one else did. Um, and then you talk about, um, there's a surgeon that. Most of these ideas and things come from surgeons.
The surgeons are looking for these ways [00:27:00] of trying to take care of patients and physician up in Los Angeles, Steve Snyder, if you ever met Steve, Dr. Garcia and Steve Snyder's shoulder surgeon was the first one to start putting people in a postoperative pillow position themselves and take strain off of the, you know, the reconstruction for their, their shoulder.
And, and, and so it's what I'm most excited about this as a company and as an, and continuing to work for another 38 years or whatever it's gonna be, is the innovation that's coming from the surgeons. When they see a problem and they're not satisfied with what they're trying to, to do for that patient, they raise their hand and they, and they're, they, they reach out and say.
Hey, I have an idea, or, boy, have you guys thought about this? Um, it, it's, and, and that's gonna continue. That, that's not gonna change that, that I can see from, certainly for sports medicine surgeons.
Dr. Grant Garcia: Yeah, I mean, I think that's an important point. We've talked about this before, will, [00:28:00] but you know, the innovation is a collaborative effort, as you mentioned, right?
It's not only do we see, how do we see the problem finding the company to work with and finding the right people to work with from both parties. Right for the company's party and then finding the surgeon the best fit and then finding a problem that actually works, and then looking at the science behind it.
It's all really important. We've talked about this from the sort of, we talked about from the napkin to reality, like one of our first episodes, how you take an idea. It's a lot and it's a lot, and again. What's different though, I think which you could bring this up, is from the bracing standpoint, the innovation is still a pretty strong long period, but it's a little bit faster, right?
You don't need the same regulatory stuff as you would. That's with like a biologic or something else. So you guys can have ideas to, I mean, what would you say? This is interesting for the listeners, and actually I just think for all of us to hear, what do you think, like, let's say I came to you with a great idea, right?
And it's something that we kind of just knew you gotta test the water, see if there's any patents or other things out there. But let's say it's a good idea, it's a, it's a workable idea. What [00:29:00] is kind of the timeline for you guys to kind of put a product out like that roughly?
Michael McBrayer: So it's a great question because we, we do get the napkins occasionally of the, the napkin to, to a product.
Uh, we get, um, individuals who have. Fully blown, uh, prototypes and, and have worked on their ip, et cetera. So you have that spectrum that you, you just described. So the napkin to something could be, you know, like, like a three year project, uh, to get it all through your, our requirements. So these devices are what we call class one devices and Class one devices do not have very large hurdles.
To get over in order from an FDA standpoint? Um, yeah. So we don't have those kind of requirements that, uh, implants have, uh, for bracing. So obviously our implants for foot and ankle and our surgical total hips, total knees, total shoulders, all have those requirements. And, and those, like you said, take longer term because of some of the, those requirements.
Um, but [00:30:00] it's still an arduous mechanism to try to get something that's a manufacturable. Reproducible economic product, um, that you can launch and, and have an impact in the marketplace.
Will Sanchez: Are, are, Michael, are you, are you seeing or have you seen in the last 12 months? Six months, three months and uptick of ideas now that everyone, uh, has access to ai.
Where they can pop in ideas and that's, and come up with things. And so are you seeing anything like that futuristic that's kind of going across your table or maybe the table of others in the company?
Michael McBrayer: No, and I, so no, there hasn't been an influx of new ideas. Now we're, so AI for us as a company on the bracing side.
Mm-hmm. Mm-hmm. Um, we haven't. Really made much progress with it in the standpoint of [00:31:00] creating manufacturing product. Okay. Where the implant or the importance for AI has been for us is we, we have a software package and program that runs D-M-E-D-M-E is durable medical equipment, so all the braces and supports that are in a physician's clinic.
Are can be insurance billed. So if you went in to see Dr. Garcia and he says, you need a walking boot, or you need a, um, an elbow brace, or whatever the case is, those products have a billable code that then insurance companies will reimburse that patient for those items. But it has to be done properly. It has to be coded properly, the inventory has to be done.
So this. What we call Motion MD is this operative software system that gives information to the clinic. We run, uh, clinics for that as [00:32:00] well, but it, it's complicated business. You know, it used to be the practice of medicine. Now it's the business of medicine. Right. You can't, you used to be able to not worry about whether you build something properly or you gave product away or something and you, you just, you can't do that anymore.
So this product, what I call a product, but it's a, just a software that you can get the patient's insurance in real time. Medicare and these entities are making requirements. There's a thing called Same and similar. So if you had a product four years ago and Dr. Garcia decided that that's, he wanted to prescribe that, didn't know that that patient had already had a product similar to that, that Medicare would call that.
It's, it's pretty scary. Um, so we have the same in so we can, we can quickly check for the patient to see if they had something like that. So it's operationally we're using [00:33:00] AI from the standpoint of how we react, you know, work with a clinic and, and a group. Um, we haven't used it much in, in what I call product development yet.
Dr. Grant Garcia: I think that's a good point. Will, I think the thing you're, the thing we keep thinking about is we still think I, AI is so smart that it's, you're gonna be like, Hey, gimme the next bracing idea and we're gonna put it out. The problem is, I think right now, we talked about this on our AI in Medicine episode.
We did it a few months ago, but it really, right now it's just not smart enough. To come up with that level of whatever. And then, okay, by the way, we need to do this. It's multiple levels of steps, right? I see a problem. How do we fix the problem? What is the problem? What's realistic problem? Before you even come to a company like this to show that?
And we've already, I mean, I know this 'cause I work with a bunch of comp different companies on different product design things, and you think you have such a good idea, you spent years planning, prepping, thinking about it, and then you send it out and it's like. Yo dude, that's like, we've done that like seven times.
Like that's not the idea. [00:34:00] So, you know, and then, and then it's more like, you know, it's, I guess AI can throw more things at the window till they get the right one. But it's, it's, it's not so straightforward and the command you need for that. So I think we've, I think Will was, will, so this when we did our episode is that a lot of times this AI really is just how does it make your things more efficient and not make mistakes?
And within insurance companies, how do we, how do we improve our efficiency to get our things approved and make sure we follow all the rules. Really, no one here is here for any fraud or any other attempts in medicine. All we wanna do is make sure the patients get what they want, and our barrier is insurance and we need to make sure we do that appropriately so.
But they make it complicated. Oh yeah. I know. I have a lot of You have the best
Michael McBrayer: intentions. Yeah, so the intentions are not, you know, I agree with you. Nobody's sitting out there going, Hey, I wonder how much I can get out of an insurance company. You're just trying to follow. Stay on the road, keep on the guardrails.
And, and go about your business and that's what this software can [00:35:00] do.
Dr. Grant Garcia: Can you talk about, uh, some of the, I guess this is important. There's two parts. I think the first part is has is three. We've talked about 3D. We're gonna talk about 3D printing I think in the near future. Yeah. For an episode. It may come actually out before this episode, but we have to see.
But how is 3D printing is any part of that part of your scale or where you guys are going in the future?
Michael McBrayer: So we're, we made a, um, recent acquisition, uh, Lima, uh, which is a surgical, uh, company in, in Italy. Um, they, we actually house a 3D printing segment at HSS in New York City. Uh, but it's for surgical implants.
Um, our experience for 3D printing on the bracing side has been. That it's a very expensive mechanism to create something that we make with different materials already. So, um, so far the expense of 3D printing has [00:36:00] not allowed us to, to do it On the bracing side, it, we are as, as I said, working with it, uh, as a surgical implant product.
Dr. Grant Garcia: Cool. Yeah, that's a great segue. That's perfect. Um, on, so go bracing. I kind of wanna get into the major company itself too in a second. Mm-hmm. Um, but I really want to know the, we talked about the surgeons. Do you guys ever, how do you guys work with, like, you know, you have the athlete, right? You have that initial start, right?
The guy wore the sleeve, doesn't wanna show it in the games 'cause he doesn't wanna have his things. And now it's all about branding. I mean, we've talked to a few companies, which we, we will, we can go into later. But that have said that, you know, like they have a lot of trouble. Some of the athletes wanting to, I mean in the NFL and those things sometimes we're embracing, you can't, right?
You just don't Correct. You can't wear the elbow brace. You can't in some cases.
Michael McBrayer: W
Dr. Grant Garcia: have you, what barriers have you had from, for athletic adoption of these braces? If it was allowed? So like, you know, we saw Thibodaux, uh, for the Giants, he wears an elbow brace, like that's allowed, right? So there's certain things that are allowed, certain things, but they don't have the [00:37:00] brand on.
Michael McBrayer: Okay, got it. So, so that's important. So no branding. So the, so the equipment manager, at least in the NFL world mm-hmm. Is responsible for what they call uniform infractions. Yep. And we get away with a couple. I'm not gonna tell you how, um, no, I'm kidding. The, but they, they're serious. I mean, like, if the quarterback when he goes to the sideline doesn't wear the right hat, the NFL says, you didn't wear the right hat.
Um, all of our braces, so they're, you're not supposed to show the DonJoy brand 'cause we put it on the calf cuff of a brace, knee brace. Uh, we have these wrist wraps that a lot of players wear and has DonJoy on it. You know, they'll typically tape over that so that, uh, the NFL is very, the no fun league, if you wanna call it.
Um, they're very critical because there are. They know if we [00:38:00] wanted to get a sponsorship from them of, and, and we can, we could approach the NFL and say, Hey, we, we want to be the knee brace of the NFL and it costs an a significant amount of money and we just don't see, the patients are not making a choice.
They're following their doctor's orders. So it's not like they're going to the store trying to find a DonJoy knee brace. Um, so we haven't done anything like that from a, what I would call a commercial standpoint, except I would, and the NFL is very, would,
Dr. Grant Garcia: I would second to you on that one. I do have patients asking for a DonJoy, even though it is not good a, uh, but you know what I mean?
People ask for these braces will, I don't know if you've ever heard the name, but people ask for, I want, I, and I'm not, I don't wanna bring up your competitors, but I have, you know, they ask about the competitors and they just say, I want this. Predator. I'm like, but you don't even know what that means.
They're like, I've heard the name, so I want the DonJoy. But there's like you, you guys have probably, I mean, how many different braces do you think you have even for the knee? [00:39:00]
Michael McBrayer: Oh my gosh,
Dr. Grant Garcia: too many, quite honestly. So when someone asks for a DonJoy, they don't really know what they're asking for. They're, they have like no idea, I want a car, I want a Mercedes, Jordan's.
Michael McBrayer: Well, because we have osteo arthritic knee braces, we have patella femoral knee braces, we have, so all these, in fact, Dr. Cole actually helped us with a, uh, our OA Rome brace. Um, so yeah, you're right. They have no idea what they're talking about.
Dr. Grant Garcia: Yeah. Um, so I want to pivot, even though I love the bracing, we could always come back to it, but we also have a, in a matter of time, we, we have to, we always do this, but at 60 minutes we have to cut it off 'cause it's just 'cause of the way social media.
Oh. I'll be tired of you guys
Michael McBrayer: by then
Dr. Grant Garcia: for sure. I'm tired of you guys right now. So can you talk about the other companies you guys work with? Uh, yeah, because I think, I think the biologic one is gonna be hot. Like what companies do you have from the biologic standpoint and how does that influence, you know, the other sports medicine realms?
Michael McBrayer: So we, we haven't entered the biologic, uh, [00:40:00] space yet. So the, the areas of, um, of the company that we haven't, um, if you want to call it musculoskeletal care, um, we. We don't have anything surgical in spine. We don't have what you would reference surgical sports medicine. So those are big, big segments for, in Novus to, to consider, to try to enter as a market because they're, they're large, they're growing.
Um, our largest, uh, growing segment is our foot and ankle surgical business, and we put that together through acquisitions. Multiple acquisitions now has made that a hundred million dollars, uh, surgical foot and ankle business. And, and I, I, I, I profiled sports medicine surgeons as the, the darlings, you know, foot and ankle surgeons are good people too.
They, they, they kind of have the same profile of, of approach to patients and such. [00:41:00] Um, our total joint business. Total hips, total knees, and total shoulders is very, very small in comparison to the large competitors. Uh, where we do compete quite well is in, uh, the total shoulders. Mm-hmm. Reverse total shoulders being the, the probably the biggest, uh, competitive piece that we have.
Um, and, and, and a. A surgical intervention that's, that's quite successful. Right. I How do you find that integrates
Dr. Grant Garcia: well with the bracing side of things? Like, I mean, again, the comp, the company's got multiple brands to it. Right. You guys have talked about, you know, you do, I wanna talk about this electrotherapy, some of the other equipment stuff you do on side of the braces, uh, in a minute.
Um, but how does your abil, how does your company having reconstructive implants. You know, for hips, knee, and obviously biggest is shoulder. I've heard about the shoulder for sure, and a lot of the other ones. But in Nova, uh, NVU, uh, for the shoulder is important. How does that help integrate with the protein?
How does that make you guys better?
Michael McBrayer: Yeah, so again, we're, if we take [00:42:00] this continuum of care approach, so you may or may not be fa familiar with the No Pain Act.
Dr. Grant Garcia: I ha It's a little bit, I mean, I think I get too many emails about it, and I, I can't imagine that I, I'm not gonna say I read 'em all. Yeah. But I So you explain that
Will Sanchez: because I, I, I'm not aware of that.
Yeah. So, so,
Michael McBrayer: so the, the No Paying Act was a recent act and, and by the congress and Senate to pass to include mechanisms for reducing opioid use, postoperative care. So they were looking for, um, products that would be, um, use that would reduce opioid use and be safe and effective. Well, cold therapy, motorized, cold therapy has been, and a very, very effective product.
And there, there used to be a billing code. You guys are wonderful with the yard. A little [00:43:00] flash up there. Good job. Um, but cold therapy had a code that people were billing, but it was abusive. They, they were billing it improperly. And so Medicare just stopped reimbursement for cold therapy 20 years ago. Uh, even though it's a very, very effective mechanism for postoperative pain.
So through the No Pain Act. Uh, we've been going through a comment period. We're supposed to hear quite soon whether or not, uh, this iceman device is going to be approved by Medicare to be reimbursed. So, Dr. Dia, when you were saying, you know, how does it, how does this happen now? Okay, I have a total shoulder surgeon or have a, a total knee surgeon, so.
Now we say, even though they're two different entities, the divisions are different, but we can introduce the cold therapy now to take care of this opioid issue and pain relief as one entity, right? [00:44:00] We're gonna come to you and say, Hey, we know you use our shoulder. This No Pain Act now gives us an opportunity to take care of your patient with a reimbursed cold therapy device.
That's important point. And so that's where's important point connection
Will Sanchez: can come. Gotcha. Thank you. And
Dr. Grant Garcia: also, I think the thing you bring up was like, like a lot of you said, we keep talking about these cold therapies. They're not covered by insurance because it, it's just, even though, even though I will tell you, and you know this and we don't need to go into different products that we use, but the cold therapy situation, it, it, it makes a huge difference.
I will tell you that, that it's not just anecdotal. It is, I, I, I don't know enough about the data on cold therapy and I wish I did. Um, but I can't imagine, I think will, will say the same, that cold therapy is not, does not reduce opioid use. It's just, I mean, I'm sure it does, but I'm just, I can't believe there's not more things.
The problem you have obviously with all these studies, postoperative pain is that, you know. All surgeries eventually stop hurting, hopefully, if they're done well, and it doesn't usually take that long, so it's hard to [00:45:00] capture that data. Right. Like two or three days left. Pain.
Michael McBrayer: Well, pain studies period are difficult to do.
Uh, yes. The one study that we, um, that was recently done, I don't know if you know the name, Sarah Edwards. University I do not of California, of San Francisco, so, oh, okay. Look, look for her recent, uh, research that, um, we think her paper was the thing that crossed the barrier from Medicare to get it reimbursed.
So that study was, was paramount to, to our approach in getting, um, getting it, getting it approved.
Will Sanchez: W was that a postsurgery study?
Michael McBrayer: A post-surgery postsurgery recovery, yeah. Post
Will Sanchez: study.
Michael McBrayer: So it's, um, so Sarah Edwards, like I said, is at the University of California San Francisco. The paper, I'm trying to remember where it, so she's presented already and it's been accepted in one of the journals.
I don't know if [00:46:00] it's the Anna Journal, but it, you'll find it. Yeah, I can. I mean, again, the key here is just abstract. We wanna
Dr. Grant Garcia: show, you know, we want to show, basically the key is for patients to hear. This is like, it does make a difference. Opioid reduced reduction is very important. It's now tied to insurance reimbursements.
Uh, and again, hopefully it's just, again, hopefully it all, it all comes down the same line. Can you, um, talk about now do you have any, like, how, how does this sort of, I know you, I'm again, I I have the list of the brand portfolios that you guys work with. Yeah. And I'm interested in each one of these things.
How does the re rehab, so you, you can talk about this, you have all the lines, right? You have the surgery, you have the pre-surgery, you have the post-surgery, you have going towards potential long-term. Biologics, things like that. How do you, how does the electrotherapy and the rehab sort of side of things help with your stuff?
I mean, I, I kind of know where it's going, but what are your thoughts? Yeah. Like how does that go?
Michael McBrayer: So, some of the recent, um, product [00:47:00] enhancement, so we, laser therapy Yes. And shockwave therapy, both, um, are very effective and. Can take care of tendinopathies. So when, when patients come to you, um, with a tendinopathy issue, so like, you know, the, the Achilles flaring up, not a tear, right?
Uh, tennis elbow, you know, golfer's, elbow, whatever. All these littleon issues are non-operative issues for an orthopedic surgeon, and you don't want a lot of those people coming into your office because. You're a surgeon and you want to do surgery. Um, so I'm not gonna deny you, I'm
Dr. Grant Garcia: not gonna deny you. I,
Michael McBrayer: I, you're called a surgeon for a reason.
Um, but the, what I, I mentioned the American Medical Society for Sports Medicine. These are fellowship trained primary care. You know, sports trained individuals [00:48:00] and so they can take care of non-operative issues in using laser, using shockwave and mechanisms for these patients to, again, get back to, to the level of what they were trying to do without a, uh, you know, getting cut on, so to speak.
Um, so that whole spectrum for primary care sports as well as physical therapists, sports, physical therapists. You know, the, the, the, the PT networks and, and you know, there's a, again, the specialty of sports, physical therapists, um, that know how to take care of these patients, um, again, potentially non-operatively.
And then, you know, I. Every good orthopedic surgeon has their favorite physical therapist to take care of their patient after they do an an operation as well.
Dr. Grant Garcia: Yeah. Well, I, I think that's great. I think that, that, I don't wanna segue too much in that will, but that obviously the laser therapy and the shockwave therapy is humongous.
It's humongous for tendinopathies, but also the [00:49:00] laser for postoperative, which a lot of there. But also as an orthopedic surgeon, you're entrepreneurial business-minded. A lot of us, I'm private practice, so you always look at how a way to keep the patients to make sure you have every level for them to take care of it.
So, you know, a lot of people use the laser therapy preoperatively and also sometimes postoperatively for wounds, et cetera, and pain control. And there's been recent some AO s data on that, which we won't go into too much, uh, today, but that's a really important part you brought up. So again, you see, sorry, you keep going.
Michael McBrayer: No, I was just gonna say, and those, those types of, uh, procedures are un unfortunately today at least, that those are things you have to talk to the patient about paying cash for.
Dr. Grant Garcia: But, so as we know in this day and age, there are patients that want to pay that, which we've talked about before. Absolutely.
And the thing is, I would rather my patient be offered at a cash option than nothing. So at this point, it's not like I always tell that to the patients. I think Will, this is obviously a topic we talk about. We've talked [00:50:00] about it with the recovery shop I brought up. Yeah. A lot of things aren't covered by insurance, but patients want more.
I know I'd be in the same boat. I know a lot of us would be in the same boat. We all know that. Like if we want, as much as the surgery is covered by insurance and it's a huge financial burden and it covers. You don't want a problem with it. And so sometimes the, the little extra things to reduce those things are a big deal and people are willing to do it, especially if it's not covered by insurance.
Again, my whole goal as we talk about before and you talk about this, is get as much as you can from the insurance company to approve and if you want something extra, here are the options. Here are the risks and benefits. And again, the goal is to make it, you're not gonna break the, you don't wanna break the bank.
You just want to offer something that's you think is gonna be helpful to them. And we all know that insurance is 10 years behind what we're doing, if not more, in terms of the options that they can give to patients. It's just, I mean, sports medicine, we know this all the time. I have this on a daily basis with, talked about recently the fertilized ACL right?
Insurance won't pay for it, but there's good data on it. And we just talked about it with Chad Lavender. So [00:51:00] it, this is important, uh, stuff to talk about. I don't want to, well I think it's belabor
Michael McBrayer: it. Well, I think it's, I, I reference it now as the consumerism of medicine. So now an educated consumer can make a choice about their care.
Um, and, you know, in the past I've just, well, my insurance is gonna take care of it. I'm so, so having an intelligent choice and having them be a consumer of this kinds of things, I think is, is good for, for everybody.
Dr. Grant Garcia: I think one more question then we'll do kind of a wrap up future question. Do you guys deal with, oh boy, pediatric p No.
It's hopefully easy for you 'cause you've, you've done this for so long, you know this, so the PIA pediatric bracing, do you guys deal with that and is that a different level of what you have to, is it anything different for you or is it just part of the same envelope?
Michael McBrayer: Yeah, so we've been treating it in the same envelope and we [00:52:00] shouldn't, um, pediatric, um, injuries and, and pediatric patients are not small adults.
They're, they're, they're different. And, and we, we as a company need to make an effort related to changing our thoughts and, and how we approach these, um, injuries in these types of patients. Um, the pediatric sports medicine specialist. Is, is now a thing. You, you have organizations that are strictly, uh, focused on pediatric sports medicine, pna, um, as an organization.
So, you know, people are doing a sports fellowship and then doing a specific pediatric sports fellowship. And, and so the, the number of these individuals is growing. So the fact that that specialty is growing, we as a company have to. Listen and start approaching these patients differently than what we, and then just making an extra, extra small, that's, [00:53:00] that's not gonna get the job done.
Dr. Grant Garcia: I brought this up before on the show and Will knows this, but we've, we've come along in sports medicine, which is whether you wanna say it's good or bad, but we've had become more aggressive with pediatric patients because it used to be the thing like, dislocate your patella as many times as you want, you're fine dislocate your knee as much as you want, your fine dislocate your shoulder.
And I mean, there are a number of papers coming out that. Even first dislocation is not okay. Correct. Second dislocation agree is not okay. And so as a result, this is a really important point because that's why you have more surgeries, more people being involved in pediatric. 'cause we realize that if I can, that's the whole point of joint preservation.
Like I just saw a 16-year-old girl today dislocated her kneecap and broke off piece of cartilage. It's like, ugh. Some people might have just left it alone for another 10 years and waited till she had a lot of pain, but we're gonna actually take care of it because I know that that's not gonna be good.
10 years. I know that's not gonna be good in 20 years if we don't intervene. And we've learned that. Yeah, I agree. Right. It's the same situation. I completely agree. Is what you're talking about. Uh, [00:54:00] the, I guess we'll probably ask any closing questions, but where do you see the kind of, I know the company itself, where do you see the future of DonJoy going and where do you see the future of the company going
Michael McBrayer: and the, the future I, I, I referenced earlier is, is that these physicians are gonna continue to make us.
Change and do things. So that collaboration, um, which we have a, a reasonable reputation that people approach us because we have a, uh, we've done things with surgeons and, and reputable surgeons, and people know that we will at least listen and try to do some things. It may not turn into a product, but the innovation and needs for, uh oh.
Did you guys leave?
Will Sanchez: No, we're still here.
Michael McBrayer: We hear you. Oh, good. We are here. My, my screen just went blank. Um, I think when you look, you still look good. You
Dr. Grant Garcia: got it going. Keep going. Sorry.
Michael McBrayer: The collaboration between [00:55:00] surgeons who are gonna want to try to continue to take care of their patients and companies, not just a ovu, um, is still the most exciting thing for me to, to, to be involved in.
Will Sanchez: Awesome. Michael. Uh, thank you so much for your candor and really, uh, honest answers. I, I mean, it, it was, uh, it was a privilege hearing about your journey, the vision for the future. Uh, not only the company but sports medicine and, um, it is just, uh, we really appreciate your time. We're glad you're feeling better.
Uh, tell Christina I hope her, uh, dolphins are doing well from all of us. And, um, once again, thank you so much for your time. We'll, we'll let you go. I know it's laid out there on the East coast.
Michael McBrayer: Oh no. I'm in California, brother. I'm all good. Oh, sorry, Christina, go to
Will Sanchez: bed. It's late for Christina.
Michael McBrayer: Thank you so much.
Hey guys, I enjoyed it. It was, it was, it was a nice experience. I appreciate your time. Thank you, Michael. Thank you. Take care.
Bye.
Audio Transcript
A Deep Dive into Cartilage Innovation with Dr. Brian Cole
Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon in sports medicine specialist. That man right there, Dr. Grant Garcia, Dr. Garcia, exciting. We have a new show. We have a great guest, but first and foremost, how are you?
Dr. Grant Garcia: I'm good. It still sunny for another day or two where summer's just stretching on in Seattle, so I can't complain.
Uh, unfortunately the giants are back to being terrible, which we don't have to talk about today. But the Seattle teams are doing well decently, so that's good. Mariners won. So we're excited about that. I guess.
Will Sanchez: Yes. Let's not bring up, why are we starting off the show with the Giants? Dr. Garcia? Man, you, you know,
Dr. Grant Garcia: it's always
Will Sanchez: we need
Dr. Grant Garcia: something.
Will Sanchez: Not doing this.
Dr. Grant Garcia: We had one game. We had [00:01:00] one game.
Will Sanchez: Oh my Lord. All right, man. Let's get to people that really care about us, 'cause obviously you are just trying to break my heart. Let's talk about the good folks at the Recovery Shop. The shout out to contact Mike b. Talk about the recovery shot and why you love them.
And our guests as well loves them as well.
Dr. Grant Garcia: Great. Yeah, so we, we like them because honestly, patients ask for a little bit extra sometimes, and it's challenging as a surgeon, you send them to, you know, Amazon or online to look for their stuff. So the option of having this for the patients is really nice. Uh, and the patients do appreciate it too because it's all kind of there together.
And you have the nice machine, which Dr. We, I think just tried out one of the new elbow devices, uh, which is really nice for patients. That's really a, a niche that many of the companies can't provide. Uh, so they've been really happy with them and I think the patients are really happy, which is more important.
Dr. Wayne Weil : Mm-hmm.
Dr. Grant Garcia: Uh, so if you're a surgeon, reach out to them. If you're a patient, you don't have that option, reach out to them. They can try to get your surgeon set up with it so that you can have that opportunity.
Will Sanchez: Let's get right to our guests [00:02:00] because we're keeping him from getting dinner, and that's a tease for something that we'll talk about later on.
Um, let's bring in the doctor, the hand, the wrist and elbow specialist himself. Dr. Wayne Wild. Dr. Wild, thank you for being on. Thank you for hanging with us and I apologize for Dr. Garcia bringing up things to start off the show in a negative way. How are you?
Dr. Wayne Weil : Uh, doing great. Uh, happy to be here. Thanks for the invitation.
Dr. Grant Garcia: Yes. Uh, so for the viewers introduced Dr. Al. He's a hand surgeon, actually, he's my partner. And we do a lot of cases together. Complex, uh, elbow surgeries. Um, and he specializes in hand, uh, wrist, um, and elbow and then dabbles with trauma as needed, uh, but really super specialized in the hand and nerve, uh, surgeries.
Also, chief of orthopedics at the Swedish Hospital system. And board of directors. So he is got extensive title and Pro Alliance as well as Pelto and he actually does family stuff as well on top of all that huge list. [00:03:00] So pretty impressive. Well, thanks for coming on. Really appreciate it. I'm sure Will's gonna have lots of questions to ask too.
Um, for the viewers, do you think you can kind of give a quick background? You know, I know you came from New York. Talk about your stuff and you know, now you're in Seattle, so just give us a little update and into who you are and where you came from.
Dr. Wayne Weil : Sure. Uh, yeah, I'm an East Coast guy originally, uh, grew up, uh, outside, uh, Bethesda, Maryland.
Uh, ended up, uh, uh, doing my, uh, college in Philadelphia and then, uh, resident med school and residency in New York City. Uh, then ended up out here, uh, for a hand surgery fellowship. Uh. And just kind of fell in love with the Pacific Northwest. And one of our other partners, uh, Dr. Shapiro, uh, who's a shoulder specialist here, uh, I knew him from New York, from, he was a fellow while I was a resident, and he ended up recruiting me to stay out here.
And, uh, now 21 years later, I'm, I'm [00:04:00] still here in Seattle. Uh, we now have five kids. As Dr. Garcia mentioned, uh, I've gotten involved in, uh, sort of, uh, non-practice stuff, uh, with, uh, being chief at, uh, Swedish and the board positions at Proliance. And, and then I've still, uh, at my, uh, practice where, uh, you know, I really enjoy just treating, uh, elbow, wrist, and hand and, uh.
I do a lot of that, whether it's uh, you know, sports injuries and, and younger folks or, or degenerative stuff and older people, arthritis, uh, stuff. So kind of do a little bit of everything, uh, except maybe sleeping, which, uh, I would like, but that's okay.
Will Sanchez: Dr. Uh, what can you tell us what first sparked your interest in hand in, in microvascular surgery, you know, how do you go along that [00:05:00] path and have that interest?
Dr. Wayne Weil : Yeah, so that really started in, in my, uh, fourth year of, uh, residency, um, as part of our residency program at NYU and Hospital for Joint Diseases. Uh, we do, uh, a four month rotation down in Baltimore at, at, uh, shock Trauma Hospital down in Baltimore. Um, and at the time, uh, there's a surgeon there, uh, Andy Seder.
Um, and, uh, Dr. Seder, uh, to this day, I think is the, the best surgeon I've ever seen operate. Just, uh, you know, I think, you know, for, for lack of a better, uh, descriptor, you know, gift from God in terms of, uh, he could do anything and it was always perfect. And, uh, so he really got me interested in, in microsurgery and, um.
Uh, kind of the rest is history from there. [00:06:00] Uh, so, so it's, I think, you know, in a lot of our lives, uh, you know, just exposure to, to, uh, a good mentor really can pave the way moving forward in terms of, uh, uh, really career paths in general. And, uh, yeah, I think, uh, Dr. Seder is really the, the, the person who who got me interested in, in, in what I'm doing today.
And then, um, you know, fast forward a couple years, uh. Doug Hanno, um, at, at University of Washington, who I did my hand surgery fellowship. Uh, another just phenomenal surgeon. Um, and, uh, you know, uh, Doug in, in a very similar way with Dr. Eder, you know, could fix anything and, and just an incredible surgeon and, and so, you know, like having the exposure to those two docs in particular. You know, I, I, [00:07:00] I stand on the shoulder of giants, uh, and, um, you know, I, I, I certainly give a lot of credit to those two guys for, for getting me to where I am today.
Dr. Grant Garcia: Uh, Wayne, I wanted, I wanna bring this up. I, because I think that's probably your answer is gonna be this too, but. You know, we see in the office, we talk about, I do a lot, you know, we talk about the sports surgeries that I do, but I see you doing a lot of really complex hand and wrist surgeries that not everybody would want to take on, even as a hand surgeon.
Do you think, and I don't wanna put too many words in your mouth, you think that stems from that background you're talking about? Or why do that? Like you could, your private practice, you could just do carpal tunnels. Yeah, procedures. You don't have to do the hard stuff. Why do you choose to?
Dr. Wayne Weil : Uh, you know, uh, maybe I'm just a masochist.
Uh, but I think that's true of kinda all the guys in our practice. I mean, we could all just do the simple stuff, but, uh, I think [00:08:00] we all enjoy the challenge. Um, you know. For me personally, if, yeah, I enjoy doing carpal tunnel surgery, but you know, uh, I would get bored if I just did that all day long. And, and, you know, for me, uh, maybe I'm blessed with the ability to do the hard stuff.
Uh, and, and I enjoy doing it. And, and I think that serves a, a niche for our patients. Uh. In terms of, you know, we, we see a lot of patients in our practice and, and, and you do, uh, as well, where, you know, they've bounced around to different docs in the community and, and just, uh, for whatever reason, you know, I haven't been able to, to get the care that they need.
And, and so for me it's, it's very gratifying to, to see a patient who's maybe seen a few docs, uh. And, uh, [00:09:00] has been told, you know, uh, we can't help you. You gotta live like this for the rest of your life or whatever it is. And, and to be able to see them and say, actually that's not true, uh, that we can help you and I can make you better.
Um, and, and I think. You know, that's why we went into medicine is, is to make people better. And, uh, um, you know, it's very gratifying. I think the, the more complicated a, a problem is in a lot of ways, it, it's even more gratifying to, to get to the other side where, where you've made somebody better. Like, um, so, and, and again, I think, you know, going back to the training, um.
Both at Shock Trauma in Baltimore, both at Harborview. I mean, we saw the craziest stuff you could ever imagine, you know, horrible injuries, uh, you know, whether it's, you know, explosives or industrial [00:10:00] injuries or, or what have you. And, you know, those two guys in particular, handle and Eder, they were just, you know, always so calm, always had a plan and, and able to execute it.
And I think having that kind of exposure where, where you've seen, you know, everything. Um, so when somebody walks in the door with something complicated, uh, you know, you, you, you rely on your b on your training and then your experience, you know, I've been doing this now for 21 years, been in practice. Uh, so I feel like, you know, there's not much out there that I haven't seen.
Uh, and so. That, that makes me prepared to, to take on the complicated stuff.
Dr. Grant Garcia: Awesome. Um, do you, so I know we talked about this, but the, obviously we might switch gears a little bit. Yeah. But the, coming from the complicated to maybe the more minimally invasive stuff that you do, I know you're, [00:11:00] you know, we know you're one of the only surgeons in the area that does this sort of endoscopic carpal tunnel, endoscopic cubital tunnel.
Will you talk a little bit about those procedures? The audience. And then what is the benefit, in your opinion, of doing it this way? I mean, it's also more challenging technically, but obviously what's the benefit to the patient? Why would you do that versus the standard open?
Dr. Wayne Weil : Yeah. Well, I mean, uh, the name of the game in, I think all of surgery is, you know, being less invasive, less destructive to the tissues.
Um, and, and that really. Um, you know, helps on the backend in terms of there's less stuff to heal. Right? Um, again, going back to my residency, you'll, you'll appreciate this story. Um, I was a third year resident and, uh, uh, scrubbed a case with a doctor, uh, who was, he was the only one in the NYU system still doing open [00:12:00] acls and.
And I done it. I'm shivering
Dr. Grant Garcia: by the way.
Dr. Wayne Weil : I'm
Dr. Grant Garcia: shaking. I'm having like,
Dr. Wayne Weil : you've probably never even seen one. Uh, so, um, and, and this is now circa 2003. So at this point, uh, or 2000, 2001. Uh, at this point, you know, uh, arthroscopic ACL surgery was a standard thing. I mean, it's not like, uh, it was brand new. People have been doing arthroscopic ACLS for 15, 20 years probably at the, at that point.
Um, and so yeah, so I scrubbed this case with this guy who's doing open ACL and, you know, the whole knee's filet open and, and. I couldn't believe what I was seeing. I, and I can't imagine what the recovery from that was. Uh, and having had an ACL done on, on my own knee, arthroscopic [00:13:00] ACL, I mean, it's, you know, worlds apart.
And so that experience in particular was like, well. Why would I ever do something that that was that traumatic, uh, if I can do it in a way that's, you know, not nearly, uh, as, as destructive to the surrounding tissues. Um, and so, you know, in residency actually, uh, we started doing, uh, endoscopic carpal tunnel releases.
And again, uh, smaller incision, less tissue invasion. And we'd have patients who, you know, had an open on one side and then came back and had the endoscopic on the other side, and they were like. The, every single one of those patients couldn't believe how much easier the, uh, the recovery was with the [00:14:00] endoscopic.
Just less pain, quicker return to work, better function. And, um, you know, the data has kind of borne that out, uh, when you look at the recovery. Um, again, just less pain, quicker return to bur and, uh, better grip strength in, in the first three months of recovery. Um, the opens end up catching up in the end and they do fine.
And, you know, at, at nine months, one year, everyone's the, the same. But why have an operation that takes you nine months to recover from when you can have the same operation, but it only takes you, you know, three months. Uh, and so similar to, to the, uh, ulnar nerve, uh, the cubital tunnel. Decompression the ulnar nerve.
Um, same idea, uh, is, you know, little incision. We do everything from the inside out instead of the outside in. And so, uh, again, you don't have to cut through any of the [00:15:00] muscles to get to where you wanna be. Um, and that just decreases the amount of time for recovery and, and, and gets people going a lot faster.
Um, and I think that's really. The exciting part in orthopedics, uh, where we're moving towards in general is, um, all the stuff we do is becoming less and less invasive. Uh, you look at a hip replacement, you know, you were in the hospital for a week when I was a resident. Now we do hip replacements, and you go home the same day.
Um. Same with, you know, knee replacements, uh, you know, a lot of the, the cartilage stuff that you're doing. Um, all of it is, is really starting to become outpatient surgery. I mean, even spine surgery is moving to, to outpatient surgery. Uh. And, and you look at the results, people do better when they're [00:16:00] home, uh, versus sitting in the hospital.
You know, you take the same operation, same person, your risk for infections and, and, and worse outcomes are higher if you stay in the hospital than if you go home. Um. So, uh, I think all of orthopedics, and especially in my specialty, you know, trying to do things in, in a minimally invasive way, it just, it just makes sense and it's better for the patients.
Um. In a lot of ways it's more fun for the surgeon 'cause uh, we get to play with cool, uh, new instruments. High
Dr. Grant Garcia: priority. That's the high priority there.
Dr. Wayne Weil : That's right. Um, you know, it's fun to go to the lab and kind of innovate and, and, and work with, uh, some of the, uh, companies to, you know, come up with, uh, you know, novel ways to do things.
Um, so, uh, I think it's sort of a win-win all the way around.
Dr. Grant Garcia: Will, can you pull up that slide? [00:17:00] Um, on the nano? I don't want to see, 'cause we're talking about, we're in the perfect example. Segue. Go to the next slide here. Lemme just do it.
Will Sanchez: Yeah, I have, I have, well,
Dr. Grant Garcia: yeah, Wayne right
Will Sanchez: there.
Dr. Grant Garcia: Yeah. So this is a, this is good.
You, I mean, we don't have to do the proprietary discussion here. I just was a picture, 'cause I know you've used this before. So for your minimally invasive situation, I mean, what would you use. Something small like this for, right. Yeah. Like the idea behind patients are always curious like, well how, how small can you go?
I've seen you scope some pretty small joints, right? Something I would never consider doing. So what are your uses of this and like how do you help, what does it help you with?
Dr. Wayne Weil : So, uh, yeah, we've gotten to the point now where, uh, you know, the instruments, uh, have gotten small enough where, you know, in the old days you could basically do a shoulder, uh, and a knee, and, and we've now, you know, uh, gotten to where we [00:18:00] can basically scope.
Pretty much any joint in the body for the most part. Uh, uh, you can scope out to even, uh, the PIP joint, um, proximal interphalangeal joint in the finger. Um, you can, uh, scope, you know, the base of the thumb. That's probably the most common one that I, I do now. Um, 'cause the base of the thumb, the carpal metacarpal joint, that's the one that, uh.
Becomes, uh, classically arthritic. And so, uh, there's, uh, procedures now that we can, uh, do kind of like in the knee where we do, uh, for arthritis, uh, some clean out procedures. So the instruments, not only the camera, but also, um, the different little shavers and the probes and instruments that we use, uh, are small enough that they fit in there.
Uh, so you can really do kind of what the large joint [00:19:00] arthroscopists do. Uh, you know, the stuff that you do in the knee and the shoulder grant. Now, now I can do, uh, to some degree in, uh, the base of the thumb and, and in the wrist. Um, and so we're, we're definitely catching up, I would say, to to the large joint, uh, uh, arthroscopists.
And a lot of it just has to do with. The ability to, to make the instruments smaller and smaller. It's kind of like our, uh, computers and our iPhones and everything else in the world. Yeah. Um, you know, the first iteration is, is big and, and then, uh, as we get, uh, better with manufacturing and, and the technology, it just.
You get smaller and smaller and smaller, so then we can start really having a good time, uh, with the, the small joint instrument, uh, small joint arthroscopy.
Dr. Grant Garcia: Would you say with this, I mean, when I first saw you do one of those thumbs, I was like, this [00:20:00] is crazy. This is cool. Uh, would you describe, like, what were you like for that patient?
You know, you, when you do the metacarpal, when you do the scope of the thumb
Dr. Wayne Weil : Yeah.
Dr. Grant Garcia: For some arthritis. Yeah. What were you doing before for them? Right. Because these are patients, they're not, they're not old enough for you. Sure. Or any other thing. So what were you doing before? Were you, or just is this at a new surgery for you?
Dr. Wayne Weil : Yeah. So, you know, uh, I think of it like arrows in, in, in your quiver, right? And, and so. Um, you've got only a certain amount of, uh, arrows in, in the quiver. And, and if you can have more arrows, that's awesome. So, uh, for those patients, you know, that was like your, your 40 and 50 year olds with, uh, early stage degenerative arthritis.
Uh, they've had, you know, splints and braces, but nobody likes those. 'cause uh, you need your thumb to actually live life and do things. And so if you lock up your thumb. You know, it's pretty miserable. You can't [00:21:00] really do much at all. You can't type on a computer, you can't hold an iPhone. Um, you know, you can't garden or play tennis or whatever it is.
Um, so people don't tend to wear 'em 'cause they're, they really inhibit your activities. Um, so you, you know, the, the braces were sorta, yeah, you can wear a brace, but nobody likes that. Uh, then there's occupational therapy. Um. You know, to some degree, some patients find it helpful, but it's not really solving any of the issues, uh, internally.
Um, then we move on to steroid injections and sometimes those can be helpful. Um, PRP injections, sometimes those can be helpful, and then you're kind of stuck after that. There's not really any non-operative treatments that, that are reasonable to do. And then operatively, then we start talking about joint replacement, uh, which, you know, it's a big step for a [00:22:00] 40-year-old to, to undergo.
And so now we're able to do a, uh, procedure that can, uh, potentially buy people some time. Uh, and put off, you know, the eventuality of a joint replacement by ideally 10, 20 years when it's more appropriate to do the joint replacement as opposed to when they're 40 or 50. So, so it's really opened up a whole new, uh, ability to treat patients.
'cause otherwise it was, well you're 45 years old and we've tried everything. So either live with it or, or have a joint replacement. Whereas now I can say, well, you, you've, we've tried all the non-op stuff. We can, uh, now think about doing an arthroscopy and kind of clean stuff up for you. And, and ideally we'll buy you another 10, 20 years and then you have your joint replacement, you know, when you're 60 or 70.
Um, so it is been fantastic in, in being [00:23:00] able to, you know, treat patients, uh, uh, in a, in a much better way, uh, as opposed to just telling them well live with it.
Will Sanchez: I had a question for you. Um, talk about common hand and wrist injuries, uh, whether it's the pro and recreational athletes, and what's your thoughts on some of these names, like the skier's thumb?
Yeah. Or the jersey finger. You're from the East coast? I don't think the Jersey finger is what I'm thinking of. Ain't
Dr. Wayne Weil : the Jersey Shore,
Will Sanchez: it's not the Jersey Shore. So can you talk about that a little bit? Because the names are absolutely fantastic and Jersey finger means a thing on the East coast.
Dr. Wayne Weil : Yeah, no, it's, uh, so, you know, the hand world, uh, ends up with lots of crazy EPIs and uh.
As Grant knows, you know, people, uh, call us the hand weenies, uh, 'cause kind of the, the, it's the reputation of the hand. Surgeons are kind of the nerdy guys who, uh, [00:24:00] are way into minutia and. You know, uh, Dr. Gel Seder used to always say, you know, the leg is just a stupid weight-bearing joint, right? You can cut a leg off and put a piece of wood and give someone a peg leg and they can walk.
Um, but the hand, you know, that's a whole nother kettle of fish, right? You take somebody's hand off and, and they're really debilitated. Um, so, um. Yeah, the hand world. We've got all kinds of names for crazy stuff. Uh, you know, skiers thumb, uh, which actually was a gamekeeper's thumb in the old days. Uh, and not 'cause you're, you're playing games, but, uh, keeping game like small games, small animals.
So, uh. You know, uh, the farmers would be, uh, the classic is snapping the necks of rabbits, uh, with their hand and over time. Story
Dr. Grant Garcia: is crazy.
Dr. Wayne Weil : The ligament, uh, of the, uh, the [00:25:00] ulnar collateral ligament of the thumb would, would basically just tear. From overuse in all the years of snapping rabbits. Next. So Dr. Grant Garcia: we'll pull that slide up.
Pull the, not the rabbits. We don't have a rabbits.
Will Sanchez: We don't have the dead rabbits. No, no.
Dr. Grant Garcia: Hold the thumb. Uc. Pull the thumb UCL up while he continues. Keep going Wade.
Dr. Wayne Weil : So, so, you know, fast forward a couple of centuries and, uh. You know, skier's thumb or mountain biker's, thumb, you know, if you can imagine you're holding a ski pole and uh, you fall, your thumb's kind of exposed out there and it gets wrenched back and, and it gets torn, uh, the ligament gets torn.
Or if you're mountain biking, uh, same idea. Your thumb's kind of exposed and you go over the handlebar and kind of superman out and your thumb gets yanked back. Uh, so it, it ends up tearing, uh, the ulnar collateral ligament, um, [00:26:00] which is the, the kind of, i I tell people that's the ACL of the thumb, right? So if you tear your, your ulnar collateral ligament, what it ends up happening is, is.
You can use your thumb and you can move it. And once it's the, you're, you're, uh, recovered from the acute injury, but the, the cartilage is going to, uh, be stressed in a way that it was not built to be stressed, uh, as the thumb kind of pivots abnormally when your power pinching and grasping. And so, you know, the reason to repair the thumb, UCL.
Kind of like the ACL is in a large ways is to prevent arthritis, uh, from happening, uh, in a pretty short, uh, amount of time with the cartilage damage that occurs with, you know, in the knee we call it pivoting. Where, where you have these moments where, where the femur and the tibia kind of shift on each other.
Same thing [00:27:00] in the thumb. So, so the goal and when we repair these is, is to restore that stability, uh, to the joint so that the, uh, cartilage, uh, doesn't have that or abnormal stress on it. And, and so folks can have, you know, a good joint, uh, moving forward. Um. You know, it looks like here we've got this, uh, slide with the internal brace, which, uh, that's been, you know, in talking about sort of minimally invasive surgery and innovation in, in, in surgery.
There's been a real game changer for us, uh, in the hand. Um, and, and really what it does is it, it allows folks to, to start their rehab basically, you know, the day after surgery in large part. So in particular with thumb, uh, ulnar collateral, ligament repairs, uh, in the past, before doing internal braces. Um, we [00:28:00] would put people in a cast for six weeks.
I, oh, sorry guys. Um, and after, uh, after being in the cast for six weeks, they'd come out and they, they'd be really stiff and then, you know, it takes another six, eight weeks to get them moving. Then once we got them moving, then we'd add in strengthening. So, so the whole rehab process was, was probably more like four to six months.
Whereas now with the internal brace, um, we, uh, we can basically, um, get people moving. I get people moving about five days after surgery. Uh, so. My protocol now is, um, a post-op splint.
They see the hand therapist at day five. Uh, splint comes off. They get a removable brace and they start, uh, working on range of motion, uh, so [00:29:00] that by basically six weeks they have their full range motion.
Uh, and we've already started working on some strengthening. So, um, the total rehab program is, uh, basically three months before back to normal. So it, it's, it's shortened their total rehab time by about 50%, um, which is awesome.
Dr. Grant Garcia: Yeah. And we've seen some crazy ones, right? You know, there's Joe, your, I know one of your friends is one of the guys that.
Proponents of it, kind of taught it to many and to a lot of the pro athletes. Uh, somebody trained with
Dr. Wayne Weil : Yeah, yeah. Lots of, lots of pro athletes now get the internal brace and, um, you know, that's kind of the way things evolve, right? Is uh, you know, the, the pros get, uh, the stuff first and then it kind of trickles down.
But, uh, at this point, uh, I, I wouldn't. Necessarily even think about doing the, the surgery without an internal brace. [00:30:00] 'cause I just, again, it's like an open, uh, an open ACL versus arthroscopic ACL or an open carpal tunnel versus endoscopic, you know, people just get better faster. And, and, you know, in our patient population here in Seattle, um, you know, people don't wanna spend, you know.
Months at a time, either outta work or not kayaking, or not skiing or mountain biking or doing, you know, the things that they'd love to do. Um,
Dr. Grant Garcia: and for the listeners too. Oh, so I was gonna say the listeners too. It's also important that it's now that we'll stand line, right? So people are looking this up, they're already coming to you.
We're in a tech heavy market, so it's not like, you know, open ACL in New York is different animal. In Seattle, you wouldn't even see a patient in the office. They wouldn't show up to your office knowing that you do open acls. I mean, and this is, we can say Mike Trout, Bryce Harper. These are some names that done.
I did. We actually worked with Curtis Anderson when he had his UCL, [00:31:00] uh, Terry. You have Drew Brees. I mean, it's pretty extensive. The list is pretty impressive. Yeah. How people have had this surgery done. So sorry. We'll keep going.
Will Sanchez: No, no, I was gonna follow up on that. You know, uh, we're talking about pro athletes and we know that they kind of en endeavor this, uh, pain threshold.
What are some of the ramifications if you have a pro athlete or a quarterback or a golfer that puts off surgery when they need it, waiting for the off season or something like that? What, what are some of the repercussions or some of the concerns when you have, uh, a high profile athlete that really needs surgery?
Dr. Wayne Weil : Yeah. You know, that, that, that's a, that's a great question. And, and sort of that intersection of medicine, sports business, uh, you start really having different forces at play, right? In an ideal world, you know, somebody has a torn ligament, you know, you get 'em in, you fix 'em. Uh, they rehab. [00:32:00] But, uh, you know, with, with these, uh, high
performance athletes who, you know, getting paid, you know, millions of dollars to, to play, um, and these are all, you know, super competitive people too.
They, they want to play, they, they don't want to just kind of ride the bench and, and, and miss out on a season. Um, so not only are they super. Um, uh, competitive and want to, to, to be out there. Um, but the, you know, the teams want them out there. The agents want them out there. Uh, so you definitely have to navigate those forces.
Uh, you know, when you're treating, uh, a professional athlete or, or a high level college, uh, athlete. Um. You know, as a physician, I, I always just, you know, uh, kinda, um, uh, harp back to [00:33:00] you gotta do what's right for the patient. And, and so, you know, I tell my patients, look, you can play, uh, you can grin and bear it, but there, there may be serious consequences, you know, down the road, uh, when we.
You know, ultimately fix it. If there's, you know, been further damage, um, I might not be able to make you as good as you once were. 'cause you've damaged that joint to, to a point where now it's, it's, it's, you know, a salvage operation versus an operation where, where you're gonna be, you know, basically normal again.
So you may play this year, but you may not play, you know, for the rest of your career. Um. So, you know, and, and some of this has to do with just timing of things, right? So, you know, beginning of the season versus end of the season teams, you know, in the playoffs, not in the playoffs. Uh, [00:34:00] so, you know, you, you gotta kind of juggle all those, uh, factors.
Uh, but at the end of the day, I think, uh, as a doc, you know, my job is to educate my patients. Um, and it is a, you know, ultimately it's, it's their decision. Um, you know, patient autonomy is important. Uh, and I feel really strongly that, you know, if I give somebody all the information, uh, that they need to make a, a decision that's, that's good for them, then I'm okay with whatever they, they decide.
Um, but, uh, I'm not gonna sugarcoat it. I'm not gonna tell them. Oh yeah, you can delay and you'll be fine. You know? Yeah. I tell them, I tell 'em the truth.
Dr. Grant Garcia: Yeah.
Will Sanchez: Gotcha.
Dr. Grant Garcia: Uh, with that, uh, I want to go back and I appreciate all your insights on these. We talked about scoping, but the risk scope stuff that you do, especially with the TFCC and some of the ligament stuff, like what sort of newer stuff you [00:35:00] talk about the wrist arthroscopy a little bit.
I mean, that's the stuff that. The minimally invasive stuff that you're doing now, you're adding more things, right? You're doing different things you weren't able to do before with the scope. Yeah. Like what do you, what new stuff are you doing with the risk scope then why is that beneficial to patients?
Dr. Wayne Weil : So, so yeah, with the risk, the arthroscopy and especially the the TFCC, which stands for triangular fibro cartilage complex. That's why we call it TFCC 'cause. Is pain in the ass to say, but, uh, so, uh, and that's a pretty common injury from a fall and, and people think of it, ah, it's just a wrist sprain. It'll get better, but.
People, uh, oftentimes will end up, uh, with sort of chronic, uh, ulnar sided wrist pain, which is kind of the pinky side of the wrist, and oftentimes that that's due to, uh, this tear of the TFCC, which, uh, again, I like to use the knee as, uh, uh. Uh, an example for folks. 'cause everybody's heard of the meniscus of the [00:36:00] knee.
Uh, the, the TFCC is kind of similar in that it's the shock absorber, uh, for the ulnar side of the wrist and helps with some stability of the wrist. Uh, and so, uh, now that again, we've gotten sort of minimization of the instruments, uh, and the anchors. Um, we can start really, uh, doing much, uh, better, uh, repairs of the TFCC as opposed to just cutting it out.
So, uh. You know, like Dr. Garcia does in the knee in terms of repairing the meniscus versus chopping it out. Uh, our ability now to, to do repairs is, is much, much better than even five years ago where, um, you know, we were doing repairs but they were not so easy to do. And the default was always, you know, just cut the min, cut the TFCC out, um, which certainly helps with pain relief, but you [00:37:00] know, it's always better to repair something than chop it out if you can.
Um, so that's really been one of the big innovations in terms of, uh, uh, wrist arthroscopy, uh, and um, then also on, on the ligament side. Um, working, uh, to, to get some better, uh, repairs, uh, of those ligaments. Arthroscopically, uh, is, is certainly in the works, um, to, to work on instability issues, uh, in the wrist.
Arthroscopically. And then, uh, you know, starting Wayne,
Dr. Grant Garcia: would that be, would that be like, uh, people that have unstable ligaments, like they, or they tear like a mechanism that keeps, will you describe that briefly for the patient? Dr. Wayne Weil : Yeah, so, so like, uh, potentially, uh, STA four ate ligament, uh, repairs, uh, done arthroscopically, uh, again, uh, the SL ligament, uh, very similar, uh, to, uh, ACL in the knee.
This is. You know, we have the [00:38:00] ACL of the thumb, that's the ulnar collateral ligament. And then we have the ACL of the, uh, wrist. That's the scavo lunate ligament. Um, and so, yeah, well they can
Dr. Grant Garcia: internally brace those. Do you internally brace those? Ev don't get well, too excited. Try.
Dr. Wayne Weil : We're getting there. Uh, so, so yeah, that's sort of the next iteration of things is, is, uh, doing those, uh, repairs, uh, arthroscopically instead of open.
Um, and, uh, then also, uh, maybe doing some cartilage work as well. Um, and, and just really being able to, um, minimize, uh, all our surgeries that we're doing open. So, uh, we are, uh, definitely pushing the envelope all the time. Um, in terms of what, what we can do
Dr. Grant Garcia: when you do those scap illuminate ligaments, can you.
Can you do like an arthroscopic assisted, like that's sometimes what I do for some of my surgeries. Like you could see 'em go back together. So you don't have to do x-ray. You really can see 'em touching with the [00:39:00]
Dr. Wayne Weil : thought process. Yeah. So that's, that's, I think, uh, you know, kind of the, the, the spot that we're in now is, is arthroscopic assisted.
Um, really just kind of helps, uh, see, you know, where you are with the, uh, joint surfaces, um, and, and when you're closing them down. And then you can even stress, uh, the, the joint and really see that, you know, the, the ligament that you fixed. Um. Uh, is stable. Uh, and, and you can see, just see it much better than an x-ray.
Right? Uh, you're looking directly at it with the scope, uh, versus, uh, with an x-ray. You know, you're just kind of interpreting, you know, the, the shape of the bones and how they're relating, but you're, it's, it's better to see it directly.
Dr. Grant Garcia: Yeah. And for the listeners you're talking about. The ankle. A lot of people with ankle fractures, you see the, nowadays, all these newer surgeons like Dr.
Yee, we talk about, or Dr. Reed. Yeah. [00:40:00] They're scoping the, they're scoping the ankle with the fracture of the ankle. Right. So they're making sure that the cartilage is not too damaged. Or when the knee, when we have a tibial plateau fracture, sometimes we do an arthroscopic to see how well we line the surfaces up.
'cause as you said, x-ray's only so good. Plus it reduces x-ray time, which is always better for. The patients and for the surgeon not having to get fluoroscopy all the time.
Dr. Wayne Weil : Yeah. So, so one of the things that, that you mentioned, yeah. I think in, in fracture work, uh, arthroscopic assisted is, is, is awesome.
Like I, I will, uh, for wrist fractures just to raise fractures, uh, I'll put the scope in at the end. Uh, sometimes, uh, if I'm concerned about the, uh, articular surface, the joint surface to, to just make sure that all the little. Uh, surfaces are, are well lined up. 'cause you know, with fractures, the, the biggest thing is, is getting that joint surface smooth again.
You don't wanna leave the joint surface with the giant pothole in it. 'cause, because that's where, when people end up with, [00:41:00] you know, post-traumatic arthritic problems is, is 'cause the joint surface wasn't, uh, fixed properly.
Dr. Grant Garcia: I think that's an excellent point 'cause it's always hard to see sometimes on these, and you're dealing with even smaller bones.
So for the listeners to hear that like. If you've got some issue, you know, that's something you talk to your surgeon about, right? Like arthroscopic assisted is is the, the new gold standard.
You know, not in every case, but in those challenging cases it's, it's important factor to have in order to preserve the joint, which is really where you're going.
It's going joint preservation. I do knee joint, sometimes shoulder joint, and you do hand and wrist joint preservation and so that's a key point preservation. 'cause we don't want to be fusing and replacing, its. Not nearly as much fun too, right?
Dr. Wayne Weil : That's
Dr. Grant Garcia: right. So, uh, will you, were about to jump on something.
You had a question?
Will Sanchez: Yeah, no, just a quick question. Uh, regarding, you know, anyone that's listening that's either a patient or just, uh, nothing personal. I really don't want to come see you because I have a broken hand or wrist. Right. So is there any hand [00:42:00] exercises or stretches or anything that. That's been documented to kind of maybe reduce the risk.
Obviously if there's trauma, that's something else, like falling off a mountain, grabbing and twisting your arm back. Yeah. Are there exercises or, or stretches that you can utilize to unfortunately not go see you?
Dr. Wayne Weil : Yeah. Yeah. Great question. So, uh. In terms of, uh, you know, I think just holistic view of, you know, our bodies in general.
Um, you know, there's clear data that just, um, you know, use is good. Uh, sitting around on the couch doing nothing. That's bad for you. Right? So, so being active and, um, that I think is number one, the biggest, uh, benefit to, to longevity in general. So, you know, if you look at sort of those blue zone studies, you, you know, people who live on, [00:43:00] uh, hilly areas.
Live longer. Why? Because they have to walk up and down hills all day long 'cause they're getting exercise. So, so same thing with hands. Uh, and I think that's, you know, true of any joint in our body is, is using it, staying, um, flexible, uh, working on your flexibility, uh, working on your strength. Um, and, and ideally you, you know, I think there's not, I would say one specific exercise that's awesome for you, you know, working on your grip strength, and if you lead an active lifestyle, you know your hands will be exercised.
Uh, you know, it's the folks that, you know, sit around on, on the couch watching TV all day. Those are the ones that I worry about a lot more. Got you.
Will Sanchez: Thank you.
Dr. Grant Garcia: Let's, we wanna, in the sake of time, make sure Wayne has, can get outta here. Eventually meet the traffic. The, uh, but one other, I want one other talk [00:44:00] topic to talk about really quickly and then a little bit of fun, and then we can get you outta here.
Will you, okay. I know Mike Trout had this recently. I've seen you deal with some of the baseball players
Dr. Wayne Weil : Yeah.
Dr. Grant Garcia: On Merc round teams, et cetera. This one happens a lot. We hear this a lot. And this idea of removing the hook of handmaid or doing something, can you describe it to. What's the most common person athlete you see with this?
And then how, what's the kind of treatment regimen you normally deal with?
Dr. Wayne Weil : Yeah, no, these are, uh, this is a great, uh, uh, photo. Actually. I just saw a patient today, uh, with this injury, um, the most common baseball players. Um, and it's an interesting injury. In that you would expect it's a blunt force trauma, but it, it typically happens on a, on a swing and a miss.
Uh, so where, where they strike out, um, and it's the rotation of the bat, uh, through the follow through when, uh, the, the hook of the handmade [00:45:00] fractures, uh. And so, um, the hook of the Hamid, as you can see here, acts, uh, a little bit, uh, like a pulley, uh, on that, uh, small finger flexor tendon. Um, and it, it has a reputation for, for not healing.
Um, the blood supply to there is not great. And so, um. The, the treatment for this typically is just you excise that portion, uh, that's, uh, where that arrow is pointing. So, so the top part or, or the hook. Uh, as opposed to the body of the hamate. And then you kind of smooth out the, the fracture zone. Um, 'cause you don't want the flexor tendon, uh, a braided by the, um, the, the bone, uh, that's been fractured to kind acts, uh, almost like a [00:46:00] saw on the, uh, on the flexor tendon.
So, so you smooth out that fracture and. And it is an operation that, uh, works really well in terms of, uh, relieving pain, uh, and getting people back, uh, uh, to, to playing baseball. Golfers can get it as well. Um, and then, um, the other sort of cohort of folks who, who, uh, break their, uh, hook of the hammit, uh, are people who kind of use their hand like a hammer.
And are are banging on, on their hand. Uh, uh, you know, there's a, a board in your porch that's a little bit up and so you, you know, you smack the, the board down with your hand and you can injure your handmaid that way. Um, but uh, yeah, it's, it is interesting. It's an interesting injury. 'cause, 'cause you'd think it was more of a blunt force injury or, or, you know, when, when, in baseball, when.
And the batter connects with, [00:47:00] with the ball, but it's, it's actually when they strike out, when it happens,
Will Sanchez: is it the hand, is it the bottom handle of the bat that's rounded, that's coming through on the follow through and grabbing that part of the hand? Is that what
Dr. Wayne Weil : some of that also is just the force transmissions, you know, as the hands are turning over and you've got this giant lever arm, which is the bat.
Will Sanchez: Yeah.
Dr. Wayne Weil : Uh, and it just torques the, the hand just in a perfect way to, to break off the, uh, hammit, um, really common in, in actually, uh, pro baseball players. Uh, um, we, we see it kinda, uh, pretty regularly.
Will Sanchez: And you don't see it with golfers.
Dr. Wayne Weil : Yeah. You see it with golfers too. Okay. Uh, usually with golfers it's more they hit, you know, a really fat shot and their club gets stuck.
In the ground and then their hands kind of rotate over it. Um, but, but [00:48:00] it's a gratifying injury to treat 'cause uh, you know, you just take out the hook of the handmaid and, and people get back really quickly. So, yeah. Um,
Will Sanchez: that's interesting.
Dr. Grant Garcia: Awesome.
Dr. Wayne Weil : Yeah.
Dr. Grant Garcia: Uh, so I guess since you know, you're well known for all your hand surgeries.
But actually what the viewers don't, may or may not know if they're doctors or patients listening to this, you actually are more popularly known for something else. So as of now, you are now famous for other things. So I'd like to show the viewers and maybe a better understand and hear the background story behind this.
Dr. Wayne Weil : So lonely. That's, yeah. This is, uh, this is my, uh, new, uh, sky gig,
Dr. Grant Garcia: and he's [00:49:00] smiling the whole time positive. Amazing. Well pull, pull
Dr. Wayne Weil : up his
Dr. Grant Garcia: followers,
Dr. Wayne Weil : director in the background. Smile.
Dr. Grant Garcia: That's pretty impressive.
I think it went up since we started the show. When I told you how many followers you had, it literally went up between this entire show recording 'cause Will just changed it.
Dr. Wayne Weil : Yeah, it's uh, it's gotten kind of crazy. We, um, yeah, this is, uh, something that's just kinda come out of the blue for us. It was kind of a joke.
Uh. Started actually December 1st, last year after Thanksgiving. Um, we, uh, my wife is, uh, used to be a private chef, so she's a, she's an awesome cook. [00:50:00] And, uh, and all our friends, uh, and family know that she's amazing. She should open up a restaurant. Um, but, uh, her classic, classic Thanksgiving is. To die for and, and it's our family favorite.
My wife was actually born on Thanksgiving, so it's kind of a big deal for, for our family. And she does this really traditional Thanksgiving with, you know, giant Turkey. Usually it's like a 28, 30 pound Turkey and, uh, with, you know, four different pies and all the sides you could ever want. You know, it's a massive undertaking. And so this year she's like. We're not doing Thanksgiving. I'm tired of it. And
Will Sanchez: what
Dr. Wayne Weil : everyone, we were so depressed. 'cause it literally, our whole family looks forward to it every year. It's like, I wanna make a Turin. Uh, so, um, for those of you who are, uh, [00:51:00] John Madden fans, back in the old day, if you look up some of the videos of John Madden in, in New Orleans, uh, this comes back to, uh, the Turin.
Um mm-hmm. So a Turin is a, is basically it's a Turkey and a uh, uh, a chicken and a duck all stuffed, uh, inside the, the Turkey. And so, um, my wife asked me to learn how to deone the Turkey and chicken and duck and then, uh. Um, so I, you know, watched a couple videos on how to do it and so we, we made this tur Duckin, um, and uh, at the end you, you basically, you sew the Turkey back, uh, together.
So it looks kind of like a Turkey again. Uh, and it's stuffed with the stuffing and the chicken and the, and the duck. And I don't know why, uh, 'cause we never video stuff. [00:52:00] Uh, or we hadn't videoed anything previously. We, we took this video and it was like three in the morning. I, you know, just got back from skiing and so it was kind of an unhinged video in general.
Um, but, um. So we go to, we actually had Thanksgiving at a friend's house, and, and there's about four other families there. And we brought the Uck in and, and, uh, one of the docs, uh, actually, uh, one of the, the families, uh, who was there, she's, she's a doc, uh, but she all night long was like, you gotta post that video.
It's awesome, and blah, blah, blah. That's great. And so we made a TikTok account. We just posted the video after being browbeat all night. The next morning we had like 40, 50,000 views on this video. My wife who works in social media for a skincare [00:53:00] company, um. She's like, that's actually really odd 'cause you have no followers.
And uh, you know, that's a lot of views for a brand new, you know, account with no followers. And so then we posted another video, um, and that got, you know, like. Another 50, a hundred thousand views pretty quickly. And so then we just started posting these videos of, of me cooking We, and we called the account Seattle Hand Doc.
And, you know, fast forward 11 months or 10 months, we, yeah, we have, you know, 360,000 followers on Instagram, about 350,000 on TikTok. And, uh. It's become, uh, our, our, our, you know, nighttime activity, our, our, our second job for both of us. So yeah, we we're now the [00:54:00] point where, you know, starting to get recognized by people out and about and, uh, you know, different companies are reaching out to us to, to collaborate with them.
And, uh, so it's been really fun. Uh, I've actually learned a lot. Um. You'd think as a surgeon I'd have good knife skills, but, uh, uh, when it comes to the kitchen and chopping onions, uh, mine are terrible compared to my wife's, but, uh, I'm getting better. Um, well in
Dr. Grant Garcia: general, in general, you have to realize your wife's better than you would, pretty much everything.
Dr. Wayne Weil : yeah. Well, that goes without
Dr. Grant Garcia: saying you, you and I already have figured that out.
Dr. Wayne Weil : Yeah, we
Dr. Grant Garcia: knows that.
Dr. Wayne Weil : Yeah, no doubt about it. Uh. But, uh, yeah, it's been really fun 'cause uh, you know, uh, traditionally, uh, my wife did all the cooking. I did all the cleaning. Uh, but now we kind of do everything together. So it's, it's brought us, uh, together to some degree.
Although I screw up almost every night and I [00:55:00] get yelled at, but that's okay. Um, for the most part, we're having a good time. And, um, yeah, I've learned a lot and it's, and it's, it is, it's fun. It's, it's, uh, it's brought us together, which is really, really, um, the best part of all of it.
Dr. Grant Garcia: What's your highest views on a video so far?
Dr. Wayne Weil : Oh, wow. We, we've got, uh, I, I think it's still our nachos video, uh, which is up, it might be 12, 14 million views. Yeah, it's pretty crazy. Uh, and we,
Dr. Grant Garcia: dude, when are you gonna have speed? When are you gonna have speed speed on your cooking show? You mean That's the key. He's all over the place. Yeah.
Dr. Wayne Weil : Yeah. No, it's, it'd be awesome.
Will Sanchez: what do, what do your kids think about this? I mean, they've gotta be like, mom and dad is rocking it. I mean, you know, the, the younger generation, oh, they're on it now. This is supposed to
Dr. Wayne Weil : be, yeah. So that's been
Will Sanchez: seen on there. What are their thoughts?
Dr. Wayne Weil : It's been interesting to, to see that. [00:56:00] So, so we have five kids, so I think that's part of the draw in terms of, uh, you know, our, our account.
So our two college kids, uh, you know, from the get go, they were, they were all in and they thought it's awesome. Um, my, uh, at the time they were in middle school, now they're, they're freshmen in high school we have twins. Uh, they were horrified. Um, you know, like, can, you know, 'cause you know, when you're 13, 14, 15 years old, you know, nothing your parents do is cool, right?
You just, uh, they, your parents are, you know, the worst people ever. Um, and then my junior, now senior in high school, he was kind of lukewarm on it. Um, and so, uh, but now the kids have, have gotten around to, uh. Um, having a good time with it, and we pull them in on some of the videos. The, the three older kids are definitely more into it, uh, [00:57:00] than, um, than the youngest, the twins.
But we, we can cajole them into a video too, here and there, and. Actually my daughter, Charlotte, uh, one of her videos I think has about 4 million views, so she's a rockstar. Um, wow. But, uh, yeah, it's been fun. It's, it's, uh, and I've learned a lot in terms of just the whole social media world and influencers and, um.
To me, that's one of the things that I, I found most interesting is just that, you know, it's a lot of work and, um, you know, I used to kind of poo p the idea of, uh, social media and influencers and. You know, you look at people like the Kardashians or, or Jake Paul and, and Mr. Beast, and you know what they're doing.
And, you know, someone who's was basically uneducated like me would, would just say, well, that's ridiculous. You know, [00:58:00] why, why do they have so many, you know, why are they making millions of dollars doing this stuff? And, and now that I've, you know, just, just scratched the surface of, uh, of this whole social media world.
You know, I get it. You know, they, they have a product that, um, you know, people enjoy, uh, and, and they work at it. I mean, you know, they're putting up content every day. Um, it, it is a job, uh, no doubt about it. And, uh, so for me, that's, that's been kind of fascinating to, to come through that, uh, experience, to, to really have an appreciation for, for what people are doing out there.
Dr. Grant Garcia: So as we saw that we, uh, we went too long, we have, um, exactly a minute and 22 seconds before we have to stop because of the one hour social media limit. So you did good job, Wayne. You
Dr. Wayne Weil : awesome.
Will Sanchez: Thank you so much. Dr. Wayne Wild and a Seattle Hand Doctor, uh, orthopedics, [00:59:00] uh, surgeon, hand rest and elbow specialist, TikTok, influencer, you name it.
They've got too many titles. If not, we'll spend the next five minutes talking about the titles. Most importantly, thank you for spending some time with us and educating, uh, the listeners and patients and everyone. So once again, thank you for your time and have a good night.
Dr. Wayne Weil : Awesome. Thanks guys.
Dr. Grant Garcia: Safe drive home.
Dr. Wayne Weil : Alright, appreciate it. Been fun. Thank you very much. See y'all. Bye.
Will Sanchez: Bye.
Audio Transcript
Precision Hands: Dr. Wayne Weil

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon in sports medicine specialist. That man right there, Dr. Grant Garcia, Dr. Garcia, exciting. We have a new show. We have a great guest, but first and foremost, how are you?
Dr. Grant Garcia: I'm good. It still sunny for another day or two where summer's just stretching on in Seattle, so I can't complain.
Uh, unfortunately the giants are back to being terrible, which we don't have to talk about today. But the Seattle teams are doing well decently, so that's good. Mariners won. So we're excited about that. I guess.
Will Sanchez: Yes. Let's not bring up, why are we starting off the show with the Giants? Dr. Garcia? Man, you, you know,
Dr. Grant Garcia: it's always
Will Sanchez: we need
Dr. Grant Garcia: something.
Will Sanchez: Not doing this.
Dr. Grant Garcia: We had one game. We had [00:01:00] one game.
Will Sanchez: Oh my Lord. All right, man. Let's get to people that really care about us, 'cause obviously you are just trying to break my heart. Let's talk about the good folks at the Recovery Shop. The shout out to contact Mike b. Talk about the recovery shot and why you love them.
And our guests as well loves them as well.
Dr. Grant Garcia: Great. Yeah, so we, we like them because honestly, patients ask for a little bit extra sometimes, and it's challenging as a surgeon, you send them to, you know, Amazon or online to look for their stuff. So the option of having this for the patients is really nice. Uh, and the patients do appreciate it too because it's all kind of there together.
And you have the nice machine, which Dr. We, I think just tried out one of the new elbow devices, uh, which is really nice for patients. That's really a, a niche that many of the companies can't provide. Uh, so they've been really happy with them and I think the patients are really happy, which is more important.
Dr. Wayne Weil : Mm-hmm.
Dr. Grant Garcia: Uh, so if you're a surgeon, reach out to them. If you're a patient, you don't have that option, reach out to them. They can try to get your surgeon set up with it so that you can have that opportunity.
Will Sanchez: Let's get right to our guests [00:02:00] because we're keeping him from getting dinner, and that's a tease for something that we'll talk about later on.
Um, let's bring in the doctor, the hand, the wrist and elbow specialist himself. Dr. Wayne Wild. Dr. Wild, thank you for being on. Thank you for hanging with us and I apologize for Dr. Garcia bringing up things to start off the show in a negative way. How are you?
Dr. Wayne Weil : Uh, doing great. Uh, happy to be here. Thanks for the invitation.
Dr. Grant Garcia: Yes. Uh, so for the viewers introduced Dr. Al. He's a hand surgeon, actually, he's my partner. And we do a lot of cases together. Complex, uh, elbow surgeries. Um, and he specializes in hand, uh, wrist, um, and elbow and then dabbles with trauma as needed, uh, but really super specialized in the hand and nerve, uh, surgeries.
Also, chief of orthopedics at the Swedish Hospital system. And board of directors. So he is got extensive title and Pro Alliance as well as Pelto and he actually does family stuff as well on top of all that huge list. [00:03:00] So pretty impressive. Well, thanks for coming on. Really appreciate it. I'm sure Will's gonna have lots of questions to ask too.
Um, for the viewers, do you think you can kind of give a quick background? You know, I know you came from New York. Talk about your stuff and you know, now you're in Seattle, so just give us a little update and into who you are and where you came from.
Dr. Wayne Weil : Sure. Uh, yeah, I'm an East Coast guy originally, uh, grew up, uh, outside, uh, Bethesda, Maryland.
Uh, ended up, uh, uh, doing my, uh, college in Philadelphia and then, uh, resident med school and residency in New York City. Uh, then ended up out here, uh, for a hand surgery fellowship. Uh. And just kind of fell in love with the Pacific Northwest. And one of our other partners, uh, Dr. Shapiro, uh, who's a shoulder specialist here, uh, I knew him from New York, from, he was a fellow while I was a resident, and he ended up recruiting me to stay out here.
And, uh, now 21 years later, I'm, I'm [00:04:00] still here in Seattle. Uh, we now have five kids. As Dr. Garcia mentioned, uh, I've gotten involved in, uh, sort of, uh, non-practice stuff, uh, with, uh, being chief at, uh, Swedish and the board positions at Proliance. And, and then I've still, uh, at my, uh, practice where, uh, you know, I really enjoy just treating, uh, elbow, wrist, and hand and, uh.
I do a lot of that, whether it's uh, you know, sports injuries and, and younger folks or, or degenerative stuff and older people, arthritis, uh, stuff. So kind of do a little bit of everything, uh, except maybe sleeping, which, uh, I would like, but that's okay.
Will Sanchez: Dr. Uh, what can you tell us what first sparked your interest in hand in, in microvascular surgery, you know, how do you go along that [00:05:00] path and have that interest?
Dr. Wayne Weil : Yeah, so that really started in, in my, uh, fourth year of, uh, residency, um, as part of our residency program at NYU and Hospital for Joint Diseases. Uh, we do, uh, a four month rotation down in Baltimore at, at, uh, shock Trauma Hospital down in Baltimore. Um, and at the time, uh, there's a surgeon there, uh, Andy Seder.
Um, and, uh, Dr. Seder, uh, to this day, I think is the, the best surgeon I've ever seen operate. Just, uh, you know, I think, you know, for, for lack of a better, uh, descriptor, you know, gift from God in terms of, uh, he could do anything and it was always perfect. And, uh, so he really got me interested in, in microsurgery and, um.
Uh, kind of the rest is history from there. [00:06:00] Uh, so, so it's, I think, you know, in a lot of our lives, uh, you know, just exposure to, to, uh, a good mentor really can pave the way moving forward in terms of, uh, uh, really career paths in general. And, uh, yeah, I think, uh, Dr. Seder is really the, the, the person who who got me interested in, in, in what I'm doing today.
And then, um, you know, fast forward a couple years, uh. Doug Hanno, um, at, at University of Washington, who I did my hand surgery fellowship. Uh, another just phenomenal surgeon. Um, and, uh, you know, uh, Doug in, in a very similar way with Dr. Eder, you know, could fix anything and, and just an incredible surgeon and, and so, you know, like having the exposure to those two docs in particular. You know, I, I, [00:07:00] I stand on the shoulder of giants, uh, and, um, you know, I, I, I certainly give a lot of credit to those two guys for, for getting me to where I am today.
Dr. Grant Garcia: Uh, Wayne, I wanted, I wanna bring this up. I, because I think that's probably your answer is gonna be this too, but. You know, we see in the office, we talk about, I do a lot, you know, we talk about the sports surgeries that I do, but I see you doing a lot of really complex hand and wrist surgeries that not everybody would want to take on, even as a hand surgeon.
Do you think, and I don't wanna put too many words in your mouth, you think that stems from that background you're talking about? Or why do that? Like you could, your private practice, you could just do carpal tunnels. Yeah, procedures. You don't have to do the hard stuff. Why do you choose to?
Dr. Wayne Weil : Uh, you know, uh, maybe I'm just a masochist.
Uh, but I think that's true of kinda all the guys in our practice. I mean, we could all just do the simple stuff, but, uh, I think [00:08:00] we all enjoy the challenge. Um, you know. For me personally, if, yeah, I enjoy doing carpal tunnel surgery, but you know, uh, I would get bored if I just did that all day long. And, and, you know, for me, uh, maybe I'm blessed with the ability to do the hard stuff.
Uh, and, and I enjoy doing it. And, and I think that serves a, a niche for our patients. Uh. In terms of, you know, we, we see a lot of patients in our practice and, and, and you do, uh, as well, where, you know, they've bounced around to different docs in the community and, and just, uh, for whatever reason, you know, I haven't been able to, to get the care that they need.
And, and so for me it's, it's very gratifying to, to see a patient who's maybe seen a few docs, uh. And, uh, [00:09:00] has been told, you know, uh, we can't help you. You gotta live like this for the rest of your life or whatever it is. And, and to be able to see them and say, actually that's not true, uh, that we can help you and I can make you better.
Um, and, and I think. You know, that's why we went into medicine is, is to make people better. And, uh, um, you know, it's very gratifying. I think the, the more complicated a, a problem is in a lot of ways, it, it's even more gratifying to, to get to the other side where, where you've made somebody better. Like, um, so, and, and again, I think, you know, going back to the training, um.
Both at Shock Trauma in Baltimore, both at Harborview. I mean, we saw the craziest stuff you could ever imagine, you know, horrible injuries, uh, you know, whether it's, you know, explosives or industrial [00:10:00] injuries or, or what have you. And, you know, those two guys in particular, handle and Eder, they were just, you know, always so calm, always had a plan and, and able to execute it.
And I think having that kind of exposure where, where you've seen, you know, everything. Um, so when somebody walks in the door with something complicated, uh, you know, you, you, you rely on your b on your training and then your experience, you know, I've been doing this now for 21 years, been in practice. Uh, so I feel like, you know, there's not much out there that I haven't seen.
Uh, and so. That, that makes me prepared to, to take on the complicated stuff.
Dr. Grant Garcia: Awesome. Um, do you, so I know we talked about this, but the, obviously we might switch gears a little bit. Yeah. But the, coming from the complicated to maybe the more minimally invasive stuff that you do, I know you're, [00:11:00] you know, we know you're one of the only surgeons in the area that does this sort of endoscopic carpal tunnel, endoscopic cubital tunnel.
Will you talk a little bit about those procedures? The audience. And then what is the benefit, in your opinion, of doing it this way? I mean, it's also more challenging technically, but obviously what's the benefit to the patient? Why would you do that versus the standard open?
Dr. Wayne Weil : Yeah. Well, I mean, uh, the name of the game in, I think all of surgery is, you know, being less invasive, less destructive to the tissues.
Um, and, and that really. Um, you know, helps on the backend in terms of there's less stuff to heal. Right? Um, again, going back to my residency, you'll, you'll appreciate this story. Um, I was a third year resident and, uh, uh, scrubbed a case with a doctor, uh, who was, he was the only one in the NYU system still doing open [00:12:00] acls and.
And I done it. I'm shivering
Dr. Grant Garcia: by the way.
Dr. Wayne Weil : I'm
Dr. Grant Garcia: shaking. I'm having like,
Dr. Wayne Weil : you've probably never even seen one. Uh, so, um, and, and this is now circa 2003. So at this point, uh, or 2000, 2001. Uh, at this point, you know, uh, arthroscopic ACL surgery was a standard thing. I mean, it's not like, uh, it was brand new. People have been doing arthroscopic ACLS for 15, 20 years probably at the, at that point.
Um, and so yeah, so I scrubbed this case with this guy who's doing open ACL and, you know, the whole knee's filet open and, and. I couldn't believe what I was seeing. I, and I can't imagine what the recovery from that was. Uh, and having had an ACL done on, on my own knee, arthroscopic [00:13:00] ACL, I mean, it's, you know, worlds apart.
And so that experience in particular was like, well. Why would I ever do something that that was that traumatic, uh, if I can do it in a way that's, you know, not nearly, uh, as, as destructive to the surrounding tissues. Um, and so, you know, in residency actually, uh, we started doing, uh, endoscopic carpal tunnel releases.
And again, uh, smaller incision, less tissue invasion. And we'd have patients who, you know, had an open on one side and then came back and had the endoscopic on the other side, and they were like. The, every single one of those patients couldn't believe how much easier the, uh, the recovery was with the [00:14:00] endoscopic.
Just less pain, quicker return to work, better function. And, um, you know, the data has kind of borne that out, uh, when you look at the recovery. Um, again, just less pain, quicker return to bur and, uh, better grip strength in, in the first three months of recovery. Um, the opens end up catching up in the end and they do fine.
And, you know, at, at nine months, one year, everyone's the, the same. But why have an operation that takes you nine months to recover from when you can have the same operation, but it only takes you, you know, three months. Uh, and so similar to, to the, uh, ulnar nerve, uh, the cubital tunnel. Decompression the ulnar nerve.
Um, same idea, uh, is, you know, little incision. We do everything from the inside out instead of the outside in. And so, uh, again, you don't have to cut through any of the [00:15:00] muscles to get to where you wanna be. Um, and that just decreases the amount of time for recovery and, and, and gets people going a lot faster.
Um, and I think that's really. The exciting part in orthopedics, uh, where we're moving towards in general is, um, all the stuff we do is becoming less and less invasive. Uh, you look at a hip replacement, you know, you were in the hospital for a week when I was a resident. Now we do hip replacements, and you go home the same day.
Um. Same with, you know, knee replacements, uh, you know, a lot of the, the cartilage stuff that you're doing. Um, all of it is, is really starting to become outpatient surgery. I mean, even spine surgery is moving to, to outpatient surgery. Uh. And, and you look at the results, people do better when they're [00:16:00] home, uh, versus sitting in the hospital.
You know, you take the same operation, same person, your risk for infections and, and, and worse outcomes are higher if you stay in the hospital than if you go home. Um. So, uh, I think all of orthopedics, and especially in my specialty, you know, trying to do things in, in a minimally invasive way, it just, it just makes sense and it's better for the patients.
Um. In a lot of ways it's more fun for the surgeon 'cause uh, we get to play with cool, uh, new instruments. High
Dr. Grant Garcia: priority. That's the high priority there.
Dr. Wayne Weil : That's right. Um, you know, it's fun to go to the lab and kind of innovate and, and, and work with, uh, some of the, uh, companies to, you know, come up with, uh, you know, novel ways to do things.
Um, so, uh, I think it's sort of a win-win all the way around.
Dr. Grant Garcia: Will, can you pull up that slide? [00:17:00] Um, on the nano? I don't want to see, 'cause we're talking about, we're in the perfect example. Segue. Go to the next slide here. Lemme just do it.
Will Sanchez: Yeah, I have, I have, well,
Dr. Grant Garcia: yeah, Wayne right
Will Sanchez: there.
Dr. Grant Garcia: Yeah. So this is a, this is good.
You, I mean, we don't have to do the proprietary discussion here. I just was a picture, 'cause I know you've used this before. So for your minimally invasive situation, I mean, what would you use. Something small like this for, right. Yeah. Like the idea behind patients are always curious like, well how, how small can you go?
I've seen you scope some pretty small joints, right? Something I would never consider doing. So what are your uses of this and like how do you help, what does it help you with?
Dr. Wayne Weil : So, uh, yeah, we've gotten to the point now where, uh, you know, the instruments, uh, have gotten small enough where, you know, in the old days you could basically do a shoulder, uh, and a knee, and, and we've now, you know, uh, gotten to where we [00:18:00] can basically scope.
Pretty much any joint in the body for the most part. Uh, uh, you can scope out to even, uh, the PIP joint, um, proximal interphalangeal joint in the finger. Um, you can, uh, scope, you know, the base of the thumb. That's probably the most common one that I, I do now. Um, 'cause the base of the thumb, the carpal metacarpal joint, that's the one that, uh.
Becomes, uh, classically arthritic. And so, uh, there's, uh, procedures now that we can, uh, do kind of like in the knee where we do, uh, for arthritis, uh, some clean out procedures. So the instruments, not only the camera, but also, um, the different little shavers and the probes and instruments that we use, uh, are small enough that they fit in there.
Uh, so you can really do kind of what the large joint [00:19:00] arthroscopists do. Uh, you know, the stuff that you do in the knee and the shoulder grant. Now, now I can do, uh, to some degree in, uh, the base of the thumb and, and in the wrist. Um, and so we're, we're definitely catching up, I would say, to to the large joint, uh, uh, arthroscopists.
And a lot of it just has to do with. The ability to, to make the instruments smaller and smaller. It's kind of like our, uh, computers and our iPhones and everything else in the world. Yeah. Um, you know, the first iteration is, is big and, and then, uh, as we get, uh, better with manufacturing and, and the technology, it just.
You get smaller and smaller and smaller, so then we can start really having a good time, uh, with the, the small joint instrument, uh, small joint arthroscopy.
Dr. Grant Garcia: Would you say with this, I mean, when I first saw you do one of those thumbs, I was like, this [00:20:00] is crazy. This is cool. Uh, would you describe, like, what were you like for that patient?
You know, you, when you do the metacarpal, when you do the scope of the thumb
Dr. Wayne Weil : Yeah.
Dr. Grant Garcia: For some arthritis. Yeah. What were you doing before for them? Right. Because these are patients, they're not, they're not old enough for you. Sure. Or any other thing. So what were you doing before? Were you, or just is this at a new surgery for you?
Dr. Wayne Weil : Yeah. So, you know, uh, I think of it like arrows in, in, in your quiver, right? And, and so. Um, you've got only a certain amount of, uh, arrows in, in the quiver. And, and if you can have more arrows, that's awesome. So, uh, for those patients, you know, that was like your, your 40 and 50 year olds with, uh, early stage degenerative arthritis.
Uh, they've had, you know, splints and braces, but nobody likes those. 'cause uh, you need your thumb to actually live life and do things. And so if you lock up your thumb. You know, it's pretty miserable. You can't [00:21:00] really do much at all. You can't type on a computer, you can't hold an iPhone. Um, you know, you can't garden or play tennis or whatever it is.
Um, so people don't tend to wear 'em 'cause they're, they really inhibit your activities. Um, so you, you know, the, the braces were sorta, yeah, you can wear a brace, but nobody likes that. Uh, then there's occupational therapy. Um. You know, to some degree, some patients find it helpful, but it's not really solving any of the issues, uh, internally.
Um, then we move on to steroid injections and sometimes those can be helpful. Um, PRP injections, sometimes those can be helpful, and then you're kind of stuck after that. There's not really any non-operative treatments that, that are reasonable to do. And then operatively, then we start talking about joint replacement, uh, which, you know, it's a big step for a [00:22:00] 40-year-old to, to undergo.
And so now we're able to do a, uh, procedure that can, uh, potentially buy people some time. Uh, and put off, you know, the eventuality of a joint replacement by ideally 10, 20 years when it's more appropriate to do the joint replacement as opposed to when they're 40 or 50. So, so it's really opened up a whole new, uh, ability to treat patients.
'cause otherwise it was, well you're 45 years old and we've tried everything. So either live with it or, or have a joint replacement. Whereas now I can say, well, you, you've, we've tried all the non-op stuff. We can, uh, now think about doing an arthroscopy and kind of clean stuff up for you. And, and ideally we'll buy you another 10, 20 years and then you have your joint replacement, you know, when you're 60 or 70.
Um, so it is been fantastic in, in being [00:23:00] able to, you know, treat patients, uh, uh, in a, in a much better way, uh, as opposed to just telling them well live with it.
Will Sanchez: I had a question for you. Um, talk about common hand and wrist injuries, uh, whether it's the pro and recreational athletes, and what's your thoughts on some of these names, like the skier's thumb?
Yeah. Or the jersey finger. You're from the East coast? I don't think the Jersey finger is what I'm thinking of. Ain't
Dr. Wayne Weil : the Jersey Shore,
Will Sanchez: it's not the Jersey Shore. So can you talk about that a little bit? Because the names are absolutely fantastic and Jersey finger means a thing on the East coast.
Dr. Wayne Weil : Yeah, no, it's, uh, so, you know, the hand world, uh, ends up with lots of crazy EPIs and uh.
As Grant knows, you know, people, uh, call us the hand weenies, uh, 'cause kind of the, the, it's the reputation of the hand. Surgeons are kind of the nerdy guys who, uh, [00:24:00] are way into minutia and. You know, uh, Dr. Gel Seder used to always say, you know, the leg is just a stupid weight-bearing joint, right? You can cut a leg off and put a piece of wood and give someone a peg leg and they can walk.
Um, but the hand, you know, that's a whole nother kettle of fish, right? You take somebody's hand off and, and they're really debilitated. Um, so, um. Yeah, the hand world. We've got all kinds of names for crazy stuff. Uh, you know, skiers thumb, uh, which actually was a gamekeeper's thumb in the old days. Uh, and not 'cause you're, you're playing games, but, uh, keeping game like small games, small animals.
So, uh. You know, uh, the farmers would be, uh, the classic is snapping the necks of rabbits, uh, with their hand and over time. Story
Dr. Grant Garcia: is crazy.
Dr. Wayne Weil : The ligament, uh, of the, uh, the [00:25:00] ulnar collateral ligament of the thumb would, would basically just tear. From overuse in all the years of snapping rabbits. Next. So Dr. Grant Garcia: we'll pull that slide up.
Pull the, not the rabbits. We don't have a rabbits.
Will Sanchez: We don't have the dead rabbits. No, no.
Dr. Grant Garcia: Hold the thumb. Uc. Pull the thumb UCL up while he continues. Keep going Wade.
Dr. Wayne Weil : So, so, you know, fast forward a couple of centuries and, uh. You know, skier's thumb or mountain biker's, thumb, you know, if you can imagine you're holding a ski pole and uh, you fall, your thumb's kind of exposed out there and it gets wrenched back and, and it gets torn, uh, the ligament gets torn.
Or if you're mountain biking, uh, same idea. Your thumb's kind of exposed and you go over the handlebar and kind of superman out and your thumb gets yanked back. Uh, so it, it ends up tearing, uh, the ulnar collateral ligament, um, [00:26:00] which is the, the kind of, i I tell people that's the ACL of the thumb, right? So if you tear your, your ulnar collateral ligament, what it ends up happening is, is.
You can use your thumb and you can move it. And once it's the, you're, you're, uh, recovered from the acute injury, but the, the cartilage is going to, uh, be stressed in a way that it was not built to be stressed, uh, as the thumb kind of pivots abnormally when your power pinching and grasping. And so, you know, the reason to repair the thumb, UCL.
Kind of like the ACL is in a large ways is to prevent arthritis, uh, from happening, uh, in a pretty short, uh, amount of time with the cartilage damage that occurs with, you know, in the knee we call it pivoting. Where, where you have these moments where, where the femur and the tibia kind of shift on each other.
Same thing [00:27:00] in the thumb. So, so the goal and when we repair these is, is to restore that stability, uh, to the joint so that the, uh, cartilage, uh, doesn't have that or abnormal stress on it. And, and so folks can have, you know, a good joint, uh, moving forward. Um. You know, it looks like here we've got this, uh, slide with the internal brace, which, uh, that's been, you know, in talking about sort of minimally invasive surgery and innovation in, in, in surgery.
There's been a real game changer for us, uh, in the hand. Um, and, and really what it does is it, it allows folks to, to start their rehab basically, you know, the day after surgery in large part. So in particular with thumb, uh, ulnar collateral, ligament repairs, uh, in the past, before doing internal braces. Um, we [00:28:00] would put people in a cast for six weeks.
I, oh, sorry guys. Um, and after, uh, after being in the cast for six weeks, they'd come out and they, they'd be really stiff and then, you know, it takes another six, eight weeks to get them moving. Then once we got them moving, then we'd add in strengthening. So, so the whole rehab process was, was probably more like four to six months.
Whereas now with the internal brace, um, we, uh, we can basically, um, get people moving. I get people moving about five days after surgery. Uh, so. My protocol now is, um, a post-op splint.
They see the hand therapist at day five. Uh, splint comes off. They get a removable brace and they start, uh, working on range of motion, uh, so [00:29:00] that by basically six weeks they have their full range motion.
Uh, and we've already started working on some strengthening. So, um, the total rehab program is, uh, basically three months before back to normal. So it, it's, it's shortened their total rehab time by about 50%, um, which is awesome.
Dr. Grant Garcia: Yeah. And we've seen some crazy ones, right? You know, there's Joe, your, I know one of your friends is one of the guys that.
Proponents of it, kind of taught it to many and to a lot of the pro athletes. Uh, somebody trained with
Dr. Wayne Weil : Yeah, yeah. Lots of, lots of pro athletes now get the internal brace and, um, you know, that's kind of the way things evolve, right? Is uh, you know, the, the pros get, uh, the stuff first and then it kind of trickles down.
But, uh, at this point, uh, I, I wouldn't. Necessarily even think about doing the, the surgery without an internal brace. [00:30:00] 'cause I just, again, it's like an open, uh, an open ACL versus arthroscopic ACL or an open carpal tunnel versus endoscopic, you know, people just get better faster. And, and, you know, in our patient population here in Seattle, um, you know, people don't wanna spend, you know.
Months at a time, either outta work or not kayaking, or not skiing or mountain biking or doing, you know, the things that they'd love to do. Um,
Dr. Grant Garcia: and for the listeners too. Oh, so I was gonna say the listeners too. It's also important that it's now that we'll stand line, right? So people are looking this up, they're already coming to you.
We're in a tech heavy market, so it's not like, you know, open ACL in New York is different animal. In Seattle, you wouldn't even see a patient in the office. They wouldn't show up to your office knowing that you do open acls. I mean, and this is, we can say Mike Trout, Bryce Harper. These are some names that done.
I did. We actually worked with Curtis Anderson when he had his UCL, [00:31:00] uh, Terry. You have Drew Brees. I mean, it's pretty extensive. The list is pretty impressive. Yeah. How people have had this surgery done. So sorry. We'll keep going.
Will Sanchez: No, no, I was gonna follow up on that. You know, uh, we're talking about pro athletes and we know that they kind of en endeavor this, uh, pain threshold.
What are some of the ramifications if you have a pro athlete or a quarterback or a golfer that puts off surgery when they need it, waiting for the off season or something like that? What, what are some of the repercussions or some of the concerns when you have, uh, a high profile athlete that really needs surgery?
Dr. Wayne Weil : Yeah. You know, that, that, that's a, that's a great question. And, and sort of that intersection of medicine, sports business, uh, you start really having different forces at play, right? In an ideal world, you know, somebody has a torn ligament, you know, you get 'em in, you fix 'em. Uh, they rehab. [00:32:00] But, uh, you know, with, with these, uh, high
performance athletes who, you know, getting paid, you know, millions of dollars to, to play, um, and these are all, you know, super competitive people too.
They, they want to play, they, they don't want to just kind of ride the bench and, and, and miss out on a season. Um, so not only are they super. Um, uh, competitive and want to, to, to be out there. Um, but the, you know, the teams want them out there. The agents want them out there. Uh, so you definitely have to navigate those forces.
Uh, you know, when you're treating, uh, a professional athlete or, or a high level college, uh, athlete. Um. You know, as a physician, I, I always just, you know, uh, kinda, um, uh, harp back to [00:33:00] you gotta do what's right for the patient. And, and so, you know, I tell my patients, look, you can play, uh, you can grin and bear it, but there, there may be serious consequences, you know, down the road, uh, when we.
You know, ultimately fix it. If there's, you know, been further damage, um, I might not be able to make you as good as you once were. 'cause you've damaged that joint to, to a point where now it's, it's, it's, you know, a salvage operation versus an operation where, where you're gonna be, you know, basically normal again.
So you may play this year, but you may not play, you know, for the rest of your career. Um. So, you know, and, and some of this has to do with just timing of things, right? So, you know, beginning of the season versus end of the season teams, you know, in the playoffs, not in the playoffs. Uh, [00:34:00] so, you know, you, you gotta kind of juggle all those, uh, factors.
Uh, but at the end of the day, I think, uh, as a doc, you know, my job is to educate my patients. Um, and it is a, you know, ultimately it's, it's their decision. Um, you know, patient autonomy is important. Uh, and I feel really strongly that, you know, if I give somebody all the information, uh, that they need to make a, a decision that's, that's good for them, then I'm okay with whatever they, they decide.
Um, but, uh, I'm not gonna sugarcoat it. I'm not gonna tell them. Oh yeah, you can delay and you'll be fine. You know? Yeah. I tell them, I tell 'em the truth.
Dr. Grant Garcia: Yeah.
Will Sanchez: Gotcha.
Dr. Grant Garcia: Uh, with that, uh, I want to go back and I appreciate all your insights on these. We talked about scoping, but the risk scope stuff that you do, especially with the TFCC and some of the ligament stuff, like what sort of newer stuff you [00:35:00] talk about the wrist arthroscopy a little bit.
I mean, that's the stuff that. The minimally invasive stuff that you're doing now, you're adding more things, right? You're doing different things you weren't able to do before with the scope. Yeah. Like what do you, what new stuff are you doing with the risk scope then why is that beneficial to patients?
Dr. Wayne Weil : So, so yeah, with the risk, the arthroscopy and especially the the TFCC, which stands for triangular fibro cartilage complex. That's why we call it TFCC 'cause. Is pain in the ass to say, but, uh, so, uh, and that's a pretty common injury from a fall and, and people think of it, ah, it's just a wrist sprain. It'll get better, but.
People, uh, oftentimes will end up, uh, with sort of chronic, uh, ulnar sided wrist pain, which is kind of the pinky side of the wrist, and oftentimes that that's due to, uh, this tear of the TFCC, which, uh, again, I like to use the knee as, uh, uh. Uh, an example for folks. 'cause everybody's heard of the meniscus of the [00:36:00] knee.
Uh, the, the TFCC is kind of similar in that it's the shock absorber, uh, for the ulnar side of the wrist and helps with some stability of the wrist. Uh, and so, uh, now that again, we've gotten sort of minimization of the instruments, uh, and the anchors. Um, we can start really, uh, doing much, uh, better, uh, repairs of the TFCC as opposed to just cutting it out.
So, uh. You know, like Dr. Garcia does in the knee in terms of repairing the meniscus versus chopping it out. Uh, our ability now to, to do repairs is, is much, much better than even five years ago where, um, you know, we were doing repairs but they were not so easy to do. And the default was always, you know, just cut the min, cut the TFCC out, um, which certainly helps with pain relief, but you [00:37:00] know, it's always better to repair something than chop it out if you can.
Um, so that's really been one of the big innovations in terms of, uh, uh, wrist arthroscopy, uh, and um, then also on, on the ligament side. Um, working, uh, to, to get some better, uh, repairs, uh, of those ligaments. Arthroscopically, uh, is, is certainly in the works, um, to, to work on instability issues, uh, in the wrist.
Arthroscopically. And then, uh, you know, starting Wayne,
Dr. Grant Garcia: would that be, would that be like, uh, people that have unstable ligaments, like they, or they tear like a mechanism that keeps, will you describe that briefly for the patient? Dr. Wayne Weil : Yeah, so, so like, uh, potentially, uh, STA four ate ligament, uh, repairs, uh, done arthroscopically, uh, again, uh, the SL ligament, uh, very similar, uh, to, uh, ACL in the knee.
This is. You know, we have the [00:38:00] ACL of the thumb, that's the ulnar collateral ligament. And then we have the ACL of the, uh, wrist. That's the scavo lunate ligament. Um, and so, yeah, well they can
Dr. Grant Garcia: internally brace those. Do you internally brace those? Ev don't get well, too excited. Try.
Dr. Wayne Weil : We're getting there. Uh, so, so yeah, that's sort of the next iteration of things is, is, uh, doing those, uh, repairs, uh, arthroscopically instead of open.
Um, and, uh, then also, uh, maybe doing some cartilage work as well. Um, and, and just really being able to, um, minimize, uh, all our surgeries that we're doing open. So, uh, we are, uh, definitely pushing the envelope all the time. Um, in terms of what, what we can do
Dr. Grant Garcia: when you do those scap illuminate ligaments, can you.
Can you do like an arthroscopic assisted, like that's sometimes what I do for some of my surgeries. Like you could see 'em go back together. So you don't have to do x-ray. You really can see 'em touching with the [00:39:00]
Dr. Wayne Weil : thought process. Yeah. So that's, that's, I think, uh, you know, kind of the, the, the spot that we're in now is, is arthroscopic assisted.
Um, really just kind of helps, uh, see, you know, where you are with the, uh, joint surfaces, um, and, and when you're closing them down. And then you can even stress, uh, the, the joint and really see that, you know, the, the ligament that you fixed. Um. Uh, is stable. Uh, and, and you can see, just see it much better than an x-ray.
Right? Uh, you're looking directly at it with the scope, uh, versus, uh, with an x-ray. You know, you're just kind of interpreting, you know, the, the shape of the bones and how they're relating, but you're, it's, it's better to see it directly.
Dr. Grant Garcia: Yeah. And for the listeners you're talking about. The ankle. A lot of people with ankle fractures, you see the, nowadays, all these newer surgeons like Dr.
Yee, we talk about, or Dr. Reed. Yeah. [00:40:00] They're scoping the, they're scoping the ankle with the fracture of the ankle. Right. So they're making sure that the cartilage is not too damaged. Or when the knee, when we have a tibial plateau fracture, sometimes we do an arthroscopic to see how well we line the surfaces up.
'cause as you said, x-ray's only so good. Plus it reduces x-ray time, which is always better for. The patients and for the surgeon not having to get fluoroscopy all the time.
Dr. Wayne Weil : Yeah. So, so one of the things that, that you mentioned, yeah. I think in, in fracture work, uh, arthroscopic assisted is, is, is awesome.
Like I, I will, uh, for wrist fractures just to raise fractures, uh, I'll put the scope in at the end. Uh, sometimes, uh, if I'm concerned about the, uh, articular surface, the joint surface to, to just make sure that all the little. Uh, surfaces are, are well lined up. 'cause you know, with fractures, the, the biggest thing is, is getting that joint surface smooth again.
You don't wanna leave the joint surface with the giant pothole in it. 'cause, because that's where, when people end up with, [00:41:00] you know, post-traumatic arthritic problems is, is 'cause the joint surface wasn't, uh, fixed properly.
Dr. Grant Garcia: I think that's an excellent point 'cause it's always hard to see sometimes on these, and you're dealing with even smaller bones.
So for the listeners to hear that like. If you've got some issue, you know, that's something you talk to your surgeon about, right? Like arthroscopic assisted is is the, the new gold standard.
You know, not in every case, but in those challenging cases it's, it's important factor to have in order to preserve the joint, which is really where you're going.
It's going joint preservation. I do knee joint, sometimes shoulder joint, and you do hand and wrist joint preservation and so that's a key point preservation. 'cause we don't want to be fusing and replacing, its. Not nearly as much fun too, right?
Dr. Wayne Weil : That's
Dr. Grant Garcia: right. So, uh, will you, were about to jump on something.
You had a question?
Will Sanchez: Yeah, no, just a quick question. Uh, regarding, you know, anyone that's listening that's either a patient or just, uh, nothing personal. I really don't want to come see you because I have a broken hand or wrist. Right. So is there any hand [00:42:00] exercises or stretches or anything that. That's been documented to kind of maybe reduce the risk.
Obviously if there's trauma, that's something else, like falling off a mountain, grabbing and twisting your arm back. Yeah. Are there exercises or, or stretches that you can utilize to unfortunately not go see you?
Dr. Wayne Weil : Yeah. Yeah. Great question. So, uh. In terms of, uh, you know, I think just holistic view of, you know, our bodies in general.
Um, you know, there's clear data that just, um, you know, use is good. Uh, sitting around on the couch doing nothing. That's bad for you. Right? So, so being active and, um, that I think is number one, the biggest, uh, benefit to, to longevity in general. So, you know, if you look at sort of those blue zone studies, you, you know, people who live on, [00:43:00] uh, hilly areas.
Live longer. Why? Because they have to walk up and down hills all day long 'cause they're getting exercise. So, so same thing with hands. Uh, and I think that's, you know, true of any joint in our body is, is using it, staying, um, flexible, uh, working on your flexibility, uh, working on your strength. Um, and, and ideally you, you know, I think there's not, I would say one specific exercise that's awesome for you, you know, working on your grip strength, and if you lead an active lifestyle, you know your hands will be exercised.
Uh, you know, it's the folks that, you know, sit around on, on the couch watching TV all day. Those are the ones that I worry about a lot more. Got you.
Will Sanchez: Thank you.
Dr. Grant Garcia: Let's, we wanna, in the sake of time, make sure Wayne has, can get outta here. Eventually meet the traffic. The, uh, but one other, I want one other talk [00:44:00] topic to talk about really quickly and then a little bit of fun, and then we can get you outta here.
Will you, okay. I know Mike Trout had this recently. I've seen you deal with some of the baseball players
Dr. Wayne Weil : Yeah.
Dr. Grant Garcia: On Merc round teams, et cetera. This one happens a lot. We hear this a lot. And this idea of removing the hook of handmaid or doing something, can you describe it to. What's the most common person athlete you see with this?
And then how, what's the kind of treatment regimen you normally deal with?
Dr. Wayne Weil : Yeah, no, these are, uh, this is a great, uh, uh, photo. Actually. I just saw a patient today, uh, with this injury, um, the most common baseball players. Um, and it's an interesting injury. In that you would expect it's a blunt force trauma, but it, it typically happens on a, on a swing and a miss.
Uh, so where, where they strike out, um, and it's the rotation of the bat, uh, through the follow through when, uh, the, the hook of the handmade [00:45:00] fractures, uh. And so, um, the hook of the Hamid, as you can see here, acts, uh, a little bit, uh, like a pulley, uh, on that, uh, small finger flexor tendon. Um, and it, it has a reputation for, for not healing.
Um, the blood supply to there is not great. And so, um. The, the treatment for this typically is just you excise that portion, uh, that's, uh, where that arrow is pointing. So, so the top part or, or the hook. Uh, as opposed to the body of the hamate. And then you kind of smooth out the, the fracture zone. Um, 'cause you don't want the flexor tendon, uh, a braided by the, um, the, the bone, uh, that's been fractured to kind acts, uh, almost like a [00:46:00] saw on the, uh, on the flexor tendon.
So, so you smooth out that fracture and. And it is an operation that, uh, works really well in terms of, uh, relieving pain, uh, and getting people back, uh, uh, to, to playing baseball. Golfers can get it as well. Um, and then, um, the other sort of cohort of folks who, who, uh, break their, uh, hook of the hammit, uh, are people who kind of use their hand like a hammer.
And are are banging on, on their hand. Uh, uh, you know, there's a, a board in your porch that's a little bit up and so you, you know, you smack the, the board down with your hand and you can injure your handmaid that way. Um, but uh, yeah, it's, it is interesting. It's an interesting injury. 'cause, 'cause you'd think it was more of a blunt force injury or, or, you know, when, when, in baseball, when.
And the batter connects with, [00:47:00] with the ball, but it's, it's actually when they strike out, when it happens,
Will Sanchez: is it the hand, is it the bottom handle of the bat that's rounded, that's coming through on the follow through and grabbing that part of the hand? Is that what
Dr. Wayne Weil : some of that also is just the force transmissions, you know, as the hands are turning over and you've got this giant lever arm, which is the bat.
Will Sanchez: Yeah.
Dr. Wayne Weil : Uh, and it just torques the, the hand just in a perfect way to, to break off the, uh, hammit, um, really common in, in actually, uh, pro baseball players. Uh, um, we, we see it kinda, uh, pretty regularly.
Will Sanchez: And you don't see it with golfers.
Dr. Wayne Weil : Yeah. You see it with golfers too. Okay. Uh, usually with golfers it's more they hit, you know, a really fat shot and their club gets stuck.
In the ground and then their hands kind of rotate over it. Um, but, but [00:48:00] it's a gratifying injury to treat 'cause uh, you know, you just take out the hook of the handmaid and, and people get back really quickly. So, yeah. Um,
Will Sanchez: that's interesting.
Dr. Grant Garcia: Awesome.
Dr. Wayne Weil : Yeah.
Dr. Grant Garcia: Uh, so I guess since you know, you're well known for all your hand surgeries.
But actually what the viewers don't, may or may not know if they're doctors or patients listening to this, you actually are more popularly known for something else. So as of now, you are now famous for other things. So I'd like to show the viewers and maybe a better understand and hear the background story behind this.
Dr. Wayne Weil : So lonely. That's, yeah. This is, uh, this is my, uh, new, uh, sky gig,
Dr. Grant Garcia: and he's [00:49:00] smiling the whole time positive. Amazing. Well pull, pull
Dr. Wayne Weil : up his
Dr. Grant Garcia: followers,
Dr. Wayne Weil : director in the background. Smile.
Dr. Grant Garcia: That's pretty impressive.
I think it went up since we started the show. When I told you how many followers you had, it literally went up between this entire show recording 'cause Will just changed it.
Dr. Wayne Weil : Yeah, it's uh, it's gotten kind of crazy. We, um, yeah, this is, uh, something that's just kinda come out of the blue for us. It was kind of a joke.
Uh. Started actually December 1st, last year after Thanksgiving. Um, we, uh, my wife is, uh, used to be a private chef, so she's a, she's an awesome cook. [00:50:00] And, uh, and all our friends, uh, and family know that she's amazing. She should open up a restaurant. Um, but, uh, her classic, classic Thanksgiving is. To die for and, and it's our family favorite.
My wife was actually born on Thanksgiving, so it's kind of a big deal for, for our family. And she does this really traditional Thanksgiving with, you know, giant Turkey. Usually it's like a 28, 30 pound Turkey and, uh, with, you know, four different pies and all the sides you could ever want. You know, it's a massive undertaking. And so this year she's like. We're not doing Thanksgiving. I'm tired of it. And
Will Sanchez: what
Dr. Wayne Weil : everyone, we were so depressed. 'cause it literally, our whole family looks forward to it every year. It's like, I wanna make a Turin. Uh, so, um, for those of you who are, uh, [00:51:00] John Madden fans, back in the old day, if you look up some of the videos of John Madden in, in New Orleans, uh, this comes back to, uh, the Turin.
Um mm-hmm. So a Turin is a, is basically it's a Turkey and a uh, uh, a chicken and a duck all stuffed, uh, inside the, the Turkey. And so, um, my wife asked me to learn how to deone the Turkey and chicken and duck and then, uh. Um, so I, you know, watched a couple videos on how to do it and so we, we made this tur Duckin, um, and uh, at the end you, you basically, you sew the Turkey back, uh, together.
So it looks kind of like a Turkey again. Uh, and it's stuffed with the stuffing and the chicken and the, and the duck. And I don't know why, uh, 'cause we never video stuff. [00:52:00] Uh, or we hadn't videoed anything previously. We, we took this video and it was like three in the morning. I, you know, just got back from skiing and so it was kind of an unhinged video in general.
Um, but, um. So we go to, we actually had Thanksgiving at a friend's house, and, and there's about four other families there. And we brought the Uck in and, and, uh, one of the docs, uh, actually, uh, one of the, the families, uh, who was there, she's, she's a doc, uh, but she all night long was like, you gotta post that video.
It's awesome, and blah, blah, blah. That's great. And so we made a TikTok account. We just posted the video after being browbeat all night. The next morning we had like 40, 50,000 views on this video. My wife who works in social media for a skincare [00:53:00] company, um. She's like, that's actually really odd 'cause you have no followers.
And uh, you know, that's a lot of views for a brand new, you know, account with no followers. And so then we posted another video, um, and that got, you know, like. Another 50, a hundred thousand views pretty quickly. And so then we just started posting these videos of, of me cooking We, and we called the account Seattle Hand Doc.
And, you know, fast forward 11 months or 10 months, we, yeah, we have, you know, 360,000 followers on Instagram, about 350,000 on TikTok. And, uh. It's become, uh, our, our, our, you know, nighttime activity, our, our, our second job for both of us. So yeah, we we're now the [00:54:00] point where, you know, starting to get recognized by people out and about and, uh, you know, different companies are reaching out to us to, to collaborate with them.
And, uh, so it's been really fun. Uh, I've actually learned a lot. Um. You'd think as a surgeon I'd have good knife skills, but, uh, uh, when it comes to the kitchen and chopping onions, uh, mine are terrible compared to my wife's, but, uh, I'm getting better. Um, well in
Dr. Grant Garcia: general, in general, you have to realize your wife's better than you would, pretty much everything.
Dr. Wayne Weil : yeah. Well, that goes without
Dr. Grant Garcia: saying you, you and I already have figured that out.
Dr. Wayne Weil : Yeah, we
Dr. Grant Garcia: knows that.
Dr. Wayne Weil : Yeah, no doubt about it. Uh. But, uh, yeah, it's been really fun 'cause uh, you know, uh, traditionally, uh, my wife did all the cooking. I did all the cleaning. Uh, but now we kind of do everything together. So it's, it's brought us, uh, together to some degree.
Although I screw up almost every night and I [00:55:00] get yelled at, but that's okay. Um, for the most part, we're having a good time. And, um, yeah, I've learned a lot and it's, and it's, it is, it's fun. It's, it's, uh, it's brought us together, which is really, really, um, the best part of all of it.
Dr. Grant Garcia: What's your highest views on a video so far?
Dr. Wayne Weil : Oh, wow. We, we've got, uh, I, I think it's still our nachos video, uh, which is up, it might be 12, 14 million views. Yeah, it's pretty crazy. Uh, and we,
Dr. Grant Garcia: dude, when are you gonna have speed? When are you gonna have speed speed on your cooking show? You mean That's the key. He's all over the place. Yeah.
Dr. Wayne Weil : Yeah. No, it's, it'd be awesome.
Will Sanchez: what do, what do your kids think about this? I mean, they've gotta be like, mom and dad is rocking it. I mean, you know, the, the younger generation, oh, they're on it now. This is supposed to
Dr. Wayne Weil : be, yeah. So that's been
Will Sanchez: seen on there. What are their thoughts?
Dr. Wayne Weil : It's been interesting to, to see that. [00:56:00] So, so we have five kids, so I think that's part of the draw in terms of, uh, you know, our, our account.
So our two college kids, uh, you know, from the get go, they were, they were all in and they thought it's awesome. Um, my, uh, at the time they were in middle school, now they're, they're freshmen in high school we have twins. Uh, they were horrified. Um, you know, like, can, you know, 'cause you know, when you're 13, 14, 15 years old, you know, nothing your parents do is cool, right?
You just, uh, they, your parents are, you know, the worst people ever. Um, and then my junior, now senior in high school, he was kind of lukewarm on it. Um, and so, uh, but now the kids have, have gotten around to, uh. Um, having a good time with it, and we pull them in on some of the videos. The, the three older kids are definitely more into it, uh, [00:57:00] than, um, than the youngest, the twins.
But we, we can cajole them into a video too, here and there, and. Actually my daughter, Charlotte, uh, one of her videos I think has about 4 million views, so she's a rockstar. Um, wow. But, uh, yeah, it's been fun. It's, it's, uh, and I've learned a lot in terms of just the whole social media world and influencers and, um.
To me, that's one of the things that I, I found most interesting is just that, you know, it's a lot of work and, um, you know, I used to kind of poo p the idea of, uh, social media and influencers and. You know, you look at people like the Kardashians or, or Jake Paul and, and Mr. Beast, and you know what they're doing.
And, you know, someone who's was basically uneducated like me would, would just say, well, that's ridiculous. You know, [00:58:00] why, why do they have so many, you know, why are they making millions of dollars doing this stuff? And, and now that I've, you know, just, just scratched the surface of, uh, of this whole social media world.
You know, I get it. You know, they, they have a product that, um, you know, people enjoy, uh, and, and they work at it. I mean, you know, they're putting up content every day. Um, it, it is a job, uh, no doubt about it. And, uh, so for me, that's, that's been kind of fascinating to, to come through that, uh, experience, to, to really have an appreciation for, for what people are doing out there.
Dr. Grant Garcia: So as we saw that we, uh, we went too long, we have, um, exactly a minute and 22 seconds before we have to stop because of the one hour social media limit. So you did good job, Wayne. You
Dr. Wayne Weil : awesome.
Will Sanchez: Thank you so much. Dr. Wayne Wild and a Seattle Hand Doctor, uh, orthopedics, [00:59:00] uh, surgeon, hand rest and elbow specialist, TikTok, influencer, you name it.
They've got too many titles. If not, we'll spend the next five minutes talking about the titles. Most importantly, thank you for spending some time with us and educating, uh, the listeners and patients and everyone. So once again, thank you for your time and have a good night.
Dr. Wayne Weil : Awesome. Thanks guys.
Dr. Grant Garcia: Safe drive home.
Dr. Wayne Weil : Alright, appreciate it. Been fun. Thank you very much. See y'all. Bye.
Will Sanchez: Bye.
Audio Transcript
Protecting your Ankles with Keke Lyles and Betterguards Technology.
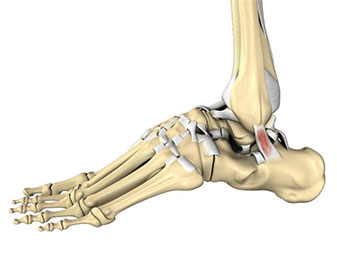
Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with Dr. Grant Garcia, our orthopedic surgeon, sports medicine specialist, Dr. Garcia's. I had to take out my Allen Iversson SL short shirt. We're talking a little basketball, we're talking a little rehab. We're getting into everything. Um, 12 months out of the year, we can talk basketball, but before I get into all that stuff and introduce our guests, Dr.
Garcia, how are you? I'm
Dr. Grant Garcia: good. I'm good. I'm, things are good over here at summer in Seattle. Can't complain. I'm really excited for our guests coming up. Uh, we've talked at nausea about ankle sprains and how long the issues with them and the recovery process and, you know, on our football updates, we're always like, well, when are they getting back?
I don't know. I don't know. Yeah, it's a huge, it's probably, it, it goes every one of these [00:01:00] sports and, and it's not above that. And for the NBA, so I'm really excited for this.
Will Sanchez: Yeah, so am I and someone that's had major, uh, ankle injuries as well. Um, you know, we probably could have used some of that technology and some of the things that we're gonna talk about, but we're talking about injuries, so we're talking about recoveries.
Let's give a shout out to our folks there at the Recovery Shop.
Dr. Grant Garcia: Yeah, so special thanks to Mike and those guys for Recovery Shop and Sponsorship. Again, like I say before, you know, this is maybe something that you can eventually find better guards on. The idea behind here is that for people that are recovering from something or some sort of rehab ability, uh, you can use this especially as a surgeon, to kind of keep everything put together for your patients.
They're always asking, what more can I do? What better can I do? How can I protect myself? And this is your option. So it works great. It can be customized and the patients like the personalized experience similar to something we're gonna show in a minute.
Will Sanchez: All right, let's, uh, let's not waste any more time.
Let's bring in our guests. Uh, we're really excited to have our guests, uh, KK Lyles, thank you so much for being a part of the [00:02:00] show and being with us and sharing your knowledge. I will do my best to keep Dr. Garcia under control. He likes to ramble a lot. Um, love it. Yeah. Yeah. So first and foremost, what, what are we thinking about the Allen Iversson shirt?
How you feeling about that?
Keke Lyles: I love, I, I miss the old Slam Magazine, obviously. That's what we grew up on, right? So,
Will Sanchez: yeah.
Keke Lyles: Yeah. I loving it that
Will Sanchez: that was, that was kinda like the fangoria for sports fans, basketball fans. I don't even know if Fangoria still exists. And as you see, I digress. I go off all.
Different tangents, which is one of the things that gets me in trouble here. But, um, let, let's talk about your career. We have so many things to get on, uh, to talk about, but you, you've worked with some of the top athletes in the world. Um, you have NBA experience. Why don't you just give, uh, our folks, our listeners, our viewers, a little bit of a background on the things that you've done and will lead up to the things that you're doing now.
Keke Lyles: Well, first appreciate you guys having me on as a guest. So excited to have this conversation. Um, yeah, my background, uh, doctor in physical therapy, uh, grew up [00:03:00] playing sports and, and really is when I was in PT school, uh, I, I started working as a strength and conditioning coach. For the university. I went to Northeastern, uh, out there in Boston.
Mm-hmm. Um, and it, it was during that time when I really started to develop this idea of like, especially in athletics, like injuries and performance is really, uh, on a continuum. Uh, and especially during a season, you know, we're either, uh, trying to optimize performance or maybe, uh, recover from an injury.
And so it's kind of all along that same continuum. And I love technology. I love, um, trying to understand things at a higher, maybe a deeper level. And so I've always been, uh, attracted to different, different tech, different data sets, uh, to inform my decisions or kind of my hunches and, and have kind of, uh, you know, built a career around that, I suppose.
And so. Fortunate after grad school, um, got on with the Minnesota Timberwolves as a head SNC coach. After a few seasons there went to Golden State, uh, as director of performance. Um, had obviously [00:04:00] success, uh, team success, winning a championship in Golden State, which I think opened up more opportunities for me.
Um, and, and eventually went to the Atlanta Hawks as executive director, kind of overseeing everything sports medicine, sports performance. Sports science, you name it. Um, and, and try to build systems, uh, build out systems in place that we can, uh, assess our athletes, try to understand 'em on an individual level and, and build programs to, uh, help them achieve their goals.
Dr. Grant Garcia: Yeah, I think it's important for we listeners to see that we're the person here who's gonna talk about this product we're gonna talk about. This is not something where you just all of a sudden showed up and decided to do this. It's, you lived it, breathed it. You've had to deal with injuries to all those sort of high level players and with the professionals.
We keep talking about these injuries, right? Like one day out is a lot of money, two days out's a lot of money. Mm-hmm. It's a huge investment for the team. It's also hugely dissatisfying and frustrating for the players. So I think that this is a great setup to kind of the, the next steps.
Keke Lyles: Yeah, and I [00:05:00] think honestly, you know, I mean obviously you said it all sports deal with ankle injuries.
Uh, but a any injury to your point, like our job is really to try to prevent as many as the, you know, kind of preventable injuries that are out there, soft tissues, overuse injuries, things like that. Uh, but some injuries are unavoidable. Um, and when that happens, our job is to get the player back as quick as we can.
So, uh, we, we kind of look for anything and everything that's gonna help us in that process. And over the years, um, you know, since being with the NBA team, obviously meeting better guards and the ankle bur company that we're gonna talk a little bit about, like it's just a game changer, not only helping prevent the injury from happening, but then also speeding up the recovery afterwards.
Dr. Grant Garcia: Awesome. So what we kind of hinted at it, people have seen in my background, they saw it on the intro, they're gonna see it on all the blasts, but tell us how you got to that point and then I kind of wanna show off the product really quick with the video and then we'll go back to doing more questions.
Keke Lyles: Yeah. [00:06:00] So, uh, when after departing with Atlanta Hawks, uh, moved out to Southern California where I'm still at, and, uh, worked with Navy Special Warfare and started consulting with teams and individual athletes. Uh, did some projects, uh, around, uh, with the NBA League office. As well. And that's when they started the launchpad, uh, program.
Uh, and that's when how I got introduced to better guards. And so when I first met that team, uh, through the launchpad program with another company I was working with at the time, advising, I just immediately was like, oh, where has this been? Uh, I got super excited about it, obviously. Um, and started advising, working with the team, um, and, and really just trying to get it out in, in front of as many athletes and get feedback.
And obviously they're coming out with their 3.0 brace. So, you know, they, they do a great job of taking feedback from athletes more around the comfort, um, than anything and making it more and more comfortable, which, you know, it's just testament to the company 'cause. I thought the version one was really comfortable.
So the [00:07:00] fact that they're on version three already is is pretty awesome.
Dr. Grant Garcia: Well, and I think one of the negatives of all these braces is you can constantly hear like. It may be high stiffness, but maybe not in this case. We'll show that in a second, but really, it's comfort, right? And a lot of the players don't wanna play it.
It's just like ACL braces. Like if you're not gonna get a player to wear an ACL brace, they're not comfortable. And maybe they protect you, but they're not comfortable and you're not gonna play your higher performance. So it's a really important point.
Keke Lyles: Yeah. And you know, to be honest too, I mean obviously in Golden State working with staff like, and through some of his injury stuff, like, I mean, the comfort of the brace is gonna be probably more important to the player than the function of the brace.
And that's just the reality of it. Um, and so you may have the best brace in the world, but if the player, to your point, if the player's not comfortable wearing it. They're just not gonna wear it. And so there has to be, uh, a perfect balance of comfort and function. I think
Dr. Grant Garcia: that's
Keke Lyles: an
Dr. Grant Garcia: awesome segue. Will pull up the video and then let's go back.[00:08:00]
You got it.
Will Sanchez: Great videos. Doesn't get any. Yeah, you're seeing the flexibility, you're seeing the jump. I used to jump like that many moons ago. Not really. Actually you catch like that too, right? You got, oh yeah. Well, you know, to be fair with the gloves that they have now, any of us can pretty much catch. But yeah, I don't wanna get in trouble with any, uh, any of these athletes here.
But anyway, go ahead.
Dr. Grant Garcia: Anyhow, so [00:09:00] I love the video. Obviously it shows, you know, you've got the next step, right? You see someone actively using it in addition to the fact that. There. They're playing football, they're able to do their thing. So we obviously not talking about football today, but I let you know the promo video's a good setup for this.
So maybe, uh, kike you can kind of explain to the, the viewers and stuff kind of what this is. 'cause here, this podcast, we focus really, we get a lot of guest requests and we don't take many of them because the focus is on sports, medicine, rehab, and athletics, and how it all mixes together. How can you make my job easier by not having to constantly fix these ankle surgeries and or deal as a team physician?
As you know, you've worked with, I'm sure all the team physicians for those teams. They're really good guys. Uh, but it's a pain in the butt, right? Like double time of rehab. These ankle sprains are not fun to treat, right? Yeah. It's just you can't fix 'em all the time and you're just waiting and waiting for them to recover.
So kind of talk about the better guards and your stuff.
Keke Lyles: Yeah, I think, uh, so one of the things that really stands out and is unique about the Better Guards Brace is that it's [00:10:00] actually quite flexible. And, and I have one here so I can just show it like, you can see, like, it looks like, yeah, that's super flexible.
You know, that look like that
Dr. Grant Garcia: looks crazy.
Keke Lyles: Yeah. And so, like, when you put it on it, it really feels like a compression sock, which is great. I mean, because it, it, it allows freedom of movement. And so that
Dr. Grant Garcia: slide, while he's talking.
Keke Lyles: Yeah. And I know when I grew up playing sports and had my fair share of ankles, pants too, like I used to wear the, the like the really thick ankle brace that pretty much restricts all movement.
Um, and even as a kid and I just didn't like it, you. No even, well, those are pretty bad too. But even the, you know, the, like the ones after you have surgery where you, you know, they're just plastered on the sides. You can kind of dorsiflex and plantar flex and that's it. Um, and so I think having this freedom of movement is, is the thing that at least the athletes love because it's like they don't feel like they're wearing an ankle brace now.
The protection. Their tagline is, it's [00:11:00] a, a seatbelt for for the ankle. And you can see it in the picture there. But what it has is, and the technology is pretty cool, is this little piston on the side there.
Dr. Grant Garcia: Go to that slide. There's a slide there. I wanna show the viewers this. This is cool. Yeah, I mean, you guys can see really quick, we can see all the people that use this.
It's pretty fricking awesome. So yeah. And all these other things, but go to the, the tech, the tech slide is really good. Keep going.
Keke Lyles: Oh, with the different braces. Oh yeah. Here we go. So here's, here's like, the magic is that little piston. And so even the one I'm holding, like you can kind of pull it out and you know, it's not that big of a deal, but when you go fast, it locks up just like the seatbelt, right?
You can pull a seatbelt on nice and slow, buckle it in. Oh, but when you go to pull it fast, it locks up. And so that's the idea here with this little pissing and, and how the brace works is it allows freedom of movement. But when there's a sudden. Roll of the ankle, quick movement, then it stiffens up and protects the ankle.
And so that, that's really what sets this brace [00:12:00] apart. Um, it's really unique and obviously genius designed by the group, uh, in Germany that created it.
Dr. Grant Garcia: That's awesome. And then in, so like in here, this is, it looks rigid only because of the way you guys had to make it for the 3D, but your one is like so soft, so it's like almost like a sock kind of material.
You said neoprene. And then it has that one hinge or the piston?
Keke Lyles: It has the one piston, yep. And, and what's different? You know, I was talking about the different versions, like you can see here, like where this little, uh, bracket is. Like some, some athletes would complain, like they could feel that bracket.
And so they've, they've moved that up on, on the 3.0 just to make it more comfortable. So it literally feels like you're just wearing a compression sock.
Dr. Grant Garcia: Awesome. And then, um, yeah, keep going while you go.
Will Sanchez: Yeah. Yeah, I, no, I just wanted to kind of bring it up. Did was some of the inspiration or, um, any of those conversations, obviously you dealt with Steph Curry, right.
And he had, I mean, he's probably, besides Grant Hill, one of the most famous athletes that I can remember, [00:13:00] that we actually considered or was concerned that he may not have a career because he had so many ankle injuries. Davidson, 2011, he had a bunch of injuries. 2012, he, I, I believe back to back years, he had the surgery while 2012, they went in, they cleaned everything up.
Um, and there were a lot of concerns. So working with him, working with the, with the team doctor, you know, everyone involved, was there some inspiration on that where you saw firsthand like, these are the problems that we deal with and with my expertise, I can give that feedback to a company like this.
Keke Lyles: Uh, it was a little bit of that, although by the time I met better guards, they had already designed it.
Um, and so I was, I was more of like the, the assurance of like, yes, this is gonna make a difference. Um, just working with all the guys that I've worked with, like wishing we had this back, you know, in 20, I joined the Warriors in 2013, so right after Steph really had all his surgeries and everything like.
We were exploring everything on the market [00:14:00] back then, uh, obviously, and that's what you do in the team setting. Like you, you kind of have to leave no stone unturned. Um, and so yeah, I wish I had this, uh, like I said, when I first saw it, I was like, this is a no-brainer when you put it on, feel it, start moving around, feel the protection.
Uh, and so, and I think that's why they're having the success. Like, I mean, it's, it's blown up really in the last year. I mean, it's going off like gangbusters now. Hmm,
Dr. Grant Garcia: kk, will you describe to the viewers? You know, I could do like the surgical side of things, but I think from you being the performance coach, like you guys.
I mean, this is actually a really cool side conversation that we can have with the viewers hearing this, because what they don't understand is that the conversation between the doc, the team doc, like myself and the performance coach is actually really vital. And we do that a lot behind the scenes, as you know.
I mean, you probably spend more time with the doctors than you even do with the players sometimes. Yeah. Like, Hey, what do I do here? I tried this. It's not working. What are your thoughts? This is all a team collaboration. And you know, it's funny, most of the doc, most of the teams think the docs do all the work and they do like very little comparative to people like you.
Like you do most of the work and you're the one [00:15:00] that's like doing all the titrating and you're like the chemist, right? Yeah. And I come in, I'm like, Hey, listen, may not surgery, may need surgery, but you're the chemist. I'm like, what do you think? Yeah. You know, it's always like you're the ones in charge.
Yeah. So it's really, so how would you, so before this, how would you rehab or try to prevent ankle injuries, these sprains? 'cause they're so common. And then let's talk about after.
Keke Lyles: Yeah. So I think, you know, yeah. Um, I, I think you're right. I probably did have more conversations with our team docs than, than the actual players.
And part of that is, you know, we're working with athletes every day, um, and so we kind of have an idea of their strengths. Well, we better have an idea of their strengths and weaknesses for sure, but how they're moving, how they're responding to different things that were thrown at them. Um, and so we, we kind of have that intimate knowledge, and then we have, you know, obviously when the team docs gets involved, it's like, okay, this is what we're seeing as a performance staff or as the medical staff on the, from the team side, right?
And we're saying, Hey, you know, he. We may look at force plate, we can look at balance, we can look at, you know, use [00:16:00] all the technology in the world and then use our eyes on the court. This is how they're moving, this is how they're responding. Uh, and then when we kind of have this conversation with the team docs, it, it, it's really about, okay, from a medical standpoint, what.
What can we do? What are our options? Right? Surgery, yes or no? Um, is it some sort of orthobiologics, some injections or something like that, right? That can this help or that help and um, or we bring in a podiatrist and what can we do to the footwear? Um, what, what is his current footwear or her current footwear, and how is that affecting their kind of biomechanics?
Um, and so what we try to do is have this really holistic picture of like, okay, here's what we think is the problem. Here's ways we can address that problem. And depending on, you know, the athlete, where they're at, uh, where the injury's at. We may be super aggressive or we may be super conservative. Um, and, and so that's part of the conversation as well.
And so we take the plan, we go back, we implement the plan, and we start working on it. And then, you know, depending on how the, [00:17:00] the athlete's responding, we we're gonna have to adjust. And sometimes that goes well and sometimes it doesn't go well. And so, you know, an example is we may. We may know surgery is an option, but we may not want to go there first.
Right? And so we're gonna try some of the other exercises and, and kind of building up, you know, you asked like, what did we do before this? And it's really building up like the foot and the ankle. Muscles, but it's also like the whole kinetic chain, like all the way up, um, how they're implement or how they're using their movement strategies.
Do they load their hips or are they very knee dominant? Um, and all these things that, how someone moves will determine, you know, our intervention. And so. Sometimes that intervention works, but when it doesn't work, we say, okay, I think we need to go to surgery. Um, and and that's where having the team docs involved in the process.
'cause they know what we're trying, they kind of sense, hey, this is probably going down the right path, or Hey, this is not. Really going down the right path. Let's jump in now. And I think with [00:18:00] athletes, it's like you, you know, if you have to have surgery, then you want to have it sooner than later, but you don't wanna have it too soon if you don't have to have it.
Right? So, well, I think that's, I think that's an important point
Dr. Grant Garcia: too. That's a really important point for people to hear right From, from, because they can hear it from me. But hearing from you. The when to do surgery sometimes is really challenging. Decision motion too, right? Yeah, because like, yeah, they wanna get fixed, they wanna get back, they wanna get back on their contract or win the championship or whatever else they're gonna do.
But you also don't, that's the art, right? That's the art of working with guys like you. To decide if this is the time to, to pull the trigger. And you know, all these sports docs you see that come outta school and they're like, I'm gonna be a sports surgeon. I got this. And then you get to like team coverage and you're like, whoa, this is totally different than what I learned.
Right? Like the book answer is like, if you tear this, you fix this. Not in professional athletes, it's a whole nother, there is like a different category, which there is no book written for it. And it's feel, and it's learning with your team and it's why like. It's funny, we're used in the operating room being kind of like control of the thing.
When you're on a team, like the team doctor is like, let's talk to all [00:19:00] the other people like you guys. Tell me what you need. I'm here as a resource. You gotta put your ego down when you work with the professional teams and it can be challenging for some surgeons. So the important part is to like, it's a team environment, but jumping a little forward.
So talk about what do you think now with, I mean. People still probably get some sprains of this. Maybe not. We can show the data, but like do, have you noticed, like, we'll look at the data in a second, but have you, what would you say now, like if you, I know you work more with the company, you've done a little less with the teams in the last few years because you're more of the consulting.
But what do you think a team now having this product would feel in terms of their rehab or how they're feeling? Like, is this a, is a product just if you sprain your ankle, is it a preventative thing? Use it for both. Or like, what I care about too is like you sprain their ankle. Let's say the player doesn't wanna use it, right.
They're like, I don't wanna use this new product. Which again, some people might won't want to. So they sprain their ankle or they injure their ankle. And then do you use this afterwards too? Like what are the uses for it?
Keke Lyles: Yeah, so, uh, definitely a couple, a couple good points there. You know, being a new product, uh, [00:20:00] you can imagine, especially professional athletes are like.
There, there's a handful of guys who are just like, no way I'm wearing that. Uh, it's new, right? And so, um, they, they, they had to find the right players who were willing to try it and, and give it, give it a shot. Um, and that's been happening over the years. And I think that's why I'm saying like, there's been a lot of growth this last year because now like players and athletes across leagues have been using it and getting more and more comfortable with it.
Um, and, and I think, you know, the biggest thing is you, what you see is, yeah, you can still, obviously if you land on someone's foot, right? Even if you're wearing this, like you could roll your ankle. Um, but what, what we're seeing and what the data has showed is like, it's, it's a major reduction in severe ankle sprains.
So now you know potentially what might have kept you out for four to six weeks may only keep you out for one to two weeks. And obviously, you know, that that's huge for us. Like it's huge for the athlete. Um, and then the other part is, is yeah, if an athlete [00:21:00] really doesn't wanna wear it, um, you know, as a protective mechanism, they can certainly wear it post-injury.
And the reason that's valuable is, is because it gives you the natural mechanics and, and the freedom of movement like. You're not compensating, you're not developing an abnormal movement pattern. And so you get the protection of, you know, the athlete feels the proprioceptive, protection of the compression, obviously the pistons there.
So if they were to roll it, it's protected. Uh, so that's why they're seeing, uh, an increase in return to play from a normal compared to not wearing it post-injury.
Dr. Grant Garcia: Awesome. So, yeah. So can I ask clarifying, so you're saying. So the, let's go 'cause let's try to convince more people on this show. Like that's better, right?
Like players that are already using it, they know it's better, right? Yeah. That's the easy one. Like those are on hard cells, but the players that aren't using it or the people that aren't using it. So you get, let's say you get, we can already show the reduction in risk injury, and I wanna talk about that.
That's an easier discussion. Let's say you get injured. So if you were the performance coach, let's say you're back on the [00:22:00] Warriors, right? Player gets injured right away, they injure their ankle, they're the ones that didn't want to do it. And you don't wanna say I told you so, but you just wanna say, Hey, here's what I would recommend.
So how would you rehab a player now with this brace?
Keke Lyles: So as soon as they injure it, uh, we'd get 'em in the brace and have them wear it just all the time walking around everything, you know, and depending on again. Okay. Yeah. Depending on the severity, you know, if they're not walking yet, they can still wear it.
Um, and, and develop that confidence in it, that it's gonna protect them. And that's what the, the study showed a, I think it was 54% faster return to play with wearing the brace. Yeah. We pull that after the injury. Um, and so after somebody gets, gets hurt, that's awesome. Yeah. 54% faster. So you're essentially half the time.
Right? And, and that, that is huge for, uh, any athlete to get back. And so I, I mean, we we're still gonna treat it the way you would treat any ankle sprain, right? You're gonna do all, you know, whatever you have access to, you're gonna [00:23:00] do what you nor normally would. We're just adding the brace on.
Dr. Grant Garcia: Do you, do you see, again, I know, I know.
You work with a company, probably not on the floor, giving these out every time, but in what you've heard anecdotally from the athletes, this 54% return to sport faster, do you feel like they're just, they're meeting all their checklists? Like is that, is that what's getting them back faster? Like, Hey, listen, you no longer have pain in there.
You're able to run with confidence you're not limping, right? 'cause there's always a return to play protocol for all these things. Concussions, acls, you name it. So are they, basically, you're saying that they're, they're beating, they're checking the protocol faster with this, roughly. Yeah.
Keke Lyles: Right? Yep. Yeah, that's it.
And I think the biggest thing, like when you compare, just anecdotally, like in my experience, uh, before kind of better guards, you know, this like early 2000 tens, like when someone rolls their ankle sprain, you know, rolls their ankle has an ankle sprain. Um, you know, around like the three or four week mark, they're feeling pretty good, but they, it's always that last like 10 to 15% that just seems to [00:24:00] drag out forever.
Um, and I think to me that's the biggest thing that's changing is like, this is all happening much quicker now. And you hear athletes use the word, like, I just feel so much more confident in it. Um, and so I think that's a huge aspect, like, because it's protecting them because they have their normal kind of, um, biomechanics at, at the foot and ankle, like they just are confident in, in returning to play.
And I think it just gets 'em over that last 10 to 15% much faster than what they previously did.
Dr. Grant Garcia: Right. So you just, you're just gonna see less long haulers. I mean, we've seen these, N NFL is notorious for it, NB a's notorious for it, right? The, the guys are like, they should be back, you know, like you see the ankle sprain and you're just like, you know, will and I have talked about this injuries.
You're like, is this gonna be a one or two weeker or is this gonna be a six weeker? Is this gonna be half the season? It's crazy 'cause it it, for injuries that I deal with, it's kind of on a minor level, right? 'cause it's a sprain.
Keke Lyles: Yeah. But they're
Dr. Grant Garcia: so, they're so frustrating to take care of and so, and there really hasn't been a good eye mean.
Doing surgery is all great, but you're out for a [00:25:00] while and like, you can't just do surgery on everyone. That's not the right answer. Right? So like, and you can pump them as much biologics as you want, but it's still not the answer. I mean, we will to her to say so many times, prevention. Is by far the best medicine for injuries, right?
You can prevent it if there's something you can prevent. If I had something to prevent all my injuries, I would give it. Like if we had a better brace for acls to prevent tears. The data's not there yet, right? Like skiing and I think MCLs and linebackers or in, um, and linemen. But this, this is pretty awesome.
We'll pull up that. I wanna talk about injury prevention now because we're kind of talking about it, but I wanna run through that number, uh, that 40% or think there was something like that up there. Can you pull that up?
Keke Lyles: Yeah. And as you're pulling that up, you know, the one thing, I'll tell you a story, like we had, we had a guard, uh, who is a chronic ankle sprain, you know, guy his entire life.
And I'm sure you see this and I'm sure people listening, you know, there's gonna be a handful of people of like, just sprain their ankle over and over and over to the point where there's really, there's no integrity of the [00:26:00] ligament anymore. And we, we had a guard who came down on someone's foot in the middle of the game, in his lateral malleolar.
So the bone on the outside. Hit the ground. I mean, he rolled it so hard that it hit the ground. And everyone heard that from the, and we, we thought he just broke his ankle. Uh, and, and so at that point, like, you know, what kept him out was the bone bruise, not the, the, the ligament damage. And so that's the other part of this is like if you just chronically or spraining your ankle, like the integrity of the ligaments become.
You know, gone useless. Yeah. And, and now you're dealing with these bone bruises. 'cause when you roll the ankle, you know the bone is hitting bone and, and, and that's usually their pain. And those can take forever. And, and, you know, and, and there's not really anything you can do with bone bruise other than like, we kind of just deal with it and eventually you gotta work your way through it.
And so that, that's another reason. To your point. Prevention is so key because it's like if you get to that point, it's just really difficult.
Dr. Grant Garcia: Well, and also the surgeries are long and not always successful. [00:27:00] This might be a good segue will at some point to have our, our in-house Dr. Yi, on the episode to talk about this for the full ankle.
Ankle, but like, it is a good point you're making, I mean, right. You have no, when your ligaments torn, it's no longer there. You basically are adding another ligament. I don't wanna oversell the product with the piston. The idea behind that is like, that's a cool, I'm sure that's not like a super common injury.
Like it's common, but I'm sure it's not like the, so it might be hard to study, but the idea behind like the, it's more than just about ankle sprains, right? Only the public only sees ankle sprains. Like, we all know this, well, we've seen this on the injury report. The injury report's like, yeah, uh, he's got a knee sprain.
It's just bull. It's not a knee sprain. There's something really wrong with his knee. They just don't wanna mention it. So it's like he's got an ankle sprain, but he may have much worse than that. He may have a high ankle sprain, he may have a bone bruise there. And obviously that scares the people, or it can change the perspective of the team.
Um, but you know, there is more that these can prevent than just that alone. Um, do you, and do you say like, so if someone has this, would you recommend both sides or just the injured side? How does it work for you guys? Like when your players have done it, what do they usually do?
Keke Lyles: Yeah. Um, [00:28:00] there are some, some athletes who are just really concerned about 1, 1, 1 foot, one ankle.
Uh, but the idea to, you know, you said it and that's what we preach. It's, it's prevention. So it's like, why would you not wear it in both? And I think, you know, traditionally what athletes are used to are these more bulky braces. And so for them, the idea of wearing on both, they're like, I don't want to do that.
Like, forget that. But then once they try it. The better guards and they're like, oh, this is comfortable. Um, you know, the adoption to use in on both seems to be much higher,
Will Sanchez: but what's the best feedback you've gotten from a professional athlete wearing the product, you know, with someone you know, with a word of mouth or directly to you where you went, man, that, that, that was pretty good.
Keke Lyles: I think for me, honestly, it's just hearing ev like every athlete say, like it feels like I'm not wearing an ankle brace. Like I'm not, you know, it doesn't take up all the space in my shoe. Um, it, it just feels normal and I think like, and at least when I hear like. An athlete say it feels normal. Like that's [00:29:00] huge because I want them to be comfortable.
I want them to express their athleticism, do everything they want to do. I don't want them thinking about, oh, I have an ankle injury or an ankle problem, or I got this big, bulky thing in my shoe that I have to worry about. So for me, uh, that's huge.
Will Sanchez: Across the board. So you could wear this with low mids and high, right?
Yeah. So it doesn't matter if, if KD has a line out and he's got some mids on, or somebody's wearing high tops, which I'm not seeing a lot of high tops, but that's a whole conversation. Yeah. You know, this so low. So this, this, um, ankle protector can, you could wear with any kind of shoe. So if they have endorsements, sponsors, it's not gonna affect them because it is.
Not bulky, it'll fit with anything. Right. So that has to be a plus as well. 'cause now we're talking about money sponsorship, your own brand. Sure. Right. We're thinking big, big picture when it comes to something like that.
Keke Lyles: Yep. Yeah, I mean that was, it's funny that you mentioned some of the sponsorships.
'cause even like the early adopter. Players in the NBA. Um, you know, that was a big [00:30:00] talk, like where the better guards kind of logo is. Can it be shown? Can it not be shown? Like there's lots of rules around that. Uh, and so That's crazy. Yeah. But yeah, you can wear it with whatever you want. And I actually had a guy that I was working with just two years ago.
Um, who, who had an injury? You know, like I think most athletes, like when they're at home, right, they wanna wear sandals and everything, and it's like, just wear the brace even when you're wearing your sandal. Like, just wear it. Um, and so for them, they're, you know, they thought that concept was formed, but then they loved it and, you know, they saw the results.
So, uh, that
Will Sanchez: always helps. Are you doing multiple colors for like, you know, let's say it's golden State, you got the gold, or are, are you doing things like that? The bucks green or purple? What? No. Right, right,
Keke Lyles: right now it's white and black are are the options. Um, yeah, and mostly because, you know, especially at the professional level, it's a lot of like color of the socks and team socks, what's allowed, what's not allowed.
Mm-hmm. Um, it's more around that, but yeah, I, I'm sure, I'm sure as the company continues to grow, especially like for youth, [00:31:00] uh, you know, it's gonna become like style. So for sure.
Dr. Grant Garcia: Uh, kk do you, one thing we noticed, we talked about the Guardian helmets on one of our episodes and some of the things how the NFL now is saying, Hey, listen, you know what, like you probably need to wear this.
And like, they start recommending it. Like, what do you think the data's gonna have to show on this thing before? I mean, like if I'm a team owner, right? And I know that my players had six ankle sprains and they refused to get surgery and I just paid this guy 20 or $30 million a year. He doesn't wanna wear a brace, that's still a relatively reasonable cost.
When do you think the owners say, you know what, it doesn't really matter if you don't like it or you don't wanna use it, or, not that, not like it, but like when does that, but like at some point some of this technology comes in, right? We know about this. It sucks. But then when the player gets, kind of forced into it.
But like if you guys eventually show that, I mean that's, that would be obviously amazing for you guys to have that sort of reputation, that it's so good that the owners think you need it. But like that could be a situation where you're at Theron coach, like, listen, [00:32:00] are you di of getting ankle sprains?
Like you're gonna be outta commission more. Like you need to try this. Like you, you don't wanna lose any more money on your contact.
Keke Lyles: Yeah. And I, I, yeah, it's an interesting question. And that's where it's like you gotta get the players union kind of behind it as well. You know, there's one NBA team that does force, uh, players to wear ankle braces and like knee pads for practice.
Uh, and, and there's a lot of pushback initially, but now it's the culture there, right? Um, I've been involved with conversations with players that previously did not wear any sort of ankle protection, uh, who've had, you know, recurrent ankle injuries and it's like, okay, ownership does get involved and say, Hey, we gotta do something right.
Like, nothing, like we can't, no longer. Do nothing. Uh, so let's work with the athlete to figure out what's gonna work. Uh, and I think better guards is gonna ultimately start winning a lot of those kind of conversations. Because again, if a guy who, or if an athlete who doesn't like wearing ankle braces, puts this on, it doesn't feel like an ankle brace.
And so now they're like, okay, I'll try this. [00:33:00]
Dr. Grant Garcia: We'll pull up that slide to show the comparison. I mean, I know we kind of talked this in nauseam, but you can do like the mobility high, low. Uh, you have one more?
Keep going. Keep going. Right there. Yeah. Yeah. So you can see, I mean, this is what we have option wise, right? Like, I mean, you've got, there's some fancier looking ones, but nothing does what this does. No one has. The key is you check off all the highs, right? Yeah. High protection, high mobility, high comfort.
You have to have all of those. The problem is it's really easy to get the fir, the second two, if you have no protection. Yeah, exactly. So you can do, so you gotta have, it's like, it's like the, it's the mix of the two. Um, and so, you know, like when someone, when a player's looking at this, right? That's their alternative option.
So it's a huge niche too, right? Like underserved. Which is why I think the technology is so cool. And having you on here discuss this is really cool 'cause it's something we talk about and we have not seen anything in the news or anything that's been other way to like help this. And the negative of anco sprains is that they're not like sexy, right?
Like the Tommy John surgeries or like the. [00:34:00] ACL tear so they don't get as much publicity. But right now you can see it right here. But the big data shows that obviously it's a problem. I mean, one in, one in four NBA players injure their ankle each season. That's crazy. And it's the most com, as I mentioned, like if you just take, it's agonizing how many of these you see.
Keke Lyles: Yeah, no, and, and you know, that's the other thing, like a player may kind of sprain their ankle and it might be a pretty minor sprain and they miss a week and you don't think much of it. But then it happens again in what we were talking about. Earlier, it's like these recurring ankle sprains and how much worse it gets each time.
And so it, you know, I think a lot of people think of it like the first time anyone sprains their ankle, it hurts, right? Like they're crying. It hurts so bad. Uh, you ask someone who's like, sprained at the 10th time and they're like, yeah, it's not as bad, right? And it's like, that's not a good thing. Uh, that, that, that's much worse than what, what people think.
And so. Um, yeah, I think there's, you know, obviously a massive opportunity to help athletes across, [00:35:00] across sports to kind of, you know, get ahead of this. Are you
Will Sanchez: seeing, um, any, I I know we're talking about the ankle, right. But you know, the big conversation this past NBA season was the Achilles. Yeah. Right.
And are are, is there any data or anything that leads up to, like, let's say, if. You, you have a bad sprain on your right ankle and obviously Dr. Garcia is right up your alley here. You know, uh, it's right, you know, spraining your right ankle, it's not healing right now you have some soreness in your calf and you know, now you're leading into other injuries.
Is there any data that kind of shows any correlation with that? And I know we're talking apples to oranges. As far as the injury uptick that happened this season, I believe it was seven NBA players had Achilles injuries. Nine altogether, including the two players that got hurt in, uh, summer ball. I forgot their names.
So I don't know. Or was, am I going off on a, a whole different, well you're going
Dr. Grant Garcia: off on a tangent, but you, like I always do. But you're helping with a [00:36:00] question would be, I would rephrase it 'cause it was so, it was well put. But I would add a question in there to say, is there a future for better guard's, piston and other.
Opportunities. I'm not trying to give away your future RD. Yeah. Um, but you know, the idea is if it works that well on the ankle, why the hell wouldn't you use in other places?
Keke Lyles: Yeah. So I think to answer both of those, um, you know, I, I don't know if there is clear data that shows ankle injuries to like Achilles injuries, but for sure, like there's plenty of research that suggests after an injury, you know, movement patterns change, which then, you know, can affect.
More, uh, other injuries, right? Uh, and so I think there's a, a link there for sure, uh, to some degree. Um, not to say that all Achilles come from prior injuries, but for sure, and that's why, you know, restoring normal movement is so key. Uh, and that again, that why I was personally excited about better guards.
Um, and then yeah, to your second question, yeah. They're already exploring the pistons in, in different, like knee braces, elbow [00:37:00] bracing, uh, there Yeah. There's lots more opportunities to kind of apply this technology to other joints.
Dr. Grant Garcia: Yeah. This is cool. I'm already thinking about some things in my head. I like the, the MCLI like some ACL stuff.
I mean, if you have a brace that smooth. And then you've got an acute piston thing like that is pretty sick. I, it's funny, when I looked at your product, I, I saw the piston and I learned about it, but I didn't really get it until you showed it. So today is pretty cool. It's a little eyeopening. Um, so hopefully for the listeners too, they can see it.
I think, I mean, like I said before, like the idea of putting, like, to me, like I put on these ankle braces before the old ones suck, right? Like the stiff ones, they're like this. I like, I wouldn't wear it. Like, I'm like, but if I had something, I'm going out and I have a loose ankle. The other thing is like a lot of people don't want surgery.
I mean, no offense, but like I do a lot of surgeries and like you just don't wanna have surgery on your ankle. Ankle surgeries are hard. They take longer to recover. The blood flow's different down there. Listen, I have tons of friends that have had ankle surgery. They do well sometimes, but sometimes they don't.
And so it's like, yeah, if someone's like, well, [00:38:00] why would you just do the ankle surgery? I'm like, it's not a hundred percent right. So if you have something that's preventative, like, I'll be honest with you, if there was a brace good enough to stop people from dislocating their knee with acls, there probably would be less ACL L surgery.
Right. Like people don't want surgery. They'd rather wear abrasive. It's comfortable. And so another point you made, right, that person with the chronic ac, the chronic ankle, they probably should have gotten surgery, but they're not ready to, they're an NBA player and they don't wanna take the risk. So like that's another important point.
Or athletes, they don't wanna do anything until they're done with their career. So that's even more important.
Keke Lyles: Yeah. Yeah, absolutely. Yeah. It's funny, uh, you know, coming from physical therapy background, like I, we, I think myself, but I'm sure plenty of others like view surgery as like a chance to reset everything.
Like sometimes there gets to a point where it's like, you need the surgery, you need to reset, but it's like. You have to put in the work, right? And it's like the rehab is, you know, just as important as the surgery. Like if you just have surgery and do nothing, it's like usually those patients don't do very well.
Dr. Grant Garcia: I, [00:39:00] I, dude, that's exactly right. Like I spend my time in the office. I'm like, my job is like an hour or two hours, maybe I talk to you a few times afterwards. And then all the work is done with the physical therapists and strengths and conditioning coaches. And so you don't put the work in, you don't have patients, same surgery, same surgeon, four different patients, same day of the office.
Two are killing it. Two, were not killing it. Exact same technique. There's a reason. There's a lot of reasons there, but one of them is the work. There is a really, there is a difference and it's hard, you know, and you get to the bottom of like, and they won't bring it up with you. Maybe you, in the professional level, they tell you, but in that one or two instance, if you're seeing them, they might not say, oh, I stopped doing my stuff, I only do it once a week.
Right. You're like, that makes sense.
Keke Lyles: Yeah, and I think that's the big difference between professional athletes and general population, like professional athletes, like they have teams of people to take care of them and making sure they're motivated. Obviously it's their job to be out there performing, uh, where the general population, like you might see a physical therapist to three times a week [00:40:00] post-surgery.
It's just not the same level. And then, you know, life gets in the way. You're busy. I got school, I got the, and then now next to your point, like you can have the exact same thing and have some patients do really well and other patients do really poor. Uh, and so it's like if you can just avoid all that to begin with, it is so much better off.
Yeah.
Dr. Grant Garcia: Well, and I think. I actually think as much we talk, we keep talk the professional stuff's super sexy. Talk about like, you hear the word NBA on a podcast and you're like, oh, this is interesting. Right? But like, to be honest with you, this is probably be more important for non NBA, right? The kids, right?
Because like Curry's talking about Davidson, right? Like that's before the NBA. So like you have like this is the end. Once you got to the NBA, you like, we've seen this in Tommy John's. I do players all the time. These young high school players, they have trash ucls, right? Can we prevent these before that even happens?
So like, is this kind of like the concussion protocol? Like let's get these ankle sprains down at the high school level. You know, and I think that's something has what's better guard's thoughts on sort of the [00:41:00] education? Obviously they're doing well with the marketing and the products. They've done a good job with the design.
Like how does that work? 'cause like that's a hard part, right? Like you can only market so much, but you really gotta get the, the buy-in and, and the lower down.
Keke Lyles: Yeah,
Dr. Grant Garcia: athletics or the high school athletics or college is honestly more important sometimes.
Keke Lyles: Yeah. And I think actually the, you know, this year I think is a big opportunity for them.
They did a, a big partnership with the NBA Athletic Trainers Association, uh, kind of built around this of like, how do we spread the word to athletic trainers? Across, across, you know, across sport, across levels, you name it. Um, you know, being the NBA Athletic Trainers Association, they, a lot of people look up to them and Okay, what are they doing?
Yep. Right. What, what do they have? And so I think that partnership's gonna be huge to kind of reach the, the high school levels and that, that's part of the mission of the brand too. Like reaching kids at a younger age. 'cause Yeah. Obviously if we can prevent it much younger than those, those kids are gonna have.
A, a better career, whether that's professional or not. Right. And, and they're, they're not gonna be dealing [00:42:00] with pain and injuries as much. I think that's a win-win.
Dr. Grant Garcia: And then, can I ask, I mean, I'm assuming you guys did NBA, 'cause it's probably one of the highest ankle sprain populations. Yep. Um, and that's been your focus.
And then obviously, I mean, I'm assuming you're branching out to other sports. I know you've got a lot of other sports on that list. Yeah. Um, but your focus has been NBA because of the highest, it's one of the highest ankle sprain populations. Is that correct?
Keke Lyles: Exactly. Yeah, that's kind of the initial focus.
Uh, football, NFL, like it was surprising. Athletes responded really quick to it. Um, baseball had a quick response. Um, and then what was really interesting, and I, I work with a couple of soccer players. You know, soccer is so unique because those cleats are so small and compact, um, that like ankle braces are just.
Out of the question. Um, if they do anything, it's usually tape. And you know, most tape is like after the first like 10 minutes, whatever kind of protection it provided is not there anymore. And so now we're seeing as soccer players are starting to get exposed to it, like, oh, this can really help. Um, you'd be surprised, you [00:43:00] know, ankle.
Ankle sprain or you're not surprised, but the, the listeners would be surprised. Ankle sprains. And I'm surprised soccer players are super hot. Surprised. I like it. Yeah.
Will Sanchez: I mean, our famous, I had no idea. That's awesome. Williams. You know, she always had her ankles, you know, uh, you know, braces and things like that.
So, you know, tennis also is probably a great sport. We just saw Roland Garrels where they're running back and. Forth and do it splits and sliding, and I don't, I don't understand how they're not having, uh, higher ankle injuries, but let alone maybe on the lower level they are. So that's an interesting support as well.
Dr. Grant Garcia: I, I think it's interesting too, you always notice on this. Podcast. He always said, you learn something, right? Well, we learn so much from everybody about these different sports and the injuries and no matter how much you think, you know, you know, this is why, like getting people on, talking about this stuff, hearing the details, it just really breaks everything down to understand it better.
Right? It's not just a product. It's like, no, this is a product that's been tested, it's been revised, it's been improved. We're on [00:44:00] 3.0, um, with two more follow up and I want to kind of let you go so you're not being on all night. Uh, first one is like, so I know we kind of advertised for the 2.0. Initially when I was working with you guys to kinda get this podcast set up, it was a 2.0.
Now you get a 3.0. What's the difference in the upgrade? For the 3.0.
Keke Lyles: Yeah, mainly the positioning of, of this little part here at the bottom. So that, like I said, like some players, and I think it was really dependent on the type of shoe that they're wearing. Like they would feel like it kind of dug in and so they moved that up and outta the way.
So it's just, yeah, totally removed that. Um, but no change in the
Dr. Grant Garcia: PIs.
Keke Lyles: No, no, the piston's the same. Yep. And so that, that's the same, that's, uh, tried and true. So no, no reason to change that. It's really just creating more comfort around the brace and, um, they did relieve the 3.0 is out now, so everyone is, is getting that now.
Okay.
Dr. Grant Garcia: Perfect. And then I would say, sort of, kind of follow final up question. And then I know Will's maybe has a fun question or something, who knows? He's always got something hidden there. The, uh, the, what's the future? I mean, we kind of talked about it, but what's the future for you guys? Where do you guys [00:45:00] see yourselves in the next three to four years?
Or what do you wanna do for these products?
Keke Lyles: I think, you know, as we mentioned, like it's definitely gonna be, um, some expansion into other joints, protecting other joints. Um, you know, obviously working with NFL guys like knees are a big, a big issue. Um, and just alignment, like you, you said it, MCLs are like, I think it might be the number one injury for offensive and defensive linemen.
And so if if there's a way to help protect them, uh, yeah, we're gonna do it. And so I think. Exploring what other joints, how much of a difference we can actually protect you. You mentioned the UCLL in, in the elbow and, and pictures like, is there something here? You know, we're exploring that and so I think that's gonna be really interesting.
Uh, and then just generally, like the more adoption, the more people are hearing about it, learning about it, uh, and understanding how beneficial it it will be for them, I think is, is gonna be the real focus. Awesome.
Will Sanchez: Great. Um, I'll do a two part question. Um, when you first came over, right, and I believe you, you mentioned you came over for the [00:46:00] Minnesota Timberwolves.
You show up to Golden State Warriors the year after the surgery for Curry. Uh, what was the pressure like for you saying, man, I'm coming over here. We know what the bread and butter is for Golden State right now is making sure that we're getting curry back on the court. You know, changing maybe his regimen.
Obviously he got bigger, I believe when he first came in he had some hip issues and things like that. So if you could explain some of that. And my second part is. What did it feel like winning A NBA championship?
Keke Lyles: Yeah, so first part of that question is kind of interesting. So I'll tell you my first, uh, day in, in the practice facility of Golden State, I joined the team during the summer out in Vegas, during summer league and then after summer league, uh, we come in my first day in, um, I won't say who, but it was another player who's dealing with a knee, a knee injury.
And he kind of put me to the test. Like he didn't tell me what was going on. I didn't know what was going on. And I just kind of like, Hey, something doesn't seem right. What's going on? [00:47:00] What's going on? You know? Um, long story short, uh, you know, he goes, you think I need surgery? I was like, no, I don't, I don't think you need any surgery.
And he, he kind of starts yelling, I told you I don't need surgery. I told you. I was like, what did I just, what? What's going on? Uh, so long. Story short, but essentially he, he, he had a, um, a, a small quad tendon tear that the team, you know, everyone's trying to figure out and they kind of had settled on doing a surgery and he was gonna miss, you know, obviously at the beginning of the season.
Uh, he really didn't want the surgery for whatever reason. Uh, and so I was like, okay, I think we can, we can handle this and, and kind of rehab him back. And so, uh, to be honest, like I was. Literally like, am I gonna get fired on day one? Like what did I just cause? Uh, and so thankfully it all worked out. He played, he didn't miss any games that season, uh, the player with the knee, which was pretty awesome.
And so, to be honest, like with Steph though, Steph is such a great like dude and a good person. And, and I think he saw honestly what we were doing with that other player in his knee. And he is like, all right, just [00:48:00] tell me. And I also, I tell everyone all the time, I had the advantage of like coming in when they.
Tried millions of things and it's like, okay, well let's look at this one other thing. It's like, let's just think outside the box and see how this helps. And obviously it's a combination of everything, right? Like it's the surgery, it's his work that he put in on the rehab part of it. His willingness to like do what I was asking of him, uh, to try to help kind of change some of his movement patterns a little bit.
And so it's everything that kind of made it like, to me, the step part was kind of easy. It was the other guy that I was like, oh my goodness, get on day one. Yeah. Good test
Dr. Grant Garcia: now. We'll know that for now on. Good test. Yeah.
Keke Lyles: So, uh, and then winning a championship, I mean, it's, yeah, it's incredible. I think you hear a lot of people say like, there's so much work that goes into, I think any, any sport, right?
Professional sports, like you're in it day in and day out. Um, holidays, weekends, you, you know, I kind of told everyone, like when I worked in the NBA is. Like 12 years, you know, seven [00:49:00] days a week. I've, you know, I got maybe a week off here or there, uh, in the off season over that course. And it's just like, you put so much time and energy into trying to win and it's like one team wins.
That's it. Like it, you know, it takes a little bit of everything to come together. Uh, so it was incredible. Uh, and at the same time it's like, okay, what else? How do we get better? You know? And you get like, that's next year. Repeat. Yep. And that's the thing about sports. It's like you, you win it and you celebrate it, and then it's like a couple days later it's like, all right, let's get back to it.
Let's, how do we get better? So it's, uh, that's just, it's pretty wild.
Will Sanchez: Last thing, um, if you had your choice, when you win a NBA champion Chip. Should you be able to take the trophy and celebrate the way they do with the Stanley Cup? Everybody gets it. You get a few days, you could travel with it, take pictures, put babies on it, whatever it is.
What, what, what, how do you think, what if you could change one thing for the championship, what, what would it be? Would it be something like that?
Keke Lyles: Ah, yeah, man, that's a good question because I [00:50:00] think me personally, and you know, I can't, it's not really fair to speak for players, but I don't think players get caught up in the trophy as much as the fans do.
Like for the fans. It's really cool and it's special to like see it, to feel it, to touch it. But I think for the players, coaches, staff, everyone, it's like, it's the work, the, you know, it like, it's the memory of like the whole process that matters more. Um, so maybe for the fan's sake, it would be cool to travel it around and get it out there.
I think some teams try to like show it off a little bit, but yeah, I, I think for them, for sure, it would matter. I think for the players it, it probably doesn't matter to them as much.
Dr. Grant Garcia: Makes sense.
Will Sanchez: I like it. Uh, listen, thank you so much for your time. Um, as Dr. Garcia mentioned throughout, uh, the show, we, uh, we learned so much.
We're really excited about the product as well. It's very unique. It's very different, and, uh, all the points that you highlighted, it just illustrates why, you know, players should be using it, but just not. Only at the professional level, but [00:51:00] obviously at the amateur level. We'd love to see some high school kids, uh, use it as well because maybe then that allows them, you know, to not have these injuries and maybe their career could go a little bit further.
'cause we've seen so many talented individuals never make it to the highest level. So, uh, Dr. Garcia last words, but, uh, kk, thank you so much. I can just
Dr. Grant Garcia: say, I'm gonna get a lot of ankle sprains outta this episode. Ask me about my better guards. Yeah, no, we gotta show that off in the office. This is awesome.
So anyhow, I, I, I love it. Thank you so much for being on. This is really cool. I love the new tech, um, and anything to help the players and the, the kids and not have to do as many surgeries as good. So, thanks for coming on. I really appreciate it. Thank you. Thank you. Shout out
Will Sanchez: Danielle. Thank you, Danielle.
We didn't hear from you. Thank you, Danielle. Thank you. Take care.
Dr. Grant Garcia: Thanks.
Audio Transcript
Turf Toe in the NFL: Joe Burrows and Brock Purdy Recent Injuries

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez and that man that you see there if you're watching us on YouTube is Dr. Grant Garcia, our orthopedic surgeon in sports Medicine specialist Dr. Garcia. Um, this will be a really interesting, uh, conversation, but an important one. It's been an exciting NFL season unless you're a Giants or Jets fan, so let's not get into that.
Once again, the New York team start out oh and six. And I may need some therapy. I may need something stronger than water, but, um, anyway, how are you? What's going on
Dr. Grant Garcia: outside of the Giants? I'm good. Things are good. You know, it's, uh, unfortunately end of summer in Seattle here, but we're still getting a few [00:01:00] more sunny days and, uh, yeah, it's been good.
Everything's going well. I'm excited to talk about this topic. It's, uh, it's interesting 'cause it's kind of like you hear it, but. You don't really see it that much and you, you heard about it. Everyone knows about it. You know, the doc that's doing a lot of these surgeries. Um, but you know, it's just one of those ones, it's kind of like the hidden, the hidden injury. We don't talk about too much, but it really affects people significantly.
Will Sanchez: Yeah. And before we get into the topic, I mean, we can talk injuries every single week. I mean, we could turn this show into that. We, once again, Nick Bosa torn ACL out for the season cd Lamb High Ankle Spring. We've talked about that in the past.
Three to four weeks, but that's, that can be something that just lingers for a lot longer. Um, an Najee Harris is out with a non-contact football, uh, foot injury. And James Connor, severe ankle injury. We're talking about major, major stars in the NFL that are hurt. We had five quarterbacks last week starting quarterbacks that didn't play.[00:02:00] So this, this is, this is something that reoccurs, it's part of the business. It's why we love the game, uh, just because it's exciting, it's fast paced, but there comes a cost. And with that cost as they get recovery, you know who we're gonna shout out. We're gonna shout out Mike b at the Recovery Shop. Dr.
Garcia, man, let's talk about the recovery shop a little bit.
Dr. Grant Garcia: Yeah, shout out to our sponsors. They've been awesome for the last year or so since we've been working with them, but you know, they're, they're really great. Honestly, I have 'em in my practice and my patients. Always asking about this and always complimenting about this ability to order sort of aftermarket things that'll get them back like the nice machine or, um, you know, more innovative braces or more innovative machines.
Like the Relists, like the ability to have that option in all in one area is really great for your patients from a recovery standpoint and working towards more nutrition, which again, we've had two nutrition specialists that are doctors on this show. So, you know, it's, it's, it's not just about the surgeries.
These cool things we'll talk about. It's about [00:03:00] the. Postoperative care, and that's really what they specialize in. So reach out to 'em. If you're a surgeon, if you're a patient, talk to your surgery surgeon, they might be able to offer it. So,
Will Sanchez: you know, the topic that we're gonna get into is turf toe and um, and.
It's a, it's a great segue, especially what happened with Brock Purdy. He's supposedly going to be out for a few weeks and we're gonna get into some of those things. When I think of turf toe, uh, Patrick Mahomes recently, you know, a few super bowls ago, he played through it. I can't imagine the pain that goes through it, and you're gonna explain why that is.
And then Dion Sanders, you know anyone that knows Dion, that knows about his story you suffered through this injury that pretty much led to amputation of toes. So it is, it is, it has a funny name, turf Toe. It doesn't sound like a strong football player. Should be out for the season or alpha weeks with a name like Turf Toe.
But what is Turf Toe? Uh, anatomically, you know what, what, what, what structures are [00:04:00] affected by this?
Dr. Grant Garcia: Well, so yeah. So let's show that diagram so it's easier to describe to our listeners. Um, yeah, that's a good one. We can do that one first. So we're talking more about the Joe Burrows thing, right? Yeah. He's gonna have surgery now on this.
It's a really big deal, but again, it's so small and you're kind of like, what are they dealing with? And you know, this may be what Malik nabs is dealing with. They don't really talk about his toe injury. He had. Okay. You know, there's all these recurrent injuries you hear about with players, and we'll go into some of them.
Yeah. But basically this is that the first. It's a big toe and where it connects to what we call the metatarsal, that's the long shaft there. And underneath that there is something called a plantar plate. And that plate gets torn. Now, here is not the best anatomy, so if you want to go to, let's go about two slides, I think over one more.
You're perfect right there.
Will Sanchez: Yeah.
Dr. Grant Garcia: So you can see this is again, a really anatomic figure. You underneath that, you have the tendons that allow you to flex the big toe, and then underneath that is a capsule and a plantar plate now, and that tears. The thing is when you [00:05:00] have it on your foot, the most important toe is that big toe for planting flexion and explosion.
And just the tear of this can reduce your explosiveness significantly to the point now where basically you go from an NFL player to to a recreational athlete. Right. And it's pretty impressive that they can be knocked down that far. You lose your explosiveness, and this has been a problem for a number of NFL players, and it happens outside of the NFL too, but this is a big deal.
And so that's what happens here. Now sometimes, which we'll talk about in the potential surgical, you can see there, there's something called these little sesamoids or tiny little bones that sit in the middle of this sort of ligaments. These all these accessory ligaments and everything else. Well, those can be injured too.
With this. Now again, it's like, it's like we talk about a knee sprain, right? It's not just a knee sprain. It may be an ACL, it might be a meniscus, it might be cartilage damage, right? The turf toe has various. Degrees. You can get cartilage damage of the two joints, just like you can get cartilage damage of the knee and you can tear these, the plantar plate and split these sesamoids.
Or you can tear the sesamoids or you can fracture the sesamoids. And so there's various different things that can [00:06:00] happen with that. Now we don't know exactly which one he got, but we know that Joe Burrows is probably a high level one given the fact that he
Will Sanchez: Rock. Rock. Yeah. Yeah.
Dr. Grant Garcia: Rock pretty up.
Will Sanchez: Yep. Um, so how, how do you grade it from a mild to severe?
What are you looking for when you're assessing that? When he comes over from the sidelines saying, you know, I've got the discomfort. Um, what are you doing there?
Dr. Grant Garcia: So the first thing you're doing is you're, you're looking at this and you're trying to assess, like you basically, you're gonna test that ligament out.
You're gonna basically try to extend the, the toe, oh, flex the toe down. And you're gonna, I mean you pretty much can probably make some of your diagnosis there, but really the key here is gonna be that MRI, so to look and see whether or not it's the, you know, what we're dealing with. And so that's first thing.
Is there
Will Sanchez: anything instantaneously, like, you know, obviously you took, you tear. Your Achilles, you squeeze the calf. If the foot just dangles and doesn't flex, then you know that it's, you know, the Achilles has popped. Is there anything that you can see on the field right away, [00:07:00] or is this something that's just a pain threshold and then you have to get to an MR? I
Dr. Grant Garcia: mean, generally your NFL, you're going straight to that. So, you know, that's a combination of, of both and for us to clarify for the players. So the Joe Burrows underwent the surgery just recently and Brock pretty also got the injury. So actually we're talking about two players here.
Will Sanchez: Yeah. Okay.
Dr. Grant Garcia: So Burroughs, it looks like he went actually to the Andrews Institute intra, interestingly enough.
Um. To repair it, but I was under the impression he was gonna go to Bob Anderson. So that's a, that's an interesting finding. But Bob may have flown down there to help out 'cause he's one of the Green Bay Packers team doctors. So, sorry, let's continue on. So the, yeah, yeah. So you're gonna get the, every, all these players, all these players are gonna get MRIs and they're gonna get 'em on the next day.
I mean, when we were taking care of the Giants, we would have Monday morning MRI review of all the players that were injured during the week. Then we'd go through them and say, okay, this is what it is. This is what it is. So they've got the M MRI the next day. [00:08:00]
Will Sanchez: Okay. And then you don't think that's something, if they're at their home stadium, that they could go do?
Well at that point they're still kind of in the middle of the game.
Dr. Grant Garcia: They're not gonna do it mid game probably because it just doesn't make any sense to do it. It's not urgent enough to do that. And it wouldn't generally. Right. It's always about like, what would the management do? Right? You get the x-ray, make sure they don't have anything broken.
Yeah, not broken. Then. And they're good enough to play, then maybe they put that back in. But if they're worried enough in this situation, they're out for the game. Right? And then they're gonna reevaluate on Monday in the facility. 'cause it's kind of a standard practice, right? You want your own radiologist to look at it.
Like a lot of these teams, even if the, let's say all the radiologists, I mean, we know a lot of these doctors, they're all great. Like, you know, they, as much as they like, appreciate the team physician taking a look at their guys, they're like, no, no, no, no. We'll take care of it. This is our team. They're very possessive of their players, which is totally acceptable.
You just wanna keep everything in inside, so they'll fly. I mean, we know this, how this works, but pretty much every time a player, when they finish their game, even if it's 10 o'clock at night, [00:09:00] they're hopping on the private plane and they're flying straight home and they land at 4:00 AM and then they're gonna MRI at 8:00 AM So they're, they're always at home the next day, unless there's some sort of unforeseeable storm, um, that they can't make it.
But it, it, it, they're getting this MRI as soon as possible.
Will Sanchez: Alright, so explain the severity difference between a Brock Purdy that they said, I don't know, ev between two and five weeks, which to me is, that's a pretty big range when you say two to five compared to a, you know, Joe Burrow. That possibly could be the season if they haven't already declared 'em out for the season yet.
Dr. Grant Garcia: I think he's out now because he had just had the surgeries. I'd be shocked. Maybe he'll get back. But we can talk about ways that people are accelerating those. Will Sanchez: Okay.
Dr. Grant Garcia: So you know, you have different levels. You have grade one, two, and three. So you know the grade one is just sort of a sprain. Grade two is a sort of partial tear of the turf.
Turf toe, and that's the mild turf toe injuries. When you do kind of rest, you tape 'em anti-inflammatories. That's about a two to six weeks. So it's a pretty broad range. [00:10:00] Yeah. When you get to severe, that's where we have them full rupture, so he probably had a partial tear of his plantar plate, and so that's why he was in that small level, but now they're finding out.
Again, this is similar to many of the injuries we're seeing that like sometimes when you have these full tears. It's faster to fix 'em and more reliable than a partial and try put the player back out there more than a partial or than just continuing to non-op them, right? Like we know that like some of these players that we'll talk about later continually had non-op treatment.
Non-operative treatment and they would push limp them along for weeks and weeks and weeks, and they re-injure themselves the next year. And now we're realizing with a lot of these things, like, you know, some of these players are the baseball players. It's like, you know, they're just not throwing as well.
Like, we should just pull the trigger and do surgery. Yeah. Yeah. So it's like we're, we're learning more, unfortunately in some cases, that surgery sooner. As much as we wanna be a conservative. Culture that surgery sooner for this with a fresh tissue or with these newer techniques like internal bracing, which we'll get into.
I know you love that word. Oh baby. The, [00:11:00] I need a t-shirt. We, there's just, we do do need a t-shirt. So I mean with that, the, there's no reason why you wouldn't be more aggressive with this. So mild turf tour is different. But this plantar plate rusher, I mean, did you they with burrows? They did, he injured it and like a week later they said he is getting surgery.
So there wasn't even a question that, well, it was clear. The
Will Sanchez: MRI clearly indicated that this is, yeah, we're done here. This is not treatable. 'cause obviously with someone at his level, one of the top three, top five quarterbacks in the NFL, you know that they would say, no, there's just no recovery from this.
Let's go the route of Brock Pur. Let's say it's two to five weeks, two to six weeks for that recovery. I don't know if you could you fully recover when, you know, when you finally get back on the field, you're planting, you're stepping, you're planting, you're throwing, you're running away from very large men, you know people are landing on you.
I, I don't, and it is early in season, not lake, where it like happened with Patrick Mahomes, where he is like, I'm almost at the finish line. I'm just trying to [00:12:00] gut it out. But you still have the whole season. What are the repercussions? What are the, what is Brock Purdy gonna have to go through for this season?
Dr. Grant Garcia: I mean, it's, it's, if he gets back too early, he could chance to re-rupture. Right. And then he is gonna get surgery on it. The other thing is like, does he just play, you know, basically with a, with a lack of push off. Is there some sort of du he's gonna have some sort of bracing on for a while. Even when he gets back, they're just not gonna let him go full boat unless he's completely pain free.
And maybe an MRI shows he's completely healed. Where does, remember the MRIs are only so good.
Will Sanchez: Does foot on a toe, where does a brace go? Is, is it a shoe, is it a ankle stability? What, what do you mean brace? Well, it
Dr. Grant Garcia: depends on the, depends on the injury. But in these cases, you know, they have, sometimes they have these like extended foot toe things.
So it's like a, it's like a, um. It, it's like a, basically like a sole of the shoe, but as an extended toe plate. Like a metal toe plate he might have on there probably wouldn't be able to play with that. Um, but they, you know, these guys have like master orthotics, right? So there's someone in there like molding these custom things and they're like, [00:13:00] okay, let's try this.
Yeah, yeah. Boom, that doesn't work. Go to the next one. Mean it's unlimited supply of cash here. So they can try all these different things. For him, and they're gonna do literally everything to get this tow. They're gonna use all these sort of fancy gadgets, um, that we probably haven't even heard about yet.
So, I mean, it's gonna be, they're gonna try everything they can to get him, to get him back.
Will Sanchez: So rest, um, immobilizing taping 3D models of somebody mad scientist, Dr. Frankenstein, trying to create something that will fit his foot and, and in a kind of a way you go, uh, next question is, why is this called Turf Toe?
Why don't we have like a cooler name? Like, you know, when you hear rupture. Or, you know, tendon, you know, or, you know, ACL knee blown turf toe. Hey, can you come up with a creative way to rename this? And maybe we could kind of rebrand this and take credit for it. What, what, how would you go with it about that?
Dr. Grant Garcia: I, I can't think of a good name for this 'cause it's, it's, it usually happens in [00:14:00] football players. That's why they call it turf toe. It's the, it's a, it's 'cause it happens. And maybe we could, this nother discussion we talked about turf versus grass. Yeah. But maybe, you know, grass, toe doesn't sound any better, so at least it turf
Will Sanchez: toe.
Okay. Alright. Alright. We're going down the Rex Ryan tree right now with these toes. You we're done with the toes. Let's go with, uh, today's, uh, technology. Right? Uh, Deion Sanders went through this in the nineties, right? He, he had severe, uh, you know, with the turf toe. It's something that lingered. What are the differences between in the nineties when Dionne was suffering through turf toe and probably playing with it where he probably shouldn't have.
Right. You know, especially with that man up, you know, mentality. What are the difference from then to now that you can explain to our audience?
Dr. Grant Garcia: Yeah, so go back to that picture before you can show the fan the new technology, which we'll talk about. Again, we've talked about this at nauseum, but that's one more.
So this is a picture. Go back. That's perfect. Of all the ways [00:15:00] we use internal braces now and. This while these, some of these things are a little newer. Some of these are a little bit older. This is older in like the last few years, so they're talking about internal bracing now for even bunions. But you know, you have ankle fractures.
You add internal brace in there to help with the stabilization. You're doing these sort of ankle, the ankle instability. We talk about ankle sprains and adding internal brace.
Will Sanchez: Yeah. But
Dr. Grant Garcia: you can see there in the bottom left hand corner, there's plantar paint, internal bracing.
Will Sanchez: Yeah.
Dr. Grant Garcia: And so this is sort of one of the additions.
It's just like the UCL repair with internal brace. Right. Without that internal brace, UCL repair is not a good surgery. Like very few people to success. It was very, it was very unsuccessful.
That's why for years it wasn't successful. That's why ACL repairs, we talk about now saving acls 'cause we add the internal brace.
So this internal brace has been a game changer for these more simple repairs or 'cause or. In a lot of cases the repairs sometimes suck like this. Don't do that. Well. Yeah. And so now we have so many more surgeries that we can repair so we keep the [00:16:00] person's native tissue and avoid adding graft and tunnels and holes.
Will Sanchez: Yeah.
Dr. Grant Garcia: And that we can do this the more, if we can repair everybody, that would be the best case scenario. If you could repair all ligaments that ever got injured. That would be the holy grail, and we're getting closer. We're not there yet. And of course there's chronic injuries, which are different than acute injuries, but now they have this ability to internally brace the plantar plate.
And so as a result, they see that. They see him tear it. They're like, we have this new surgery, and maybe he'll get back instead of the four to six months, maybe three months. And so three months is not as bad, maybe two and a half months. Who knows? I mean, they tried to get Aaron Rogers back again. It was the Jets, but they tried to get him back in 10 weeks after an Achilles rupture.
'cause he had an internal brace as well. Yeah. So the idea is that these guys are gonna start pushing the envelope on this. Because remember in orthopedics, everything goes in like six weeks, 12 weeks, four to six months. It's just.[00:17:00]
So, you know, it's the, it's a pretty, we have these standard metrics that aren't always perfectly scientific. Right. You know, you always, you've always heard the word, it's four to six months. Right? That's a very common orthopedic term. Takes six weeks for the bone to heal. Well, it doesn't always heal in six weeks.
Sometimes it heals in four weeks. Sometimes it heals in eight weeks. But we like that word. We like the six weeks, we like the 12 weeks. We like the way the follow ups work.
Will Sanchez: Yeah.
Dr. Grant Garcia: So. The idea is that people are gonna keep pushing the envelope on a procedure like this, but remember, there's other things that go on with this procedure.
So not only is he gonna so go to the two slides over, I, it's, it's the best image I could find of this without grossing out the audience and showing an actual live surgery of this. So now this is not. Um, the actual turf toe repair, because this is the second, which is the other toe. It's the toe next to the big toe.
Will Sanchez: Yeah.
Dr. Grant Garcia: But this is the same sort of technique. So what, what they do is this, that plantar plate, you can see it's popped there in the bottom. And that's, so basically if you go on over the gray toe, that's what, that's how you'd fix this.
Will Sanchez: Yeah. Yeah. [00:18:00]
Dr. Grant Garcia: And they were threading the suture through, and then they do this very complicated repair technique, and then you anchor it on the other side.
In addition to that, you add something called the internal brace. So you add this synthetic suture, this thick fiber tape, and you anchor that on both sides as well. Obviously there's a little, there's a little bit room, there are very few room for air. You can see how small this is. Right. So you really wanna make sure you're accurate.
Yeah. But there's sort of kits and things like that that, that Arthrex has to help with this as well. So that's the, that's the first part. Another part is, you know, adding some sort of PRP or biologics sometimes can help. Yeah. We've talked about the fertilized ACL. We literally just had Chad Lavender on here.
Yeah. Um, having that conversation. So that's important. And then. As you see between those toes, there's cartilage. And so sometimes that cartilage is damaged. And so that may be something that we want to additionally do because if you don't take care of the cartilage damage and he has it there, it could go on to being painful.
So now you have lost power. Or let's say your plantar plate heal great, but now you still have pain 'cause the toe has [00:19:00] arthritis in between it. Mm-hmm. And that's a big problem.
Will Sanchez: Yeah, and we talked Dr. Grant Garcia: about this a long time ago. I think it was Serena Williams had this and she had to have a fusion, so it's not ideal.
To have cartilage damage there. So all those things. And then the last one, which again, little simple injury, that's so astic, the moid bones, those little tiny Holt bones that I showed you on the previous thing.
Will Sanchez: Yep.
Dr. Grant Garcia: If those are fractured, they can sometimes fix them or take them out, which is uncommon. But the other thing is they can tie all this in 'cause those sesamoids live inside of that plantar plate area.
With the ligaments, those little bones live in there. You see how they're all connected together? Yeah. Right. When you do the, when you do the dissection, it doesn't look like this. I wish it did. That'd be amazing. Every surgery would be amazing if it always looked like the picture. Right. But we know that's not real life.
So anyhow, so no. So the idea is you repair it all together. So that's what they did for, uh, Joe Burrows and I have a feeling that he'll be back faster. But again, it just depends too about, you know, the Bengals don't do well. Like why race him back? You know, if they're doing [00:20:00] really well, maybe they change their mind on when he comes back.
It's really tricky. I think that's the hardest part of some of these recoveries is you don't really know what the true return to sport is for this player. Because let's say they're, let's say now it's September, so October, November, December, three months, and they're not even close to playoffs. Why would they put him back in?
Will Sanchez: Yeah, I, I agree. I agree.
Dr. Grant Garcia: You're never gonna know. I mean, he could take him, they're gonna say he got back in five months, but he could have gone back in three. It all depends on when they get hurt. It's just like all this in-season stuff.
Will Sanchez: Yeah. Yeah. Um, and so can cleats help lead to these type of injuries?
Is is that common or is this just the way it is, you know, stressing that area? Pushing off. All of a sudden that you developed it? Or is it maybe
Dr. Grant Garcia: 300 pound people landing on your foot? Yeah. You know, there's lots of things on there. I'm just wondering
Will Sanchez: footwear as, because foot, the cleat is very different than anything else that we wear.
Right? Yeah. Mean this
Dr. Grant Garcia: is, this is a, this may be a, I mean, the challenge is on [00:21:00] the bottom to protect it. It's different than like ankle sprains, which we may have a sneak peek at that later on in the next few weeks with, um, some new episodes being released. Yep. But I'm sure there's people that are looking at it.
I mean. Anytime an injury happens, we've looked at the numbers, it's extremely expensive. I think I texted you recently that the number we had wasn't even close to what they're seeing now. They're like, yeah, talking about in the, in the billions of dollars lost per these players because it's so much money.
What about
Will Sanchez: training? Is there anything that you can do? You know, I, I'm reaching over here with the bottom of your foot, trying to see if there's anything that you can do. Is it training, is it strength? Is it, is it flexibility? Is it stretching? I know that there's been these contraptions that you put over your foot and you can pull, you know, are you doing anything with band work to just kind of keep that, uh, inflection going on in that area?
I'm just curious for what you've learned and spoken with your colleagues. Is there anything that says if you do this, you lower the risk by, you know, 3% [00:22:00] or something like that? Dr. Grant Garcia: So this is a great point. I don't wanna belabor this on the show 'cause it's a lot, but there is this small sub faction of people that have started talking about prophylactic surgeries, prophylactic internal bracing.
So. In these people that are really high risk is adding like an internal brace ahead of time where there's really no recovery, right? You just anchor it and you just let 'em go back. You let the incision heal. Yeah. Would that protect someone from having a turf toe and not in this case, but they talk about it for ACL tears, or do you add like a second ligament?
Back it up so you can prevent the ACL. I mean, it's a little crazy right now, preventive
Will Sanchez: medicine then. But the
Dr. Grant Garcia: idea of preventing, I mean, let's say you kind of knew you're like this, these, these six players are at high risk from AI algorithms, right? Which talked about before AI in medicine. Yeah. Yeah. So let's say you have an AI algorithm and it shows that like you, these are your top 2% of players that are at risk of getting.
W, and you're out for four months or lingers. You're never the same, [00:23:00] right? Yeah. I mean, some people might consider it, or do we do a minimally invasive thing where you just do two micro incisions, you throw the tape underneath, you avoid the tendons, you do it all in their ultrasound guidance, and you can do it in the player's back in two weeks.
Right. Like that, we may get there at some point. Yeah. So this is, this is something to be considered. 'cause if nothing else is torn, then it's, again, I'm not advocating for surgery that's not indicated or surgery before someone gets hurt. Uh, but, but it, the concept's pretty crazy because, or if we all of a sudden did it and then saw that no one got turf toed for like an entire season.
Will Sanchez: Yeah.
Dr. Grant Garcia: You know, we don't know. That's,
Will Sanchez: maybe we get to the point where it's not permanent, that you plant something in just for the season and then you remove it.
Dr. Grant Garcia: Or do we have biologics? Right. You start having soreness. You see that you throw biologics in there. I mean, that's probably where we're going.
'cause that's the easiest sell. To these NFL athletes is like, Hey, did you, you know, like, oh, your toe's turning into Season MRI shows as a small partial tear. Let's just pump you with a little bit of [00:24:00] some PRP or bone marrow or other stem cell options. And then, you know, you heal, then you're good. It scars in.
We got a new MRI. It looks good. Yes. So, you know, there we're, we're not there yet, but it's, uh, there's more things down the pipeline and there's things we're not even talking about on the people are working on. So,
Will Sanchez: yeah. And we're talking about a billion cazillion dollar industry where the quarterback position.
Is by far the most valuable position no matter what anyone says. Well, it's the past rusher, the running back, the wide receiver. No, your, your team cannot function without a, a high level quarterback, uh, as we've seen for the last decade with the New York Giants.
Dr. Grant Garcia: And he didn't even have turf toe. That's a sad, and
Will Sanchez: he did.
They have turf toe. This is a, this is a great topic. We're gonna have a lot of, uh, other topics to follow. We always wanted to let everybody know. Check us out@sports.talk.com for more episodes, transcripts, and we've had some. Very welcoming, curious, and talented, uh, request to be [00:25:00] on the show. So, but keep it coming.
We, we love it. We love to talk to you. We love that you reach out, so we really appreciate it. Uh, Dr. Garcia, you got anything to put a bow on this or internal brace on this?
Dr. Grant Garcia: Internal. Exactly. That's right. So, no, thanks for listening and, uh, yeah, keep the requests coming. We get a lot of requests, so it's, it's nice.
It's just, again, we want to stay focused on the, uh, sports talk, talk and, you know, all orthopedics, all sports all the time. So that's our, we try to keep that focus for our, for our viewers.
Will Sanchez: All right. Thank you very much, Dr. Garcia. Take care.
Audio Transcript
Elite Mindset with Gary Chupik

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. Do not adjust your sets. I am Will Sanchez, along with our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia. Uh, Dr. Garcia, this is a topic. A conversation that we have wanted to have for quite some time. So I'm really excited about our guest today. Um, we've talked about the mental mindset, the, the mindset of the athletes, and we have the perfect guest to talk about the elite, the elite mindset.
There you go. Right there. The elite mindset. It's, uh, and before we get into that, um, you had the elite mindset just recently, you know, at your, uh. Competing and swimming and, and I, I, I, I have to bring it up 'cause I know you don't like to bring it up because you're killing me here. People don't realize that you are a, a d one athlete.
You [00:01:00] love your swimming, you love competing. So it's not just what you do, um, you know, with your surgery and, and everything else and, but the guidance which you patients, but you know, you are a dude that gets out there and you wants, you know, you want some, so how was that?
Dr. Grant Garcia: I, well, I would tell you that I make a joke that people, I'm not very competitive, but everybody knows that there's a, it's like I'm a type AAA personality, I call it. So a little bit competitive. I try not to pawn it off too much on my children, so I get to have, I keep it to myself, which is good. So, but again, it was good. We did a swim for our club or local club that I used to coach as a kid. And now it's full circle 'cause my kids swim there and then I actually swam there as a kid.
So it's pretty awesome. So it's a full circle moment. Uh, and then I got to do something I really enjoy, which is swimming in the lake. But it was a little harder than I remember the last time. So I gotta work on my fitness. This
Will Sanchez: you getting old. Um, you know, it's, it's great that you didn't get hurt because you know we have some friends that would've taken care of you at the Recovery Shop.
Let's give a [00:02:00] shout out to Mike b. Tell the audience about the Recovery Shop and all the things that they do for us.
Dr. Grant Garcia: Yeah. Well first off, I love our new flashy yellow. This is awesome. So, yeah. Anyhow, thank you again to Recovery Shop. You know, they've been our sponsors for a long time. I mean, just the other day I had a patient that got injured and they're like, Hey, I want the same thing that your other player got.
Like, I want that nice machine. I want to be, I want that accelerated recovery program that he got. And I'm like, no problem. Happy to do this. It's, it's funny, I actually had a friend's family member in the middle of the country just called me and they're like, Hey, my, your, my sister had surgery with you.
She did awesome. Can you just gimme, you didn't operate on me, but can I have your thing? Because I can't get ahold of it. So he was able to go to the recovery shop and use that. So this is something that's really good for you to have at your fingertips as a surgeon. It'll help with the physical aspect.
There is no mental recovery aspect of this area, which we're gonna go to the second part of that in a minute. Um, but the goal here is for surgeons to offer all the latest things for our patients to get 'em back to what they need. Before we jump in our next topic, I think it's really [00:03:00] important. We have brought up so many times and behind the scenes we have so many checklist items.
Yeah, of things we wanna show to our, to our listeners. But the one biggest one has been the mental aspect of injury. And we've talked about it. I get it all the time in my office, all the time. I was just talking about today. I had it right, but we don't have anybody. It's always hard to find an expert and then we happen to cross paths with one of the elite sort of mental aspect.
Athletes in all levels. And so I really like to introduce, uh, Gary Chopik for his, uh, and I'm really looking forward to hearing more about this from the elite mindset. So thank you so much for coming on.
Gary Chupik: Yeah, thanks for having me, fellas. We're all Seattle guys. Huh?
Will Sanchez: Yeah, it's nice because sometimes, uh, a lot of times we have, uh, east coast guests and, and it's tough if we have a six to seven o'clock, you know, show based on our schedule and things that we're busy.
You know, we, we've got people coming on nine, 10 o'clock at night and sometimes, and they're tired. And Dr. Garcia just rambles on and [00:04:00] on and on. So we go really late, you know, so we always thank them. So it's nice to have someone on the west coast that we know that we are. Hopefully not being too intrusive with your time.
And once again, as, uh, Dr. Garcia mentioned, you know, thank you so much for, uh, being on the show and, um. Sharing your, your knowledge. So, Dr. Garcia, why don't you, uh, kick us off and, uh, talk about Yeah. Um, you know, let's get on topic here.
Dr. Grant Garcia: Well, again, we're, this is, we always jump around, but obviously we have an expert here.
So will you go, will you just initially, first off, introduce yourself, tell us about this elite mindset that you've developed. You know, brief game plan and kind of how you became a mental coach. Like, it's such an important thing, but it's actually kind of hard to find someone that's really good at this.
Gary Chupik: Yeah, it really is. Uh, it's a really interesting field. So I grew up a pastor, believe it or not, for 28 years. And I'm originally from Saskatchewan, Canada. So I just, I'm a prairie boy at heart, but I've been another Canadian, another. This is
Dr. Grant Garcia: awesome.
Gary Chupik: Yeah. And uh, and I got married to a [00:05:00] girl from Seattle, Washington, and so love brought me south.
And I've been here, uh, 33 years now, and it's, it's been a wild ride. There's a lot of interesting, uh, dynamics between what it's like to live in Canada and what it's like to live in America. But, um, but I grew up a, uh, a pastor. I've kind of been a reluctant leader all of my life, and I, so I'm an ordained pastor and have been for 28 years.
And then in, in 2017, I had a burnout. And I just hit a wall and I didn't know what to do. And I think when you're in an industry for so long, the language becomes so familiar, especially when you're on the helping side of things. And I, I think I just needed a different framework. And so I ended up, uh, studying sports psych for about a thousand hours for the next couple years, just trying to figure out how to get out, out of this exhaustion phase I was in in my life.
And, uh, and then I had a, a friend that I had met. Who knew Trevor Moad and Trevor Moad at the time was Russell Wilson's mental performance coach. I read his book, it Takes What It Takes, and then this [00:06:00] friend said to me, would you like to meet Trevor one day? And I said, well, of course I would like that. Who wouldn't wanna meet someone who was at the top of their game?
In fact, at that time he was on ESPN. He was. NBC, he was like top of the food chain in our industry. And, uh, and then to be mentored by a guy like that, it was just a, a once in a lifetime opportunity. And so one day, uh, he said to me, Gary, if you were to help a professional athlete, uh, tell me your process, what, how would you help them?
What, what process would you take them through? And so he said, 30 days from now, I want you to show that to me. And so 30 days went by. And I was prepared and showed him the process that I had come up with and he hired me on the spot. And so I worked with Limitless minds for the next couple years and then went out on my own the last five.
So it's been a wild ride to get here. I just would've never have thought that in my lifetime that I would be doing what I was when I'm doing, but I can't imagine doing anything else right now. And in fact, in many ways I live a dream life partly because, uh, of the clients that I get to work with, but also.
Just my, my challenge [00:07:00] to other people to live life to the fullest and make sure their head is in the right place and the right spot. And so I now, I work with professional athletes, uh, TV celebrities, uh, yeah. And businesses all over the area in the country and in fact have started traveling internationally.
And so it's just been a lot of fun. And, uh, yeah, I just, it's a wild ride and I, I just can't imagine doing anything else.
Dr. Grant Garcia: Um, and then will you kind of go into, I mean. I'm, I imagine there's probably different types of ways you have to structure it, or do you have the same sort of similar structure for an executive or, you know, like, or a surgeon or an athlete, or is it kind of all different?
Like how do you break that down?
Gary Chupik: Yeah, for me it's about 80% commonalities between, uh, whether it's sports and business or different fields. And I would say 80% of it's the same. I would say 20% of it's different and you gotta learn that 20% 'cause it's pretty crucial. And so I often find myself having to call up other mental performance coaches that are experts in that particular sport and learn all that.
I can chat. GPT can be [00:08:00] helpful, but one of the shortcomings of chat GP Ts, it doesn't understand sequence. And, and how to teach someone how to, um, you know, get, get control of their thoughts and their mindset. There's an actual sequence to it. It's like baking a cake. You can have all the right ingredients, but if you don't know how to sequence it, you're not like, not gonna get the intended result.
And so teaching someone how to sequence all the mental skills is actually really, really crucial.
Will Sanchez: You know? Um, I, I love kind of where you're going with this because a lot of us know what we're supposed to do. But getting to do that or acting upon it and, and taking those steps, that's a whole other area that a lot of people struggle with, you know?
So what are some of those things, or, or how do you communicate that to someone that. Knows what's happening or knows what they need to do, but you help them, you know, see it clear clearly and start them to, to, to get on that right path.
Gary Chupik: Yeah. So sometimes you do a crisis [00:09:00] intervention, right? Like you're gonna step in and, and rescue someone or, or something.
And there is a time and a place for that. And so there're in crisis and you deal with that issue. But if you have a little bit of time, that's when you can really lay a really solid foundation. So for me, and, and the way that I think, and in my world. For me, uh, motivation is not the holy grail of all performance.
I think it's helpful to have it. It's almost like an icing on top of the cake, but it's really not that necessary. What really is, I think, the holy grail of all mental performance, if you have the time to teach it, is self-leadership. And so the self-efficacy of someone understanding their life and getting to choose the thoughts that they think, like a lot of people think that they don't have a choice to think what they think.
You know, they kind of feel like, you know, it's kinda like a bird landing on your head. You know, someone once said that you can't stop a bird from landing on your head, but you can certainly stop it from building a nest there. And your thoughts are really quite similar. You can have all types of crazy thoughts and thank goodness we don't act on all [00:10:00] of them, but we can kind of police them and we can kind of say or reject some thoughts and accept and receive others that are more productive for us.
Dr. Grant Garcia: Is that kind of the thought in the sense that like, oh, I'm in my own head, but I, you know, I can't fix that. Like, that's just me. I'm kind of like a, you know, I would say there's certain different surgeon mentalities, like, you know, hey, like I'm just anxious for this case. 'cause it's a tough case, right? Like, that's just, I'm just never gonna get over that. That's just the way it is. And, and what you're saying is that's a wrong, that mindset already is the wrong thing. Right? That's, I'm making that up in my head.
Gary Chupik: Yeah, it's really strange. Like I, I, you know, one of the things that I've been teaching recently in my business that it's made a lot of sense to me is having your thoughts be outside of yourself.
Because when you're so introspective, and we just live in this dage of analytics now, like, I mean, there's wearable tech, um, people are looking for data. I mean, and it is just the information's everywhere. And so what happens is, is that we just intend to internalize everything and we overthink everything, and then it paralyzes us and it causes us to hesitate [00:11:00] and hesitation, whether it's in sports or business.
Or in the medical field can be quite costly if you're not confident enough to, to remove the hesitation. So the issue really is in, in my view, is limiting the amount of thoughts that you have so that you can be successful at the things that are the most important. For example, I think thoughts are like calories.
If you have too many calories that you don't expend what happens to you, you get slow and lethargic in the same way. Thoughts are like that. When you have an abundance of thoughts that you can't expend, then you just kind of eventually carry them and they get really weighty. And so you have to figure out what thoughts are producing something good in you and what thoughts are not so helpful.
Dr. Grant Garcia: Is this kinda like the idea of over extension. You know, it's the, the idea that like, hey, listen, you know, a lot of us are going different directions and these athletes are getting, you know, sponsorships and then they're getting told performance, and if they get hurt, they're told recovery. And like, it's kind of, is that the idea of like, you just have too many things come in at once.
You need to focus on the high efficiency. Directions [00:12:00] Or what is that? Just to clarify?
Gary Chupik: Well, both. So internally, you can have too many thoughts that you have to be able to narrow down. I mean, uh, Steve Jobs would talk about signal, uh, the signal and, uh, and a distortion ratio, right? Would like or signal to noise.
So you have to like focus on the things that are the most important in that moment and then outside of yourself. Yeah, I mean, athletes are more distracted than ever with social media and with the opportunities that are coming their way and, and now with NIL, it's like just focus on the game. But you know, a young athletes can't even barely do that anymore because they're looking for sponsorship deals and they're looking for opportunities to get paid.
And so there's so much distraction. In our world today for athletes and I'm, I'm not sure it's that much different for the rest of us in different vocations where the, the distractions are s immense and your ability to learn and know things are just immense. But there's a difference between knowing [00:13:00] something and experiencing something.
So we might be book smart with something, but in terms of like actually getting to know something intimately, it's just very different. And there's no way to really know things until you experience them. But if we're spending so much time in the knowledge arena, uh, and inside of our own heads, or we're, you know, studying something on our phones or using chat GPT, that's not really knowledge per se.
It's information, but it's not really, you know, intimate knowledge of something. Uh, do you want, do you have an
Dr. Grant Garcia: exercise you use? Oh, sorry. Will
Will Sanchez: No, no. Go ahead. Finish, finish that and I'll jump in. Go ahead.
Dr. Grant Garcia: Do you have an exercise? Like, what would you do for, for that player? Right. So like, let's say you're kind of saying, Hey, you have to experience, right?
But if your experience is like, you have to experience winning the game, right? They're not gonna win the game to exp like the whole point of what you're doing is hoping that they can win the game. 'cause they're clear and their mind's clear. Like, how would you get them to get that experience or knowledge rather than.
Just seeing it on chat GBT or the internet or talking about it? [00:14:00]
Gary Chupik: Yeah. I mean, there's no way to help a player by teaching them and adding on to what they already know without removing something. So there's gotta think of it like a cup. Like you can only pour so much into a cup where you have to say, okay, listen, what do you, what thoughts do you need to let go of?
Like, what do you need to subtract from your life? I remember, uh, being a leader, uh, in a nonprofit in the church for many, many years. I led on a, a local, national, regional and national level. And my wife would always say to me like, Gary, you know, for everything that you take on, you have to let go of two things.
I'm like, there's no way I can do that. Like this is such a great opportunity and, but she would just sort of ground me and say, no, no, no, you gotta let go of two things because it has to be that important. And I think in the same way, you thoughts just have to be poured out of your head. There has to be some type of subtraction so that you can perform at a high level.
And in fact, I call it intentional naivety. You have to like choose to be naive about something or not know [00:15:00] something so that you can become really excellent at what you do. So in some ways, I like to teach it as perfecting the simple. So just perfect the simple things. Perfect. Your thought process, so it becomes so instinctual that you don't really have to think about it.
But there's no way to do that without getting in the mental reps and the physical reps so that you can, you can perform at a high level.
Will Sanchez: I wanna go back to the NIL and, and it's clear now that your wife is the original elite mindset master behind all this because she has set the guidelines, given you, the tools for you to share with the rest of us.
So we want to thank her in advance for everything that she has done to get you where you need to be. Um, going back to the NIL. Obviously this is all brand new, right? And we're seeing kids it, it's remarkable. I think I saw recently this week that another athlete is changing school. This is the sixth time in their college career.
That they have moved on. [00:16:00] What are some of the, some of the conversations you're having or maybe some of the advice, because you said something really important there with having too much information and maybe they're getting that from the parent coach agent, where they're not really enjoying or fulfilling their obligation to themselves to having a sustainable college career.
And they're, they're looking for the next thing and they're moving around. What, what have, what? What are some of the concerns when you have athletes that are going through something like that?
Gary Chupik: Well, it's interesting how important environment is, and in order to be successful you have to be in an environment long enough.
But we live in this day and age now where, where you're right, you know, players are moving back and forth and now what they're doing is signing one and two year contracts. Because with a college, because they wanna, they want the freedom after a year or two to be able to go somewhere else. And the, and the colleges with the really good players are asking them to commit to longer contracts.
And so we're just in [00:17:00] territory that we've never been in before. And it's incredibly confusing and, and everyone's just trying to keep up with the changes. But in order to be successful at something, you really do need a level of consistency. And, and, and repetition and rhythm. Like a lot of people don't like to talk about discipline and habits and that kind of thing, but even in terms of like being in one place for a given amount of time can be so valuable.
In other words, you can take an athlete that's really good in one environment, change the environment. And he's not very good or she.
Will Sanchez: Mm-hmm. And in the
Gary Chupik: same way, you can take an athlete that's really struggling in one environment or on one team and change the team, and all of a sudden they start to thrive because of the system or because of the players that are around them or because of the culture.
But you don't ever really get a chance to grow roots in a system or process or environment if you're not there long enough. So it's a crazy world, like, I don't even know. Like, I have a couple, uh, baseball players I'm working with right now, and this is his third team in three [00:18:00] years. And Wow. And he just doesn't feel like he's getting the plane time he wants.
And he was a stud in high school and Yeah. A stud in his first year. And so when you're a stud in your first year, you wanna go to a bigger and better school, but you might be sitting on the bench at that school. It, it wasn't what you were expecting. Whereas if he would've stayed with the program that he was in.
He could have very well, um, you know, he knew the system, he knew the process, he knew the coaches, but that disgruntledness is always there thinking that the grass is greener on the other side of the fence, and oftentimes it's not. I,
Dr. Grant Garcia: is this something now that you're, do you feel like this is something that's trickling down on a professional level?
Like obviously the pros are making still more money, but there's a lot of money in NIL. Mm-hmm. Do you feel, from your experience working with some of the professional athletes, like is this something that's already been there and kind of like for you, is this harder now to deal with the NIL players because of your, or is it you're like, okay, now I already have this, I have these older players, right, the ones at a professional level and I kind of have the framework?
Or is it a different framework you're dealing with? 'cause obviously they're. [00:19:00] They're younger and they still have parental advising, advising and things like that. So it's a little bit more challenging. And the school things different than the teams?
Gary Chupik: Yeah, it's, it's diff it's, it's a lot of it's the same.
There are differences, but a lot of it's the same. In other words, like, I'll never forget, I was in Buffalo watching the bills play the dolphins, and I'm sitting with a player agent, and the player agent is watching his defensive end play. And Buffalo would score a touchdown, um, or probably the other team.
Uh, no, Buffalo would, would get a sack, but it wasn't his player.
Will Sanchez: Hmm.
Gary Chupik: And let's say he's rotating in and out. Let's, so let's say every, let's say every drive, they rotate. Yeah. Well, the, the guy that was rotating in, the other guy that was rotating in, that was not this agent's player when he got a sack. He would be so angry and frustrated.
That's crazy. 'cause it would make his player look bad. And so it was just like a world that was like so foreign to me that I, it was hard to even comprehend. And so this is the day [00:20:00] and age that we live in where those agents, when they get to the players at a really young age, they can take advantage of them.
They can, uh, at least the pro player sort of has been around a little bit and they kind of know in addition to a player agent, they also have a player manager. And those managers are gonna become more and more popular at the college level. In other words, you have these, they're not really an agent. Well, in addition to the agent, now you have a player manager who's managing that player's life.
So it's like appearances. It's brand deals. It's not done by the agent, the NIL agent. It's done by the manager. Of that player. Wow. So that if that manager isn't a really, a great person with high integrity and high character, they control so much of that player's life, where they go, what they do, and what they say to that player and their interaction.
So it is, it is a very difficult world. And I'm 56, like I, I've been around a little bit, so, you know, I've lived, lived a little bit and you see a lot of things. But when you're, [00:21:00] you know, even an NFL player seems really young to me, right? Like they're, they're just 2020s. Yeah, I feel so old. And, but they're in so many ways, they're so young.
But when you start talking about college players, they're huge human beings. Like they're massive and you, and you think that they're older than they actually are, and when in reality they're just, they're 22-year-old, you know, young men. I,
Dr. Grant Garcia: I think talking about the players. Can we, um, go into this next slide Will too.
I don't wanna get, I love tearing all the Gary's information. I wanna make sure we talk about, you know, will you describe this a little bit to us? Is this sort of like something you use in sort of your initial assessment or how does this work for you?
Gary Chupik: Yeah, so, uh, this is something I created and I've taught it to obviously professional athletes.
I've also taught it to the FBI, I've also taught it to, um, you know, you know, uh, you know, law enforcement and, uh, fire. It's, it's just been so helpful in so many different ways. I've also taught to businessmen, and so I [00:22:00] created a four step process that brings the best out of athletes and high performers when the pressure is on.
So I call this Cape like a superman Cape, CAPE. So C stands for control yourself. A good example to use in all of this is baseball, but if, but we can change the vocation later and we can even change it to your vocation as you're gonna do something that requires a lot of attention and focus. So C stands for control Yourself.
The universal sigh to relax and slow down your breathing is just to take a deep sigh. Okay, so when you play tense, you don't play as well. And I think in the same way with other professions, it's the same thing. When you're more relaxed, you're more limber. For example, I saw a tennis player play recently, a pro tennis player who.
As the match went on, he became more tense and he started to tighten up his swing, and I could see it happening because he was feeling the pressure instead of being really just kind of loose and flowing. So C stands for control yourself. So in baseball [00:23:00] it's take that deep sigh, right? Look around, look up, look in the stands for a second, and then focus back.
So it's C stands for control yourself. So that definitely has, there's also, uh, some, uh. There's also some hormonal aspects to what we're talking about when you take that deep sigh, but really it's getting your breathing under control. So it's C stands for control. A stands for assess the situation. Now, this is the one, one of the most interesting things to me in the entire world, because if I said to you, you know, look behind you just for like half a second and then look back into the camera.
You don't really realize it, but you could probably tell me 50 or 60 things about your surroundings in that one second. That's how fast neurologically your brain functions. It's like faster than the fastest computer. It's unbelievable. So the amount of information that your brain can assess very quickly is remarkable.
In baseball, the, the average in a time between a pitch is [00:24:00] like 13 to 16 or 17 seconds. So that baseball player that pitcher's assessing. All types of things where the runners are in base. What's the pitch count? Um, you know what the, he is getting the, the signal from the manager where the pitch clock, there's pitch clock, there's the catcher throwing signs.
Like it's just remarkable how much information that he's assessing. So that's assess the situation. And there's a limit to it though. You can't keep assessing. You got, you gotta cut it off.
Then p is, you gotta make a plan. So not only is it what happens if the ball comes to me, it's like, what happens when the balls hit to the shortstop?
What happens when the balls hit to the first baseman? What happens when there's all these different dynamics? So you gotta make a plan. And then E is, is stands for execute, which is trust your plan. Trust your training and trust your instincts, because we know that when an athlete trusts their training and they play instinctually, they, that's usually where their best [00:25:00] performance is.
So the overthinking piece and the too many thoughts come into play here where we do really just want you to play instinctually. But you gotta, you gotta put in the work though. You gotta, you gotta do the C, you gotta do the A. You gotta do the p. You gotta understand the plan, you gotta trust your training, but we do want you to play instinctually, and that's where your money's made is, is your instincts.
Will Sanchez: It's funny you mentioned, uh, control and um, the famous story for me is in the Super Bowl against the Cincinnati Bengals, Joe Montana is on the game winning drive. And everybody's kind of feeling real tight and he's looking around and he is like, oh, you see that? And it's, it is John Candy that he is hanging out in the end zone and the players around him looking at it, are you serious?
We're trying to win this game. We're we're the Super Bowl drive. He is like, yeah, Joe. Cool. What's the perfect nickname for him? Him, he used hanging around, looking around. So where he's assessing, right? He's looking around on the timeout, pointing things, being under control. So, uh, I, I, I think there's a lot to it, especially when we see the elite [00:26:00] athletes, whether it's a, a Joe Montana, a Brady, some of these other athletes, they just find a way to control Andrew.
Andrew Huberman talks about breathing control and taking that deep breath and that extra sniff. Yeah. And then double breath. And the double breath and how to reset your body and what you're doing. So there's so many things that are resonating when you're talking about this Kate, uh, program that, that you're, you're utilizing to help people mo navigate through all this.
So anyway, go ahead, Darthy. And,
Dr. Grant Garcia: and Gary, would you say, uh, for this, like how would you approach this sort of timeline? Obviously the, an acronym's great. The title's great, everything's great, but how does that kind of work? Would you have a plan? How do you do, I know you have sort of a plan you listed as sort of like a way that you go through this with athletes.
Like, how would you do this for an athlete if they came in and they're like, Hey, we're gonna do this for a, you know, a week period, a month period. How does that work?
Gary Chupik: Yeah, it's very interesting. So, again, if I have a little bit of time, I can go through my process. So think of it like, um, like a pyramid [00:27:00] with a circle in it and in the, and the core of that circle is self-leadership, your ability to lead yourself.
Is, it's everything. Whether you are, uh, playing a sport, whether you're in your vocation and you're, you're, um, you know, you're, you're about your craft, your ability to lead yourself even when you don't feel like it is everything. So if you don't get the self-leadership piece down, you're in big trouble. So I teach something called the Leadership Pyramid.
It was something that I came up with years ago that every time that I. I don't do it. I regret it on so many different levels, especially if, if you've ever hired anybody, it's such a great, uh, analogy. So the bottom layer is self-leadership. If you mess up on the self-leadership at at the bottom or, uh, the foundation of the pyramid, you're in trouble And, and your actions and, and the lack of your integrity and self-leadership.
Is gonna cause the entire pyramid to fracture, and you'll see why in a moment. So that bottom layer of self-leadership, it's [00:28:00] everything and it never ends. It's always present. So you investing in yourself, you, um, taking time to, uh, recover, you having, uh, integrity and character as a leader and, and being self led, it just never ends.
So the bottom layer is self leadership. The next layer is couple leadership, but I don't necessarily mean romantic. It's just. You think of like, um, you know, being an example to somebody else or coaching somebody else, or mentoring somebody else or leading somebody else. So when you do self-leadership. The next in the sequence is that you can do couple leadership and why shouldn't you lead another person if you don't lead yourself well, you're being a bad example, right?
You're bringing in all this baggage into this relationship, and it's actually not helpful to the person you're trying to help. The next layer is group leadership, but we all know that a great group leader is mentoring the next in line, right? So whoever's next in the bullpen. But you can't do that if you've never led at the couple level.[00:29:00]
So we want you to lead at the group level, but we, you need to have at least had couple experience and self-leadership experience. You have to be able to demonstrate that you are capable of leading a group by the previous two levels. And then you have area or department, and then ultimately you have organizational leadership.
So when you put somebody in leadership at the group or area, department level, that has never done group leadership or couple leadership, you're in trouble. So they might have, you know, they might be charismatic or have charisma, but they actually don't know what they're doing. So when we hire people as leaders in our businesses, or the people that we associate with, if we don't have them go through those steps or that pyramid, we're, it's really to our detriment and our organization's de detriment.
Because when you have a leader, let's say an organizational leader, that doesn't show good self leadership, it affects everything. The entire organization, the entire [00:30:00] structure. All of a sudden people don't know that, you know, they're supposed to be accountable for their actions or what they say. People will lie to one another and be dishonest.
I mean, it doesn't take, doesn't take a pair of binoculars here in the Seattle area to see which companies really have struggled by passing the buck. And which ones take responsibility for them. So I think in a CEO or a business leader who takes responsibility is a great self leader. So I've set all that to say self-leadership in that leadership pyramid is, if you have time, is to teach people that there's nothing more important.
Than you leading yourself even when you're not motivated. And then you can reinforce that by a next concentric circle with your habits and daily rhythms that you have in your life. A lot of people are viscerally, uh, moved when I say the word disciplines or habits, but just think of rhythms. So now that you have self uh, leadership, you wanna reinforce that with rhythms in your life that put you in the best position to succeed.
So one of the things I say in [00:31:00] my business all the time is you can't control outcomes. But you can always put yourself in the best position to succeed. So let's work on the best position to succeed. What does that look like when you wake up every day, what, what puts you in the best position to succeed?
And then you have different parts of the inside of that triangle now in the corners. And to me, mental imagery and having or knowing your personal philosophy and having domain management. Is, are the three keys to, uh, you know, causing this, you know, this paradigm or this, this entire image work? Because if you don't have control over the different domains of your life, it affects your play on the field or affects your craft at work.
In other words, uh, we can all point to athletes that when they get, uh, whether it's distracted or they're struggling in a different domain of their life, it totally affects their gameplay. It Totally. And, and it affects, you know, even for me, it affects my life when things aren't going well with this, you know, wonderful woman called Molly in my life, if I'm struggling in my marriage, it totally [00:32:00] affects my craft.
Dr. Grant Garcia: Mm-hmm.
Gary Chupik: So the domain management is just as important as, as anything. And so when we talk about helping an athlete, what we're really trying to do is, number one, we're trying to put out the fires. So I, there's a, uh, there's a image that I have that you guys have there. It's the mental health, uh, mental health bridge, bridge assessment.
So if there is a crisis going on in their life, or let's say that they're really struggling in an area of their game, let's say, and well, the idea is to put out the fire and, and figure out the crisis as quickly as possible. And then we can help stabilize them, simplify the complex, you know, give them the support that they need.
So, and then help them create a short term plan. And then re again, remove any of those unhealthy thoughts. Or a stimuli that's in their life to help them go from crisis to coping. So coping is super helpful because we can give them tools to be able to, um, help them get outta that crisis. And if they can, [00:33:00] uh, implement those tools on their own and we can teach 'em how to use those tools, then they, they don't always need, you know, someone who's performing surgery on them all the time.
But this is the big fault of mental health in our society is that we almost always stop. At the coping and prevention level. It is one of the, really the, one of the great tragedies of our day and age where we pour all this money and, and time and energy, even at the school, elementary school, high school, middle school level.
We just stop at prevention and we don't actually teach kids how to thrive and transcend. There's, there's, in fact, when we're thriving or transcending, we're almost distracted by all the best things in life and all the good things in life so that we're not even thinking much about crisis and coping.
We've already. Like decided that we are gonna be the very best we can be. So I think we just, we stop at the coping and prevention, uh, pillar and we just don't go far enough. It was like me walking [00:34:00] into a, a professional football facility and the coach and I are walking around the facility. And we walk by the training room and I say, Hey coach, you know, that's a, a lot of what mental health is all about is, you know, getting bandaged up and taped up and getting iced.
But mental performance is like the gym. And so we walk into the gym and we hear the clank of the weights and guys getting stronger and there's a lot of energy and a lot of excitement in the room. And that's what I feel like I do as I help the athletes to thrive and, and elevate their game. So is there a place for crisis and helping a player that's really struggling with something? A hundred percent. And the job, my job is to assess that as quickly as possible, and sometimes we can do it. Sometimes it's easy to do. Like I had one defensive tackle that said, Gary, can you make me two tenths of a second faster? And I was like, Kay, I'm on it. Let's go. And I had about two or three sessions with him and he was two tenths of a second faster.
He was on one of the, ended up being on one of the best defenses, uh, an integral part of one of the best defenses in the NFLA year and a half ago. [00:35:00] So sometimes we can do that. If the player knows exactly what they want and I can help them do that, then let's go for it. Other times, um, you know, you're sort of slow dripping your mental performance, so they get a more well-rounded view of, of performance.
Dr. Grant Garcia: That's awesome. So you're, so what you're Stacy's saying is that, you know, most of the time these athletes, you know, they've, they've got crisis, they have coping, but really sometimes any, those are the ones that are recovering from some sort of major injury, uh, et cetera. But there are a lot of times many these athletes are, they're fairly healthy, right?
And so they need to go to more of the thrive. The Thrive and whatever the other slide, the other part was transcend. Yeah. So that's kind of where that transcend, that's, that's where you're stepping in. In majority of the cases. Right. So you're saying that you could cover all the areas, but in a lot of times these, for the higher level athletes, you don't, you only need to go to those next two steps, uh, to get them to the next level, but it's also less covered.
Gary Chupik: Yeah. I mean, so yeah, that's often the case, but there's a lot of players who, let's say, I mean, every player gets in a slump or they don't perform as well, [00:36:00] and you don't always know why and nor do they. 'cause if they knew they would fix it right away. So sometimes it takes a little, like, I, I, I mean, I, I like it to digging for treasures.
It's like, I'm, I'm gonna go dig in here and find out what the pain points are and figure out how I can help this player. And it might take me a while. Like, I, this is really embarrassing to say. 'cause it's not, it is not really, um, you know, it doesn't reflect well on me, but it took me a year to figure out a player one time.
An entire year, and once I figured it out, I was like, oh, like I'm connecting all these dots. I'm meeting with him four times a month or three times a month, and I just, I couldn't figure it out. I couldn't figure why he was just sort of plateaued in his performance. But after a year I was like, oh, I started to connect the dots a little bit.
It's, it's kind of like staring into the sky, looking at the stars, and all of a sudden seeing a constellation, you're like, okay, now it all makes sense. Okay, this is what we need to work on. And then we, we really spent the next four [00:37:00] weeks working on this one issue and solved all the problems. Like, well, I mean, performance changed.
Dr. Grant Garcia: don't think, I think, I think that the best leaders, like you mentioned, can admit that they're not always perfect and that they would take some longer for certain aspects. I mean, I'll be honest with you, I have patients come in, I have patients occasionally that I'm like, first time I see them, I know exactly what they need.
It could be crazy complex. I know the exact surgery they need, and sometimes I go patients I'm like. I don't know what you need. And it takes multiple visits, right? So you're, we're supposed to be the experts, but the expert expert doesn't always mean fast. It means we're gonna be, we're gonna do our best and use all of our knowledge to figure it out.
So, I mean, the fact is that you didn't give up. I think that's probably the most important aspect. I'm not trying to mental health coach you, but I'm just saying that's a great, that's a really, that's a great asset that you
Gary Chupik: brought up. But the grant, I mean, there's, there's pressure, right? Like you get hired to do a job and it's not working.
And so you just kind of go, wow, like I gotta figure this out. And you start reading books and talking to people and replaying the conversations. And then [00:38:00] we're talking to one of their friends or their loved one, like you're trying to, you're going digging and it just takes a little bit of time. And you know what?
Sometimes the client isn't aware of what the problem is, like it's subconscious for them, and they don't even know what it is. So it just, it takes a while and the patience is really helpful. And you know, at one point I was thinking like, well, maybe they need to get a different mental performance coach.
'cause it's not, I, I don't see it like I'm, I'm really having a, a struggle trying to find out what the, the issue is and what the cause is. But sometimes, you know, it, it, it takes a while.
And you know what, there's a definition of mindset. There's, they're like a generic definition of mindset, which for me is, is too generic.
It is a condition set of beliefs that drive behavior. Well, yeah, but where do your beliefs come from? Like where do, where does that come from and how do we form thoughts and, and beliefs about things? And so it took me seven years to figure out what I'm about to tell you. Seven years, but it was really helpful for me in deciphering what was going on with this athlete.
So my definition, it's [00:39:00] kinda like a physics equation. My definition is you have an experience. Could be it happened to you or you initiated it. You just have an experience. So think of your own kids, right? Like they have an experience, maybe they're playing a sport and they have an experience, and then you have thoughts and feelings and brackets.
You have thoughts and feelings associated with that experience. And they could be positive, they could be negative. You don't know. They're just, they are thoughts and feelings. Sometimes you're aware of them, sometimes you're not. But if you go outside of that parentheses or those brackets, and then you get to choose a response.
Now when you're older, you probably get to choose a response. When you're younger, you, you don't often don't get a chance to choose your responses. So you might not even be aware. Your response might even be subconscious. So for example, when I was younger, I was in geo trade class. I don't know anything about geo trade.
Like that is not my strength. But I was in geo trade class and so I would go to this class and my teacher. Would embarrass me 'cause I didn't know [00:40:00] the answers. And he was kind of a fun guy. He was a hockey fan. I was a Bruins fan. He was a Canadians fan. So we kind of were bantering back and forth and, and whenever, you know, the Brus would win.
He would be extra mean to me. But he made a put, sort of put me on spotlight and embarrassed me. So my response to being asked a question he knew I didn't answer was to be the funny guy. So I would just like say, well, yeah, the answer is 3.7 1 6 8, 9 4, 2, 3, 1 2. Mm-hmm. The entire class would laugh and I'm not a funny guy, but I didn't, that was my response in that moment.
'cause I didn't know how else to respond.
Will Sanchez: So your coping, your coping mechanism
Gary Chupik: totally was a coping mechanism. Yeah. So out of the experience, thoughts and feelings, my response, now I have a belief. So you form a belief that's the next part of the equation. You form a belief about yourself. Well, what do you think my belief was about myself and I wasn't very smart.
All right? I wasn't a smart kid, right? So I just figured I, I wasn't really gonna [00:41:00] do much in my life, and I just had to get used to it. So my mindset was no school for me after high school because I wasn't smart enough. I was gonna swing a hammer. Not that there's anything wrong with that. Mm-hmm. But I just figured for the rest of my life, I was gonna have to use my hands to make a living.
And so when I decided to go to college, um, you know, my grades weren't very good because I believed that I wasn't very smart. Well, what's really interesting about this was that I ended up graduating in my master's degree with high honors. Not to brag, but just to say I barely passed high school. But it, when I dialed in and I took the right subjects that were more up my alley, I ended up killing it.
And I came to realize that if I could go back to my former self, to my 16-year-old self or 15-year-old self, and if I could whisper, if I could coach myself in the moment when my instructor was making fun of me, you know what I'd probably tell myself? I'd probably say, Hey Gary, you know what? Did you know that there are nine different kinds of intelligence [00:42:00] and geo trade's not yours?
I, I, I wish I could have told myself that, but in that moment I just believed that I was stupid. You know, there's spatial intelligence, there's linguistic intelligence, there's musical intelligence, there's kinetic intelligence, there's philosophical inte intelligence. I mean, there's all these different kinds of intelligence, but a couple of the subjects they didn't teach in high school was psych and philosophy, and those were my two best subjects, but they did, I didn't get to take that in high school, so it was only when I went to college that I figured out, Hey, wait a minute, I have an aptitude for these.
Kinds of arenas of knowledge. So the, the where a mindset comes in and that, that's how you form a mindset. In fact, Andy McKay from the Seattle Mariners, um, he taught me, Gary, you just can't end with mindset. So you have your experience, thoughts, feelings, your response. Your belief. That forms your mindset.
But he said, Gary, you can't end with your mindset. It always has to result in new and improved. Behaviors, which is kind of like a new experience, [00:43:00] right? So this is how like it cycles back to experience. So you start to give yourself new and improved experiences with new and improved thoughts and feelings, with new and improved responses with new and improved beliefs. That create a new and improved mindset and it keeps cycling over. And so that's how you build a mindset. But sometimes you have to go back to that experience. And it was really funny because I didn't think that I had anything in my past that, you know, people always say, you know, are you gonna go back in your past and figure yourself out and whatever?
I'm like, I don't know. I don't, I don't have anything. But when I took the time to really slow down and say, oh, you know what, that classroom, that geo trade class was very formative in my mindset for many, many years. And it had a huge impact. And that's how I put together my equation. So I think you can build a mindset.
I think you might have to do a little digging sometime with a client, Hey, what happened? And sometimes I'll just say like, somebody is like a player is struggling with something, or a business owner is struggling with something, and I'll just say, Hey, what [00:44:00] happened? They're like, what? What do you mean what happened?
I'm like, yeah, what happened? Well, what are you talking about? You're stuck here, right? Like, tell me about something that happened in your past where you're really struggling with something, you know, that was really painful or hurtful. All of a sudden, no one, no one's ever asked them that question, and all of a sudden you start digging up.
Junk or stick or digging up garbage, but you kind of gotta get there and it might take a little while 'cause you don't know how hidden that treasure is, but once you find it, it unlocks people. And so that's what I do is I unlock performance. Sometimes I gotta find out where that treasure is. Sometimes it takes me a little while on a wild goose chase.
But I can do it pretty quickly normally.
Dr. Grant Garcia: What, uh, I know we were in the sake of time for your time, but what percent, and maybe one of our last questions, what's your percentage of these players with slumps? Do you find that a lot of this is the, you know, you're unlocking something, right. It sounds like, to me, like I keep bringing up in the show is like, there is, it's, it's [00:45:00] everywhere, right?
I mean, how frequently are you getting asked to help a player? And then you realize that like your job is the most important thing, right? It's, they've done all this stuff, they've had the doctors check them, everything else is good, and now it's your turn.
Gary Chupik: Yeah, it's, it's, it's so weird. Like I remember Tom Brady, the Tom Brady said after Bill Belichick, the head coach, the most important coach on the team was the mental performance coach.
I. That was such a telling. And Pete Carroll told me one time, Gary the best, always want a coach. They always want, and Trevor Moad, my mentor, said, Gary, I talked to Russ 365 days a year.
I'm like, get outta here. Like what? Is there something so wrong with Rus Will? No, he just wanted to keep sharp all of the time.
And I just, I respect that so much. And so Trevor would always say, you don't have to be sick to want to get better. And if, for those of us who are, you know, if you're looking, you know, especially an athlete, you're looking for that constant competitive edge to be better. 'cause everyone [00:46:00] is good at that level.
You're always looking for that competitive edge. So, you know, I think living a lifestyle of high performance. Now kicks in and comes into play. So the question is, is can you live a high performance lifestyle? So I have something called the Game Plan for life, which is, so I have my elite mindset stuff, my process.
But what I learned was, was that if I can teach someone how to live a high performance life is, is you get to live on those two last pillars. The thriving and yeah, elevating or transcending pillars. And if you can kinda live between those two pillars, you live a totally different life. So I think the best players always want to get better, but it's the players.
And Pete Carroll told me this, it's the players who don't think they need coaching are the ones that need it the most. Hmm.
Will Sanchez: Yari. And I know we gotta let you go. Um, but before we do, I know you are a foodie guy, right? I, I know it. You love it. How did you know this? I, I, you [00:47:00] know, I gotta do my research here, so, we'll, we'll pose one question here.
Okay. So if you can have dinner, you can have an, an athlete, a coach, and maybe a, a spiritual advisor or someone from Faith, since we know that's part of background. If you could have these three individuals come to dinner, who would they be and what are you cooking?
Gary Chupik: Oh, man. Okay. So I would probably start up my smoker.
And I would be doing probably beef ribs. Okay. Would be my, my favorite. I was doing pork ribs forever, but beef ribs always going dry. Rub what? Do, what, what's going on there? Yeah. I would say definitely dry rub that. Yeah. Like, I like to enter competitions with my smoking. And so definitely that's the, that is the telltale sign that it's a, that that person's a good smoker.
So I would say, I would say, uh, you know, brisket and, and uh, and beef ribs and the three people who they would be Wow. Um. [00:48:00] So I'm a big fan of Saint Ignatius. Okay. Just 'cause I think we're body, mind, soul, and spirit. And he really focused on the soul part of, so like where your emotions come from, where your personality comes from.
So he would probably be one, another one would probably be Sigmund Freud. Um, he was so instrumental, I think. In, uh, in this field of psychology. And then, uh, you know, besides my Christian faith and being, you know, saying something obvious, um, I would say Tom Brady would be fascinating, just his mentality to be around him.
And I think most athletes pay a real cost. Like I think there's cost to thinking, uh, there's a cost to thinking well. And it, it doesn't come free. Like if you're gonna be an elite athlete at, at that level, you're gonna probably gonna burn a lot of bridges. It's gonna be really tough. Like you just, you just sort of expected the great Thomas soul.
Maybe he would be another one if I could invite four. Mm-hmm. The [00:49:00] historian said everything in life is a trade off. And that has been such an amazing phrase for me because now I can think to myself, well, yeah, I mean, I want something, but what? What's it gonna cost me? Well, it might cost me something that I.
I really enjoy what I really like, but that's the cost. So we call it the illusion of choice. It's like if you want to be average, you have lots of choices. Think of the menu at the Cheesecake Factory. You wanna be an average eater. Pick anything you want. You wanna be a good eater. You have to really limit the amount of choices that you have.
But if you want to be an elite eater, you have no choice. This is just how you. And so, uh, Thomas Sole, I think would be another one because it just, he really impacted my life. He has like, you know, his top 10 greatest quotes or things like, they're just mesmerizing. So I think it would be Thomas Sole as well.
Awesome.
Will Sanchez: Gary, thank you so much for your time. Uh, Garcia, last words here as we wrap it up. I just, I'm motivated.
Dr. Grant Garcia: I, I cleared my mind. I am ready to [00:50:00] crush my cases tomorrow. This is gonna be awesome. So, no, I really appreciate it. Thank you. I think this is really good. This will be something we can pop back on and discuss, uh, other times as well and jump back to this episode.
And this will be really great. I think that the listeners are really gonna appreciate it, the athletes listening, the ones that recovering from surgeries. Uh, so thank you so much for your time and it's really awesome to have someone like you on here.
Gary Chupik: Yeah. Thanks
Dr. Grant Garcia: for having me,
Will Sanchez: Gary. Tubik.
Dr. Grant Garcia: Founder
Will Sanchez: of Elite Mindset.
Thank you for your time.
Audio Transcript
Gridiron Rehab Injuries That Could Shape the Season

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon in sports medicine specialist Dr. Grant Garcia. He is not only a pretty face, he is not someone that you're just gonna listen to and watch on social media, but he is one of the top doctors. Out there. So check out his credentials.
Dr. Garcia, how are you?
Dr. Grant Garcia: I'm fairly certain that that intro changes every single time. I have no idea where it's going, so I just have to sit there and smile. I'm good. Yeah, no, it's a, it is a scorching day in Seattle, but, uh, super nice. So we're, we're lucky we're soaking up the last few weeks of summer, so.
Will Sanchez: 100%. And as the title showed, we're gonna talk a little bit about the [00:01:00] 2025 kickoff. We're gonna get into some key injuries for some of the players and, uh, and we're just gonna have some fun banter because this is what we do is football season. I'm super excited about this season because, uh, as some of you know, we are miserable New York Giants fans.
And once a while, long time ago, we were very happy with our team. Celebrating Super Bowl championships at the defeating the New England Patriots. But we've been suffering. That was a Dr. Grant Garcia: long time ago,
Will Sanchez: and I, I don't know about you. It, it hurt a little bit. I felt good for him, but it hurt a little bit to see Saquon win a championship more because he was with the Eagles than anyone else.
So I'm still trying to get over the season. What are your expectations for the Giants before we kick off this show? I,
Dr. Grant Garcia: I mean, the problem is, it's just, they're so hyped right now. They're like, they're, they're so hyped. This is like one of the best I've ever seen the introductions for the team. I think the challenge will be like, we'll see what happens in those first few games.
The [00:02:00] NFC East is tough. They have three really good teams they play against now, and there's no schmuck, quarterbacks or anything. I mean, it's just, it's legit. Every team is legitimate.
Will Sanchez: Yeah, they ranked, uh, the New York Giants as the hardest. Schedule for this upcoming season out of all 32 teams,
Dr. Grant Garcia: that's what they need for so and so poorly last.
Yeah, yeah,
Will Sanchez: exactly. You had the worst record where, here's the hardest schedule. Go off and be somebody. They've got the chiefs, they've got the Lions, Minnesota, the NF Cs, the A FC West. It is going to be a gauntlet and you know, if I have a, have trouble sitting there on Sunday. Trying to recover from the pain and misery.
Hopefully not from the Giants. This is not the same, but it's a weird segue. Let's shout out to the recovery shop. Can they help me recover on a bad Sunday?
Dr. Grant Garcia: They might be able to. They've got all sorts of things. So, you know, the, the nice thing is that this is, again, I, I, even today I had patients asking about this, so.
For [00:03:00] surgeons, it's nice to offer to your patients. They can use this for things extra they want, right? They want to have a nice machine, they want to do relists. They wanna have other different innovative tools to get them back. We're starting potentially working on more nutrition supplementation and other things as well.
So it's all part of this sort of package deal you can have for your recovery, and the patients have been elated with the service. And I have been as well as a, as a surgeon, to give it to my patients and hear about it. So it's just another thing that makes that whole postoperative recovery process good.
So thanks again for our sponsors
Will Sanchez: and shout out to Mike b at the Recovery Shop. So please reach out to Mike b He can help everyone out there. So we, uh, we can't thank Mike and the, that entire team enough. Listen. 2025 is gonna be real interesting. Before we get into some of these injuries, we, you know, we're gonna have a little bit of fun.
We're gonna talk a little bit of tech, we'll talk about some injuries. This is not a fantasy football show, but if you are a fantasy football fan and some of the people that we talk about help you make [00:04:00] a decision whether you're gonna grab 'em in the first round, or maybe you hold up to the second. Hey, listen, we're, we're, uh, we're we, we can help you in many different ways, but looking at the 2025, we have some NFL fun facts.
The international games, we know that football is global, is king of sports, at least here in, um, in the United States of America. Soccer rules the world globally, but for, for us, here it is, football League record, seven games. Oh, look at this. Where, what's that? That game up there. Chiefs versus charges. Where they're playing at.
Dr. Garcia.
Dr. Grant Garcia: Sao Paulo.
Will Sanchez: Sao Paulo. What, what, what are your thoughts on that one?
Dr. Grant Garcia: That's pretty cool. That's gonna be awesome. That's like, yeah, that's a big deal. That's a long flight though. That is a long flight. Uh, but that'll be really interesting.
That's, I mean, SA Paulo's off the hit, I mean, they do the F1.
: Yep.
Dr. Grant Garcia: Uh, in November. Um, so they've been really big and they, they had a game there, or didn't they have a game there last year or two years ago? I thought the chiefs, I thought the Eagles [00:05:00] played at some point, if I remember correctly. But maybe I'm wrong.
Will Sanchez: Yeah, I'm not, I'm not sure. If not, I would be lying.
But the fact that they're getting them, they, you can't have enough good, good games at Dublin. Obviously. We see a lot of college football games. They've been going out there. I know, uh, Notre Dame. Is a big fan of going out there. Lots of Guinness. We have a good time. Madrid, I love Madrid. I love Spain, dolphins and the Commanders.
I'm hoping that the Dolphins win, knock out the commanders because like we said, we're Giants fans and we could, anytime we can get a loss from one of those NFC East teams, we appreciate it. London, three times, Berlin. Uh, once real quick. This is not the topic of the show. Concerns with doctors, team doctors.
When you're traveling so much, you're traveling so far, making sure the recovery, what are some of the things, or at least highlight one specific thing that a team doctor will make sure that his, their players are doing.
Dr. Grant Garcia: I mean, as a team physician, your biggest [00:06:00] concern is not really the injuries, but rather sort of the sleep performance.
We've talked about this, we should probably get someone who manages sleep and athletes, because I think that would be a really good thing. I know we have some other episodes coming up, uh, that talk about the mental aspects, but the sleep is no joke. I mean, that is one of the hardest things for these athletes, uh, to deal with is how you change the sleep time zones.
I mean, I do. A lot of consulting things and I'm flying 24 hours down to Florida and back and, and that isn't a joke. And again, I'm not having to perform mentally. Yeah. Maybe a little bit physically, but not constantly doing that. I mean, the time zone is a big deal. I mean, this is, they're probably gonna leave a, I think they leave a little bit earlier Right?
If it's a, probably a few extra days. Yeah. Um, but generally they make them come right back, uh, on that next. Flight out for the following thing. So it's hard. I mean, the good news is they're all younger and healthier than we are. Yeah. So they can handle it a bit better. Mm-hmm. Um, but that, that is a, that's a topic in of itself is the, the challenges of sleep.
We brought it up once before, I think a couple times in our show.
Will Sanchez: [00:07:00] Yeah.
Dr. Grant Garcia: Um, but that is a big deal.
Will Sanchez: Yeah, we think it's important to just kind of highlight, but that's part of the recovery and that, you know, that's part of everything that these players can, are concerned about or could possibly lead to injuries.
Uh, quarterback carousel 12 new starters. Who knows? It might be more. We just know that that's kind of the way here in Seattle. Sam Donald Gold from Minnesota Vikings. Now the started quarterback for the, for the Seahawks. Uh, the Raiders get, um, you know, those old Seahawks quarterback, he's there. Our old friend Daniel Jones, he's gonna be the starter for the Indianapolis Colts.
So lots of moving and shaking. I mean, Aaron Rogers with the Steelers, you name it. Lots of storylines. This,
Dr. Grant Garcia: this is just the classic NFL. It's just a shake around the box, grab the quarterback and hope that there's a, there's a chance he's better than the last time we got them. : Yeah,
Dr. Grant Garcia: I, we'll see. I mean, we, it worked with Sam Darn.
But you know, it's, it's, unfortunately the roulette doesn't always work in [00:08:00] everybody's favor. So hopefully the fresh start for the Giants is the one that wins out.
Will Sanchez: Yep. And we, we will have Russell Wilson. We'll see how long he stays there, uh, before they'll start calling for the Dart Man, Jason Dart. So anyway, let's talk about this.
We wanna talk about some of the NFL Tech, and this was really fascinating because. The NFL always, you know, staying ahead of technology. They're using different, um, tech. For their players, for their organizations. I think it was a year ago, something like that. I was making fun of the urinals. That's a whole other conversation.
If anybody wanna goes back to that. My favorite
Dr. Grant Garcia: NFL tech. That is my favorite
Will Sanchez: monitoring, uh, hydration there with the UR urinals. But, uh, to, to kick it off the catapult GPS with speed, load and fatigue. Uh, why don't you talk about this and how that's beneficial to some of these teams, um, as they're, uh, partnering with Catapult for the monitoring.
Dr. Grant Garcia: I mean, the one thing [00:09:00] you always know is like all these teams that go after the NFL first or these, or these, uh, companies, right? Because if they can get them on board Yeah. They're willing to spend the money for their players to give 'em a little bit of an edge. Mm-hmm. And everyone's looking for that. I mean, you go into these team locker rooms and they've got tech you've never seen before.
They're like, oh, this is a startup. This company's a startup, and we're trying to get this. So the idea here is obviously you're. Using this GPS wearable technology. Um, and then you're really gonna get a lot more detailed information, like, again, like how fast are you're doing, what kinda load are you putting on, uh, the body.
And then by that, there's some calculations that can do algorithms to determine fatigue. And I, I think the key here is we always say like, as a cer as a physician on the team, you want to know when the player's too fatigued. It's very hard to figure that out. And so if we can find an algorithm or.
Proprietary information that'll tell us, Hey, this player is like, pretty close to getting injured. Or like, you know, you know what I mean? Like, you've seen it in the NFL, you've seen it little, you've seen it in all levels of football. The player's, like, I, you're like, you're out, you know, and the [00:10:00] coach is yelling them to come out and they're like, screw you, screw you.
I'm staying in. Mm-hmm. Right? Like, so can we, it's the same thing with the concussions, right? They have the helmets, not as much in the NFL, but our high school team, she's got, we, our trainer has a helmet monitor, right? When they get hit really hard, we'll know before the player will know. Yeah. And so the idea is that like, can we track all these things in real time?
'cause as much as they're players, they're also. They're owned by the, by the NFL teams and there's a lot of money on stand if they get hurt, which will show about how much the injuries cost. It is a massive amount of money. So can we find a way to reduce injuries And yeah, he's, listen, this person needs this, this guy needs two downs, right?
He's, we use him on first, let's save him for third or four or on the fourth tower going forward or something. So it, it's really important to all that stuff. I think that other, the other tech you wanna talk about, that next one's gonna be really interesting 'cause that is something that's more universal, I think with a lot of people.
Will Sanchez: Yeah. And right before I get to that, and I know that you're on the orthopedic side, so you're, you're, you're kind of getting the, you know, after the [00:11:00] injury has been, has happened, but is there anything that you're doing, or at least the people that you're working with, whether it's, um, a watch or whoop or anything like that, that you're kind of incorporating, or at least the partners that you have, are incorporating for the regular, you know, the regular Joe's that are trying to recover?
Dr. Grant Garcia: I think, I think the answer is we're always looking for something, but the problem you have is the market's really saturated. Right. The, the challenge here is like if I go and sell a watch, I'm competing with Apple, right? Like there was an article I read about one guy that had a fitness app and he was basically bankrupt until LeBron James happened to be the one of 200 people that bought the watch, right?
And it was like his last dollar. And LeBron James like showed it off in a commercial by accident and he went from that to like. A hundred million dollars in like a couple weeks by accident because just Wow. Sans happened to be wearing his device. So, and I've worked, and I've been part of discussions with, you know, as a, as a, on being [00:12:00] social media presence and being on the podcasting because I get emails all the time for New tech, uh, saying, Hey, you wanna look at my new product, this, that, and that.
And, you know, it's, it's really common. So unfortunately there is a lot of stuff that we do, so it's always hard to tell, uh, and to get really involved in one particular thing. And I, I think that the, I think that that's where more of the physical therapy side of things in people coming injuries, but also it's just really about stuff like this, right?
Can we talk online and say, Hey, listen, you really need to be using your watch, like your heart rate's dropped. Like, but we just don't have enough good stuff out there yet. It's all really expensive and it requires, you know, subscription based. It also requires someone, an algorithm to do it in, like, what they really need to do is like partner with a place like Apple or, or uh, Fitbit or things like that.
Yeah. And basically wear it on your wrist and it says you are getting fatigued. Like you were at, you were at a 64% chance of injury. You know, like from the minority report type of like Yeah, yeah. Fewer algorithms like ai, right? Can we predict regular people getting injured like, you're skiing and like you're just outta control like your legs are, or your [00:13:00] legs are gassed, like you're not firing everything in sync.
But again, it's. There's so many different muscles they have to monitor, but can you think about different things? So like, you know, maybe we're coming up with an idea, maybe we just let on some information that we shouldn't have, but who knows? So anyhow.
Will Sanchez: Yeah, I, I love the example that you just gave because I remember one time I went back up snowboarding.
I was like, I got one more ride in me, you know, and I got up there and I maybe got a quarter of the way down and I was like, oh no. Like my knees, I was starting, my legs were getting shaky.
And I was like, I still gotta get off this mountain. I should have stopped when I was still feeling good. I should have went to the clubhouse, get the hot cocoa, kind of relax, wait for the friends to finish off their last run instead of pushing it.
Anyway, I digress. This is what happens. This is what we do. Let's hop hop onto the next tech on the underwater treadmills, uh, joint protection, things like that. Um, let's talk about this. Joint protection and benefits of having these underwater treadmills, especially for these NFL teams.
Dr. Grant Garcia: This is huge. I mean, we [00:14:00] were winning the White Sox.
They had underwater pools. The underwater treadmills are expensive, but they're really nice. It's almost, I actually would think this is a little bit better. Then the, the G treadmills, you guys know those, they're very hard to find, but you basically strap yourself in and it lower, it lowers the resistance you can have on there.
Yeah. I've had a couple high level players, soccer players and basketball players that are basically almost pro level to pro level, and they usually, you use this and you could see the recovery difference is huge. Right. But again. The challenge here is like, how do you get access to this? Like, I'll be honest with you, outside of working with the teams, I've never even seen an underwater treadmill.
So like, it's not like you go to the gym and you're like, you're like, oh, there it is, right? Like, it's expensive. Like they have these treadmills actually for dogs that go underwater, but it's, I don't think it's the same, the same caliber. Uh, but nonetheless, the, the idea is that obviously it's just like blood flow restriction, right?
You want to put load on the joint, you want to have mobility on the joint without putting a lot of load. So when I tell patients like, you need 25% of your weight on the joint, well, you know, [00:15:00] when you get in the water, you lose a lot of that weight. It is buoyant. And so can you do this therapy low load the joint not cause inflammation, and then get stronger.
The, the whole key between like PRP and all these other injections is can we find a way to get that knee to not be so swollen so that you can strengthen the area around it and then therefore you can recover back to the level you were at without having continued setbacks. I mean, like, I, like I asked multiple patients today that are recovering from my surgeries, you know, the number one complaint was like, Hey, my knees have is a little bit swollen.
It still feels a little bit sore. I, I feel like I can't get the strength I want back 'cause it's still a little bit bothersome. That's pretty part, that's part of the normal recovery. But women have found a way to reduce that, right? If all these patients just went to the underwater treadmill, they could get it back.
So this is a big deal Now again. We've talked to and we will talk to more strength coaches for professional teams, right? And these strength coach professional teams will tell you that everyone has different philosophy. There's a, there's a general philosophy, but these strength and kissing coaches, which we, we [00:16:00] don't wanna let onto new episodes coming up, but we've had a few we've talked to.
: Yeah.
Dr. Grant Garcia: And the, you know, they, if they have a different philosophy, they'll say, Hey, I think the anywhere treadmill's best for me. This is best for me, you know, type of thing. So they're not always gonna have the same stuff. Now again, they also. They're very competitive, right? Yeah. So if someone's like, yeah, the chiefs have it, I'm sure the other teams are gonna be considering it, so
Will Sanchez: Oh yeah, definitely.
Um, force plates jump asymmetry. Um, we're gonna talk about that. They're, they're saying that the teams are known to use force plate ta, uh, plate testing, talk about forced plates and how they're so beneficial, um, for recovery.
Dr. Grant Garcia: Yeah. Well this is huge. I mean, we just saw this recently. You probably saw the, when, when we showed the Pro Mobil uh, video for Driveline.
Yeah. And you saw the guys jumping, that's the forest plates. Yeah. So the idea behind this is obviously. Asymmetry is humongous problem. I mean for, especially for soccer players, right? That increase the risk of ACL. Like these, when females, they land, they land in vow kiss. So I had, you know, three [00:17:00] female, or more than that, maybe four female acls just today, this morning.
Jesus. And, and they were all young females and they probably landed in, you know, they were at attack, they were injuries, like on the field somewhere. Hit somewhere every, but females are a much more common risk. And so something like this, you know, in athletes to find the how you're, how you're landing. So that's a preventative situation.
But also for professional athletes, especially for these professional teams. If the players like, oh, I feel great, but they're like, wait a second, no, you're not great, right? Like, this thing is off from this one. When we look at testing, we generally do asymmetry, uh, for acls and recovery. And so if you are, if your strength is down, your power's down, you have imbalances in that one knee, you're not ready to go back.
Even from a short period of time. But you know, the most commonly studied injury is acls. But there's so many of the things that we do and there's so many long recoveries, like it's really important for you to have this. And the jump asymmetry is that whole motion from the initial [00:18:00] takeoff to landing, and that's really where the power comes from.
So you really wanna make sure you're powering the whole leg appropriately.
Will Sanchez: Yeah. And that was a great segue to, um, talk about, uh, you know, if you haven't checked out our episode with Driveline, uh, that, that's a good one. So check that one out as well. Um, we're gonna go on to the next one. Sleep trackers.
We've talked about this in the past. Um, I, I gotta be honest with you, sometimes they make me a little bit nervous. I gotta be honest. I wake up. I saw that I didn't sleep as well. So obviously if you're gonna work out, it kind of tells you, you know, take it easy. Phone
Dr. Grant Garcia: alerted,
Will Sanchez: but at the same time, it makes me a little bit nervous going, I hope I got a good night's sleep.
Because if not, you know, it makes me feel a certain way. I don't know, I'm a little bit weird. I don't know if anybody else feels that way, but when it comes to sleep trackers great to know how I'm gonna prepare for the activity level in my day and how hard I'm gonna hit the gym. But at the same time, there's kind of like this competitive thing going, you know, I wanna hit a X amount percent on my [00:19:00] sleep recovery.
There. It's,
Dr. Grant Garcia: I I don't think that you're weird. I think that that's exactly what your other cohost does. So I think that what you're feeling is totally normal. That's the point of these apps, right? They get you hooked, they get you, you're like addicted to your sleep. But the problem you have is that you. It.
This is, so we had a, a while ago now, maybe multiple years, we had someone come in who used to be a Navy Seal and they do a lot of corporate stuff. So as for surgeons, we're known for high stress environments, very similar to some of these, some stressful things. Mm-hmm. Yeah. And they do a lot of stuff with professionals like that or athletes and help them get their stuff back. So companies will kind of monitor the sleep and actually help working with your staff and say, Hey, listen, you've got six surgeons on your staff, or you've got 20 players or 53 players on your team, and half of them are like totally undersleep. So that is actually a huge deal. We were just, this will be a good topic, maybe we can add this later, will, but longevity, right?
That's just athletics, but in longevity. Uh, read an article just. [00:20:00] Top 10. We won't go through all of 'em, but one of the number one things is outside of exercise was sleep. You're writing it down. I like it. Yep. But the, the, the sleep issue is humongous and it's the one that we can do. It's kind of messed up, but it's actually one of the easiest of all the things that we can do for optimization.
But it's also the hardest because it means we can't be doing fun stuff. We have to sleep, we have to like go to bed early. We have to like. Prioritize. And even though I continually harp on this and I know that if I get one more hour of sleep, I think I'll perform better. And I can know when I, my numbers go from, you know, I'm like a seven, I'm a six a low sixes.
I'm really, it's a, I can get through one or two days, but I really need, I really need to be a seven. Yeah.
Dr. Grant Garcia: and if I get eight, I'm like killing it. Right. But eight might be too much if I'm hyped up before surgery. So I'm more like a seven. See, I know my numbers. So the, the fact is like. When I'm at a, if I hit five, three days in a row, that's a disaster.
And so if you're an athlete, it's the same [00:21:00] way. Yeah. But you don't know it until you're tracking it. Right. Like I used to never know it until I had my Apple watch. Um, and now I kind of know and I actually, and you're right. But there is definitely a mental component. Like am I looking and saying, oh God, it says five.
Five hours and 30 minutes, like that's not good.
: Yeah. Yeah.
Dr. Grant Garcia: Right. And I don't know how well they work. 'cause I feel like sometimes I get less sleep than it actually says I did and things like that. But I, I definitely know that it gets me, I think it alerts you more to it and it makes you more aware and it prioritizes something that's a very simple fix.
And so I, it makes perfect sense to me why sleep quality and duration is so important. And I, I hate to say it, but my, my patients ask me all the time, like, what else can I do? And like, this should be brought up. Like, you can sleep more during your recovery and, and you gotta find ways to do that. You gotta be active, you gotta, you know, shut down the electronics an hour before.
Yeah. Yep. You gotta get clear the mind. I mean, there's nothing, like, the worst possible thing I've ever, I ever do in the last few weeks was check my email. Two minutes before I went to bed and found an email that made me frustrated. Oh, no, no. For some reason or another, gotta respond. I mean, it had [00:22:00] happened to me last week.
It was the stupidest thing ever. And so you can't do that stuff to yourself. You really have to stay fo, you have to really focus on, just clear your mind.
Will Sanchez: It's hard, you know? It's, it's amazing. Like you, you've heard Mark Wahlberg talk about, I go to bed at 8:00 AM and I wake up at, at, you know, at, I'm sorry, 8:00 PM wake up at 4:00 AM and I go work out in the train.
Go, there's that eat and go back and train and work out and sleep. And that when you go on the David Goggins of the world and so many other, uh, high level athletes or performers, um, I'm envious that they're able to be so dedicated and get to bed and get X amount of sleep. Now, I don't know if they're lying.
I don't know if it's just the social media, you know, where they're saying they're doing X, Y, and Z and you know, maybe most of the time they are and they're not. But, um, it, it's a hard thing as you, as you. Preface it. It's easy, it's simple, but it's not. So I,
Dr. Grant Garcia: I think actually we should try to find a sleep expert.
This is gonna be really good. I have it right now.
Will Sanchez: Sleep and longevity. We're, [00:23:00] we're ready to go. We're definitely ready to go.
Dr. Grant Garcia: So the sleep. So one more thing on the sleep. So another thing is they showed professional athletes and some of the best athletes in the world actually sleep a ton. Ronaldo, he does, they said he does 14 hours a day.
Now, again, I don't know how that's possible, but is he a dad?
Will Sanchez: We need to
Dr. Grant Garcia: show the, we need to show the sleep. There's a, there's a sleep bar graph. I know we're di I know we're gonna, I know we're going off topic, but there's a sleep bar graph, which we need to show the, the viewers at some point and it shows a bell curve and there are, there's, majority of people are in the seven to eight.
There are people in the nine to 10 and 11 hours. I know my best friend is actually an a 10 hour person. What? Which is unusual. Yeah. It's crazy. Yes, I know, and he'd be laughing if you heard me talking about this, but he is a solid nine to 10. Every time we were college roommates it was nine to 10 hours solid and it, I, there is people on that bell curve, but there are also people which have these special abilities that can do four to five.
And so this will be a great topic to come up with later. 'cause I kind of love this [00:24:00] idea. I love thinking about this 'cause I always wish I was a four to five, but unfortunately the four to five also lives shorter. So there is a, a whole nother discussion topic.
Will Sanchez: My, my wife has a, an incredible skillset that she can take a nap.
We could stay up for an hour and then it'll be like bedtime and she can go back to bed and not have any issues. I take a nap. I'm up to two, two o'clock in the morning. I don't, I don't know how she does it. It's a superpower. It's amazing. It's a
Dr. Grant Garcia: superpower. It's your wife and you just shouldn't ask questions.
That's problem. The problem is that you're even thinking about it. Follow to you.
Will Sanchez: I'm making sure she's not looking at me.
Dr. Grant Garcia: I think she follows us. We might be screwed right here. We're gonna have to mute this out.
Will Sanchez: That's all right. Okay. I will, I'm gonna edit this out. All right, let's talk about helmet sensors.
We've talked about the, the helmets, we've talked about the guardian. There's so many, so much that's kind of going toward the helmet, toward the sensors. Um, let's just kind of get into a little bit. More about that and the benefits of the helmet sensors and [00:25:00] how teams are utilizing them. Um, I just kind of, I put this together, it said the NFL had a pilot program using helmet sensors to measure impacts, but this was suspended due to concerns over data accuracy, and we're gonna get into that real quick.
And reliability according to science and ESP. While the specific program was halted, the lead continues to research and invest in advanced concussion assessment tools, including eye tracking technology and impact sensing mouth guards. Dr. Garcia, when it comes to accuracy and re reliability, that's one thing. And then going into the other assessment tools, what are your thoughts on that?
Dr. Grant Garcia: I don't mean to smile, but I'm smiling because this happened to us on our teams. So we had the tracking sensors, the impact sensors, and one time my trainer looks at me and she goes, check this out. And like the, the player was just running around.
It just showed they had a massive impact. So, oh, there, there is some inaccuracy in the sense that it might over call things, um, or sometimes it doesn't, doesn't register it. Now [00:26:00] again, that was 3-year-old tech. Not in the NFL. And so was it the top of the line? Yeah. I don't know. The challenge you have obviously is they're getting hit.
They have these like chips in them and registering. And you also gotta be really careful, right? Because the last thing you wanna do is pull out your player during a playoff game because it says they got hit really hard and they have no symptoms. And then you gotta do a full assessment. So this is really complicated.
And the other thing is like, what do you do with that data, right? Like if you, if you see it and they get hip, but you know it's not accurate, but now you've got it documented. As a team physician that this player just had a massive hit. You kind of have to pull them out. For medical legal reasons. So it's really tricky.
And the NFL obviously there's a lot of money and there's both two sides to the story, right? There's the owners and the players association. Yeah. And so did the, did the players want them tracking them? The players don't wanna get pulled out because all of a sudden now they, they, they took 60 snaps instead of a hundred, uh, 70 or 80 snaps, and maybe they dropped their contract.
Right. And they're gonna be like, oh, well you keep getting hits on the, on the thing. Yeah. So there's the, [00:27:00] this is a business, this is a, this is a. A big, a lot of money involved with this, and unfortunately you want to protect the players, but at the same point, there may be situations where if you, you don't wanna have mismanagement of the system or inaccuracies.
So until it's perfect, it's gonna be really challenging and it's gonna be a lot of work. We know this is like always on the forefront of them because
: Yeah.
Dr. Grant Garcia: Concussions, we've talked about this at nauseam. Yeah. Especially with the recent two episode we had and other issue, other episodes we've had regarding this, like this is. This is their hot topic. If they could choose one thing to figure out and be done with, it'd be concussions.
Will Sanchez: Yeah, I, I agree o over anything else, right? So, and that, whatever. I'm not gonna get into it 'cause we've, we've gotten into this discussion and you know, so anyway, I'm gonna move on 'cause we're already yip yapping for almost 28 minutes.
So let's kind of show this here. Uh, the trends last year. Apparently everything kind of went down a little bit. 17% overall. Awesome. Less concussions, uh, kickoff con concussion, 43% [00:28:00] with the new rule. So it, some of those, I'll just quick recap. You no longer allowed to run down the field. You're no, no longer able to load up extra players on either side of the ball.
It has to be the same amount of players you're kicking off into a specific area and then no one's starting to run until the ball is. Caught or lands in that area. So the con, the collisions are less. You don't have someone running down 30, 40 yards to field before they smash into somebody. So that's makes sense that the concussion rules, uh, have led to less concussions, a drop of 43%.
Kickoff leg strains. That's really kinda interesting. 48% lower extremities strains in general. I don't know what to make of that. What does, what does that mean? Lower extrem, uh, lower extremity strains? Is that just kind of fall under some of the, I think that's
Dr. Grant Garcia: like hamstring, quad, achilles calf. And it makes sense, right?
Because the, I'm assuming that's not just the, the, the [00:29:00] kicker. Yeah, but like you're going full. Like those guys go so much faster than the average player. 'cause like most time, like you're not getting a breakout, right? Like maybe the wide receivers are running for a route, but generally, unless there's an explosive play, they're not very far distances, but the kickoffs, you're just going as fast as you can.
And a lot of those players aren't playing the rest of the game. Yeah, right. So they're not warmed up and then they're like, let's just go as fast as we can to make my mark. I gotta get the tackle. So they'll take me off special teams and put me in the regular game.
Will Sanchez: 100% and that, and that is coached, right.
You know, you've, you work with high school football teams. I've worked with high school football teams. That is something that we used to say, you run down there and if you're, if you're the first one, be the first one down there running through the end zone. Even if you see on fair, you know, catch a ball, they're running through the end zone.
So that kind of piggybacks. They're flying as fast as they can. Having these collisions. We talk about cost not only in this show, but on on previous shows, the cost of injuries, right? We, we mentioned it [00:30:00] when we were talking about basketball, uh, and now we're talking about football. It's just some of the numbers there.
Bucks. 23 million last year, 21 million for the Steelers. And this is not even true numbers to me. I think that some of these, I don't think those are true. Yeah, they're, they're not. Those are, those are too low. That's just a portion of some of those numbers, not including the ones that got hurt before the season started that went right to the ir, you know, things like that.
So, but it, it becomes interesting, um, as far as the topic of just saying. Injuries, cost, money, and NFL and every professional team are gonna do everything possible to reduce injuries, whether it's tech, whether it's sleep, whatever it is, they're gonna keep investing in that money.
Dr. Grant Garcia: Well, and I hate to say this, but no matter how expensive everything is, it's not near as expensive as the player getting hurt.
What So there is, there, I know the cost of a lot of these things and they are not even [00:31:00] close to a 20 million.
: Yeah,
Dr. Grant Garcia: they can't. They won't. No. What team's gonna pay that money? But the fact is you have something that's, you know, we talk about products on here, there are sometimes 200, 500,000. That's a lot of money for the average person.
: Yeah. But.
Dr. Grant Garcia: For an NFL player that's making 20 to $30 million a year, that's around. I mean, we talked about what before, got 55 million a
Will Sanchez: year. What if he's out for the year? $55 million investment.
Dr. Grant Garcia: Or what about, we talked about this before with like, LeBron spends a million dollars a year on his thing.
That's a, that's like a, that's a rounding error for him. That's nothing. But you know how much ti much he can get for that? A lot because a million dollars is still a lot of money. Yeah. And so as a result, these guys will do whatever it takes and there's no number. We, we could, we can go at nausea and different players.
We might not, probably don't have time to go through everything, but the idea behind this is like if you find anything that reduces injuries, it's game changer. That's why the guardian helmets blew up. Right. It is like reduce the concussions for practices. Increase it for certain players, like that's a big fricking deal.
I mean, concussions are a nightmare. [00:32:00]
Will Sanchez: Yeah, and you know, and we've seen it, uh, we'll talk about a couple players and then we'll just kind of wrap it up. Obviously our focus was on the tech and, you know, the, some of the excitement about the NFL, but, uh, key players to kinda look at Matthew Stafford, 37 years old, low back, uh, uh, disc issues.
Uh, he's had back issues in the past. He's played her tough guy throughout his career. A long career concerned because once again. Of money starting quarterback for the Rams. You know, if he stays healthy, they have a team that can be a playoff team. When I say low back disc issues, what is your red flag?
Dr. Grant Garcia: I mean, red flag is the idea behind, like, what's that?
Not only is the disc out, but is there more damage to the actual, the two spaces and it becoming a little bit of arthritis in that area. Um, and he has a disc. He's getting injections. He's probably getting PP, he's doing traction. He's doing all sorts of fancy things under the sun, but he's not gonna get a surgery and Right.
So if he's got nerve issues, if [00:33:00] he, you know, lower back pain from disc can happen. That's really common. And the nerve issues are the pre problem, right? Because if he starts getting nerve weakness, he herniates more. Like those are bigger issues and we know we've had a couple other high level players in the basketball realm, just recurrent, right?
And those things are nasty. I mean, disc, I've had this before. It's horrible. And so the idea is like, you don't, you really don't want to do it. You don't wanna have, if you can, and obviously of all the injuries, like you get a, you have an injured arm or something, he can still throw, you get a little bit of a leg injury, you can still push through it, but lower back, like everything's involved with that.
So anyhow, it's, it's not, it's not a great thing. But to get these, tend to be more chronic and I bet you'll play through it. He'll, you know, get an epidural, make it four or five games, throw one more epidural in there. They'll get 'em through the season with us most likely.
Will Sanchez: Um, you've had back issues, you've had back pain.
How does a 275 pound man run at you and then hitting you and laying on top of you? How does that, how does your, how does your back feel when I say that?
Dr. Grant Garcia: Well, if you're paying me $55 million, I might change [00:34:00] my response. Um, but if I had to just take that hit and not get anything for it, I think that the answer is that I'd be pretty, pretty terrified.
Will Sanchez: Oh man, Tyreek Hill, one of the most explosive wide receivers in the NFL. Um, he's coming back from an oblique injury, right? This core injury for an explosive wide receiver, not a big framed, uh, player. I'm not sure if that matters whether the, the size of the player, but what are some of the concerns with, uh, with this type of injury?
Dr. Grant Garcia: Well, these injuries suck. Look, that's all I gotta say. I mean, so the, the answer is that like the, the problem with the obliques is people don't realize is like all your power comes from your core, right? Like they're like, use your core. Use your core. Mm-hmm. So these oblique injuries, these rib injuries, the intercostal injuries, they are really, really tough.
They're painful. There's really nothing you could do. Uh, I can tell you this 'cause I just recovered from one of these. I was foiling and I fell at 20 miles an hour and I had a, oh. Bad intercostal, and I thought it was totally fine, right? I could push through it and after the week of trying to push through [00:35:00] it, it just got worse and worse and worse.
You couldn't do core exercises, you can't do anything. You can't run, you can't lift. Even though every other part of your body feels good, it's literally just hurts to do anything. So these, this is a, this is gonna be a challenge for him. He's, you know, he's relies on speed, right? That explosive speed that he has.
Yeah, yeah. Change your direction. Yep. The other challenge is that just they're usually not fixed and you just sit there and wait for them. Now again. The challenge is which type of core injury? There's lots of core muscles, so if it's something that he can get through, maybe he'll push through it. We wrap him up.
What the like reinjury. I mean, if he doesn't wanna wait for it to reinjure, it doesn't to heal. It could happen continually and then it could full tear. Now again, it depends, right? There's, there's always like three levels of most of these. There's like the partial tear. Or the, the like small, tiny tear.
There's a full, near full tear and then full, full tear. Yeah, full, full tear is usually surgery again. Depends on this area. Um, probably has a one or two, probably more like a two if they're bringing it up. Yeah. Uh, but I mean, generally these do end up returning to stuff, so I think it's [00:36:00] just gonna be a little bit of challenge.
Will Sanchez: Uh, this player's not gonna play this season. Um. Uh, Rashaan Slater, he, uh, signed a massive contract with the, with the Chargers, uh, trying to protect their quarterback as we talk about injuries for quarterbacks, the patella tendon rupture, even though he is not gonna play, it's something that's kind of right up your alley.
So I wanted to bring it up, you know, what does that entail? Especially for a man that size, he's gonna miss the entire season, you know, that patella tendon rupture. How does that affect him going forward?
Dr. Grant Garcia: I mean, this used to be the player killer. Right. I mean, with this before, some newer techniques, this was a 50% return to sport.
Yeah. So one of the lowest in the NFL. I've talked about this before on previous, I think, radio shows, and then I think we had it on here a while ago. Um, but this is, this is not a good one. Uh, the good news is that we've got some new stuff. I mean, they'll do. Standard repair. We've got videos even on the website of how we do this kind of enhanced repairs.
They, you know, they, now we add, now we add internal braces. If you've done correctly, it's, [00:37:00] it's a little bit trickier to set the internal brace of this 'cause it's so much flexion. Yeah. So you don't wanna obviously put an internal brace that doesn't move. Um, but there are, there are lots of tricks that these docs can do with some newer implants and techniques.
Um, and we have definitely seen a higher return to sport over the last few years with this injury. So I wish him well, but this is a solid seven, eight months.
Will Sanchez: Um, let's saw Christian McCaffrey. I'm kind of jumping around. I have a long list of injuries, but you know, for time I'm gonna jump around and kind of key on some of the, the top players.
Uh, Christian McCaffrey, 49 ERs running back all pro stud, uh, coming off the season, uh, that he sustained an Achilles injury. We're gonna talk about some of the recovery a little bit later on. What are some of the concerns? He's had quite a few injuries, even though his production has been high. He's had a lot of injuries throughout his career.
What are some of the concerns with that Achilles injury besides, you know, what we've normally talked about?
Dr. Grant Garcia: I mean, the challenge with him is it's, it's not a full [00:38:00] rupture. Right? So it's just like dealing with the inflammation. Dealing with the inflammation. Bilateral tendonitis is not ideal. You know? And this is also a guy, like you said, he's very productive, but he's, he continues getting injured.
I mean, it took him, all, people couldn't figure out what was going on with him for weeks. Yeah, yeah. Right. He just wasn't back. Right. That's never good. Like the thing is, if they're not publicizing what he has, they might not know how to fix it. That's, what does that
Will Sanchez: mean? Bilateral Achilles tendonitis? Just for the people that don't really understand what that means.
I mean, Achilles, I'll be honest. It's clear, right, but what does that mean? Yes, I,
Dr. Grant Garcia: I mean, Achilles tendonitis is basically like, it continues to hurt. The idea of that tendonitis means that there's inflammation in the tendon. So he's just got, every time he is running, and he's probably pain in the back, his ankle.
The challenge is right, like, is this tenitis gonna lead to rupture? Well, bilateral rupture is pretty unusual. Achilles can happen. K McCaffrey's not really the type of guy that would get it, but he could get it right. You know what I mean? Like usually it's bigger guys, like the, the defensive ends and you know, the linebackers, [00:39:00] he's a little bit built a little bit differently from that, but it can always happen to any of these high level sprinting players.
Um, but I mean, that guy has tried everything, you know, I think he went to Germany for some specials, type of cell injections, gyros, he's gone.
Will Sanchez: He's doing gyro, gyro
Dr. Grant Garcia: stand,
Will Sanchez: you know, that, uh, doing a, but, and here you go. Not to start any, any, uh, any rumors here, but the 49 ERs traded for Washington. Uh, commanders starting running back.
Brian Robinson, uh, right before the start of the season. So going back to what did the 49 ERs know, even though McCaffrey's saying I look good, I feel good, I sound good. I, you know, everything's in order, but the 49 ERs go, yeah, we're gonna trade for another running back. You know, besides what they have, so, you know, if you're in the room, what's the, what's the thought process there?
Dr. Grant Garcia: Thought process is you need an insurance policy. I mean, he could do everything he wants, but the problem you have is, a lot of this is talk, like we've talked about before, like we talk about all this tech, but does it really work? [00:40:00] Right? Is it really getting you that much better? Like yes, but like, do you, I mean, McCaffrey would be good probably without any of this stuff.
Like he, he was, he's naturally talented. Right? And he's, he's the same thing we talk about with some of these other players, right? Even when they're a little bit injured, they're still better than most. So yeah, the challenge is are you gotta be able to pick up and right. And he, he knows he's now more on the chopping block than before.
Right. He's been out so much. Is it worth paying him? Is it worth doing all his things? And hate to say it, he's kind of getting old for a running back. Yeah, it be, yeah. He's a tremendous lifespan of running backs are a challenge.
Will Sanchez: I mean, he's exciting, he's great to watch, you know, it's just, uh, injuries.
Right. Um, I want to touch on two more players and then, uh, we will get ready to wrap it up. Uh, Jonathan Brooks from the Panthers, ACL. The reason I bring it up, because there's bio biologics, there's some graft shifting. Is this a lavender style kind of, uh, surgery [00:41:00] that Jonathan Brooks may have gone through?
Is, is it our, our buddy Chad Lavender? Is he involved with something like this?
Dr. Grant Garcia: Uh, I wouldn't be surprised with this one. The challenge here is that the biologic, ACL requires a quad, so it's a different type of graft. The issue you have is that a lot, even though the quad ACL is a very popular graft, I do a lot of matric, majority of my acls, which is the similar thing that what lavender was saying.
The challenges that patella tendon, which is what most of the professional athletes get. Like even Ella, who's amazing surgeon. Yeah, yeah. He, if he, he's he love, he likes the quad idea, but he's kind of like. And you know, in the NFL, he is like, I'm not NFL player. I'm not gonna mess with it. Right. I'm gonna do the Patel attendant.
That's what we've been doing for years. That's the, that's the option. And so, but we all know that, like nowadays with this, with the media and agents hearing more stuff, like something like the lavender ACL would get picked up on and potentially could he return a bit faster? Yes. But we [00:42:00] also heard from lavender and he wanted to emphasize this, this is not like four months, this is six months.
So it depends on when he has the ACL tear, is it even worth it? Right. You know what I mean? Yeah, yeah. Or is it just like they're going to, the thing is to me, I tell people there's no downside. If you wanna return in the same window. You want to have the biologics to hopefully help enhance the bone to bone, the healing of the tendon.
Yeah. There's no downside, but the costs right in the NFL, they don't care. That's cost. It's small cost. Yeah. But for my, I mean, a patient this day that asked about the fertilized acl l they wanted the bio acl l and I said, here are the risks. Here's the benefits from the podcast. Here's some understanding my research.
Um, you know, and they, and they opted in that space actually to not do it. But sometimes they play, you know, I have someone, I have one a couple weeks that wants to do this. They want everything under the sun to get back to the best possible level. Gotcha.
Will Sanchez: That'll be interesting to see how he recovers and, and get a little bit more information.
Uh, last but not least, um, really, he was in the running for defensive player of the NFL last year, the heart and soul of the [00:43:00] Detroit Lions. I think if he would've been healthy, I think they could have gone to the Super Bowl. I think they potentially could have beaten the Eagles and advanced, uh, Aiden Hutchinson, uh, for the Detroit Lions went to University of Michigan. Tibula, fibula, fracture, surgical, uh, nail fixation, advanced bone stem. What Yeah. Does all of that mean?
Dr. Grant Garcia: So you, you said it well, which is good. So basically, we've had this before, some of the players where they snap the mid shaft, this is actually what Alex Smith had.
: Yeah. So, but
Dr. Grant Garcia: his was open.
: Oh,
Dr. Grant Garcia: much worse.
Yeah. Yeah. So when you break the middle of the, the bone and the tibia. It can just be a break, which is bad. It can be a break with a hole. It can break with a bigger hole, and the bigger the hole, the increased risk of infection and wound complications, which is what Alex Smith had.
: Yeah,
Dr. Grant Garcia: but a clean break with maybe a poke hole or nothing.
Usually what they do is they could put a rod down there. The nice thing about the rod is that it's [00:44:00] instantaneously stabilized and it's inside the knee, so the incisions are really small, right? You go from a certain angle, you usually put it from the top down in someone's leg, and it can stay there permanently.
From the kneecap, correct? Yeah. Uh, there's two ways to do it, but usually from the kneecap areas, the way you do it then, are you keeping it
Will Sanchez: it permanently or is this something that's an option to take out? Because I've heard different variations. Go
Dr. Grant Garcia: ahead. So generally you just take out the screws that hold it in.
Imagine you gotta like, you know, you got the, the big pipe in there and then you gotta pin it right. To keep it in there. Yeah. So a lot of people get the screws out. 'cause taking the pipe out is a nightmare. Oh, you can do it, but you can imagine it's very hard once it grows in to try to pull that thing out and things are so that's actually
Will Sanchez: right.
And they, they're healing around it as well.
Dr. Grant Garcia: Like, we have one guy in our office, our PA that loves to take him out. So it takes him like 30 minutes of just hammering to get this thing out. And we literally, him come to every case. He gets so excited to help out. But anyhow, so the, the long story short is like generally we leave the metal in there.
Um. Then the advanced stem, I mean, the [00:45:00] idea here is like, can we make someone heal faster? Right? Like that's the whole point of the biologics. Can we, and again, the stem for a general patient would be really hard to get, right? Like, I can't get these, I can't get these approved half the time for insurance.
Yeah. Unless they have a really, really bad issue. But obviously, you know. No big deal, just throw some money at it and get it to heal the bone stimulators do help. And so the idea is like anybody's willing to do it. If it was me and I had to pay outta pocket to so I could heal and walk faster and run faster two months later, earlier, I'd definitely do it.
Will Sanchez: Wow. Okay. I'm grossed out a little bit on that one. Um, are you, before we wrap up, are you, are you, you, I think you want some trivia, right? You want a little trivia? A little NFL trivia to kick off this season. Everybody loves
Dr. Grant Garcia: this part.
Will Sanchez: I think I know you love it. This is your favorite part. This is better than surgery right now.
That's right. I love it. I love it. Okay, listen, week eight, if nobody gets hurt, this is, which is we're talking about injury. Uh, Michael Pennix from the [00:46:00] formerly from the University of Washington for Atlanta Falcons is going to match up with two uh, taco Viola. It'll be the first time since 2000, I believe 12.
Since two left-handed quarterbacks have started against you against each other, which is really, really interesting. Can you name the last, there's only been two Super Bowl winners, super Bowl quarterbacks. Can you name either one of them that have won a Super Bowl, the last left-handed quarterback to win a Super Bowl?
One of two.
Dr. Grant Garcia: I'm like, in my head, I'm trying to think about them playing, but then half the time you see 'em, they're like, you're seeing 'em from the other directions. So you don't even know. I don't know. We'll say Kurt Warner,
Will Sanchez: he's not left-handed.
Dr. Grant Garcia: I have no idea. This is absolutely impossible. Trivia.
Will Sanchez: All right, so the hard one is Ken Stabler.
Jake the Snake finally got into the Hall of Fame [00:47:00] postmortem and, um, Steve Young. Steve Young.
Dr. Grant Garcia: Oh.
Will Sanchez: Last left-handed quarterback. Uh, interesting. There's only been 11 left-handed quarterbacks to come into the NFL since Michael Vick got drafted back in 2001.
Dr. Grant Garcia: That's crazy. Well, it's less common. I mean, I'm left-handed.
It's 10%.
Will Sanchez: Why, why do you think, real quick before we wrap it up, why do you think that we're not seeing left-handed quarterbacks, uh, in the NFL?
Dr. Grant Garcia: First off, there's not an advantage. So if you're not an advantage, like in baseball, there's an advantage, right? Like in you're
Will Sanchez: onto something. I, that's my thought. I think what you're doing is you're getting left-handed hard throwers and you're getting them to commit to baseball.
Instead of football,
Dr. Grant Garcia: which is more lucrative. It's much more lucrative.
Will Sanchez: That's my guess. So,
Dr. Grant Garcia: yeah, I mean, I agree with you.
Will Sanchez: That's my guess why we're not seeing left-handed quarterbacks, but they're going, wait, if you're left-handed and you throw [00:48:00] 98, don't go throw a football, go throw a baseball and we'll make you filthy rich and a 275 pound man, it's not gonna land on.
Dr. Grant Garcia: Well, I also would say that you don't have to be as good and left-handed. Does that make sense? So like, you're not even like, they're not even getting that level. Like if they're that good, they're getting recruited hard from the baseball, but like, they're just pull basically, basically baseball's pulling anybody that's decent thrower that's left-handed.
: Yeah.
Dr. Grant Garcia: Because there's so, there's so much less common, right? Like if you have, if 10% of the population is left-handed. Ideally you have the same amount of throwers that are right. You, you have the same, probably less. You have only 10% that throw as hard as Right-handers. That's a small pool. And then they're throwing 'em so much money on them 'cause they're so uncommon.
Yeah. But that's why you see so many more left-handers in MLB, but it's actually not even close to equal.
Will Sanchez: All right. Let's say goodbye. We went over our time because that's what happens. Um, thanks for listening to Sports Doc talk. Check us out sports doc talk.com. We have transcripts, we have shows, uh, check out our [00:49:00] polls.
We are getting requests for, uh, topics and new shows. Thank you for everyone that's reached out to us. We've had plenty of people reached out and email us. Um, we we're very thankful for our guests, so. I don't know what else to say. Dr. Garcia, you wanna wrap it up?
Dr. Grant Garcia: Yeah. So thanks again to all listeners and, uh, for the, we had a lot of guest requests this summer, so hopefully we get to see some of those show up.
Um, and again, if you're interested in being a guest in the show, let us know. Obviously it's important to us that. We get a lot of requests that may not fit the show book. We're really gonna try to stick with this sort of orthopedic sports, uh, kind of innovation topic. But, you know, it doesn't hurt. Reach out and we'll, we'll vet it and see if it works for us.
So thank you. We really appreciate everybody. Let's go Big blue baby.
Audio Transcript
Faster ACL Recovery: Inside the fertilized ACL Technique with Dr. Chad Lavender.

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon in sports medicine specialist Dr. Grant Garcia. Obviously, Dr. Garcia is paying hefty money for his chat. GBT background for his mind is looking a little. It stabs me in the head there. I mean, I'm, no, I, I don't know what
Dr. Grant Garcia: you did.
I'm gonna have to work on some of your typing skills. I don't know what's going on over there. Yeah. Okay.
Will Sanchez: Yeah, yeah, I definitely do. Listen, we're really excited about, uh, our guest today. Uh, but before we get to our guest, Liz Handel, a little housekeeping there. Uh, you know, we love Mike B and The Recovery Shop, but who can talk about the Recovery Shop better than You can take it away, [00:01:00] buddy.
Dr. Grant Garcia: Yeah, so again, big thanks to our sponsors, you know, from these, for any surgeons out there. This has really been nice for me because the patients always ask what extra we're gonna get into, extra you can do during the surgery. But how about after the surgery? Right? So after the surgery, the ability to have sort of sort of advanced rehab stuff, nutrition, things like that, it's all available here.
And the nice thing is each surgeon can have a customized page for their patients. So it really is nice. It's sort of like an a la carte option. So my patients in Seattle, they love it. They're always asking questions on what else they can do. Um, they're gonna, we're gonna bring up one of the topics they talk about all the time, but before we jump to that, uh, this recovery shop thing is awesome.
So look into it.
Will Sanchez: Yeah. And maybe they can find a way to fix my background since they're able to fix everything else. So I don't think that's what they mean by the recovery shop, but shout out to Mike B and everyone else, uh, you know, we really appreciate them. Listen. We don't care about the doctor that's coming on because he's the pride of Chesapeake, West Virginia, [00:02:00] right? He is the pride of West Virginia. Let's bring on Dr. Chad Lavender. Dr. Lavender. Listen that, how big is that town? That town is less than what? 1500 people? 1200 people. I mean, you must be the talk of the town. Not only. In your town, but across the United States, across the globe. But what's the feedback just getting, uh, you know, from, uh, the folks in your town?
Dr. Chad Lavender: Oh, you know, I think, uh, so I practice maybe 30 minutes from where I grew up and, uh,
Will Sanchez: beautiful
Dr. Chad Lavender: in, in a, in a slightly larger town. Not much. But, uh, you know, um, that's part of the, the beauty of, uh, being here, uh, where I grew up is I get a treat. Fan, you know, basically my extent of everybody here is related some way to me, right?
So, um, you know, many people I've known all my life or their kids, you know, and I think, um, so that's why I've chose to stay in this area, uh, is very fulfilling.
Dr. Grant Garcia: So, again, to overall, to introduce him, [00:03:00] uh, Chad Lavender is Marshall Orthopedic Surgeon. The big reason, obviously he's here for many reasons we'll get to in a second, but you guys have all heard the thing we've talked about at numerous episodes even before we had our video episodes, the Fertilized ACL.
I will tell you that pretty much weekly to every other week, I get someone asking about this. I hear it at conferences. I work with Arthrex too, just like Chad does. So I get people talking about this as well. This is a very hot topic and we'll get into in a second why it's so important. Then obviously we got some other twists and turns here. So we're gonna talk about the nano scope. We've heard about it with, uh, we talked with Chubb when they talked about how his recovery was better because of the nano scope surgery he had done.
So we'll pop in and ask Dr. Lavender, who's sort of a specialist at this, and then obviously as a football player so we can tell us about his experience with little players and how that coalesced.
Um, and then just classic board certified. So this is awesome. So thank you so much, Chad, for coming on. I think everyone's really excited. I. I want to, you know, kind of hear more about [00:04:00] your background, maybe kind of, I know you told briefly, but sort of how'd you get to this point, and then we can jump into some of the topics.
Dr. Chad Lavender: Yeah, so we talked to a very small town in West Virginia. Uh, very blessed to have a great family, uh, support and, and community support and coaches. And, uh, ended up, uh, walking on at WVU and played backup long snapper there. Um, and then went to medical school at WVU and then attended Marshall, which is where I currently work for residency.
And then I spent a year specializing in sports medicine in Richmond at Orthopedic Orthopedic Research of Virginia.
Will Sanchez: So nice. Yeah. Dr. Lavender, I, I, I know what you do is really complicated. Um, and you know, as Dr. Garcia mentioned, you know, we've talked about, uh, this procedure in numerous shows, so we're really glad that you're here.
But is there anything harder than walking on to West Virginia and China? Get on the team team as a long snapper, and not [00:05:00] only getting off of that season, but pretty much the, the seasons that came after that. How difficult was it, was it to just be in that situation and be blessed to be a part of that university?
Dr. Chad Lavender: Oh, it was, it was a dream of mine. You know, to be able to live your dream is something very few people. I get to do and I had a dream to do that and then be an orthopedic surgeon and I'll tell you that I can remember vividly coach Neland, he looked at us, our first team meeting and he said The hardest thing that you'll ever do in life is maintain on this football team for four to five years.
You know, um, because it takes consistent work, much like medical school. I mean, it's very, very similar to medical school. I think it prepared me very well for those years in residency because. Um, it was grueling, not just physically, but also mentally, you know? So then you get to medical school and it's mostly mental, right?
It's not as much physical, but like, uh, I think it was, it was [00:06:00] the 5:00 AM workouts and the things they put you through that really helped the mental toughness, you know. Um, so yeah, it was really hard. I mean, I'm five, I was five 11, maybe I'm five 10 now. I was listed as six foot, so
Dr. Grant Garcia: I love it. Well, you can see Will though, again, this is the reason, and Chad can remember this, but the athlete checkbox is huge for orthopedic.
There's a reason for that, right? They just don't give up. I did four years. I was not football, but swimming, you know, it's, it's the, it's the commitment, right? Like the one year athlete, like that's great, right? That's, that. You can do that. That's, that's easy to do. That's hard to do in some cases. But the four years, what you did, you know, that shows dedication and it's, it's gonna jump right into the next topic, right?
Because what you did for four years now, you've gotta basically do something and you wanna do something that's different than what people have done before. Like, yeah,
Will Sanchez: the,
Dr. Grant Garcia: this fertilized ACL, and we can get into it in a second. Like, this is bucking [00:07:00] the norm will, like, this is not like, like we've talked about, like ACL repairs, like mm-hmm.
It's the same sort of situation. Like nobody, everyone's against you. Right. You're really, they're really against you and No, and you have to like, kind of be like, am I gonna take this on? Right. I mean, Chad, you had the, you have the weight of. You know, 10,000 or more surgeons that are like, no, this is the way we've done it for years and years and years.
I mean, what was even that that started making you think that you could take this on?
Dr. Chad Lavender: So, um, I think it, I would go back, I would go back a second and say where we're practicing. Okay. Which is in small town West Virginia, and I wasn't a team doctor for XNFL team or. Division One Power Five program, and the patients that came to me trusted me.
And, you know, and, and we would have informed consent and I would say, look, I think this is going to help you. This is what we, you know, we're planning. [00:08:00] Um, this is research and they trusted me and the patients that are in the trial that you're gonna mention, many of those are from this area and they had full trust, uh, in what we were doing, you know?
Um, so it, it's, it's, it's interesting. In the very, very early days, we weren't under the micro microscope like you're discussing, and then really quickly it turned into, okay, I'm on a stage and there's a thousand orthopedic surgeons out here. They're wanting to throw tomatoes at me. I mean, it, I can remember it.
I can, I wa I can remember the first time that I presented just the technique. Okay. Just the technique. And I'm outside and I'm nervous. And, um, you know, because like you said, it's one thing to present in front of people about acls and hamstrings versus quad tendons. It's another to present a completely.
Mind, uh, changing, you know, procedure. And so, uh, I remember [00:09:00] the guy outside, one of the reps, he, uh, came up to me, he said. And he was telling me this story about a mountain biker or an ex games type guy, and he was like, and he said, the worst thing that can happen is I could die. You know? And I was like, why are you telling me that when I'm getting ready to go on stage, man, come on.
And uh, so that kind of lightened my mood. I went up there. I think it's all about putting things in perspective and really, um, you know, I would, and I, and, and I've talked to other innovators, uh, since in the last eight years. And, you know, I would say that. There's really, uh, there's really three different phases.
There's the very difficult early phase where everyone is against the idea. They really don't want to believe or ha don't have open minds. Then they start asking questions and they're inquisitive. Then you get to the phase where people start to adopt the procedure and ask about the procedure, and want to learn about the procedure.
Um, we really got to the third phase [00:10:00] fairly quickly. Um, and I would say, you know, I think our first, our first publication, um, on the procedure was around 2017, 2018. Um, and you know, there's two different parts of the procedure we'll talk about again, but I would say that the internal brace was more controversial than even the biologic portion.
Interesting.
Dr. Grant Garcia: That's, it's funny. 'cause Will, and I think about that, and that's Will's favorite topic, so be careful when you bring up the word internal brain. Internal brain. Will Sanchez: He gets way too excited. I love it. Every
Dr. Grant Garcia: surgery I bring up, he wants to add it. So, uh, but anyhow, the, that's, that's amazing, right?
Because to me, I had, you know, I had six people with ACL tears today in the office, and every one of 'em, I was like, that's internal brace part's not the problem. Like, that's been studied, you know? And so they, and they're, and they're coming in like two of 'em asked for. So to me that you say in the internal brace part was, the hard part at the beginning is super interesting because that's just the difference now with the internet, [00:11:00] right?
Like the last two weeks I've had people with chat, GPT, they came to me, we talked about ai, and they're like, Hey, my surgery, I need to have this. I'm like, came up with that idea. They're like, yeah, it's an internal brace. They wanna have a quad. And I'm like, did you talk to the surgeon? They're like, no, chat.
GBT told me what I needed. I'm like, oh, that's interesting. But anyhow, the fact that that's out there, right? Yeah, it, it's, yeah.
Dr. Chad Lavender: Yeah. So, you know, I can remember in the early days, uh, we were in Naples and I ran into Dr. Pat Smith, who, um, he was doing it with hamstrings and, um, some canine research at the same time that I was using it as part of our fertilized bio, ACL.
Okay. And so we were simultaneously really doing the initial research on the internal brace. And there were so many questions about does it cause synovitis, does it work, does it over constrain the knee? You can talk about all those things. And um, now sitting here eight years later, it's not controversial [00:12:00] anymore, but like when you asked me the question, what was the hardest, uh, part of the selling the procedure or talking about the procedure, I would say I had a lot more questions.
And concerns about the internal brace than using the bone graft in the bone. Interesting.
Dr. Grant Garcia: Well, I, I see that part. I meant more like, I think we'll get into the recovery timeline. Yeah. Uh, but yeah, I mean, selling the biologic idea, at least in my practice, has never been the challenge in terms of like, you know, everyone wants, like we talked about this to recovery shop, we talked about these other things, will, like, everybody wants the best right.
These patients are coming in and they want the best. And so, you know, Chad's got this sort of super innovative new technique, like they're super interested and he is got the trust locally. Like I know I grew up, I grew up where I practice. So I have the same situation. I mean, I see people I went to school with, coached, you name it.
Like those are the patients that are more willing to trust me and try something like this that's different. And I understand that, which is, that's interesting that that background was there for [00:13:00] you. Um, do, do you know what, so can you explain, and I want to go over this eight fertilized ACL in a second.
Can you explain what the importance of dealing with the ACL was? Like, what's the, I can go in nauseam, but obviously you're the one here and you're the expert. Why did you choose the ACL? Like why did you choose ACL reconstruction and why'd you choose something like this? What was the reasoning?
Dr. Chad Lavender: Man, rotator cuffs are a lot more easy for me, uh, in the, or like, I mean, you know, you can do a, a double row rotator cuff and like, I can't tell you how many times I've said, man, I should have developed a new rotator cuff procedure.
It takes 35 minutes, you know, but, um, and, and the, and the ACL all, you know, an autographed ACL takes longer than that. But, um, no, the reason is because in my opinion. When you have a re-rupture of an ACL in a 17-year-old, you're almost, that's almost like athletic, the end of their athletic career in most cases, [00:14:00] because you take an injury that was maybe one year, and now you've made it at least two years long off the field, right?
So in most cases, let's say you get hurt in August, you miss that football season. You come back in the spring, you re-air, you miss a whole nother season. So my goal was, and, and here's how we got started with this process. A patient came in, for example, and did not want a staged reconstruction. Okay? And so you start to think about ways that you can improve the healing process and the bone.
And that's kind of how I came up with the idea of using bone graft in a primary setting. You understand what I mean? So instead of staging, yeah. Instead of staging with bone graft and then going back in, I said, okay, wonder if this would work. And then once I did it, once I started saying, okay, let's just do this in all of our primaries to improve the healing process.
And it made sense to [00:15:00] me.
Dr. Grant Garcia: Yeah. Um,
Dr. Chad Lavender: so Will,
Dr. Grant Garcia: that's to jump in that, that's, we talked about this with Chubb. So basically you get these patients with big tunnels and so you don't want to do another ACL on them. And so what he's saying is that he found this way to try to like, can I bone graft and do the ACL at the same time to skip that step.
Will Sanchez: Yeah, but the inspiration is off the re-rupture, right? So after the re-rupture, that was the inspiration. And then once you caught onto something that you're like, this is working, then that became your primary, uh, for any procedure that had to do with the ACL, not just a re-rupture, but the inspiration to kind of, you know, be motivated about finding a solution, especially for these young adults that are losing two plus years of their athletic career.
Came from this re-rupture, which is, which is fascinating. So it's as, as we talk to other doctors and we hear about inspirations, it is usually that inspiration to help someone to help the patient have a better quality of of life. So I always find that key when I hear [00:16:00] these things and saying, this is what motivated me.
This is what inspired me, was to find a solution. And, and Chuck, can you talk
Dr. Grant Garcia: about the delay? What's the delay? What is the delay in the recovery of ACL? Right? Like you talk about tunnel healing, right? So what's that? That is part of your process as well, I'm assuming.
Dr. Chad Lavender: Yeah, and I think, um, the biggest, the biggest reason I, I chose ACLS is my main, um, interest of, of research and, and innovation.
It was because of my, it goes back again to my, my upbringing and, and you know, having friends that tore their ACL both in high school and college, and seeing what they went through to get back from that surgery. And my thought process was okay. Yeah, the patella tendon may be a, a great autograph. But it are, is there another option that hurts less, possibly long-term, hurts less earlier, and we can get patients back easier and, and, and, and maybe let their recovery be, be easier and, and more thorough.[00:17:00]
You know, that, that was my, that was my whole thought process. Some of those questions we're actively still studying almost a decade later, guys. I mean, and when we get to the study, we can talk about that, but I mean. It is, it's, it's unbelievable how long it takes to find answers. You know? I mean, real, legit answers, not just, we can do this.
I think it works. It works in some people. Right? You know? Does it actually work? And so
Dr. Grant Garcia: can you describe, I know we have this really nice slide here, and I want to get to this and just kind of show this for the viewers, but can you describe your newest tech? 'cause obviously you've done some slight modifications in trying to make the perfect titration.
You don't have to go through too crazy details. People have seen this. I've already talked about the first slide, this is like the fourth time. But obviously the first time having someone like you, the expert that invented it on, can you tell the viewers kind of what you're doing right now, uh, to do a fertilizer seal so they understand the differences?
Yeah, that was because people think they think they do. But
Dr. Chad Lavender: man, that's an excellent point. [00:18:00] Um, that's a really excellent point because early on, the first time that I published it, it was with a patella tendon graft. And I, I, I threaded an internal brace through the interference screw on the tibia. Long story short, I was using a patella tendon graft, then I used, um, amnion, you know, I went through an amnion stage and then I settled on the use of a quad tendon with the composite graft, the bone grafting in the tunnels, and an internal brace right next to the, to the quad tendon.
So I settled on the soft tissue graft. With an internal brace, um, and the composite grafting of both tunnels and that, that period and that process probably took a year or two. And then we started actively looking at our results. And still to this day, um, now I'm looking back at some of the six year data that we have, you know, and, and trying.
[00:19:00] I mean, we had a research meeting this evening before I came on here, and we're actively trying to find. Uh, those that may be interested in looking up those results, call 'em patients still, you know, finding patients, seeing how they're doing. And I mean, it, it's a la it's a labor of intense love. You know, research is, I would say.
Dr. Grant Garcia: So, and then you're adding biologics. So what are you usually adding to this? Because, so for the, for the listeners, you got the bone graft you take, which is, we can learn about that, but
Dr. Chad Lavender: in, in simple terms, what we're adding is, we'll, we start the procedure and we take bone marrow aspiration from their shin bone.
Okay. Okay. That liquid gets spun and you could take, you can use PRP or you could use BMC, which is bone marrow concentrate. That's been, that has, um, stromal cells. Don't really like to use the word stem cells. Okay. So stromal cells. Uh, so it has stromal cells, uh, within that BMC. So that's liquid. And we'll add that to, [00:20:00] uh, a demineralized bone matrix.
That's, that forms a putty. Okay. It's, it's thicker and it, and it forms a really almost solid putty that's a graft. Um, and those two components, um, really form our, our composite graft that we inject into the, into the tunnels. That's kind of how we come up with, with, with the, the slush puppy. Pe People like to call it a slush puppy because it's, it looks like a slush puppy.
Yes.
Dr. Grant Garcia: And it coats the graphs. The idea is it coats the inside the tunnels for the listeners, and there's a gap right now. There's just, there's just nothing's there. It's a, if you, unless you like, have a perfect tight squeeze, which you won't get the ACL through, you have to have a little bit of a gap. So now you're basically accelerating that hopeful healing process.
So let's go to the clinical trial and then maybe, uh, Chad can explain it to us. 'cause this is sort of the big one.
Dr. Chad Lavender: Yeah. So, uh, this, you know, uh, let's go ahead and talk about this. So, 2021 is your date here, and it [00:21:00] didn't fully publish in arthroscopy, the Journal of Arthroscopy until late last year, 2024. So the, and I, and we started before COVID, so we're talking about 2019.
Uh, we started enrolling in this trial or earlier, and the reason is, so you enroll, okay, 60 patients or a hundred patients, you do their surgeries. Then after their surgeries, you have to wait two years to properly publish. It doesn't matter if you're looking at six month CT scans. Two week results, three month hop test.
It's not getting published until two, two years after that last patient. Well,
Dr. Grant Garcia: especially in the journal, you published it, right? Yeah. I mean, you go, you went big.
Dr. Chad Lavender: Yeah, that's that. We went big and, and, and there's always flaws that people will point to in any study, but in our study it was randomized and it was controlled.
It was a [00:22:00] randomized controlled trial. Uh, 60 patients, and we used both autographs and allograft based on age. So it wasn't just a bunch of 18-year-old soccer players, right. We're, we're looking at across all age ranges and made sure that all that was even okay. And, um, half the half the patients received the, uh, augmentation with the internal brace and the biologics. The other half didn't. And what we found is. The half that had the, uh, bio ACL fertilized, ACL, um, had improved function at just 12 weeks, as you see, 80%, uh, they scored 80% on their HOP testing, which is a measure of their function compared to the opposite group, which was around 35%. And many of those patients didn't even perform the HOP testing.
So, yeah, that's pretty
Dr. Grant Garcia: impressive at 12 weeks. That's just not common. Yeah, it's,
Dr. Chad Lavender: no, it's not. And so not, [00:23:00] and the, and the bigger issue is we found that the, um, the tunnel widening was less. Okay. So radiographically the bone incorporation was better and there were no re ruptures in either group. Uh, and several, every single subjective measurement that they filled out.
On their surveys throughout the study favored the group that was augmented. Only a couple were statistically significant, but they all favored the augmentation group. So, um, based on this study, we put our heads together and we said, okay. How do we see if, uh, what's important now? So we did the randomized control trial.
So we said, well, let's look at this in a larger population of athletes and let's look at less than 25 years old. Okay. So currently right now at Marshall, what we're doing is we're doing a 125 patient [00:24:00] prospective earlier return to play study. And what we're doing is looking, we're seeing if that three month hop test.
Is similar. And I think right now, if I pulled it up on my computer, it's 70%, 75, so very similar to that. 80% at three months. Um, we're testing MRIs at six months and we're seeing on average less than or equal to one millimeter widening on the femur in the tibia, which is about exactly what we found. And we're also seeing, um, you know, we're, we're not seeing poor results.
Does that make sense? So not re-rupture those types of things.
Dr. Grant Garcia: This is great. So I, I don't want to cut you off. I wanna make sure that we, you're doing a fantastic job presenting. I wanna make sure the layman people can hear this. Yeah. Because this is, these are the people coming in, like the orthopedic surgeons.
Like we read the fertilizer cell, we get it. Like I, I'm all on board. I love this. So this, the tunnel widening, the CT scan for everybody listening is like, the concern with some of these soft tissue grafts is they have bigger tunnels. That's one issue. The second issue is the, the reason [00:25:00] they can't get back faster is for many reasons, but one of them is because the ACL isn't healed to the wall fast enough.
So that's why people are scared to let people go back at 7, 8, 9, 10 months. So you basically showed that your way is getting the bone heal faster and that they're stronger. So it's like the perfect trifecta, which is why you've shown some crazy videos of some people doing insane things at a much faster rate.
Dr. Chad Lavender: Yeah, those, I
Dr. Grant Garcia: mean, I know you're laughing, but I videos, those didn't go over well. Those
Dr. Chad Lavender: didn't go over very well in the orthopedic community. I'm sure it
Dr. Grant Garcia: didn't. I'm sure it didn't, but I loved it. So, I mean, I remember seeing the first one like three years ago. I was like, is this real? So it's pretty awesome.
Dr. Chad Lavender: I talked to somebody today, um, I don't know, they were maybe six or eight weeks, and I said, uh, so, so they were asking about an activity and I was like, listen, if. If you do that, just don't tell me about it. You know what I mean? So I was like, no.
Dr. Grant Garcia: I think the idea is that you're this, it's, you feel a lot more confident with, you know, I have those patients come in there six months, they're like, I'm still nervous.
And you're like, no, listen, I know that [00:26:00] this is stronger. I've done the tests on this. Right. Like, just so the listeners know, you don't normally get a CT scan. You don't normally get an MRI at six months, right? No, that's a study based thing. So you're doing every check right. Right. A JSM is going to be like, I don't trust this thing.
It's totally out here and we need to make sure, like this was literally sealed, tight study. So they did everything possible, like anything negative that someone can think about. You already covered it. And so that's really important for the listeners.
Dr. Chad Lavender: So we did cts and MRIs in our previous trial when we compared the groups.
This trial, we're doing six months MRIs, and the reason is. We can, you know, it's less radiation on 125 patients. So
Will Sanchez: yes,
Dr. Chad Lavender: that would've been hard to get through the I rrb. So, uh, the MRIs can still tell us the, the tunnel widening, which, you know, it's like, uh, like I said, less than one millimeter at six months in both groups right now, and I think we're up to 70 patients.
Wow. Um, so the other thing that we're finding and we're looking at is I have an independent radiologist that's [00:27:00] looking at the signal of the ACL graft. So I'm trying to, so some of what we do in research and what we're doing with this study, um, we're also doing hop testing at three months, four and a half months and six months, and I'm doing virtual reality testing.
So I hook 'em up to a, I have somebody that, that's their whole job is they take our ACL patients and they put sensors on them and they do dors CV testing and they do virtual reality testing.
Um, on a, on a screen, like a PlayStation move, you know, it's not that. Yep. But it's simple. And then that gives them limb symmetry, indices and things of that nature that we'll be able to go, hopefully, four years from now and say, okay, the patients that had issues.
Or re ruptures or didn't do what, you know, when you look at their RSI scores and, and all these things, we'll, we'll go to try to correlate that with all that data that we're getting. So, you know, we're trying to get a treasure [00:28:00] trove, uh, if you will, of data not, and like I said, maybe we'll find that. You know, um, the, the signal to noise ratio on an MRI of the ACL graft after, after this is improved and that helps, helps you with your re rupture rate.
I don't know, but like, you're right, we, we wanna look at every detail that we can and not just, not just say, well these patients scored better on a subjective measurement. Yeah.
Dr. Grant Garcia: And, and, and it matters too, right? Like the data's good, but you wanna make sure you have everything covered, right? Like, 'cause patients don't really know what the.
Your, their IKD score means or anything else. They're like, oh, that's great. They want to know, am I gonna be stronger, faster? Am I gonna get back longer and is there higher? Am I gonna rupture sooner if I go back earlier? 'cause right. The whole debt, the whole thing we've ever been taught is that the sooner you go back, the sooner you re rupture.
Right. You go back before six months, you know, there's a concern. Not in this case, but you know what I mean, like there's been data about that. Yeah. So that's a concern. Which is why we never let people rip until [00:29:00] seven, eight months until we've had new data. I know you're, I know you're laughing about it, but it's a big deal.
I mean, that's patients. Well, I,
Dr. Chad Lavender: I, I'll tell you a story. Um, so Dr. Tim Hewitt, who is a world expert in biomechanics after ACL uh, reconstruction, he's the one that wrote all of the data that we have on preventative techniques for ACL, you know, uh, for female athletes and things. So, um, a, a mutual acquaintance of ours, uh, we're at a conference we didn't know each other.
Um, he had just written a paper that said, you need to wait two years to get back after an ACL or else. Right? And so, uh, oh, this is gonna go well. Yeah. So they, they set us down to the lunch at a, it was at a, it was at a meeting in Nashville. And so we sat down and, um, we started talking, we're across from each other, and, and he.
He's hammering me about the technique and my thought process and, you know, and I'm listening to [00:30:00] him and his, his views on things, which he makes sense and he has data behind. And, um, and he's a, he's a world class researcher. So rather than us getting into an argument, we end up realizing that, hey, the only way to really figure this out is to work together.
So he comes to Marshall. Now we're working together on this research study, and he's studying the biomechanics. I'm studying, you know, I'm doing the surgeries and the clinical scores and the MRIs, and we're putting our heads together to find out if six, and we're letting patients go back at six months.
And then we're gonna say, Hey, is it smart or not? You know, and, and let's figure this out, is if they did, if they went back at six months, what was their re-rupture rate? And what's that compared to in other studies and, um, will show
Dr. Grant Garcia: that comparison up there.
Dr. Chad Lavender: Yeah.
Dr. Grant Garcia: So Chad, I mean, this is amazing, right? Will he found the highest critic possible?[00:31:00]
For his study and decided to make him his colleague.
Will Sanchez: Like
Dr. Grant Garcia: that's insanity. Yeah. I love it. Like if your study works, I am all in. I already believe in this, but like you did the worst possible research thing ever and you found your biggest critic to do the work
Will Sanchez: for you.
Dr. Grant Garcia: So like this is incredible. Like listeners, like there is, you cannot fight this man.
Like he has done everything possible to try to destroy what he's doing and he is still not doing it. So this is fantastic.
Dr. Chad Lavender: I think you, you don't want to, uh, no matter what you're doing, you know, you don't wanna surround yourself with, uh, yes people. Mm-hmm. You want people in the room that are gonna question everything you do, because if I get on a show like this, or if I get up on a podium.
I want to have already answered those questions that you're gonna ask me. I mean, it just makes sense, right? So, so he was able to come in and really look at, look at, help us design this, this, this study that we're doing now, which is, it's, it's called a early return to place study after, after fertilized ACL.[00:32:00]
And, uh, yeah, we're doing 125 patients. We're gonna follow 'em for, um, two years and then five years and, and, and all that. So.
Dr. Grant Garcia: We'll pull that back up. Don't go away from that slide. I need him to look at that. I like this so everyone thinks this is good 'cause Chad's getting the heat here, but I'm about to get the heat in like a co like a month when this, when this, uh, publishes and I'm gonna get the heat in terms of like my own patients asking about this.
So it's important that I show them all this stuff because they're gonna want to know it. Like this podcast can be listened to. And I'm gonna hear you're on your podcast, you said this and so it's important like right Chad. Chad has his own thing. He's invented this fertilized ACL, but there's hundreds of thousands of doctors that are doing this, and they're gonna see this and they're gonna say, Hey, listen, tell me more about this.
I want to know about this six month recovery. We're looking at it, the limb symmetry, the tunnel widening, but this comparison's really important and people come to that. So again, six month is not crazy, right? We have our own patients that are non traditional acls that are six months, seven months. So this is not insane.
And [00:33:00] again, I think. Part of this is what your technique is and part of it's probably you feel comfortable at 12 weeks with them doing the strengthening the limb symmetry, right? Yes. I would imagine it's kind of a combination of everything.
Dr. Chad Lavender: Let me explain our thought process there for a second. Yes. Um, so when we went into the design process of the study and I talked to Dr.
Hewitt, we were going to do like several different arms of the study and have some patients able, if they pass testing that to go back at four and a half months. I go to a couple conferences and I realize that, hey, people are still up there on stage talking about nine months, and I come back, I talk to him, I said, listen, let's just, I've let every patient for 10 years go back at six months.
Let's just show that that's safe. Let's get an actual re-rupture rate at six. Work your way down six months with the internal brace and the biologics, and let's prove that part of it before we go crazy. Try to and try to reinvent the whole rehab [00:34:00] process. You, you see, I think that's why, that's how we fell on a, on a six month timeframe.
And the other thing I wanna point out if I can, is people and surgeons and patients sometimes take grains of what's out there and they say, oh. I'm going to get back like within six weeks or 12 weeks because these patients did well at 12 weeks. That's not what we're promoting, that's not what we've shown.
Yeah, we're showing improved results at 12 weeks, but in, in no case have I signed a letter of release at 12 weeks. Okay. So I think that's, that's important to point out. I wait until the six months, even if they pass their, their hop testing and, and, and are doing excellent, I wait until six months. So,
Dr. Grant Garcia: and, and it's
Dr. Chad Lavender: important too
Dr. Grant Garcia: that you're saying that, right?
Because they all take this and they're like, well, that was me, but I'm not average. Right? Right. I'm better than average. And so I'm a four monther. And what you're saying too is the shock factor, right? Like the [00:35:00] video I had seen showed the four and a half months insane response. Yes. And so, like you said, like even someone like myself that's all on board with this, I work with Arthrex, I do the biologics, I'm all into the innovative stuff.
And I'm looking at this like, holy cow. Right? Like, it's not someone who's been indoctrinated for 20 years into the exact same surgery. Right. It's a, it's a shock. Yeah. So the six months, to me, I'm like, I can handle that. Like, I can easily tell my patients three more months. Yeah. I'm gonna cut your time in half.
That sounds insane. Like, that's the other thing too, is that it almost seems like too good of a, I hate to say the word sales pitch, but you know, locally, right? But you've got patients flying in for the surgery right now, and so the idea is that like. You wanna be careful with your pitch too, because you are selling it, you're still selling the procedure, uh, to the patients.
So it making sure that it's sort of like the appropriate expectations. Uh, but this is awesome. I, I think it's really important that we brought that up.
Dr. Chad Lavender: So thank you, Chad. I really appreciate it. I, I do think there's, we have a, um, important aspect, uh, protection for our patients, you know, I mean, and, and [00:36:00] because sometimes, and, and a lot of times patients will call from, you know, I mean, we've had patients come from other countries.
To, to this small town in West Virginia. And I know they get here and they're like, what in the world is this the right idea? You know? Um, so, and they, and sometimes they get lost to follow up. I mean, you know, as much as we try to call. But anyways, um, I'll tell you that, um, that it's very important, uh, to make sure you carefully word what you're saying.
Especially in promotional activities. I've learned a lot about that. I mean, and we still do let patient, like any videos that you see me repost, generally are posted by the patient. Okay. So I don't really do a lot of posting of the videos anymore. Like most of our videos are patient driven. Post because they're excited about their rehab.
And you know, I, and I, and I, and we wanna support that, but we don't let them go out and play at, at three months. And, and I think that was the, that was a [00:37:00] big misconception, um, that we were rushing people out there. Um, and that was, you know, let's, let's talk about that for a second. 'cause that was frustrating to me.
Okay. That's important. This is good. Yeah, because, because we were putting so much work into. The design of the technique, the design of the research. And following up on patients and, and really closely mo, I mean, I literally at, at times have sent people to high schools to make sure we get data on patients that were lost to follow up at certain time points.
That's how, I mean, that's how much we're, how passionate we are to get the research data, you know? Yeah. And so it's frustrating when people would come back and say, you're out here telling people they're going to just, you're rushing 'em back to activity. And, and that's just not, that's not true. That's a false narrative, um, entirely.
Did you hear that more from your peers? More than anybody else? Not so much people. Yeah. Oh, yeah. I mean, because head mouthing, because what happens, I dunno if
Dr. Grant Garcia: I call the [00:38:00] peers, but they, yeah. I mean, what
Dr. Chad Lavender: happens is somebody goes into his office and they say, yeah, well, Dr. Lavender over there at Marshall is letting people go back at three, three months.
That's just not true. And so when they call us, you know, and, and they get to me and, and what, and our, we have a protocol we do with out-of-state patients. Um, yeah. When they, when I do finally talk to them, I spend 20 minutes or more talking to them about expectations.
Will Sanchez: Mm-hmm.
Dr. Chad Lavender: Don't come here for surgery if you think.
You're going to be released at three months. That's not okay. And it happens this time of year every year because they, the football players want to get back before football season. Yeah. It's just not gonna happen. Okay. Now, maybe the end of the season, maybe if they're a high level player and they play in December or January or whatever, that's different.
But like, um, it's just not gonna happen in three months. And so, um, very, very, I make sure that I'm very clear with them about expectation. And, you know, come [00:39:00] here if you, if you believe in the procedure, if you believe in the science, or you know, if you, if you trust us. But, but don't have that expectation that you're just going to be, um, progressed at a rapid pace, uh, on purpose and, uh, you know.
Yeah, and, and you know, I mean, I, every night it seems like I'm texting with patients about their rehab and things like that from out of town, and I mean, I think that's a very important part of the process is making sure they have an understanding at each stage what they're allowed or not allowed to do.
Will Sanchez: It sounds like you've had a, a lot of support, um, from Marshall. What, what, what has that that experience been for, for you and, uh, and, and for your peers there? Um, just kind of working at the facility, embracing the fact that you're, you're doing something that's cutting edge and embracing all that. What, what has that experience been and how has that helped, uh, you know, to get you where you're at now?
Dr. Chad Lavender: Um, really it's the hospital system and, uh, and Marshall [00:40:00] both, you know, I can't say enough about some of the residents that have been involved with me. Um, I mean, we've had residents that have won awards and, um, really put in, you know, that study that got published. For example, I'm gonna say his name, Andy Shaver, uh, Dr.
Shaver. He put in at least 50 hours of work after this, after the study got. Really not denied, but you know, the re like accepted with revisions kind of stage. I mean, yeah, it was, it was a ton of work on his part. And without people like that in your life and, and in your workplace and supporting you, man, you can't do this.
You know? I mean, it took me, I mean, we got the book finished in maybe six months, but it was every morning I was up, you know, five 30 or six because. They're in a different country doing their revision. So they would send it to me late at night and then I'm up doing it before I go to work. It was, that was the thing that was [00:41:00] different than a study, because you write a study once you write that book chapter, it seemed like over and over and over, you know, there was always a different edit.
But, um, but yeah, back to your point, you know, Marshall's been great and I think, um, you know, I, I, I'll say this, as you go through your career, it's very difficult because. You know, um, you, you exponentially grow in volume and it's very difficult to continue to grow with that volume. You know, there's days, uh, we'll go to clinic and see 90 people, 80 people, and um, and have patients from, you know, have telehealth and all this stuff, you know, and, um, and it's very, you have to add staff and, and kind of grow with that.
And, uh, Marshall's been great about. Uh, supporting this in all aspects, you know? Yeah. And, uh, it's really cool to look back on where we came from and, you know, and, and the area we're in. Uh, if you've never been here, you should come and, and see how small of an area it is, you know? I mean, it's really [00:42:00] remarkable that it, that somewhere like this, um, people come to, you know, but That's amazing.
That's awesome.
Dr. Grant Garcia: Well, I think, I think that, that, this is a, it's a perfect segue, but also. For all listeners, we've talked about this, what does it take, right? Like this is not like a guy woke up, orthopedic surgeon. He came up with the idea. He started doing this on people, and now like a week later he is got results.
This is hours and hours and hours of grind. This is years of discussion, and this is also understanding that like innovation's not easy. Like there's nothing easy about what you had to do. And the heat that you had to take and like, it's all great. Now we can talk about this, like we got pictures from ai.
I got patients coming asking about the fertilized acl. Mm-hmm. Who are in Seattle who have seen your stuff, right? Like this, you've had, there's a lot of work to get here. Now you're at the top and you've done it and it's really awesome and I'm, and I, I would just say it's extremely impressive. But thank you for sharing your story.
'cause I think people need to hear this. 'cause again, this is the most important part. What's the background, right? The sexy stuff's great. Like at the end you got the [00:43:00] marketing. You got arthrex backing you. Like all those things are amazing, but that is not it. It is not easy.
Dr. Chad Lavender: Right. And you did it. I'd like to say something about that because you, that that's a, that's probably the most excellent point that anybody could ever make is research is hard.
And when I got, when I got started with that study, as we mentioned six years ago, I was 38 years old. And, uh, you know, I'm like a young guy then. And that thing got, finally gets published, I mean, a half a decade. And so they're like, well, what are you gonna do now? And I said, I don't know, probably my last study.
I'm just gonna be honest. You know, it takes, if it takes almost a decade to do a do that, I'll say too, I wanna point out that, um. One interesting thing that you learned. So, you know, our re-rupture rate right now has been about 3% compared to [00:44:00] 10% that we've seen. Um, so we have 3% re-rupture, over 10% contralateral tears in our patient population.
Yeah. Okay. We haven't, we haven't changed contralateral tears, which in my opinion points to two things, the validity of our research, but also the fact. That contralateral tears are a separate subset and unrelated to how well the ACL is on, on that knee. You know, I th I th I think, I, I think, I think it proves the patients are getting back to a high level of sport and therefore they're, they're, they have, uh, a high level of contralateral tears.
The other thing I wanted to point out is we found, uh, I think it was nine to 10% of a re. Um, of a, of a, of a, of a need for necessary of a need for a manipulation and or release in our study. And, and it wasn't different between the two groups. That's important. And [00:45:00] so, you know what I did? I said, Hmm, what, what is different about my out-of-state patients? Because my out-of-state patients, man, they came in here and, and, and they're here for two weeks. And they come in inevitably at two weeks, and they've got 120 degrees of motion. They've got quadras, they're walking. I mean, the one guy, you know, that went viral with a TikTok who was walking without crutches, like literally the same day of surgery.
And I said, what's, what's different about this patient population? Well, you could, you could, you can say several things. One of which is they're here solely focused. On their ACL and they've made a major commitment financially and timewise to come here to have it a hundred percent so that that's a separate population of folks.
Or you could say they just want, they knew that I wouldn't let 'em outta West Virginia until they get their,
Dr. Grant Garcia: I, I don't know. I think, I think both points of, but I would tell you my out state patients in [00:46:00] general have some of the most incredible results. Yes. 'cause it's like. I, it, I kind of, I hate saying the word outta state, like professional athlete, but they're like, they got all the time in the world.
Like they're like, I'm taking off two weeks. I'm flying out there. I don't care what happened. I'm gonna make this look good. And you know, the TikTok guy probably had a lot of motivation for it to look good. He is now exploded on there. He's like, I gotta show on my knee. Right? Like, they're more in, they're, the social media aspect of it is also, and I
Dr. Chad Lavender: think so, so what the point I was gonna make is, so, um, what I started doing is I said, well, maybe my local patients.
Are not going through therapy, uh, as frequent, okay? Mm-hmm. So I went old school and, and got as many CPM machines as I could possibly get, and we leased these to the patients now. And so we retrospectively looked, and I haven't published this, if anybody out there wants to publish it, a medical student or whatever.
Call me, call, you know, I, I don't have time reference Spark stock talks. They know you gave me here. I don't have time to [00:47:00] write up every paper. But, but, uh, anyways, what we found was, you know, that 10% went down to, I think two out of the last a hundred patients. Wow. Yeah. And so you could make a case, you know, the reason CPMs went away is they didn't make long-term differences.
Remember we talked about two year dates. Yeah. But man, for an athlete getting that motion back and not having to have a manipulation. Is everything. And that 10%, um, manipulation need is very similar to I think, nees data a after quads, you know, with, with his, uh, I think he presented, uh, it was like seven or 8%.
So I think that's pretty, it's the
Dr. Grant Garcia: most common surgery I do for acls. Yeah. It's the most common second surgery by far. Right. Like this week, last couple weeks I spent half the patients are mine and half somebody else's. Yeah. From an ACL surgery. So it, it, it's. It's no doubt a problem. It's funny, my complex knees, my meniscus transplants, hts, they don't get stiff 'cause I give 'em CCP M right away.
Cole and I, I learned that at Rush, like I'm [00:48:00] super aggressive with the cpm so my bigger surgeries actually get s Ahe less than my acls. Yeah, it's 'cause of what you're saying. I'm like, oh, CPMs old school. Right. And that's not the case.
Dr. Chad Lavender: You were talking about secondary procedures. I wanted to go ahead and tell you I've had about four patients, two of which of which I think were in our trial.
Um, that. I had secondary meniscus tears. Okay. Late, like a year or two out after they played a season and they had major knee injuries tear their meniscus and I go in and they tore their internal brace. And the ACL looks great. Yes. I just had one of, had one of these. See, so it's, we weren't crazy eight years ago, you know what I mean?
Dr. Grant Garcia: I literally just had one two weeks ago, meniscus tear, internal brace tour. Somehow I forgot to hit the video button 'cause I wanted to show that off on social media. 'cause I was like, this is crazy. It's, I've seen it before, but this was like very obvious. ACL perfect quad, just like you're talking about like.
I wish it was a [00:49:00] fertilized ACL that would've been sicker, but it wasn't. But anyhow, it was, uh, it was pretty cool. Uh, Chad, I want to do your last part 'cause if I don't, we have to get off at an hour. 'cause that social media is not like over an hour. Gotcha. So we got 10 minutes to talk about Nano and if I keep going we could talk to you for like two minutes.
No, we got like
Will Sanchez: five minutes. 'cause we, we need to little football. So can we just, we gotta talk to Chad. We're not interrupt,
Dr. Grant Garcia: we're not trying to cut you off. You're just an amazing guest. But can we talk about the nano really quick for you? Because I know you wanted to bring that up. Yes,
Dr. Chad Lavender: here's the nano needle.
This is live, and, uh, that's what it is. So you might want to go to the slides you have, um, and we can talk about it real quick. Show us. So, yeah, explain
Dr. Grant Garcia: to the patients what's the difference, like why do nano,
Dr. Chad Lavender: okay, so the nano needle is much, I think I sent a slide over, but the nano needle is much smaller.
There you go. It's 2.4 millimeters versus 5.9, or slightly smaller than on a regular sheath. Uh, so you're, you're, you can do it through a really, a needle stick. Um, [00:50:00] really with, it's, it's so much less invasive. You're push pushing less fluid into the joint. Um, and um, you know, I was an early adopter to this back when it was called the nano scope, which was way, you know, it is bulkier now, it's just a needle scope.
They're also getting ready to release hopefully soon. Uh, the Nano Needle 2.0 show that Will, is going to improve resolution greatly. I've had the chance to look at these in the lab. So the old nano I've, I've got video comparing the old nano to the new nano to a regular scope and the new nano that's coming out.
Is very, it's very, very close. It's HD and it's close to a standard scope, and you're just using a needle. And so it's remarkably, uh, more vivid and gives you that great visualization that you need. Um, and so what we're gonna be able to do with that is you're gonna be able to do, um, uh, secondary viewing.
[00:51:00] Like I wrote about this in the book years ago because I knew this was where this was headed. You can park that in a joint, say the shoulder, and it'll give you, and now with the new software, you'll be able to put picture and picture or side by side views and have a standard scope view with a nano needle or multiple nanos, and be able to work almost hands free.
Right. And so that's where I think it's going. Um, but I, I think the nano is, is outstanding. Um, also, so we just finished a randomized control trial with the nano, uh, multicenter showing that it had, uh, 56% less narcotic use in the first 24 hours. Wow. That's huge, right? That's huge. That's huge. This was just for standard neco, partial meniscectomies.
Um, Dr. Arar, uh, who was in Washington, DC was the other site, and we randomized patients. I think we had 70 or 80 patients in that trial. We'll be publishing that. Um, sooner rather than later. I'm not waiting for [00:52:00] two years on that one because we're just gonna, you don't need to. No, it's two, it because two, the two and six week scores were better.
And so that's all we're looking for, right? So I don't, I'm not waiting two years. So we'll get that out there. But, um, we also did a retrospective review and showed the same. So I can tell you with certainty that the nano. Uh, it gives you very similar to better scores and less pain, you know, less narcotic use.
Yeah. Which I think we're all trying to decrease the amount of narcotic need after any surgery. Right. So I think that, that, that has long lasting, that's why I wanted to bring that up. 'cause I think the nano has long lasting ramifications.
Dr. Grant Garcia: Well, and the thought process will always asking what's next, right?
Mm-hmm. Smaller scopes. Tighter spaces and multiple views, right? Like what's gonna make me more? So you have the nano scope, right? Newer technology, maybe a little higher cost with newer technology, but like it comes at a price, right? Faster or time? Can you get two? Two. So you're not having someone [00:53:00] hold the scope, moving around.
You're trying to play the game like sideways, upside down. What are they looking? Right now you've got multiple views and can you do your surgery more efficiently? Right. You said a 35 minute rotator cuff. Can you do it in 20 'cause you're not spending so much time transferring portals.
Dr. Chad Lavender: Yeah. And safer. So I'll put it in the back of the knee when I'm doing a PCL.
Yes,
Dr. Grant Garcia: this is
Will Sanchez: huge.
Dr. Chad Lavender: It's direct visualization so I can tell a patient I'm gonna be watching while we're drilling your tunnel right next to the vessel. You know, I mean, so we have, we put all those techniques in the book years ago, and now I think people are actually gonna start adopting them when the, when the visualization becomes hd, you know?
But, uh, but. Yeah, it's been fun, man. You know, I, uh, I've had a lot of fun doing these innovative techniques and learning. Um, and I, I will say to any younger surgeons out there, um, or residents, uh, research makes you learn and question more each day. You know, you, you find [00:54:00] answers. But for every answer you find, it seems like you asked 10 more questions.
So
Dr. Grant Garcia: Well, and I would also say what's interesting is you, you know, you went from a small town team, doctor, now Marshall, people are flying in for your surgery. Right? You've, you've now had this sort of fame of your innovation and that adds another layer too, right? You did all this work and all of a sudden now you get on a podium for Arthrex or for some other company, and you're, and you're up there and you're talking.
Now you got a thousand surgeons and you know, the first time you're bringing this up, it's no joke, right? It's not, it's no longer you're just in this small little facility or small area talking like this. People are listening, right? You know, you're on this podcast, you're on other podcasts. Like you, you've got a presence, so you've also gotta back it up too.
You've had a lot of, like, a lot of P practice.
Dr. Chad Lavender: It's been a lot of fun. You know, I can remember when we had, uh, we had an article one day. Um, you know, life has a way of just completely, I, I will say this, completely humbling you. But, um, you know, uh, we [00:55:00] had, I can remember one day the, the sporting news article hit and I thought, I knew it was coming out sometime soon and, and, you know, and I thought, man, this is gonna be awesome.
And then it hits and like. My day was the same as every other day of my life. You know what I mean? And it was just like, okay, onto the next day. You know, what's the next, what's the next? But, but it's taken us all over the country. I mean, I've been all over the country doing, um, education and, and talks and, and really have, I've met some fascinating people across this country.
Um, surgeons, patients, um, and really talented individuals across all, like from, from all walks of life. You know, you just, it's, it's, it's really remarkable. And, um, so yeah, I think, I think that there's that small town appeal of the story. Uh, but, you know, um, it's been a lot of fun and I think, um, you know, I will always say, you know, Keith, the main thing, the main thing, and that's, that's patient care, and [00:56:00] that's, that's what we, that's what we're trying to improve the patient experience and their outcome.
Dr. Grant Garcia: hundred percent. Well, Chad, this has been awesome. I know Will has some will. You're, you're, no, we're just gonna wrap it up. You're ready to go? You have a few minutes.
Will only,
Will Sanchez: no, no. We're just gonna wrap it up. Um, uh, once again, uh, Dr. Lavender, thank you for, uh, taking so much time. I know you're excited you brought back Coach, uh, rich Rodriguez, are you excited about your mountaineer?
Dr. Chad Lavender: We got a
Will Sanchez: Woo,
Dr. Chad Lavender: really excited there. What's going on with that? I play, I played for, um, I played for Rich Rod. Yeah. And then also Marshall's new coach, Tony Gibson was on that staff. So both coaches in state, you know, I played for at WU and I was down. My son, he's like a, he's nine. And um, he was down at Gibson's camp and I got to talk to him and I was saying, man, life comes full circle, you know, that's great.
I mean, here you are here. And uh, but what was funny is he called, he told me, he said. I never dreamed my first day [00:57:00] here, uh, at Marshall. I get called about somebody wanting to get in to see you for an ACL.
Dr. Grant Garcia: So
Dr. Chad Lavender: he,
Dr. Grant Garcia: he told me
Dr. Chad Lavender: that story, dude, you're,
Dr. Grant Garcia: you're doing the hometown of awesomeness. That is so fun.
Will Sanchez: That, that is great, man. We, we, we we're getting excited about that football season here. Yeah. We're excited,
Dr. Chad Lavender: we're excited at Marshall and WVU, you know, with two new coaches, so we're excited with both of 'em. So, uh, you, you got your tickets, you're gonna go, uh
Will Sanchez: oh. Yeah. Okay. I knew that. I knew that Dr.
Lavender, thank you so much for your time. We really appreciate it. This was absolutely wonderful. I, I felt like we have so many other things to, to chat about and I mean, we can go on and on.
The good, the good guests
Dr. Grant Garcia: like you, we could go forever. This is like, we're gonna have to have like a 24 hour show sometime at this.
Great. I, these guys are so fun.
Dr. Chad Lavender: And uh, you know, I think the great thing is, I don't know how many years ago we were on together, but, um. We have a lot more to talk about this time. So, you know, that's, that's a good thing, right, guys? Always, always. It is a good
Dr. Grant Garcia: thing. You're doing good work. So thank you, Chad.
I really appreciate it.
Will Sanchez: Thank you [00:58:00] guys. Dr. Chad Lavender. Thank you so much. Thank you for your time, Dr. Garcia. Say goodbye. Bye-bye. Thank you. Bye.
Audio Transcript
Grigor Dimitrov’s Wimbledon Exit – The Pec Tear That Ended His 2025 Run
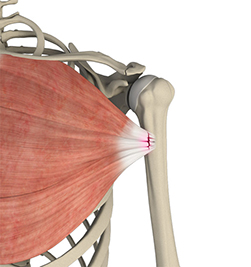
Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon and sports medicine specialist,
Dr. Grant Garcia:, you, you see how that just kind of flows outta my mouth at this point? Dude, you're getting better each time. You are our specialist and top doctor, but enough with the accolades 'cause you don't need any more hyped up.
Uh, we've got a great show. We have a topic that, um, it's really concerning, really interesting. So I'm really looking forward to, uh, discussing it. But before we do all of that, we're talking about injuries. That means that we need to talk about the recovery shop. Let's give a shout out to Mike B and tell everybody why you love the recovery shop.
Dr. Grant Garcia:: Well, big thanks to our sponsors. They've been our sponsors for a long time now, man, it's been at least [00:01:00] a year or more. Uh, no, we've been, yeah, I appreciate it. So, any else? So the idea is if you're a surgeon, you're taking care of the injuries we're gonna talk about today, right? These patients get a lot of swelling afterwards.
They ask for, what else can I do? It's not just the standard medicines you can give them, there's other options for them. Supplements, nice machines, more advanced recovery systems. And so we have those there at the recovery shop. And as a surgeon, you can have your own specified section, which is really pretty cool.
'cause you know, patients can use it for non-surgical injuries, surgical injuries, whatever they want. It all kind of comes in one package and the nice thing gets vetted by the surgeons. You can vet, we own products with them on things that are, you know, DME approved, et cetera. So it's pretty awesome. So reach out to Mike b.
I've been super happy with it. I have patients all the time calling me, even non-patients, asking, Hey, can I get something your got? I'm? Yeah, no.
Will Sanchez: The reason we wanted to do the show, um, was because of this injury and I was watching the Match Live and we're talking about Gregor [00:02:00] Demerol's, uh, Wimbledon exit, uh, as he was up two games or two sets.
To none on the number one player on of the world, Yannick Sinner, which eventually won Wimbledon. And he was cruising along and I'm watching it and I'm like, man, he's, he's gonna beat this. I think he was, I think they were tied two, two in the third set and playing so well. Um, it, it was absolutely incredible.
And then you see a serve and he kind of grabs his pec a little bit. And then when he goes to serve again, which was an ace. He collapses to the floor. Um, first off, did you see the injury live or did you just go back to the video? You know, as we just decided to discuss exactly what had happened, what's your, your take on this, this?
So
Dr. Grant Garcia:: I didn't see it live. Uh, yeah, probably working, who knows what I was doing, but the, but nonetheless, the, that next day in the operating room, my tech was coming up to [00:03:00] me and my PA was like, Hey man, did you see what happened? It was crazy. It's really unusual for tennis and again. We hear about it in some of football players, right?
But to see it, you know, happen on real time and a tennis player is very unusual.
Will Sanchez: Yeah, there's picture there. If you're watching, uh, on YouTube, he is reaching for that right pec, and when I first saw it, I thought it was just some kind of like, yeah, maybe a muscle injury, a pull. You know, they're, they're, they're swinging so hard, right?
You look at 135 miles an hour, 118, you know, return serves at, you know, 87 miles per hour. Every swing, forehand, backhand, just, you know, it's, it's at the highest level, right? We're talking about the best athletes in the world. Why don't we talk a little bit about what this injury is and how it will affect, uh, g Gregor going forward?
Dr. Grant Garcia:: Yeah. [00:04:00] So why don't you pull up the slide. Uh, you wanna put that slide, that one Perfect. Yeah. Pull that slide up. So, uh, he had a pec tendon tear and I know we put downward partials 'cause you know, they're not always fully torn off, but you have a lot of issues with the lower part of the pec. You can see right there.
So there the peck has two heads. There's a particular head and the sternal head. Um, and sometimes you can get a partial tear and a lot of times the challenge here is as soon as it's hard to see exactly what type of tear they had. But a lot of times it's from, you know, getting caught on a tree. I've had caught on a tree.
You've had wrestlers, you have bodybuilders, you have football players. A lot less common in throwing sports and tennis. This is actually one of the first professional athletes I've seen with a pec tear that was a tennis player. So it's quite unusual, but that massive force caulking back. Basically what that tendon does is it gives you that nice cont where we all know about, you know, pecs Yeah.
And pec flex. Um, but it usually pops off of where the humerus is, so there's a little tendon. The misnomer though is that it's apec tendon tear. 'cause usually the tendon is so [00:05:00] thin and the tendon's so short that you pretty much never have tendon left on it. It's very unusual. It's usually something we call a myo tenus junction tear, where it tears where the muscle and the tendon connect together.
What's interesting though, as you guys see on the picture there, on the top right, that's the muscle, but underneath that is something called a fascia. So you've probably seen, like when you're cutting meat, you have got that thin white stuff in between. That's kind of hard and tough.
Will Sanchez: Yep.
Dr. Grant Garcia:: When you're cutting the steak, that's exactly what that is.
So that fascia that gets ripped off, it's a lot harder to fix, but that's the ones we want to have. Get the, get the fascia on there, plus the tendon and that pec, but it's such a big muscle, it balls up and you can really see a lot of deformity. So he was clutching the area that he tore it on. Um, the problem is sometimes it depends on what type of tear you have.
Now, his was something, you know, he had surgery. Like be successful. Obviously the tear that was repairable. Sometimes though you can tear it in the middle of the muscle and those are not fixable, but it's a different look. So it's a little bit tricky 'cause these are kind of hard to see on MR mri. Like no matter how much people say they look at these [00:06:00] MRIs, they know exactly what they're looking at.
These MRIs are a little challenging to read compared to my, you know, rotator cuff tears, shoulder dislocations, acls, you name it. Uh, they can be more challenging. And obviously this is a time dependent thing, which we can get into in a second.
Will Sanchez: Yeah. Yeah. Um, so I, I wanna go back to what you said. You said if it's in the middle, it's unrepairable.
Why can you explain that? Because, you know, that was Yeah. So the key that you mentioned there.
Dr. Grant Garcia:: Yeah. So it can attach to the humerus, which is around the biceps area, and that's where there's tendon attached. It attach it to the chest wall on the inside, right? That's when people have their pecs. They, you can see it flexes all the way to the middle of their sternum, and so if it tears off there, the good news about those is they usually heal a lot faster and they usually get the contra back.
The problem is if they tear the other one. That's where the power comes from with this muscle. 'cause the muscle is so big like this. Yeah. And then it weaves down into some tiny little bit of a tendon and the muscle attachment. So that's usually the weaker point. And that's the, the, [00:07:00] the way it happens is usually the last four to five inches of the bench press, that's almost always where it happens.
Or an abrupt check, or from what he had is that tennis serve. But these linemen that have gotten, you know, we talking about JJ Watt shortly, but they get caught and then it pulls back. And it pops a tendon. The challenging part here is that, you know, if you don't do a lot of these, I've been in surgeries before when even in training with some good guys that they were, it was challenging to fix sometimes because it gets really distorted in there.
It's not the same as like a biceps tendon. Where it pulls off, you can see the muscle. The te the muscle is like a three dimensional, it's like a u, it's like a circle and it, it folds on itself. So you have to understand the anatomy a little more when you fix these. Plus it's such a powerful muscle, and the time is dependent, right?
Like we can fix bicep tendon tears up three months, but you get past. Six weeks, five weeks, you have to reconstruct this, which is a big problem, right? Like it's not, they just don't do as well if you have to reconstruct it. They, they [00:08:00] have good results, but it's just not the same as if we have a fresh pec tendon repair.
Uh, back to the bone. Right. Anything's always better when it's your own natural anatomy.
Will Sanchez: Yeah. And if you're watching, I, I put, uh, some of the examples between the surgical repair and the non-operative for, for partial tears, a low demand patient. Yeah. Uh, if you could just explain, uh, both options when it becomes a non-operative and how you make that decision.
Yeah. Compared to the surgical repair, which may seem obvious, but still, I would like for your input on that. Yeah.
Dr. Grant Garcia:: So the word partial tear is kind of a misnomer, right? Like a partial tear here, he partially, he didn't tear off both heads. So usually you still have the sternal head. Yeah.
So he pulls off the sternal head and then he keeps the clavicular head.
And then the thing is that basically that's a partial tear, but all the contour and muscle strength is gone. Does that what make sense? Yeah. So that still needs to be fixed. Now. Someone really low demand like. You know, maybe eighties, maybe seventies. They don't really need to do a lot. Yeah, it's a [00:09:00] big surgery 'cause you're pulling that all muscle back.
You gotta make a big incision in the shoulder and pull it back. You wouldn't do it for, but even up to sixties. I've had weightlifters, bodybuilders in their sixties that I've done it on and they've done quite well. It kind of depends on the patient. It's exactly the same thing. It's a custom approach.
Let's say you have that, it pulls off, then you want to fix it. Usually we try to do it in the first six weeks, but I'll be honest with you, I have a guy who's actually, thankfully he's doing well. He was like seven, eight weeks out. I thought it was gonna be super straightforward. I went into the P tendon, I tried to pull it back, and the tendon was about four centimeters too short.
So look at this. That's a lot, right? You gotta fill that with something or you leave him, right? But this is the guy. He's 40 years old and he has, he can't get his, he can't pull his arm in like this total contour loss. Oh. So I remade it with a cadaver tendon. Um, and that, that's a pretty effective cadaver and s
Will Sanchez: scooters and things like that.
They're just trying to, at that point you're connecting.
Dr. Grant Garcia:: Yeah. Well, we'll see that. The audience will see shortly in about six weeks we're gonna post the technique and how I did it. Uh, but the idea is that you basically take this Achilles tendon. [00:10:00] The Achilles is from. The lower part of your ankle, you fan it out and then you weave it into the muscle, which is pretty sick.
And then you sew it in. There's some, there's a little bit of techniques, but on this one, you're gonna love it. 'cause I added an internal brace, which has not been out published yet. So that is a pretty cool con. I knew it. I knew it. So the cool part about this is, it's amazing. He came back at eight weeks and he looked like JJ Wall, not the same size, but the same outcome.
I mean, literally killing it. So. I wonder if that had some level to do with it. But the idea is that basically now we're using these, as long as we can fix the brace from one side to the other side, we're adding these fiber tapes, internal braces, uh, to patients. So I'm finding any ways I can do it. So, you know, they got the graft, they have the graft tendon integrase, and now they also into the bone, have this internal brace.
Will Sanchez: Um, you brought up JJ Watt and I remember when he tore his pack and you know, over here it says that, you know, it's supposed to be out four to six months, but he was back in [00:11:00] 10 weeks. And for the football fans, they remember he wore that big, bulky black. You know, restraint on his arm that went all the way down and he pretty much, I think he played with it for the rest of his career, I think at that point.
Yes. He kind of kept that on. So let, let's talk, it's twofold. The question one, what did they do for him to get back so fast? And then two and two. Why? Why should he, you know, especially playing football, keep that protected for the rest of his career? Is it something that at that point it would've been vulnerable?
Yeah. Due to age sport or maybe the procedure itself in order for him to get back fast.
Dr. Grant Garcia:: So let me make the caveat that you have now hosed me for any of my pet tendon repair patients, because I used to think that not as many people were listening to this, but I've had multiple patients ask me, they're like, you said on your podcast that this is the way it is.
So just so everybody here, there's a disclaimer here. This is [00:12:00] JJ Watt, a professional athlete with millions of dollars on the line and the playoffs. This is a different level. If he had torn it like his other, uh, Whitney Marcellus, who was also on the team. Yeah. If he had torn it at the end of the season, they would've taken him out for the entire recovery period. Right. So that's, that's a first caveat.
Will Sanchez: Six months to six months. Correct.
Dr. Grant Garcia:: Yeah. I'm sure they did some crazy stuff during his surgery. I'm sure they repaired it. And I used to work with some of the guys that did a lot of the football players and whatever they did. They might have added something, addition.
So if they got an acute repair, which is what they did. For, for our, for, uh, Gregor, they got to him so quickly, like, you know, my average time to see these is three to four weeks, just 'cause you gotta wait to see the doctor and get an MRI and everything else. But if you're on the field and they tear, they can fix it right away.
You can get a really good fixation right away, but I bet you with him, they added something else too, right? Did they add a patch? Did they add some extra stuff in there that, you know, not always the best case scenario, [00:13:00] but in this case helps him back it up. But at the same point, you know, if he's not. I mean, grappling is good, but if he's got this so solid restraint, he's really not using his arm.
He just needs to use it as like a peg.
Will Sanchez: Yeah, yeah,
Dr. Grant Garcia:: yeah. Right. So when I let him play. I can't say that I feel comfortable enough to let my a player play at 10 weeks after a massive injury like this, but again, I am Will Sanchez: was defensive player of the year. Also, as they're making a run, they gave them all this money.
Like yeah, we, we've talked about, we don't know
Dr. Grant Garcia:: what the contract was though either. So the answer is that that's really impressive. We know they continue to prove it. Right. We've always said like, some of these players get back faster, but the, the, the part of it that's important for people to understand is that the average time.
For this is like a six month recovery, right? The average time is six month recovery. That is what you should expect if you're getting this surgery. He is an outstanding one. Now I know there's been other players that have been in like the 10 to 11 week recovery, but you need to understand again that this is, there is [00:14:00] different constraints on the line here, so this is what the point, pardon?
You got this sort of immobilization phase four weeks, then you start working on gentle motion. 'cause remember this muscle's so massive. So strong in many of the players and patients that we take care of, you know, no offense, but the little old ladies are not popping their pecs.
Will Sanchez: Yeah, yeah, right.
Dr. Grant Garcia:: The guy I just saw today that I need to fix his pec tear, he's 280 pounds and he moves stones, right?
Like this is not you. This is not something that these people are not weak liens that are hearing something. So there's massive muscles and massive strength you need here, right? They're bodybuilders, they're high level weightlifters, they're football players. They're very. High intensity laborers, right?
This is, or there are massive injuries where they hit a tree or something, so you're progressively letting this muscle sort of scar down, and then you start the motion, usually four to six weeks, then they start moving their arm and strengthening, and really six months is that sort of return to sport, four to six months?
It depends on the athlete. Depends on the, on how they're doing and [00:15:00] what they have to get back to. It also depends on getting emotion back the
Will Sanchez: sport. Right? I mean, I would think for, uh, for Gregor, that has to swing his arm, right? His, his tennis season is completely done. He won't be back in time for us open.
Yeah. The next time that he plays maybe is AAU Australia, or if not, maybe waiting to Wimbledon. Well, let's, but let's
Dr. Grant Garcia:: talk about what I think might happen to him, because if he doesn't get a perfect repair. That whip that he does that in, we call that like that's the internal rotation where you're like belly pressing.
Mm-hmm. And you're pushing in, that's his pec. His pec allows him to whip it around that fast. Does that make sense? Yeah. Yeah. It's his rotator cuff, but really the pec is what's pulling on it. And it, as it as it, it's, yeah. It's like basically launching that arm forward. So the concern we have here, right, is he gonna be the same in terms of his, his serve speed
Will Sanchez: 30?
He's probably gonna have a
Dr. Grant Garcia:: lot of it.
Will Sanchez: 34 years old. Doctor, I just wanna add that as you're speaking.
Dr. Grant Garcia:: No, and I, I think that's important. And I think, [00:16:00] you know, modern medicine, we've talked about this, I'm sure maybe the, maybe they added an internal brace to 'em, maybe they added some graft, maybe they did all these fancy things.
And the recoveries are quite good. I mean, usually we can get them relatively symmetric. We can get really good results with these, and my patients tend to do quite well with this. So it's not like it's something that's like, you know, incredibly poor results and people don't do well, but. It's you. The data shows you will lose power, right?
You lose some bench press power no matter what. Talk show you look at. This is not something we're like, we've looked at this return report. It's actually on one of these papers for p and the, the bench press max decreased on the injured side, no matter how much we try to do. So again, we know this are papers, they're not perfect.
It's an average. So there's always someone that's above and there's always someone that's below. So it's important to have that in understanding of this. Now, again, there are young pec tears, the 20 fives, thirties high level athletes like this.
Will Sanchez: Yeah.
Dr. Grant Garcia:: They're a different animal than the [00:17:00] 50 to 60-year-old pec tear.
Yeah. So it's just, there is still a difference and the recoveries are faster, but also some of these bacteria get really, really, really stiff. Right. Because you're not moving them and you're trying to get it up. And my biggest thing to turn is can he get his motion back? Because that's his sort of.
Throwing, serving shoulder. I mean, we talked about some baseball players. You stiffen up the shoulder in a baseball player. They're done.
Will Sanchez: Yeah. Yeah. No, that, and that's what I was gonna ask. So, uh, you know, when that injury looked, I mean, he finally sat down right after he felt it the second time, so I'm not sure what the damage was.
Obviously he tore it on the first time when he felt it, and then finished it off on the second one, and then sat down, grabbed the. Himself. I mean, I'm assuming that in that muscle area, by the chest area, by the arm area, that's extremely painful as well, right? From a cough to a move to laying on your side.
Yeah. They hurt everything [00:18:00] that that's going along with it, let alone, because you know, on the graph they were talking about, it was like zero to four weeks. We're just managing and we're managing pain. You know, and, and they, well, and
Dr. Grant Garcia:: he, and he might start earlier, right? Because I mean, there's no way JJ Watt was zero to four weeks if he's that fast at 10 weeks.
No, but I mean, the good news here is there was a recent, there is 2022, there was a study by ggi, uh, at all and 90% return to sport. Now, again, they're not looking at professional tennis players 'cause it's not that common. But here's the caveat, 74% return to pre-injury performance. So it's not a hundred percent.
We know of players. Terrell Suggs is one of them. He just was never the same. Afterwards, like, you know, not everybody comes back at full motion, but again, tennis serving me, me, a little bit less power needed if he's got other muscles and he is that good. But we also talked about this before, that some of these professional athletes, if they lose 5%, they're still elite, right? Like if LeBron James has three body [00:19:00] parts out of four total limbs. It'd probably still be equivalent to maybe some of the average players in the league. Right. So this just, it's a different animal.
Will Sanchez: Uh, two questions. Um, I've seen this scar from the injury in the past. It looked quite big with, in 2025. Has that SHR and down, or is this still something Yeah, 'cause of the, the operation, you're still dealing with that scar.
Dr. Grant Garcia:: It just depends on the. Surgeon approach, et cetera. And obviously as we get better, like I do, I do a fair number of these. So my incision, this is my phone right here. It's about half the size of my iPhone. I'm sorry. It's hard to see the picture. Yeah, but probably like my average size is like five to six centimeters, so it's not terribly big.
They're definitely. We definitely move it over to make it a little more cosmetic. It kind of depends on your approach. You can't go much smaller than that, especially on a big guy. Right? Like he's, the good news here is this is gonna be an easier approach than doing JJ Watt. [00:20:00]
Will Sanchez: Yeah,
Dr. Grant Garcia:: right. Like imagine it's probably half the distance.
Yeah, you gotta go to get in down there to the bone, right? Because he's not a very big guy. He is skinnier. So this is gonna be a pretty straightforward situation and it's acute. So, you know, you get in there and it's gonna basically show itself and you be able to fix it. I mean, it probably would take the surgeon under an hour to do that, which is good.
Obviously the, the surgery's not the big part. It's the recovery. Um, but, you know, this is a good outcome. I mean, this is of some of the, the times we talked about this is a good outcome.
It's just uncommon, especially in most players. I mean, we know JJY is a big deal. We know Dante Hightower, we know, uh, you know, Terrell Suggs, but it's overall not a common thing.
Like if you look up all the number of athletes, there's a handful. It's under 12.
Will Sanchez: Um, silly question, would this be a procedure that you would possibly use, kind of like that lavender effect, uh, to treat it depending on that surgery or is that something We're, we're talking about apples and oranges at this point.
Dr. Grant Garcia:: So [00:21:00] the idea behind biologics is, can you do like amniotic wraps? Mm-hmm. Or anything else to get adhesions, right? Like, 'cause really anything we do, we want it to heal faster. So like, if I could get the tendon to heal to the muscle in two weeks instead of six, then I would start moving them and then they'd go, they would, as soon as, because the, the challenge here is once you fix it, sometimes the patients take forever.
Like some of these patients are so tight 'cause I, I don't want to do a graft on them because a graft in my opinion is it's good, but it's not as good as the actual tendon itself.
Will Sanchez: Yeah. Yeah.
Dr. Grant Garcia:: I put 'em so tight that they're like this when they start and then they stretch out over time. Right. Some people like put 'em loose enough because they're not able to do, they're able, they're, they're fine.
You don't need to stress about it too much. But the ones that are super tight, they take a while to get back. But if I knew that they would be healed right. Faster with biologics, like using some sort of putty, some sort of bar, bone marrow aspect or amniotic thing, we could, the problem you have too though, is you don't wanna increase the risk of infection.
You start throwing on patches and everything else. [00:22:00] Oh, that's good. You don't wanna cause
Will Sanchez: Yep.
Dr. Grant Garcia:: It's different in the knee because the knee is getting flow with fluid. It's much lower risk. But, and also it's, the challenge here is like the outcomes aren't bad, right? Like there's not enough of them. They're kind of rare, like even high volume surges, they do like 5, 5, 10, a year.
Like I remember I saw a study, some guy like 26, I was like, that's incredible, right? It's not that common unless you cover the CrossFit games where they had almost over 20 of them in one event.
Will Sanchez: Wow. Wow. Well, you know, they're, they're, they're moving so much weight and it's so fast. You know, they, it's, it's almost kind of like you tell people when you're working out the gym, like, slow down, take your time.
You're trying not to get injured CrossFit games. You're, you're, you're just moving heavy weight and you're trying to get through it as fast as I'm just telling
Dr. Grant Garcia:: you that surgeon was very busy. Very busy that day.
Will Sanchez: It is like, we got another one. Geez. Um, yeah. Listen, you know, we, we hope for the best obviously as being a tennis player with that type of injury and his age is a little [00:23:00] bit concerning.
I know he's a fan favorite. I know a lot of the tennis players, uh, like him, sinner was really disappointed. This is the. Fifth major in a row that he has sustained an injury that, um, that made him pull out, uh, of the tournament, you know, for various reasons. I think it was one, a couple of them were leg injuries and groin and things like that.
So. Um, you know, maybe the toll of the body with this sport is not ideal. But he's a, he's a great player. He was phenomenal and I thought he was gonna be the number one player when I was watching him. And he, he, he had him right there until he suffered that injury. So, uh, you know, we wish him the best and hopefully he'll get a chance to, uh, play and going into, uh, next year.
So we'll see. Hopefully speed, speedy recovery. All right. Any last thoughts? I know you kind of teased it a little bit, that you're gonna have a video coming out in about six weeks, that's gonna discuss six weeks, all these things. So, uh, we'll, yeah, check it out.
Dr. Grant Garcia:: We'll refer back to this episode and, uh, hope you guys learned a little bit more about this.[00:24:00]
It's a, it's a really interesting injury. And listen, we, we always have this. Sports Talk com. We get guest requests all the time. We're getting them like, geez, like two, two a month now, uh, or more. We get questions from the audience, so let us know if you have any questions about this. We're happy to answer them and always refer to our websites.
Uh, there's tons of information on this, more than you need to know. So,
Will Sanchez: all right. Say goodbye, Dr. Garcia.
Audio Transcript
AI on the Field: Wearables, Recovery & the Future of Sports

Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. Do not worry. I am real.
00:00:00,160 --> 00:00:00,720
Will Sanchez: Foreign.
00:00:16,160 --> 00:00:20,800
Welcome to Sports Doc Talk. Do not worry. I am real.
00:00:20,880 --> 00:00:22,560
This is not AI I.
00:00:22,560 --> 00:00:25,000
At least I hope maybe. I don't know.
00:00:25,000 --> 00:00:25,760
Dr. Grant Garcia: We never know.
00:00:26,360 --> 00:00:30,480
Will Sanchez: Yeah, I didn't know if we should do the Terminator music, but I was worried about copyright
00:00:30,480 --> 00:00:33,240
issues going into this AI discussion.
00:00:33,480 --> 00:00:36,440
Anyway, I digress, as I usually do. Dr.
00:00:36,440 --> 00:00:38,680
Garcia, welcome to the show.
00:00:39,800 --> 00:00:42,840
He's our orthopedic surgeon, sports medicine specialist.
00:00:42,920 --> 00:00:53,490
Before we get started, once again, sorry to do this to you. You're named top doctor. Once again. Congratulations.
00:00:53,730 --> 00:00:55,530
I mean, you have a lot of accolades.
00:00:55,530 --> 00:00:59,570
You put in a lot of work, you travel, you do your thing. This is not a.
00:00:59,810 --> 00:01:02,050
A show about, you know, pumping you up.
00:01:02,050 --> 00:01:07,170
And I didn't tell you about this beforehand, but I want our listeners to know that you're constantly
00:01:07,170 --> 00:01:13,050
getting recognized, not only in your state, but nationwide, how talented you are.
00:01:13,050 --> 00:01:16,690
So I just want to say congratulations before we get into real conversation here.
00:01:17,690 --> 00:01:21,810
Dr. Grant Garcia: I definitely blindsided by this, but I appreciate it. Thank you so much. Yeah, no, it's.
00:01:21,810 --> 00:01:23,010
It's a really nice honor.
00:01:23,010 --> 00:01:25,370
And, yeah, we take good care of patients.
00:01:25,450 --> 00:01:27,050
And this stuff's the fun part.
00:01:27,050 --> 00:01:30,290
We get to talk about the random stuff and chill podcast mode.
00:01:30,290 --> 00:01:31,130
I get to wear my hat.
00:01:31,130 --> 00:01:36,010
About to go in the sun after this. Nice, relaxed, casual. So this is the.
00:01:36,010 --> 00:01:37,290
This is the fun part for me.
00:01:37,290 --> 00:01:43,450
And then in the office, you know, we make sure we take care of the serious issues. But no, as. Yeah, I appreciate it. No, it's been fun.
00:01:44,040 --> 00:01:49,760
Will Sanchez: All right, let's give a quick shout out to our friends at the recovery shop. Dr. Garcia, take it away.
00:01:49,760 --> 00:01:54,920
And just let everybody know why the recovery shop is number one on your list when it comes to recovery.
00:01:55,480 --> 00:01:58,080
Dr. Grant Garcia: I mean, I think the biggest thing for me is it's a busy day.
00:01:58,080 --> 00:02:00,240
You're scheduling patients for surgery.
00:02:00,240 --> 00:02:04,360
You're trying to make sure everybody's on time, give them their time, and then, you know, the
00:02:04,360 --> 00:02:07,400
patient gets through the whole surgical conversation about schedule for surgery, and they're
00:02:07,400 --> 00:02:08,760
like, what else can I do, right?
00:02:08,760 --> 00:02:10,700
How do I make my thing better?
00:02:10,860 --> 00:02:13,860
So this allows me to say, hey, listen, I trust this recovery shop.
00:02:13,860 --> 00:02:14,700
I work with a lot.
00:02:15,020 --> 00:02:19,260
We've handpicked some things from there, and so the patients afterwards can sort of have a potpourri
00:02:19,740 --> 00:02:23,980
or a sort of catalog of what they want to get after surgery, of things that I would recommend
00:02:24,540 --> 00:02:27,500
anywhere from recovery, the nice machine, to nutrition.
00:02:27,500 --> 00:02:32,700
We've talked about this with two of the least the players on there and, you know, many other different things.
00:02:32,700 --> 00:02:35,590
And if there's something that they want we can get it for them, which is really nice.
00:02:35,740 --> 00:02:37,180
So it's all kind of one stop shop.
00:02:37,260 --> 00:02:38,380
It's great for the patients.
00:02:38,380 --> 00:02:43,820
Patients have loved it, had a lot of good reviews and for the doctors, you really should be
00:02:43,820 --> 00:02:46,380
doing this or having something like this for your patients because the patients are going to
00:02:46,380 --> 00:02:50,700
ask for more and so to be able to give this to them, it makes them feel and a lot of it data
00:02:50,700 --> 00:02:59,660
driven that you can get people back with better outcomes as well. So it's been great. So contact Mike B. He's awesome. Yeah.
00:02:59,740 --> 00:03:02,380
And maybe there'll be AI for that soon too. Who knows?
00:03:02,800 --> 00:03:07,880
Will Sanchez: Who, who knows? You know, let's kind of get into that and we, we utilize an AI.
00:03:07,880 --> 00:03:16,080
And what's amazing is that we've only had access to AI as far as common folk for a very short
00:03:16,080 --> 00:03:20,080
time and it is booming in every aspect of our lives.
00:03:20,880 --> 00:03:26,720
I'm, I do events, I do a bunch of different types of events in person hybrids, things like that.
00:03:27,120 --> 00:03:28,800
I do a lot of work for Microsoft.
00:03:29,730 --> 00:03:37,410
Constantly using AIs, constantly being part of conversations with AIs, senior leadership teams talking about AI.
00:03:37,570 --> 00:03:39,490
I utilize it in my everyday life.
00:03:39,890 --> 00:03:43,810
This boom of AI that's happening across the world.
00:03:44,210 --> 00:03:49,090
How are you seeing that effect not only your everyday, but at work as well?
00:03:50,210 --> 00:03:55,650
Dr. Grant Garcia: I mean it's not only from when I get home and open the news talk about AI, but you know, obviously
00:03:55,650 --> 00:03:58,130
chat GPT everybody knows about and now everything's great.
00:03:58,130 --> 00:04:02,870
Yet like, you know, the idea is that chat GPT in the next few years will be the new Google search terms. Right.
00:04:02,870 --> 00:04:03,990
So no one's using that anymore.
00:04:03,990 --> 00:04:08,670
My wife basically uses ChatGPT on her phone to figure out if she has questions rather than googling it. Right.
00:04:08,670 --> 00:04:13,670
It's chat GPT in it, so it's here to stay and it's moving its way.
00:04:13,670 --> 00:04:18,550
I think, I think the biggest thing for me is the goal is here is to make our jobs easier.
00:04:18,550 --> 00:04:24,870
I think the concern, and we can jump to this in a second is for patients, is that, is it, is it a takeover? Right?
00:04:24,870 --> 00:04:29,090
Like is this artificial intelligence from the movies where all of a sudden you have robots doing
00:04:29,090 --> 00:04:32,210
everything for you and you never really see a human. Right.
00:04:32,210 --> 00:04:36,410
There are certain aspects that there may be that case, but there's certain aspects where really
00:04:36,410 --> 00:04:38,130
it's going to enhance the care that you're getting.
00:04:38,290 --> 00:04:42,170
And that's what we're here to talk about today is really help the patients understand from the
00:04:42,170 --> 00:04:44,970
sports and from the medicine side of things, where is AI?
00:04:44,970 --> 00:04:49,170
Because I've been seeing way too many articles about this and they each touch on little tiny topics.
00:04:49,330 --> 00:04:51,770
And patients are constantly asking me like, what's the future?
00:04:51,770 --> 00:04:56,320
Well, this is the future, but this is a broad future. Right.
00:04:56,640 --> 00:05:01,120
And I think again, the misnomer is this is version 2.0 of medical care.
00:05:01,360 --> 00:05:04,000
This is not a complete flip 180.
00:05:04,320 --> 00:05:09,959
You're not going to come into the office and see like, you know, you're going to see Dr.
00:05:09,959 --> 00:05:13,360
Garcia for your knee surgery and you meet a robot, right?
00:05:13,360 --> 00:05:14,640
Like that's not what's going to happen.
00:05:15,200 --> 00:05:19,200
What's going to happen is that you're going to make a phone call and it's going to be easier
00:05:19,200 --> 00:05:20,240
to get in touch with somebody.
00:05:21,220 --> 00:05:24,020
Simple questions may be answered by some sort of artificial intelligence.
00:05:24,180 --> 00:05:27,580
More detailed questions will get pinged up faster for you, which means that you're going to get.
00:05:27,580 --> 00:05:29,460
Because the workforce can only keep up so much.
00:05:29,700 --> 00:05:31,460
So now everything is going to be smoother for you.
00:05:31,460 --> 00:05:35,260
You're not even going to know that it's AI and then what's going to happen is when you actually
00:05:35,260 --> 00:05:40,460
really need to get the in depth stuff, you're going to meet the provider or the doctor or the
00:05:40,460 --> 00:05:46,060
nurse or the PA and your whole experience could be better rather than, I mean, how many doctor offices have you called?
00:05:46,060 --> 00:05:48,510
I mean, I would tell you that my doctor office does a really good job.
00:05:48,510 --> 00:05:54,390
We do our best to get things moving along and we still have delays and people waiting on hold and they're frustrated.
00:05:54,390 --> 00:05:56,870
Even in my office we're very efficient or private practice.
00:05:56,870 --> 00:06:02,310
I mean my wife's call for appointments, 45 minutes hour for other providers in different hospital
00:06:02,310 --> 00:06:06,990
systems on hold, waiting to get in touch with somebody and then delays in calendars and things like that.
00:06:06,990 --> 00:06:07,950
So that's the whole point.
00:06:07,950 --> 00:06:12,510
That's what it's going to improve, is improve care for patients, which people, it's hard for
00:06:12,510 --> 00:06:13,590
them to think about it right now.
00:06:14,660 --> 00:06:17,100
But let's not get too sidetracked with that.
00:06:17,100 --> 00:06:21,860
I think really the continued discussion here is that it's, it's going to address everything
00:06:21,860 --> 00:06:23,380
in all aspects of medicine.
00:06:23,380 --> 00:06:29,140
And we know this is the future because we don't always talk about investment on this standpoint.
00:06:29,859 --> 00:06:33,780
But, and we could put this, put this slide first before we get too far into that.
00:06:38,180 --> 00:06:42,540
So and go one more further, we'll just talk about the investment thing first and then we can
00:06:42,540 --> 00:06:44,180
pop back over to proceed barriers.
00:06:45,040 --> 00:06:48,760
So this is a really good graph, but you can see the billions of dollars that are going into this.
00:06:48,760 --> 00:06:54,760
So when you have companies like venture capital investing in healthcare startups, in AI, and
00:06:54,760 --> 00:06:56,120
this is like, where they're all going, right?
00:06:56,120 --> 00:06:58,480
Like, they're like, this is the next big thing, right?
00:06:58,480 --> 00:06:59,680
You know that you're onto something.
00:06:59,680 --> 00:07:00,719
You know, this is the future.
00:07:00,800 --> 00:07:02,920
But it's also, it's good for patients to see this, right?
00:07:02,920 --> 00:07:04,240
Because this is where the money's going.
00:07:04,240 --> 00:07:06,480
So this means that this is where the innovation is going to go.
00:07:06,880 --> 00:07:12,560
As much as we don't want to talk about money on this doctor's podcast, the money drives innovation.
00:07:13,280 --> 00:07:17,120
None of these companies, it's reality. It's drug companies, too.
00:07:17,120 --> 00:07:19,840
Like, you don't get these amazing new drugs because they're cheap and free.
00:07:20,000 --> 00:07:24,160
You get these amazing new drugs because there's a lot of financial gain for the pharmaceutical company.
00:07:24,320 --> 00:07:26,080
It's the same thing with these implant companies.
00:07:26,320 --> 00:07:27,720
There's a, there's a financial gain.
00:07:27,720 --> 00:07:30,800
We want to make patients better, we want to make them get back faster.
00:07:30,800 --> 00:07:33,840
But there's also a, there's also a monetary aspect of this.
00:07:34,000 --> 00:07:35,000
So it's the same thing.
00:07:35,000 --> 00:07:36,920
They're in VCs, investing, AI startups.
00:07:36,920 --> 00:07:39,840
So this is here to stay and this is where the industry is going.
00:07:39,840 --> 00:07:44,080
I mean, I've gotten calls with financial advisors and talking about, you know, we're really
00:07:44,080 --> 00:07:48,840
looking at AI as the future, but how can we use it to decrease some of the workforce that we
00:07:48,840 --> 00:07:51,920
don't need as much and switch over the jobs, not stealing jobs.
00:07:51,920 --> 00:07:54,120
But now you have AI jobs, right?
00:07:54,200 --> 00:07:58,600
You're in charge of designing AI programs rather than the AI taking your job.
00:07:58,840 --> 00:08:01,960
Now, again, I'm not going to go into too much detail with this because obviously I'm not the
00:08:01,960 --> 00:08:04,440
world's expert on it, but that's what we're seeing.
00:08:04,900 --> 00:08:09,860
But if you want to go back to that first slide, I think this is really interesting for someone
00:08:09,940 --> 00:08:12,820
maybe you, for more layman terms, can under, can think about this.
00:08:12,820 --> 00:08:18,820
There's perceived barriers, right, in healthcare, and the one that you don't see is implementation
00:08:18,820 --> 00:08:24,500
costs as much as this is going to speed us up, make us better, make us faster and make us stronger.
00:08:25,140 --> 00:08:26,820
It is not cheap, Right.
00:08:26,820 --> 00:08:29,900
And everybody's trying to make a buck off this. So you have companies.
00:08:29,900 --> 00:08:34,500
I mean, I literally opened my LinkedIn yesterday and had six, six AI offers for companies that
00:08:34,500 --> 00:08:42,820
wanted to AI my revenue, AI my billing, AI this, AI that, and for a small fee, they'll help you implement it, right? Yeah.
00:08:42,900 --> 00:08:48,060
Or you have the people that are the chat GPTs that are not chat GPT, but they're faking it, right?
00:08:48,060 --> 00:08:50,740
They're charging you for chatgpt on top of it, right.
00:08:50,740 --> 00:08:53,020
Like everyone's trying to make a buck off this. So they're expensive.
00:08:53,020 --> 00:08:57,860
I mean, and as much as AI is just computer, you think it's, it's low cost.
00:08:58,020 --> 00:09:00,980
There is still a cost to it because people are programming this AI.
00:09:01,290 --> 00:09:04,650
Maybe at some point you won't need to, but there are still people that have to be involved in
00:09:04,650 --> 00:09:06,650
this and there's still implementation costs.
00:09:07,050 --> 00:09:09,650
So that's really important to be aware of.
00:09:09,650 --> 00:09:12,650
And obviously like you said that here you can see the workflow integration.
00:09:12,650 --> 00:09:16,810
Like how do you work it in to a doctor's office that has really minimal medical records?
00:09:16,810 --> 00:09:19,690
Like we have, we have a lot of digital, but some offices are paper.
00:09:19,690 --> 00:09:23,330
How do you do an AI with a paper office? That's very challenging.
00:09:23,330 --> 00:09:26,930
You got to start the infrastructure of that in Seattle.
00:09:26,930 --> 00:09:32,310
It's less, but, but there's still plenty of offices that still do paper with some respect to the other, especially across.
00:09:32,310 --> 00:09:38,910
Will Sanchez: The country, depending the communities and you know, how old people have been there, what you
00:09:38,910 --> 00:09:46,150
know, because as most of us, you know, we kind of stay formatted with what we know best. Right.
00:09:46,150 --> 00:09:48,390
And sometimes we don't proceed with change.
00:09:49,190 --> 00:09:53,510
Kind of piggybacking on the fact that you're talking about how some offices wouldn't be there.
00:09:53,590 --> 00:09:54,990
But the big one that I'm.
00:09:54,990 --> 00:09:59,700
When we're looking at the graphic here, privacy and compliance, right, that to me is the big concern, right?
00:09:59,700 --> 00:10:02,340
That's, that's going beyond AI.
00:10:02,340 --> 00:10:07,980
Those are the Facebook conversations and data that's being shared.
00:10:07,980 --> 00:10:12,260
And so when it comes to concerns, right, those are the big things.
00:10:12,740 --> 00:10:19,780
Are there certain things that are happening in offices or are we still too early as far as making
00:10:19,780 --> 00:10:27,070
sure that the privacy and compliance doesn't spill when it comes into AI and how information is being shared.
00:10:27,950 --> 00:10:31,750
Dr. Grant Garcia: So I think when you think of AI, you think of like, you know, I think the layman person may
00:10:31,750 --> 00:10:33,590
think like AI, this is a compute.
00:10:33,590 --> 00:10:38,270
This is a self thinking learning module that we're going to set up.
00:10:38,270 --> 00:10:40,190
So you really can't put bars on it, right?
00:10:40,270 --> 00:10:40,630
Will Sanchez: Yeah.
00:10:40,630 --> 00:10:44,230
Dr. Grant Garcia: But the thought process is this is still a program, it's still designed and then it has its
00:10:44,230 --> 00:10:45,590
own learning capabilities to it.
00:10:45,590 --> 00:10:48,830
But it really is, not only is it learning, but it's basically can pull a lot more information
00:10:48,910 --> 00:10:54,140
from around the world and through the Internet than the average program too can do. Right.
00:10:54,140 --> 00:10:55,060
It's just not as clunky.
00:10:55,060 --> 00:10:57,620
It's like the upgraded computer, but much better. Right.
00:10:57,940 --> 00:11:01,500
And so the, the process here is that, you know, there is HIPAA compliance.
00:11:01,500 --> 00:11:05,939
We have hipaa, which is where we try to protect people's things. But it's hard, right.
00:11:06,180 --> 00:11:09,940
Like if you, I think the thought is that basically it's not going to be an exput.
00:11:09,940 --> 00:11:12,620
Like basically the idea is like it can gather information from you.
00:11:12,620 --> 00:11:17,100
It's not going to like start sending off your data to other people. But yeah, you're right.
00:11:17,100 --> 00:11:21,250
I mean if you have, if you design something that can like break through firewalls and it's like,
00:11:21,250 --> 00:11:22,970
okay, how do I diagnose this patient?
00:11:23,130 --> 00:11:27,490
Well, the only way this AI knows how to do it is to break into someone's records and take everybody,
00:11:27,490 --> 00:11:31,530
every patient's ever had that diagnosis, look at all their symptoms and then diagnose your problem
00:11:31,770 --> 00:11:35,090
that's concerning, so you have to have it.
00:11:35,090 --> 00:11:35,810
But the problem is too.
00:11:35,810 --> 00:11:37,530
It's also got to be more of a global thought. Right.
00:11:37,530 --> 00:11:42,890
So, so we're not there yet, but there's certain implementations that are not really needed for hipaa.
00:11:43,050 --> 00:11:49,060
Right there you're talking about like making a diagnosis without any provider available, without any other records.
00:11:49,140 --> 00:11:52,260
But there's enough stuff online that like, you know, it.
00:11:52,420 --> 00:11:54,060
Much as I hate some of the Dr.
00:11:54,060 --> 00:11:55,260
Googlers, you know what I mean?
00:11:55,260 --> 00:11:57,860
If you would come in and they maybe Dr. Jack Gpters.
00:11:57,940 --> 00:11:58,300
Will Sanchez: Yeah.
00:11:58,300 --> 00:11:59,180
Dr. Grant Garcia: You know what I'm talking about.
00:11:59,180 --> 00:11:59,620
Will Sanchez: Yeah.
00:11:59,780 --> 00:12:02,179
Dr. Grant Garcia: Diagnose themselves on chat GPT.
00:12:02,500 --> 00:12:06,420
And I have to explain to myself how that may not be exactly right. Right.
00:12:06,420 --> 00:12:08,140
Some of them are right and sometimes they're not.
00:12:08,140 --> 00:12:08,780
Will Sanchez: Yeah, yeah.
00:12:08,780 --> 00:12:15,110
Dr. Grant Garcia: But the, the point being here is that, you know, they, there is some aspect that you have, you
00:12:15,110 --> 00:12:18,350
can get that innately you don't need to go into somebody's records and get that information.
00:12:18,430 --> 00:12:22,910
Like if it's, there's enough data and enough textbooks out there that don't have patient information
00:12:23,070 --> 00:12:26,510
that most of these programs can learn from. So I have low.
00:12:26,510 --> 00:12:31,630
I don't much concern about it because I feel like it's very stringent and fortunately the medical
00:12:31,630 --> 00:12:33,390
field's way more stringent than anything else.
00:12:33,550 --> 00:12:37,440
So basically like, if I want to do something like, it's got to have gone through multiple checks. Right.
00:12:37,440 --> 00:12:38,720
It's like the pharmaceutical injury.
00:12:38,720 --> 00:12:42,240
Like you can't just like start putting things out there versus there's a lot of other things
00:12:42,240 --> 00:12:46,840
which we can, we don't talk about now that are industries where there's no bars, there's no checks and balances.
00:12:47,080 --> 00:12:48,920
I have tons of checks and balances on me.
00:12:48,920 --> 00:12:51,200
So there's still always room, as we know.
00:12:51,200 --> 00:12:52,919
If you look at the news, you've seen it before.
00:12:52,919 --> 00:12:57,560
There's different ways people can be scrupulous, but it's a lot less likely in medical than is other fields.
00:12:58,040 --> 00:13:05,720
Will Sanchez: That leads me right into this question between using AI as a diagnostical tool versus a decision making tool. Right.
00:13:06,040 --> 00:13:12,170
You're still relying on everything that you've learned, all of your experience, maybe peer to
00:13:12,170 --> 00:13:14,210
peer, how does that compare?
00:13:14,210 --> 00:13:20,250
Or is that some of the conversations that happens within your office and just, you know, your peers?
00:13:20,970 --> 00:13:24,450
Dr. Grant Garcia: Yeah. So let's go to that slide on the top clinical uses of AI in 2025.
00:13:24,450 --> 00:13:27,850
I think that'll be good to go over that one and then we can kind of ping into the doctors.
00:13:27,850 --> 00:13:31,010
So, yeah, I'd say next slide, because that AIs. Yeah.
00:13:31,010 --> 00:13:32,170
So this is really good for patients.
00:13:32,410 --> 00:13:37,900
So when you think of diagnostic tool, it really kind of depends on what you're talking about.
00:13:37,900 --> 00:13:42,420
So the real use of this has been radiology and medical imaging. Right.
00:13:42,420 --> 00:13:43,940
Can we use AI to help?
00:13:44,020 --> 00:13:44,820
Will Sanchez: Why is that?
00:13:45,780 --> 00:13:52,820
Dr. Grant Garcia: Just to get. Because radiologists are very important, but there is a lot more black and white there.
00:13:52,820 --> 00:13:54,900
Like, you're not interpreting that picture.
00:13:54,900 --> 00:13:56,900
They're looking for something on the image. Right.
00:13:57,060 --> 00:14:02,070
And it's a lot different than, like, you don't have to listen to the patient, calculate the
00:14:02,070 --> 00:14:04,790
mri, calculate physical exam, and then hopefully use your experience.
00:14:04,790 --> 00:14:06,630
And then sometimes it's the patient's decision. Right.
00:14:06,630 --> 00:14:10,670
You'll, like, you get a patient that comes in and they have an ACL tear.
00:14:10,990 --> 00:14:13,870
The program may just say, you just need to fix it, fix it, fix it, fix it, fix it.
00:14:13,870 --> 00:14:14,990
Like everything says fix it.
00:14:14,990 --> 00:14:17,070
But the patient doesn't want that surgery. Right.
00:14:17,070 --> 00:14:20,870
So how is the AI machine going to back off and say, listen, I got to listen to the patient here.
00:14:20,870 --> 00:14:21,510
Will Sanchez: Yeah, yeah.
00:14:21,510 --> 00:14:24,190
Dr. Grant Garcia: Versus in radiology, there's no conversation between the patients.
00:14:24,950 --> 00:14:29,270
They're maybe talking to the doctor occasionally, but they're all they have is that one thing in front of them. Right.
00:14:29,270 --> 00:14:32,230
And they have data pieces, maybe the patient's diagnosis.
00:14:32,470 --> 00:14:34,310
So it's a lot easier to put in the data.
00:14:34,630 --> 00:14:36,390
And then they can look at patterns. Right.
00:14:36,870 --> 00:14:41,750
We all use patterns in our brain, but a lot of times my patterns are developed from multiple pieces.
00:14:41,750 --> 00:14:46,390
It's physical exam, which you can't get from AI until it's actually been done. Does that make sense?
00:14:46,550 --> 00:14:47,030
Will Sanchez: Yep.
00:14:47,030 --> 00:14:52,820
Dr. Grant Garcia: And then there's experience. Then there's also conversation with the patient, hearing what they're
00:14:52,820 --> 00:14:55,860
saying, because sometimes they don't know, like they'll give you exam findings that'll be all off.
00:14:55,860 --> 00:14:59,140
And you've got to interpret that plus the mri, plus that. Does that make sense?
00:14:59,140 --> 00:14:59,860
Will Sanchez: Yeah, yeah.
00:15:00,740 --> 00:15:03,460
Dr. Grant Garcia: It's just a little bit, a little bit more complicated in that sense.
00:15:03,460 --> 00:15:06,740
Not that radiology is not complicated, but it's pattern recognition.
00:15:06,820 --> 00:15:08,460
They're very, very good at, these radiologists.
00:15:08,460 --> 00:15:09,220
I mean you can see.
00:15:09,220 --> 00:15:11,700
Go to the side before, just really quickly and show this.
00:15:14,180 --> 00:15:15,220
If you can go by there.
00:15:15,220 --> 00:15:16,340
I just want to show this for them.
00:15:16,340 --> 00:15:20,710
I mean, that's AI versus for breast cancer, lung nodules, fractures.
00:15:20,710 --> 00:15:22,190
I mean, it's very similar.
00:15:23,870 --> 00:15:24,310
Will Sanchez: Yeah.
00:15:24,310 --> 00:15:28,630
Dr. Grant Garcia: So it's not like it's, it's not like these, it's not like these radiologists are making mistakes and they're finding it.
00:15:28,630 --> 00:15:30,910
And this is again, this is certain studies, right?
00:15:31,150 --> 00:15:34,830
If you look at a thousand studies, some studies will be positive, some studies will be negative.
00:15:34,830 --> 00:15:40,870
That's the problem with some of these massive problems that we look at, because you can interpret the data either way.
00:15:40,870 --> 00:15:43,590
You can interpret this data and say, well, they're all higher in the AI.
00:15:43,590 --> 00:15:44,900
So AI is better than radiology.
00:15:45,610 --> 00:15:47,170
But like what are they diagnosing? Right?
00:15:47,170 --> 00:15:49,370
Are they diagnosing non cancerous breast cancers?
00:15:49,370 --> 00:15:52,330
Dan's gonna see cancerous breast cancers. They're different, right?
00:15:54,970 --> 00:15:57,210
Yep. Let's be honest right here. Lung nodules.
00:15:57,210 --> 00:16:01,209
And I look at MRI, saw two MRIs in the last three months that have shown a lung nodule.
00:16:01,209 --> 00:16:03,210
But they're usually benign, right.
00:16:03,210 --> 00:16:08,730
So now that person's got like extra aggressive findings that the AI machines like you have a
00:16:08,730 --> 00:16:10,170
lung nodule and now they're freaking out.
00:16:10,500 --> 00:16:11,540
Ends up not being a big deal.
00:16:11,780 --> 00:16:14,820
So we gotta like, we're not there yet and we gotta like interpret that.
00:16:14,820 --> 00:16:18,420
Like how, you know, when the, when the radiologist sends us the lung nodule thing, they say
00:16:18,420 --> 00:16:21,340
cannot, you know, not concerning for major cancerous things.
00:16:21,340 --> 00:16:25,180
But by this criteria, you know, you should look in six months and blah, blah, blah, blah.
00:16:25,180 --> 00:16:29,940
But maybe the is just gonna be like long nodule, not good. Right. Like you don't know.
00:16:32,900 --> 00:16:38,420
Will Sanchez: Also a checks and balances, you know, as far as in conjunction. Right.
00:16:38,990 --> 00:16:46,110
So based on your diagnosis and then checking it with AI, you know, so is that tool being utilized
00:16:46,590 --> 00:16:49,230
in that manner or in a different manner?
00:16:49,870 --> 00:16:50,990
Dr. Grant Garcia: I think that's an excellent point.
00:16:50,990 --> 00:16:54,430
I mean that's really what AI is for us in medicine. It's a conjunctive tool.
00:16:54,830 --> 00:16:59,950
Like the, the expectation is not that you're going to send this, your images to an AI radiologist.
00:16:59,950 --> 00:17:05,639
The area is going to scan it, and then they're going to send it back to you and no one will have checked it. Does that make sense?
00:17:05,719 --> 00:17:08,759
Because I can tell you right now that I would never want my images done like that.
00:17:09,159 --> 00:17:14,479
But what is going to happen is, let's say the radiologist, like t I had this week, I had a radiology
00:17:14,479 --> 00:17:19,399
report that was not accurate compared to the mri, but I checked my own and it happens. It's the same way.
00:17:19,399 --> 00:17:22,759
Someone can check me and they'll say, maybe Garcia is not perfect all the time. We're not perfect.
00:17:23,159 --> 00:17:27,639
But what's going to happen is the radiologist reads the report and then the AI double checks
00:17:27,639 --> 00:17:33,380
it, and if it finds a discrepancy, it calls the radiologist before they send it to you. So there's less mistakes. Right.
00:17:33,380 --> 00:17:36,020
And so that's really what's going to happen. That's where we're going.
00:17:36,180 --> 00:17:40,820
Or for very simple things, let's say you're in a rural place and you get an MRI and you can't get a radiologist.
00:17:41,300 --> 00:17:43,020
You don't have a contract or something happened.
00:17:43,020 --> 00:17:47,780
Or let's say you find a weird tumor and you're in the middle of somewhere and you don't have a.
00:17:47,780 --> 00:17:51,100
You don't have a contract with a radiologist that knows that specialty well.
00:17:51,100 --> 00:17:55,300
Now you can use AI to be like, okay, this is what I think it is, and it's a lot cheaper.
00:17:55,540 --> 00:17:58,490
And then you can send it over to the appropriate people. Right? That's where.
00:17:58,490 --> 00:17:59,730
That's where we're going to go with that.
00:18:00,690 --> 00:18:08,610
Will Sanchez: Those interpretations more as a tool than just a straight hand over, say, well, you do it. You know, it's. It's in conjunction.
00:18:08,770 --> 00:18:10,770
And then how does that benefit you?
00:18:11,090 --> 00:18:18,730
Or does it at this juncture, as far as planning for surgical procedures or having conversations?
00:18:18,730 --> 00:18:23,250
Because I'm, I'm assuming that you're having different conversations with different peers, especially
00:18:23,250 --> 00:18:29,750
when your group, if it comes to something that needs multiple discussions depending on.
00:18:30,950 --> 00:18:36,310
Dr. Grant Garcia: All right, so we're going down a rabbit hole. So we'll go. That's what I do. No, no, it's great. I love it.
00:18:36,390 --> 00:18:39,390
But we'll go to this topic and then we'll bounce back because I think we're going to miss some
00:18:39,390 --> 00:18:40,630
things that people want to hear about.
00:18:40,630 --> 00:18:43,510
But the idea is guidance, right?
00:18:43,510 --> 00:18:48,630
So like you get a CT scan, which is a scan you guys all know when we look at X rays, but a lot
00:18:48,630 --> 00:18:53,150
of them combine so we can look at bones, and it's really good for guidance of Cutting, like
00:18:53,150 --> 00:18:57,150
bone gutting things or shoulder replacement surgery. Talked about knee replacements.
00:18:57,710 --> 00:19:02,790
So basically now you get the CT scan. You tell the. You tell and.
00:19:02,790 --> 00:19:05,910
Or the CT scan tells you what you're going to do. Right.
00:19:05,910 --> 00:19:07,710
And people were like, well, why would you need to be told?
00:19:07,710 --> 00:19:09,590
Well, sometimes you can't always figure it out.
00:19:09,590 --> 00:19:12,110
Or there's some subtleties so they can use more experience.
00:19:12,190 --> 00:19:17,760
Like, if you're a new surgeon, then you have AI to help you, guide you what to do, and then
00:19:17,760 --> 00:19:19,120
helps with the surgical plan.
00:19:19,360 --> 00:19:21,600
Because sometimes that's the hardest part.
00:19:21,600 --> 00:19:25,120
Like when you start doing osteotomy is like I've talked about before, where you correct the knee.
00:19:25,120 --> 00:19:25,600
Will Sanchez: Yeah.
00:19:25,600 --> 00:19:27,240
Dr. Grant Garcia: It's a lot more complicated than it sounds like.
00:19:27,240 --> 00:19:29,320
The surgery itself is not like the execution.
00:19:29,320 --> 00:19:33,920
If someone always told me what the right surgery to do every time was, my job would be a lot easier. Right.
00:19:34,080 --> 00:19:37,400
The whole purpose of coming to my office and getting this special stuff and me being like, you
00:19:37,400 --> 00:19:41,360
know, even though I do so many of these, I'm not always 100% sure what the right osteotomy is
00:19:41,360 --> 00:19:42,560
until I get the final scan.
00:19:43,130 --> 00:19:47,130
And so for me, and that's like, now I've done this for like seven years, and I've done a ton
00:19:47,130 --> 00:19:50,490
of these and like, super high volume, so it's easier for me because I had the experience.
00:19:50,890 --> 00:19:54,650
But if you're seeing like one or two of these a year, which is what the common person with a
00:19:54,650 --> 00:19:58,010
common surgeon sees, like, how are you supposed to have that experience? Right?
00:19:58,010 --> 00:20:01,090
Like, you can't just ping a friend every time you want to do something and.
00:20:01,090 --> 00:20:02,010
Or you may not feel comfortable.
00:20:02,010 --> 00:20:04,730
I mean, we all know that, you know, surgeons are.
00:20:04,730 --> 00:20:06,330
They ask for help, but not all the time.
00:20:06,490 --> 00:20:08,090
And some they don't know what they don't know.
00:20:08,660 --> 00:20:09,660
And so it would be good.
00:20:09,660 --> 00:20:10,740
It's good to have these programs.
00:20:10,740 --> 00:20:14,380
That's what these CT programs do is they kind of, hey, this is where I recommend. This I recommend.
00:20:14,380 --> 00:20:18,220
But even when you get a CT program now, it's not smart enough to say, hey, listen, surgeon,
00:20:18,220 --> 00:20:20,100
you're not doing the right surgery for this patient.
00:20:20,100 --> 00:20:21,540
You need to do this surgery instead.
00:20:21,940 --> 00:20:24,180
And so that's where we're. That's where head is.
00:20:24,260 --> 00:20:26,180
Those, like those tweeners, right?
00:20:26,180 --> 00:20:30,980
Like the 10%, 20%, that's more complicated. That's when something.
00:20:30,980 --> 00:20:35,620
That's when it basically gets bumped up to the AI and AI starts to help out with guidance here.
00:20:35,960 --> 00:20:39,080
Or when you're doing, like, spine surgeries, like, it's guiding where your Placement is.
00:20:39,080 --> 00:20:42,040
And says, oh, you're off by 2 millimeters. 2 degrees.
00:20:42,120 --> 00:20:47,240
Move it 2 more degrees so you don't damage a nerve, right? So that stuff's like. And we're. We're kind of there.
00:20:47,240 --> 00:20:49,720
We have some guidance, but it's just going to keep getting better.
00:20:49,960 --> 00:20:54,680
Because I think one thing is, like, we keep saying in conjunction, it's version 2.0, right?
00:20:54,680 --> 00:20:59,520
Like, I do dictations in my office, and so I do a dragon.
00:20:59,520 --> 00:21:00,480
You may all know dragon.
00:21:00,480 --> 00:21:02,200
It's old, it's been around for a while.
00:21:02,430 --> 00:21:05,070
So basically I say, I tell it what I want it to say and then it spits it out.
00:21:05,630 --> 00:21:07,710
I can tell you it's not perfect all the time.
00:21:07,950 --> 00:21:11,790
And despite how fast I talk, it, like, cannot keep up even.
00:21:11,790 --> 00:21:13,310
What's supposed to be this AI thing.
00:21:13,630 --> 00:21:14,510
So we're not there yet.
00:21:14,510 --> 00:21:15,830
So that's the same way with the computer.
00:21:15,830 --> 00:21:17,830
Like, we need a faster. We know.
00:21:17,830 --> 00:21:20,510
I was just telling Will, right? We design these backgrounds.
00:21:20,670 --> 00:21:22,750
Takes like four minutes for it, right?
00:21:22,750 --> 00:21:27,110
Like, yeah, you don't want your patient, thankfully, for planning purpose, doesn't matter how
00:21:27,110 --> 00:21:31,000
long it takes, but you don't want your patient, you know, being, like, on the table.
00:21:31,000 --> 00:21:36,600
And your doctor's using AI and AI is stalling out because it's too much bandwidth, right?
00:21:36,600 --> 00:21:37,960
And that's not what you have to worry about.
00:21:38,840 --> 00:21:41,560
Will Sanchez: We're just going to keep that knee open as we try to figure all this out.
00:21:41,800 --> 00:21:45,520
Are these the conversations you're having, which appears like, what's the most interesting?
00:21:45,520 --> 00:21:49,120
And I apologize, I'm kind of going sidetrack. What's the mo?
00:21:49,120 --> 00:21:55,900
Like, the most interesting conversation you've had regarding AI with a peer or peers lately?
00:21:57,260 --> 00:22:01,460
Dr. Grant Garcia: I think it's like, for me, it's like, how? Well, for what.
00:22:01,460 --> 00:22:04,820
For what I could use AI for is, like, the complicated surgeries, right?
00:22:04,820 --> 00:22:06,420
Like, how's it going to plan it for me?
00:22:06,420 --> 00:22:11,460
Or also for me is like, this is the one thing I think AI is really important for is like, how
00:22:11,460 --> 00:22:15,380
can I do all the things that I don't want to spend my time doing, like website design?
00:22:15,380 --> 00:22:18,900
I mean, this sounds bad because it's like, we're not talking about the crazy cool stuff, but,
00:22:18,900 --> 00:22:20,980
like, AI is literally freed me up.
00:22:20,980 --> 00:22:22,460
I mean, everyone that says, like, you have.
00:22:22,460 --> 00:22:26,370
You do too much stuff, like your website, you have your videos, you have your podcast, you do surgeries.
00:22:26,840 --> 00:22:29,280
But, like, I have to do all this, all this with myself, right?
00:22:29,280 --> 00:22:33,760
So now I can, like, have my website designed with my company and then spit out a Lot of information
00:22:33,760 --> 00:22:36,200
with AI and then check it and then send it up.
00:22:36,360 --> 00:22:38,640
Or, like, when we're designing this podcast, right?
00:22:38,640 --> 00:22:42,400
We've had AI help us design this podcast because there's absolutely no way we could do this much research.
00:22:42,400 --> 00:22:49,040
The amount of research that we were able to get from the AI could take literally, like, 25 hours, 30 hours, right?
00:22:49,040 --> 00:22:52,520
Like, we're able to get a lot better content to patients. And then.
00:22:52,520 --> 00:22:56,400
And then when we review it, I'm like, okay, that doesn't seem right. That's not accurate. That's not accurate.
00:22:56,400 --> 00:22:58,440
That's definitely what I was thinking, you know?
00:22:58,440 --> 00:23:01,760
And then, like, even making the images, right, like, this image before would have been a copyright
00:23:01,760 --> 00:23:05,280
infringement, trying to find the right image, right? So it's just.
00:23:05,280 --> 00:23:06,680
It saves us hours of time.
00:23:06,680 --> 00:23:11,280
So now what I do is, instead of stressing about the small things, I only focus on, like, doing
00:23:11,280 --> 00:23:16,720
a good job on surgery, talking to patients, making sure that we do a podcast that's got a ton
00:23:16,720 --> 00:23:20,900
of content in it, and we're able to focus on that rather than been like, I'm just gassed, man.
00:23:20,900 --> 00:23:24,140
You know, we spent 20 hours getting this ready. I'm done.
00:23:24,140 --> 00:23:26,140
Like, I can't even talk about it right now. Like, it's just.
00:23:26,140 --> 00:23:30,580
It's just all my brain is totally scattered, you know, Even, like, designing projects or research
00:23:30,580 --> 00:23:32,780
papers or things like that, it helps with guidance.
00:23:32,780 --> 00:23:35,580
I think of it as, like. Like, if you.
00:23:35,580 --> 00:23:38,820
You get writer's block or something, and it's like, now you don't need to worry about that. Like, your.
00:23:38,820 --> 00:23:40,820
Your skeleton's made, and then you can design it.
00:23:41,300 --> 00:23:43,300
Obviously, it's a concern with some of these companies, right?
00:23:43,300 --> 00:23:46,310
Like, is someone gonna have a whole PowerPoint made by AI?
00:23:46,710 --> 00:23:49,270
But it's not there yet, at least maybe I don't know how to do it.
00:23:50,710 --> 00:23:55,310
But I think the thing is, like, even when you ask it to, like, I want this article, make me
00:23:55,310 --> 00:23:58,230
this article with these citations, it has, like, no idea what it's doing.
00:23:58,230 --> 00:24:01,270
So it basically, like, it does a good job, and then it starts making up citations.
00:24:01,430 --> 00:24:03,110
So you gotta be careful, right?
00:24:03,110 --> 00:24:04,310
Like, what you tell it to do.
00:24:05,270 --> 00:24:07,350
Will Sanchez: Have you seen anything on your end?
00:24:07,350 --> 00:24:09,590
And I know you have kind of.
00:24:10,770 --> 00:24:12,450
This is the surgery that we did.
00:24:12,610 --> 00:24:18,690
This is kind of what I want to see after week one of the surgery, week two, a month, so on and so forth.
00:24:18,690 --> 00:24:26,770
Are you utilizing AI as with part of the rehab now, or you incorporating any of that?
00:24:26,770 --> 00:24:28,850
Or is that something that you know?
00:24:28,850 --> 00:24:32,290
Or you're just kind of like, hey, this is what I normally do with this process.
00:24:32,530 --> 00:24:34,930
So I'm sticking to what I know works best.
00:24:35,820 --> 00:24:38,220
Dr. Grant Garcia: I think we're not there yet, but there are so many wearable devices.
00:24:38,220 --> 00:24:41,100
I mean I think we're going into the path you want to go, which is great.
00:24:41,420 --> 00:24:47,500
So I think that AI we're looking at from an, from a sports standpoint, we're looking at a bunch of things, right? Wearable devices.
00:24:47,500 --> 00:24:50,020
So can we collect data on movement, vital signs?
00:24:50,020 --> 00:24:52,140
I mean we got AI on my wrist, right.
00:24:52,140 --> 00:24:54,140
Like, you know, the Apple watches are all smarter.
00:24:54,460 --> 00:24:56,460
Apple got its huge AI upgrade recently.
00:24:57,100 --> 00:25:04,060
You know, can we detect if someone's, you know, you're sick or you're not feeling well or you're dehydrated or everything else.
00:25:04,060 --> 00:25:09,300
But then from the, where it's really the, the money's at is the professional level, right. Or athletes. Right.
00:25:09,300 --> 00:25:11,940
Because that's where you know, we know these contracts are so expensive.
00:25:11,940 --> 00:25:17,300
And now with the nil, it's like the college players and the pre high school players and everyone
00:25:17,300 --> 00:25:18,820
else is making a bunch of cash.
00:25:19,380 --> 00:25:21,380
So you know, we got to keep them healthy. Right.
00:25:21,380 --> 00:25:24,540
You know, like the, the, the player has the investment, right?
00:25:24,540 --> 00:25:29,940
Because now it's really nice too because it's not just the schools looking at your best interests, it's the player.
00:25:29,940 --> 00:25:32,700
They're like, I want to stay healthy because I've got a five million dollar contract.
00:25:32,700 --> 00:25:35,500
I'm a freshman in high school or freshman in college.
00:25:36,860 --> 00:25:39,740
So yeah, I mean we want the, the wearable devices is huge.
00:25:39,980 --> 00:25:43,140
And then there's like, there's different things like personalized rehab program, right.
00:25:43,140 --> 00:25:47,620
Like so you know, I tell it, you tell the patient tells it what surgery it had and then it uses
00:25:47,620 --> 00:25:51,300
like the best doctors around the country, if it somehow finds them and then puts together a
00:25:51,300 --> 00:25:55,710
PT protocol for you and then it can make adjustments as needed. Right. So that's really good.
00:25:55,710 --> 00:25:57,310
And like the real time feedback too, right?
00:25:57,310 --> 00:26:00,430
Like you're doing something like this hurts and the knee and it can adapt it.
00:26:00,430 --> 00:26:06,070
Now we're not there yet because again the problem with all of this stuff is it's super sexy.
00:26:06,070 --> 00:26:11,190
But in the, in non professional or college sports it's very hard to do this because it's expensive.
00:26:11,350 --> 00:26:11,750
Will Sanchez: Yeah.
00:26:11,750 --> 00:26:17,350
Dr. Grant Garcia: Right. So insurance and so there's, so there's, there's, we have rehab machines like we've talked
00:26:17,350 --> 00:26:20,230
about the Rebliss and other things, but you can do remote monitoring.
00:26:21,120 --> 00:26:23,440
Insurance does not pay very much for that.
00:26:23,440 --> 00:26:26,440
It's a very, very low reimbursement cost.
00:26:26,440 --> 00:26:30,080
So if you have a machine that's designed not saying that that machine particularly, but if you
00:26:30,080 --> 00:26:34,480
have a machine and they're like, it's a thousand dollars for that machine program. Right.
00:26:34,480 --> 00:26:39,360
Or 500 bucks or something, like the insurance will pay like $35.
00:26:39,680 --> 00:26:45,040
And so like there's just no way that with insurance that these, these fancy devices are going
00:26:45,040 --> 00:26:48,170
to be paid for because you need to show that they're a huge difference.
00:26:48,170 --> 00:26:51,450
And even at that, we all know, I mean, I hate to say I don't want to go off on insurance companies
00:26:51,450 --> 00:26:53,730
on this thing, but like, look at the news.
00:26:54,370 --> 00:26:56,130
Less care is more for them.
00:26:56,450 --> 00:27:01,730
So why would they pay for something that's not going to be hugely beneficial unless there's a huge uproar?
00:27:01,730 --> 00:27:07,410
But rehab is like, this is, is amazing and it's so important for patients, but I feel like it's
00:27:07,410 --> 00:27:12,890
really neglected, it's very neglected by the insurance companies, this personalized idea.
00:27:12,890 --> 00:27:17,010
Like they, that's not the way we're going with insurance.
00:27:17,010 --> 00:27:21,450
And so there may be an uproar, but patients are willing to pay for it on their own, which I think is reasonable.
00:27:21,450 --> 00:27:24,370
And I think that's, that's, that's unfortunately the way we have to go.
00:27:25,250 --> 00:27:30,050
Will Sanchez: Yeah, it was interesting when you know, we first started talking about the show and you know,
00:27:30,050 --> 00:27:35,850
we, we kind of went back and forth and I sent you some stuff on the smart console system and
00:27:35,850 --> 00:27:41,000
there's a bunch of companies that are using that, you know, and they talk about injury prevention
00:27:41,000 --> 00:27:48,480
and you know, subtle movements, you know, symmetries and compensations and you know, real world data collection.
00:27:48,560 --> 00:27:54,879
I my long winded version of getting to a point of the more companies that come out with AI tech,
00:27:54,879 --> 00:28:00,840
whether it's, you know, smart insole systems or wearable shorts and shirts.
00:28:00,840 --> 00:28:07,180
We, I believe Gabriel Landscott, which we talked about with the hockey player that had the injury,
00:28:07,340 --> 00:28:14,380
he was wearing that tech also so his doctors can monitor him and hopefully we get a chance to talk to Dr.
00:28:14,380 --> 00:28:19,180
Cole and we can have this conversation again when it comes to smart tech and how that's being
00:28:19,180 --> 00:28:26,300
utilized for rehab as companies develop and there's more of them that are hitting the market,
00:28:26,460 --> 00:28:33,210
hopefully the price drives down and not so much athletes that will have access to this, but
00:28:33,210 --> 00:28:40,730
you know, mom and pop and you know, Joe and Jill can also now maybe afford this and we see an
00:28:41,050 --> 00:28:45,650
uptick in the rehab and monitoring and what that's going to be like.
00:28:45,650 --> 00:28:46,969
So to me that's exciting.
00:28:46,969 --> 00:28:54,130
What are your thoughts on that excitement level and where AI can Advance the future when it
00:28:54,130 --> 00:28:57,370
comes to rehabbing and being beneficial to your patients.
00:28:58,440 --> 00:29:02,800
Dr. Grant Garcia: Yeah, I mean, I think when the, when the, we keep that slide originally implementation costs.
00:29:02,800 --> 00:29:08,000
So when implementation costs come down, then it's either affordable for the patients or the
00:29:08,000 --> 00:29:12,200
doctor's office or which actually is gonna be more important is the rehab office.
00:29:12,200 --> 00:29:14,680
We already talked about this. So perfect example.
00:29:14,840 --> 00:29:18,200
Dylan Newcomer, physical therapy for players. Right.
00:29:18,680 --> 00:29:21,080
They do some insurance and some cash options.
00:29:21,080 --> 00:29:23,790
So the cash options are obviously the super fancy stuff you saw.
00:29:23,860 --> 00:29:25,700
And there's just no way insurance would cover that level.
00:29:26,100 --> 00:29:31,020
And that's okay though, because that's the players usually, and people want to pay for it because they want extra.
00:29:31,020 --> 00:29:35,140
That's the way that works in the United States and that's just the way it is here, unfortunately,
00:29:35,140 --> 00:29:36,740
or fortunately, whatever you want to say.
00:29:37,460 --> 00:29:44,260
But that when that gets cheaper, then more people want to be involved and more people are not left out. Right.
00:29:44,420 --> 00:29:46,900
But like, health care is also really expensive.
00:29:46,980 --> 00:29:49,220
Like if you don't have insurance. Right.
00:29:49,220 --> 00:29:50,500
And you just pay per meal.
00:29:50,500 --> 00:29:54,000
Most healthy people actually save money not having health care insurance.
00:29:54,000 --> 00:30:00,280
It's horrible to say that, but like when your premiums are $10,000 a year or $15,000 a year,
00:30:00,280 --> 00:30:04,000
there's no way a young person is going to spend that much on health care unless they have a major accident.
00:30:04,080 --> 00:30:04,520
Will Sanchez: Yeah.
00:30:04,520 --> 00:30:08,840
Dr. Grant Garcia: So like these patients, and a lot of them work for high level companies where they're paying
00:30:08,840 --> 00:30:09,920
very little for their health care.
00:30:09,920 --> 00:30:12,960
So they're, they have extra expenditures they want to put towards other things.
00:30:13,200 --> 00:30:18,520
I mean, we've seen these, these nutrition, we've seen these guys, you know, live forever type of situations.
00:30:18,520 --> 00:30:23,810
The longevity thing, it's all about that, well, this AI is going to help people get back better.
00:30:24,610 --> 00:30:28,130
And this, this rehab monitoring, this, the kinematic analysis is the pre.
00:30:28,450 --> 00:30:29,530
But like, can we reduce.
00:30:29,530 --> 00:30:34,130
You know, there's a, there's a machine learning for these athletes to find out who's higher risk.
00:30:34,130 --> 00:30:38,850
I mean, I had two patients today or two patients today and a few this week.
00:30:39,490 --> 00:30:40,610
The moms came up to me.
00:30:40,610 --> 00:30:43,890
Obviously there's, there's a kid in there with an ACL tear. Right. And they need surgery.
00:30:44,210 --> 00:30:46,130
One of them had actually the tore the other knee.
00:30:46,130 --> 00:30:47,690
I did surgery on one and they tore the other one.
00:30:47,690 --> 00:30:49,970
It's very, very frustrating and sad to see that.
00:30:50,410 --> 00:30:51,850
And they ask, is there anything we can do?
00:30:52,090 --> 00:30:54,050
And the answer is, yeah, you can do all these different things.
00:30:54,050 --> 00:30:55,890
We can try to do it, it can try to reduce it.
00:30:55,890 --> 00:31:00,890
We know females that are higher risk, but really like, can we do, you know, can we have an can
00:31:00,890 --> 00:31:05,930
like the high school or, you know, the high school coach have this kinematic analysis at the
00:31:05,930 --> 00:31:09,970
beginning of the year for every kid, especially girls and females in soccer, and then say, okay,
00:31:09,970 --> 00:31:14,730
these three girls are at higher risk because of their kinematic analysis and, or they're at
00:31:14,730 --> 00:31:15,870
higher risk of ACL tears.
00:31:17,060 --> 00:31:19,420
And then from that, say, those.
00:31:19,420 --> 00:31:23,260
Pick those three girls and say, hey, listen, you need to work on this, this and this to try to reduce it.
00:31:23,260 --> 00:31:27,060
I think we can get it down, but it's just something they have to be continuing to work on.
00:31:27,620 --> 00:31:31,460
Will Sanchez: Yeah. And I think you brought up an important part of it cost.
00:31:31,460 --> 00:31:37,380
I mean, you know, we know how high school sports are and we know certain programs are going
00:31:37,380 --> 00:31:38,820
to be able to afford certain things.
00:31:38,820 --> 00:31:43,950
And you have other programs that can barely get cleats for kids. So that be.
00:31:43,950 --> 00:31:45,110
That plays a big part.
00:31:45,190 --> 00:31:53,310
So hopefully, as you know, the market gets flooded and there's more affordable, available options for them. You know.
00:31:53,310 --> 00:31:58,310
Any concerns or have you heard any, any feedback from patients that talk about.
00:31:58,390 --> 00:32:00,470
Well, I'm concerned about privacy.
00:32:00,790 --> 00:32:03,030
I personally think it's kind of.
00:32:03,030 --> 00:32:06,910
It doesn't make any sense to me since I feel like they have all our information anyway.
00:32:06,910 --> 00:32:10,930
If you have a computer, you have a, you have a smartphone, they have all this stuff anyway.
00:32:11,090 --> 00:32:18,130
But have you had any of that feedback from, from patients or peers when it comes to AI and that
00:32:18,130 --> 00:32:20,530
data information that's being shared?
00:32:21,650 --> 00:32:26,610
Dr. Grant Garcia: I haven't. Maybe after this podcast we will. I brought it up. So I haven't.
00:32:26,610 --> 00:32:28,930
I think, well, I mean, it's. I think it's good.
00:32:28,930 --> 00:32:32,610
My patients trust me, that I'm doing the right stuff and making sure that if I'm implementing
00:32:32,610 --> 00:32:38,390
a tool in the office or post surgical or pre surgical, that I vetted it. It's HIPAA compliant. Yeah. Yeah.
00:32:40,070 --> 00:32:41,430
But I haven't come up.
00:32:41,430 --> 00:32:45,430
But again, you know, this is the same people that, like, these are generally younger patients.
00:32:45,590 --> 00:32:51,630
They're on Facebook every day or Instagram getting all of their data tracked, and all of a sudden, like, they moved.
00:32:51,630 --> 00:32:55,710
You know, it's like, I think we've all become kind of mute to it.
00:32:55,710 --> 00:32:59,150
There are certain people that are like, you know, they'll do whatever it takes and not have their data.
00:32:59,150 --> 00:33:00,790
They want privacy, privacy, privacy.
00:33:01,030 --> 00:33:05,790
But to be honest with you, I think we're so inundated with it and so involved in our lives that
00:33:05,790 --> 00:33:08,790
we kind of just gave up our privacy, which is sad.
00:33:09,030 --> 00:33:15,070
Will Sanchez: My daily spam just becomes, you know, delete Report junk and move on. Like, it's just, it's.
00:33:15,070 --> 00:33:16,470
Dr. Grant Garcia: I mean, medical stuff is scary.
00:33:17,270 --> 00:33:21,270
A lot more private than like, okay, knowing that I like to watch cooking channel videos.
00:33:21,750 --> 00:33:23,990
But you know, nonetheless, it's.
00:33:24,070 --> 00:33:26,710
I think people, people are, they're.
00:33:26,710 --> 00:33:29,430
People are more open nowadays too, which is good and bad. Right?
00:33:29,730 --> 00:33:32,570
You know, like, how many times I got to.
00:33:32,570 --> 00:33:34,090
I work on this myself, I'm not good at this.
00:33:34,090 --> 00:33:38,930
But a lot of these people, you know, I see like these high level celebrities are like, I just had a massive surgery. Wish me luck.
00:33:38,930 --> 00:33:41,690
You know, like I, I tore like everything in my knee.
00:33:41,690 --> 00:33:42,530
I'm going to get surgery.
00:33:42,530 --> 00:33:48,330
I got, you know, I hadn't recovered from cancer. Look at me, right? It's all great. It's awesome. But like there. People don't.
00:33:48,330 --> 00:33:50,090
The privacy thing is kind of gone nowadays.
00:33:50,090 --> 00:33:54,170
I feel like, I feel like it's obviously like if you're these influencers, right, they get hurt
00:33:54,170 --> 00:33:57,300
and they use it as like the next step to get up to whatever.
00:33:57,300 --> 00:34:00,940
I don't think it's obviously like a, a bad thing that they're telling all.
00:34:00,940 --> 00:34:04,220
I think it's really great that they have the guts to go over there and talk about all their
00:34:04,220 --> 00:34:09,340
medical conditions and feel really good because not all of us do that, but I think or lay out
00:34:09,340 --> 00:34:11,460
all their laundry and their family and things like that.
00:34:11,460 --> 00:34:16,220
But at the same point it's, I don't, I don't think it's as different day and age. Right?
00:34:16,220 --> 00:34:17,580
People used to be a lot more conservative.
00:34:17,580 --> 00:34:19,380
They used to be a lot more quiet about their stuff.
00:34:19,460 --> 00:34:23,260
I mean, I, I've seen like nine surgeon speeds where they're just like, they're literally in
00:34:23,260 --> 00:34:26,340
bed, like about to die and they're like, look at me, I'm about to get surgery.
00:34:26,780 --> 00:34:30,460
And they're like, they're like, they, it's, it's just, it's just interesting.
00:34:30,460 --> 00:34:31,900
It's totally different than what they used to do.
00:34:32,220 --> 00:34:34,460
Will Sanchez: Yeah, I'm more concerned about the cooking shows.
00:34:34,460 --> 00:34:37,500
Let's go back to the cooking shows that you're apparently watching, man.
00:34:37,580 --> 00:34:38,780
What, what should go to?
00:34:38,780 --> 00:34:39,740
Dr. Grant Garcia: Cooking show here.
00:34:42,619 --> 00:34:46,100
Shout out. This is my new cooking thing. My partner, Dr.
00:34:46,100 --> 00:34:52,859
Wayne Weil, Seattle hand doc, is a tick tock monster for cooking.
00:34:53,019 --> 00:34:57,699
And he and his wife, he has a cool kitchen setup where he has the, like, he has like the, the
00:34:57,699 --> 00:35:00,099
kitchen on the island so you can put a phone right in front of it.
00:35:00,099 --> 00:35:01,339
Like they're, that's really hard to get.
00:35:01,339 --> 00:35:02,779
Like my kitchen doesn't have like that.
00:35:02,779 --> 00:35:03,899
And like it's very hard.
00:35:04,139 --> 00:35:10,619
And he and his wife Nancy, they do it and fast forward and they cook and they have so many followers.
00:35:10,699 --> 00:35:14,059
It's so funny too because it's linked to his account for orthopedics.
00:35:14,059 --> 00:35:15,819
So he has like no orthopedics on there.
00:35:15,899 --> 00:35:20,380
He just eats and makes food and he is killing it. It is awesome.
00:35:20,700 --> 00:35:25,660
So we were going to have them on hopefully in the summer or a little bit later to talk about this cooking experience.
00:35:25,660 --> 00:35:27,420
So that's the only really cooking thing I watch.
00:35:27,420 --> 00:35:31,620
But I think because I'm friends with them and because I look at it, I think I get other cooking
00:35:31,620 --> 00:35:33,100
stuff that I'm not interested in.
00:35:33,660 --> 00:35:35,620
So, you know, I'm a big fitness man.
00:35:35,620 --> 00:35:41,900
I have like the craziest workouts ever showing up on my stream and that is like the number one thing.
00:35:41,900 --> 00:35:44,300
It's travel, crazy travel stuff.
00:35:44,790 --> 00:35:48,150
And the workouts, like workout like exercises.
00:35:48,150 --> 00:35:49,910
There's like, there's no humanly way I could do that.
00:35:49,910 --> 00:35:52,070
Like, I'm gonna rip every part of my body apart. Yeah. Yeah.
00:35:52,070 --> 00:35:53,070
Every once in a while I get one.
00:35:53,070 --> 00:35:54,230
I'm like, I'm gonna try that one.
00:35:54,950 --> 00:35:59,430
Will Sanchez: Oh, man. Dr. Weil, by the way, back surgeon. Surgeon.
00:35:59,510 --> 00:36:02,710
Oh, but tick tock influencer first and foremost.
00:36:03,430 --> 00:36:03,910
Dr. Grant Garcia: Yes.
00:36:04,790 --> 00:36:10,030
Will Sanchez: That's hysterical. Real quick. I, like I said, we, we kind of go off the sidetrack, man.
00:36:10,030 --> 00:36:11,830
What's the, what's the go to workout right now?
00:36:11,830 --> 00:36:16,390
What, what's the one that you're like, this is my go to. I, I'm loving it. I know, I know.
00:36:16,390 --> 00:36:17,550
We talked about this before.
00:36:17,870 --> 00:36:20,110
You like the hit workouts, right?
00:36:20,110 --> 00:36:21,350
You're a big travel guy.
00:36:21,350 --> 00:36:24,710
Your itinerary is you, you should be posting itinerary.
00:36:24,710 --> 00:36:26,190
We had this conversation last time.
00:36:26,190 --> 00:36:27,110
You haven't done it yet.
00:36:27,110 --> 00:36:30,190
Dr. Grant Garcia: I know. I'm not ready to crack yet.
00:36:30,350 --> 00:36:35,870
Will Sanchez: Let's throw it on sports.talk.com we're going to drive all the travelers there and then they'll,
00:36:35,870 --> 00:36:37,950
by the way, they'll see the shows as well.
00:36:38,270 --> 00:36:41,800
But what's the, what's the workout right now that you're loving?
00:36:42,840 --> 00:36:46,360
Dr. Grant Garcia: I mean, I just, I'm all about the hit, right?
00:36:46,360 --> 00:36:51,480
Like high intensity burpees, box jumps, you know.
00:36:51,560 --> 00:36:55,120
But again, I don't want to get hurt now because I unfortunately have to take care of all those
00:36:55,120 --> 00:37:01,960
people that are my age doing hit and like coming in with like the meniscus tear or the ACL tear or whatever.
00:37:01,960 --> 00:37:06,800
I mean, the CrossFit injury rate's like 78%, right? Like, CrossFit's great.
00:37:06,800 --> 00:37:08,840
For Ortho, not good for the body.
00:37:09,160 --> 00:37:11,080
Everyone who does it, they all look incredible.
00:37:11,480 --> 00:37:13,880
But it's, it's, it's a, it's a scary thing.
00:37:13,880 --> 00:37:15,400
But I mean I just.
00:37:15,880 --> 00:37:17,080
For me it's just routine.
00:37:17,080 --> 00:37:22,480
It's just continue to do it day in and day out and a little bit addicted to it. So obviously that's a.
00:37:22,480 --> 00:37:23,240
But it's a good thing.
00:37:23,240 --> 00:37:26,560
It keeps me sane and hopefully it keeps me.
00:37:26,560 --> 00:37:27,400
The thing is, you got.
00:37:27,880 --> 00:37:28,880
I think we should bring this up.
00:37:28,880 --> 00:37:30,360
It's actually we should have this talk, right?
00:37:30,360 --> 00:37:34,130
This is like surgery is a little bit like athletics.
00:37:34,450 --> 00:37:42,650
Like my surgery days are so much like pumping, pulling, pushing stuff that like a lot injury rate.
00:37:42,650 --> 00:37:46,010
Orthopedics is probably one of the highest of any of the surgeries. Right.
00:37:46,010 --> 00:37:52,730
Like I'm leaning back, cranking my back, turning it sideways, lifting a 250 pound patient, lifting
00:37:52,730 --> 00:37:56,050
a high level athlete, like six, seven leg. Right.
00:37:56,050 --> 00:37:58,490
Like I'm doing that during the surgery. Right.
00:37:58,490 --> 00:38:00,210
Like there's assistance, but I'm doing it.
00:38:00,320 --> 00:38:00,680
Will Sanchez: You gotta.
00:38:00,680 --> 00:38:04,240
Dr. Grant Garcia: When I was injured, it was a nightmare because it's so hard to do.
00:38:04,480 --> 00:38:08,040
So like I've had to stay fit as possible. Right. And you get exhausted.
00:38:08,040 --> 00:38:12,880
I mean there's some older surgeons that you can hear them like literally like huffing and puffing during the procedures.
00:38:13,120 --> 00:38:15,680
And we're standing the whole time running around full speed.
00:38:15,920 --> 00:38:20,240
And also that's not to mention the stress level of actually taking care of the person under
00:38:20,240 --> 00:38:22,320
anesthesia and doing the complicated procedure.
00:38:22,640 --> 00:38:27,820
So most orthopedic surgeons, they make a joke because the orthos are always like gym jocks, right?
00:38:27,820 --> 00:38:29,340
They're in the gym, they're working out.
00:38:29,340 --> 00:38:29,740
Will Sanchez: Yeah.
00:38:29,740 --> 00:38:32,380
Dr. Grant Garcia: Like that's the medicine stereotype of orthopedics.
00:38:32,620 --> 00:38:38,300
But this, the part of it is you actually need to be that fit to be able to do the surgeries
00:38:38,300 --> 00:38:42,860
effectively because it's because of the grind you're doing all the time for the most part.
00:38:43,020 --> 00:38:44,220
So like I love this.
00:38:48,060 --> 00:38:52,700
Will Sanchez: Spartan race. This is like orthopedic surgeon, spartan race.
00:38:52,780 --> 00:38:58,410
You jump over the, the operating table, you know, you do a couple burpees, you jump in.
00:38:58,410 --> 00:39:03,530
Dr. Grant Garcia: I've actually been caught. I've been caught in the operating room once I fell over because someone
00:39:03,530 --> 00:39:06,770
had, someone had took the steps to the sitting still away from me.
00:39:06,770 --> 00:39:12,570
When I sat down and didn't see it and my tech grabbed me and caught me, it was the most incredible thing I've ever had.
00:39:12,810 --> 00:39:17,450
It was, it was weird for like 10 seconds, but then it worked out. It was great.
00:39:19,290 --> 00:39:20,890
Will Sanchez: This is the new, the new race.
00:39:20,890 --> 00:39:22,530
We're going to be on espn.
00:39:22,530 --> 00:39:25,630
The Ocho with his new obstacle course.
00:39:26,110 --> 00:39:28,830
Dr. Grant Garcia: Right next to this. The squirrel in the water, the jet, the.
00:39:28,830 --> 00:39:30,750
In the little water skis.
00:39:31,790 --> 00:39:32,710
Will Sanchez: That's hysterical.
00:39:32,710 --> 00:39:35,950
Dr. Grant Garcia: All right, dude, let's, let's digress back in. So let's go.
00:39:36,030 --> 00:39:37,950
So we talked a little bit about sports, right?
00:39:38,270 --> 00:39:41,310
And then for joints, you have these patient specific instrumentation.
00:39:41,550 --> 00:39:43,870
So you have patient comes in, they get it.
00:39:43,870 --> 00:39:47,550
The robotic machine, or the machine calculates it and says, this is exactly what you need.
00:39:47,710 --> 00:39:52,880
Now, obviously the problem here is that like, patient specific is more expensive.
00:39:53,280 --> 00:39:55,280
So we need to find a way to get that cost down.
00:39:55,280 --> 00:39:59,520
Can they 3D print those for the same price as a regular implant? Right.
00:39:59,520 --> 00:40:02,040
And we'll get there eventually. Robotic surgery.
00:40:02,040 --> 00:40:05,880
This is the, this is the number one thing people want to talk about robotic surgeries.
00:40:05,880 --> 00:40:12,960
They're worried that like, you get a robot done, it does your surgery, there's no actual surgeon there right now.
00:40:13,760 --> 00:40:17,920
The way it works is again, there's these rare cases and there's some of the general surgeries
00:40:17,920 --> 00:40:21,440
that are robotics and they've heard about remote surgeries for like a good surgeon that does
00:40:21,440 --> 00:40:22,560
the surgery in like another country.
00:40:22,560 --> 00:40:27,720
And they do it for people with underserved or whatever that's there, but we're not there yet.
00:40:27,960 --> 00:40:32,280
But like in joint replacement, there's robots that help guide the surgeon.
00:40:32,280 --> 00:40:35,840
Either newer surgeons, which is you always want to have obviously the highest level of skill
00:40:35,840 --> 00:40:39,120
when you're doing this, but also helps with alignment and things.
00:40:39,120 --> 00:40:41,710
There's certain things just hard to calculate on the fly. Right.
00:40:41,710 --> 00:40:44,990
Like you can do everything you want there, but when you get in there, it's never always the same. Right.
00:40:44,990 --> 00:40:47,950
Like as soon as you always say, you know, yes, the mechanic, like, what are you going to do in my car?
00:40:47,950 --> 00:40:49,350
They're like, well, I think I'm gonna do this, this, this.
00:40:49,350 --> 00:40:50,790
But we'll figure it out when we get in there. Right?
00:40:50,790 --> 00:40:54,590
Like, there is some things you have to figure out when you're in there and you can't anticipate.
00:40:54,750 --> 00:40:56,790
That's why our job is what it is.
00:40:56,790 --> 00:40:58,270
And that's why our job is a little bit stressful.
00:40:58,270 --> 00:41:06,230
Because I'll go into, you know, I did, I did 15 or 12 surgeries last week, and 10 of them were
00:41:06,230 --> 00:41:07,500
exactly what I thought they were going to be.
00:41:07,730 --> 00:41:11,330
And two threw me a curveball regardless of preparation.
00:41:11,730 --> 00:41:13,970
And two of them were the same surgery they'd done the same week.
00:41:14,530 --> 00:41:15,610
So you just never know.
00:41:15,610 --> 00:41:16,690
You've got to be Prepared.
00:41:16,930 --> 00:41:22,290
And so this robotic surgery is going to help to hopefully eliminate some of that and take away the stress.
00:41:22,290 --> 00:41:23,890
But also as a stress factor, right?
00:41:23,890 --> 00:41:30,050
Like, let's say you're doing a replacement, and all of a sudden you start doing it and you're like this. You can't.
00:41:30,050 --> 00:41:31,570
You've had a really rough day, right?
00:41:31,570 --> 00:41:33,750
You're doing your best, but you're tired, right?
00:41:33,750 --> 00:41:39,310
It's the end of the day, your last surgery, and no matter who you are, you're a little gassed, right?
00:41:39,310 --> 00:41:42,870
So you're trying to get your best to do the surgery right, and you're having trouble calculating.
00:41:42,870 --> 00:41:44,670
You can't get the exact move fit. Right?
00:41:44,670 --> 00:41:46,550
But we're all normal human humans, right?
00:41:46,550 --> 00:41:47,790
And we have to deal with a lot of stress.
00:41:48,350 --> 00:41:51,550
So the more frustrated you get, the less you start thinking. Right.
00:41:51,550 --> 00:41:54,910
It's not like you're going to have an error during the surgery, but it's going to take you a
00:41:54,910 --> 00:41:55,950
little longer than it should.
00:41:56,270 --> 00:41:59,470
So having these robots to be like, listen, I have no emotion.
00:41:59,470 --> 00:42:01,440
I'm going to calculate this for you. You're.
00:42:01,440 --> 00:42:03,200
I can't get tired because I'm in a robot.
00:42:03,360 --> 00:42:05,680
So they're going to be like, okay, it's 13.4 degrees.
00:42:05,680 --> 00:42:07,760
And I'm like, oh, thanks, I don't have to do that math.
00:42:07,760 --> 00:42:09,920
And they're like, you know what? This is not working.
00:42:10,160 --> 00:42:12,600
When I put the two implants in, it feels tighter.
00:42:12,600 --> 00:42:15,000
And you're like, you know, you're kind of already gas from the day.
00:42:15,000 --> 00:42:18,000
And it's like, okay, drop it down 1.25 degrees.
00:42:18,000 --> 00:42:19,280
Okay, so you can go do that.
00:42:19,360 --> 00:42:20,440
So that's what I'm talking about.
00:42:20,440 --> 00:42:23,560
So like a sensor or these are body things. Where do you put.
00:42:23,560 --> 00:42:24,320
Where do you put it?
00:42:25,040 --> 00:42:26,880
Yeah, so it can do those things.
00:42:26,880 --> 00:42:30,320
Like, we have monitors with the pictures up there, so I can calculate in my head.
00:42:30,320 --> 00:42:33,120
But this robot will be like, no, move your hand to the right a little bit.
00:42:33,120 --> 00:42:36,400
Move your hand to the left for the really precise part, Right?
00:42:36,400 --> 00:42:40,640
But then, of course, you know, if the robot's reaming and something starts bleeding, the robot's
00:42:40,640 --> 00:42:42,200
not going to know what to do. Right?
00:42:42,200 --> 00:42:43,920
So you do all that. That's the.
00:42:43,920 --> 00:42:47,200
Then the surgeon steps in, so it's an assistant to help him.
00:42:47,200 --> 00:42:49,920
And also makes your job a lot less stressful, right? If you have it.
00:42:49,920 --> 00:42:54,730
I do a lot of planning ahead of time for some of my big surgeries because it makes it way less
00:42:54,730 --> 00:42:56,690
stressful or it's a lot faster. Right.
00:42:56,690 --> 00:42:57,730
Like, because I don't have to.
00:42:57,970 --> 00:43:04,530
These patient specific instrumentation that I use for my osteotomies, it's cut down like 25 minutes of my surgery.
00:43:05,170 --> 00:43:08,090
So I put it on there, I throw the pins in, I check it.
00:43:08,090 --> 00:43:09,330
If it looks good, I'm done.
00:43:09,330 --> 00:43:10,810
Like it's already been done for me.
00:43:10,810 --> 00:43:15,890
All the hard, all the like, okay, check X ray, check less radiation. All that's done.
00:43:16,130 --> 00:43:21,410
And so now we, you can get a surgery in half the time, which means less anesthesia, it means
00:43:21,970 --> 00:43:24,850
less blood loss, Everything's better for the patient.
00:43:24,850 --> 00:43:28,970
More surgery, as long as it's being used more.
00:43:28,970 --> 00:43:32,210
And then for, you know, obviously you can do more surgeries and all those other things are important,
00:43:32,210 --> 00:43:35,970
but the surgeon is also less stress, which makes your whole surgery go better.
00:43:36,130 --> 00:43:39,690
I mean it's, it's a win win for everybody, honestly.
00:43:39,690 --> 00:43:40,930
The number one thing is getting cost.
00:43:41,170 --> 00:43:42,930
Will Sanchez: I like this. I could see it in my head.
00:43:43,010 --> 00:43:48,400
So you, you kind of put on this, maybe even a helmet or like these meta goggles with a microphone
00:43:48,400 --> 00:43:51,680
and say, I'm now cutting this part and I'm doing this.
00:43:51,680 --> 00:43:53,640
And it's talking to you as well.
00:43:53,640 --> 00:43:57,120
It's like, don't you know, it's 1.2 millimeters and this is that.
00:43:57,120 --> 00:44:00,400
And then you're talking, you're talking through it.
00:44:00,400 --> 00:44:02,040
So everyone in the operating room can hear.
00:44:02,040 --> 00:44:06,000
But also the AI is hearing and is reminding you of the steps.
00:44:06,000 --> 00:44:12,680
And then you're having this imaging with the goggles to see what you're viewing and assisting you along the way.
00:44:13,810 --> 00:44:16,170
Dr. Grant Garcia: Yeah, you know, what's that, what was that movie with Jennifer Lopez just came.
00:44:16,170 --> 00:44:19,810
I was like maybe a year old down the Avatar movie where you were like, they were in the machine
00:44:19,810 --> 00:44:20,970
and the machine synced with you.
00:44:20,970 --> 00:44:22,610
It's like the neural link. Yeah, yeah.
00:44:22,610 --> 00:44:26,250
Like that's kind of like, that's kind of the future where we're going with this. Right?
00:44:26,250 --> 00:44:30,210
Like you'll come in like there's already a, there's a new company that's coming out, has ac.
00:44:30,450 --> 00:44:32,450
It can guide where you put your ACL tunnels.
00:44:32,450 --> 00:44:35,490
So it's for, it's for complex surgeries.
00:44:35,810 --> 00:44:38,530
Will Sanchez: Are we talking 10 years, two years?
00:44:38,930 --> 00:44:40,530
Dr. Grant Garcia: I mean, AI avatar thing?
00:44:40,530 --> 00:44:43,210
We're probably longer away from that, but.
00:44:43,210 --> 00:44:49,290
Will Sanchez: No, but I mean something kind of like that, that first prototype saying this is the first one.
00:44:49,290 --> 00:44:52,850
Like this one's been approved and you're kind of going through it as it advanced.
00:44:52,850 --> 00:44:57,210
Dr. Grant Garcia: I mean, we have, we have like, we have, we have something that's similar to it.
00:44:57,210 --> 00:45:00,570
So we're getting there again. It's just cost, man.
00:45:00,570 --> 00:45:04,170
It's super expensive to get this and then you got to get it FDA approved and then you got to
00:45:04,170 --> 00:45:08,250
get surgeons to buy on and then you need to have these, you know, you have all these hospital
00:45:08,250 --> 00:45:10,120
systems that are cutting costs, right?
00:45:10,120 --> 00:45:10,920
They don't want to pay.
00:45:11,000 --> 00:45:13,640
You know, these spine surgeries are very expensive, right?
00:45:13,640 --> 00:45:17,480
They're good revenue streams, but they're very expensive. We know this.
00:45:18,760 --> 00:45:24,000
So these robotic navigation machines are extreme, like multiple millions of dollars, right?
00:45:24,000 --> 00:45:26,440
And so some hospitals don't want to pay for it.
00:45:26,520 --> 00:45:28,000
So they're like, no, you can't have it.
00:45:28,000 --> 00:45:29,240
So the patient doesn't get it.
00:45:29,240 --> 00:45:31,080
They've got to go find someone that's willing to do it.
00:45:31,320 --> 00:45:35,720
You know, for small surgery centers, we have a robot because we have multiple surgeons that do the same thing.
00:45:36,060 --> 00:45:38,460
But it's all part of a cost negotiation with these companies.
00:45:38,940 --> 00:45:43,580
So it's a, that the cost is actually, unfortunately is the number one hindrance for this.
00:45:43,820 --> 00:45:49,420
But as we've already seen with technology, right, like flat screen TVs were thousands of dollars years ago.
00:45:50,060 --> 00:45:51,260
Now it's like dirt cheap.
00:45:51,260 --> 00:45:57,540
Like, like if I break some, it's like I'm just going to, I'm just going to buy a new one, right? Like it doesn't matter.
00:45:57,540 --> 00:45:59,020
Like it's not, they're not very expensive.
00:45:59,340 --> 00:46:00,700
Will Sanchez: So it's hysterical.
00:46:04,390 --> 00:46:10,230
I had an HDMI TV, weighed 200 pounds, like it was ridiculous.
00:46:10,230 --> 00:46:13,590
And it was the newer one, you know, for the time.
00:46:13,590 --> 00:46:18,510
And I was just praying that it wouldn't fall over and crush my child because it was so heavy.
00:46:18,510 --> 00:46:23,830
And now These things are 90 inches and they weigh 6 pounds. It's absolutely unbelievable.
00:46:24,950 --> 00:46:26,550
Dr. Grant Garcia: So, so let's go, let's go to.
00:46:26,630 --> 00:46:28,510
I mean, we can talk about the radiology, but let's go to.
00:46:28,510 --> 00:46:32,320
Like people were asking, you asked me before, like in my, in my office.
00:46:32,320 --> 00:46:33,840
How do I, how would you notice it?
00:46:33,840 --> 00:46:36,600
So I think there's different things, right?
00:46:36,600 --> 00:46:38,800
There's, there's work, so there, so there's bigger hospitals.
00:46:38,800 --> 00:46:39,560
I don't work in hospital.
00:46:39,560 --> 00:46:42,680
Mostly I consult for hospitals, but I don't work in the hospital directly.
00:46:42,680 --> 00:46:45,200
If you come to my practice, it's private practice, very niche.
00:46:45,840 --> 00:46:49,640
But if you work in a hospital, there's obviously the prioritize of intermoral findings, right?
00:46:49,640 --> 00:46:52,400
Like you come to the er, everyone screams that everything hurts, right?
00:46:52,400 --> 00:46:53,000
Like if you go to.
00:46:53,000 --> 00:46:54,080
Have you ever been to an er?
00:46:54,400 --> 00:46:59,200
And hopefully you haven't, but if you have, unfortunately you'll know that like everybody looks
00:46:59,200 --> 00:47:02,360
like most People look like they have an emergency, right?
00:47:02,680 --> 00:47:04,840
But not all of them actually have an emergency.
00:47:05,480 --> 00:47:10,120
So can AI come in there and scan them and say, okay, you're having a heart attack. You're first.
00:47:10,840 --> 00:47:15,160
Your, your, your leg is like, you have like a bruise. You're gonna wait, right?
00:47:15,160 --> 00:47:16,840
Like your liver is shutting down.
00:47:17,080 --> 00:47:18,200
You need to go to the front.
00:47:18,440 --> 00:47:25,190
Right now you're hoping the front desk person thinks you're nice and puts you higher on the urgent care. Yeah, yeah, yeah, Right. So that's one thing.
00:47:25,990 --> 00:47:29,950
And then workflow, that would be huge. That would be huge.
00:47:29,950 --> 00:47:30,990
And I'm sure it's coming the way.
00:47:30,990 --> 00:47:34,870
Maybe I gave someone some idea and hopefully I'll get some royalties from that, but who knows?
00:47:34,870 --> 00:47:38,030
Will Sanchez: Yeah, you have patients that, that cry wolf.
00:47:38,030 --> 00:47:44,310
And then you have other patients go, no, I'm fine, and sit down. And they're literally dying. So that, that's great.
00:47:44,310 --> 00:47:45,630
Dr. Grant Garcia: And that's in my office too.
00:47:45,630 --> 00:47:46,870
I mean, that pops in there like.
00:47:47,430 --> 00:47:49,310
And I have that now because I have a lot of.
00:47:49,310 --> 00:47:51,430
My physician assistants will see my patients first.
00:47:51,910 --> 00:47:54,310
So they're essentially triaging the situation.
00:47:54,790 --> 00:47:59,950
But before, when I didn't have that, when I was newer, you know, I'd have three patients and I'd have two patients.
00:47:59,950 --> 00:48:04,150
One patient, you know, would have nothing wrong with them. It's not their fault. Tons of pain.
00:48:04,230 --> 00:48:06,390
You couldn't figure anything out. Everything was negative.
00:48:06,470 --> 00:48:08,870
And they're upset with you because you can't find it. Right.
00:48:09,350 --> 00:48:14,190
That patient would spend, you know, 45 minutes with me either, unfortunately, arguing sometimes
00:48:14,190 --> 00:48:17,030
or telling me I don't know what I'm talking about if I can't find it. Right.
00:48:17,280 --> 00:48:19,520
They've seen 10 doctors and I'm the one that's supposed to figure it out.
00:48:19,520 --> 00:48:21,280
I can't figure it out. So that happens.
00:48:21,360 --> 00:48:26,800
Thankfully, it's not that often, but that patient unfortunately wasted 45 minutes of resources.
00:48:27,040 --> 00:48:31,760
And now the next patient who I get to is upset because I'm 45 minutes behind, which they're not seeing.
00:48:32,160 --> 00:48:35,200
And then they have a bad experience or two or three have a bad experience.
00:48:35,200 --> 00:48:37,800
And now, like, it's more than just that. It's like.
00:48:37,800 --> 00:48:41,920
Or I'm flustered and maybe the next patient, I've got to reset my mind, right?
00:48:41,920 --> 00:48:44,440
And I maybe miss something with the next one Again, that's.
00:48:44,440 --> 00:48:47,920
This thankfully doesn't happen that often, but it's something to be aware of.
00:48:47,920 --> 00:48:49,920
So, like, if you can keep your.
00:48:51,120 --> 00:48:54,640
If you can keep the high functioning situation decrease.
00:48:54,640 --> 00:48:56,240
It's always about decreasing stress, right?
00:48:56,240 --> 00:48:58,640
Like every doctor show every doctor's channel.
00:48:58,720 --> 00:49:02,320
There's such high burnout, there's high suicide rates.
00:49:02,320 --> 00:49:03,920
These are scary things to talk about.
00:49:03,920 --> 00:49:05,080
But why are they like that?
00:49:05,080 --> 00:49:07,520
Because they're doing activities they don't need to be doing.
00:49:07,920 --> 00:49:09,600
They're, they're filling paperwork out.
00:49:10,050 --> 00:49:12,130
They're, they're the ones prioritizing the patients.
00:49:12,370 --> 00:49:14,090
What happens if your machine did that for you?
00:49:14,090 --> 00:49:19,090
And they're like, okay, now I've done like, I've done literally like 20 hours of work for you.
00:49:19,170 --> 00:49:23,330
So now your 80 hour work week is 60. Right.
00:49:23,330 --> 00:49:27,090
Like today I've got my new workflow where I see patients that really need surgery.
00:49:27,570 --> 00:49:33,210
I see 20 less patients, just like Denard was talking about. Yep.
00:49:33,210 --> 00:49:35,010
But my patients get more time with me.
00:49:35,010 --> 00:49:37,570
And so the review, I don't get reviews. Like, I've been waiting.
00:49:37,860 --> 00:49:39,820
He was late, you know, today I was a little late in the beginning.
00:49:39,820 --> 00:49:41,780
I apologize to those patients if you're listening.
00:49:41,940 --> 00:49:47,780
But for the most part I stay on, I stay on time and every patient has me sit down and usually
00:49:47,780 --> 00:49:52,500
the patients are like looking at their clock because they're done talking to me. Right. Like, so that's good.
00:49:52,660 --> 00:49:57,100
So the, the goal here is that like everybody's getting more of what they want and the frivolous
00:49:57,100 --> 00:50:03,060
stuff is gone and I am less stressed because I actually normally am full speed ahead on everything I do.
00:50:03,310 --> 00:50:04,990
And now in the or, it's more efficient.
00:50:05,150 --> 00:50:10,470
I'm more efficient with workflow in the office and with AI, it's going to make it better. Like AI notes. Right.
00:50:10,470 --> 00:50:15,030
Like the notes are great, but like half the time the note just repeats everything you just talked about. Yeah.
00:50:15,030 --> 00:50:18,990
So like there's AI programs on your watch that I can walk in and it will come out and have a
00:50:18,990 --> 00:50:23,390
note done for me and then it will document and then I can add a little bit of stuff to it and make sure it works.
00:50:23,470 --> 00:50:25,110
And so like, that's amazing.
00:50:25,110 --> 00:50:29,950
Like, wouldn't it be awesome if your doctor, most doctors said they spend like 75% and I'm in.
00:50:29,950 --> 00:50:34,590
Surgeons was different, but most doctors suddenly send like, like 70 or something of their time
00:50:34,830 --> 00:50:37,150
doing paperwork and non doctor stuff.
00:50:37,150 --> 00:50:41,150
And surgeons, we have a lot of time, we sit around in the operating room waiting for the next surgery to come.
00:50:41,390 --> 00:50:45,870
But women's, if we had like robotic cleanup so they could clean the OR faster so that we could
00:50:45,870 --> 00:50:48,990
all be ready and get all your surgeries done and you're not wasting your time either.
00:50:49,390 --> 00:50:54,110
And, and, and you're not as gas at the end of the Day because you're done at 2 instead of done at 5. Right.
00:50:54,110 --> 00:50:57,430
There's all these other things that we're not even at the point yet where we're trying to talk
00:50:57,430 --> 00:51:03,230
about limiting the surgeon or any of the staff members, but making an experience for the patients.
00:51:03,470 --> 00:51:06,070
If they like called, they got someone on the phone. Right. And it was AI.
00:51:06,070 --> 00:51:09,950
It plugged me into my office visit in the offices that saw you were like, hey, not a surgical
00:51:09,950 --> 00:51:11,590
patient, but we're still going to treat you.
00:51:11,590 --> 00:51:12,710
You can go see this person.
00:51:12,710 --> 00:51:15,950
And then so far, you've just been AI'd in, but you've gotten this all done.
00:51:16,110 --> 00:51:23,710
I can tell you right now if you pulled all the patients and I said if you like most time now in Seattle, unfortunately. And will.
00:51:23,710 --> 00:51:27,350
You may or may not know this, if you want to have a provider outside of like an orthopedic surgeon
00:51:27,350 --> 00:51:33,520
at one of the, one of the pro alliances, you're going to wait like six months to see a doctor. Unless it's an emergency. Right.
00:51:33,920 --> 00:51:35,080
So it's like five, six months.
00:51:35,080 --> 00:51:37,480
But what if I told you you could see someone in like a.
00:51:37,480 --> 00:51:40,800
You could get, you could pick up the phone, call them, it would take you two minutes.
00:51:40,960 --> 00:51:45,960
You'd be hooked up, you could see someone, you could maybe even talk to an AI person thing that
00:51:45,960 --> 00:51:47,120
would kind of triage you.
00:51:47,200 --> 00:51:49,920
And like, if you're really pissed off, then you can like override it.
00:51:50,000 --> 00:51:53,320
But maybe you could be like, maybe that'd be enough for you to be like, okay, let's ping you
00:51:53,320 --> 00:51:54,480
and get you into somebody else.
00:51:54,880 --> 00:51:58,640
Or it can sense the tone of your voice, it can sense all these things and it can say, this one
00:51:58,640 --> 00:52:00,960
sounds urgent, I should get them in. Right.
00:52:00,960 --> 00:52:02,480
Like that stuff that you, Dr.
00:52:02,480 --> 00:52:05,600
Never is going to get a chance to do, but now your doctor's seeing all the stuff that's important,
00:52:05,600 --> 00:52:08,960
or not seeing patients that are pissed off because they waited six months to see you.
00:52:09,120 --> 00:52:09,520
Will Sanchez: Yeah.
00:52:09,520 --> 00:52:14,440
Dr. Grant Garcia: Right. So, like, there are so many aspects of this that are good for the patients that don't
00:52:14,440 --> 00:52:17,240
require you not getting to see a doctor. Yeah.
00:52:17,240 --> 00:52:23,200
Will Sanchez: You know, and it's going back to some of the things that I'm privileged to kind of work with
00:52:23,200 --> 00:52:33,830
is you're talking about creating the correct agent and also learning what the correct prompt
00:52:33,830 --> 00:52:42,590
is and putting those things together to have these diagnosis that hopefully will confirm, conform
00:52:42,910 --> 00:52:49,150
to, to the needs of the patient and, you know, hit the, the warning signs for the doctor saying,
00:52:49,150 --> 00:52:50,670
hey, we've got to get these patients in.
00:52:51,840 --> 00:52:55,200
Dr. Grant Garcia: I think, I think the last, the Thing I'll keep bringing up is AI.
00:52:55,600 --> 00:52:56,720
This is a good summary.
00:52:56,960 --> 00:52:59,600
AI is going to make healthcare hopefully faster.
00:53:00,080 --> 00:53:04,400
It's going to make it more efficient, it's hopefully going to make it more cost, conscientious
00:53:04,400 --> 00:53:05,520
because you're not missing things.
00:53:06,080 --> 00:53:11,760
And it's going to make it way better experience for the patients because like they're going
00:53:11,760 --> 00:53:16,520
to get their MRI done and like you have AI MRI machine so it's faster at calculating things. Right?
00:53:16,520 --> 00:53:19,910
Like the new MRI machine we're looking at, it's got AI built in to it so it can do like double
00:53:19,910 --> 00:53:21,230
the scans in a day. Right?
00:53:21,230 --> 00:53:27,150
So now you get, you sign up for an MRI and you, you get your MRI in one day rather than waiting three months.
00:53:27,870 --> 00:53:32,390
Then it's interpreted faster because it's got AI and then it's pinged to the radiologist that
00:53:32,390 --> 00:53:35,430
no longer has to look at like basic boring MRIs. It's got the ping.
00:53:35,430 --> 00:53:36,830
So it's like this one you should look at.
00:53:36,910 --> 00:53:42,110
So then the radiologist reviews the, the big ones and then that's checked off and now the radiologist
00:53:42,110 --> 00:53:43,550
is less stressed so he can do it.
00:53:43,550 --> 00:53:47,530
And all of a sudden now you're like, okay, you've got all this stuff, you've got to an ACL tear
00:53:47,530 --> 00:53:48,650
or whatever, you got something going on.
00:53:48,650 --> 00:53:50,370
So now we're going to ping you to the orthopedic surgeon.
00:53:50,370 --> 00:53:53,730
We're not going to send it to a person to do it, we're going to ping it right to the orthopedic
00:53:53,730 --> 00:53:59,370
surgeon's office and actually schedule you like you would be in like, I think that any, any
00:53:59,370 --> 00:54:06,050
American and a non American, but American using the healthcare system would be absolutely elated to have that experience.
00:54:07,010 --> 00:54:12,210
So I, I, and I think that you'll find that it'll miss less things because like I said before,
00:54:12,790 --> 00:54:18,310
if we can remove all the frivolous stuff for our surgeons, doctors, they're going to be so much better at their jobs.
00:54:18,630 --> 00:54:22,470
And so I think that's what we're going to see, is that you're going to see better health care for the patients.
00:54:23,430 --> 00:54:27,110
But I guess that's just my opinion. So we'll see.
00:54:27,750 --> 00:54:33,670
Will Sanchez: It sounds like an episode that we will eventually update and why it was.
00:54:33,670 --> 00:54:35,430
Dr. Grant Garcia: So wrong and where we went wrong.
00:54:37,110 --> 00:54:42,780
Will Sanchez: No, I think there's some great ideas and especially it's, it's a great understanding of how
00:54:42,780 --> 00:54:50,060
we're utilizing AI and really this is the infantile stages of where we are with this technology
00:54:50,780 --> 00:54:56,700
as we, you know, there are next, you know, Industrial revolution that's happening right before our eyes.
00:54:57,020 --> 00:55:01,340
So it's a very exciting time and we'll see how it all shapes out. Dr.
00:55:01,340 --> 00:55:04,380
Garcia, congratulations on top Dr.
00:55:04,380 --> 00:55:05,610
Once again, that is wonderful.
00:55:05,840 --> 00:55:11,280
One distinction that AI cannot take away because you're doing it the right way.
00:55:11,760 --> 00:55:16,240
So I, I just wanted to shout you out and I know you've got some sun tanning to do, so we're going.
00:55:16,320 --> 00:55:18,360
Dr. Grant Garcia: Yeah. Ready to go?
00:55:18,360 --> 00:55:19,760
Will Sanchez: Got your sunblock ready?
00:55:20,480 --> 00:55:24,160
Dr. Grant Garcia: I do. Well, the Brazilian skin helps a little bit, so I don't need too much on there.
00:55:24,240 --> 00:55:26,600
Will Sanchez: Oh, baby. All right, enough of that.
00:55:26,600 --> 00:55:28,960
Go do your hit and go enjoy yourself.
00:55:29,600 --> 00:55:31,360
Thanks for listening to Sports Doc Talk.
00:55:31,990 --> 00:55:33,110
We always want to hear from you.
00:55:33,110 --> 00:55:38,790
Please check out our website, sports.talk.com we've got shows, we've got great information.
00:55:39,030 --> 00:55:41,830
We've got links, we've got transcripts.
00:55:41,830 --> 00:55:43,590
I don't know what else. Dr. Garcia, we.
00:55:43,590 --> 00:55:44,870
What else are we missing from that?
00:55:44,870 --> 00:55:46,870
Dr. Grant Garcia: We got social media. We got awesome guests.
00:55:46,870 --> 00:55:51,070
I mean, honestly, this is one of our first big topic shows in like a few months because we've
00:55:51,070 --> 00:55:52,910
had so many good guests. Yeah.
00:55:52,910 --> 00:55:54,470
And we have so many more coming.
00:55:54,950 --> 00:55:59,110
Oh, if you're listening, ping us as a guest.
00:55:59,530 --> 00:56:00,850
We love to have the guests on.
00:56:00,850 --> 00:56:06,170
We have some really good ones coming up and we're not going to let it out, but we have some good ones coming up.
00:56:06,170 --> 00:56:07,050
That's all I'm going to say.
00:56:07,210 --> 00:56:08,690
And the hot topics have been good.
00:56:08,690 --> 00:56:10,650
This is the first big topic one in a while.
00:56:10,650 --> 00:56:15,090
Well, this is awesome because we just thought it was time, you guys.
00:56:15,090 --> 00:56:17,970
But again, there's a lot of good guests coming up, so stay in tune.
00:56:17,970 --> 00:56:20,810
Social media, you name it, and check us out.
00:56:21,050 --> 00:56:24,330
Will Sanchez: Yep. We appreciate the viewers, the listeners and all the support.
00:56:25,060 --> 00:56:27,460
We hope to continue to provide information.
00:56:27,700 --> 00:56:36,820
But as you said, we've got, we've got a lineup that's coming up in 2025 that's sure to be entertaining. Dr. Garcia, say goodbye.
00:56:37,940 --> 00:56:38,740
Dr. Grant Garcia: Bye, guys.
Audio Transcript
Revolutionizing Shoulder Surgery with Dr. Patrick Denard
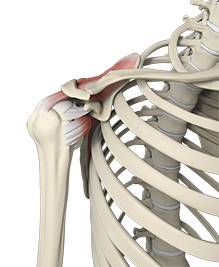
Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. Will Sanchez, along with our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia. Dr. Garcia, I am I, I started this conversation before we hit record. I am going to have to take the AI function away from you because you are getting outta hand with your backgrounds.
I don't know what's gonna happen next show, but I You have no idea. You're having too much fun, man. How, how are you man? What's going on? I'm good.
Dr. Grant Garcia: I, um, things are good. Got vacation recovering from time zone changes, and, uh, I'm really excited for our, our guest tonight. Uh, we're not gonna give away too much of the spoils.
That's supposed to be a shoulder above me, and that's some nutritional stuff. I go backwards this way, so [00:01:00] I don't wanna give away too much. We'll get into it in a second, but I'm really excited for this guest. This is gonna be, we're trying not to nerd out too much. With our shoulder talk.
Will Sanchez: Oh God, please. You know, we're gonna get nerded out.
You know, you love it. Let's give a shout out to the good folks at the Recovery Shop. Let everybody know why you love to utilize the Recovery shop.
Dr. Grant Garcia: Yeah, so big thanks to our sponsors. Uh, you know, the recovery shop's really great and actually, you know, our, our guest uses the Recovery Shop too, and, and actually sells some of this stuff on there we can talk about as well, which is great.
So the Recovery Shop for me, for surgeons, it gives the surgeons the ability to get some patients, these aftermarket things that they want. They want a little bit extra, you know, how do I get better recovery with. Complete surgery, attrition. How do I get better machine options? They have those on there, nice machines, you name it, different products that are not available through the standard insurance processes.
And my patients have been so enthusiastic. I mean, I had multiple patients today talk about the post-op recovery stuff they were able to do with something like the Recovery Shop. They were just really happy about it. It's a [00:02:00] win-win for everybody. So. Reach out to Mike b@recoveryshop.com. Uh, you know, again, this is, there's no cut from us for sponsoring you and sending you there.
Uh, but the key here is really to make sure that your patients get what they need and that the surgeons feel like they can give their patients everything they ask for it.
Will Sanchez: Yeah, and it's not just the doctor saying it is the patient as well as someone that's recovered from the torn Achilles and utilizing that nice machine, it not only made my life better, but my wife's better.
I've, I, I've told everybody that the fact that I did not have to bother my wife to go get me ice. Every 40 minutes as I iced on and iced off really saved our relationship. So if you can't utilize re recovery shop me too for recovery. Me, me too.
Will Sanchez: It it, it will save your marriage. So it's one of the great things.
Listen, I'm excited about our guest today, uh, recogniz as one of the top shoulder surgeons in the United States. Co-author of two books. I don't know how he does it. I'm gonna bring them on. 'cause my [00:03:00] first question is. Dr. Denar, thank you for being here, but how the hell have you done over 7,000 shoulder surgeries?
Where is the time? Do you do anything else besides stay in the operating room? How is this possible?
Dr. Patrick Denard: Thanks for the introduction. Yeah, uh, efficiency, man. You know, I just, um, I'm an efficiency monster and just try to prioritize. It's all about time management. A lot of people think, I don't have a life, actually, but I mean, I just got back from multiplications.
I spent tons of times with my kid, tons of time with my kids, and, you know, relationships, so, and do other things. So yeah. It's just what, it's just that's what it's, there's Will Sanchez: no rumors that you have an operating room in, in your house and you just, that's how you save time. You just go, you go to the room next door and start surgery.
Dr. Patrick Denard: I do, do two rooms. Yeah. Back and forth, back and forth. Yeah. Yeah. But, but not in his house. Stay in the zone. You stay in the zone, you know, just flowing. Yeah.
Dr. Grant Garcia: I, I think that's a good point you bring up. 'cause I [00:04:00] think that people always say Patrick, the same thing with, you know, doing videos and you do so much on your social media.
I. So many publications you're involved with industry, you ha you do a really good job with the shoulder patients. You run your own practice at Oregon Shoulder Institute. So, you know, it's a lot of things you're doing and you have fellows. Is that correct? So, I mean, you, you're doing a ton, uh, and that's not easy to manage.
But the, the key here is efficiency. We can get into this in a whole nother topic. As to how, you know, as a surgeon you can be efficient and do so many different things at once. Um, but I don't wanna take away from the all the awesome things that you have to talk about today. Uh, but really, really appreciate you coming on.
I'm really excited for the audience to hear this. So this will be great. Can you talk to us? I mean, tell us a little bit about your, your background. I mean, Medford, Oregon. That's awesome, but like, you're now people flying to see you from Medford, from all across the United States. People read your publications, Medford's a, you know, a small town place in Oregon.
Tell us, tell us why, how, how'd you do it? I mean, that's [00:05:00] not, yeah, I'm a big CD Seattle guy. Like it, I had some work to do, but it's a different animal than being in Medford. How'd you do it?
Dr. Patrick Denard: Well, I grew up in a town called Zigzag. That's where I was born, 500 people at the base of Mount Hood. And then I moved to the big city of the DAOs when I was five and I was raised there, a 10 of 10,000.
So I'm a small town guy. I mean like, I don't really like stoplights even.
Will Sanchez: And neither do I for different reasons. Yeah.
Dr. Patrick Denard: I just, you know, that's just how I was raised. And so when I was looking to start my practice, I wanted to be in a medium sized town. I was like, okay, a medium sized town so that I could specialize but have good quality of life.
And you know, the other stuff just kind of came after. I mean, I always had kind of an interest, but to be honest, like probably in residency and fellowships some or, uh, medical school, I was doing some of it just to kind of. Get to the next step. And then when I did fellowship with Steve Burkhart in San Antonio, I think that was a big sort of pivot in my life.
And I sort of saw, okay, I can do [00:06:00] this and kind of build my thing and I just, you know, slowly did it over time. It's just, I. I think most people underestimate what they can do in several years. Like the overestimate, they can do a year, but they will underestimate just with consistency what they can do over time, you know, and that's really like my secret power is just time management and consistency.
I'm just relentless about always trying to do the next thing and trying to build and make it better. So that's
Dr. Grant Garcia: how it's gotten where it's at.
I'll
Dr. Grant Garcia: tell the audience this. I can tell that Patrick's incredibly efficient. I'll tell you of all the people we have emailed for our podcast, people I have reached out to.
He is by far one of the fastest email responders. He is on top of it for how busy he is. It was so easy to set this up with you. I mean, that just shows it like, right, like you're everywhere and you're still available. And so the ability to do that kind of, right. I mean, the minute we, I reached out to him, I knew that this was gonna be, I could see the breakdown of how he works.
So it was [00:07:00] kind of cool to see that, 'cause you know, I'm known to try to get my emails done quickly and respond well, but it's, it's always like pulling t sometimes to get guests on here in terms of getting in touch with them, setting it up. I, I, thanks. So, I, I don't want to go off on tangent here, but thanks for making it so easy for me because normally it's, it's a, it's not so easy.
So I appreciate you. Yeah, thanks. So why don't we get into this, uh, you know, the conversation. I think you do so many cool shoulder surgeries. We, you just talk about your practice setup, like, you know, yeah. Fellows and shoulders. Yeah. You got it. Yeah, just talk to bit about it.
Dr. Patrick Denard: So, I do a hundred percent shoulder.
I've done a hundred percent shoulders since I started practice, probably six months in a p or a year in a practice. I did a hundred percent shoulder. So I started in 2011. Um, I a very high volume practice. Um, I actually, believe it or not, I only at this point. Work three days a week. I work Monday, I operate two days.
I do Tuesday all day clinic, and I do three and I Wednesdays, I do two rooms, [00:08:00] and then I save the other days for other things like the nutrition stuff, we'll talk about real estate investments and working with industry and meetings, right. And research. Um, the way I do that is just, I've just been really, you know, prioritized trying to make every moment count.
Um, I have two PAs. They're great guys. They've been with me for 10 years each, so they funnel a lot of patients to where when I see patients in clinic, they pretty much have a problem or need surgery. Um, so I, I don't see a lot of non-operative stuff. And then, um, you know, that makes my clinic, like I'm doing what I wanna do, right, is surgery and or guide people whether or not they need surgery.
And then I have two fellows. Um, they spend six months with me each, and they rotate with two other guys in my group. So we got to, you know, a busy group. Um, you know, we also have a research program. We do quite a bit of research. We usually have a busy international research person or two who [00:09:00] are doing a lot of work.
Dr. Grant Garcia: Did you set that up, the fellowship with them, or is that already established in place?
Dr. Patrick Denard: Yeah, I, I started it all. I started, you know, I started collecting outcomes and then I got the fellowship and I, I actually. I started doing outcomes and then I got a 5 0 3 cb, you know, created a nonprofit foundation so that I could bring in industry funding or grant funding.
Um, and, uh, had a good relationship with Arthrex. You know, I can't ignore that. They really helped me kind of support my research at the beginning, which was really key for guiding private practice. Um, and, uh, have two research coordinators who are full-time, who collect data. And I've been doing that just since the get go.
And then we developed the fellowship or started the fellowship five years ago now. I think. So, yeah, it's been a fun ride. Fun. What's fun is, is the satisfaction of like looking back and you built it, right? Like I had some opportunities at a couple of different points in my career to go elsewhere. [00:10:00] And pick up and leave.
And it was, you know, you sit there and go through and you know, what, what do you wanna do with your life kind of thing in the middle of your life. And I think having built it and feel like it's, you know, I have a lot of autonomy and control, it's been really gratifying for me. You know, 'cause then I can start transitioning into, you know, early in your career, what gets you really excited is doing surgery and doing it fast.
And I still love surgery, but what excites me more now is teaching and. Research and development and trying to, you know, move in that next phase. Right? The whole like Arthur Brooks, like strength to strength thing, right? Like how you transition over your life.
Will Sanchez: So how did you, um. How did you get involved?
What was the passion that you got into, uh, when you first got into this field? Did, was it something that as you studied, you decided to go into specializing in that specific area? Or was it a mentor? You know, I'm always curious how does this happen? Yeah. What, what got you shoulder
Dr. Grant Garcia: [00:11:00] only?
Dr. Patrick Denard: Yeah. Shoulder, I mean, back medicine.
I mean, I knew when I was like 15, I wanna go into medicine. I was gonna be a general surgeon 'cause I worked in the operating room of the Dallas and they would let me, these guys would let me like scrub in and hold the camera and, and, uh, do lap ies. And so with him, I was like, I'm gonna be a general surgeon.
Uh, it was so cool. And then I got to, um, medical school and just ended up finding that my personality fit orthopedics more. It was actually a hand surgeon. I was operating with him and I was like, this is just, I can see it and I like see it get better. And it was just, I'm a very concrete thinker. Like if you ask me an analogy like, I will fail, right?
Like every time. But I can think very concretely. So orthopedics fit and when it got to orthopedics, just shoulder just seemed to be the, you know, the field I thought was really growing, developing the most, you know, really challenging field. But also I, early on I really wanted to be a specialist. You know, I just wanted to be [00:12:00] like, good at one thing.
So, um, that's how I got to shoulder and, um, yeah.
Dr. Grant Garcia: And Patrick, I mean, there's a lot of it, it, people don't think about this. I mean, you, you, you've been doing this a while, but you're not, you know, you're not like, you're not, you haven't been this for 25, 30 years. Right? Right. And it's a lot of work that you've put in.
I mean, to start a fellowship is already a big deal. To do, be able to do a practice setup like you have then if people flying in for surgery. I mean, that's a lot of efficiency. Do you, do you, who do you think like, I mean, that's a pretty un that's a pretty uncommon. Set up. Mm-hmm. Right. To someone is who's happy as you, who's as busy as you, but also doing all this stuff.
Is there, was there any guidance? I mean, Burkhart's, we all know Burkhart, right? He's, you know, one of the world's best shoulder surgeons. Very involved with previous Arthrex stuff and doing lots of sort of design and things like that. So he had some of that. But was there anybody kind of a template? Like in my practice, I'll be honest with you, my practice is a very big template of [00:13:00] coal trained at Rush.
It was go, go, go. Multiple rooms. Very efficient. Cartilage practice. You know, I do shoulder surgeries, elbow and knee, but it, I just, that was kind of my kind of template. Was there any template or you kind of steered off the course? I mean, you def, there's not many people like you out there, but is there kind of anything that you use as your template?
Dr. Patrick Denard: I think that, I mean, I, Steve was a really big influence. So, I mean, the reason I went and did fellowship with Steve was because he was in private practice. Um, and I, I wanted to see that ability to do research and be involved and like, I didn't know it was gonna go where it was gonna go, but I thought that was, seemed admiral to me.
Um, but I, I think I, I kind of take the philosophy of like the tribe of mentors here and like the thing that I've noticed is that it's so accessible now, right? You can. You know, Brian Cole is a guy that, you know, I saw him speak when I was a resident and I was like, I wanna be able to present like that guy, right?
Mm-hmm. And or like Tony [00:14:00] Romeo is a great presenter. I wanna present like Tony. Yes. And then, you know, other people of like a, you know, like a naval ravikant, right? Like Naval Ravikant talks about. I'm a huge fan of his, and like he has no idea who I am, but he's been a big influence on my life. He talks about things like.
If you're going to, if you want to be good at something or you know, let's take money, you wanna make money, you should not do something that is below that pay grade. Right. So just sort of using your time effectively. And, and he talks a lot about specialization, right? Like generalization is, you know, the Renaissance man and in many ways is kind of gone.
You gotta be really good at something, develop a skill. So I just try to take it all in, you know? And like I'm a big reader. I'm a big podcast guy. Um. You know, I'm listening to stuff all the time if I'm on the bike and always trying to pick up new things and just try to, you know, but.
Dr. Grant Garcia: Yeah, so they said that book of I better book efficiency.
I dunno, that's the one different one. The one where it's [00:15:00] just like the one line, you know, it's like the arrow, you just go one way. There's so many different arrows going different directions. You just stay super hyperfocused. Uh, and that's, you know, that sounds a little bit like this. I, I remember Josh Dines of very HSS would kind of get involved with that book and he was like, Hey, you should read this.
And I, I'm not as a vivacious reader as you. But that one was, that one was near and dear to my heart. But anyhow, I mean, will you talk about, so I know you do a lot of shoulder surgeries and that's all great, you know, shoulder surgery's awesome. But I want to kind of hear more about, let's pull up that rotator cuff slide and I wanna hear more about this, Patrick.
I mean, 'cause you're, like I said, you're, you're, you're the jack of all trades. You do research, you do really high volume surgeries and you do a good job, but you're also involved in industry. So it's kind of the, the triple threat, which is unusual to find. So I know this is your paper, you got, we could, we could spend 200 hours reviewing all your papers 'cause you've done so many of them.
But kind of talk to us about your, what, what you're doing for rotator cuff thought process. And then we can get more into like the augmentation idea so people, so listeners can [00:16:00] hear this 'cause they, they hear word to cup but augmentation. They're like, what the heck are you talking about?
Dr. Patrick Denard: I mean, I think it's like, you know, what we're trying to always do as clinicians is we're trying to calculate all these things, right?
And get down to what is the best for the patient, right? So, you know, and there's so many variables. So what we try to do here is give people a framework to think about when should you augment rotator cuff tears and knot. So that was kind of the, the, the big idea is like, we have no guidelines. How do we get there?
25%. And Patrick,
Dr. Grant Garcia: will you, will you describe the augment idea for the, for the patients and listeners out there? Yeah. The idea of augment mean,
Dr. Patrick Denard: right? So 25% of rotator cuff tears don't heal. We know that. So the idea is that. They need something else. Something like, you know, biology, we'll talk about nutrition later, which I think is biology, but right now as clinicians, we've maximized the strength of a repair of the biomechanics, right?
So there's certain people that don't heal and they need something else to, to [00:17:00] augment. And that augmentation can be like a graft or a tissue that you put on top of the rotator cuff. That augmentation could be things like putting in. Growth factors, um, those kinds of things. Specifically here we're talking about tissue augmentation and we try to make a recommendation based on looking at patient factors going into the surgery that, you know, in advance that would allow you to a, have a conversation with the patient to say, Hey, you're at higher risk, so now we're gonna think about other things.
Be, be prepared so you can be efficient when you're going to do it. C, make the decision ahead of time versus like, we're human, right? We get to the end like, do I really wanna augment this case? No, I wanna get outta here, but if I've made a decision ahead of time and said that I'm gonna augment, that's a big change.
Yeah. And then I'm in private practice. The last thing is, you know, I'm in private practice, so I have to think these things have costs. Right. You mentioned in this relationship they have costs. So [00:18:00] I have to know what the insurance is, what the facility is, where I can go and do the procedure if I think it's indicated.
So that was the idea of this paper, is try to give people a framework
Dr. Grant Garcia: I. I think that's important for the listeners to hear because we drop all this really cool technology all the time. But I think Patrick will completely agree. He's already shaking his hand. He knows where I'm going with this. But you know, insurance companies, it's difficult, right?
They get, you get a, here's your pot for the surgery center, and if you start putting more fancy things, it's like a car, right? Well, you get your upgrades, you want your sunroof, you want your oracle play, you want your souped up engine. Sooner or later, the budget runs out and you can't do the surgery. And then the surgery center says you can't do this.
This is too cost. It depends on the insurance company. So it is, it is troubling and frustrating, right? Because if, if we didn't have to worry about that, we could augment everybody. I mean, honestly, there wasn't insurance company
Dr. Patrick Denard: come back and say, we're not paying for the surgery and you're out and the patient is out.
I've had that happen. And
Dr. Grant Garcia: they're just, and that, uh, that doesn't go very well. That's not a good conversation. So that's even the, like [00:19:00] the last piece of the puzzle. When you're augmenting, what is your sort of, so the idea behind this, uh, for will to listen, I dunno if you have any questions, but basically you gotta a rotator cuff tear.
You fix it, but now you gotta add something extra like you talked about. So he's got biologics, you're gonna add post stuff, surgical nutrition, we'll get to in a minute. Um, what's kind of your go-to? Like, what do you like to do? Does it kind of depend on the, the situation? I know again, we're not gonna go into crazy nuances.
Uh, you know, the subscap, irreparable subscap, that stuff's important, right? But really kind of, and you're, and most of the time, how often are you, I. Adding something else Intraop, when you go in there and see it. Are you, like you said, you have that plan ahead of time. You've seen the MRI, like what factors are you looking at?
You got all these things, but is the M MRI the most important for you? Is it the patient that's most important for you? Is it just like your gut feeling? Like how are you doing it? Dr. Patrick Denard: Yeah. I try to look at, I mean, most of the scoring system, the, the rotator cuff healing index was this ROI score is based off the MRI.
It's based off of age and the MRI right findings. I think that's [00:20:00] the most objective way. If you look at the time of surgery, you're probably not as good as you think you are in really deciding. Yeah. Um, the exception to that would be like, I really don't care what it looks like. If it's revision, I'm gonna, even if it's small, I'm gonna, I'm gonna, I'm gonna augment.
Yeah. But you know, to answer your question, I probably augment about 10% of my cases. A lot of people think it's a lot more, um, I told you 25% don't heal based on the data. And the, the fact there though is that in older patients who are lower demand, if they get partial healing, that's, that's, that's probably acceptable.
Yeah. So if I have a 75-year-old who has a tear that may have a ROI of seven, I, I'm probably not gonna augment because they're gonna be okay with partial healing. I'm really targeting. Well also we
Dr. Grant Garcia: know, we also know some of those patients that you, you do the augment that they don't heal and they don't have a pain, like you said, the partial healing, they may not even be symptomatic.
Dr. Patrick Denard: Right. Not all right. Exactly. That's the point. It's like not all, you know, just because they don't all heal Still, the vast majority of [00:21:00] patients do well. Right. Like 90% of the people are gonna do well from a rotator cuff repair. Yeah. So it's really those young ones I think you're trying to target to alter their natural history.
'cause in them healing's, not a lack of healing's, not acceptable. 'cause they're gonna go on to have, you know, early arthritis, et cetera. Right. Yeah. And they're hiring Are, Dr. Grant Garcia: uh, Patrick, are you doing any more of like, do you do any of the tendon transfer stuff? Are you mostly cuff augmentation? I know you do a lot of shoulder arthroplasty.
Yeah, I do. What's your thought on.
Dr. Patrick Denard: Yeah, I do 300 arthroplasties a year, right. Because it's all shoulder and about 300 cuffs and then a smattering of other things. So, um, I do it all. I mean, I do tendon transfers. I do some, you know, cable reconstructions for irreparable tears. Yeah. Do all sorts of, you know, and really to me it's about trying to define the, the, the right patient for the right indication rather than everything being a hammer as a male, you know?
Dr. Grant Garcia: Do you, um. What type of, are you doing ever biologics for your rotator [00:22:00] costs? Uh, so do you ever add that or what's your thoughts on that? Dr. Patrick Denard: Yeah, I, I offer all my patients PRP, when we do that in a cash pay model, it's a surgery center. I say here the data says support for healing. It helps with healing. That is, it's probably about a 10 to 15% difference.
It's not gonna take you from 30% to 90% chance of healing. Uh, I would have it if you want it. Um, you can pay. Fourth and Got it. We a low price point to do that. We also offer bmac in the same manner. Um, and then, and bmac is, uh, bone marrow aspirate.
Dr. Grant Garcia: Bone marrow aspiring, yeah,
Dr. Patrick Denard: just a higher concentration of growth factors.
I don't like to call it, you know, stem cells, that probably is misleading. Um, but, uh, you know what we, as far as augmentation though, if I, you know, if somebody has, you know, maybe a good chance of healing and they just wanna make it a little bit better. PP is perfect, but if they have a low chance of healing without arthritis, that's where I start having the conversation about augmentation.
You [00:23:00] know, and my, my go-to is, is dermal allografts. I mean, you basically have xenograft that same for me, comes animal, right? You got allograft, which is skin from humans. And then you have, uh, synthetic patches now emerging in the market. So I've done primarily dermal allograft and a little bit of synthetic patches in some cases.
Dr. Grant Garcia: And for people to hear the, the skin's pretty interesting 'cause there's plenty of biopsy studies that show act actually the, the blood vessels go through the skin and actually heal it pretty well, which is pretty vascularization.
Dr. Patrick Denard: Right.
Dr. Grant Garcia: And I don't, I mean, not that we wanna say they fail, but if you ever take one out, they're actually extremely difficult because they heal right in.
That's kind sock down. It can be. Yeah. Yeah. If you get a good healing response, which is impressive. Yep. So you're right.
Will Sanchez: Yeah. I was gonna ask real quick, just, um, the complicated ones where, let's say a patient is older, has an injury, uh, maybe for whatever reason, [00:24:00] they're, they live by themselves, so they really have to, you know.
Take care of themselves and do the shopping. You know, how, how are those decisions, you know, compared to a normal procedure where you go, well this is what I will do for this patient. And you have to consider maybe, uh, the quality of life that this person's going through as far as the repair, if you can take, which is impossible to do.
You know, the insurance aspect of it. The money aspect. Yeah. You know, just how hard are those decisions and, and do you consult with yourself, the team? How does that work?
Dr. Patrick Denard: I mean, there's a lot that goes into that, right? I mean, you got, you might have somebody who actually has a tear that's kind of borderline, but you might say, say that you know, there's 75 or 80 and you might, I might do a shoulder replacement because you know you want one and done and you don't wanna put them through six months.
Have it not work out. Yeah. Maybe even if it's only one in three that it's not gonna work out. But if it doesn't, then they [00:25:00] have another six months of recovery or plus. So those are absolutely decisions that, you know, are factors that go into play. The other one is, you know, I call it the, you know, the trilogy of demise, right?
It's like poor bone quality, poor strength, and poor attitude. And you know, I can tell within 30 seconds, I'm sure Grant can as well, you know who's gonna do really well. And who's gonna do really poorly? There's like these, they're far the far sides, right? If they have good strength, good bone, good attitude, you're like, you know you're gonna be great.
Dr. Grant Garcia: Gimme more of those.
Dr. Patrick Denard: You gotta in the middle, right? That you're trying to like do the best you can, but you get the people in the end it's,
Dr. Grant Garcia: it can be
Dr. Patrick Denard: really,
Dr. Grant Garcia: really hard. Yeah. And that's also will sometimes when you change your method, right? Like you get patients what, like mid sixties, late seventies, and they got a poor attitude.
They've got. Biology's on the fence and you just know there's no way they're gonna handle a rotator cuff with augmentation. Yeah. It's just reverse, reverse, reverse because it's just you. You gotta get in the best shot, you know? And it's just that that's [00:26:00] one and done and you can't do, and you do such a good job with your replacements that it's kind of like, the other thing is, you know, the nice thing about someone like Patrick, and I know, I'm sure I want to go on the next topic, but.
Because, because you do every, all those shoulder things, someone's doesn't gonna feel like they're stuck with it, right? Like I know a lot of guys in the area, they do just the, the cuff stuff or they don't do the shoulder arthroplasty. I do like the whole gamut like you do, so you can offer each step, so you don't have to feel like, okay, he's not giving me the best option because they doesn't do it.
And I think that's, that's a really important thing. That's where I think the specialization or the, I actually call it now super specialization. Like a guy like you would be kind of super specialized, like just shoulder, just high level stuff, um, uh, can make a difference to the patient. That's what patients don't get.
You know, you see someone does shoulder, it doesn't mean they're doing all the shoulder stuff,
Dr. Patrick Denard: right? Yeah. Well, patients still go to people based on proximity and convenience a lot. Right. My busiest year in practice was COVID. Because we only had six weeks off here and then I [00:27:00] didn't travel, so, and I was just available and so people would come see me in the office and, you know, we didn't have much of a shutdown.
It was, it just really showed me that I'm like. I'm not that big a deal to most people out there, it's just because they can get an appointment next week. That's how a lot of people make decisions. It's,
Will Sanchez: and you make that decision with PT also, when I, you know, I go, well, I'm gonna look at a couple places and if they're comparable, I'm going to the closest place.
Kind of piggybacking on what you're talking about, not saying specifically you, 'cause you have a specialist, but I know when it comes to pt, you know, if it's convenient for me and I could get to it quick. I'm gonna choose something that's close. Uh,
Dr. Grant Garcia: will, we gotta move, we gotta move on. I told you this was happened with Patrick.
I'm gonna be in control of this situation. Go to that next slide. Show about the Rems. I wanna talk about the instability briefly. Uh, 'cause this Patrick does more than just this and we gotta get to surgical nutrition 'cause this is gonna be. So go to the next one. I mean, this is a good one. We can, why don't you bring this up briefly.
We'll [00:28:00] jump into your nutrition in a second and then we'll pull up the shoulder stuff. So kind of go over, what's your thoughts on that? We were talking about,
Dr. Patrick Denard: we were talking about biology and what's interesting here is this study at recently outta Japan. They looked at nutritional risk, and what you see here is that people often underestimate how good their nutrition is.
The first thing you see is that actually about 50% of people or more have some risk of nutritional deficiency. Interestingly, when they looked at like all the factors, their nutritional status, if you look at the odds ratio, it was higher or more important than her size or age and fat infiltration, which is what we talk about the cuff.
So I just think when we're talking about biology, we cannot not be talking about nutrition as well if we really wanna optimize the patient.
Dr. Grant Garcia: And as a surgeons, right, I mean, you're very nutrition heavy, but there's not. Not everybody's like that, right? So we're like, go, go fix, fix, fix, fix, fix. Cuff. Patch cuff, patch.
Biology. PRP. And we totally forget [00:29:00] about this, and I've talked about this before, but like, that's why like, like the recovery shop. But that's why like the post-surgical, the pre-surgical, those are very important. And, and as surgeons we are not very good at that. You are, but not a lot of us are. Right. But thinking about this stuff, so it's really important.
I think we bring it up.
Dr. Patrick Denard: Yeah.
Dr. Grant Garcia: Uh, so will bring up this. So you do the, you do your, again, you have your cuff patient population, right? That's your sort of like, you know, fifties. Seventies, and you got your shoulder arthroplasty, your 67. Again, this is a generalization. There are people that fit in all categories, but you got your young athletes, right?
And this is actually something that you are known for as well, uh, is your shoulder instability patients. Um, and this is something that I like to specialize in as well with this sort of. Stuff. So can you expl, I mean, this is a very nice color. I know you just made it up and it's not from a paper of yours, but I've definitely, like I told you before, the audience, I've seen this plenty of times.
It's a really nice thing. Kind of just briefly discuss what this is and this, you know, you talk about a couple of the things here and to [00:30:00] talk about rum massage or whatever else. Dr. Patrick Denard: Yeah. So when you're looking at people dislocate their shoulder, you have to know who they are, like what their risk factors are.
For having repeated dislocations specifically, that's gonna be, I. Young men under the age of 2025, right? Everybody talks about bone loss and we talk about how much of the socket or glenoid you've knocked off because it's like a ball in a golf tee. Once you knock off some bone it gets, becomes very unstable.
So we talk about do you add bone graft? The point of this algorithm really is to say there's this category of people who don't have a lot of bone loss, and a lot of surgeons will still do a bank heart repair. My argument is that if you look at isolated bank cart repair and look at the outcomes, they do well for a couple years.
On average, the failure rate's about 8%, but they continue to dislocate out to two and four years. So you start approaching a re dislocation rate of about [00:31:00] 20%, which is eight percent's not acceptable, but 20% is certainly not acceptable when you go out midterm for these patients. So. That's where I basically have said even with low bone loss, you know, almost all cases I'm adding a rum massage.
Because if you look at high risk, you know that's somebody under the age of 25, you got a 25 or you know, 18-year-old male. I don't care if they have a little bone loss, they are very high risk. They dislocated a normal shoulder. They've already shown that. So everybody talks about this glenoid track stuff.
I don't, I don't care about the glenoid track. I add room massage. And the reason is REM massage helps pull his shoulder back. Biomechanically very clearly. It shows the dislocation rate drops our outcomes two years. Our dislocation rate was 8% with isolated bank cart, 2% when we had re massage.
Yes.
Dr. Patrick Denard: And other studies have shown that not only that, but you don't have that continued drop off between two and four years.
It's like re visas tend to do well mid to long term. [00:32:00] So, um, we've really done a lot of lesage and it's just become easier with, you know, the techniques with knotless anchors and. That's honestly one of the reasons we started doing it is this got easier. I was like, all right. And then, you know, we looked back and found that it, it, it got, uh, it really made a difference in the outcomes.
Dr. Grant Garcia: And for people listening. I mean, that if you look over here, it's hard to see though, maybe if you're on a, on your phone to see the sort of breakdown. But, but this less than 15% bone loss is actually a very common patient population. I mean, I, I would say in my office, it's probably one of the most common.
Would you agree? Yeah. Yes. And if you look here. More than one dis. I mean, I get a lot of first time dislocators from some of the sports teams. I do, but it's not frequent that I'm getting a single dislocation patient as often as I'm getting the multiple dislocation.
Dr. Patrick Denard: A hundred percent. Yeah, I agree with you by the time they've got to you, or honestly, if they have a single dislocation in their, you know, 17, 18, they have any health sacs, which they should, I'm going [00:33:00] to add re most of those patients because.
The, just the da. The data is so profound. The differences
Dr. Grant Garcia: what? And it's come. So for the listeners, the re massage who basically take part of the rot tear cuff in the back and we attach it. Now that sounds kind of morbid, but I mean, Patrick, what do you think now with the new techniques, and we'll get into kind of futuristic stuff for this, the Lesage, what do you think, how much longer does the rummage take you from a surgery standpoint?
Dr. Patrick Denard: Oh, three to five minutes. Yeah. Yeah. It really doesn't add much with the techniques we have now. And that used to, used to be a big ordeal. When I was in fellowship, it was like a 30 minute thing. It was like, oh my gosh, we gotta do the room massage. It's way easier now just doing it in through one cannula right above, you know, so we can just link the anchors Knotless and.
And, uh, real que like, why not? Right? And you would say why you're worried about okay time. Well, there's not time's gone. There is costs. Okay. Costs, sure. But I'm gonna try to do the right thing. I'd much rather [00:34:00] suck up a, you know, a few hundred dollars for a couple of anchors than have the patient redislocate.
We worried about loss of external rotation. The data doesn't show that that bears out.
Dr. Grant Garcia: I think that's perfect. You just did a study on that. Can you talk about that? 'cause that is the number one thing that shoulder surgeons tell. I say this word about I love re massage. So the idea, uh, will, is if you attach the back of the shoulder, there are some older data that shows maybe you'll lose a little bit of range of motion.
And obviously people are like, then why would you add it? Right? Like anybody wanting to be a skeptic of this simple additional surgery is gonna bring that up. So maybe you could bring up that briefly. Yes. We just need a big review
Dr. Patrick Denard: looking at all the world's literature and found that actually when you compare Banhart and Bank Hart with re and Ladder J, there's no difference in loss of external rotation.
If you think about this. What's going to lo lower, your extra rotation is tightening anteriorly. So you're often gonna get some slight amount of extra rotation loss with a bankart repair because you tighten the capsule, you have to make it tighten. And it was, but the back doesn't actually do anything.
It's not stopping you, you know, doing work in the back [00:35:00] doesn't stop you from extra rotating. Provided you're getting a good view, you're doing something anatomic, right. Um, it's, it's really not gonna limit you.
Dr. Grant Garcia: Well, and I think that's important. What you brought up is, again, you do a lot of teaching. You and I both work with, we've talked about this, will doesn't wanna get too excited about internal Brace with Arthrex.
Uh, but nonetheless, you and I both work with them and you know, one of the things that we are trying to do is to thank the surgery easier, right? Because like, no offense, but you saying three to five minutes in a random guy that does two a year is not gonna look at you and go, well, I don't really care.
Three to five. Good job, Patrick. You do like a make it. Exactly. That's where the future is, right?
Dr. Patrick Denard: Yeah. It's gotten a lot easier, but we need to keep taking steps forward to make it even more reproducible.
Dr. Grant Garcia: And I think that's, I think that's a really nice thing about, I think it's nice when you talk about you got your time for the industry.
The idea of the industry is that. Can we find a way to make it so that, that you coming off, you know, not maybe, you know, no, no offense. Maybe Will could do rum massage, but, so we can [00:36:00] have all of us doing maybe, who knows? He's, he could play Doctor on tv. Uh, but the, um, the idea of doing, having these guys that are community doctors that do a few shoulder surgeries a year, 2030 year, being able to do a re.
I think that it's hard for, I probably want you to explain this a bit better, but how much does it suck to have a read dislocation after you just did a labrum and repair?
Dr. Patrick Denard: I, uh, you know, so
Dr. Grant Garcia: you haven't had it, but I'm saying you're asking what's explain to the audience.
Dr. Patrick Denard: Yeah. Why is it a big deal
Dr. Grant Garcia: to stop it?
Dr. Patrick Denard: What, so the thing is like, it's the patient, right? Because it's the Yep. The, the, the surgery that bothers me the most is instability because you have a young individual who's like their whole life ahead of them. Mm-hmm. So they're often, and they're playing sports most of the time, and when they re dislocate, you're just like, oh man.
And you gotta talk to the parents and they gotta go again and do something. You know? And they have, or, and they, they go through this [00:37:00] psychological response, they dislocate and you fix them. And then if they dislocate again, then there's the, like there change for life. There's actually changes that happen in the brain as a result of this.
So. It's really, it's really a, that's the one that keeps me up at night. So the, the fellows, like, they don't get to do anything in the instability cases, right? They are there to watch those cases because it is just, I feel like the most is on the line in the, in those situations
Dr. Grant Garcia: I've noticed that as I've gotten more in practice, I do more anchors.
Now I am more careful and I'm adding more re massages because like you said. I, I can't handle like a, I can barely handle a 5% re dislocation rate in my anterior labor repairs. I mean, I, early on in practice thought I was so good at the anterior labor repairs till I got a red dislocation, right? Everyone thinks they know what they're doing.
They're straightforward, they're comfortable cases. Everyone's we're in a flow. It's like playing the piano, right? And then you do an awesome killer four anchor repair and they fail, and you're like, I don't know what I did wrong. Right? [00:38:00] And it's the exact same thing. And now I'm doing the wrong massage. It just makes me feel better.
It's just this whole thing about. And then your papers. Now I can quote them and say, you know, there's less, there's no loss of rotation. And my question, I guess to you is, other than, you know, I guess people can say the costs or challenge, why would you, I mean, this is gonna be like the LET for the ACL L, right?
The A LL. You know my question to my patients, I just taught two. I have four people indicated for L LEDs today. Why would you not do the reel massage? That's exactly why not, right? Yeah.
Will Sanchez: Yeah. I want to piggyback on something that, that you said, and, uh, I know it'll resonate with, uh, folks listening. Um, I've coached multiple sports, football, baseball, basketball, and, um, as a parent, as a coach, seeing what, uh, that athlete goes through when they get re-injured with the same injury they had, um.
Besides how the parents feel, the re. You know, the [00:39:00] going through it all over again mentally for these kids, the trauma, the lack of confidence, can they do it again. That whole process is not just starting over, but you're starting way over. And it's not just recovering from the injury, but now. Recovering mentally, depending on what your lifestyle is, spiritually, there's a, there's so much going on.
Mm-hmm. And there's so much work that it takes a community to relift. Uh, most people, other people have resolved. Right. But the majority of the cases that we've seen with athletes getting hurt, uh, whether myself and other coaches, it's, uh, it's detrimental. So I, I can imagine. And. We don't think about it from your perspective, right?
We think about it as a, as a parent or a patient or a coach or something like that, that you are going through this trauma as well. And it kind of all makes sense when you're saying, if we can do something to reduce that, why wouldn't we do it? [00:40:00] And it resonates what you guys are talking about.
Dr. Grant Garcia: Yeah, and I think as the audience listening, I mean, that's who you should be asking a surgeon, why are we not.
You told me I had dislocation, you told me I had a hill sax lesion, and then you're just gonna do a basic repair of my labor, man. No offense, a basic repair. It's still complicated, but you know, like I said, we just start looking in the back of the shoulder. You make sure you get that posterior sling.
Sometimes those are off. Right. Making sure you're adding a massage and know the order and, and again, for the surgeon listening the first few times, yeah. It's gonna be weird, right? There's an order to it. At least that's the way I do it. Maybe different from you. Mm-hmm. But you know, there's an order to it and there's a little bit of an art and three to five minutes is what you'll get down to when you know what you're doing.
Um, but you gotta do it. I mean, you just, and, and nowadays, right, it's that one of the best arthroscopic procedures we can do because we can do these bony procedures through the scope, but they're dangerous. They're hard. It's really challenging and the idea of doing an open ladder J is it's, it's got its own things, but the fact is nowadays we can get away the reel massage.
It's both spectrums, right? It's the patients with less bone loss and even the patients [00:41:00] now with a little bit more bone loss. We've seen the equivalent results and so it's got, it's got such a broad range that it really should be like a reel massage or do we big enough for a DTA or a ladder J, right?
Yeah. That's really the kind of the ram gamut we're at in that, in that ladder. JDTA group, I feel like keeps getting pushed bigger and bigger and bigger. The Ramage is filling the gap. Would you agree?
Dr. Patrick Denard: Yeah. Differently? No, no. I, I'm with you. I'm with you. My only ones are, uh, the wrestlers. Oh. Because they just, they're just crazy.
They just put their arms in the craziest positions and like those ones, I'll lower my threshold and I'll do a ladder j but that's, I had a guy, I did ladder Jay on. He's a
Dr. Grant Garcia: Oh man. Yeah. Oh yeah, the wrestlers are good. Totally, totally agree. I mean, I How about rugby for you? Is rugby the same threshold for you or is it, I don't have a lot of Dr. Patrick Denard: rugby people.
I mean, Southern Oregon is big in wrestling, so it's like mm-hmm. It's the random sports that everybody plays. Football, you know, I mean the standard sports, but [00:42:00] then like wrestling is really big in southern Oregon, so, um, that's, those are my like. High, high, high risk individuals.
Will Sanchez: Can I, can I follow up on a question there?
Uh, are you seeing any significant injuries when it comes to wrestling, uh, with football players? Usually the season is football in the fall and then going into winter, you go into wrestling. Are you seeing anything? Talking to patients saying, well, my shoulder was sore while I was playing football, and now it got exasperated, and now you have a bigger injury when it comes to a wrestler that plays football.
Dr. Patrick Denard: You know, I haven't noticed a ton of that because most of my wrestlers down here are like, they're like year round wrestlers. They're serious. Yeah. So I haven't noticed that, like transition from football to, to, to wrestl. We, we
Will Sanchez: used to see a lot of that back in the tri-state, New York, New Jersey, Connecticut, where you had the football players, the offensive lineman, defensive lineman, linebackers play football, and it goes right into the winter sport for wrestling.
And they would be a lot more wear and tear for [00:43:00] these, uh, for these players. So I was just curious to see if you had, there's
Dr. Patrick Denard: definitely, you know, this, this, this data that shows that if kids don't get enough rest, they definitely have a higher rate of injury, especially if they're doing one sport all year.
I mean that's, yeah, that's another thing. Right, right.
Dr. Grant Garcia: Alright, I don't want to cut off Patrick. We gotta get to his last piece, which is everyone's trying to figure out why I've got pills on one side. Soon. And this thing that says complete surgical nutrition, we thought
Will Sanchez: you had issues. Okay. No, I Go ahead. I
Dr. Grant Garcia: might, I think Chad, GBT, I'm gonna blame them.
Um, but can we pull up that muscle loss after surgery? I, Patrick, so you already told us how you're the jack of all trades in the nicest way possible. Uh, but you keep talking about this complete surgical nutrition. Talk about the importance nutrition. Brief background. I know we only have about 17 minutes left, so sorry to make this so much shorter.
Yeah. Uh, but will you talk about this and how this came to be and now you've got this awesome thing you work on and Yeah. So
Dr. Patrick Denard: when I was in high school, I was an athlete and I started, I was doing supplements and I started taking creatine. And [00:44:00] at time that was crazy, right? I was like reading Bill Phillips's Body for life about HMB and Leucine and all this stuff.
And um, just always had an interest in it. And I started early my practice, you know, telling patients, say vitamin D, vitamin C 'cause I would read articles on it like that makes a lot of sense and patients liked it. And then. For last probably five years, I really just saw the data on protein. And you know, everybody goes through this period where they have, after they have surgery, they have muscle loss.
And you know you're gonna hit that. We'll show that slide disuse. And so we're gonna go through this period, you know, whether it's a mobilization from a sling or you know, a brace for the knee or a cast. Have you ever seen me for cast? They come at it and they look, you know, they look C ctic, right? They look like a skeleton, basically.
So concept here is if you can intervene nutritionally. You from a muscle standpoint, you're not gonna take all that away, but you [00:45:00] can lower the recovery curve, right? You can make the recovery faster.
Dr. Grant Garcia: And that's the green for people who can't see. Is that correct? Exactly. That green line inner
Dr. Patrick Denard: nutrition.
And when you're looking from a muscle perspective, there's a lot of factors, but the biggest thing is your protein requirement doubles after surgery. Most patients get about 30% of their protein requirements after surgery. Specifically when you talk about amino acids, the most important amino acid, there's many that are important, but the most important amino acid for decreasing muscle loss is leucine.
Okay? And you need about three grams of leucine per dose. Most over the counter protein products that you can get, like Costco or whatever, you're gonna get a gram to, maybe up to two. The data on this looks at three grams of leucine per serving. That's where you really make the big difference. So you have to have overall increased protein intake, and you also need to specifically have high amounts of leucine if you're going to recover faster [00:46:00] and.
It's not just healthy or older individuals. Older individuals are more affected. 'cause you know, our muscle loss occurs with aging, but there's data showing that young, healthy adults, you bedrest them, they get muscle loss. If you supplement them with leucine, they get much less muscle loss. So it's not, you know, it's like me and you are at risk, right?
It's not just a 65-year-old, it's everybody. It's another one where you'd say, why not? So I recommend nutrition for everybody. Is there any downside, Patrick?
Oh, sorry.
Dr. Patrick Denard: Go. There's really, that's the thing. There's no, there's no downside. I mean, I'm not, I'm not recommending people are taking anything wild. You know, it's, it's increased in vitamin D, D intake, good for muscle and bone increase in their protein intake, high in leucine.
Vitamin C helps with pain, helps with, um, also tendon healing based on some studies as well. Uh, magnesium, you know, they're simple things. [00:47:00] Mm-hmm. But as a society, we, we eat very, very poorly. Right. And we think we have better, much better nutrition than we do. So I. I've just taken the opportunity to try to lean into some of this and try to help my patients get a little bit better, um, by focusing on this.
I give them a lot of information about why nutrition's important. I do have my own company, you know, like you, like you mentioned on this, but I, I offer all my patients. Information. So, and many of them will just say, okay, I'm just gonna go buy vitamins and get protein. That's fine, as long as they're doing something that's taking them forward.
Yeah. You know, and some of 'em even, you know, they even say, come back and say they, they really changed their perspective, their, how they eat in general. I. So you maybe make an impact beyond the surgery, you know? Um, so I think it's, uh, it's been a, it is been a really good thing, but the data's really clear, you know, it's across all specialties.
Um, show that
Dr. Grant Garcia: one will. The next one? Yeah.
Dr. Patrick Denard: It's not just ortho, I mean, there's, [00:48:00] there's data in colorectal surgery. There's got cardiovascular surgery. This is a study on total knee arthroplasty, supplement with amino acids for four weeks after surgery. What's interesting about this study, randomized controlled trial.
Is that patients didn't just, they did better in other terms, um, this, but this is strength. And what's interesting is those that supplemented, they did better at two years as well. Okay? That was the big difference in strength. They had earlier outcomes that were better, but what's interesting about that is it's not like you're going to, what this would say is that you're not necessarily gonna get there eventually, regardless.
It would suggest there is a critical period you have to recover in, in which you're, if you want to get to the ultimate best spot, right? So I think it's really important that we're, we're talking to people about, um, these options so that they can not only recover faster, but get to the best possible outcome long term as you're seeing [00:49:00] here.
Dr. Grant Garcia: So I have a question for you on this one. So this is a, this is a really interesting point. I had two patients today brought this up. I was talking about, you know, myself, realizing I got injured and had a recovery and realize I was kind of down still after a year. You don't realize, people always say like, I always say this first six week visit, this is like the critical one, right?
Like, you've gotta see how you're doing. Like this is how, this is trajectory for the rest of your thing and you slack off there. It's kind of those people, you know, those people come with a stiff shoulder at six weeks. They're not gonna be the same as your person that comes in. They're trying to go crazy and they feel really good already.
You know, they've worked their shoulder a bit more with PT or whatever. It's different animal than nutrition. But did they, when did they stop the supplementation in this? Do you remember? Was it a roughly a timeline? They were, this was
Dr. Patrick Denard: four weeks. This was just four weeks. Four. So they, so they gave the supplement, um, day of surgery, four weeks on.
And, um, again, there was other, other things they looked at. This, this graph we're looking at is just strength, looking at two years, but they're. The group that supplemented for the four weeks did better in the early period by other metrics. [00:50:00]
Dr. Grant Garcia: So you would say in this case that basically they, they may not have seen the strength difference 'cause at four weeks is hard in general with pain and recovery, but that basically, this is sort of like one of those sneaky ones, right?
Where like you're really gonna notice like you're basically a detriment. You don't even realize it and you're so down that basically like you've built this sort of background information, background strength. That's really not gonna show itself until the two year mark, which is fascinating. 'cause that's, I haven't seen a slide like that before and looking at all the nutrition stuff, so it's really interesting to see.
Yeah.
Dr. Patrick Denard: Yeah, it's, it's really interesting. I mean the, you know, in the, there's a question of period. I mean, some people say, you know, load a couple weeks in advance, take a couple, you know, two to four weeks after, there's some data that suggests that the first three months is critical. But I think the ear, I think the early period is probably the most critical, I think.
Dr. Grant Garcia: What's your recommended, let's say, okay. Patrick or Dr. Ard? I'm seeing you, you're getting my shoulder surgery. Yeah. What should I, I don't, I don't care about, I don't care costs. I don't care about stuff. What's the best thing I should do? What would you recommend?
Dr. Patrick Denard: Yeah, so I would, I tell patients, um, surgery, so I usually schedule out a few [00:51:00] months, right?
So I usually say, yep, see them. I say, surgery starts now, right? So I want you to start taking vitamin D right away. Um, you know, which is a month before surgery at least. But I start, if they're three months in advance, I start taking 'em now, taking it now. I have them load with protein. Patrick, is that
Dr. Grant Garcia: all patients or just your, that's your older patients.
Dr. Patrick Denard: All.
Dr. Grant Garcia: All got it. Okay.
Dr. Patrick Denard: I just don't see a downside for bone and muscle. There's good data for, for bone and muscle for vitamin D. Um, yeah. Sorry about that. I just curious And, uh, no. All good. So then I tell them to load pro with protein two weeks in advance of surgery. So they're basically doubling their protein intake to kind of load up Will, are you writing this down?
Write this down. It
Will Sanchez: it, this resonates because we had a similar conversation with Dr. Uh Jai and he was talking about the preload of the AM amino. Yeah, yeah, yeah, yeah. He's,
Dr. Patrick Denard: he's a big advocate. He's a big, so a
Will Sanchez: lot of the stuff that we're hearing, this is, this is the, the way that everything's going and I absolutely love it.
It's just [00:52:00] something that everyone should hear about this supplementation. Getting ready before surgery and post-surgery. So I hope people are just learning a lot, so I don't mean to to interrupt you. Yeah, keep going Patrick, keep going. No
Dr. Patrick Denard: pre well prehab. Well, I'll just finish the protein thing. So load two weeks in advance.
Continue. I want people to continue for three months afterwards. Okay, they should do a carbohydrate drink the night prior to surgery, you would never tell an athlete to run, you know, a half marathon with not eating for 16 hours. We have patients do it all the time, so if you do carbohydrate drink the night prior, there's good data that says they have faster recovery.
Um, and then I also think those other vitamin things are important. You know, the vitamin DI mentioned vitamin C very clearly helps decrease pain. It may help tendon healing, helps collagen, uh, production for wound healing. So. All those things are, are, are really important. But I think, you know, it's the, it's prehab in general.
We're a little bit slow to this. Orthopedics, other specialties have looked at this, but if you [00:53:00] combine nutrition and the psychosocial preparation, which I tried to do as well, it, it really matters. And we go back to that slide we talked about. We talked about augmentation, but what's funny is. When you really look at like the risk factors that were most important, like nutritional nutrition was a 300% increase in re-tear rate.
We're not talking about Oh yeah, go to the, uh, higher risk of retear, you know, that you see with a large tear or a 30% higher risk, you're talking 300% increase risk of re tearing when you have nutritional risk factors, which is. You know, a, a high, very high percentage of patients, right? And this one here, it's 20% were the moderate risk.
You know, you're talking about really, really big differences that make an impact on people. So, you know, I would argue if you're gonna spend, you know, 500 bucks on PRP, you're, or you know, a couple hundred dollars in nutrition, your money's better [00:54:00] spent. If I'm a patient and I have to pick, I wanna do it all.
But if I have to pick, my money is best spent on nutrition. Based on the data.
Dr. Grant Garcia: That's an ex, that is an absolutely excellent point. 'cause I have probably same as you, but you know, you have various options afterwards that people can choose somewhere beforehand and they always, or or people come the office, they're like, I want this or this and I want this and I don't want a budget, so I don't wanna spend on certain stuff.
So that's a really good, important point to bring up because I think. It's like when we talk about surgeries, right? Like, this part of the surgery is important, this is the extra credit part, right? We're gonna try to do everything for you the same way post-op, right? People have to make choice. Some people don't care.
They'll do everything. But that's not the way life is for most of us. Uh, and so as a result, the idea is that the nutrition, if you, so in your ca in your opinion, of all the things kind of post and pre-op, extra, not, you know, uh, you do your surgery, you do your patches, you do your biologics, or you do whatever you wanna do.
You. For you right now, priority is nutrition. Is that correct?
Dr. Patrick Denard: So I actually have now my instructions prioritize it and [00:55:00] I'll say, here's like, here's tier one, here's tier two, here's tier three. Yes. So for rotator cuff, let's say tier one is benzoyl peroxide, right? Low cost, lower the risk of infection, but that's all shoulders nutrition, and I like cold compression.
Okay. My next thing that I say I would do if it's me that I, but I would add PRP. Okay. And then if somebody really wants to get into it and they have a cash pay situation, then I talk about bmac, allograft augmentation, those kinds of things. But I think the biggest bang for the buck on the data is really those simple, big things at the beginning.
Dr. Grant Garcia: Do you, in your opinion, is you think that the bone marrow aspirate is better than the PRP? Or is it just that you kind of, the idea is there's obviously more. Potential mechy cells in the,
Dr. Patrick Denard: yeah, I think there's potential higher concentration of growth factors. Right. Okay. I don't think we, we don't know. We have three studies.
We [00:56:00] have one study from Hernial, which said that's a,
Dr. Grant Garcia: yeah,
Dr. Patrick Denard: we have Brian Cole's study, which, you know, it's really like, you gotta dive into the details that show big difference. And then we have the database study that says there's a lower risk revision. If people are kind of like, what do I do? I say, well, there's tons of evidence in PRP.
I would probably do that. But, um, if it's a larger, massive tear and they're kind of on the fence and they're interested in it, then I'm saying, you know, you're not gonna be worse off the bmac. It's, um, you know, and they're willing to spend, I'll, I'll do it for 'em. But PRP like is a no brainer
Dr. Grant Garcia: for me. Got it.
This is awesome. Well, will, do you have any more closing questions as much? I told you I could do Patrick another hour, but I think that Instagram Go nerd it
Will Sanchez: out. You went full nerd. I got important stuff like I, you know, the fastest growing sport in the country's pickleball. What has, you know, Dr. Denar been dealing with and Pat like, I've got good stuff here.
You got too nerded out. Dr. Denar,
Dr. Patrick Denard: we just submitted a [00:57:00] paper on pickleball actually.
Dr. Grant Garcia: We didn't even get into nutrition, prp, he's got it. Everything. Yeah. That's funny. Yeah, I know. Hey, what, what's the future for you on this stuff?
Dr. Patrick Denard: Uh, future, um, I mean, shoulder arthroplasty. I'm really interested in getting to an optimized convertible glenoid.
That's like, if I had like one thing that I wanna like, help develop and, you know, and like, you know, my last like kind of thing in my career, that's what it would be. Okay. Um, I think you're gonna see a lot of, you're gonna see things like these algorithms that I took and everybody's just gonna have little machines that calculate stuff right.
As we have better data. You know, 'cause it's like, it went from like differential diagnosis to like algorithms to, it's gonna be much more sophisticated individual decision making. I think that is exciting. I think that is scary. Yeah. I think it's exciting because it kinda raises the bar for everybody or raises the plane, [00:58:00] you know, uh, this playing field, like where everybody can perform at, at a certain level.
'cause so many questions. As you know, surgeons will ask, well what do I do? Right? 'cause they don't have all this information in their head. Well, they
Dr. Grant Garcia: don't have the experience of the volume either that you have. Yeah. Right. I mean, it's just, just a different animal.
Dr. Patrick Denard: Right. But what's scary is limiting our ability to do things.
We talked about insurance early on, and you wonder, okay, are these guidelines or these, you know, it's the Gatica movie, right? The guy who's like, he has the genetic disease and he, he can't perform, and of course he outperforms it and, but we might get in situations where you lose the individual patient. So I'm a little nervous about that.
Got it.
Dr. Grant Garcia: I, I wanna ask you more questions about this, but we are at one minute and 15 seconds before our timer's up the, uh, well, will, do you have anything else to add? Movie, Will Sanchez: we, we got a Gatica movie reference in, we didn't even get to, if he's going to Coachella in 2026. I'm getting my tickets, so I, [00:59:00] another year off.
Dr. Patrick Denard: Yeah. Yeah, I'll be there. I've gotta go. It's on
Will Sanchez: my list. They come out May 2nd. Uh, Coachella tickets. So these are our priorities here. You gotta get those. But Dr. Nor, thank you so much for your time. I know we're wrapping it up here. Dr. Garcia, say something nice before we say goodbye.
Dr. Grant Garcia: Patrick. Awesome. Thank you so much.
Really great having you on. Thanks for showing yourself. Anybody listening, complete Nutrition is awesome and you gave, you heard it from the expert right now. So thank you so much for everything.
Dr. Patrick Denard: Thanks guys. It was very fun.
Dr. Grant Garcia: Alright, thank you.
Audio Transcript
Dylan Newcomer: The Future of Baseball Rehab

Dylan Newcomer: The Future of Baseball Rehab
Will Sanchez: [00:00:00] Welcome everybody to Sports Doc Talk. I'm Will Sanchez, along with Dr. Grant Garcia, our orthopedic surgeon, sports medicine specialist. Really hyped to see you today. How are you? You got the fly logo behind you, so you must be really excited about today's show. Super
Dr. Grant Garcia: excited. I mean, this is baseball, baseball season started and now I got my logo chat.
GPT did a great job. I, I hit in a bunch of driveline, which we'll get into a minute. This is what it shows up with. So it thinks that that's, this is the, this is the future of baseball right here. So this is awesome.
Will Sanchez: We're really excited about the guests that we have today. But before we get to, um. Let's talk about our friends at the Recovery Shop, Dr. Garcia. I know you utilize them a lot, your doctor friends and [00:01:00] everyone else in the industry utilize them, but let the, let everyone else know how important the recovery shop is.
Dr. Grant Garcia: Yeah. So I mean, again, big thanks to our sponsors, but you know, this is a day in and day out. They deliver for our patients. The patients are pleased.
They get products that they can't normally get. Um, and it doesn't matter if you get your surgery done in the state of Washington. You go from Idaho, people who fly in for surgery with me, they're able to still get access to these high level products and really any surgeon that want gives their patients the sort of next level recovery.
They have it there. They have nutrition, they have certain machine options. They can adapt whatever you need and whatever your sort of patient population is, they can adapt to it. So reach out to Mike B If you're a surgeon, if you're a patient, reach out to them too and say, Hey, my surgeon's doing this. I'd be interested in having those products.
Because it's a pretty easy setup. So anyhow. Thanks guys.
Will Sanchez: Yeah. And you know, let's, uh, let's, before we get to our guests, we wanted to share with everyone just our teaser for the show. Let's get right to it. Let's do it. And [00:02:00] if, uh, if I could get this to, uh, work over here, we may, maybe we can't. Uh, so let's.
Get going here. Be nice people. Come on now. Here we go. Okay, we're cooking with gas. Let's go.
Baseball's number one training system has gotten even better. Our athletes have done some cool stuff over the years with the
Dr. Grant Garcia: first pick, the Cleveland Guardians Select Travis Bana, and some would be satisfied with results like ours, but not us.
Introducing Training 2.0 from Driveline. Training 2.0 is the most advanced player development system baseball has ever seen. And it's not close. Of course, it starts with the things we made famous,
but it's become so much more than that. Training 2.0 gives athletes a clear plan to achieve their [00:03:00] goals. In a way that has never been possible before. It starts with an assessment to understand exactly where you stand from there, that precise picture allows you to execute personalized training that builds on your strengths and attacks your weaknesses head on, improve your command or your contact, and become more durable by knowing how hard to train or how hard not to.
Every single day with training 2.0, you can also train from anywhere in the world with the only app built to give you your very own sports science team right there in your pocket. So when the last day of your baseball career arrives, you're going to have to be honest with yourself. Did you do everything you could or did you settle for something less?
Training 2.0 available only at Driveline.
Will Sanchez: I'm [00:04:00] hyped. Let's bring them on. Let's get Dylan. Newcomer on the show. Dylan, welcome to the show, uh, physical Therapist at Driveline Baseball. First and foremost, thank you for taking some time to join us today. Thank you. We're really excited to have you and to talk baseball, to talk physical therapy, to talk at all.
Um, once again, thank you for, uh, joining us today.
Dylan Newcomer: Thanks for having me, guys. Very looking forward to, uh, a good conversation here.
Dr. Grant Garcia: And I, I think, I think before we, you know, when we introduce him to understand, guys, this is different than, we've had a lot of athletic trainers, we've had a lot of physical therapists, but this is a different animal.
What Dylan does is extremely niche, right? Baseball players, baseball. That's what he does. And he is lives, it breathes it. He works closely with Drive Line. You can talk about his relationship with Drive Line, but this is a, a group that, that's what they do, right? You're a baseball player, you drive to Kent.
To have driveline take care of you and you will there, there are many players I take care of. [00:05:00] They will spend the extra amount of time, effort, money, whatever you say to go there, to have this type of facility and have these type of people like Dylan to do this. And Dylan's really one of the, the key foundations of this sohow.
Dylan, tell us a little bit about yourself. Uh, so the audience can learn more about this. 'cause I'm sure if you've never played baseball before, you're like, what the heck is driveline? That video was sick, but I have no idea. I just, I've never heard about this, but this sounds so, so cool.
Dylan Newcomer: Yeah, I mean, driveline is, well before my time is whenever it started, uh, I think back in 2012.
And, uh, you saw a quick clip in that video of some of the. The early days of what made Driveline famous. But, uh, it really started out as just a, a training company down in Puyallup that made athletes, uh, better than they were when they, uh, walked in the door. They were very velocity driven. Um, they've lived in controversy their whole life.
You either love 'em or you hate 'em. Um. But you, there's no doubting that they have influenced the game to a, a substantial degree. You probably can't go [00:06:00] into a major league clubhouse without seeing one of Drivelines uh, weighted balls somewhere in there, or at least one athlete wearing a pulse sensor or things like that.
So, um, it's a very influential company and, uh, I got. The privilege to become a part of it in 2022. Um, but before that, I was a, a Mizzou physical therapy student back in Columbia, Missouri. Um, and I actually was a, a strength and conditioning coach. That was my background, um, back in the day. Uh, and I was doing that with a driveline. I. Pitching, uh, certification. So I was, I was kind of doing a dual role back there. I was, I was being a strength coach and throwing coach and, uh, helping athletes figure out how to navigate that world from a performance spec, uh, side. But, uh, whenever everything wrapped up with PT school, I came out to Seattle. 'cause I had to just be part of the company that, uh, has been in such an influential part of my baseball career and my professional career. So, took that over in 2022 and I've been here ever Si ever since.
Dr. Grant Garcia: Okay. And Dylan, so tell us, tell us about how you guys like integrate, right? Because it's, 'cause then [00:07:00] obviously you work with driveline, you to the players and it's kind of like a symbiotic relationship, at least from my understanding.
Describe it to you, kind of like, how does that work with you? Because obviously you have this extremely premier facility organization that's, you know, and we will go into it, but it's not just now in Seattle anymore or in, uh, Kent. It's, it's expanded. So.
Dylan Newcomer: Yeah, so my relationship with Driveline is, um, I'm the medical provider and you know, driveline is not a medical company, so they can't outright hire a pt.
Um, and so I own my own clinic. I run my own clinic, and we have this nice symbiotic relationship where I take care of their athletes. I get to see some of my own private athletes outside of here. You know, I get to enjoy the, the odd ACL or low back pain or something like that. Um, but 99% of my time is gonna be spent on those, those baseball athletes and, and taking care of the athletes inside Driveline.
And it's also expanded, like you mentioned. So they, they've opened up to Arizona, so they're in Scottsdale. Um, and they just opened a Tampa, Florida facility. I. [00:08:00] I think it was in October of this past year. Um, and so my goal over the next year or so is to expand down there as well and get a PT stationed at each gym.
Um, and yeah, we're just gonna be taking care of all the pro athletes, the college athletes, youth, whatever comes through the doors, make sure that everybody's in a good, healthy spot and trying to put, uh, rehab initiatives in a really, uh, trying to push 'em through at a really high level.
Will Sanchez: Dylan, um, when, when was the first time that you heard about Driveline?
For me, I, I know that Driveline had, has been around for a while, but for me, the superstar, especially at the time that was talking about Driveline, was, uh, was it Trevor Bauer? Right. I. Yeah. Trevor Bowery. Yep. And, and he was like a proponent, and I know his dad is an engineer and was talking about mechanics and all these other things, and it seems like driveline and that relationship at the time really was a perfect cohesion, a perfect marriage.
Um, and really that, like I [00:09:00] said, as, as, uh, as someone that worked with Major League Baseball, I used to work with the New York Mets and being in, in that kind of, that world, when he started talking about it, that's when I was like. Who's Driveline baseball, what's going on? Mm-hmm. And all the incredible things that, that was happening back then. I, I guess that's what, 2018 maybe roughly when Bower was kind of talking about this. So what was your experience, or, or when was the first time that you heard about Driveline baseball, uh, that really kind of, you know, pulled you or gravitated to, uh, working with them?
Dylan Newcomer: Yeah, so my first exposure wasn't actually Trevor Bauer, but it quickly, quickly became on my radar.
Um, we had a student athlete at Mizzou that came up here to train, uh, one summer and he came back and was like, here's a ply ball. This is what we do. This is the drive line program. Um. He introduced it to the pitching coach at Mizzou and the director of physical therapy for the Mizzou healthcare system.
[00:10:00] Yeah. And because of that relationship with the, the director of PT I had as a strength coach kind of in the healthcare system, he was like, we gotta get this here. So, um, it was pretty much just like, Hey, you gotta learn what Jive Von is right now. You gotta start teaching it because this is gonna be. Kind of the evolution of the game.
Um, and so that was kind of my first exposure to it. And then ever since then, it's just been kinda living and breathing it.
Will Sanchez: Got you. Gotcha. Dr. Garcia back, we lost you for a second,
Dr. Grant Garcia: but we, I don't know what's going on with my internet connection, but hopefully I'll make, I'll survive the whole podcast. So anyhow, the, um, can you, can you tell, so this is awesome.
I mean, I think what we understand is like as orthopedic surgeons, right? Like I see these players. Even if you're team position when you're in the dugout or you're in back out back thing, you're seeing the players and they get injured. But really that like gap between injury and the game. We're not really seeing what's going on behind the scenes and, and, and working now with Dylan pretty closely, you know, there, there's a lot more [00:11:00] that goes into us and we know this is, this is a, this is like, it's not really the best kept seeker 'cause a lot of baseball players know about it.
But like, this is really what people do behind the scenes or say how do you get better? Can you describe to the, the audience. First off, obviously we, we go into all the things you guys do, but really why is baseball so much different? Right? Like there are other companies that do different things for other sports, but nothing at this level really.
There's just not as much technology used. We always talk about all the cool things in football and cool things in, you know, basketball, but there's nothing to the level of precision and sort of mechanics that we care more about in baseball 'cause it's such a complex. Uh, and also for valuable situation, right?
Like a, you have very few places where the pitcher is so much a part of the baseball thing or the swing. So maybe describe that a little bit more. Like what, what makes baseball so unique and why, why baseball?
Dylan Newcomer: Uh, you know, I think there's a couple, couple different things we could go there. Um, I. It's definitely one of the most quantifiable sports, and I think that's kind of the [00:12:00] obsession of driveline is like, if we can quantify it, we can train it, and if we can train it, uh, we can make the the player more valuable.
Um, so I think that that has a lot of, uh, you know, val, you know, interest for especially high level players, but even at the, just the basic level, it's just been a passion project for everybody here. It's just the, the sport that. We all love. Um, but yeah, baseball is just that very scientifically driven, easily quantifiable, and the technology is getting better every year.
So, um, we just keep trying to try, find ways to push the industry forward, to figure out, A, how do we make players better at their sport? But B, how do we also keep them safer while we're also making these gains at the same time?
Dr. Grant Garcia: Yeah. I think that's also interesting that, you know, one thing is like a lot of the other sports that people do, no one asks me, they're like, Hey, I, I'll just go to the best one in the area.
Right? Best PT in the area, or best a TC in the area. They're like, I'm, I'm fine. Just gimme the local number. But the baseball players, when they come in to see me, they're like, gimme the best one in the state. [00:13:00] Gimme the best one that's within two or three hours. Like, we'll drive, but I want like the baseball team.
Right. Like, I don't want anybody that doesn't know what I'm doing. Like my son's a pitcher, he, he's gonna play college. Like he, I need someone that does that. And so that's what's I think is really cool about having drive on. But it's also unique about the players, right? I mean, you could probably have a lot of people that come in like they already know about you.
They're so honed in and they're so motivated. Like that's a, that is probably a nice piece of for you guys, is that you're already getting people that are motivated to do it, right? They're not coming in, they're like, Hey, I don't really know what I need. I just kind of wanna go back to running, right? They, they're, these are people that really care about going to the next level.
Dylan Newcomer: Yeah, I mean, driveline is definitely a financial investment and it, it, it's, it's definitely the facility that you go to if you have, it doesn't matter what your, your desires are, but if you're committed, if, if, like, if baseball is something that you absolutely want to get better at and. You know, maybe you don't have aspirations of going to pro or whatever it may be, but you wanna play at high level in your college, uh, or [00:14:00] you maybe want to get to Indy ball.
Like, it, it is the place that like, if you are going to invest in yourself, um, there's no other place to really go. Um, I. And so especially with the rehab side, yeah. We get guys that come in a couple hours away. We will drive here. And I think it's just because baseball is so very niche, uh, when it comes to, to rehab.
Um, it's never something that you really discuss in PT school. You, you don't, you don't get trained on how to rehab a baseball player specifically. And, and maybe you'll discuss about a return to throw program, but more often than not, it's, it's, everything you learn is post grad. And so. If you're gonna find somebody that's a really good baseball rehab provider, it's somebody who kinda lives and breathes that sport.
Uh, they, they have to really go after it after graduation. It's not something that we're all trained up on.
Dr. Grant Garcia: It's interesting. Will you hear this? It's kind of the same way as we talked about this with the, with the surgeries, right? Like in Dylan knows this, right? There's only certain people. That you want doing [00:15:00] your Tommy John thing, right?
It's just not that many numbers out there, right? Like of all the surgeries we do, the UCL is just so much less common. And then even in training, you know, unless you train, if you train, unless you train with a team, you need to train with someone that does a lot of the MLB, you know, college level athletes, but you, it's just not a common thing that you see unless you sort of, with the people that are doing the most, you know, Romeo, you have.
Tro you, David Che, you know, you name it, the list can go on, but you, you gotta see high volumes. And those may seem like normal volumes until you get out in the real world and realize that that's just an anomaly. Right. This is just the, yeah, the select view. It's the same way with the physical therapy. So it all links together.
Uh, and you know, I think Will's heard this at nauseum, but can you, um, you, me, you brought that slide back up again about Driveline. Can you talk Dylan A. Little bit about the, the old versus the new principles? Because I. I don't know enough about this stuff. It's just, it's just really interesting to me.
Like I understand some of it from hearing from the players and from you, but can you talk about this sort of past and the future, and we'll get into [00:16:00] that in a little bit.
Dylan Newcomer: Yeah. And you know, driveline is, is principle driven. And what I mean by that is, um, we go back to the basics of, of sports science and what that means to like actually train an athlete.
Um, there are gonna be methods and fads that come along, come along, you know, this is the thing that gets you your next five miles per hour type trick that, yeah. Takes the trend for fi you know, six months to a year, we're never gonna be that company. We're always going to rely on our base principles of how, um, you know, we stress an athlete, we allow them to recover and adapt and, and just go down to the, the foundation of that.
But in the past, driveline was trying to solve the problem of like, how do we make pitchers throw harder? How do we make them, you know, a more valuable asset? And that's really where. The first decade of the company lived is, is velocity driven. Um, and you saw this quick, uh, for brief moment in that, that video that we played up front, um, now we're looking at how do we train command.
And if you recall in the video, there was a little board with like a, uh, projected [00:17:00] catch catchers met and you saw where the ball popped up on the screen. So we're, we're trying to measure command. Um, we have an intended zone tracker is what we call it. So we're putting up, you know, where do we want the ball to go?
Where does it actually land? Can we measure that missed distance? And then can we figure out if we can identify training strategies that makes that missed distance tighter, we get better at the command. Um, and so that's kind of our new goal now as we, we've, I. We understand velocity, but we don't understand command as the large.
And now we can start taking that data and comparing it to motion capture, strength, power, all of that stuff, and seeing what metrics actually matter when it comes to making that, that skill more impactful.
Dr. Grant Garcia: And, and, and so Dylan, you're talking about command there, there's a numerical value you guys are learning to put on command, is that what you're saying?
Yeah. You guys are trying to quantify it like you keep quantifying everything else. 'cause that's the way to get better, right? You, you're just like, oh, your command was better. It seemed better. That doesn't work.
Dylan Newcomer: Yeah, exactly. Instead of just the, the [00:18:00] old. Eyeball, IDAR is kind of what we used to say for, for velocity.
Um, now we're, instead of eyeballing the command, we're actually measuring specifically how many inches are you missing on each pitch profile? What's the average missed distance that you have? Um, and then we can start to quantify. I. Do your mechanical changes from the motion capture lab over a six week or 12 week retest cycle, do those correlate with better command or, um, does your strength, values, uh, and your rotator cuff or your forearm, or overall as an athlete, does those correlate with better command on average?
So yeah, we're trying to quantify everything that we can about it.
Will Sanchez: Dylan, how, how are you utilizing, you know, we always talk about future tech, uh, on the show, but how are you utilizing now with ai, I implementing that in some of, you know, the new technology for, you know, driveline and whether it's. The analysis of a just say, you know, player A and the development from day zero to day [00:19:00] 60 and you know, seeing those mechanics, obviously seeing whether it's the speed, the command, the strength, um, what are some of those conversations and just try to expand on that conversation.
Dylan Newcomer: So. I'll give you a quick example of one of the most recent use cases we've had. I mean, it is really infiltrated every part of Driveline as an organization where it's, it's making all of our, you know, calculating processes go faster. It helps us spitball ideas faster. Every, we have a whole staff of, you know, excellent coders with, with the founder of the company being a master coder himself.
So it's really just streamlining those processes. But, you know, one good example is we, we recently came out with, um. A feature in our Driveline app that is using computer vision to be able to do the same thing that force plates do in terms of measuring your power, uh, whenever you're doing jumps. So we put a sticker on you, we let the camera track you, and then we, we used AI to learn how to do all of this, um, that it basically built out our [00:20:00] entire code and then we validated it.
So we can just take a video of you at 60 frames per second and we can get the same data that we're getting from our vault force plates. Um, so what that means is that whenever athletes aren't in gym. We can still measure their progress and, uh, especially in the weight room, you know, and then over time we're, we're using it to solve all the issues that we have had in terms of if we have a question, where do we go?
We go, we check chat TP GPT first and see what kind of answers we can get from it, and then we go from there. So it's really just a stimulator, if you will. It just helps us make that next step faster.
Dr. Grant Garcia: That's awesome. And, and, and do you use any, do you think that's kind of helped you guys with your kind of future projects too?
You know, I mean, like you said, you're using the football, like how we wanna measure this, how do we do this? And you're using chatt, but now are you using it for like, Hey, what's the future? Or is that kind of, how is that, how do you guys determine that? I mean, how are you going, what dictates what, what's next for you guys?
Dylan Newcomer: That's a good question. Um, I. [00:21:00] You know, it's always whatever nobody is thinking of, I think is probably what's next for us. Um, that's kind of what, what Bodhi always, uh, Kyle Bodhi, the founder, he's always kind of pushing forward, is that like we are looking for to solve the problem that nobody is kind of thinking of just yet.
Um. And that's kind of where this command one, the command one's really, really recent, uh, within the last year that we've developed it. So we'll see kind of where that takes us. And then, you know, what problems come up next. Maybe this whole, uh, torpedo bat thing is a really interesting issue to, uh, to start solving.
Will Sanchez: We'll definitely get into that. Um, one of the conversations that we've had with, um, whether it's coaches or parents, is, um, what can you know little Johnny do or not do at certain ages? So with your involvement with professional college, high school, amateur, what are the barometers there? What are some of the conversations, [00:22:00] whether it's.
With the client or internally when you have, uh, certain players, um, you know, wanting to do certain exercises, how, how do you manage that? You know, saying, okay, you know, if you're under 16, you can't, you shouldn't be throwing a curve ball or breaking bolt. Like how do you determine that or, yeah, I think what
Dr. Grant Garcia: Will's trying to say is, you guys.
Do you a, like, how do you age manage as like, is who dictates what, right? Like even when I did my surgeries, I have a dictation in there, what I want you guys to do, but you guys do a lot of it. I trust you guys to make decisions on your own as experts. So how, how does that, how does that work for you guys? Is that what you're asking? Will
Dylan Newcomer: Yeah,
Will Sanchez: go ahead Dylan. You you got it? Ready?
Dylan Newcomer: Yeah. So. One of the things that we're always gonna consider is the skeletal maturity of the athlete. Um, and that's probably step one is like we've gotta make sure that we're not putting them in any, you know, extremely harmful positions based off of that specific factor.
And so that 15 to [00:23:00] 16-year-old group is definitely kind of that transitional age. And beyond the skeletal maturity, we're also looking at. You know, how quickly have these athletes grown in the last year, because that's always kind of an injury. Spike areas is, you know, those rapid growth spurts. Um, and, and when we get younger, we're also just looking at how do we, how do we look at a long-term athletic development model?
Um, and, and I. Some of the things that we do with our young kids is gonna be more of the gymnastics and calisthenics based stuff, like learn how to manage your body. Um, we're not necessarily trying to have you do a velo program at at 12 years old 'cause nobody cares about how hard you're throwing then.
But what we do care about is that you're developing your natural athleticism and that you're stacking kind of year after year of consistent. Consistent training and consistent throwing, so that way you develop into where we want you to be. Um, puberty's another big one, right? You can have that 17-year-old who still looks like he's 12 and that 17-year-old who looks like he's 25.
Um, so we're always kind of taking that into consideration as well. Um, [00:24:00] and then, yeah, like our early bloomers, we always, we always have to make sure that we aren't, you know, exploiting to an extent. We wanna make sure that they have a solid training plan, a solid foundation underneath them. Uh, and that we are, we're not doing the showcase thing where just 'cause you throw hard meaning and take you to every single showcase and try to make you, you know, throw 95 every
Will Sanchez: week.
When, when you, when you have someone on the bubble like that, do you have internal conversations saying, I know he's this age, but he's hit puberty. He's big, strong things like that. We think he's ready for the next step. Uh, what's the process, uh, for you guys at Driveline when it comes to something like that?
Dylan Newcomer: Yeah, if we have one of those early bloomers, it really does become this more collaborative approach of like getting the parents involved, getting the coaches involved, setting out this, especially when we know this kid has college potential or potentially even beyond. It's, it's what do we need to do over the next six months, 12 months, 18 months, to make sure that A, we're capitalizing on what you can already do, but B, [00:25:00] safeguarding against, you know.
Excessive use or anything like that. So we, we go back to the, the, the training foundations and our principles. It's, it's that we need to physically develop you first. We need to make sure that you can handle the stressors of the game. We need to make sure that we are monitoring and managing your workload of throwing.
And then we're also having those conversations of. You know, what are you doing outside of here? Because athletes that are, that we're talking about right now are a part of our academy program. So they're here three, four days a week, um, training. Can you explain that? All those things? Can
Dr. Grant Garcia: you explain that academy program thing?
Dylan Newcomer: Yeah. So the academy is basically, if you would imagine your, um, your typical like nine U, 10 U, 12 U 15 U type teams that you would see for like travel ball, um, except we are taking it. And kind of flipping it's on its head where instead of it being a travel ball team where they just go play, play, play, play, play, we're looking at it from a developmental pers perspective where it's train, train, train, train, train in terms of develop yourself as a physical, [00:26:00] uh, specimen and, and make sure that you're getting in the weight room and doing all the things from an arm care per perspective that you're getting on a managed throwing program that's consistently, uh, being applied throughout the year.
And we're. We're monitoring your workload, and then once we have those foundations, we go out and play. Doesn't mean we, that we have the best players in the world, but we're looking at it from a, a developmental standpoint of how do we take any player that comes to us and make them a better version of where they were when they walked in the door?
Dr. Grant Garcia: Well, and I wonder if that, I mean, that's probably what you guys feel, but to me, if my, uh, son or whatever, my daughter's trying to play baseball. And I hear this, you know, to me, I think about it as like injury prevention first show off second, right? Like, which is, which is opposite of the way I think a lot of people think, right?
Yeah. They're like, Hey, let's get my kid in front of the scouts as soon as possible. But to have a place, a, a group like yours that's so focused on injury prevention, rehab, perfecting technique, you know, we'll, we know this from like, they don't get any breaks, right? Or the coach is like, throw hard or throw hard or No [00:27:00] rest for you.
No rest for you. Versus the like, rest, train, strengthen, then throw. I mean, you probably see all the time, but do you have a lot of experience where you know someone, I mean, I know these people that they kind of give up on who they're working with and they're like, I need somebody else, and then I'm sending 'em the drive line and then they kind of get all fixed, right?
It's just like going to the doctor, but it's a doctor of physical therapy, right? They all messed up. They have mechanics off. They've been told just to throw as hard as they can, and they have, they're, they're terribly sloppy. And now they come to you guys and it's like, let's start all over again. Let's break this down.
Right? And so is that what you guys get too? Is that, I mean, that's, that's must be the feeling some of these parents get. I think,
Dylan Newcomer: yeah. I, I would say that happens a little bit less frequently because we do have, we've had these, the kids that are in our, are in our academy program have typically been around for a while.
Um, got it. And so it's been running for a couple years and, and we definitely do get, do, get new athletes every year. But, um, it's more of that. That we've had you since you were young and we've helped you develop over a long period of time. And [00:28:00] that's kind of been our goal there. Um, and so occasionally we'll get those stories of like, Hey, I've always had pain.
I. Alright, we have to go back to square one. Why are you having pain? It's because of X, Y, and Z. So we need to address X, Y, and Z before we even care about getting you back into a throwing program or anything like that. Um, so occasionally we do have to hit the reset button, but I would say for the most part our athletes are kind of in that consistent year round plan of how do we keep you healthy and developed and ebb and flow of the season of play.
Dr. Grant Garcia: And then I think this one's always a big one will ask me, but. How do you guys deal with the parents? Mm-hmm. So the, in my office I told Will that I'm known for when my doc, when the docs in my office get a baseball player and there's like two or three, two or three or four parents who knows how many parents that could be in the room.
And they're all hovering over the player 'cause they want, they wanna know he's gonna get hurt, right. And I'm the doc, they're like, this is Garcia, he'll take care of this one. I gotta go in there and try to address multiple people that are either frustrated or [00:29:00] upset. 'cause they've had different opinions.
And a lot of the parents, I'm not gonna name names, but a lot of the parents in general like to dictate the care. So how do you guys deal with that? Because, I mean, you're seeing them more than I'm, I see 'em for one short visit.
Dylan Newcomer: Yeah. Mm-hmm. Well, the nice thing is, is that when they join the academy, they, they, the parents sign a contract that we are the, the experts basically.
And like we are absolutely gonna involve them in that, in that process. And, but we are never going to put the, the player at risk. Um, so if we say that, Hey, uh, your son has had pain for throwing, uh, these are the things that we need to do. All of the coaches are on board and gonna back us up on those decisions, and this is gonna be the best thing for your athlete.
Um, and we're gonna, what, what? We're happy to sit down with the parent and walk 'em through every decision that we make. Um, luckily though, we don't, I think they realize innately that like.
This is probably what's best for the kid. And we, we really haven't had much issue with any parents in terms of, um, [00:30:00] you know, backlash or anything like that.
Uh, or, uh, a frustration with the plan of care or anything generally, if the kid needs to shut down from throwing or anything like that. We're all on board. We're all on the same page and we're, we're happy to explain our reasoning and, and I think that's really the key there is if I have to take an hour and talk to a parent, I have the luxury to do so, so we'll do it.
Dr. Grant Garcia: I, I think that's key. 'cause I mean, will will go into this. He knows he's got kids, but like, it's frustrating if you, and if someone doesn't have time for you, you are like even more frustrated, right? Like, and with you guys, they're, they're paying a premium to be with a high level place like yours. So for you to be able to give them time, it's great.
And that's also something that a lot of the PA parents need, right? These parents are like, gimme the best. I don't care what it's, I want the best person. I want the person who's gonna take care of me. And that's why it's nice for me as a physician who takes care of a lot of baseball players. To send 'em to you guys knowing that you know that they're gonna get all that they need.
Right. There's not, like you said, the fact you guys are able to, you're able to say that topic. And I know Will's heard me say the fact you're able to say that most parents are very pleased [00:31:00] with our care and they don't involve themselves very well. Shows you guys have established yourselves as a very strong program. 'cause that's a, that's a, that's a hard thing to be able to do on a day-to-day basis.
Will Sanchez: Yeah. Uh, quick question here. Um, you, you hear different. People say different things when it comes to, um, playing one sport all year round or playing multiple sports, has your data shown any numbers when it comes to someone that, let's say, will pitch, you know, most of the year, or you have a pitcher.
Then plays football or track and it comes back to pitching. So do you have any numbers to reflect that, because that's always a conversation within parents, whether, you know, someone plays one sport all year, or is it to have a more well-rounded athlete play multiple sports, and maybe we're just talking more than just pitching, but also body development and utilizing other parts of their body.
Dylan Newcomer: Yeah, you know. I don't have any data that would specifically [00:32:00] give you an answer, but I can speak to it anecdotally. Um, sure. Probably the, the most consistent thing that we see is, uh, athletes that maybe do play multiple, multiple sports throughout the year. Um, they, they potentially almost get, I. More overuse injuries in a sense.
Those are the athletes that we have to more carefully monitor, that don't necessarily get to participate at the same level as everybody else. Um, you know, if we kind of classify our, our throwing days by either, it's a low intent throwing day. It's just, you know, take it easy catch play. Maybe it's a higher intent throwing day where we're, we're purposely trying to, you know.
Stress the body a little bit. Those are the athletes where it's like, okay, you're in the middle of wrestling season, you're already getting beat up. We don't, we probably just don't need to be doing a high intent throwing day. And in the past, before, you know, a couple years ago when we were just starting this program out and we were, I.
Seeing how things would work out. Those are the kind of kids that would be like, oh, he, he had a high intent throwing day and he also had two wrestling matches, you know, this past weekend.
He's beat up now, now he's down for two [00:33:00] weeks. We need to let him chill out. So, um, it's always kind of, that's kind of the perspective that we get is how do we manage the end season athlete who also wants to continue to train baseball.
Um, so that's, that's kind of the challenging part. The, the athletes that are throwing year round. One of the things that we wanna make sure that we do is that. You can't be throwing a hundred percent all year. Um, so our throwing program is going to have intentionally no throw periods, intentional ramp up periods and things like that where we are managing the workload.
So that way we give them time to recover, we get them ready for whenever it's time to play, but it's never just like go, go, go, go, go where the athlete is, you know, gonna get burns out throughout the year. Great. And then
Dr. Grant Garcia: I don't wanna sidetrack you, but we are, we, you know, time, we see the clock ticking down and we wanna make sure we get all the good questions answered from Dylan.
Um, do you, can you talk a little bit about your experience, kind of with the, the pro level difference versus recreation? I know we have a slide on that if you wanted to pull it up, will.
Yeah. Um, [00:34:00] but I, I think that's important for everybody to hear, right? Because it's just a difference and obviously you're, yeah.
There's also bigger. Risk for you guys, right? You wanna make sure you get these players back. And, and for Driveline, the people are, these players are flying in or they, they're there for the summer, or sorry, they're there for the off season to rehab with you guys Yeah. Until they go back to their team.
Dylan Newcomer: Yeah. I mean, honestly, working with the pros is sometimes easier than working with the kids. Um, the pros have all the time in the world to dedicate to it because it's their job, it's their livelihood. So they, they, they have that. Luxury of being able to spend three hours here and do everything that they need to do.
Whereas sometimes with the kids, um, you know, they've got school, they've got other commitments, they've got orchestra or something like that where they have 45 minutes to see me once or twice a week versus come in six days a week with the pro and and check box every little thing that we need. Um, but. A lot of times whenever you are working with, uh, a professional athlete, especially an older professional athlete, it's probably a little bit more of [00:35:00] the case that I see for the longer term rehabs.
It's like that 30, 28 to 30-year-old who's trying to make his comeback. Um, you're more so managing the mileage that he's accrued. Um, the training doesn't necessarily change. Too much from like a, a, a younger pro and older pro to a degree, but it's more so the secondary considerations you have to take. So managing that mileage, um, of the past, injuries or anything like that.
They don't recover as well. Well, does make you feel
Dr. Grant Garcia: good that there's old pros at 28?
Dylan Newcomer: Sorry. Yeah.
Dr. Grant Garcia: No, it's the we. Thanks for coming.
Will Sanchez: We'll see you. Thanks coming, man.
Dr. Grant Garcia: So. So let's, I mean, let's kind of keep going with this. So like I Do you guys have a different, I mean, I know you guys follow like the protocols, but like I said before, like when I have a patient gonna drive line, I have my Tommy John surgeries, I'm kind of like, here's my protocol.
But you guys are the experts, right? I can only do so many Tommy John surgery. Do you guys see 'em from all [00:36:00] around the area? So do you guys, are there rehab differences for you or things you look differently for from a surgical recovery versus a non-surgical recovery? And, and if so, kind of what are you looking at when you do those things?
Like, you know, you, a player gets injured, he hasn't had surgery, but it's like, let's see how he does partial injury. You know, how, how do you, what do you guys do by that? How does that work for you?
Dylan Newcomer: So I. This is my personal viewpoint, and this is kind of highlighting a thread that I did that got some good traction over this past couple weeks.
But, um, when it comes to a partial injury, I see that almost as, as risky as or, or as demanding as a surgical injury, right? In a surgery we're talking about a, a longer timeframe. 'cause you know, especially in the reconstruction, you've done bone drilling and all of that stuff. You have to let everything heal.
In a, in a partial tear non-op, I think you almost have to take nearly just about the same amount of time, and that's coming from a perspective of like, we have destabilized that joint that that ligament is no longer as as strong, so we need more time to build up all of the protective [00:37:00] tissue. Around that elbow, not less.
And sometimes I think, um, the standard protocol of six to eight weeks of rehab and then try to return to throat is just too short. We need to give potentially a couple more months. And this device that you see here, I. And the image on the screen is, uh, it's called FlexPro Grip. It's a device that I'm very heavily involved with, uh, developing rehab protocols for and things like that.
But it measures the specific finger strength of some of the key stabilizers for the UCL. Uh, this is an example of an athlete who's 10 months out of, um. Post partial UCL tear but didn't have surgery. Uh, so still had it, got the PRP injection, but he was, you know, you can see on the far right, he, he was at 56 and 68 percentile of where I wanted him to be.
And he was 20 miles below his goal, still throwing, uh, he wants to be 95, still having pain at 75 type deal. Um, so we can quantify like the specific strength of these tendons and. Uh, start to identify a rehab plan. But the [00:38:00] key here with this training protocol is it takes 12 plus weeks to see the, the stiffness gains that we wanna see in the tendon.
And that's really the name of the game here, um, is we aren't just training strength of the tendon. It's a good proxy measure, but stiffness is the key quality we're looking at, uh, adapting. And that's what this whole device is built around is. Enhancing the tendon stiffness to protect the UCL. Um, and so it takes at least 12 weeks to see that gain.
There's really good research on this, um, done by Keith Barr and many of the other, uh, tendon researchers. Um, that strength will, strength will go up linearly, month one, month two, month three. Strength will go up linearly, but tendon stiffness, which is the thing that directly offloads torque from the UCO.
It takes about 10 to 12 weeks of consistency of really high intensity training, greater than 70% MVC, uh, to see the actual stiffness changes. And FlexPro Grip is currently in validation studies as well to prove that this is exactly what's going on whenever way that you use the device.
Dr. Grant Garcia: I, I think this brings up two questions for me.
One, what's [00:39:00] interesting here is that, you know, this kid in my office 10 months post UCL, not back to where he wants to do. Generally, they'll usually throw in the towel by my office and get their UCL done where we do a UCL repair with internal brace. So it's interesting to see this timeline. Right, and this is exactly the point I bring up with the players when they come in and you've had players that we bounce back and forth.
We just talked about one recently where I've been like, Hey, let's give you as much time as you need. But sometimes they just, they just can't be patient. Right? Like it's nice that you've got a player as patient as this, that wanted to wait 10 months to try to do non-operative treatment because there is a, there is a part of me that says.
And I'm just interested what your opinion is that, you know, if they had had surgery on a UCL repair for a partial at 10 months, four months of non-op, six months of surgery, uh, later, they might have been back already. Yeah. So what, what, what is your thoughts on, on that portion? Again, it's, it's player dependent.
You're not making these decisions all the time. It's what the player wants.
Yeah.
Dr. Grant Garcia: Um, but I think that's interesting just to bring up, and also, have you seen this used for [00:40:00] rehab for surgical patients?
Dylan Newcomer: Yeah. So for a little bit of context, this patient specifically the, he only started with me last week. Um, so he was actually in Florida and I Unfortunately his rehab was rice bucket and dry needling, which just is gonna miss the bucket. Right, right. Like we are just completely missing everything about the rehab process that's necessary to, to get him past the partial tear. And that's kind of what I was alluding to earlier, is like a, the timeframe is often too short, but rehab often, especially, you know, going to the non-specialized is often too general.
It doesn't hit the mark. Um, and so in that, in that kid's case. Hi. His hope was that he was gonna be fine. He's been doing his return to throw, but you know, he was a little over optimistic, I think, where he thinks that it'll just keep getting better. Um, know he's missed the mark,
Dr. Grant Garcia: but what, that's type of person you want to get him.
But the other thing is, you know, if he hasn't really had good rehab, I don't even know if that's 10 months. Right? Like we keep saying Yeah, it, the numbers will, the number [00:41:00] always starts, like even in surgery recovery, right? Like, you can't just not recover and then start throwing fastballs a year later, right?
You gotta, it's all about when you start doing your rehab. It's why guys like Driveline and why, why guys like Dylan are so important. It's the same thing with your injury, right? Like if you do no work to get back from your injury, it's when we tell people it's a three month recovery, that's three months with work.
Dylan Newcomer: Yeah. Yeah. And I think that's really important to highlight that the work has to be the right kind of work too. It doesn't, like he's been working his ass off, it's just been on the wrong things, unfortunately. Um, it hasn't gotten him to the point where he needs to be to be able to do the thing he wants to do.
And I think that's really the key is that, yeah, for him, he's probably. Day one, he's no different than a partial tail that just happened last week, uh, in terms of where he is currently at. So, um, you know, he's got a couple months ahead of him training on this device and doing some of the other rehab protocols that we have for him to see if this works out for him.
And then, yeah, we may get three months down the road and it's time to have that conversation of like, Hey, it's been, it's been 13 months, we did the things that we thought were necessary. This may be beyond. Rehab [00:42:00] considerations, but he hasn't had a fair chance at it, I think so
Dr. Grant Garcia: I would agree with that. I would agree with that.
That's, that's a really interesting point. And then last that follow up question again I told you is, are you guys doing this at all for any of your reconstructions or your repairs?
Dylan Newcomer: Yeah, so I've been, uh, heavily involved with building out rehab protocols with the device. And so we actually just start guys.
Uh, we set a target, so. The device has enough data from pro teams, college teams, all of this to say, if you throw 95 miles an hour, this is the rough strength targets that we want you to hit on this device. And so what I can say is, all right, I'm gonna take you down to 5% of that. So you're three weeks out of, out of TJ reconstruction, we're gonna start you at 5% and we're gonna start loading there.
And then week by week we can incrementally increase the targets on the device and it's all isometric training to build up the tendon. Um, so over the course of that whole rehab protocol, we eventually build you up to the training threshold that we want you to be, which is 70%. And then the other things that this device [00:43:00] does is trains rate of force development, trains, uh, endurance of it.
So we have different protocols. Um. For different timeframes in that rehab process. But yeah, basically from week two, week three out of there, whenever we feel comfortable to start doing some light form work, we're starting percentages of where we want you to end up by the end of, by the end of the rehab.
Dr. Grant Garcia: And are you doing this with the throwing stuff or This is before throwing. This is pre throwing, doing this. This are you as well? Okay.
Dylan Newcomer: Yeah, it's prerow and during throwing, so we are gonna do all the things necessary to put you in a, in a good spot. Uh, prerow our goal is to get you at least to 80 to 90% of our, of our healthy.
Like I'm full of 100% targets before you even start throwing. My goal is always to make you a monster of an athlete that could handle anything before you even pick up a ball. Um. And then, so that way whenever you do start your return to throw program, it's the easiest thing you've ever done. I don't want throwing to be the next step in the progression.
I want it to be a [00:44:00] regression, honestly, where you just feel like it, you know? Yeah, this is great. I feel comfortable and we can ride that, that through the entire return to throat progression.
Dr. Grant Garcia: As I promised Dylan beforehand, I knew this was gonna happen, but like we get a topic and then we didn't wanna ask more questions because I love this.
Yep.
Dr. Grant Garcia: So I think one thing for the, for the listeners to understand that when I always tell my players, right, they, that three month, I'm like, we start the, start the return to throwing program. But I, I'm using three months arbitrarily from what we learned, what we do, and the idea that there is now a functional test, right?
It's the same. We have an ACL L right. Functional sports test to go to the next level quad strength to go to the next level.
Yeah.
Dr. Grant Garcia: What the listeners need to understand you meant, you brought this up really well, but I wanted to summarize it one more time for listeners, but the flexor tendons are all the ones on the outside, and those are what protect the UCL.
So if the flexors are weak, no matter how good a job by surgery is, you will injure it. And I will tell my players notoriously, and you probably can attest to this, that during their throwing process, maybe not anymore with this new device. That a player will call me and say, I tore my [00:45:00] UCL again. Or I feel like I felt something bad, like my arm's really sore after throwing and nine, 9.9 times outta 10.
It's their flex retrain. Right? They get a flex restraint or something from overdoing it. And so this is, I think why you're bringing this up and why it's so important because like if they come in, like, I'm sure those old, those players that you, the last couple years that have called about that were not totally ready to go, right?
Yeah. They did not have this where they're at 90% because. If you're at 90% and you're at a level of a full thrower, you're just not gonna strain it the same way. It's just not as common.
Dylan Newcomer: Yeah.
Dr. Grant Garcia: Right. That, that, anyhow, will, you're probably, I can see Will's eyes going. He is curious. What, what question do you have?
Will Sanchez: I, I've got 15 of them, but you know, I'll, I'll keep it short and sweet. Um, you know, we're talking about the UCL, um, and it seems like there's been a uptick in UCL injuries, uh, especially league baseball. Um, are those are discussions that you guys have internally or is this something that you've noticed or.
Due to the way you guys train in the, in the time and [00:46:00] effort and making sure that you're doing the isometrics and, and, you know, strengthening the stabilizers that, that you personally and driveline personally are, are seeing less. So what about those discussions when you see a Garrett Cole go down when you see all these guys going down?
We had, um, let me throw some numbers. Uh, I'll throw some numbers up there. Uh, this was, uh, 40 starting pitchers have thrown a hundred plus pitches over 98 miles per hour since 2020. They've now had Tom, 63% of them have Tommy John surgery in their career. You know, when you see numbers like that, what are those internal discussions? I.
Dylan Newcomer: I mean, it's, it's multifactorial, right? It's, it's, this new device is great. It's probably started to really take hold in MLB in the last year. A lot of teams are getting on it. So hopefully as that continues to develop, maybe we start to see less and less. Gotcha. Um. I, I think it's mostly been around the fact that our training and our rehab demands haven't been specific enough, right?
We're like really good at building the engine, which is like, you know, the strength and conditioning of the [00:47:00] general athlete, but we haven't been as good as of building the armor at the same intensity. Kind of the old throwers 10 type model, like really easy, low load, high endurance rep schemes, all that stuff wasn't matching the demands of the game.
I think it's starting to see that shift. So that's one conversation that we've always had and we've definitely seen a lot of great rece or, uh, success with it internally. Yeah. Um, the other demand is, is workload monitoring and what that looks like in the off season, uh, what that looks like in the pre-season spring training.
Like are we actually getting guys. Fully ready for that workload demand? Or are we seeing a massive spike going into spring training? Because if you spend your whole off season, never getting prepared for, you know, going back to back or anything like that as a relief pitcher or going from a 25, 30 pitch bowl pin up to 70 pitches, like those kinda workloads spikes catch up to you.
And you see it in spring training guys go down real fast. Yeah. Um, and then it's workload monitoring in season. What does your in-season training look like? So that [00:48:00] way you maintain those things that you built in the off season. So it's, it's. How do we do it on multiple different fronts? Um, and I think every year we're getting better at it, but the game is still just so advanced.
Um. That it, it, it's just bound to happen to a degree. There's a lot of chronic injuries that are under the radar that, that catch up to them.
Will Sanchez: Yeah. And also you lost some of the sticky stuff that was helping pitchers with the baseball and I'm not sure if that has anything to do with numbers. Right. Uh, I believe it was Tyler Glass now was talking about it a few seasons ago where he was like, I had to grab grip that ball so tight.
Yeah. I didn't have a little something to, to give me just a, a grip, not, you know, something crazy. And that's when he blew out his arm. So those are whole other interesting conversations that we could even get into, whether, you know, there should be some, uh, something to help with. With certain grips because the baseball's so slick.
But then I'm really taking this off on the whole other nine three and we can go into a whole other conversation. So Will
Dr. Grant Garcia: is [00:49:00] Will's notorious for trying to break us over the hour mark? That's what he did, especially the last 15 minutes of the podcast. He's thinking about all the ways he can ask you a hundred questions.
Will Sanchez: I got, I got, I got one more thing. Before you jump in and listen. We're not gonna worry about it. We owe. We owe him five more minutes. We go five minutes longer. I'll take care In editing, we're not worried about it. Um, listen, I had the privilege of meeting two amazing women, uh, at Driveline. I've been to the facility at Kent.
I've interviewed, uh, uh, Louisa, uh, gauci at the time. Uh, she worked with my daughter with baseball. She's, is she with the Brewers now? I think?
Dylan Newcomer: Yeah. She's with the brewers. Yep.
Will Sanchez: A, a absolutely amazing person, A sweetheart. Um, and just showing her passion. That she has for the game and working with the kids.
She was working with, I believe it was 13 and under at that time. And at the same time, I'm looking and [00:50:00] I'm looking at the batting cage next to me and this woman is smashing baseballs. I'm like, who the hell is this? And is is Rachel Kovich that she's now in Miami. The Yankees had hired her as a hitting coach.
I believe she was the first female hitting coach, um, that was hired by Major League Baseball. My point is, you have amazing teachers and instructors at Driveline. How does that help you do your job better?
Dylan Newcomer: It, honestly, it's the best thing that I could ask for. Um, not only are they just like great at their, their, their craft, right?
Like they're excellent coaches at hitting or pitching or strength and conditioning. Um. They are very receptive to the feedback. Um, and I think that's really the key there is like, nobody here has an ego about their thing. Like we, we understand that every athlete is gonna have a touch point with all of the sectors of, of pt, of strength, of hitting, of, of [00:51:00] whatever they're doing.
And that we all have a, a piece of the puzzle there that needs to be considered, especially on the rehab front. If, if an athlete's starting to get a little beat up, they're the first people to, to, Hey, go see Dylan. Like, you don't need to be doing this right now if you're over here in pain or whatever.
Like, go see Dylan, get a plan figured out, modify the training plan for the next couple weeks, and then we get you back into things. Um, so they're the first ones to jump on that horse and make sure that their athletes are well taken care of. And the unique thing about Driveline is we have athletes all over the country and so it doesn't matter if they're in person, uh, if they're.
In Japan, if they're in Florida, wherever it may be, uh, I can easily consult with them, help them out, make sure that they have a plan of action, of how to carry things forward and make sure that we get the best outta their training.
Dr. Grant Garcia: Will, I think we can, will, won't go too much into this, Dylan, but I think you also brought up is that coordinated care.
This is what you guys do. Such a good job of, and I think we're, we're, we're working on something to kind of even make it better, but. The [00:52:00] will. What you don't even see is the even the next step, right? It's like, so Dylan as a player, he gets hurt. Dylan feels like this is now beyond even what he wants to deal with.
And then he reaches out to me or his other doc, baseball surgeons to see the player as well. And so that concierge service that Dylan delivers continues on. And so we're able to do this. I mean, we have a di, we had a great example, right, Dylan of our player from Taiwan. Uh. Got him organized, got him the surgery, he went back to Taiwan rehab and just got an awesome video of him throwing, he is back to baseball fully.
Um, but just to be able to do that for your players and be able to have that sort of leeway. And the nice thing is the players come in, they come informed. They're not coming into me scared. They like have no idea what's going on. Um, and I think the, the feeling's mutual from both parties, but what's been really nice too Yeah.
That way that, um, I think Driveline sets it up. That's like, this is just like professional level everything, right? Like. You get, you do, you don't, you don't, you just do your, your, with your coaches. You do all your stuff. That's great. You get hurt. You see [00:53:00] Dylan, Dylan does his thing, and if Dylan thinks it's too much or doesn't wanna deal with this, 'cause it's, it's now more of a surgical injury, then they get you into a surgeon promptly to get it evaluated.
It doesn't mean you're gonna get surgery, it just means that you're gonna get someone else to take a look at you, and then you get right back over to Dylan and right back into drive line. So it's just really nice setup. So you never feel like you're lost. I, I think that What would you, what would you say about that process?
Dylan Newcomer: Yeah, I mean, it's, it, it is, it's as easy as it sounds honestly. I send you you guys an email, you get 'em in quickly. Uh, it's honestly the biggest blessing that we have. Um, you're our go-to source for all of that. Um, so yeah, it, it's, it's streamlined. Uh, and like you said, the athletes are informed, like, I don't care how much time, how many days, day after day.
I mean, these guys are dealing with a lot of anxiety around injuries when they do pop up. They're in here all the time asking questions, wanting to learn more, wanting to know what their options are, wanting to know what their timeline looks like, so it, it's really about sitting down. I. Making sure that I'm infor or you know, they know that [00:54:00] what their options are, what they're laid out for, that their coaches are involved, and that we have somebody that is like you who's gonna be able to give them that extra look that, that deeper dive and send them back our way so that we have a more informed plan.
So it's, it's just super streamlined. It's, it's really great, honestly.
Dr. Grant Garcia: Well, and one nice thing too, I know Will may talk about, you may not this, but like. The, when you're hearing this, you think of this person's with you guys all the time, but I would tell you once every two months, especially during the full beville season spring, I get one player from you that I'm not planning on doing surgery on.
They're here for a couple months 'cause they're back in college. I. Right, and they're playing. And so the point of drive line is like even, it does even have that drop in opportunity for certain players or especially to come back for a few months and do your training and know that like you're still gonna get the same level of care.
Right? Like you guys send me your regulars, you guys send me your drop. I mean, I've had a couple players you told me, they're like, they're leaving in two weeks. You need to get 'em figured out.
It's just a nice, it's just a nice setup and it's nice that you guys just treat all the players the same. [00:55:00] Uh, and I feel like anywhere from like, you know, my 13-year-old you sent me to my, your really high level college athlete. I. Uh, it, it, it's the, I don't ever feel like anybody's getting less of care, which is just awesome.
Dylan Newcomer: Yeah. Yeah. We're just trying to make sure that everybody has the same access. You know, obviously there's some insurance games to play and things like that, but like, if we can get them immediate care and all of that, like we're getting them to you, uh, and then we're getting a plan of action out of that.
And even if they're gone, it's like you are leaving the most informed that you could be, and whether I'm taking care of it, you're taking care of it, or somebody where they live is taking care of it. Like, I want you Yeah. To have to have a full understanding of what's going on and how we're gonna get past it.
Dr. Grant Garcia: A hundred percent. So Will last thing, could we ask him, I wanna ask again be as brief as possible, 'cause I know we're running outta time, but I gotta ask the most important
Will Sanchez: question. So hurry up, wrap it up because I got the question of the interview right now,
Dr. Grant Garcia: Dylan, where is where, again, brief as you can, where is the future for you guys at Driveline?
Obviously it's expansion, but where is the future? What's the [00:56:00] next step for you?
Dylan Newcomer: Next step for us is just gonna be continuing to do the things that we already, we already do really well. Uh, we're really diving into, um, more of the health side, honestly, like the FlexPro product that I, uh, was talking about.
We're integrating that fully into our entire assessment process. We're getting EMG sensors involved. We're starting to understand how your mechanics interact with all of that. And, um. Pitching is kind of taking this shift from how do we throw really hard to, how do we command better? How do we keep you healthier?
'cause injury risks are on the rise, so we wanna make sure that we're covering it on all basis. And I think that's really where we're headed. And then with our athletes, uh, we have the pulse sensor, that's our workload monitor. We've built out these amazing smart reports that you get a report on how well you've done every single day, uh, and we're learning day after day how to better leverage that technology to keep you healthier throughout the entire year.
Awesome. Will
Will Sanchez: go for it. All right, we we're gonna wrap it up right here. This is the most important [00:57:00] conversation that we're gonna have all night. All right. So let, let's get right to it. Okay. Okay. This is what the conversation, this is what the baseball world is talking about for some reason or other, and it's the torpedo.
All right? Yeah. What is the internal conversation that's happening at Driveline about the torpedo barrel and how it's affecting baseball and maybe even it's affecting, uh, the hitters?
Dylan Newcomer: I. Yeah, I mean, we, we love it. We, we love the innovation. Um, we think it's cool. We think it's exciting. Uh, one of our, uh, employees put out a nice little analysis, uh, from the data science perspective that we're not necessarily seeing it, you know, max out any.
Exit velos aren't going any higher, but the uh, the quality of the context, uh, the average velo that you maybe see per hit, that that kind of stuff is changing. So maybe it changes the middle ground, but it's not necessarily, uh, that much of a game changer to where we need to freak out and ban it, uh, as right away.
'cause you know, now we're adding 10 miles an hour of velo and everything's a home run. [00:58:00] It's just kind of changing the middle ground from, from what I understand. But there are definitely people at Driveline that. Could answer this question way better than I could. I'm just a novice when it comes to that, but I think that's my, my current understanding so far.
Will Sanchez: I, I, I love it. Well, you did better than I was
Dr. Grant Garcia: gonna do, so that was good.
Will Sanchez: I, I, I, I love it. It is just for fun, and it is just the way the game is and more than anything else, you know, we didn't even get into the mental aspect, right. We, we, you know, we, we didn't even get into all that, but even if your opponent.
Is worried that the batter's holding the torpedo bat or the hitter is feeling extra confident because we know and, and also placebo effect.
Will Sanchez: You're just feeling great about yourself. Like, yeah, I'm rocking it. I mean, it's all good. And for everyone that may be up in arms, the game always changes, whether it's the cleats, the mound, the size of the outfielders glove that looks like it's three feet long.
It happens in sports. Let's embrace it. Let's love the game. And more importantly, we're talking about [00:59:00] baseball instead of football, basketball, and all these other sports. Baseball is front and center, and that's if you're a baseball fan. That's what we all want. Yeah. Dylan, thank you so much for your time.
Uh, we're all gonna say goodbye together due to our time on gambling, which is Dr. Garcia's fault. Dr. Garcia, I told you not to talk too much. Say goodbye, Dylan, Dr. Garcia.
Dr. Grant Garcia: Bye, Dylan. All right, thanks
Will Sanchez: guys. Thanks guys. Bye.
Audio Transcript
The Captain Returns The High-Stakes Surgery of Gabriel Landeskog

The Captain Returns The High-Stakes Surgery of Gabriel Landeskog
Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia. Um. Before we get into everything, we were really excited about this, uh, about this podcast and talking about this particular injury. But before we get into that, how are you, how's everything going?
Memorial Day weekend? You're grilling what, what's, what's happening with you and the fa
Dr. Grant Garcia: Yeah, so, uh, we're good. Life's good, you know, the usual busyness. Um, we actually like boating a lot, so we have a boat, so we're gonna go on our boat and have a good time. But right now the forecast is like in the. In the fifties and sixties.
So [00:01:00] for all of you not in Seattle listening to this, that, that's pretty normal around this time of the year. So, uh, unfortunately we're not gonna get the warm weather that we get every once in a while, so I think we'll do some, a little grilling, a little hanging out, family time away from all technology.
So that's good.
Will Sanchez: You know, you know, I, I heard the weather's gonna recover for this weekend, so the weather should be nice, but, uh. Yeah, yeah, yeah. But speaking of recovery, let's see. Uh, let's give, uh, Mike b and, uh, the rest of the fellows out there a shout out for the recovery shot shop. You know them better than anybody else.
Tell us why you love utilizing them. Yeah.
Dr. Grant Garcia: Yeah. So again, you guys have heard it nonstop. A big thanks to our sponsors, honestly, for patients. This is, this is the, uh, this is the way people ask all the time. You know? I mean, I have multiple patients even today from the office. They're like, what else can we do?
What's the next level stuff? I want nutrition. I want best rehab. I want the best machines. This is a way for you to get that. And so as a surgeon, I can offer it in sort of one big pool [00:02:00] website. You can check out my website on the recovery shop. Um, again, I get no cut from you signing up. So the key here is just that I really enjoy it.
It's patients love it. Surgeons love it. If you're a patient and you hear this, ask your surgeon about it. Ask him, say, Hey, I want you to be part of this. I wanna have the stuff that we can get. I want the extra stuff after surgery. Uh, and so it's a great opportunity. So reach out to Mike b. Uh, they're awesome.
I think you really like it. And, um, it's, it's been a popular thing and people have come up to me, different docs saying Thanks again. So it's awesome.
Will Sanchez: Yeah, it, it definitely is awesome. And, uh, you know, I've had my experience with them, so we always give 'em a thumb. Thumbs up. We're about to get into the show and the topic that we wanted to really talk about.
Um, 'cause it's, it's, it's exciting and I feel weird saying it that way because you're excited about an injury and that usually means that someone has gone through something. Very, very difficult, and we're gonna talk about how difficult, uh, this type of injury is and everything that you have to do to [00:03:00] recover from it.
But we also wanna let everyone know we've got a few submitted questions from some viewers, and we're gonna tackle that on, uh, toward the end of the show. So just kind of hang tight. Um, you know, the one that we wanted to talk about is the ca Colorado Avalanche, uh, captain, uh, Gabriel Landis Cock, I mean.
He's the type of player that most players either love or hate, but not too many players say that they hate this guy. I mean, he's an, uh, an outstanding player named Captain at 19 years old and just tells you the type of player he is and the hard work, uh, that goes into being at this elite level. Um, so we're gonna talk about he had this.
Cartilage transplant surgery in May of 2023 and finally returned to the 2025 Stanley Cup playoffs after 1,032 day absence. And I mean, as we go through this, this all started [00:04:00] with an injury back in 2020 with a skate going across his quad. Right. And he had this cut and this injury going a a across this quad, and we'll get into a little bit more about that.
But just from that injury alone, would you have thought that it could have been into a situation where he wound up being in a situation where he had to recover the way he did?
Dr. Grant Garcia: Well, no. I mean, we've seen those type of injuries in the NHL all the time, right? Skates come across somebody, skate gets cut, direct, blow.
I mean, these guys are getting hit really hard. And again, this is the first time an ever a player has had this surgery and gotten back to the n hhl. And so as a result, no, I would not have expected that. But generally these cartilage injuries they get, you're not really expecting them, right? Like you just,
Will Sanchez: yeah.
Dr. Grant Garcia: There, there's, there's two real main types of these. There's the ones that are kind of like pre degeneration, right? Because I'm a, when you do this, the surgeons, I'm a cartilage restoration surgeon, similar to Dr. Brian Cole, who's my mentor. So we, our goal is to prevent [00:05:00] arthritis. So we see cartilage damage and it's too early, so we try to replace it with other cartilage.
But there's the acute injuries, which is probably here, which is a little different than what actually Lonzo Ball had, where you get an acute injury and then all of a sudden a cartilage hole happens and you can't save that normal cartilage. So now you've gotta figure out a way to fix it or replace it or something.
So it's, this is more of a traumatic scenario.
Will Sanchez: And, and that's the difference between the type of injury that he had versus Lonzo Balls?
Dr. Grant Garcia: Yes. I mean, again, without knowing either one of their knees, but just knowing enough of the story and having a lot of experience in this. I mean, this is, this is really my main bread and butter is the cartilage stuff.
This is what I love to do. This is what people come in and see me from far away. Like it's the cartilage stuff. So feeling, I feel pretty confident in hearing, you know, you know, Lonzo Ball had a meniscus transplant, cartilage transplant. Never know what happens first. Is it the cartilage hole or the meniscus?
Usually it's the cartilage. Then the meniscus gets damaged. In this situation, we know what happened first. 'cause it was really just the cartilage damage. And so [00:06:00] hearing like an we know when it happened, right? Lonza ball can, you can look at different back stories and when his happened, but this one.
Probably, uh, the direct blow caused some sort of cartilage damage and they tried to get away without surgery for a long time. I mean, you can imagine.
Will Sanchez: Yeah.
Dr. Grant Garcia: These rou, by the way, the word routine knee surgery means he went in there and someone did a cleanup. It was the same thing he heard about with routine knee surgery with zobo.
He had routine meniscus surgery. I mean, renew routine cleanup, right? That just means something really simple. Just to kind of get something, a little bit of these pieces cleaned up. Yeah. And then all of a sudden now they're not better. Right. They're getting worse. And this is what we see out of our athletes in general, recreational athletes, but it's just rare that they end up needing something this big.
As a professional athlete. We'll get into that in a minute.
Will Sanchez: So when you say cleanup, right, I'm gonna take a step back, right? So we have this cut on the quad, right? And then what's happening? And please correct me, I'm wrong because you're the doctor here and I just play you, you
Dr. Grant Garcia: play a doctor on TV though, so this is perfect.
Will Sanchez: Play one on tv. So you have the cut on the [00:07:00] quad. And then you have this scar tissue buildup, right? And, and that's kind of what's happening there. That then that's when you, based on the pain or whatever else is happening, now you're going in to get this wear and tear. I. Kind of cleanup or scraping that's happening behind the kneecap?
Am I kind of on base there as far as just saying cleanup?
Dr. Grant Garcia: No, but it's, but you did describe what probably patients are thinking, so that's perfect. Uh, but I would say that that's probably not what happened in this scenario. I would imagine that he got skate and then had a traumatic injury and it knocked off a piece of cartilage.
Either dislocated the kneecap or just like a direct blow at the cut and then something like that. Generally the scar tissue doesn't bring the, the damage 'cause scar tissue that builds up from that unless he actually like had a big surgery at the time, would not usually, even if you have scar tissue, it doesn't usually rub away the cartilage and that takes like years to happen.
What I imagine is something like he got a piece lopped [00:08:00] off. On, uh, whatever part they had to replace of the cartilage. Yeah. And then it was probably maybe small, right? And then he kind of like lingered or because, because right after that injury, he didn't get a scope. So if it wasn't a loose piece, they probably didn't recognize it or they may have got MRI, it was small.
And then all of a sudden this happens. I said multiple patients in the last few weeks where two or three years later from this injury, they all of a sudden started developing more pain and then this hole got better and more uncomfortable.
Will Sanchez: Okay, so then. When you're going in for cleanup are are, you're just shaving down that area, getting it down to the surface now.
Dr. Grant Garcia: Yeah, so I mean it depends on what they were, what their goal was there, but my expectation hearing this, seeing like simple scope. Obviously mid-season you don't wanna knock the player out, right? But they're having pain and you're like, okay, let's try to give them some relief. So you go in there two simple poke holes, and if Brian Cole did the first surgery, I know exactly what he did.
So he went in there and he's going there with a shaver. We have like talk a little bit haircuts, kinda like you do with the meniscus cleanups. And then you kind of smooth that [00:09:00] surface out because that irritate that cartilage as it's kind of fleeing off. It can cause irritation as you're rubbing back and forth.
So it, it is a very simple procedure, right? Probably 20 minutes.
Will Sanchez: Oh, so it's a quick procedure. So we we're thinking more or less, less the timeline, right? So he has his injury in 2020. Obviously with the pandemic, nobody's playing. So all of this time he's not playing, goes back on the ice a year later or so.
Pain is there. Right. And then for this type of pain, your leg is straight. Okay. But bending the knee, skating, things like that, you think that's where that's flaring up, you know, with this type of knee pain. Mm-hmm. So that is constant, right? Are we talking about just a constant pain for a professional skater to skate left and right, stop on a dime reverse.
Yeah. Things like that. Go ahead.
Dr. Grant Garcia: Well, yeah, you're probably right. I mean, because the thing is that these cartilage holes are common in athletes, right? Like when you, we did the NFL players and we looked at MRIs of them and stuff like that. They have some bad looking injuries. We always [00:10:00] talk about that, like the, you know, when I was doing the Giants and we were at HSS and we're seeing MRIs, I was like, oh my God.
They were like, you. They'd cover the name and we'd be like, how old do you think this guy is? And that's like 45. He's like, no, 22. It's like, oh my God, these are MRIs. Or they're getting beat up, right? So. Players have cartilage injuries, but generally we don't treat 'em this aggressively because it's just the NFL.
We don't do those type of things, or we haven't done 'em before. They're not time tested or whatever you wanna say about these different procedures until now. Um, so a lot of players have these injuries. This scenario though, it was obviously bad enough that it was time to do something else. It's the same way with Lonzo Ball, but we have to come with the caveat that this is.
I don't wanna jump ahead to your next que uh, question. No, go ahead. Yeah, we're good. When you have this problem, most docs, and I mean we've talked about this ad nauseum, all these places have gone teaching talk different, um, team doctors. I saw the team doctor for jazz talk to team doctor for the Dodgers.
They're like, this is Brian Cole is awesome. Like the fact that he was wanting to be the first one to do this and now he's done it twice.
Yeah, yeah, [00:11:00] right.
Dr. Grant Garcia: So no one was willing to take the risk to do this surgery. This is not a risky surgery overall. I do almost over 30 of these a year. I do a lot of them.
The patients do quite well. This is a very successful procedure, but never done in professional athletes
Will Sanchez: because
Dr. Grant Garcia: we don't know how it can handle the crazy high impact. Right. We're just nervous about it. We can take that risk in someone who's a young athlete because it's been around for 15 years and it's got good data, but no one wants to be the first.
Right. Even in ACL surgeries, we do so many different types of ACL surgeries, but in the NFL, it's patella attendant, like 98% of them, even meal L trials, one of the best in the world for sports doctors does not want to do another type of ACL. 'cause the patella tendon is what the agents expect, right? Yeah.
So you've gotta, we talked this before, you're following old rules, but Brian Cole, right? He's the master of cartilage. He's the team doctor of all cartilage for all different, different NFLs and NBA and you name it. He says, you know what? I don't care anymore. I'm gonna do what I think is the best thing for the player and [00:12:00] it's gonna take a long time to recover.
I mean, a thousand days for both surgeries is a long time for recovery. I mean that that makes the Tommy John look light.
Will Sanchez: Yeah. Yeah. And, and we're gonna, and I, I have some questions about the recovery. I'm just kind of going through the timeline now. So he went in there, they cleaned it out.
Obviously the pain, the pain didn't go away.
Um, I'm, I'm, I can imagine how many times they consulted with the Colorado physician doctor, with Dr. Cole, with agents, with the, with the, with bob down the street and the family. Yeah.
Everybody that has to go into the decision to say, okay, this is not working. Our captain is not healed. We need to now go into another procedure and we have to go into this type of procedure that we have there.
Yeah. Why don't you describe what that procedure is and, and what this entails.
Dr. Grant Garcia: Yeah. So did you, um, I wanna double check. Do we, do we confirm that he got a tibial tubercle osteotomy or is that what you Um, did you read that? [00:13:00]
Will Sanchez: Yes. He had the osteochondral allograph. That's one per part of the procedure. Right.
And then the tibial tubical, this
Dr. Grant Garcia: is really interesting. Well, this is great. So this actually adds another little wrinkle to this because it's different than a Lonzo Ball. So Lonzo Ball had his on the in and outside of the knee. Do you guys see those? Those are the two areas. Now remember, this is a chat Jeep.
This is a AI made knee that will designed, so this is a little different animal than what we normally see. There's no patella on the front of that, right? There's a kneecap that's supposed to go on the front. Okay? So this is kind of like taking that off so you can see what's going on. Um, but what they, what Dr.
Cole did here, and this is something I do a lot, is he probably replaced either the trochlea or probably the patella, which is the kneecap with a cartilage transplant. So that cartilage, that plug, it doesn't stick out like that. That's just showing you how it's going in the bad cartilage underneath his cord out like woodworking.
And then you core fresh piece of cartilage from someone who recently passed away. Someone quite young, [00:14:00] unfortunately. And then you plug that in there, you have no usual screws, just actually press it in sometimes. Sometimes you have to kind of slightly tap it in. And then they had to shift his kneecap probably because he ha I, I'm imagining this quad thing caused his pats dislocate and it probably overloaded that.
So he did the tubercle osteotomy to shift him over, which is pretty awesome that he was able to do this and get this guy back to the NHL. But a tuber osteotomy with that is, is no joke of a surgery, but again. This is the same guy that got an NBA player back with a meniscus and a cartilage transplant.
It's like, why not go small your first time? But they did not. Uh, so both of these are legitimate surgeries and, um, we know both players got back, so it's very impressive. But that obviously adds to the timeline, right? Like if it was just the cartilage transplant, the, the length of time is still there, but the, but the overall initial period would not, is not as difficult.
The tubercle osteotomy adds definitely a level of complexity to it.
Will Sanchez: So, so you're taking this piece and then you're, you're [00:15:00] adding the, the donor piece right to it? Correct. And, and that's where you're. Um, the, the, the piece that's either been rubbed off or scraped off, that's rubbing, that's the pain you're adding.
Usually
Dr. Grant Garcia: it's a focal defect, though. You don't, it's not like the whole thing's rubbed off and you've got arthritis. It's, say that again. It's one hole. Say that again. It's, it's not like you're, it's not like it's a whole, the whole thing is damaged, like the entire kneecap. It's generally like a focal piece, right?
There's like, imagine it's a pothole. You have a pothole in the grass, so you're not gonna replace all the grass. 'cause you, you won't be able to do that. So you, you core out, you get a fresh piece of sod. What's interesting though, it's similar to the sod. You have to have the dirt, you have to have the roots, and you have to have the grass.
The grass is the cartilage. The lower layer is like the cartilage to bone layer. And you need the bone too. Because what happens is, what's really cool about these cartilage transplants is even though. At a year, if you get an MRI, you can't really see the difference. It's actually the scaffold your, the, the old person cells leave and if you were to scope them, [00:16:00] sometimes you still see the ring like a year or two later of the, the cartilage plug, but it lives on its own.
Okay? So it grows into its body is like a transplant. Now, sometimes the ring closes, but usually you can still see that very faint line of where you put the cartilage transplant in. So within a few weeks it's growing on its own and so it doesn't need to grow back cartilage, which is pretty cool.
Will Sanchez: This is a nasty injury, right?
I mean, this is a nasty No, this is scar. They're going from the quad and how far are we looking at a 10, 12 inch incision. Like what's the na here?
Dr. Grant Garcia: The, like that, that's how big mine are for this one. I mean, they're big. They're, I. 10 centimeters, maybe six inches, eight inches. It's, it's, it's, this is no joke of a surgery.
This guy was named, I mean, this
is rough,
Dr. Grant Garcia: typical, typical osteotomy with a cartilage transplant. Now these though, but, but like Cole's not gonna do that unless you absolutely need a TTO, right? Like I never do a TT o unless you absolutely need it. So they're basically breaking off part of the dcap and shifting it.
To take off the [00:17:00] load off this car to the transman. But, but here's the thing. He, Dr. Cole's so good and people and cartilage, when you do cartilage surgery like this, he knows that if the best foot shot for him to get back, if he thinks this is a, a, a spot, imagine like. The kneecap is out of whack, right?
It's not in perfect alignment. So if he does this transplant, there's still a lot more load on it. So the only way to fix it is to offload it. So to offload it, you need to do this shift of the kneecap and you kept, in order to permanently shift it, you have to actually change the bone, right? 'cause the bone is connected to the patella tendon, which is connected to the patella, which is connected to the quad.
So he probably got like hit. Smashed his knee cap broke off a piece of cartilage, they took it out or they, or was not really noticeable at the time, and now all of a sudden he starts talking pain. They re-scope him in 2022. Yeah, he's not really getting better. And then Cole's like, screw this. Let's just do this 'cause you're not getting back if we don't do it right.
It's like, I don't think that he was given too many options. He's like, either we're gonna do this and you're not gonna get back, or we're gonna do [00:18:00] nothing and you're not gonna get back. And so that changes the perspective of this.
Will Sanchez: If he's a professional athlete without knowing the level of pain, which I'm, I'm assuming is extreme.
Are you doing, this is
Dr. Grant Garcia: an NHL player? These guys, I, no offense to the other ever athletes. These are the toughest.
Will Sanchez: Yeah.
Dr. Grant Garcia: There's no way that this was not painful.
Will Sanchez: But, but if you're not, if you're not that level of athlete, are you still doing this on my, you know, someone like me or you know, someone like you or you're going, well this is the type of surgery and, you know, we can, uh, you know, make it comfortable enough?
Or is it something like, no, you would do this anyway.
Dr. Grant Garcia: So I would do this anyway. I mean, I've done, okay. I've done more than 10 of these surgeries in the last six months. So this is not something that I, this exact procedure. So this is not something that I don't do, and I wouldn't indicate generally the age cutoff on this 50 and below roughly is kind of the timeline, but it depends on the cartilage, right?
If you've [00:19:00] got great looking cartilage, but the average for this probably in their mid thirties, which is, I don't know, I'm, I'm assuming that he's a bit younger. Um, but you know, when you're younger this, you, you co think about doing this because the problem is if you leave this cartilage hole. Not only does this guy get pain, and obviously we have to realize this is an athlete discussion, right?
Like I can talk to you about in the office we get to in the patient questions. Like the patient discussion I have with him outside of being a professional athlete is like, do you wanna have a tragedy in 10 years? Right? Yeah. And to be honest with you, for a lot of the athletes, they tell it's sad, but they say, I don't care.
I wanna play for two more years. My contract's up. Right. We talked about with the Tua thing and talked about with other players. Yeah. This is discussion now where it's like, do you wanna play longer potentially, and do you not wanna have a trash knee? So it's kind of cool that we can start saying that like, Hey, we can save your knee because like we know these cleanups do nothing.
I mean the cleanups are like, they buy them like six months, they buy them a year. Right. Gotcha. I mean, I'm taking first some NFL players, I had a guy that kept getting meniscus meniscus removed and they said, you're just gonna do a cleanup. And [00:20:00] eventually he retired from the NFL and we had do a much larger surgery.
And so as a result, the these are, we try to do bandaids on these athletes because. Big stuff. If you do it and they're out for sure. Then you also have the legal liability, right?
Will Sanchez: People are not doing the Dr. Brian Cole. Yeah. It's a whole other level, right? That, that's what he said. Like you're putting the bandaid on it and kind of getting him through, and then eventually you get a scenario and, uh, in the right situation where you have a doctor that goes, this is what we're gonna do.
And because it's who he is, they're going, okay, we, you know, we trust what you're doing.
Dr. Grant Garcia: I imagine that this is not gonna be, we talked this before. Remember I mentioned to you about the Lonzo Ball? Yeah. This is not gonna be the last time this surgery's done. Now you have now two successful athletes
Will Sanchez: like the standard that have
Dr. Grant Garcia: gone back with this surgery.
And this is really interesting for the viewers. This is actually resonating with patients. I had a patient, I did a cartilage transplant on, uh, he exact same surgery. Yeah. And the TT O, he came to me last week and he said. [00:21:00] You know how I knew I could do this. He's like, it was really scary sounding. You know, I give them all the expectations.
They say, worst case, best case. No matter what I tell them, if I say, feel comfortable with this, show 'em video testimonials. They don't care. It's scary. Which is totally legitimate, right? Surgery's scary. Will you know this? We both had surgery. He said this particular player helped him get back because he said if he can get back in a thousand days, and I, and I think I'll get back in a year, that doesn't sound that bad.
And he said that this motivated him. Hearing about this story, and this is exactly why I wanted do this podcast actually worked out that we got a little bit delayed in doing this because we was able to have these patient conversations. But
Will Sanchez: yeah, this
Dr. Grant Garcia: is the second time I've heard this. The Lonzo Ball one comes up all the time.
I mean, I've had players PE people being like, yeah, I know what it is now. Lonzo Ball had it. Yeah. Yeah. And it makes it so much, I think for people listening, they're like, well, you know, when someone tells me they're complaining, they're say, Hey, six months sounds like a really long time to get back. I'm like.
It took two professional IES a thousand days. I'm telling you, I think if I think it'll take you 10 months, they're like, [00:22:00] that's not too bad anymore. Right. It sets a new bar.
Will Sanchez: Yeah. Yeah.
Dr. Grant Garcia: Right. Like and, and by the way, it's not that a thousand days means there was something wrong with his recovery. It's just that going back to the NHL hhl, I think this will continue to get, and also this will continue to get faster.
I mean. Cole's not gonna let them go back until he is Absolutely, I'm sure, I'm sure he had like six MRIs to make sure it looked good. Yeah, yeah. Right. Like everything's getting checked. Make sure it's healed perfectly. Like we're not always doing all those things in a standard practice. 'cause to be honest with you, if the in, if we don't, you can't just do an MRI for free.
And so as a result, patients are paying for it. Yeah. And they're not gonna do that unless they really need to. So it's, it's different than the end than this stuff. I mean, these guys just, they have this print MRI machine, they're like, you know, every day, every week that someone gets injured, it's like X-ray, MRI x-ray, MRI.
Will Sanchez: I, I know how, and you touched upon it right now, and that's why I'm thinking about it. I know how I felt with my surgery post-surgery. I know how I felt one day to the next gung [00:23:00] ho, ready to tackle the world. Let's go. Other times just laying around, seeing atrophy kick in, you know, seeing my family, you know, being reliant on them, just everything and you just go into this mental depression, you know, and you're trying to kind of forge through it for these athletes.
This is their career, their livelihood. You've worked with athletes. What is that mental aspect that the athlete is going through that you've experienced at the professional level with an injury like this?
Dr. Grant Garcia: I mean, it's a lot like when we get injured, we're like, okay, in a couple weeks we can go back to doing our jobs.
Right? This guy's not doing his job for 1032 days. Right. Or, and, and, and Lonzo Ball's case, he had a lot of guaranteed money. So that helped I think a little bit, if I remember [00:24:00] correctly. But that's not the way some of these contracts are being going on now, right? You can, if you're an amazing player and you can really dictate how your contract goes.
So there's a ton of stress, right? Like they came used to this thing, they got injured and you know, you get an ACL surgery, you're back a year-ish, you get a meniscus cleanup, six to eight weeks. All of a sudden now you're talking, taking a thousand days to get back. Right. That's like a humongous factor. And even though you're going through it now, you're like, I'm the first guy to get this.
Like there are, this is not a surgery without complications. 32% of these patients end up needing a cleanup at some point,
Will Sanchez: and Brian
Dr. Grant Garcia: Cole has written half the articles on it. Wow. So there's a chance that Lonzo Ball and Gabriel will need another surgery. Now, again, it's, that's the general data. I think that that's a lot lower in my practice.
And I know, I'm sure Kohl's, we didn't see that many cleanups, but. There's a risk with it. So you're going through this whole recovery, you're trying to get back and you're like, I really hope that cartilage transplant works. Right. I really hope that the osteotomy heals and then I hope I don't have [00:25:00] pain.
Oh, and then like I'm past that point now. I hope I can like skate. Yeah. Now I hope I can skate without pain. Always like, now I've gotta play in the NHL. Right? Like it's just not, the benchmarks are my patients generally, and I mean, we get the professional athletes, it's different. But the general athlete, right?
Like I'm bouldering again, like I'm back to running and doing some squats and that's already impressive for this type of surgery. You know, that's the next level they have to get back to. So mentally, yes. And when you get to a certain point, even Cole's gonna say, well, you're the first one. So we don't really have a benchmark.
We, we, you are the benchmark, but you are the benchmark,
Will Sanchez: you're the benchmark, you're the new
Dr. Grant Garcia: benchmark. So, um, it's a lot. And the mental aspect of this is humongous. I mean, it's more than that, right? It's. I hate to say this, but the athletes are more of the head cases and it's, it's, it's, it's real. I mean, we know the mental anguish of athlete athletics.
We know the mental anguish of coming back from injury. We know the mental anguish of the pressure. Right. It's, it's real, it happens [00:26:00] to both male and female athletes. Mm-hmm. I tend to think that the female athletes are more vocal, which is great about their, the pressure they're feeling, and males tend to bottle it up and that's a problem.
We've seen that as well.
Will Sanchez: Yeah.
Dr. Grant Garcia: Um, but the mental aspect of this is humongous and probably the bigger part. We talked about the set nauseum and we know we need to show about this, and it's just, it is, it is absolutely humongous and I will tell you that this is real for my patients. Absolutely real. I mean, I have patients that I tell 'em they need this surgery and they're in terrible pain and they need to get back to what they wanna do.
Probably similar to the way he was. Yeah. And I said, you need a TTO, you need a cartilage surgery, it's gonna take you 10 months to a year. And that's obviously a lot lower than a thousand days. And you know, just put their hands in their head and they say, how am I even gonna handle three weeks of not working out?
Right. Like that's,
Will Sanchez: yeah. A
Dr. Grant Garcia: humongous difference.
Will Sanchez: Yeah. In
Dr. Grant Garcia: the end they're usually pretty happy. And I'm sure Gabriel's pretty happy, but there's no way to, you can't tackle that in the first visit. You can't [00:27:00] tackle on the sixth visit. You gotta just say, Hey, listen. I am and we're probably gonna jump to our question from the audience or from the viewers.
I can't get you through this in one visit. I can get you through the process though. I'll be here with you the whole time. My team will be here with you whole time and so at six months to a year, you know, how am I doing? You're doing great. How am I doing? You're doing great. I think it's time to rip. Thank you.
Like I'm ready. Like they get there and it's usually for them, in this case, with these type of surgeries, it's usually five, six months. So it's not the first few weeks. You're like, I think it worked. I'm doing great.
Will Sanchez: Yeah. No. Yeah. I, I got one more question before we get to a submitted question. Uh, questions from our viewers.
Um, and it is funny because I was thinking about it. I was like, would this have been possible 10 years? And I go, wait a minute. That's not even the question. It's like, I. How far, like, would, would something like this have been possible five years ago? You know, three years ago? And I know for, and, and it's probably a two part question, right?
One, for someone like me getting to surgery, and now [00:28:00] we're seeing it now for professional athletes, so it's just happening now. But as far as technology and where we've come, where the surgery would've been possible. Five, 10 years from, uh, prior,
Dr. Grant Garcia: so it would've been possible. Remember, we just need a lot more data and we need someone who's willing to push the envelope.
So, you know, Brian Cole when he's 25, 30 or 40, and he is, I hate to say that, that's young surgeon, but when he's doing that, he's not ready to push the envelope, right? So you have most of these younger team doctors, they're not gonna start doing that stuff, and they're not gonna get the high level player either.
They're gonna Neil TROs, they're gonna Brian Cole. Right. And then you get to someone who, like him, who's a cartilage master and he finally gets to push the envelope. And so now we're able to do it. But he's gotta see thousands of these hundreds of these patients before he is like, I think it's time to do this in pros.
'cause this is ridiculous. They're not getting the care of the other ath the my other athletes are getting, yeah, right. My D one college player that did a cartilage transplant on, he's to athletics. Why am I not use this on the pros? [00:29:00] And so the technology improved? Yes. Over the last five years we've had the surgery five years ago, there was definitely better stuff that we do.
And what I did five years ago for this surgery is different than when I do now.
Will Sanchez: Yeah.
Dr. Grant Garcia: Not, I would say not enough that it, it would've changed my decision to do it. Pro-athlete now versus then. I think it's just that Kohl's built up enough clout that like if anybody were to say like. Why did Cole do it? Be like, of course he did.
He wrote the book on it. To be honest with you, Cole designed the system that he probably used, I know he did for Arthrex, the cartilage transplant set that he used to do his transplant and Lonzo's ball. So this is a master, like he, he's got the whole system already designed and made to make it work for him.
So if anybody says anything, it's like, this is the guy. Like if there's anybody that's gonna do it and do a good job, it's him. So, like you, there's only, you only go down from here in terms of what other options he had. A
Will Sanchez: anything. I, I know you've, you've done this procedure, anything coming out, you know, whether it's, [00:30:00] you know, donor or equipment or anything like that that's coming out.
'cause I know you go to a lot of conferences, you're in the conversation with a lot of these companies. Is there anything exciting out there that, maybe it's not today, but down the road, that you can see that when it comes to surgeries like this that you, you may be excited about or you're hearing rumors about?
Dr. Grant Garcia: Well, really everything's just to be healed faster. Right? Is there biologics that we can enhance the healing of this graft or can we grow things? 'cause the issue is when you have bone and cartilage, it's a lot harder to grow back, and especially in the patella, because less things are approved for the patella than they are for other parts of the knee.
Will Sanchez: Yeah,
Dr. Grant Garcia: right. So if you have a patella, do we have newer techniques that have better results in the transplants? To fix bone and we're gonna get there. There are a lot of things in Europe that people are trying and do we have a way to make this a faster recovery? Right? Can we, can we get this cartilage to grow, integrate, and be ready to go in six months?
Can we do the typical osteotomy and double the [00:31:00] bone healing time? Can we not use metal screws and use screws that turn into bone and no longer have that? Mm-hmm. Yes, we are getting there, but we are definitely not there yet. So I think in 10 more years there'll be a situation where this guy will have no metal in his body because he's gonna have two.
He has metal screws from the tub, gloss osteotomy. There's no way about that. Yeah. Um, and he's gonna have, you know, his cartilage will be either grown by itself with the bone or you know, something implanted where it just turns into cartilage and it's like a 95% success type of thing. Probably not five years from now.
Maybe 10. Yeah. Um, but we're gonna keep getting better. Uh, and it's gonna take guys like this to show that this surgery works for people to be like, well, wait a second. We've gotta start doing more of these.
Will Sanchez: Great. You just mentioned three possible things, even though they're not here right now, but it's already, you know, something that people could think about.
All right, let's take a look at our viewer submitted questions. For those that are not watching, I'll read it out loud. Uh, what of the questions are how much of the medical field of orthopedics have changed over time, even with the physicians [00:32:00] focusing on only some parts of the joints, such as wrist, hands, shoulders, or knees, from when you started to now?
Dr. Grant Garcia: Yeah, I think these are very broad, open-end ques, but I think really the key here is to say that over time more surgeons have gotten more specialized. So, you know, when we came out of practice with that fellowship training, we used to be say, Hey listen, we're gonna do general orthopedics, right? We're gonna see hips, we're gonna see knees, we're gonna see mom and pop injured.
We're gonna see that. When you go to a city, which is different than if you're in a smaller, small area, very small town or something, um, in the middle of the country or somewhere else in the middle of the state, that's not the big city. That still kind of works. But when you're in a place where you're in a big city, such as myself in Seattle, you have to be ready to take on the difficult things.
'cause the cases that are more difficult generally don't see that many of them if you're not highly specialized. And so. Basically what happens is I see a lot less of the basic stuff. I still do tons of basic sports stuff, [00:33:00] but I've gotten so speci specialized that there's really big topics that I will take care of, and I will see a lot of, like literally 95% more than most people in the whole area.
There's also things that I'll see very little of because I just don't do those things anymore. Right? And so that's, but that's helps the patients, right? They don't, I don't do those other surgeries. I send that to my partners. I send them somewhere else. Say, you don't want me to do the surgery for you?
It's not my specialty. But then when it's something really hard and really specialized, like something like this, like you don't want someone dabbling in this surgery that he had that is not a doubtable surgery. This, I've seen these go really poorly when you don't know what you're doing. Something like this, you can always find someone that does a lot of them and you get the best person to do it, and then you get a good result.
Because when most surgeons do one of them every 10 year over two years, some surgeons, the high volume ones, again minimal. Yeah. But there are people out there do 12 times more. So then that makes the best sense. So that's really how it's changed. And then those people also spend their time designing, helping get the products better 'cause they're higher volume and they get to see more.
Right? Like [00:34:00] if you design something new and you don't get to try it for another year 'cause you haven't seen somebody like, that's not good, right? That's just not the way it works. We always know about this. Every data point shows that. So.
Will Sanchez: Yeah. And, and it's great just from, uh, the, the amazing guests that we've had, you know, like, uh, Dr.
Denar and, you know, shoulder specialist and, you know, some of these other doctors that we've had, uh, you know, um, Andre Schafer, right back specialist, you know, so just that, that kind of more to come. Yeah. More to come, but they're amazing at what they do. So it's just a, a prime example. Kind of like this is their specialty and I'm glad you that you made a reference to that.
You know, I do these and, and when I feel like there's someone better, I'm going to point you in that direction and, and I hope that other doctors are doing the same way. 'cause that's the type of care that, that we want. Alright, let's take a look at our last. Uh, submit a question for today. How do you as an orthopedic surgeon help decide and prepare your patients who are needing to have surgery, even when the [00:35:00] surgery may change their lives physically?
And that's a really good question. I like that one.
Dr. Grant Garcia: So it's kind of the same thing we talked about. I mean, you have to address both sides of the question, right? You have to address, or both sides of the patient. You gotta address the, obviously the fear. I guess there's maybe three fear, the pain.
Expectations. Right. And all those things have two components to 'em. They have the physical component and they have the mental component.
Will Sanchez: Mm-hmm.
Dr. Grant Garcia: Right? So when we address them, the first thing I like to do with my patients is I give them sort of the expectations. So what you're expected to do on average, that's from a timeline, recovery, pain recovery.
Success recovery, then I'll talk to 'em about, you know, like what you're gonna be at. Right. And I don't go into too much detail about your mental stuff at that point, because every person's different. Right? There's patients at six months that are doing really well and they just don't have a good mental attitude, which is not their fault.
It's just the way their recovery is. And each person's wired differently. Yeah. So that person needs less discussion of how their knee's doing and more discussion about how their head's doing. [00:36:00] Some people come in and they say, my knee's doing really well, but I'm just worried about it. Those people need more like, okay, physically you're doing really well, and then they get better.
Right? And there's a third type that maybe aren't doing as well. Physically they need to focus on the physical and less on the mental. Like I, I am telling 'em, you're doing well or you're mentally not there yet. Physically, let's figure out what's going on. Do you have another complication? I. So that's really how I manage it with the patients.
But the, the biggest thing is consistency, honesty, and full explanations. The number one way that I help patients prepare for their surgery is by spending countless hours. One in the office with them, but two, all that stuff on my internet, on my website, the videos on every single one of these surgeries and how I do it.
I have spent hours making the videos. I have blogs on them, I have discussion points, you name it, video testimonials. Pretty much every surgery there's a testimonial from a patient that's done it. Doing well. There is articles published on there. There is a surgical video of how I do it, and there's a blog video, me describing it, [00:37:00] plus the website.
So when you get in there, there's no questions what you're gonna do. My patients are super informed. Now, they may be overwhelmed on the first visit. 'cause this is like a lot. I mean, you can imagine talking to someone about this. Um, but that's how we prepare them. That's how you should prepare the patient.
Will Sanchez: They can check out your website@grantgarciamd.com and then if you want to get in touch with us, check us out@sports.talk.com. All sports, all orthopedics, all the time. We've got, uh, patient information, podcast information, check out our transcripts. We want to hear from you. We're always looking for show ideas, although I think we're pretty booked in the next couple of weeks.
We've got a lot of folks there, but we we're
Dr. Grant Garcia: booked for a book for a few more than a few weeks. But that's okay. I don't wanna
Will Sanchez: discourage people. Let, let's get keep, don't discourage you, ping
Dr. Grant Garcia: us. And also depends on certain topics. If there's something you want to do. We've gotten people's topics in.
Yeah,
Dr. Grant Garcia: we've had guests that we've been able to sneak in.
I mean, again, we try to load it up so you guys have always some good shows coming up. There are a lot of good speakers coming up, [00:38:00] but it does not mean there's not a space for you on the show. Hundred percent. Um, but you know, I will say there are people we turned down 'cause it doesn't fit the mold. I wanna make sure that.
If someone's on the show that the listeners can hear. So we, yeah, we are fairly picky about our guests, but we've had some awesome guests that have come outta the blue. I. Tom was amazing. Uh, Dr. Dave was amazing. So we have a mix of everything. And you honestly, you're never just like, you're never gonna know what my background's gonna be, you're never gonna know where the next guy is gonna be.
Will Sanchez: That, that, that is true. If, if, if there's any reason to watch our show, check out Dr. Garcia's background. 'cause we never know it's gonna be, I'm pretty sure for all the Chicago Bull fans out there, when we did the Lonzo Ball with the bulls behind them, that was phenomenal. So, um. Any, uh, any last words, um, as we wrap up the show?
Dr. Grant Garcia: No, just stay tuned. Put your requests in. We love the interaction, like you said before. We are, we're open to interaction. We're open to guest requests. We have, we have had every little possibility of that. And I love the [00:39:00] patients bringing it up too. So anything you guys need, let us know. We're, we're always, we're happy for our listeners.
Thank you.
Will Sanchez: Yes. Once again. Yeah. Thank you for listening. And, uh, Dr. Garcia, thank you for your time.
Dr. Grant Garcia: Bye.
Audio Transcript
Revolutionizing Rehab: A Conversation with Tom Swales

Revolutionizing Rehab: A Conversation with Tom Swales
Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with Dr. Grant Garcia, our orthopedic surgeon and sports medicine specialist. Um, we kicked off the show with having every technical error that we could possibly have, but luckily it was at the beginning of the show, so hopefully from this point out we are moving and grooving and going strong.
Dr. Garcia, how are you?
Dr. Grant Garcia: I'm good. I don't know if anybody's gonna notice this, but uh, there is a little commonality between our two screens.
Will Sanchez: We're gonna drive, I guess, crazy. I don't, I I, I think our, our special guests, our triple threat, uh, Tom is gonna be like, this is just way [00:01:00] too much sports doc talk. I'm out of here.
But, uh, you know, we we're just really happy to have 'em. And, you know, before we get into all of that, let's give a quick shout out to our guests, our recovery shop friends. Take it away, Dr. Garcia.
Dr. Grant Garcia: Yeah. So again. You know, we keep talking about them, but obviously the idea is recovery postoperatively, um, or just when you get injured.
So obviously Tom's gonna be a great segue for this, but, uh, this allows me to offer sort of more cutting edge stuff for my patients. Um, and as a surgeon it's really important 'cause patients always ask for this. It's just, just nonstop. They want to know what's the best. How can I get the best? What can I do to be up this level?
Um, and that's what opt, that's what we have at the recovery shop. So the ability to get sort of advanced machines, advanced nutrition, et cetera. I'm sure Tom can wane on this and how he works on recovery, uh, but these guys have been awesome. So reach out to Mike. Uh, you'll not be disappointed. And I think, you know, as a patient, if you want this, you also can reach out to Mike and say, Hey, listen, I have a [00:02:00] surgeon.
I'm interested in using this opportunity and I want to have this for recovery. So this can go to patients or this can go to the surgeons. Uh, so reach out to Mike and he'd be happy to help. Will Sanchez: I mentioned at the top of the show, we have our guests here and he's the triple threat, right? When we say triple threat, it's because of the physiotherapist that he is.
And for those that are not aware, you know, that's usually a professional that deals with the physical techniques and the manual techniques and then, you know, puts it all together and.
Provides that education for his patients. So I like to call it the triple threat. So without ado, just, just talk about, uh, Tom, and let's bring Tom on.
Tom, thank you so much for being on. Um, we're really excited to, uh, to have you here and. Just to let all our listeners know, Tom's on the East coast and we're doing this show really late. So I was busting his chops when he first came on saying, Hey, I know you're a proponent of telling all your patients get, get eight hours of sleep [00:03:00] and rehydrate and do all these things, and right now we're probably keeping up, uh, keeping you up past your bedtime.
Tom Swales: I got all these bright lights in my eyes just so you can see my face, but you know, the clock's, clock's ticking. You know, we all wake up, we all make an alarm to get up, but most of us need to put a, set, an alarm to go to bed. So we're keeping that consistency and that circadian rhythm in check for, for better recovery and performance.
Dr. Grant Garcia: That's awesome. Yeah. Well, thank you so much, Tom, for coming on. I think. Yeah, no problem. I think for the viewers, they're gonna love this. You know, this is a guy, like, I would say the triple threat, I think will, we can jump in There is. You know, you have amazing physiotherapists and strength coach, you have unlimited experience taking care of high level athletes.
You'll talk about, but also, you know so much to some of these other celebrity guests that we've had on, uh, that's not all they do. Yeah. Right. He's gonna get into something. You divide a certification thing for physical therapists and strength coach, which is just the next level, right? Like that's so much extra work on top of your job.
It's like what I talk about, what I do. I'm the surgeon and then we do other things on top. Yeah. And
Dr. Grant Garcia: then he is the co-founder of [00:04:00] something called Comp Physio, which we can talk about as well. So this is somebody that's done a lot of stuff. We're really excited to have you on Tom, and I'm really excited for listeners, uh, to hear about you.
But obviously enough about Will and I, we could jabber on, as you know, for an hour with. Out talking to anybody else. Uh, so Alyssa, can you tell us a little bit about yourself so the viewers can hear?
Tom Swales: Yeah, so you guys touched upon it. I'm a physio strength coach, um, you know, uh, owner of concept of Movement, which is now com Physio and performance wellness here in Barry. Husband, father of two. Um, you know, my wife and I, we started our business 12 years ago. Uh, just the two of us. It was 4,000 square feet. I had this vision for this, not just rehabilitation, but. Full high performance facility. And we found this old garage, uh, it was a, a Harley Davidson garage. So we got the roll up door doors in the, uh, in the gym area, glass.
We turned into a big glass door, but we have a medical side and then we have the performance side of things. And, uh, it, it started with just the two of us. 12 years ago, she was [00:05:00] running the front desk. I was the only physio. We had one movement coach and we've grown it to now to 27 staff. So it's become chiro, massage, osteopath, acupuncture, the whole, the whole gamut because the way that we, we work with our clients and athletes, it's, it's a holistic approach.
And when you have more sets of eyes to look at a problem, you come up with better solutions to the problem. And that's kind of where, um, you know, over the course of my career, I've been doing this for over 20 years now as an, I'm also an athletic trainer. I got trained down in the states and, um, and. You come outta school and you're like, I want to take courses.
I mean, that, that was me. I was like, I need, I need to keep learning. I like what I have is good, but I know I could be better. And then you take course after course, after course. And it came to the point where I, I've done a hundred courses in certifications and it became flavor of the month all of a sudden.
Okay, great. I did a course. I'm excited to do my craft again. Everybody gets this this month. So then everybody gets dry needling, and then I'm like, well, this worked [00:06:00] for some people, but how come it didn't work for others? And then everyone gets manipulation, and then everyone gets positional release, and then everyone gets kettlebells.
Like it just became this guessing game. And the more I learned, the more I realized, I don't know, and I got more confused and disorganized. So I had to take a big step back and look at, okay, what are the fundamentals across all of these, all of these tools? Whether it's, you know, learn, becoming an RKC or kettlebell instructor, or learning gymnastics or, you know, all the way into needling and manual therapy.
And when you distill it down, we're, we're really composed of like five elements, and it's psychology, neurology, biology, chemistry, and physics. So I started thinking like, well, if I, if I have a better understanding of these five things, I can explain to patients what I'm doing, why I'm doing it, and how I can do it better.
Right? Like how often clients come in, they're like, oh, what does ultrasound do? Well, it's an electric concurrent coming into a crystal, creating a vibration, creating a piece, electric pulse. That pulse is [00:07:00] creating, uh, sound waves into the tissues, which is creating vibration. That vibration is, is shaking up the cells, creating heat and increasing blood circulation, breaking up scar tissue, and creating physiological effect.
We can get into light therapy and lasers and all that other stuff, but essentially it's a form of energy being applied to the body, creating a stress that causes an adaptation. So I can break it down into simple physics of like, well, it's just energy coming into the body, causing a stress and an adaptation.
That's the biology behind it, right? We know there's a lot of nuance behind it, but when you start breaking down the actual appointment, the relationship, well, what does it start with? A conversation. I. Okay, I'm gonna ask a person questions. They're immediately in the first 12 seconds, do I like this person?
Yes or no? Do I feel safe with them? Am I connecting with them? Can I trust them? Now, what that'll do is the nervous system will start to calm down if I get a positive response. If the nervous system shifts in the direction I want, well, what happens? Their breathing calms down. They go more parasympathetic.
Their blood pressure drops, and also their [00:08:00] organ, their nervous system starts to organize. All of a sudden, oh, my shoulder hurts less. Right, because they're not guarded. Even just simple words that we use have an impact on someone's physiology because of the psych psychological component. And then we look at biology and how cells and develop, like how we develop in utero, how we develop out of the womb from the ground up.
Then we look at chemistry. Everything's molecular, the food we eat, the air we breathe, the chemistry. Our pH has to be a certain way. And then we look at physics. Well, what does physics have to do with anything? Well, we live in a three dimensional world and everything's matter. Well, what's matter made of?
Well, when you start looking at Quantum, it's energy, it's com, it's composed in specific frequencies, vibration, frequency, and energy. And then when you look at the actual, like down to an atomic level, everything's empty space, right? 99.999% of all of us at every single atom is empty space. And then when you start to think about what affects that, well, thoughts do, because now it comes back up to person's psychology and belief systems because it creates specific frequencies [00:09:00] that affect biology.
So. So to come about in a very, like as short as, as a description as I can when I distilled what we do down as movement coaches and therapists, if we can understand what we do, which is relatively new. To these more, uh, older forms of education, it becomes a lot easier to explain what we're doing, why we do it, and how we do it better.
And then that allows us to build more information on top of it because if I bring in a new tool, I now have this, these principles in which I can bounce that tool off of to better explain why it has an effect. And we know that not everything works for everybody, but something will work for somebody. So having more tools, that's awesome.
Explaining what those tools do at the right time, on the right person for the right problem. Now you're gonna get the solutions that you want.
Dr. Grant Garcia: I love that. I mean, I think the point you're making for the listeners is obviously it's a lot of information you just distill. Yeah. And, uh, some things physics, some things biology, right.
But I think if I were to distill some points for the [00:10:00] listeners is you heard this is the same way as surgery, right? There is the psychological component. There's the actual component of biology, the physics of why we're doing this surgery. Um, and that's the same thing that you're talking about. And so it's really important that this is not just a concept that's to one thing.
This is the whole medical field. What you're doing versus what I'm doing is it's all the same stuff and there you have to treat everything, the whole body. Yeah. Uh, and I, I think that's a really important thing. I mean, you, you are probably dealing with this with some of the athletes you've taken care of, but I mean this is, I mean, how often do you say that you're dealing with injuries and you're having to deal with the psychological component of it
Tom Swales: all the time?
Because people come in with these beliefs of, I can't do this. I was told I will never be able to to do that. And I'm like, well, why? Because I have a degenerative disc disease. Like that's a stupid label, like that's like gray hair of the spine. Everyone's got it. Like some of the, some of the diagnoses we have, I mean, we need them so we can communicate and speak the same language.
So I can say one thing, I don't have to sit there and explain it, but to a patient who doesn't [00:11:00] understand that, it sounds scary, like degenerative disc disease, it's not disease. It's just, it's like the discs are wearing down. So why are we calling it a disease? It's aging. Okay, so a hundred percent. If we can change the language around some of these diagnosis and make them less scary all of a sudden, oh, they don't get this alarming.
I just had one of my colleagues come up to me, he had three clients doing it exceptionally well. One's a paramedic, one's a firefighter, and I think another one has a physical job. They were all doing really well. They go and get their MRIs, and one has a disc herniation in his neck, and all of a sudden everything got bad again.
So for that individual, the diagnosis made him worse. If he just focused because he put it into chat, GPT and looked at all the possible scary things that could happen. And, and he's got a, a family history of a LS, so that's where his head goes. I'm like, no, it's you. You have a disc herniation. We can change this, right?
We're gonna make this so. It's a double-edged sword. Some people need a [00:12:00] diagnosis, somebody need to know what's going on in my body so I can move past it and others if they know they're gonna get worse. So it get, it gets tricky, but the psychological component is huge and I'll, I'll give you another example because I had a personal experience last year.
I was in the hospital with an invasive strep A, and I went into toxic shock, and I was in the ICU for 10 days. They had to put me on respirators. Sure. My heart, I had heart failure, liver failure, kidney failure. My lungs were full of fluid. They put me on dialysis. Um, they told my wife, you know, um, put, get your affairs in order type of thing.
And I didn't know how sick I was. I just knew I was super sick. So my ignorance and I'm like, I'll get through this because I've put the time and energy into my health. In case shit happens. That's my insurance policy. So I get out after 10 days. ICU, the docs had to do surgery on my ankle got infected, my toes are all black.
They're like, you're not gonna come out of this with any limbs, like with your toes. I said, okay, but I didn't believe that. [00:13:00] And anyway, I have all my limbs. Um, I put the 50 pounds back on in five months 'cause I put the work in. But I didn't know how sick I was. I asked one of the doctors, I said, doc, how, how sick was I?
He's like, oh, less than 20% survival. I was like, oh, I was sick. He's like, you were super sick. So, and four other people in that same hospital that summer passed away with less stuff going on. Same thing. So he's like, the only reason you're here is because of how healthy you came in. But yes, I did the prep work in case shit happened, but I never believed I was dying.
I never had a moment of like, oh, this is it. Which may have saved me. I don't know. Right. I mean, I'm pretty stubborn. If someone's just like, yeah, you're gonna die. I'm like, no, I'm not. But not knowing and just kind of having that mindset of, you know, I'm just super sick. I'll get through this, I'll put in the work, whatever.
That may have, that may have also helped. So mindset is [00:14:00] everything.
Dr. Grant Garcia: Well, Tom, you, you, uh, I do, I do. This is classic sports doc talk. We just basically had like a billion questions come up as you were talking. Sorry. And that has nothing to do with what we were gonna talk about tonight. So this is amazing. No, it's fantastic.
Yeah. Yeah. This is gonna be. So I think, I think we, I do wanna get back to all the stuff that you do 'cause I love the listeners to hear it, but I wanna maybe like another few more minutes, we'll ping this around and we'll go back to. We will get off track for sure. I see Will's eyes, right? I, I, I got, I got, yeah.
I Will Sanchez: wanna ask some level. I'm trying to slow. Here I go. I'm slowing you
Dr. Grant Garcia: down. I'm slowing you down. You're about to go nuts. You know, you, you talk basically. Yeah. You gotta talk about this, this will thing. I mean, this is what it takes. We talk about these players too, right? Obviously, you know, I'm so glad you're here and you have this amazing recovery.
You know, medical, physical, and I have, you know, family members that have had bad lymphomas and things like that, and they, and they come in and they are only ones that didn't die. Right? Yeah. Because they had like this, this physical thing. I had a bad thing happen to me and I had to have major [00:15:00] surgery and I was shocked how well I was able to advance back.
And it was because I refused. Yep. To have to continue. I refuse to have a problem. Yeah. Um, but you know what, sometimes you can't refuse. It's just the way that the system works. Yeah. But the, I think this is a really important thing. I will, you can probably ask about this too. What you put in before does make a difference.
Right? And they're like, you know, why are you going to the gym? Why are you doing all the work? Why you do all this stuff? Because when shit happens, like you said, yeah, like you don't want to be in that type of shape. Those people are the ones that go fast. So it's a really, I mean, incredible point you just made.
Yeah. Uh, that the listeners can hear. We're getting some psychology here. We're getting some life changes. This is awesome. So, sorry, will you asked your question and then we're gonna try to digress if we can.
Will Sanchez: Yeah, I, I kind of want to piggyback on exactly what you're talking about. Right. So you, you talked about, uh, in the beginning of the show, you talked about training, right. So whether it's. I'm not sure what certifications, but you know, we know about CSCS and FRC and CF [00:16:00] SC and now Strong First. Right? 'cause now we've gone to Strong First instead of when it comes to Kettlebells, you have all these training that has built you up for a part of what you do in your profession.
Yep. But we, we talk about. Uh, mental fortitude and perseverance, not only for yourself, but also how you, uh, relay that information and encourage your patients. What, what does that training look like? How, how has that been evolved in your, your life to get mentally strong? And then how do you channel that with your patients?
Tom Swales: I always, I always, for me, for like mental health, whenever I'm in a bad mood, I. I move, I mean, to, to change the mind. I go through the body. It's, that's why Breath Works, works so well. I mean, have you guys ever told your spouse when you know if they're getting upset to calm down, like what a terrible idea.
It never works. No way. Don't do it. Telling
Dr. Grant Garcia: my, telling my spouse anything is a [00:17:00] terrible idea, right? So let's be honest,
Tom Swales: but, but don't tell 'em to calm down when they're upset because you're trying to change the mind with the mind. Now with my children, when they would get upset, if I can catch them in time, I would have 'em slow down their breathing because now they're taking their thought off the thing that's bothering them.
But I'm changing their physiology and their nervous system instantly just by changing their breathing. Because breathing is that bridge between the mind and the body. When we are upset, our breathing changes. When we're happy, our breathing changes. When we are sad, our breathing changes. When we're calm, our breathing changes.
So our breathing changes with our neurological state, sympathetic parasympathetic. But you can also back out of that by changing your breathing to change your state, which is why breath work has become so popular. Mm-hmm. I mean, aside from the Wim Hof and doing all the ice baths and all that cool stuff, which is fun to do.
I mean, it's a little bit of suffering, but you feel good doing it. The idea is you are, you're changing your state intentionally. You're [00:18:00] applying a eustress, a stress that's positive to create an adaptation to make you more resilient. So if, if I gotta get my clients outta pain, if someone's coming in and they're talking quickly and they're bracing like.
I can't, like their shoulders aren't gonna move their neck, nothing's going to move because they're in this locked up protective state. Their nervous system's too sympathetic. I just like, Hey, let's put one hand on your chest, one hand on your belly. See where you're breathing. I create awareness to what they're doing and how they're breathing.
Which hand is moving? Oh, the top hand. Which hand do you think is supposed to move? Oh, the bottom. Let's do that. Get them to do that five times and all of a sudden their shoulders come down. They start to slow down. Their, their, their breathing ray, they slow to slow down their talking, and all of a sudden they're like, oh, my neck doesn't hurt as much.
No, because we just, we, we, we took your foot off the gas or your nervous system off the gas to allow things to calm down a bit, and it's simply because of the state that they were in. But I didn't tell them to calm down. I told 'em, Hey, what's your breathing doing? And they shifted their [00:19:00] mind away from their pain.
Into what they're doing, into the first movement that we do, which is breathing. Which is why a lot of clients, athletes, especially, we look at their breathing. I'm like, how CO2 tolerant are you? Are you using your diaphragm? 'cause if you're not, guess what you're not using? You're not using your core muscles.
No wonder your back is all jacked up. No wonder your shoulders and neck are all jacked up because you can't even use the first core muscle that we started to use when we first came into this world.
Dr. Grant Garcia: This is awesome. I, you, we were gonna, we're gonna jump actually to a question we're gonna do later, but you just literally, we're going in different directions.
I love this. This is my favorite type of conversation. So you talked about athletes, right? Yeah. And you get 'em back and like there's different approaches, right? Yeah. So do you, what do you use as some of your tricks? You already mentioned some of 'em as the breathing. Yeah. What do you use to get some of these patients back?
Like, so when, let's say an athlete comes in, high level, athlete comes in and, and they're coming in obviously to you, not 'cause they're doing well, right? If they're doing well, they don't come see you. No. Right? That's generally natural. They don't come see me if they're [00:20:00] doing well. No, they don't come see me to say hi.
So the, if you, if someone comes in, do you, are you, you know, automatically saying there's something that can change. Is there genetics involved with these people? These sort of like accentuate healers, you know, like if someone were to put you in a lineup, they'd say, that's very impressive. Right? This guy survived.
Right. One out of five odds, right? Like, but those are what those athletes do, right? When they get injured, there's a certain percentage that don't get back and there's some that do. So what tricks do you use to try to get them back that area and try to enhance their recovery?
Tom Swales: So I think, I think a lot of us, a lot of people are getting caught in the weeds with all the, the nuances and the, the fancy sexy stuff to, to know where somebody needs to go. I need to know where they are right now, which comes into the assessment. So someone comes in, they got groin and low back issues. You know, they've been, I, I've had dry needling in my groin and they, I've had my back cracked. And I'm like, okay, cool. Well if we understand. What pain is. Pain is a signal for change.
Pain is a signal to pay attention, [00:21:00] saying, Hey, there's something wrong here. It might not be the problem, but I'm gonna create a loud enough signal here to make you pay attention to find out where the problem is. So some, even something as simple as, you know, a groin issue or low back. I wanna know, can you move your neck?
Like do you have dural tension coming from the neck? If you can't get your chin to your chest without any tension, there might, the dural tube might be not sliding up and down, right? Which is the covering of the spinal cord. If that's not sliding well, all the nerves out of it. Now you've got nerve tension.
Well, if I see Will and
Dr. Grant Garcia: I trying to go like this, both women are like, if you can't, you're done. You're done. Will's out.
Tom Swales: Right? Can you look up without any pitchiness? Can you rotate your head and touch your collarbone? If you have pin or pull, okay, then we need to find out why can't you do that? And then you might be asking, well, what does the neck have to do with a groin?
Well, a neck, the neck is a reflex, okay? It's a cervical colic reflex. When I look to the left, it initiates turn to the left, but that initiates rotation, which is a pivot or a cut [00:22:00] change in direction because where the eyes go, the neck goes, where the neck goes, the body goes. So if I can't turn my head to the left.
What might I be doing from my lower back? I might be rotating. Guess what? The low back doesn't do. It rotates. So now all of a sudden, oh, you're rotating for your lower back. You're destabilizing the pelvis and now you might be using hip flexors and groin muscles to try and stabilize the pelvis to do the best job it can to protect the spine.
'cause you're moving too much into the spine. So now we're looking at, oh, the hip is moving. The hip is doing its job, but it's doing two other, two other jobs that it's not supposed to do. And now we have overuse. We have these progressive tears, and it's not the groins fault, it's because the groin is trying to do too many jobs to protect other structures around that aren't doing their job.
So now we look at physics. Well, your, your head doesn't turn to the left, so you go into your lower back, and now you're rotating too much into the hip and overstretching the groin. Well, energy moved in into the area of least resistance, which is the groin. [00:23:00] So now we have this overuse problem, but it's an, it's an energy accumulation problem because.
Other parts around it aren't distributing forces across the body effectively. So I need to know what parts are moving, which parts are not moving first, and then I need to restore some balance because if I have somebody who's trying to snatch overhead, but they can't rotate through their T-spine, those shoulders are gonna get torn up
Tom Swales: because they can't extend and rotate to that one side.
Well, that's gotta go someplace. They're gonna over rotate through the shoulder, and all of a sudden now they're destabilizing their shoulders and then over time we're tearing them down. The shoulder moves well, but the TS spine doesn't. So when we, this is why, this is where physics come into play, and when we look at something as simple, can you touch your toes?
Like, if you can't touch your toes without tension, why are you swinging, kettlebells and deadlifting? Mm-hmm. Like, it's probably not going to go well. All right. Runners. I talk about runners all the time. They come in, I got knee, I got low back. Okay, great. Stand on one leg with your eyes closed for 10 seconds.
They can't [00:24:00] do it. I said, okay, you can't proprioception.
Dr. Grant Garcia: That is huge,
Tom Swales: right? You can't stand on one leg for more than three seconds. How do you think running's going for you when you're putting two to four times body weight through your limb? Now all of a sudden you got an Achilles issue, you got plant fascitis, you got low back issues, and it oftentimes, it's not the leg that's deficient, it's the side that works pretty well.
'cause guess what? You're doing a little bit more on that side. You're leaning into it. 'cause your nervous system says, well, this side's safer. So I'm just gonna overuse that. Then you can start looking up kinetic chain. Well, maybe the ankle doesn't reflex, maybe the glutes aren't turning on 'cause of the hip capsule issue.
And now we moved into the Achilles. Like when you start to look at injuries from what's moving and what's not moving, it gets so simple as to, oh, this is why you blew this up, because you accumulated forces into this area because the parts above and below aren't doing their job.
Dr. Grant Garcia: Is so important. You just said, will we need be done with the rest of our podcast?
We have all the answers to the injuries now. We've been waiting for this.
Will Sanchez: Yeah, it's, it's [00:25:00] really important. Right? So you, you guys mentioned that, that you, people usually don't come see you until there's a problem, right? So. How do we get ahead of this? Right? Because you're saying, you know, that it's almost kinda like the, the wrist bone connected to the elbow bone, like we're kind of going through all that stuff.
Yeah. How do we get that information out there? Or, or where it becomes preventative? Yeah. What, what's the, the, the thought process going forward and how do we channel this information to say. This is what you need to do to in order to run. Yeah. Or it, you know, when you wake up and if you can't do this, this, and this, then you should avoid these exercises or you might have complications.
How, how does this grow?
Tom Swales: Um, the, the, the solution I came up with, at least for my athletes, because I'm not gonna teach 'em the A MT stuff, it's, it's very clinical, it's very, you know, nuanced. Yeah. So I, I created what's called a SAM scan, a self-awareness movement scan. The research says, well, the biggest predictor of an injury is [00:26:00] an old injury.
And I agree with that when it comes to the, if it's, if it's a repeat injury. But I think the greatest predictor of an injury is a lack of self-awareness because people come in and they're typing at their desk all day and then they're doing this right, turning their head to the right a thousand times and they're like, my neck, oh, I got this neck pain, shoulder pain, and I have no idea where it came from.
No, you do. It's just you did a thousand of these for the last 10 years, and all of a sudden you drove. Now you can't turn your head to the left and everything's moving and you're compressing joints and nerves. I'm getting should,
Dr. Grant Garcia: I'm getting neck pain talking about this right now. Right?
Tom Swales: So it hurts. Wait, hold hip.
There's always a reason. It's just people aren't aware of what they're doing in their environment. So the simplest thing I could come up with. I kind of streamlined a little self-assessment scan. I call it the SAM scan, and I used three cerebellar tests to make sure there's no top-down control issues. So rebell like sharpen Romberg, a facu test, and some coordinated movements.
If those are clear, then we look at what's the neck doing? Can you [00:27:00] bend it, extend it, rotate it, side bend. Can you touch your toes, can you back bend? Can you rotate? Can you side bend, can you single leg balance? Can you squat? If any of those things feel different. It's hard to assess ourselves, but I tell the athletes, I'm like, you feel pinch painter?
Pull, and does one side feel different than the other? If there's a yes, now we go. It's a little bit of an algorithm. Okay. You feel like rotation's not working? Check the hip. Can you open up the hip with a favors test? Can you rotate your T-spine? Yes or no? And if there's a no to those, great. Now you know you need to improve rotation to the TS spine and rotation through the hip.
Go back, check your global rotation. Clean. Good. Off you go. It streamlines a lot of their prep work because the older they get, they come in with 30 exercises that they need to do before training. I'm like, you don't have time for this, so now you're gonna do a three minute scan, two minutes of corrective exercises, re-scan yourself, and then now you're balanced.
Now go do your warmup. So it's just helping them create a [00:28:00] little bit of self-awareness in what's optimal, what's suboptimal. What is deemed as if it's pinchy might be a joint, if it's pulley might be soft tissue. And if it's, if it does, if it doesn't feel right, it might be just a motor control problem. So then you have solutions to the problems that you're feeling as an athlete or even as a, as a just a general person who just doesn't want to get hurt.
But I think you, we have to have these baselines of movement and that's, that's the kind of the simplest thing I could come up with. And then you can even use something as simple as, you know, you go, it's deadlift day. Go lift, go deadlift your warmup weight. What does that feel like? If it feels like a one outta 10 easy, great.
You're probably good. If you approach it and you're like, this feels like a seven outta 10 effort, something's not right. So now you're using warmup weights that you know are safe. So it's a form of evaluation, but it doesn't feel right. Go do something to make that feel easy, because the nervous system loves easy.
Something feels easy. That means everything's organized. That means [00:29:00] the nervous system's all switched on the right way. If something feels difficult, the nervous system is protecting something. It's inhibiting, it's downregulating, it's guarding. So now when we look at the neuro, the nervous system, which is that second pillar, well, when we measure movement, that's neurology.
That's looking at our output. That's looking at is what we're doing safe. Or is it not safe? Is it desirable or undesirable? Because if something is desirable, the nervous system takes the brakes off, it organizes and it increases motor output, which is mobility, which is strength. If it doesn't like something or you moved inappropriately, it locks it down, creates inhibition and weakness.
Now we, now we feel weaker, so when we're paying attention to these things, our body will tell us exactly if we're doing something wrong or not. We just have to pay attention to it. Because the body's not stupid. If it was stupid, we wouldn't be here as a species
Will Sanchez: can you that you were talking about, it's that, that awareness, that self-awareness that we tend to [00:30:00] neglect and maybe you're trained at this point that you're really hyper aware of what you're doing.
Mm-hmm.
Will Sanchez: I think a lot of us, and I'm speaking for myself, that sometimes we kind of. We have awareness, but we kind of move through it anyway. Right, right. Yeah. And, and then that's where we kind of put ourselves in situations where, um, they can be, you know, consequences. Yeah. Or we're like, well, today was debt lift day, I'm going to go debt lift.
Mm-hmm. So how do we, you know, have that mindset to say, it's all right bro. Let's do something else.
Dr. Grant Garcia: Yep. And
Will Sanchez: back off of this anyway, go ahead Dr. Garcia.
Dr. Grant Garcia: No, I was gonna say, I don't wanna say track from comment. Do you do when you talk to these athletes about the sort of reset, right? That's the three minute, two minute kind of thing.
What's the re what's the evalu reevaluation period that you recommend for that? Right? Because like you're gonna each, you see these athletes, right? Like they, all these pros, it's like there's a new injury each, each time, right? So is it, when do you recheck yourself? When do you reset yourself? Or do you keep the routine [00:31:00] for a certain amount of time?
Tom Swales: Every time. Every time. Every, every client coming in. I, I do a quick scan. I wanna see how they're moving globally. Did the exercises that I gave them, the, the, the session before, did it make a change and did it make lasting change? Because if it didn't make lasting change, I have to start thinking, okay, that didn't hold why?
I need to go back through the system to find out what, what did I miss? Or maybe there's a higher priority that I missed because the body is organized in priority. When you think about how we're developed, embryologically, we're just layers. Like we have those germ layers, right? And they're all tubes. But then you look at how we're organized from, from just a structural perspective.
Where's all the important structures, right? In the midline, right? Spinal cord, organs, brain. And then as we move to the periphery, those structures are less important for survival. We need all this in the middle for survival. So if there's compromise to our center, then when we, if we start working outwards and we start increasing power and output, the nervous system [00:32:00] won't let us increase strength because this is compromised.
We developed from the ground up when, when we're looking at, you guys have children.
Yep. Yeah. Right.
Tom Swales: Where did they first learn to move on the ground? Yep.
Tom Swales: What are they developing? Their center of strength, their center of gravity, their neck control. How important? Like you're watching your baby and you're like, oh, neck control. Okay, but you see the head doing this?
Yep.
Tom Swales: It's a writing reflex. It's all reflexive. You put your, you put something in their hand. It's a reflex. When they activate the hand, the shoulder packs. Everything is reflexes early on. Right? And if we go back down to the ground and we start looking at our center, if we develop scent, strength, and mobility from the center out, well the periphery tends to take care of itself a lot of times too.
But if we start to sit on machines too much, or we start to strengthen the periphery, we. We start overpowering our center of like our spine. The nervous system starts to shut down and we get plateaued and people are just like, oh, I plateaued on my squat. I'm like, yeah, but you, you can't touch your toes [00:33:00] anymore.
Like you've got this little pain in your back. So your nervous system is protecting you. You should thank it. Why it gave you that plateau? Because plateau plateaus are protective. If, if there's no pain or dysfunction. Then we know it's a connective tissue or structure problem because the, the, the nervous system will not allow you to keep loading muscles.
If the joints and the tendons can't handle it, it's going because you're gonna blow them out. But when we look at biology, how long does it take muscles to adapt? Six to eight weeks. How long does it take tendons to adapt? Six to eight months. So it's a slower process, which is why when we, when we plateau, we have to be patient with that, keep working the repetitions, and all of a sudden, once the connective tissue and the structure catches up to the neuromuscular system, all of a sudden, next, next, next level.
Dr. Grant Garcia: I think this point you're making is really important. I think that the listeners always wonder, what do the athletes have that we don't? And they get someone like you, right? So that's, that's the difference, right? They're, they're special patients, but then they're, you hear [00:34:00] this like. All the knowledge that we just heard is, is fairly unique.
Even though this is something that you guys teach and some of the high level people teach. It's just that we don't hear this as layman people. I mean, even as orthopedic surgeon, I don't hear this that often. Right? And when the athletes say, how do I get back? I'm like, well, I can fix you. But you know, after the surgery's done, you're 90, near 95% of the work.
When they come to see you.
Yeah. And
Dr. Grant Garcia: so that's really important and hard, and hard for me to understand. Right. I'm in the office, I got five, 10 minutes with a patient. Yep.
Dr. Grant Garcia: Uh, they come in, they're in pain, or they're post-op and they're trying to recover. They're like, well, what else can I do? I'm like, honestly, they gotta see people like you because you guys can look at the whole body.
You can recenter them. I'm not the expert at the lower back. I'm not the expert of the core, but as you keep talking about. Core, well, core and lower back is just boring. Right. It's it's not no glamor there, right? No. You can get abs That's great. You can have a nice lower back. You don't ever say that guy's got a nice lower back.
I mean, maybe I, I don't usually say that, but Will Maybe does, but a different animal. Yeah, all the time. We, all the time. But you know what I mean? Like we all want [00:35:00] buys. We all want nice legs. We wanna be super athletic. Yeah. But this is the, it's the, I mean, there's so many people, I mean, look at me. I, I could barely lift my neck up 'cause I have so much surgery and I'm just like, my back's always in full spasm.
Right. And, and it's because we forget about that. I mean, those power lifters, like you said, like people can't touch their toes. Yeah. Right. Like it's a huge problem. Mm-hmm. And that's one of these things we always talk about, like, you see Will, we've talked about this, like these athletes that are doing like yoga and they're doing ballet and Right.
Why are they doing that? Because they're trying to go back to the basics, the idea of like. Simplest, like, you know, people used to tease about this stuff, but really it's, the funny part is like, that's what makes these, the, the really good ones. Yeah. Better than the lots of good ones.
Tom Swales: Yeah. I mean, so you, you can look at the other, you, you know, you have one end of the spectrum where you have your power lifters who are very tight and stiff, which to, to their sport can give them a mechanical advantage because they can use that stiffness, right?
They're a stiff spring. They don't have to use as much muscular energy to push and load the weight. They can use their connective tissue. But then you have the other end where [00:36:00] the, you have the yogis and they're two hypermobile or the dancers and Yeah, you got, you can do a full back bridge, but you have back pain too.
Yeah, but they're unstable. They can't hang on to tension long enough and they're moving too much. So now they're down. The nervous system is trying to lock up and stabilize them to prevent them from moving because they just can't hang on to tension. They're not strong enough. And then you have the power lifters.
Well, they have back pain because nothing moves enough.
Dr. Grant Garcia: So Well, I need something you have to worry about with surgery too, right? Yeah. Like our patients, like is this a loose patient or is this a tight patient? Right. People don't realize that, you know, the patient comes in, she's like, I've had 25 surgeries.
I keep dislocating things. I can go put my hand behind her back. Right? That's this. I have the same patient with dislocation of one thing. And I'm like, listen, it's a totally different perspective, right? One of them, I'm gonna force like no surgery. This is a bad problem. The other one I'm like, maybe this is an issue.
So the same thing you're talking about, we, I, in my head, each patient I see, I'll see three or four of the same thing, and each one has different category. Yeah. And it's what you're talking about. And the connective tissue makes a huge difference. This is [00:37:00] something that's important. Will you have something you're about to say?
Will Sanchez: No, I, I was just kind of. Pretty much, you know, what you guys are talking about, right? You're, you're talking about, you know, reducing pain and improving movements and, and I know that you've been teaching these, you know, neuro hacks, uh, to, uh, clinicians. I just wanted to see if, you know, if these were some of the examples that you're teaching, or do you actually have other ones that involve with the neuro hacks?
Tom Swales: Newer hacks as in like using
Will Sanchez: Yeah, like just to improve, um, movement. Oh, yeah. And, um, also creating strength, you know, as you're teaching that not only to, you know, the, you know, your patients, but also to the people that are working with you.
Tom Swales: Yeah. So we, we can use the, the fun part about the nervous system is when you apply something to it, if it's desirable, it changes pretty quick.
So will I see you're standing up, right? I am. Okay, so if you take a step back, can you touch your toes?
Will Sanchez: Oh, [00:38:00] probably not. I'd be standing up. Okay. Let's
Tom Swales: just, I wanna see if I can get you touching your toes right now.
Will Sanchez: Um, I, I touched my ankles.
Tom Swales: Okay. Not too bad. Okay, so you have a tight neck, correct?
Will Sanchez: Uh, a little bit.
Yeah,
Tom Swales: A little bit. Okay. I want you to just use a simple isometric. You're gonna take your hands, you're gonna take your neck as far as you can go. I want you to look down at the floor, okay? Push your head into your hands. Five seconds. I'm gonna do this too. Okay. And now bend forward and touch your toes.
Okay. Take your hands off. Touch your toes.
Will Sanchez: Yeah, I touched my toes, right? All right. Thanks for coming,
Tom Swales: Tom. We're done with
Will Sanchez: you, Carlos,
Tom Swales: but you, you can see how this is amazing. One end affected the other, and everyone's just like, well, I have tight hamstrings. I'm like, you probably don't. I mean, you might. You don't, but if your neck doesn't bend, these flexors, tie in with these flexors.
So if these aren't working, these flexors are not working. If these ones aren't working, guess where you're overusing? You're using all the extensors too much on the backside and now you're trying to use extensors to lower yourself to touch your toes [00:39:00] rather than use the flexors to pull yourself. All we did is we, we facilitated a circuit.
Flexor circuit starting from the neck and your eyes, because when you look down, it initiates flexion and all of a sudden the nervous system organized from the top down and all of a sudden you could touch your toes. It works the same way, like if you've got a tight neck or a tight low back.
Here we go, go
Tom Swales: here and then do a little back bend and see if it takes away a pinchy low back.
Dr. Grant Garcia: It feels good. I think we got, I think we got our new, uh, sports doc talk, rehab specialist. You know, every time we call someone, we get the docs are, the docs are tired, stiff,
Will Sanchez: be sick of us. He's gonna Guys, come on, man. Now I do. I do. You're Dr. Grant Garcia: gonna, you're gonna get so many people calling you for help after this episode.
I can't wait.
Tom Swales: I do, I do. I have a presentation that I, that I do. Um, I've done it at the Ontario Physiotherapy Association. It's my, uh, eight neuro hacks to move better and reduce pain in 60 seconds or less. And I make it interactive because it's a 30 minute presentation. But I, I use, uh, different breathing techniques, [00:40:00] eye exercises, isometrics, tapping for proprioception, um, and a few other, a few other things.
And all of a sudden everyone's touching their toes, their single squat, and. You know, I ask people, which one worked for you? And they're like, oh, for me it was the eyes. I'm like, okay, cool. Because we stretched out the eyes, and the eyes initiate the cerebellum. The cerebellum is the part of the brain that that, uh, measures rate, rhythm, force, and accuracy.
But it's 10% of the mass, but it's 90% of all the neuron, or 50% of all the neurons. So you've got a majority of those neurons in that 10% mass, but it regulates all your movement. But if you stimulate it. With canal balancing in the inner ear, the visual system isometrics, you know, spiraling anything, cross body or crane figure eights, it stimulates that part of the brain and that's the part of the brain that we first learned to use to move as children.
This is,
Dr. Grant Garcia: I, I feel will I, I feel do, I don't know about you will. I feel, I feel stiff, but I feel enlightened. [00:41:00] So this is great. Uh, Tom, I, I do not wanna miss out on the opportunity to talk about your certification. Sure. Okay. So, uh, we would, if we could have you on for like three hours. Then all the social medias would hate us.
Three hour show. No, we're not doing that. It'd be, it'd be, we're not gonna keep you on for three hours, I promise you. But I want get to the advanced movement therapist certification because obviously this is unique, right? Yeah. There's not many people I know. I do know tons of therapists in the area. I work with tons of'em as a sports doc.
Uh, but I wanna learn about this. Can you talk about like. The process you went through, what does it mean? I mean, this is something that people are gonna wanna know about. They're gonna wanna know, hey, if someone, one of the therapists I know sees this, they might be like, Hey, I'm interested in learning more of these, sort of the stuff that you're talking about.
So can you talk about what the, the certification is?
Tom Swales: Yeah. So I mean, it came outta my own frustration where, you know, like I said, I, it was flavor of the month for every client. I do more courses. I'm like, here's the answer to all my problems. And I, it just became Guess Wing and I hate guessing. And then finding these, these principles across it.
I started to organize it. [00:42:00] So what I did is I created a framework. We use, we look at posture assessment. How's the body holding itself? What's it avoiding? What's it hiding? I mean, a lot of people say, well, posture doesn't tell you much. No, it's true. It doesn't tell you much, but it can kind of guide you as to, well, what's the body hiding?
What's it protecting? What's it guarding? What, where's the atrophy? You know, like all these little things. And then you look at the how the body's moving as a system first, and then you start breaking down the parts. The third thing we always check is the neurological system because everybody is neuro until proven otherwise.
Why? Because the nervous system controls everything. If I have neuro tension, if I have central neurodynamic issues in my spine, if I do a slump test, I need to take care of that before I try and go after tight hamstrings or tight, low back. 'cause if the nerves aren't sliding. Nothing's gonna work. I need to look at myotomes.
I need to look at upper extremity. Then we look at the pieces. We start to split it upper, lower body. We start to look at what are the shoulders doing? What are the hips doing? What are the ankles doing? So we look, we start to break it down into the parts, but we need to know what the difference is between active and passive and what is [00:43:00] optimal.
If you don't have optimal range of motion, I'm like, well, why is that side moving different than that side? Is it an anatomical problem or is it a mechanical issue that we have to go after? Because if we can change it, I want to change it. So, because again, when we look at physics, we wanna see where's energy moving?
If forces are avoiding this area, but moving over here, this could be why you have this injury. And then we start to look at, and then you like the later things are the special test, but I literally organized. Everything we do as clinician in an orthopedic assessment in an algorithm, it's in this specific flow, and it starts with communication and then it works at the global movements.
It looks at neurology, and then it starts to look at the parts, and then as you move from there, you can start doing what, what I call connectivity testing the foot. Just like the, the hand in the shoulder, they have a reflex, but you can test them together to see if the muscles of the hip are being turned off because of a foot issue.
If you've got an over collapsed foot or there's a proprioception problem, if I put my hand on that foot and I [00:44:00] test the hip rotators, the hip turns off. Well, why? When I tested the hips on their own, they were fine, but we know, okay, the foot is inhibiting the hip, so then you can start to look at all this connectivity and what's influencing what in the system because nothing works.
Independently. So we, it, we, we start to go through the, the pieces and the parts, and then once we find those linchpins or those primary areas of dysfunction, we correct those and then we start working our way back up so we correct from the ground up. Most of the times people have to go back on the ground to reset stuff.
But then we start to look at, well, what can, what directions can you control? What body parts aren't talking to one another? If they have a concussion, there's a whole separate algorithm to look at. Cerebellum, visual vestibular, and then inner ear. So when somebody tells me in their history, oh yeah, I have an old concussion.
I need to screen that first. I can't assume that that's gone because even old, like old concussions can still cause new orthopedic problems because one side can fight different than the other. Dr. Grant Garcia: I don't wanna interrupt you, Tom, but this is a constant topic on our show concussions. [00:45:00] Yep. Right, will. Yeah. Yep.
So I think this is huge. I mean, it's always hard to find someone that deals with concussions. So the idea, I'm not gonna go after you with concussions right now, but. I wanna make sure listeners here, we, we later. But the idea is that, like, you just brought it up, it's just like he's, he's thinking about everything here.
Yep.
Dr. Grant Garcia: Um, Tom, will you tell us, uh, what sort of the, the, I saw on your website there's different certification timelines, like how long would a therapist most, I'm assuming most therapists are the ones that would do this course. Yep. Uh, how, how long would that take a therapist to do this course? Roughly certification.
Tom Swales: So the, it's a total of 28 hours. Level one and level two. I mean, it's go, it's go at your own rate. We have anybody who starts with our company, they have to have the level one done in the first three months. So this is a, I think this is a live workshop that I was doing. I was doing it live before, but now it's on demand.
So you can, everybody can start today. You go through quizzes, you go through the textbook, and then you finish the, the examination at the end of level one, and then you can [00:46:00] apply to take level two, which is when we get into the neurology, the uh, gate. The, uh, ballistics, the, all the high performance stuff is in level two when we get into kettlebells gymnastics and all the other, um, training components of it.
But, uh, I mean somebody, if, if someone's eager, they can finish it in a couple months. Level one and two.
Will Sanchez: Do you have a requirement for the type of person that you're looking forward to be with these, you know, be involved and learn from these courses? Or is it just open to anyone that just wants to learn?
Tom Swales: So over Covid, I was able to test this hands-free. This doesn't have to be anybody who's working with people who trying to get them out of pain. You could be a kinesiologist, you could be an athletic trainer. Yeah. What? So if you have hands, if you have a license to use your hands and test and use manual therapy, great.
Because that allows you to change the inputs faster. If you don't, well, this is when you use specifically lacrosse balls and foam rollers and bands to go after joint issues. But you're gonna learn wh when you apply those, at [00:47:00] what parts at the right time. Because a lot of times people just randomly foam rolling everything.
I'm like, what the hell are you doing? Like you don't need to foam roll. Like, you should be doing some rolling patterns, like you're not stiff. What? That was me
Dr. Grant Garcia: for a while. I understand. Sure. And it, it feels good. I've learned, but I've learned now from Tom. I'm not doing that ever again,
Tom Swales: but, but if it feels good.
Okay, so here's the thing I, I'll get on the formula. My lots tighten up. You know, it changes the inputs as long as you know what you're doing and what you're doing it for. And as long as it's making a change, I'm all for it. But if you don't know why you're doing it. If it's just randomly rolling around and you haven't checked anything to see if you're changing anything, then we're wasting our time.
Dr. Grant Garcia: Right. I think that that was, what you said was perfect. I don't want to interrupt you, but I love, I don't mind popping in, but I wanna make sure the listeners hear this. If you don't know if you made progress, there's no point in doing it. No, I think that is excellent. Because there's patients that come in and I'm like, so how do you feel?
It's been three months since we saw each other. I don't [00:48:00] know. Right. Geophys? I don't know. Uh, okay. Um, where does it hurt? I don't know. Um, or I can't tell you. Right, right. That is extremely important because if you don't have self-awareness of what's going on, you don't know. I mean, I, one of my, uh, my father-in-law is a occupies surgeon.
He talks about the pain scales. Yeah. And the interesting thing he brought up is that. Someone comes in to say the pain level of six or five, and the next six months they say it's the same level. It hasn't gone better. Right. Usually it means it actually has, it's just they got so sick of the pain that like they just can, they can't tolerate anymore.
Yeah. And
Dr. Grant Garcia: the ones that tell you that it's gotten worse, that's where it's actually gotten worse.
Right.
Dr. Grant Garcia: Uh, so you just, it's this concept of there's also the mental aspect.
Yeah.
Dr. Grant Garcia: But the idea is like if you have, you don't know how you were and where you're going Yeah. Or what you were at before, and you don't write it down or learn about it, you can't understand your progress.
And like you said. If you're rolling your foam and then like you never checked you, you know, will did his test, right? He put his hands, his head. Yeah. He's able put his lit feet down. If you don't check it and you don't know what you can't do and what you do now, yeah. Then you have no idea what's going on and you can't conceptually make progress.[00:49:00]
Tom Swales: No. You can't manage what you don't measure. Right. And what you don't measure, you can't change. So this is where like when I got will, I'm like, touch your toes first before we do anything. Okay, we have a baseline now let's do an intervention. We did the intervention, let's check our work. Let's see if it changed.
If it didn't change, let's try something else. Mm-hmm. The one thing that drives me bonkers is therapists. I'm gonna blame therapists. They're doing the same treatment on, on the person. There's no change. And when they finally come and see me, they're like, yeah, I was seeing so and so for like a year. I was like, well, they're super nice and you know, it felt good, but nothing changed.
I'm like, well, were they doing the same treatment all the time? Yeah. Well, percent. How did, how did you measure change? Oh, I don't know. I'm like, well, you know what? The definition of insanity is
Dr. Grant Garcia: doing the same thing, but not, yeah.
Tom Swales: And expecting it. So I blame both of them, but I blame the therapist more because they're the person in charge and who should be checking their work to see if the patient is making changes and if they're not, shame on you.
Dr. Grant Garcia: This is, [00:50:00] this is ex uh, will, this is like, this is literally like my day every day. Right. You have the patience. I have the patients that come in and I have my go-tos. Right? Am I really wanting good ones? Yeah. And I, and they come in, I, I know the patient's been checked, right? I'm like, what's your quad score?
Yeah. No idea, right? Like, what's your quad score? 75%. Boom. They know. So that's the therapist or that's the A TC or whatever's Doing the checks and doing the reset. Like, okay, you're not you, let's check your progress. I know there's some people and I go, wait a second. Who, what do you who you go to? Like, what are you doing?
Because you're clearly are not making progress. And then the problem is, see, for you, you're coming in, you're the opinion. For me, I'm the surgeon. I've fixed them. So they're expecting the results they want. I have the same surgery. One patient is absolutely killing it. One patient is not. And the reason is that some, a lot of times it's because they're not getting those checks and I have to switch things up.
It's like what you're saying. They're really nice, but they haven't done a great job. And I will fire people frequently and move on to another, a group because I'm not happy with the way the progress is going and I know what my patients should do. Right. It's [00:51:00] like you see this person. So that point is, uh, that point is so important for the patients to hear.
Yeah. Right. There's times when there's complications from surgery and you're not doing well because there's a. There's way more often a time where you've got stalled because you're not getting the repetitive checks and no one's giving you the goals where you actually need to be. Exactly.
Will Sanchez: You know, you're, you're such a passionate educator, right.
And we start off the show talking about you're, you're always consuming knowledge. You're at a standard now for yourself. Yeah. And for others. What, what are you looking for? Internally, externally, to keep growing in the areas that you are. Like, is there something there that like, yeah, I do this, this, and this.
I wanna keep building on that, but I wanna focus now on something else. Is there something else that, that, yeah, you're kind of looking forward to and being passionate about, that you're just kind of tacking onto your resume as your career, uh, continues to grow? [00:52:00]
Tom Swales: Yeah. No, like everything, everything is moving in the direction.
I can, I like to think outside the box. Mm-hmm. Because the more things, the more perspectives. Again, this is why I came up with those five tenets. 'cause I love learning about physics. Well, how can I apply that to the, the, to the physical body? How does that pertain to injury? How does that pertain to pain?
That's how, where I started to, you know, I started looking at physics. I'm like, oh, this is an overuse injury. Right. Uh, when I was, uh, when I was working with one of my mentors, he was huge in traditional Chinese medicine, acupuncture, and he would use some language that I'm like, I have no idea what you're saying, but I appreciate it.
I'm like, oh, shit. He's talking about physics and neurology. Like when he, when he is talking about the, the channels in the meridians, I'm like, oh, that's physics. I get it now, right? Mm-hmm. Like when, um, you know. When we're looking at, uh, specific things, I'm like, oh, that's the nervous system, right? Like it's when you, when you start to pull from all these different realms, you, and, and you have principles that you bounce those ideas off of, now you can [00:53:00] assimilate information more easily because I can compartmentalize it.
Gotcha.
Tom Swales: And, and now I can hear something once as soon as I compartmentalize that into the framework that I've created. I know when to pull that out because I've, I've, I've placed it in the right spot. It's not random information anymore. And now I can pull that out whenever I want that anecdote, that, that case study or whatever, because I've, I've put it into a file that makes sense in a framework based on principles.
Dr. Grant Garcia: Gotcha. And, and Tom, do you think that some of the stuff that you talked about, like you said, the certification and. Hearing your podcast with, you know, being on this podcast and seeing your stuff on your website, is that gonna help someone get up to speed? I mean, you have a lot of knowledge. You have a, you have a strict, you have an unusually awesome desire for more knowledge based of how many certifications you've done.
You know, I, I, I really hear what you're saying and learning all this stuff so quickly. But do you think, how would someone who's young, you know, and I know you're, you're young too, and we're all young, but basically someone who's new, how, how are they, how are [00:54:00] they gonna. How are they gonna not see this and go, oh my God, that seems like a no possible way.
I could be that way. What do you, what's your suggestion for the new, the new one? The new person?
Tom Swales: All I did was, I just distilled it down the way. I'm talking about the principles. We don't go over that in the certification. I'm actually writing a book right now on my experience and how to stay
Dr. Grant Garcia: tuned, guys.
Yeah, stay tuned
Tom Swales: that that is another journey on its own. So. A lot of the things that we talk about is gonna be in the book, but when it comes to the actual certification, it's, it's the nuts and bolts, it's the practical use stuff. You know, it's a lot of, it's gonna be very familiar to people, um, but it's gonna be organized in the exact way in which to apply it.
So I just helped create organization from the chaos in, in what we do as practitioners. Um, I'll give you, so as an example, we, we always, hi. We hire new grads. I love new grads. And, you know, when we first opened our clinic, we're like, okay, we're, we're the top clinic. The high expectations are high, [00:55:00] and we would hire 20 year vets coming in.
And they have so many bad habits. I'm like, okay, this isn't working, and they don't wanna learn. And then, and then like, okay, let's try new grads. And then they would wash out after six months because they're not effective at a school. And they lose confidence and their caseloads are emptying. Right? 'cause the expectations are high.
Coming into our facility, I'm like, what is it we're doing? Like how do I, how do I teach this? Mm-hmm. And then, so I use this as part of one I'm organizing what I'm doing. Two, it's a training system for all my staff so that they get really good, really quick. And then even for, for clinic owners. They can use this as a training manual, as a, a high standard across all clinicians, young or old.
Everyone's talking the same language. Doesn't matter who the patient sees, everyone's gonna be good. So I have, uh, I have a two year clinician. I would pit him against a 10 year who's got their f camped and needling any day to find the actual problem and be effective quickly. So. It really [00:56:00] shortcuts your, what I'm seeing and what the feedback I'm getting back, it's shortcutting a lot of their success.
We'll show
Will Sanchez: that feedback. Hold on a second. You just throwing stuff here. Well, we
Dr. Grant Garcia: got, we got four minutes left. I want you to show the feedback before we get up. I don't want to kick off Tom, but the, the social media's gonna be mad at us if we go over an hour and I knew this was gonna happen with him. So the, so, so basically, you know.
Obviously we gotta wind down. Sure. Uh, I know we, you know, maybe have you on in another year or so because it's been awesome and I wanna make sure that. But again, we really appreciate you coming on. What do you, what's, so what's the, you talked a lot about all the stuff you do and obviously you can see, look at these glowing reviews, um, to really sidetrack maybe your final comment for patients listening.
Right. 'cause not everyone can go visit you in Ontario. Sure. Right. That'd be awesome. They could, uh, but not everybody can, we are not doing
Will Sanchez: I thought we were going up there.
Dr. Grant Garcia: I'm,
Will Sanchez: I'm
Dr. Grant Garcia: ready to go up there.
Will Sanchez: I, he, I.
Dr. Grant Garcia: I got my plane ticket [00:57:00] book. I've been booking it while you guys have been talking.
Will Sanchez: Sure. Had a couple of nice restaurants that we could go to and hang out and meet the wife. We, we talking about his wife that's working with him. Will, you're digressing my question about,
Dr. Grant Garcia: I said we have three minutes left and now you're disrupting me.
My bad. I apologize. Uh, no, no. So for patients long lasting effects, like how do you keep this like, right, like how do patients see. 'cause someone's not gonna be able to see you all the time. Right. Either it's in the US it's insurance based or things like that. And Canada, it's sometimes a little bit different.
But nonetheless, like what's your sort of goals for these patients that get all this information? Like, you know, like Will's should, will go home every day and do this just so he gets self into a stretching mode. Right now, what's my
Will Sanchez: wife and daughter we're gonna, a lot of, a lot of
Tom Swales: it's just educating the patient, what's going on, what they can do.
Don't focus on what they can't do. Um, show them the changes that are happening so that there's buy-in. You know, you know, clients that come in for that first appointment, if all of a sudden I get their pain down from a 10 to a three and they're moving better [00:58:00] than they ever have, great, now I have buy-in.
They have belief because I showed them their ability and belief often comes before ability. Sometimes I have to change their ability to change their belief. And once we've changed that, now we've affected their psychology and then they can move forward and then they're gonna take what they know to continue to apply it, to continue to move forward.
Awesome.
Dr. Grant Garcia: Well unfortunately our time has ended 'cause we are 58 minutes and 26 seconds. Will do you want any closing remarks?
Will Sanchez: Tom, thank you so much for your time. Thank you for having me. We know it's past your bedtime. Uh, so it's, uh, it's something that, uh, we recognize it's great information and we, uh, once again, we're, we're just really thankful that you could take some time, join us.
I. Really educate the listeners, educate ourselves, because God knows what I'm going to show my wife and daughter now and see what we could take from that. But, uh, just remind everybody, check us out, sports.talk.com. Uh, we've got shows, [00:59:00] transcripts and we're always looking for, uh, other shows. Uh, so we're very happy and pleased with the feedback that we've been getting from everyone.
And as always, we're really thankful for our guests like Tom. Tom, thank you very much, Dr. Garcia. Say goodbye. Yep,
Dr. Grant Garcia: grant,
Will Sanchez: thank you. Thank you so
Dr. Grant Garcia: much Tom. I'm really excited for the listeners to hear this one. Awesome. And, uh, I think, you know, this is gonna be a real, um, uh, this is going, this episode's gonna come up a few times in our next podcast 'cause this is, we learned a lot today.
So thank you so much. And as always, this is not what I expected this episode to be, so this is absolutely awesome. It's way better. So thank you, Tom.
Will Sanchez: Thank you for having me to change the mind. I channel the body. I love it. Good stuff.
Audio Transcript
Gerrit Cole’s Season Ending UCL Surgery

Gerrit Cole’s Season Ending UCL Surgery
Will Sanchez: [00:00:00] Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia. Uh, Dr. Garcia, before we get into this, um, there's a Simpson kind of cartoon meme where, you know, uh, the dad kind of walks in and then grabs, puts his hat down and grabs a hat and walks back out.
That's how I'm starting to feel about my Yankees to start off this 20, 25 season. It's a revolving door of. I don't think that this is going to be a great season because of what we're going to talk about right now. And I know for most people watching this, they could give two hoots about that because they is, uh, as most people like to, uh, root or not root against the [00:01:00] Yankees.
Uh, this is sweet music to their ear. How are you? What's going on?
Dr. Grant Garcia: I'm good. Yeah, I know for us Yankees fans, this is a good, this is a tough one, but obviously if you are, you're either a Yankees fan or you're not a Yankees fan. That's pretty much the way it works. So, uh, the, this is a big, this is big news, but obviously I think the reason we want to talk about this is the fact that you can see how the news can construe things, right?
Like we saw with Aaron Rogers, Achilles repair or other things like, and what are these products that they're construing or what does it mean to try to like help the viewers understand better, right? Cause this, these two topics we're going to talk about are not new. But what does it mean? What are the nuances behind it?
Because obviously even CBS News and ASPN, they kind of got it a little bit wrong and a little bit different. So we've got to go over it.
Will Sanchez: Yeah, you know, and it's probably something that, you know, Cole's going to need down the road. But, you know, let's talk about our people over here at the recovery shop and might be just give a little shout out to these [00:02:00] folks out here.
Dr. Grant Garcia: Yeah, so shout out to our sponsors recovery shop. They're awesome. You know, patients love it. You know, my partners are doing more of these now too Because the patients really want to have that sort of extra special stuff I'd help them with their recovery from the nice machine to the rebless, you know, to all other options, scar creams, you name it.
And so they can all find it here and it can be individualized to the surgeons. So the patients feel like they're getting really a custom experience. Um, so reach out to Mike B. Uh, they're awesome. They'll work with you. They take care of a lot of different surgeons across the country. And we're happy to have his sponsors,
Will Sanchez: you know, um, it's tough, right.
As we go into the Yankee fandom here, uh, we lost Juan Cotto, you know, and kudos to him. He's staying in New York, um, with the New York nets, but that was a loss. We heard about, uh, Stanton and what he's going through. He's having this tell. tennis elbow issues. And there's some other stuff going on with his calves.
I think we could do a whole show on not [00:03:00] only his injuries, but past injuries that will probably check off every box that you have when it comes to orthopedic surgeons and surgery. But the big one was with Garrett Cole. right? And there were conversations at the end of last year that he was starting to have, um, potentially medical issues.
He wound up kind of just, you know, grin and bear in it and pitching throughout the season and finishing off, which pretty much you know, took him to the World Series as he tried to compete. Um, knowing now that he had to have Tommy John surgery, and this is exactly where we're going to talk about the procedure.
I want to reflect going back to, uh, last year. What do you think were some of the signs that The doctors were seeing that they were discussing within an organization and how they came to the conclusion to have the Tommy John surgery. Do you think that was something that came up in spring or this was something that was brewing since last year?
Dr. Grant Garcia: Well, what's [00:04:00] interesting is, if you look at, like, if you take care of baseball players, the small, the, you know, the High school level, college level, they tend to come in and they need it, right? It's like, there is some things on the fence and we have a lot of discussions with our players, but generally they come in, especially with the reconstruction.
They come in, they've blown out the elbow and they can't play again. It's a little different with some of these pros. I mean, you've seen a number of them where they kind of like limp along. They're still playing at a pretty high level. And then all of a sudden they like shut them down and then they get the surgery.
Right. And you're like, what happened? Like they didn't, they didn't throw in this blow out the elbow. So I, I think from the pro level, these guys are so good. And also I think there's a level of like, if he's dropping like two miles an hour. You know, or he loses some sort of pitch velocity pitch change, like it may not be enough that he's just going to not be an ace.
Right. And so they may have to just pull the trigger. Obviously, it's no small feat with a player of his level with his contract and the amount of money he makes and who he plays for.
[00:05:00] There is a situation where it's like, if they just can't be optimized, do we just go do certain, right? Like their arms are worth so much money, it's not worth it for them to try to play and hurt themselves.
So. It could, it could have been an acute issue, but generally it's also hard to tell on these guys because the MRI is all kind of, they over time, the UCL or the ligament, which you're talking about the one on the inside of the elbow. it gets stretched out. And so you don't always know if it's a good ligament or not just from the MRI alone.
So there's lots of other things that go into factors and all of it's also player, agent, surgeon, team's decision. So this is not just one person deciding on that.
Will Sanchez: Yeah. Yeah. And we've talked about that before and that was a perfect way to explain that. It's, there's so many people involved, including the player, uh, whether, like you said, the agents.
you know, general managers and you know what's good for the franchise, especially long term as he still has a hefty number on his contract and [00:06:00] they're just not looking at 2025 for the rest of his career. He just completed his 12th season last year. He was about to start the 13th season. Um, and we've seen these, um, these injuries occur.
Any concern with his age, the miles on the elbow as far as recovery. And I know I'm jumping ahead, right? I'm kind of putting the carriage before the horse because I'm already talking a little bit about post. But I'm just curious what your thoughts on initial thoughts on when it comes to someone that has had this longevity has been a power pitcher and is performed at the highest level.
Dr. Grant Garcia: I mean, you're always worried, right? I mean, any big surgery on the elbow. The return to sport is good, but it's not amazing. Now, this is one of the surgeries where people actually get back and they do play at a high level, and they've shown that even the first few years are really important. You know, maybe four to five years on the road, they drop off.
But at the same point, you know, he's, I think he's [00:07:00] 34. Uh, and so, or something like that. And so as a result, he's, by the time he's at that point, he would expect to have declined anyways, you know, maybe, obviously he's not a Berliner or whatever. Um, and maybe he will be. But, you know, that's something to be aware of.
Right? So it's like they do get back and they get back to a pretty high level, but not 100%. Um, but it's just something to be that you'd need to be on the radar for people that, you know, this is a good surgery, but again, it's always surgery. There's a chance he's going to back to his normal level and they kind of limp along.
Now, again, these guys are so high level that they can limp along and still be considered good. They're just not the best.
Will Sanchez: All right. Let's talk about what this surgery is. You know, we've heard, uh, Tommy John. surgery, and it's really this UCL surgery, right? And then I got excited because anytime that we could talk about internal brace, because, uh, if I'm going to sneak into an operating room, this is exactly what I want to perform.
I've watched too many videos and gotten my, my overall, uh, information on internal [00:08:00] brace. So I was like, Dr. Garcia. We got Tommy John and we got internal brace. Talk about what this procedure is and what's going on with that.
Dr. Grant Garcia: Well, let's back up in a second. So when we got the text, you texted me about this injury and we're like, let's do this, this podcast.
The The CBS article was incorrect. So this is why this is most interesting to talk about. So the article cites internal brace now going to recover faster. Good news. Yeah. Right. So the first thing I'm thinking is, wow, this is a high level picture that had a UCL repair with internal brace, which means we talked to us before and you can show the picture of it.
So we'll go through it very briefly. I will tell you that that is not the surgery end of having. But the way that the article spun it, this is what they thought they were talking about. So they, unfortunately, they didn't do as much research as they probably should have because if you look at three more articles, it tells you actually what he had.
So you can see here, this is the internal break. So what happens is there's the UCL, that's the elbow and that's the ligament that is. So that's the multimillion dollar ligament right there. [00:09:00] That's the Tommy John baseball ligament. So that ligament gets partially torn. And then over time, we can fix it. Now we have this internal brace, these sutures that are college and impregnated.
And the idea is that they grow into the ligament and add stability. And it used to be that you could ever do this. And now we've got this type of technique, which internal braces now all over the body that basically found that people will go back to throwing faster, like significantly faster, like six, seven months versus 12 to
Will Sanchez: 18.
And
Dr. Grant Garcia: so when we initially read that, we said internal brace surgery. So now as we get back faster, I'm like, wow, you got to use your repair. The problem is that the internal brace can also be added in a reconstruction. And so that's really what he had done because Neil L trusted. And we know he's the, you know, the man, the man of all men, uh, the surgeon of all surgeons.
Will Sanchez: Yeah.
Dr. Grant Garcia: So he added some extra flavor to it. So, uh, he ended up getting a reconstruction. The thought was he added the internal brace. So maybe you'll get back past, you know, there's not a lot of data to show that an [00:10:00] internal brace. With the reconstruction is going to get you back faster. So that is something that people should be aware of.
This is probably what he had done. This is the docking technique. It was designed by somebody, HSS. Um, and he might have done even a small hybrid because we're all working on ways to make this better. Right? But this is taking a ligament from his wrist or probably his hamstring, one or the other. Um, and that's the reconstruction that we all know that's the most commonly done one for pitchers.
That repair is becoming more popular in pitchers. And in fielders and MLB, and now, you know, all over the place, you've seen it multiple times, um, in, uh, in football, we talked about Brock Purdy, uh, Ben Roethlisberger had that, there's been a number of other quarterbacks, so there's, and then, there's a gamut of players that have had it in college and high school, but this reconstruction is really what he had done, but what they did is they added the internal brace in the middle, it's interesting because you can't find a photo of this on the online, like I have a picture from my own surgeries, But you can't find a photo of it online because the techniques have not been refined yet.
So these are sort of still [00:11:00] doing new ways to do this. The reason it's hard to do the internal brace with this surgery, if you go back to it real quick, I want to show the listeners. So normally the internal brace is fixed by two points, right? With those anchors. So go previously one more time. I want to show them, explain them again.
So you see how that internal brain has two little holes. Those are anchors. Now go back one more. I want to show that again. I know we're jumping around. Look at this. Here's a bone tunnel there. So you have to pull the brace through the tunnel. It's different than when you do it. And there's no anchor on the other side.
It's just another tunnel where you tie it. Now, Ella trash. I know this because I work with a company, Arthrex, just like he does. We're working on ways to make this better. So there's certain techniques like I've come up with the technique to try to do this with an internal brace and anchors built in. So that's pretty cool idea, but, and they're doing the same sort of thing.
So there is new stuff where they're going to have a brace more easily added, but right now this is the way you do it. And there obviously is, it's shown biomechanical benefit, but we're not seeing players get back faster. So that's obviously going to [00:12:00] be a little bit, you know, if you read the second or third article, it says.
They had the internal brace, but they ended up getting the reconstruction. So actually may not get back faster. And so that was like an ESPN one. So it's interesting. Normally these articles all get them right, but if these were not as accurate. So I think it's interesting for the viewers to hear this. So he's probably coming back mid 2026.
Uh, but we'll see.
Will Sanchez: Instead of potentially the beginning of 2026, if potentially. If you would have went the internal brace route, not the reconstruction with so.
Dr. Grant Garcia: So I think that that's the thing. It's a UCL. It's not the internal brace. So he got internal brace. You can do it with either one. The idea of the internal brace is to fix it on both sides.
So both of them, I would do an internal brace now to be honest with you.
Will Sanchez: Yeah.
Dr. Grant Garcia: But when they say internal brace, they were thinking he got the UCL repair and they didn't know. They didn't say that in the article. So that's what they were assuming he got and they were assuming it's going to get back faster.
They didn't realize the internal brace [00:13:00] because it's just the same way when we had the Achilles, right? With Rogers, everyone's like, yeah, the internal brace, it didn't make it get back faster, just protects it. Because while we want to get our players back faster, we add biologics and things like that. We don't want them to tear again, right?
That's the most important thing. And so the idea is by adding this internal brace, you're reducing the chance of them tearing again.
Will Sanchez: You know, um, one of the things, and you know, I'm going to bring up the stats here. I saw an article and it said 40 starting pitchers have thrown 100 plus pitches over 98 miles per hour since 2020.
63%, 25 out of 40 players have now had Tommy John's surgery in their career. When you hear numbers like that, and these are pretty big numbers, right? What stands out f you've worked with athlet the Mets organization, yo in hospital for special s a lot of different things that kind [00:14:00] of, you know, r you when you see numbers
Dr. Grant Garcia: be honest with you, this this level, this is an in For the viewers, Will sent this to me before this Jared Cole thing, and then all of a sudden, Jared Cole popped up and I'm like, this is a stat that the listeners need to hear.
So we've known about some of this stuff, right? There's an uptick. We know this in Tommy John surgeries, right? Because specializations happens earlier. So the ligaments are getting trashed much earlier, unfortunately. Um, and in players, they're being expected to throw harder, right? We talked about before a while ago, sowing over a hundred was considered incredible, right? It's very rare. Not anymore. I mean, there are a number of players that throw over 98 miles an hour, 40 starting pitchers since 2020.
Will Sanchez: Yeah. And
Dr. Grant Garcia: that's not counting the relievers too. So we know there's an uptick and there's an uptick in revision reconstructions, but this is a very good layman's term for us to see.
I mean, 63 [00:15:00] percent is the same. Yeah, right. That's the one good thing to hear is that I mean, in my assumption from the stat is that they're still throwing that is that 63 percent of players who had this or that means that those players who had the surgery, they got back up to the over 98 miles an hour.
Now that's not directly said here, but the assumption from that data would be there. But you can see, look at the, there are, there are 1, 2, 3, 4, 5, 6, there are six with multiple Tommy john surgeries. So those are revision surgeries.
Will Sanchez: And big names, right? Jacob deGrom, Nathan Evaldi, Dustin May, Shea McClanahan, Shohei Ohtani, right?
So that'll be interesting to see what happens with the Dodgers where they go, Hey, we need your bat in the lineup. Not sure if we actually need the pitching because we're staffed with pitchers. So it'll be interesting to see how that happens. I haven't followed along. at this juncture to see what's going to occur with their season and how it plays a part for [00:16:00] Shohei Ohtani. But for Shohei Ohtani to have two Tommy John surgeries already, that, that's, that's gotta be a warning, right? Or, or, you know, that's not in
Dr. Grant Garcia: good company. We've seen, the thing is that because there's more revisions now, we have more data. To know that there are certain again, these are very convoluted statistics when you look at the research projects.
I mean, they're very well done. I know a bunch of the guys that do the Brent Erickson, Tony Romeo. They're amazing surgeons. They've done these for they've done hundreds of these. They look at the hot stats. They look at other stats. Um, on what these are. But what we're seeing is that in revision patients, revision surgeries, uh, players do get back.
They just, it's not the same, right? There's just long term, they don't have the same data, but also it's just smaller numbers, right? You're looking at 10 starting pitchers. Like that's not enough to give you what we call a power or sample size. We know that it works. Now, again, we're not even talking about the surgery issue, right?
This is not an easy surgery to do. When you have to do a revision, Tommy John surgery, that is very rare. And it's very unusual. The person who has the most in the [00:17:00] country is probably Neil Ellitrage, right? I think he did probably almost all those players.
Will Sanchez: Yeah,
Dr. Grant Garcia: this is not easy to do because of the technical aspect.
And the main reason it's so hard to do is you probably saw that first image. You can go to that Tommy John reconstruction. When you have those two bone tunnels and you have to try to revise it, you can't do another bone tunnel. because you'll just break it. So what you need to do is like a button technique or something even more fancy, but like sometimes they blow through that tunnel and they break it.
And then you're like in a really big bind. So these are, these are not easy surgeries and they're scarred in and usually the nerves moved. So it's all going to be all over the place. I mean, the fact that these players are getting back to any level, you should be, you should be giving yourself a huge pat on the back for completing that type of surgery.
Cause that is not easy.
Will Sanchez: I can't imagine the rehab for the for the player to go through it twice and and to put yourself through it. And then you talk about it from the doctors or the surgeons perspective. We talked about this for those that are listening that didn't check us out when we talked about Nick Chubbs [00:18:00] injury, and when he sustained it, saying, whoever's going back in there to fix that knee again is it really has to start from scratch, kind of go through the mess of what's happened in the knee and then reassemble it. And that's kind of something that you're alluding to right now when you have to have a surgeon go back in to kind of fix whatever's happening in that elbow.
Dr. Grant Garcia: Well, and I would say it's even harder because, um, when you go back into a joint, like fluid in a knee, like the ACLs or PCL or whatever else, Nick Chubb tore, the scar tissue's not nearly as bad as when it's on the actual part of the body, like when you open up a part of the body.
The scar tissue is much harder and there's nerves in the way with some of Nick Chubb stuff. It was a very good surgery. Uh, James Vuze, I know him, he's a solid surgeon for the Cleveland Browns, but that, was a hard surgery, but going back into like an open surgery again, it just makes it way harder. It's a whole nother level.
And especially with the nerve being encased in scar, you're, you're [00:19:00] trying to figure out where it is and not damage it. Um, and again, preserving the ligament concern for the nerve itself during surgery. And that's exactly, uh, right. And also, I think Jared Cole probably got some nerve work, because we talked about one of the things, if you ask our players, is do they feel numbness when they're throwing?
So by throwing, they're damaging, they're injuring that nerve. That's actually what Tommy John, I think we brought this up before, but the original Tommy John surgery, they didn't move the nerve. And so as a result, he actually ended up getting a claw hand. After the UCL reconstruction. And that's because you lost his ability to use this on their nerve, which is the nerve right next to where we do the Tommy John surgeries.
So they're going to probably do something about Cole's nerve because he was having nerve issues. They said in some of the articles previously.
Will Sanchez: So do you think when they went in there, they could, could you potentially see if something was pinching that nerve? Right. Um, like I said, I've been spending way too much time on the Arthrex website and seeing how, seeing the surgery itself and they're moving things and they're, they're being very careful, careful with that [00:20:00] nerve and how that's going to move.
So when you go in there. And you already have this history of, you know, maybe complaining already by the player with the nerve, you know, you're going in there and you're going to be working around the nerve for, for, uh, the reconstruction. What is something that perhaps you're looking for before you even get into that elbow saying, I'm going to look for this because he's been complaining about that.
Well,
Dr. Grant Garcia: you're going to look for the nerve to be encased. So that's the normal one. The one you don't, the one you want to make sure you're aware is if the nerve is popping out. So people, I got a player that I did that did Tommy John on. And if you don't realize the nerves popping out when you go down into your dissection, you could actually injure it.
I didn't injure it. I knew it was there, but you could miss it because the nerve moved, right? You're so used to being a certain spot, right? Like this is not a real elbow because it's chat GPT. But you know, if it's in, it's supposed to be in a normal spot every all 500 times and it's in a different spot as a surgeon, like you don't, you only know so much, right?
You want to make sure you watch out for those things because you don't want to, it's like, it's like going down a road and all of a [00:21:00] sudden the roads has a cut. Huge drop off that never had before. Right. All of a sudden your car's in the dump. Is that
Will Sanchez: the first thing you're looking for when you, when you cut up, whether it's the knee or the elbow or anything like that, that you're going in there.
So I have to, I guess I'm curious about the steps, right?
Dr. Grant Garcia: That's the worst case scenario. It is
Will Sanchez: for that.
Dr. Grant Garcia: Well, that's like, you don't want to damage it. And again, it's pretty unusual. I examine it beforehand in the office, so I'm looking out for it because that is the one that you can nail if you, if you do an elbow scope, which some of these guys get elbow scopes, like when I used to work with all check and we did all these professional athletes,
Will Sanchez: we
Dr. Grant Garcia: would scope the elbow first and then do it.
So if you don't notice that nerve is popping in and out, which is like less than 5 percent of the population, I'll tell you, I have it so I can know that when the nerve pops out, sometimes you can feel it. And so as a result, the, if you can injure somebody, if you don't know, it's there ahead of time.
Will Sanchez: Okay.
Um, I had another question regarding, you know, you go in there, you're placing the anchors, right? You're, you're, you're setting up that [00:22:00] brace, you know, what, what are you determined, what's the determining factor for you as far as the amount of anchors you're putting in place? What stands out for you? You're going, okay, this needs another.
Yeah,
Dr. Grant Garcia: I mean, you wanna do smallest is better, right? 'cause it's you. Every time you, in my head, you're always like, am I gonna be back in here again, right? Mm-hmm . So you just don't wanna keep using Bigger is better 'cause you have bigger holes and then the next time you do it you need a bigger hole and right.
And, and these are elbows, despite gear hole, you know, being a big guy. Right. The elbow is only so big and you run out of room really quickly. So smaller anchors is better. Usually just two. Um, and that's the idea is these internal braces to use two anchors, one on each side, and that locks that thing in and fixates it.
Will Sanchez: Yeah. And then what is it? You use like that zero size anchor in my, in my deep dive in here.
Dr. Grant Garcia: Uh, I mean, you're doing a great job, but usually the anchors at zero would mean that it's not, uh, they do, the measurements are [00:23:00] usually based off of like They're 3. 5. So they're 3. 5 millimeters. They have 4. 75 millimeters, 5.
5 millimeters. Obviously, this is the Arthrex ones. Um, but they're, they're based off their certain millimeter sizes. Uh, and so as a result, you go with the three, usually three fives, they come with smaller too, but those are not used for the elbow.
Will Sanchez: Gotcha. And then you started off the show talking about collagen, right.
And, and utilizing the collagen. So just describing what that means when you're, you know, That fiber tape is dipped in that collagen to repair the native ligament. What, what's the, why, why do you need that?
Dr. Grant Garcia: Well, so the idea behind this, this is the same thing with all the internal braces. It's the, the collagen dipped in the theory is supposed to help with healing, right?
You all take, you've heard of people healing. They take the bone broth. Or they take collagen powder. Yeah, right. You know, I took collagen powder after one of my surgeries to help with healing. There's data to show that. Right? It does help your fingernails too. Uh, but nonetheless, uh, the [00:24:00] idea is that it's supposed to help with the healing process because this collagen, we have collagen, the meniscus and cartilage, their collagen.
There's different types of collagen in your body. So having the dip basically makes it more, uh, how will I say? More like your body. So the more like your body, the better it heals, the less it scars. You don't want to have a, the last thing you want to do is having a reaction, right? Your body doesn't like that.
It says this is a bad thing and tries to get rid of it. So by having this collagen, it's like, Oh wow, look, a part of my body's here. I'm going to come, come, come, come, come attached to me. Will Sanchez: I got you. I got that. That makes, that makes a whole lot of sense. Uh, describing it that way to make sure that your body doesn't reject this foreign object. Right. So you're, you're dipping it in and saying, Hey, he's one of us.
Dr. Grant Garcia: Well, it also just gives a little bit of boost, right? The key is a boost. We talked about this as biologics are, we talked about those ACL biology. Boost the gear is can we boost healing? And so this, this has been a mainstay for them for a number of years, this college and dip fibers tape.[00:25:00]
Will Sanchez: All right, I've got two more for you. Um, you know, we've talked about this in the past, right? And where that ligament is too tight and you've mentioned before that you've done some repair and realize that, hey, it's just a little too tight, a little too stiff. You kind of go back and loosen it. So you know, what is the determining factor?
Is it moving it to a certain degree, whatever that is, the knee or the elbow moving into a certain degree and seeing how that tightness is? What do you do, Dr. Garcia? What is Dr. Garcia go to? Dr. Grant Garcia: This is, this is what makes this surgery no longer a simple surgery, right? Because the idea is you have to know what you're doing with this because that ligament is unforgiving, right?
That internal brace is a solid construct. So if your tunnels are off or you put it too tight, Right. You just basically lock themselves elbow.
Will Sanchez: No, you can't pitch or what, what do you mean? What do you mean done?
Dr. Grant Garcia: You can't even get all your emotion back. You don't lock them up. Like literally like a, like a vice [00:26:00] grip.
Right. And again, it's not, I've never seen something with it. So thankfully, but again, I'm, I'm only seeing my own or occasional second opinions, but that's generally not the complaint with that. Cause people are so concerned about it, but there's so many different tricks to reduce that. But obviously the number one thing is getting all your stuff, right?
It's the same thing in the need to internal braces. You can internally brace someone too tight in the ACL. Like there's so many different ways you can, you can mess this up. Thankfully it's not commonly done because we all know there's certain steps we have to do and we double check ourselves. Like that's my number one thing I'm thinking about before I finish the case.
Um, and so the way I do it is I, I do a throwing position when I set it, which is their position where I want it to be the tightest. But I make sure that I can at least get beyond 90 degrees and it's not too tight. And then actually when you're in full extension, the brace should get loose. And so there's certain ways that I've tested it.
And then I'll check it throughout that. And then the thing is also knowing that it's going to be a tiny bit loose until you connect it to the UCL. Because you may have watched the video, but that brace has a tiny bit of bounce to it. And if [00:27:00] you don't have bounce to it, it's too tight. And you have to then, then as you repair it back to the UCL, it actually gets tighter.
It kind of sucks down. And that's how like, that's a sweet spot, but that's why we go to residency and why we go to fellowship so we can learn how to do that. So we don't do it for the first time on a patient.
Will Sanchez: Yeah,
Dr. Grant Garcia: that's without someone to monitor this.
Will Sanchez: Yeah, we don't want, we don't want that. We want you to get all your practice somewhere else.
Uh, is there any concern when you have a major league, uh, major league pitcher that maybe, do you leave it a little looser for the elasticity? Like, is there, or it's just like, nope, this is, this is the way we do it every single time.
Dr. Grant Garcia: I will tell you that's like operating on somebody you know. So, you operate on somebody you know, operate on a high level athlete, it's the same level of pressure in my opinion.
Will Sanchez: Dr. Tim Jackson
Dr. Grant Garcia: Okay. My strongest recommendation to anybody operating on them, and again, I am myself, there are these surgeons have done hundreds of these. You do exactly the same thing you do for everybody else. [00:28:00] If you're worried about something, maybe you add, you know, if you're doing like some sort of crazy ligament thing, maybe you add biologics because the person can, you know, they want to pay extra for it and they want to do this sort of fancier stuff.
But don't change the surgery because of them, that's where you're gonna have a problem. So you don't put it looser, you don't put it tighter, you do it exactly the same way. If you need to give yourself a double check because there's a level of stress involved with this, you do that. you know, I'm sure Neil L.
Trosh was cool as a cucumber doing this surgery. So I don't really think that there was a stress level for a guy like that.
Will Sanchez: All right. As we wrap it up, I want to know, you're already telling me I'm missing half of next season already with Gary Cole. So I'm not sure if I want to continue that conversation, but What's, what is the post op?
Like the first two weeks, uh, right away. Right. We we've talked about, especially, you know, the way things have moved forward, um, getting, whether it's movement or some kind of exercise, Garrett Coles gets out of surgery [00:29:00] three days later. What are you having him do at post op? You know, the first two weeks.
Dr. Grant Garcia: So, I mean, probably because of that internal brace, that's where that's where the internal brace comes in, right?
The internal brace is there. So you're probably going to start them. Maybe just. chill them out for like a week or so and then you start moving the elbow, right? Because you feel the issue is you don't want to stretch out the ligament reconstruction or the repair. So nowadays we move them a lot faster. We used to do like Casts and splints and really shut them down.
I mean, what I expect from these guys that six weeks, they're completely normal motion. And then they start working on strength and all the return stuff. So they're probably going to just let them chill out for a week or two, knowing that because if he said it right, and he has the internal brace and you're going to let them rip in terms of range of motion.
But that's big, that's been the, that's for me is the real reason the internal brace works so well. It's because it lets us move faster because we're protected, right? Like I always tell the people this for the most part, Adding the trinobrace for me helps the overall ligament itself long term, but it's [00:30:00] really small compared to the ligament, right?
It's not really like if you're using the AUCL returnal brace just for the whole repair, it really protects it so the thing doesn't stretch out. It's that first year. It's like wearing a brace on your knee. It's the same way, but it's internal. I got it. And so the idea is that you just want to protect something for the first year until it gets fully healed.
So now you have much more protections and stretch out and then you get better long term results.
Will Sanchez: So, so is he just in the sling at that point, knowing that you don't want to put him in a cast or you don't want to put him in a I mean,
Dr. Grant Garcia: he's probably in an elbow brace. That's what I would do. An elbow brace.
Will Sanchez: Right.
Dr. Grant Garcia: Yeah. So he has some sort of lock, so he can't go too crazy. And then you unlock it so he can range. So he has that sort of, he protects himself from those random forces, right? Like, let's say he had a couple extra pills of medicine or something and he got tired, he fell over, like you want to protect the elbow.
Will Sanchez: Yeah. Yeah. So, so does that get locked into like a 90 degree angle? Like what's that lock? All right.
Dr. Grant Garcia: Yeah. And then you start the ranging and then, you know, the whole standard protocol, I mean, this guy's going to get millions of tests and he's going to go to the best trainers and they're going to fly in anybody.
And he's going to get, you know, a little knob found him to check his throwing [00:31:00] motion and it's going to be insane.
Will Sanchez: Pretty bad, right? With amino acids and God knows what else. Well, you know what?
Dr. Grant Garcia: We, we don't want to go seek peak, but we have a guest coming up. That's going to go all over how this works.
Will Sanchez: Oh yeah, that'll be a, that'll be a show for there.
And then just to tie it back to the recovery shop. Is he getting a rebless? Is he getting something like that down the road? Well, how does that
Dr. Grant Garcia: probably getting some sort of fancy ice machine, the nice machine or another option he's getting biologics. I'm sure added. He's having the top of the line, everything. I don't think you need to read this for this one. He's going to have people that are probably going to hand bend his elbow.
This is the man on the Yankees. This guy's not getting the lack of treatment.
Will Sanchez: No, no, no. And if they need any help, I'll come over and move his elbow for him or something like that. I'm sure you will. I'll put your name in the list. We'll get them all taken care of. All right, man. What are the, some of your final thoughts as we wrap it up?
Um, you know, as far as, you know, the procedure that was done, you know, what really stood out for you? [00:32:00] Um, you know, and the reason that, you know, we taught, we wanted to, uh, talk about, yeah, well, this is such a,
Dr. Grant Garcia: such as like, if you talk to like a hundred people on the street, no one's had this surgery. Right.
But it's such a niche surgery. But in baseball, it's such a huge deal. It's like probably one of the biggest deals in baseball. So the only thing we talk about in baseball players when they get injured for the most part, um, cause the picture is so valuable and they're made, they're paid a lot of money.
And so it's just interesting to see at some such a niche surgery. That's so popular and everyone knows him. You say the word Tommy John surgery, like anybody on the street who watches baseball knows about this. But I think for me, the reason the show is important was we've talked about this a lot, but I think to understand the differences of what's going on and understand what you're reading these articles, right?
We we're here to help explain some of the layman terms. For the listeners, but also to explain what it means and to also change misinformation, right? If they're hearing that he gets some fancy new procedures and get back faster, if it's really true, I love to talk about it. But also understand [00:33:00] that some of the articles got it wrong and some got it right.
And it's just interesting to have this conversation because it makes it to me. If I'm if I'm not a educated. Reader, because I don't do these surgeries, which is most people aren't like, I would not understand what that is. I go, Oh my God, he's coming back in six to eight months and he had the reconstruction.
That's unheard of. But really that wasn't accurate. Like the other articles were like, no, 12 to 18 or maybe a year or more.
Will Sanchez: Yeah, I know. And that's, and that's what I was like, okay, yeah, we're starting off the season and then you start finding out that it was like, ah, okay. Uh, and, and I was excited about it because I thought it was going to be something kind of like when we talked about Lonzo ball.
We finally had this, this procedure that we don't see, uh, these high level athletes go through, you know, for many of reasons that we've gotten into in the past, you know, safety and concern and kind of stay in the course with their norm. So, uh, it was interesting to see, you know, what type of internal brace that, uh, Cole was going to have anyway.
I hope the season is going [00:34:00] to be good. Regardless, I'll be out there. I'm going to go check out the Mariners in a couple of weeks. My friend's birthday, we'll be out there checking out the A's and enjoying, uh, enjoying the baseball season. We've got soccer coming up this summer. It's going to be amazing. Uh, we should have a lot of fun.
We have some amazing guests. Check us out sports. talk. com. We're on YouTube. We're on your favorite listening podcast, Spotify, iHeart, you name it. We're everywhere. And we just want to, uh, let everyone know. We appreciate it. We hope, uh, people learn something at the same time.
Dr. Grant Garcia: Thanks guys. Appreciate it. Join us, listen to us.
We got more fun coming up. So, and thanks again.
Will Sanchez: All right. Thanks for listening.
Audio Transcript
Revolutionizing Cartilage Repair: The MACI Breakthrough with Nick Colangelo
Revolutionizing Cartilage Repair: The MACI Breakthrough with Nick Colangelo
Welcome everyone, Dr. Garcia. I'm clicking way too many buttons here.
I've got the title page. We've got music going on. Our guest is giving me a hard time about talking so he's not even on the show yet and already give me a hard time about yippity yapping.
Welcome everyone to sports. talk. I'm Will Sanchez along with Dr. Garcia, Dr. Garcia. How are you, buddy?
I'm awesome. I'm excited for this one. I also love the that our guest is giving you trouble already.
This is going to be good. I'm excited well you know what everyone knows we got our uh this is the new product we're gonna be talking about. I got my new background you never know what's going to be so it changes every show but we're really excited for this.
I think this is something that patients don't know about. I constantly get questions and it's actually not as much in the office because they commonly already know what they want. But the patients that I come on the street.
They're like, hey, your surgeon. I'm like, yeah, they're, if you really cool if we could like regrow cartilage. Don't you think that'd be really cool?
And I'm like, we actually can and they have like they're totally blown away. So from a layman terms, this is one of the most common questions that I get when they find out that I do sports surgery. So I thought it was kind of good for the the people out there to see what what's out there once's one of the sort of hottest most talked about products. um and uh learn about this and obviously we got super lucky because the CEO wanted to come on uh Nick and I'll be really excited to talk to him.
So Yeah, we're going to get into that in a in a second. um For me, when I saw the product and I saw you posting videos of LinkedIn and I was like, oh, this is this is pretty cool stuff, you know, and it's just once again, we're always talking about innovation.
We're talking about the future. We're talking about more importantly what these products do for the patient, right?
Because obviously you have, you know, your colleagues and then more importantly, it's the patience and how they benefit from this. So we're really excited about doing that.
But first, you know what we're really excited about?
We're really excited about the recovery shop. Why? Because we got a lot of love for the recovery shop because they help you, the patient just as we were discussing.
Dr. Garcia talked a little bit more about the recovery shop. So big thanks to our sponsors. I mean, it's not it's pretty much every day that I hear patients postsurgical say
how much they're happy about how happy they' about this, you know, the ability to get all these aftermarket things that they want, you know, patients coming in, especially in Seattle, I asked asking for like, I want everything, right?
I want to have the best machines. I want to have the best recovery. I want nutrition.
It's all there for the patients. It's a one-stop shop. It's really allows them to have this sort of extra stuff.
And we're going to talk about cutting that stuff today. You know, they get to offer that stuff from the rehab standpoint. Sohow, so it's been great.
Again, any doctor surgeon interest in using it for their patients, let us know and or just just talk to space with Mike because it's easier that way. So thanks again, guys. All right, man.
Let's bring on our guests, uh, Nick, Nickangelo. Welcome to the show. uh Thank you for taking some time and being here. You have an awesome step and repeat behind you.
I mean, that is professional. Dr. Garcia, I think I may need one of these cool step and repeats. We talked about hats and things like, but, I think we have had a lot of guests on here, but I think you're the most professional looking.
Well, I'm going to guess that's a good thing and it's'll take care of you. We'll get you something for you. Let's make sure.
You know, first off, I'm sorry. I'm taking it over again. I apologize here.
You're from Pennsylvania, right? Is that where you were originally from? Are originally from Pennsylvania or Indiana?
Tell us a little bit about your background because uh, you know, I know you're on the east coast, so we want to share some of that before we get into everything else that you do here. Yeah, so it's upstate New York, uh so that's uh where I am from and you know, actually just by way of background. So lawyer by training, um and I actually started my career in industry about 30 years ago when I joined Eli Lilly and you know, I was really fortunate to, you know, start there as a tax lawyer, but, you know, after a few years to actually be moved over to the business side, which doesn't happen very often, and, you know, ultimately became kind of the director of strategy and business development for Lily's diabetes and obesity product group.
And, you know, it was a great foundational experience for me because the product group president of the the time was more of a commercial guy and he said, if you're coming over here to work for me, you're going out in the field to learn our customers. And so I was a sales rep for a little while, um selling, you know, Prozac and Lily's uh insulin products, which was great. And then, you know, really just kind of being in the middle of the whole product development commercialization and so on of a of a pretty important product group for Lily was just a great experience.
And ultimately ran Lily's venture funds for a while. So, you know, over the course of my career kind of just had a lot of business development experience, acquiring developing and commercializing products and and enjoyed what was the predecessor company aerrisal about 12 years ago. So it's been quite a bit of time, but it's been a great, great experience as I'm sure we'll talk about.
So I think for the viewers too, to know, obviously, Verrisel is the major company, right? And then we hear this word Macy, right? So can you explain the difference in the two?
Because everyone hears me, you say the word Mac. They look at you, they see CEO of Veracel and they see Verasso in the background, so it'd be good for us to kind of understand that better. Yeah, so Vercel corporation is the company that commercializes, developed and commercializes Macy.
So, you know, we acquired Macy uh back in 2004. So the company that I joined um was actually called astron bioscices and it was a company that was in the cell therapy space conducting clinical trials for the treatment of severe, uh cardiovascular diseases, basically using a bone marrow derived multicellular therapy, uh, which was really attractive at the time. um and, you know, cellingene therapies weren't quite as prominent as they are now, but, you know, really reped sort of the next frontier of innovation uh in the industry. And so I was really excited to join a company that was kind of on the leading edge of of these emerging technologies.
So that's what brought me to the company. um, you know, at the time, Sonnofi, which is one of the largest pharmaceutical companies in the world, bought genzyme. and after they bought the company, they decided to divest what was essentially the genzyme biosurgery business. So there were a Pharma company. They weren't really a med Tech company, so they decided to divest what was called the cell therapy and regenerative medicine business.
And that's how we acquired this portfolio. So initially, it was the first generation cartilage repair product called cardicel. epicel, which is a skin graft product that uses a patient's own cells for severe burn treatment, essentially a a skin graft product. And then Macy was approved in Europe, but not in the US.
And so part of our, you know, development of that product was that we ended up submitting the BLA to the FDA and the US and getting approval for Macy in December of 2016. you know, so essentially that was a kind of a strategic um transaction for us that essentially took us from a development stage company to a commercialization company. And then we changed the name of the company to Verousel. We moved our headquarters to Boston, where our manufacturing is now.
And so it really was quite a transformative time for us. And as you alluded to, Dr. Grant, you know, now we're we're seeing as kind of a leading provider of advanced cell therapies for the sports medicine and severe bird care markets and we have highly differentiated portfolio of innovative advanced cell therapies and specialty biologics that essentially repair tissues and restore function. And we're really focused on changing the standard of care for patients with knee cartilage injuries.
Yeah. So I was thinking I think you did a good job of leading to this. I only reason I know is to hear this this little story from your rep.
So basically I heard a very positive story how you basically this was a herding product in 2014. And I know that some of the reps are going to kill me for telling you this, but it was a herding product in 2014 or not doing as well and you basically found a way to acquire this and now you have this situation where you you have a sort of, I would call the golden ticket of cartilage where it's under this biological option. It's been FDA approved.
And for those listeners, and I want to make sure Nick can respond to this, this is not easy to do, right? There are lots of car inserties that I'm telling you about that one insurance companies won't cover and two they're not FDA approved yet. So there's some sexy stuff in Europe that we hear about all the time, but you can't use it in the US.
Or there's some sexy stuff we've talked about on the show and you can't use it that frequently because it's hard to get insurance to cover it. This is a insurance covered FDA product. So it's a big deal.
And now it's a, you know, one of the most popular carage products and one of probably the most studied cartilage projects. So, I mean, I think that's if you want to kind of comment on the fact how you basically, how did you know this was going to be like this? Or and you don't have to go into a big detail, but kind of that story is kind of incredible.
Yeah, I mean, we, yeah, it really was because, you know, we were kind of really focused on, you know, focusing the predecessor company on which programs, we should be, you know, obviously kind of bringing forward in the clinic. But again, you know, it was a pretty nas industry at the time and you really want to diversify uh your your risk in a higher risk uh development, you know, situation. And so we were very, very fortunate to sort of, I mean, Sidi was running a process like, you know, many large companies do where they contact a lot of companies and, you know, we were probably one of what were a few natural buyers of the business.
We knew the cell therapy space. There weren't that many companies working there, developed a great relationship with our business development partners in Paris at Son.
It's a French-based company, um and kind of entered the process late, but sort of ended up winning the deal.
And to your point, yeah, at the time, you know, the whole business was doing maybe $40 million in revenue. It was kind of flat to declining. um and we were able not only to kind of get the commercial business sort of growing again at sort of industry or above rates, uh, but we also were able to get Macy approved in the US with a pretty creative regulatory strategy where we took one pivotal study from Europe, the extension study that I'll talk about later, the carticel data that existed in the US. and we actually didn't have to run any additional studies. And so we were able to get to the market very quickly with the, you know, the pivotal data from the phase three study in Europe kind of leafrogged the competition first to market.
And, you know, obviously that's allowed us to kind of achieve the growth that we've been able to achieve to date. So it's been a, you know, like everything itself a lot of hard work by a lot of really talented people, but, you know, it's very rewarding when you're able to take what was essentially, I'll call it a neglected business, right? Because genzyme had bigger products that they focused investment on.
And you see it a lot in the industry where companies, even my predecessor, you know, the company Lily, that I worked at when we would divest products, sometimes they get into other companies' hands and they grow into being multiillion dollar companies like varioscels become. And it's really because you've got a, you know, focused management team that's really kind of nurturing the product, um which again, may just not have been as high a priority in a bigger company at the time. Yeah Well, put up that slide the first one.
So I think I think you I think it'd be good for you to touch on on. We kind of can, you know, I can also charm into because obviously I know this product pretty well. But I think for the viewers, I don't understand sort of what the which we treat this articular cartage damage you see here with the Macy, that's how it's delivered for all those listeners, but really sort of what is what's unique about the Macy compared to other products out there?
I mean, I've had my podcasts, I've had every possible cartilage thing I've talked about. So what's the uniqueness of this Macy procedure? What what do what do you feel is the uniqueness of it?
Yeah, so Macy is the leading product for the company, so, you know, this we just, you know, released our kind of preliminary financial results for 2024. And, you know, Macy will be close to a $200 million product in 2024 growing at, you know, around 20%. So as you mentioned, it really has become the leading restorative cartilage repair product on the market. um It's basically an advanced cell therapy that, you know, will show you more about that uses a patient's own cells to repair, you know, the damaged cartilage tissue and restore function.
Emis is unique in that. It's the first and only FDA approved product that applies tissue engineering processes to grow a patient's own cells on a scaffold, um basically, you know, using a healthy cartilage tissue to do that. And, you know, cartilage injuries, while everybody sort of hears more often probably about ACL terrors and meniscal injuries.
I mean, cartilage injuries are a significant issue. You can expound upon where, you know, basically cartilage is unique in that, unlike most other tissues in your body, which, you know, have intrinsic healing properties, that's not the case with cartilage, because there's no blood vessels to bring repair cells. There's no emphatics to get rid of cellular and tissue debris and no nerveves.
So, you know, cartilage, a focal cartilage injury, like weat tree is like a pothole on the surface of the knee. And if it's like untreated, uh, you know, it leads obviously to joint pain and dysfunction, but ultimately to ostearththritis and partial and full knee replacement. So, you know, that's the progression that we're focused on halting.
Yeah, that's perfect. And I think it's good for this slide. I'll show the listeners, but basically there's three types of cartilage stuff.
So we have the ones you clean up, which is what a lot of people used to do has been around for a long time. And you have the microacture and the drilling that's a little bit more old schooled, but it's not really it's just sort of trying to repair and try to fill it with something good. And then these are sort of the main products and obviously ACI, so the viewers don't the to not get confused.
ACI and Macy ACI is just the older version of Macy, right? And so the and now we have this better matrix. So obviously before we had to use the periostrial layer, which was as as you can put it, it was more challenging, right?
So now it's a lot easier to do these these procedures. I think this is kind of a good slide for to bring up. So you know, you guys went from sort of this arthronomy carticel, then you join the company, the company takes off 2016 big jump, right?
Like it just was a lot different. And so you guys described that in the process briefly sort of you went from now like when where did you how did you go from the this this really tedious So well, this used to take like three times longer. And then they figured out a way to make it so it did.
So how did you guys do that? You know, what was your thought process in going from that to this sort of 2016, 2018 product that's now, you know, much easier to use and much more reliable? Yeah, so, you know, in the US, so when we bought the business, Macy was already approved in Europe.
That's where the technology was developed by Dr. Peterson in Sweden. It was approved in Europe, uh, but cardicel was the product that, you know, was shown on the lefthand side of that slide. That was the product that was approved in the US when we bought the product.
And as you mentioned, it was a first generation ACI, so that's autologyus condorsite implantation, so taking a patient's own cells and implanting them in the defect. First generation ACCI product that was really a first commercialized in the US in the in the 1990s. And, you know, the as we'll talk about with the Macy procedure, what ends up happening is you can explain it, you know, add any color that you'd like, but, you know, when you suspect there's a cartilage injury, you know, often you'll go in and do what you' referred to as sort of the palliative techniques that do a contro plasty, a diagnostic arthroscopic procedure just to see what's going on in the knee.
And at that point, that's where you take a biopsy of healthy cartilage for at the time cardicel and not now Macy. So out of a non a tic-tac size biopsy out of a non- weightbearing portion of the knee that is sent to our manufacturing facility in Boston, where we process the biopsy, we isolate theondracytes, which are the cells that make cartilage, and we expand those cells, and then we cry or preserve them. So we freeze them down.
We wait till surgeons like you are and the patient are ready to move forward with the surgery. Once that happens and you pick a surgery date, we kind of work backwards. We thaw the cells, we further expand them.
We seed them onto that college of membrane that's shown in the second image from the left. At a density of about half a million to a million cells per square centimeter package it up, send it to the surgical site where the surgeon obviously kind of prepares the defect and essentially cuts the Macy membrane to the size of the defect, lues it in with fibberglue and is done. So in the case of cardicel, which was the predecessor product, the front end of that process was essentially the same.
Take a biopsy, expand the cells, but as it shown in that vial, the final finished product was a liquid cell suspension. Now, you can imagine that you alluded to this how hard it is to fill a pothole on the knee with a liquid suspension, right? We we like torture.
Yeah, you know, we we liken it to kind of spackling, you know, a wall, you know, with water, right? I mean, it it's it's very hard to do. And so what that required was opening up the whole knee, as you alluded to, you taking a periostial harvest off of the shin bone, microsutureuring that into place, injecting the cell.
So it was highly invasive, technically demanding, very time consuming. And so it became kind of a niche product at the kind of high-end cartilage repair specialists. And that's because, again, it's really the the way one of the only ways that you can truly repair the tissue because you're using a patient's own cells to regrow that cartilage.
Around the year 2000, in a company called Veren and Europe developed Macy, which was a next generation cartilage repair product, where those cells were seated onto the membrane, as I just described, and then genzyme acquired Vogin in 2004. We acquired the business from genzyme. And that's how Macy sort of made it into our hands.
And and as I mentioned, you know, it wasn't approved in the U. at the time. We ended up submitting the BLA in 2015, the FDA approved it late in 2016, and we launched the product in 2017. So the real sort of, as I mentioned, you know, this was kind of a niche product, you know, used because there's actually 20 year outcome data with cartil with carticel now.
So once you regrow this cartilage, correct me if I'm wrong, but it can really last a lifetime unless you have another injury, right? So that's why surgeons would take the time to do that. You know, the beauty of Macy and you see this often in the med Tech industry that when you take a highly invasive surgery, open heart surgery, and you and and you kind of progress to minimally invasive cardiac extents, you see that there's this broad adoption as the standard of care changes.
And that's really what's going on with Macy right now. So because you can't you have this product now that has the cells already on the membrane, as I mentioned, as you can see in the third image from the left, we actually developed custom cutters that actually would make an open Macy procedure. So it went from highly invasive to a miniarththotomy, um kind of trying to make it even simpler and less time consum consuming for surgents in an open procedure by developing these custom cutters that would allow you to score the cartilage and then stamp out the membrane exact size that you could then glue in.
And really, that was a big technological advancement that made it a less invasive, faster, simpler, uh surgery for the surgeons. And that's why our surgeon base has grown so dramatically since we launched the product., I want to stop for a second. So so first off, that's great.
So I think for the listeners to hear what he's saying, you know, they basically took a very challenging situation. They may keep making it simpler. I know people always think simpler is, you know, never good.
We want complicated. But in this stage, we want it simpler, right? The the last time under anesthesia, the simple cutters, you want more adoption, and then the more adoption means more people to see it.
So the idea that behind this is pretty cool. And I think will, you, I don't know if you have any questions about this, but he basically just said to the the listeners that we're going to take your cartilage, we're going to send it to Boston. We're going to it, we're going to freeze it.
This sounds like a movie, right? And then we're going to send it back to you in a box and then it's going to be sterile and then you're going to glue it on your knee. And when I tell it to patients, they don't like they were like what can actually work?
I don't know if you have anything else will you want to chime in being I mean, you a dinner you play doctor on TV, but well just the fact that it's a, you know, regenerating cartil, right? And and utilizing this component and I can imagine, right? We talk about sports uh, you know, on the show, the the athlete now, uh is recovering faster long-term effects, uh the flexibility, right?
When you think about what you're utilizing as this component. So I know if if, especially if I'm an athlete but just anyone else, that I can have mobility, quality of life, you know, um in movement utilizing this, that that's all you want, especially after you've suffered a injury to kind of go back to, you know, this, this uh normality. And I think what you guys are hearing from Nick two is you have this product, right?
Like so the product has been around for a long time. And then every time they make a tweak to it, right? Like you don't want to make big tweaks with the FDA and everything else.
But, you know, they found like, we have this really great product that works. How do we make it work better? So how do we make it work better open, which is with a bigger incision?
That's what those cutters. And now, which we'll talk about, and I don't want to get away too much behind me, but the arthcopic approach to do this, which again, the goal here is extremely high technology, very small incisions. And we can get to that.
That's like sort of the perfect, the perfect formula, which we finally got to. Nick very briefly, can you kind of talk on touch on the slide and explain the dual membrane idea so people can understand and we'll show how it regrows in a minute. Yeah, so, you know, as I was describing earlier, once we expanded the patient cells, they're seated onto this college of membrane and there's a dense side that is on the top and then a kind of less dense side on the bottom. um the way we seed those cells is you kind of flip it over and, you know, contrytes are spindle cells, so they attach themselves to those collagen fibers. and then when it's implanted, it's the dense side up, the sort of cell side down.
And once the the um implant or the membrane is implanted at the bottom, as you show here, those spindle cells kind of migrate down to the subcondral bone. They start producing extra cellular matrix, which is essentially the cartilage, and it fills that defect from the bottom up and allows patients, as well alluded to, to kind of resume their normal activities, right? So our core patients in it'd be interesting in your take on this Dr. nursey, are really those sort of younger active patients.
So, you know, think about a bell curve from sort of late teens into early 50s, thinking the the summit pivotal study, um average age was about 35 same thing in the publication of the first thousand patients we treated in the US. So it really is that patient population that is suffering from significant knee pain that wants to fix the cartilage injury and get back to their sort of normal activities. Well, and I think what's interesting is we' con see that, you guys, I'm not sure the viewers saw that how it grows back.
That's literally how it works. And if you scope patients at three months, six months, nine months for other reasons, or they want to have, you know, there's some issue they're getting stiff or something because again, we all do these surgeries. You want 100%, but the word hundred percent never exists.
But if you go in there and you take a look, you can actually see that at certain stages, there's ways this thing looks. And when it gets up to the full stage, and I know because I do a lot of these, you can't get that cartilage off. Like Nick keeps saying like when you have a solid regrowth, will it like literally like even a night, you cannot take it off.
Like the first time I saw it, you it's very hard because you have to if you a surgeon had never seen one of these before, it's very hard to process because we're not used to products that do this. But when you see it, you can literally put your finger on it and it feels just like the rest of the knee. So the ability to regrow when you've been around for a long time and known that this doesn't really happen that often that we get really good regrow the cartilage, it's just mind boggling.
I remember the first time I saw it when I was like I called my rap and I was like, this actually works. Like it legitimately regrew. It looks just like the other stuff.
And if you were you know, you core out things or do things around that area, if there's if there's a part of it that you don't doesn't fully regrow and you have to redo something, you can't get rid of that other stuff. It's like stuck on. It's just like the solid good stuff.
So well, I don't know if that's any have you any questions about that because that is that's interesting. So obviously, um, you know, with something like this, we're talking about maybe severe cartilage damage. But have you seen anything come across your operating table where it's minimal, but based on the athlete or the patient, you're kind of going in and using this technique to make sure that whatever you're working on is extra sturdy because of of this product.
Well, Nick can probably jump on this too, but I basically, you know, we don't do this as preventative, but we do prevent other things, right? Nick, I mean, the idea is that you put this cartilage hole on one side to prevent damage the other side. Imagine this well, you got to tire and you got a road, right?
The road has a pothole in it. You'll damage the tire or the tire has a nail in it. You don't want to damage the road.
So if you fix one side, you avoid damage to the other side. So that's that's the preventative nature of this. It's it's still an invasive surgery and you know, we talk about 10 months to a year recovery, you got insurance authorization, everything else.
You don't want to go through this willy nilly, but but these patients are as nic will tell you, this is these patients with the carage damage are much more severely impacted than the ACL terms. Agreed. Yep.
Yeah. So, um the uh, I think one thing can chim in is, you know, you guys have done if there's a there's a couple of studies we've seen where it shows all the cartilage surgery and it shows the number of research projects research studies. Macy will has the most research on it of any of the current cartilage products on the market, which is pretty crazy.
So when people ask, like, is this been around? Do you trust the results? You know, if you don't trust the results of this one, you shouldn't trust any of them, because, you know, there are some strong results.
But I mean, I don't know if you can I mean, it's amazing that you guys just continue to I mean, Nick, you have so many projects out there and so much research out there. Why keep doing it? You know, you have so much data already.
So explain what's the desire for Macy to always keep doing it keep getting better, right? Like you ready you've already won the game. So why do you keep doing it?
Well, you know, I do think, you know, one of the advantages, well, several advantages to Macy that we talk about all the time. First of all, Macy has a very broad label that basically covered the indication for Macy covers, you know, single or multiple defects anywhere in the knee, you know, regardless of whether there's bony involvement or not. So it's applicable for a large number of patients and really has unsurpassed clinical data.
So Macy is the only FDA approved product that demonstrated superiority versus micro fracture, which Dr. Garcia mentioned, which is what the FDA requires as a compar in these phase three pivotal studies. So the summit study, which is the basiivotal study, basically demonstrated statistically significantly greater improvements in pain and function versus micro fracture at two years. That's the common end.
And then there was actually an expansion phase of the study that went out three additional years to five years, and the FDA was very interested in making sure we included that data in the label as well, which showed that the improvements that we're seen at two years carried all the way out to five years. So that's a pretty significant sort of longitudinal data that's in our label to begin with. But because Macy was approved in Europe and Australia since kind of the early 2000 thousands, what you're seeing now is even last year in the American journalist sports medicine, there was a publication of a prospective ten year outcome study, which showed, you know, positive improvements for Macy out to ten years.
And even one other publication, up to 15 years, and as I mentioned, Cardicel has data out to 20 years. And so, you know, it is really important, uh, especially when you have kind of an innovative premium priced kind of product that, as you mentioned, is covered by all the major insurance plans in the country, that you can continue to demonstrate that this is really kind of a restorative procedure that can last as it mentioned. And Nick, I want to I don't want to interrupt you, but I want to bring that point up you just said.
So you just said an expensive product, because that is a common misconception for patients. Right? And and I I'm I'm this in really important because I want the the viewers to hear this because I bring this up on every single talk and no one listens to me because somebody's doctor like this is an expensive product.
This is a pharmaceutical product, so it's very cool because it's you guys got a pharmaceutical allocation. It means you have a lot more rigors you have to go through, correct, right, for the biological stuff? But this is a pharmaceutical.
So this product is paid for by the insurance company. It's not paid for by the patient. It's not paid for by, you know, the hospital.
It's paid for by the insurance company, which we all know in the news that's that is not that that's the one we're okay with them paying for it because they're doing pretty well. But the important thing, I think is for people to understand that while all this product is expensive for the insurance company, for the patients, it's the same as anything else. And that's and now you get the superior product.
So it's really important for people to hear that, I think, because they hear, oh, you know, this is sounds so fancy. It sounds like the Mercedes-Benz or the BMW of products.
Maybe I can't afford it. has nothing to do with that.
This is an insurance provided coverage. Yeah, and you know, the interesting part of that, so as you alluded to, you know, unlike most devices in the Med Tech industry, um, you know, Macy is actually very different. So Macy is actually regulated by the FDA as a combination product.
So there's different combinations, you know, there can be a drug device like the drug eluding stents, et cetera. In this case, you know, Macy's again regulated as a biologic device product with the college and membrane as the device component, and then, of course, the patient's own cells is the biologic component. And that has a lot of important implications, you know, in terms of the regulatory pathway that we had to pursue to get the product approved and on the market in the U. intellectual property protection and and as you alluded to, how the product is reimbursed compared to a typical product device.
So, you know, because Macy's bi a biologic, it had, you know, for example, additional 12-ear data protection, uh, which are, is afforded to all uh biologic products in addition to the patent life, it's actually reimbursed under a J code. So it's not part of a CPT code professional fee for the surgeon or facility fee. There's actually a J code that's listed in
the compendia like other biologic and pharmaceutical products um that is uh reimbursed by the patient's insurance plan, as you mentioned.
And I think, you know, an important part of that. First of all, you know, well overin0% of the submissions for approval get approved, right? And a lot of that has to do with basically differs a little bit from a normal biologic or drug product, which are dispensed in a pharmacy, right?
So every insurance plan has a pharmacy benefit that we're all familiar with and a medical benefit, which is what Macy's comfort under. So a pharmacy benefit, you know, basically the the manufacturers kind of discount to get a formulary position and then once it's sort of on a formulary, you know, your your physician can write a script. Nobody really says, Dr. Garcia, do you really have hypertension?
It's just sort of managed by where they kind of discounted on a formulary tier. In the case of a product like Mac that's reimbursed under a medical benefit. Again, every major plan in the country covers it.
And they basically have to approve it in advance of the surgery. So there will be in, you know, pick a Blue Cross Blue Shield plan. It'll say a patient's, you know, eligible for me
see if they are this age with a grade three or four focalchondral defect, their ability, you know, they have an ability to do the rehab, et cetera.
The point being that the insurance plans know that every time Macy's being used, it's on an appropriate patient. So they know the price, they know the clinical benefit. They know, you know, the patients are going to benefit from that.
And that's why you get the prior approval. So I think one of the things that the company has done over the last decade is really sort of unlock a lot of value because we try to carry a lot of that load for the surgeons in terms of the benefit coordination between a patient surgeon, the insurance plan to make sure that the submission is done in a timely fashion doesn't sort of slow things down for when the patient and surgeon want to, you know, have the surgery and we invest a lot in that to make sure that, again, it makes it as streamlined as it possibly can be. But but that, you know, that is an important point that you brought up that, you know, when an insurance company is able to know that they approve every patient before the products used, and they know the benefit, that sort of, you know, erases the whole sort of, you know, kind of, I won't call it a phantom objection, but, you know, discussions around the price.
We've seen it right nick on the Internet. You see all these papers where someone posted like look at my rejection for my surgery that I need. Look at the rejection for my surgery that I need.
You don't get it with this. And I think will, we should for the listeners, you we just keep this, right? This is a innovative product.
And I told you that, you know, this is obviously, it's a pharmaceutical. It's expensive for the insurance company. But if listen, the insurance company would never approve it if it didn't work so well.
That's the point we're trying to make. You have a company that you hear about all these insurance companies and how they're very stringent about costs, right? So if this is this has to be a product that has such a good quality of life improvement that they're willing to pay for it.
And so that shows you the value of this because you've already this it's approved with pretty much any insurance. Like people come in and like, oh, sure my insurance are covered. I'm like, I'm pretty sure that it'll insurance.
It's very rare that it's difficult to get approved. So, well, that's interesting, right? Like you have something it's like basically like you have a you have insurance companies that we hear all these things online.
We're not going to have a whole talk about that right now. But the, you know, you hear all this stuff online about these insurance companies and and you know that they're very stringent about costs and now you have a product that they're willing to do reimbursement for despite the cost because of the quality of life. Because quality of life is a really big deal, right You get your ACL and you don't get it fixed.
Sometimes you can get away with it and you can run around with it and you can do things when you have a cartilageole will, it really, really hurts. It's it's it's up there to like nearththritis because actually it's pre-arththritis. And so that's something that's really important for the listeners to hear.
They think Carlishold, that's not a big deal, but they hurt way more than anything else. These are my most satisfied patients, my cartil patients. And I would say there are publications out there that show, even though Macy is, you know, may cost more up front over the life of the patient or long term, it actually is equal or less than some other options that could have been done by the time you add in what will ultimately have to be done and just to kind of reinforce that innovation point. when you think about the cost of Macy, um, you know, compared to gene therapies that can be in the million to $2 million dollar range or or cartis cell therapies, which are half a million corpation.
I mean, yeah, that's the kind of innovative manufacturing and other development, you know, processes that you have to go through. But again, it's nowhere near that kind of of price point. And it's important what you said one second before what you said is like that the there this, when you do lesser surgeries will in these cartage stuff, people fail and like they come back and we're talking about my average cartilage surgery patient or sometimes I get to them, six surgeries, five surgeries.
Woms if I could do it in one surgery and avoided five more. And so you imagine that what he's saying is like, maybe each individual surgery is less expensive than the Macy, but it's going to prevent long term. And I I've seen what you're talking about.
So sorry, Will. I just want to bring that point up. No, it's fine.
It's right line cut of what you guys are talking about. I just wanted to ask Nick if he's gotten feedback from a patient, a doctor, um something that really resonated with you saying, man, your your product either save me money or save me from going back and having multiple surgeries changed my life. What's the story that you went home and you, you know, you told your significant others and say, man, this that this was a good, this is why this is why we do it.
What what what's that what's the one that sticks with you? Well, you know, we have all sorts of basy patient videos of kind of what it means to a young mother who couldn't
walk up and down the stairs with her with her baby and how it changed her life to be able to do those things. And, you know, that is exactly why we're doing this.
And and it's interesting. This is a good time of year. You know, we typically and we'll do it again this year.
We'll be at the Super Bowl for Radio Row and we go on a lot of the sports medicine or the sports, uh channels and you know, one of the folks who would do it with me in the early days was Dere Torris, who was an Olympic athlete. She actually had carel in her in her left knee and she was one of the first Macy patients in her right knee. and she was actually able to go back and compete in the Olympics after she had her first, you know, surgery done with Cardicel. So, you know, those are the kind of life-changing outcomes that, you know, you're she was one who said, you know, would talk to me about how hard it was for her to even walk up the stairs, let alone sort of train for the Olympics, right?
Um And so that's kind of a, you know, you could probably say that about almost every patient we treat. They couldn't do the normal things that all of us do or whatever athletic activities and and, you know, Macy allows them to do that, which is obviously extremely rewarding.. Yeah.
Yeah, well, I think that what he touched on is perfect. I think I don't want to pivot, but obviously we still have a little bit of time with him so I promised him that we would pay under an hour. He didn't know if we could make it to an hour.
I think we're going to go over so that's what we're going to end up he down. But the well check off that cybercycle. I want to bring up this point.
I want to ask him. So I think we've talked a lot about, you know, you did some awesome job talking about the business behind Mac, which I think is super unique. I don't ever get to hear that perspective.
We don't ever hear that because we're mostly focused on the medical side of things. But for the listeners, we like to start from the ground up, you know, like with nap into reality, well, which is one of our first shows. Like how do you take something small and make it something big?
And we have the man here that did it, which is awesome. But so but Nick, there's obviously the postpart, which is or the stuff is like you have this awesome product, right? You keep making modifications to it.
You keep making it better. But there's something unique about you guys that I wanted you to talk about. So when it comes to like informing people, you have different ways of doing it, right?
You guys have, and you have Karla and other people in your office that do amazing job. But you know, you do local labs so that people locally can find out. You have people like me that fly around the country to talk about your product.
You have different directors that talk about your product, but you guys do so many things. And and there's some will you've seen me do this. You know, the headset thing I did on Friday.
That was Macy. So like they're so into like every possible way that can show people how to do this surgery and they're dedicated, right? Like I just got on a phone call this morning and I was talking with the entire team on why I did the certain steps and they're just so into like how do we get better?
But it's where does that come from? Because I worked a lot of companies, some do some things, but they don't go to the extent that you guys do, which is like, I want to find every possible way to teach someone about this and it doesn't mean sell it. Don't sell the product card.
Just tell us how you do it and how we can make it better. Yeah, you know, I think it comes back to, you know, we have a unique sort of place in the industry and it's certainly the case with Macy, where we get a patient cells. We know every patient that we're treating, right?
We're not stamping out a million, again, hypertension pills and they're going to whoever they go to. I mean, it's a very patient centric and customer focused group. And that's true for Macy.
It's really true for the catastrophic burn patients that we treat, you know, with epicel uh and exibt, our our other products. So that kind of culture of we're focused on the patients. We want to make sure surgeons really understand how to identify appropriate patients, make sure that we have good clinical outcomes.
That just kind of is built into the DNA of our company. And you're right. We we invest very heavily in surgeon, peerto- peer educational programs, including these boskills labs on, you know, with cadavernes and things like that.
And in fact, you know, it's really the largest discretionary commercial budget item that we spend money on, right? Because, you know, when we do these these programs and we fly surgeons in from around the country to train over the weekends, et cetera. I mean, it is a big investment, but, you know, again, it's all geared tours.
We want to make sure. First of all, we're so fortunate that we have surgeons like you and dozens of these passionate, dedicated surgeons that we partner with to make sure we're bringing quality educational programs to surgeons who are interested in sort of adding Macy to their practices and treatment algorithms. And, you know, the it's it's definitely the most important thing we do again, to make sure we optimize patient selections outcomes and so on.
So, you know, it's really just that. It's just sort of built into sort of how we operate and and what we do. we we because you know, we have an advisory board, we have speaker bureaus that we partner closely with. We want to know from the surgeons, sort of how can we best teach other surgeons, right?
So whether it's educational content or new technologies that we can leverage to make sure it's easier easier to consume by the surgeon customers? I mean, we're just always interested in that feedback. And I think, you know, as we were developing the Macy Arthro instruments, that was an iterative process where we would develop prototypes.
We'd have surgeons come in and work with them, make tweaks, develop, you know, come back with another one. You go through that four or five times and and again, it's just about getting that input to make sure we're kind of delivering the right innovation and technology for the surgeons in addition to the educational component. All right.
So I I know, I see the timer clicking down and I need to get to this last topic because no one has any idea what the thing is behind me and we've been here for 46 minutes and 53 seconds. So let's go to the next dick I appreciate everything you said this is awesome. So well, I'll say you keep hearing all this stuff.
We got the sexy carage surgery. We can grow it in the lab. We can glue it on your knee.
But until a year ago, other than some kind of offshoot random stuff that you people were doing, there was no way to do it through an incision this small. All right? It's always been incision this small, long in my hand, big incisions open.
I said, every time I told the patients, I was like, I'm just give me an open incision. The first step is a scope, that's easy, second step's open. You'll get through it not a big deal, but it's open.
It's big. And there was a lot of work that I went into this and it took, I was involved in this FDA trial and it's different than other companies, right? You can't just start to tweak the product a little bit and get it because it's a biologic, and we don't have to go too much into it so we can show the product.
We don't know if you can pull it up. there you have to do a lot more thing we had to do the FDA trial to show that it was not damaging the cells. And normally you wouldn't have to do that, but only because your product because it was so stringent because of the FDA that you had to basically show this product would be just just as good as the open one, even though it like all this kind of knew that. But you had to do it for the FDA and that you had to do some so many extra hoops that the average company doesn't have to do.
Is that correct? Yeah, that is, you know, when you develop kind of an instrument set like this for the arthroscopic delivery, you know, there's multiple workst streams, right? This took us two or three years to kind of develop.
There's the instrument development itself. And, you know, obviously that involves, as I mentioned, sort of the design phase of it where you develop, you know, you work with a vendor, we have a local vendor that you know, they did our custom cutters for or they'd done other work for us. the instrument kits for open, et cetera. um you know, we work with them. We develop prototypes.
We have surgeons come in, we refine it. You get a year, you know, that probably took almost a year till you finally even get to design phase. Then once the instruments are done, you go through a whole sort of set of validation, testing, et cetera, to make sure that they meet FDA requirements to make the the instruments commercially available.
Now, at the end of the day, as you alluded to, I mean, these are class one devices that we actually registered before Mac Arthur was approved. but that was just the device component. The trick here was that, you know, because Macy's approved under a biologics license application to be able to add the Arthuroscopic administration to the product label, we actually had to do what you were referring to, which is a human factor study that says, if we give surgeon this surgeon's this set of instructions, can they reproducibly um basically administer the implant uh using these arthroscopic instruments? And so to get it on the labels so that we could promote the instruments and then teach surgeons how to use them appropriately, we had to go through that was essentially a 10-month FDA uh review process, which, you know, we obviously were able to do successfully, which was was just great.
I think Will Ens to hear this. I can say it now the trial has been approved, but Will, you get a phone call. You got to fly out to Boston and then they don't tell you how to use it and they want to see how you do it without that in a black box.
And then you're on a video camera and then they say here's four different ways to do it. Let's see if you can do this without any instruction. And if you can do it without any instruction, then we know it's safe.
And that's what they did for what, 16 or something? They're more than any more than that surgeons. But basically, that was the game.
It was like almost a game, but it wasn't really a game because if you don't do it right, then you're either you're out or the FDA trial It's your own version of squid games. I got it. But you know, you know me you know me long enough that we love the game.
It was a fun game, but you're under scrutiny for it, but you can see guys, I mean, think people this like they foundarches they thought would do a reasonable job. They flew them all out there to do this just to show that this product was saved to put in the scope. So when people ask me, what you about thinking of this new thing?
I'm like, this has been tested more than anything I know, right? You guys have gone through so many hoops, but now you have this product that basically we've done five of them now and the first one in the Pacific Northwest, and we have this product where we can now insert this this product that's 20 years tested through a scope through an incision this small. I mean, what is your what is your feedback then so far?
I mean, I don't I could go on and on about this part. We've seen way too many of my posts, but Nick, I want to hear from you. What is your feedback then on the company in the first six months of this new product?
Because it's been out since it got approved at the end of August. Is that correct?, yeah, kind of launched sort of at the end of the third quarter. And you know, the physician feedback, surgeon feedback has been correct.
You know, I think in the market research we did before launch, you know, whether surgeons were Macy users at the time or not, you know, there was a high interest level. You know, surgeon said I would expect to do more procedures or even if I wasn't a user, I'd shift some of my procedures if a MacR throw, uh option was available. And, you know, so we have seen that out of all of our surgeon segments.
So we have, you know, folks like you who are, you know, strong users of the product now doing Macy Arthur cases. We had sort of our original set of surgeons that maybe hadn't adopted it yet. They're starting to use it.
And then we had another set of new surgeons that really just do arthroscopics, you know, procedures and that had never even used Macy. And and we've seen sort of cases scheduled or completed out of all of those segments. So that's great from a surgeon perspective.
And then from kind of a patient perspective, as you know, Macy open was is kind of a go-to product if you have a deep defect on the back of the kneecap or the Patella, if you have a larger defect four square centimeters or above, that's kind of like the go-to for Macy. uh but we've seen since we launched Macy Arthro that not only are you seeing these procedures? You know, the whole thing was designed to be to treat two to four square centimeter defects on the femmeral condile, which is the largest part of, you know, the Macy address of the market because you can explain this better than I, but, you know, the the end of the thigh bone, you know, bears a lot of the weight and that's where you get a lot of the injuries and and it there's just more smaller than than larger.
So that's what we were designing the instruments for, but we have seen now that those instruments are being used in the trolea behind the Patella.
We actually had a patella case where people can lift it up into the Patella without having to flip.s not easy to do well. I haven't tried it. It doesn't look easy.
It's not easy to do, but that's impressive. Sorry, keep going. Yeah, so so that's a feedback.
So just kind of on surgeon use of for Macy users and non-users, using it in different locations of the knee, not just the femmeral condile. And then I think what we've seen anecdotally, and you can share this better than I can. But you've seen what the reason the surgeons were interested in it based on our market research was less invasive surgery, less post-operative pain, faster post-operative recovery, better aesthetics.
And so you see these things on social media where, you know, they're talking about range emotion being, you know, significantly better than you would see from an open procedure and and so on. So I think, you know, that's something we, to your point earlier, we have, you know, different, you know, we have a registry going on now so that we can look at those early post uh surgical outcomes. And I think, you know, because we didn't do a clinical study, you couldn't measure them prior to approval.
So that's something we have to do post approval. uh and you know, hopefully, you know, that kind of bears out that you're seeing all those benefits that you would expect from less invasive yeah, I think that you might as been one of my LinkedIn posts then. So yeah, that's the uh, yeah, no, but will, I mean, I think people you can't slow them down now. They get this surgery now and before it was a lot slower and now you can't slow them down.
I mean, I've had out of the five I've done, I've had three where I've had to tell them to stop moving so fast. So that's a good thing when you're slowing the patients down that much, well. So anyhow, so the um, I think, Nick, we don't want to cut you off too soon, but I want to make sure you have a few minutes.
If you got about like two minutes, can you talk about what you think of the future is for this? Yeah, well, you know, for Macy generally, you know, we think, because again, I as I mentioned, um, we're still, I mean, we're eight years into the Macy launch, right? And you're still seeing this product grow 20% a year as we're adding more surgeons. you know, we look at how many biopsies or surgeries are done per surgeon as surgeons kind of identify more patients within their practice.
So, you know, we think the core Macy, you know, will continue to grow. We think with Macy Arthur on top of that, there's an opportunity, you know, for better patient outcomes and and more surgeries. And then, you know, they see in other joints.
So we expect to, you know, there's cartilage on the end of all the bones in your body articular cartilage. And, you know, the next biggest opportunity is in the ankle. And so we've been working with the FDA on kind of developing the the plan for us to launch a Macy ankle study, which we expect to do in the second half of this year.
So file an IND in the first half of the year, um and then initiate the study in in the back half of the year. And we think that will be we already know, you know, we can't promote it because it's not an approved use, but there's certainly publications out there of surgeons that have had that have treated ankle cartilage injuries with Macy. I mean, it's been used in the hips, the shoulder.
Again, we can't promote that. And, you know, in some of those other joints having an arthroscopic option will be important. hundred percent, especially the ankle, but that's the I mean, you're getting into the perfect topic. I think for the viewers, this is a knee surgery product off label uses the other areas like coming down the line, um and you heard it from the man himself.
So that's the plan. And once now that we've built our new manufacturing facility, which you need to come up and see in Burlington, uh which has its own training lab, so you uh I think you'll you'll enjoy doing that. But that also is has been, you know, this facility has been built for global manuf to meet global manufacturing requirements.
So our we're doing right now an assessment of sort of OUS opportunities in Europe, Latin America and certain countries in Asia. So that's an exciting opportunity for us as well. That's awesome.
Well, Nick, thank you so much for being on. I don't want to cut you off, but you know how the social media doesn't like it if we go over an hour. But like like, I think I think I think I told you so, Nick.
We went to an hour. one quick. Hey, um you said you're going down to Radio row getting ready for the Super Bowl uh down in New Orleans. What are you going to eat Johna Beets?
What is the gay plan? We don't care about anything else. What's the food that you're going to consume?
It's going down to New Orleans? It is absolutely delicious down there. Will, I told you I grew up in upstate New York.
When the builds got bounced, you down? We're going to let the team uh take this one. I've been to a number of them, so other members of our team and other surgeons actually um a great guy, a former NFL Solomon Wilcott, who's was a CBS announcer and a member of the Bengals. uh he kind of does it with us. um and so there'll be other surgeons from around the country that that do that as well.
So I will be sitting this one out, unfortunately. Yeah it makes sense. I've I've got a lot of friends.
I'm originally from New York. I got a lot of friends back in New York that are um all I said was, I'm sorry and and I left it as that and and we're going to move on because I don't want to end this on a bad note. and I want Nick to be upset with me. uh Dr. Garcia made me ask that question. I'll just say that.
That's true. Thank you so much for being a part of. We appreciate your time.
This was fantastic and I hope everyone got some great information out of this. Thank you. Really appreciate it.
Thanks everyone. All right. Take care. Have a good night. Bye.
Audio Transcript
Victor Wembanyama’s Season Ending Injury: The Risk of Blood Clots in Athletes.

Victor Wembanyama’s Season Ending Injury: The Risk of Blood Clots in Athletes.
[00:00:00] Will Sanchez: Welcome to Sports Talk. I'm Will Sanchez, along with our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia. Dr. Garcia, uh, we almost didn't have a chance to do this episode because the weather out here is a little bit crazy. Lights are flickering, so hopefully we'll get through this. Um, but this was a good, uh, Good episode to talk about first and foremost, before we get into it.
[00:00:41] Will Sanchez: How are you? Are you, are you by candlelight? Are you ready with your lamp, your flashlight? What's going on over there?
[00:00:47] Dr. Grant Garcia: Uh, we're good. I was literally telling you right when we about to record this and then it kind of, everything shut down. I was like, do you hear the hail outside? And then lights went out, internet went out and about 40 minutes, we lost it.
[00:00:59] Dr. Grant Garcia: And we were thought we're [00:01:00] not going to get this episode recorded. So this is exciting. Uh, we may get cut short. Who knows how this is going to go. Um, I have candles, I have regular lights, so we're good. Uh, internet's working for now. So we're in a, we're in a good state.
[00:01:13] Will Sanchez: You know, we're about to have this conversation about the former number one pick in the NBA draft, uh, Mr.
[00:01:20] Will Sanchez: Win by Nyama. But before we get to it, because we're discussing injuries, we always want to give a shout out to our good folks here at the recovery shop, take it away.
[00:01:30] Dr. Grant Garcia: Well, again, you know, our sponsors recovery shop, and hopefully at some point we can have them on us can learn even more about them, but yeah, as a surgeon that does the complex surgeries.
[00:01:39] Dr. Grant Garcia: Uh, having the stuff here again today, I had a bunch of patients in the office that needed surgery and they were asking, you know, what else can I do? What else can I have? I know you're going to do a good surgery. I know you're going to give us the best that you can give us. But what about the post recovery?
[00:01:53] Dr. Grant Garcia: And that's really what's key here. So we have nutrition options for patients. We have the options for the nice machine, which has been fantastic. My patients [00:02:00] love it. Um, you know, the re bliss and other innovative things. And really, if there's a product that the patient wants, I can get it and put it on the recovery shop, which is really nice.
[00:02:08] Dr. Grant Garcia: So it all comes together in one thing. It's essentially hate to say is, you know, the equivalent of an amazon for surgical stuff, but really it's all vetted. It's good quality vendors, which is really nice. And as a surgeon to have this at your fingertips, to have your own personal shop that patients can go to and easily get what they want has been fantastic.
[00:02:24] Dr. Grant Garcia: So the, the reviews have been rave. So if any of the surgeons listening are interested, uh, let Mike know. And if you're a patient and you want something like this, uh, for your surgeon, you should let them know about it because it's pretty easy and anyone can do it. So thanks guys. Mike
[00:02:38] Will Sanchez: B at shop recovery.
[00:02:40] Will Sanchez: com. That's, that's a cool name, man. Mike B, Mike B. It's like a rapper. I don't know. I'm kind of going through, uh, my hip hop days. I've been listening to a lot of old school music. So I think that's what I'm triggered. Anyway, I digress like I always do. So let's get into this. The unicorn. Victor Wimbayama, right?
[00:02:58] Will Sanchez: [00:03:00] 2023 Rookie of the Year. 2024 almost upset the United States, won the silver, had an opportunity to win the gold. The, I mean, the sky is the limit for this athlete and Uh, less than a week ago, we get news that his season has ended and not in a way that we usually think, right? When you have someone that's seven, five, seven, six, right?
[00:03:27] Will Sanchez: And for someone that is a knee specialist, having someone that big, I'm pretty sure if I would have said, uh, Dr. Garcia, man, uh, uh, when by Yama's out, you would have, where are you? The first thoughts would have gone. injury knee, something like that. Like Zion. I'm thinking like Zion.
[00:03:44] Dr. Grant Garcia: I'm thinking meniscus. I'm thinking cartilage.
[00:03:47] Dr. Grant Garcia: I'm thinking, you know, just the, the, the sheer size, you know, you have Yao Ming, who is obviously a lot older player now, but foot injury, you know, it's always lower. [00:04:00]
[00:04:00] Will Sanchez: Yep. And instead we get a diagnosis of this deep vein. Uh, what is it? Thrombosis, a DVT, uh, in his right shoulder. So why don't you explain to the viewers, the listeners on really what this means.
[00:04:15] Will Sanchez: And, you know, I, I'll let you talk about it because I've got lots of questions. Awesome.
[00:04:22] Dr. Grant Garcia: Um, I thought it was a good episode because I think that for. For people listening, they're gonna say, what the heck is this? This is like really weird. And for my patients, this is actually a very high concern level for them.
[00:04:35] Will Sanchez: Yeah.
[00:04:35] Dr. Grant Garcia: And I would say that every day when I'm counseling patients, this is something that comes up and they ask about this. So as an orthopedic surgeon, I deal with DVTs all the time because it's lower extremity or upper extremity. Um, and so this diagnosis is a big deal. So basically what it means. is that there are different areas you can caught the blood.
[00:04:53] Dr. Grant Garcia: So the blood flows around your body like pipes, right? So you got the hot water, the cold water, the cold water is the veins, which is the blood coming back [00:05:00] that has no oxygen. And the hot water is the red part. That's your arteries. That's where the blood is fresh with oxygen. Now. Most of the time, the arteries don't get clotted very often, except for like, you know, heart attacks or things like that.
[00:05:12] Dr. Grant Garcia: But the blood clots usually happen in the veins. So that's why you call them the, you know, deep vein thrombosis. That's where it's most likely caused. The problem here, which is really weird. So basically, if they get a clot somewhere, and that clot backs up fluid, and you can get pain and everything else.
[00:05:30] Dr. Grant Garcia: That sounds bad, but the real problem with this is when the clot goes to either your brain, which is much less likely. But the one that you worry about the most is the lung. And even doing some research on this, there's a few famous people that have actually died from a blood clot in the lung. And I have thankfully never had a patient have this, but I have heard of patients that have had blood clots and it's gone to the lung.
[00:05:51] Dr. Grant Garcia: So that's what we worry about more, Beth. The DVT idea is not as stressful. The idea of the blood clot going somewhere else is a concern. [00:06:00] And that's why it's going to be really important discussing this situation. Because in, there's other athletes that have had this, even basketball players in the last few years.
[00:06:09] Dr. Grant Garcia: And those Were a lot of them were lower extremities. So the leg, which is much, I see much more commonly, this was in the shoulder. So how many shoulder blood clots do I see a year? Maybe one, if we're lucky, we actually saw them increase a little bit with COVID. But this is not related to that, um, but upper extremity blood clots are very uncommon.
[00:06:30] Dr. Grant Garcia: They're actually more common in athletes than anybody else, but they're just not common. And so one of the thoughts here, we can go into this in a minute is how did he get this, right?
[00:06:38] Will Sanchez: Yeah.
[00:06:38] Dr. Grant Garcia: What size was it? So they're diagnosed with something called thoracic outlet syndrome. If you read some of the articles again, we don't have a diagnosis yet.
[00:06:45] Dr. Grant Garcia: Yeah. Um, the number one thing is to get the blood clot out of there. So not with surgery, but to thin it out. But anyhow, so I can go off on this in a second, but this is a big deal because obviously he's out for the season. And the question is why, right? Why is he out for the season? Well, he has to be on [00:07:00] blood thinners for six months.
[00:07:02] Dr. Grant Garcia: And if you're on blood thinners, imagine your blood, like six months.
[00:07:06] Will Sanchez: Wow. Is that just standard? I know you're getting into the explanation, but I just want to cut you off there. Is that standard if you're having a blood clot that you go, hey, automatic, we're getting you on thinners. You're doing a mandatory minimum of six months.
[00:07:20] Will Sanchez: What's the protocol when it comes down to something like this? Or does it vary due to age, size, location?
[00:07:28] Dr. Grant Garcia: So first off, many people get blood clots are People to post surgery. So they're not going back to sports at three months, three to six months ish is when we treat these blood clots. The thing is he's playing high impact sports.
[00:07:39] Dr. Grant Garcia: So if he hits his head or he hits his arm and he cuts himself, he could bleed and not stop with this. So that's the biggest problem. And the number one risk is the head, right? Because if you hit your head, usually, you know, you knock it, you get a concussion, right? Like to a stuff. The blood vessels are small, but they can clot pretty quickly.
[00:07:59] Dr. Grant Garcia: If he's on [00:08:00] blood thinners and he gets hits his head, he could die. It will keep bleeding. It will not stop. And so that's the reason that he stopped having to stop doing these things because he could get bl blood bleeding other places. And that could cause much more serious issues. Right. Like let's say he was elbowed in the spleen or something and it popped.
[00:08:16] Will Sanchez: Yeah.
[00:08:16] Dr. Grant Garcia: Right. Or he has like a, he has an injury to his something. 'cause he gets, and these guys are getting knocked, all
[00:08:21] Will Sanchez: burn in the ball, right? He, he dunks the ball, doesn't land on his feet, lands on the side. We've seen that a lot of momentum. Somebody's hanging off the rim, legs go flying up in the air.
[00:08:31] Will Sanchez: come crashing down into the back, the lung, the kidney. Those are some of the ramifications, not just getting elbowed or, you know, or bumped into, right?
[00:08:43] Dr. Grant Garcia: Yes. And that's the reason to stop him playing. But also the reason is because if his blood clot's not gone and you hit him or he moves around, you could release the blood clot into his lung.
[00:08:52] Dr. Grant Garcia: Now, the weird part here is they're thought, they think that maybe this blood clot came from his leg and got into his shoulder. But [00:09:00] that's kind of weird because you got to go through the heart and there's not, you can have a hole in the heart where it goes through, but imagine there's got to be certain stops.
[00:09:06] Dr. Grant Garcia: But the problem is you don't want it to go to his lung because that's called a pulmonary embolus and that one is not good.
[00:09:12] Will Sanchez: So as a doctor, how do you, how do you check that? What's the, what's the process if, because you just told me three different things. It's in the shoulder. They think it's in the leg.
[00:09:21] Will Sanchez: You may come from the heart. So how do you, how do you backtrack to find out where the source is and then at that point go forward in treating?
[00:09:31] Dr. Grant Garcia: So generally patients with blood clots in their, in their legs or their arms, they're going to have a lot of swelling. So like for instance, you know, even one of my partners who I work with, I got a blood clot after a surgery.
[00:09:41] Dr. Grant Garcia: It wasn't mine, but it was still a surgeon nonetheless. And you know, even some first orthopedic surgeon, it took a while for them to figure out like a couple of days. And basically what happens is a lot of patients, at least post surgical and in this case, probably similar. When you get a blood clot all of a sudden it really hurts and it's really swollen and it's red and it's inflamed because remember now the blood [00:10:00] it doesn't always completely clot off but the blood can't go anywhere so it's getting blocked so then it starts to swell up and sometimes it can even get like little infections and things like that but generally it just swells up and it's really red.
[00:10:10] Dr. Grant Garcia: So it looks like it's an infection, but a lot of times it's a blood clot. And so this is most common in the calf. And so you'll, you'll, you see these patients and you say, when you're surgery recovery, you're two or three weeks out. If all of a sudden you get worse, there's generally only one thing it can be, and that's a blood clot.
[00:10:28] Dr. Grant Garcia: I got you. And so to be honest with you as an orthopedic surgeon, I probably see one of these every month or so, you know, if you, if you don't see these blood clots, either you're not looking for them and that's really scary. Or you don't do enough surgeries because the odds are very high of seeing them.
[00:10:45] Dr. Grant Garcia: And everyone, every orthopedic surgeon I know has seen one of these. And you can get them before or after too. Like, like your Achilles injury, that is extremely high risk for a blood clot.
[00:10:54] Will Sanchez: Yeah.
[00:10:54] Dr. Grant Garcia: Beforehand. Or ACL tears. You have patients come in, I had a patient that flew in for surgery [00:11:00] recently. And they didn't even check her before, and they didn't realize that she had a blood clot, so I caught it before the surgery.
[00:11:05] Dr. Grant Garcia: That's okay, as long as you catch it, then you put him on something which he's probably on, which is a blood thinner.
[00:11:11] Will Sanchez: Yeah.
[00:11:11] Dr. Grant Garcia: And then you can do your surgery, you take a break from the blood thinner for a couple days, and then you go right back on it to prevent the clot from expanding.
[00:11:20] Will Sanchez: Is it normal for someone his age that didn't have surgery, that is in great shape, that runs around, not overweight, he's a slim guy, he was just in the NBA All Star game where they announced this, what, a day or two later, he was just there participating.
[00:11:38] Will Sanchez: I mean, are there some things that you're going, hey, wait a minute, what, you know, we haven't seen this or we didn't see it coming. Or is it something like it doesn't matter? It just occurs out of, it could come out of anywhere.
[00:11:50] Dr. Grant Garcia: So there are, there are certain rare conditions. So baseball players get this and it's from overhead throwing and it can be from two scenarios, one constantly [00:12:00] moving the arm and irritating the vessels.
[00:12:02] Dr. Grant Garcia: So there's something called burkhouse triad. So it's, it's where you have blood that's extra clotty. Probably not in his case. They would have caught it already, but he could be diagnosed with something like that. Right. So some people who have this cloudy blood, they don't find out till they get their first blood clot and then they get tested and they find out or they have a family member that passed away from a blood clot and then eventually they get tested.
[00:12:25] Dr. Grant Garcia: So I've seen all these different scenarios. This is probably not that case. Then there's something where he's like, It's not moving, right? Where it's like he just like sits around like you go on a plane flight, right? People get blood clots after plane flights sometimes. It's why you can't fly after surgery for the first few weeks That's why you're not recommended because you can increase your risk of a blood clot Yeah, you probably see people walking around the plane on long flights That's what they're trying to stop and then the third one is injury to the blood vessels and that's what he could have had which is you know got smacked in the arm or got nailed the arm or the leg and And then somehow that injury caused the clot.
[00:12:59] Dr. Grant Garcia: Now, [00:13:00] again, not that common, but Will, we were looking to show up. There's been what? There's been four that we know of that are big. Chris Bosch, right? We all know Chris Bosch.
[00:13:09] Will Sanchez: Yeah. Yeah. So
[00:13:11] Dr. Grant Garcia: many clots.
[00:13:12] Will Sanchez: Yeah. Yeah. They, he, he thought he could complete, uh, he could play through it. He thought he took enough time, but, uh, and you're the perfect person to talk about this.
[00:13:24] Will Sanchez: The doctors were like, I don't feel comfortable, uh, clearing you, you've had a great career. Why don't you, uh, go home and chill out, you know? So when it comes down to something like that, and maybe you could talk to the severity and that's what we're getting at, you know, what is the ultimate right as a fan and just, you know, being concerned about the injury, what's the level of severity, it can be, you know, something that it's on one scale of severity, or, you know, if you have.
[00:13:54] Will Sanchez: whatever signs that you want to call it, this can be a little bit more concerning than what you [00:14:00] originally may think. What, how does that get diagnosed now?
[00:14:04] Dr. Grant Garcia: Well, I think the thing is figuring out what he has, right? So everyone you've talked about are generally lower extremity. So there's been Brandon Angram in the New York, New Orleans Pelicans.
[00:14:13] Dr. Grant Garcia: He made it back after a season, but his was a lower, he was a lower extremity, a blood clot, if I remember correctly. And then Azura Thomas, he's the Pistons. He was actually just diagnosed in March. with another blood clot again in the leg. And he's going to eventually be cleared, hopefully at the end of the season.
[00:14:30] Dr. Grant Garcia: So the question is, why did he get this? Because those are all leg ones, right? I think Chris Bosch's was the leg. I think actually Chris Bosch got something to the lung too at some point. Yeah. Which is not good. Yeah. That's what we talked about, right? The, the danger in the lung. Go ahead. Yeah. And it's usually from the leg, right?
[00:14:46] Dr. Grant Garcia: Because the leg goes all the way up into the heart. The heart can distribute things out to the arms.
[00:14:50] Will Sanchez: Yeah,
[00:14:51] Dr. Grant Garcia: so there is some thought this came directly from the arm itself If it came from the arm itself, it can be random, which is very rare again I've seen in covid covid [00:15:00] shots or could be like at covid.
[00:15:01] Dr. Grant Garcia: I've had a couple that got it from that That's a weird one We only saw that we saw like two in one month in our practice and then we hadn't seen him since then But that's a very rare thing, but generally it can come with tos. So thoracic outlet syndrome now again we don't have time to go through this entire thing, but basically what it means is like Your brachial plexus.
[00:15:19] Dr. Grant Garcia: Why don't you pull up that uh, that image and see if we can show people So this is this is a good thing go to the next one Let's see if we can show so before we go back to tos you guys can see so the blood clot in the leg It's the swelling, the redness I told you about, and then it can go to the lung.
[00:15:37] Dr. Grant Garcia: If it goes to the lung, that's when people get a lot of symptoms. They have trouble breathing, and they can do a, they usually do a CAT scan or a CT scan, and they check to see how the arteries in the lung are doing. Now, people can survive from this. I mean, I have had patients that have gotten PEs, probably three or four off the top of my head.
[00:15:54] Dr. Grant Garcia: Now, they all were healthy, and they all did fine. Big blood clots can kill and or [00:16:00] if patients are older that can also be an issue. So it is real but just because someone says they got a PE doesn't mean that they're going to die. That's something that's something good for people to know. But obviously we don't ever want that, right?
[00:16:09] Dr. Grant Garcia: Like do everything we can to avoid it. Um, Why don't you go to the, uh, the next slide? Um, One more over there. Um, go to the end ones that we showed him. I'll show him thoracic outlet. Keep going. Yeah, that's good. Go back to the other one. So this one's really good. So this is a good image. Again, you can see there's that big blue vein.
[00:16:29] Dr. Grant Garcia: That's a subclavian vein. I don't want to gross out the viewers too much, but that vein can get compressed and that's probably what he got here. Uh, blood clot and blood clot went all the way down into the arm. Now, thoracic outlet is where you can see that kind of in the middle of the neck. There's, there's, there's a muscle there.
[00:16:46] Dr. Grant Garcia: There's, people can have an extra rib and it can push on, it can push on the area as they get like more tension or they do something like their throwers. Throwers get it from this constantly cocking back scenario. And the TOS can [00:17:00] come in three versions where it can be a version where it pinches the nerves.
[00:17:04] Dr. Grant Garcia: And people talk about their hands going numb. That's not what he probably had. The other one is where they feel like their arm goes to sleep. So they lose all their sensate, all their blood flow to the arm. That's an artery one. And then the third one is a blood, the vein where it pinches the veins. And that could be what he had.
[00:17:21] Dr. Grant Garcia: He could have been doing so much of this and blocking and doing all these things. He compressed it.
[00:17:26] Will Sanchez: His arms are usually up. He blocks shots. You know, he's, he's maybe, you know, he's, he's a unicorn, right? That this, this monster giants of a man that's just makes it impossible. He was runner up for defensive player of the year where his countrymen Rudy go bear one last year.
[00:17:44] Will Sanchez: So he's intimidated on the floor, but going back to having those arms up, moving around, you know, especially in that upper area, um. you know, whether that played a part or not. So knowing the information that we have right now, what [00:18:00] is the main concern for you? If you go, hey, we're gonna test, we want to identify where this started, wasn't the shoulder, was at the leg, wasn't somewhere else and then go from there.
[00:18:11] Will Sanchez: So what's your biggest concern? Um, when you're doing this evaluating evaluation process and you've already put them on these blood thinners.
[00:18:21] Dr. Grant Garcia: So let's assume, so to diagnose it usually other than the SCAT scan, usually it's an ultrasound. So they look at the blood clots and they can see the arteries and the veins.
[00:18:29] Dr. Grant Garcia: So for me, one, the number one concern is making sure it's not from anywhere else, because if it came from the leg, we have a big problem, right? Cause I mean, it's floating around, right? If it came from the shoulder directly, that's a better scenario in my opinion, because a TOS thing, a thoracic outlet thing, that's something that's not always that easy to treat, but if you know, he's got it, you could, you know, be much more cautious about it and maybe do repeated ultrasounds, which are really low risk.
[00:18:51] Dr. Grant Garcia: Um, but what worried me the most is that they found out that he had a blood clotting disorder, right? Because if he can, if he makes his blood extra thick, then he [00:19:00] has to be on constant blood thinners. That could end his career. I don't think that's the case here. Um, and I think they would have been a little bit [00:19:05] Will Sanchez: more.
[00:19:06] Will Sanchez: How do you check for blood clot disorder? What are the signs and how do you check for that?
[00:19:11] Dr. Grant Garcia: So the signs are you get blood clots, but that's generally the, there's other things that can be associated genetically, but it's very uncommon. Okay. So I got a
[00:19:18] Will Sanchez: quick follow up question here. I, I, I'm going to interrupt you here.
[00:19:22] Will Sanchez: So do you think San Antonio spurs? They have this information when they got it. It's really interesting because like I said, he, this was announced right after the NBA all star break. He was at the all star game, but now what's the documentation as a professional trainer with the information you have, and now you're reaching out to maybe.
[00:19:45] Will Sanchez: The, the French ball club, the other clubs that he had been with in the past, how far back now you start tracking down that history to see if they've been any other sites,
[00:19:56] Dr. Grant Garcia: probably not that much. Cause I feel like if you have a clot like this, either [00:20:00] he would have had a major problem or not, or not. I don't think I probably did a pretty good background check for his family.
[00:20:06] Dr. Grant Garcia: So he may have reached out to his family and they would have been like, Hey, you know, tell us if history of blood clot in your family, but generally you don't, that doesn't really matter because if all, if everyone, his family got blood clots. You'd probably know it's genetic, but if they didn't, it doesn't mean he doesn't have it.
[00:20:20] Dr. Grant Garcia: So I think, it's a, it's, it's a lot of, I think what they do is there's these, there's people, doctors called hematologists, and they can run these panels where they take your blood and they look for anything genetic in there. And they have all these different clotting disorders. There's rare ones. I don't think this is the case here, but I will tell you in my opinion, in my practice, the people that I told you that got those lung clots or people that have gotten really bad blood clots and have had.
[00:20:45] Dr. Grant Garcia: Almost all of them, we're the ones that found out they had this. Because it was the first time they ever knew it. I mean, I can think of a girl, uh, two years ago that got a blood clot after a big surgery I did, and it went to her lung. She did really well afterwards. No issues later on. And [00:21:00] we turned out that she found out she has a special clotting disorder.
[00:21:02] Dr. Grant Garcia: She had no idea. She was 33. She made it all the way to 33 until she figured that out.
[00:21:08] Will Sanchez: So with this disorder, right, we're talking about minimum six months. That puts us probably end of August, right? So shortly after that, maybe we're looking at a month or so, maybe six weeks before they start to do training camp and they kind of ramp up, you know, you know, all get, uh, October.
[00:21:26] Will Sanchez: So what does that look like now? Six months, we've done six months. What's the process? What's the next steps? So if you're a fan of the Spurs fan of this young man, you're kind of going, okay, this, this should be the steps. And if he clears these steps, we can see him participate back in activities for the start of the 20, 25, 2026 season.
[00:21:51] Dr. Grant Garcia: Well, obviously, you're going to probably get repeat ultrasound to make sure that blood clot goes away, right? The blood clot's gone. And that's a good thing. Right. And then what you're going to [00:22:00] do is he's going to go to this fitness to play panel. And it's made up of three different doctors and they're going to review the case and they're going to make sure they feel it's safe and they're not really related all to the San Antonio Spurs, which is good.
[00:22:11] Dr. Grant Garcia: It's the same thing. It's a concussion thing we talked about, right? Because as much as we're team physicians and we want what's best for the player, there's also the team that, you know, they can always be in your ear. And you know, if it's kind of a gray zone, you don't want the doctor to feel obligated one way or the other.
[00:22:27] Dr. Grant Garcia: Right? So you pull out that scenario. Um, interesting enough, actually, we were looking this up. There is actually a study on this, and they found that upper extremity, they found that athletes with upper extremity played return to play faster than those with other type of, uh, uh, blood clots. So even though I told you six months, it's actually average of 4.
[00:22:49] Dr. Grant Garcia: 3 months for return. If you have isolated upper extremity, which is what which what upper isolated with the two key things that you said their upper and [00:23:00] isolated. So those other players were lower extremity. They were a longer recovery. So it's just interesting to, to see that. Um, the one other thing is sometimes they do surgery on this.
[00:23:11] Dr. Grant Garcia: Hopefully he won't need that, but they can actually go in there and core out the blood clot. They probably won't need to do that in him, especially if they caught this early enough. Um, but again, there are, there are not that many cases of this. So it's not like we have a lot to go on. I'm giving you, you know, over the last five, 10 years, I just told you about four players.
[00:23:29] Dr. Grant Garcia: That's not very many in basketball, right? If you talk about how many people have ACL tears or cartilage injuries and things like that. But it's also not, I mean, I don't know if anybody knows this, but we, we found this out too. Serena Williams had tons of blood clots and she was able to play with it. Now again, tennis, not contact, even though it's a, you know, it's a tough sport, it's not contact.
[00:23:51] Dr. Grant Garcia: And. You know, it's, it's just a different animal there. But the problem you have too, is what people don't think about is, and I didn't even realize until we did this, this [00:24:00] episode, the travel, right. They're constantly flying. That's what I
[00:24:04] Will Sanchez: was going to bring up, man. I'm so glad you brought that up. That's exactly what I was going to ask you, you know, the travel, do you.
[00:24:14] Will Sanchez: stretch, cool down a certain way before you get on the plane. Uh, Steve Kerr was recently complaining about you want his own prime time tv. We're finishing up and getting out of the locker room at one o'clock in the morning and we have to get on the flight for three a. m. Because we have a tip off at noon on the east coast.
[00:24:35] Will Sanchez: So You know, someone that is in your position, you know, and we'll treat athletes and someone that travels as many times as they do right. LeBron James recently posted on X saying, look at all the games that we have back to back nights that he was complete. He's like, this is ridiculous. So what are your thoughts with travel, professional athletes [00:25:00] and from going from zero to 100 back to zero and now on a flight?
[00:25:06] Dr. Grant Garcia: I mean, it's, it's no joke. I mean, that's one of the reasons these guys have trouble getting back sometimes. I mean, they can return to well, but the, but he's going to be always forever risking this happening again, regardless of what people say, because as soon as that word blood clots in your history, if I have that in my patients, like you get, you tell me I've had a blood clot, like I'm automatically putting you on blood thinners for every surgery.
[00:25:29] Dr. Grant Garcia: Like I'm, I don't want that ever to happen again. So like, you know, if he ever needs a, if he ever gets a surgery, he's getting a different level. Now, again, Upper extremity is a bit different and if they find out that he has TOS and it was caused by that rather than anything else in his body. I think the biggest concern for anybody with PIM is that whether they, if they found nothing.
[00:25:50] Dr. Grant Garcia: We have no idea why he got it. We have no idea where it came from. Which I'd be surprised, hopefully they can find a reason. Um, that's when we get a little bit more concerned, right? Because then, [00:26:00] do we just have to assume he's, this is, we have assumed worst case scenario for, you know, this could be a cloudy disorder, we can't figure it out, or something else, and we have to be extra cautious of him.
[00:26:09] Dr. Grant Garcia: Um, but I can sure as heck tell you that if he has any issues, anytime in the next multiple years of playing, they're going to check everything again for this and it will be on everything. And again, I, I think a couple of years of playing really well without any new more blood clot. That's fine. But we know, I mean, look at that.
[00:26:24] Dr. Grant Garcia: I told you Serena Williams had multiple. Yeah, this may not be the last time.
[00:26:28] Will Sanchez: And would you just assume that she was on those anti anticoagulants, you know, when, because of those multiple blood clots and even when she was pregnant, right? I mean, she was yeah. She was pregnant. She gave birth. That's a really
[00:26:41] Dr. Grant Garcia: risky.
[00:26:42] Dr. Grant Garcia: That's really risky because some of the medicine can have problems. So there, I'm sure there are different things. Now you can get something called a filter where they put a thing inside of your vein to prevent it from going to the lungs. But in his case, there's no way to prevent it from the shoulder.
[00:26:57] Dr. Grant Garcia: So, like, this is, it's a very, it's a little bit [00:27:00] more complicated, just the way the blood flows.
[00:27:04] Will Sanchez: Extremely interesting. This is, this is absolutely fascinating, especially to see what the outcome's going to be. Uh, I'll be curious to see if they ever, you know, uh, share that type of information and say, No, this was isolated. We're good. He's, he's good. Don't worry about it. But as you have already mentioned, Yeah.
[00:27:25] Will Sanchez: Now that I, I'm aware of this blood clot next time or anytime that I'm treating that particular patient that's in the back of your mind and you're making sure you're doing your due diligence prepping the patient for wherever, you know, he may need in the future. Because as we know, we're professional athletes.
[00:27:46] Will Sanchez: He is only a matter of time. It's not if it's when. That they're going to eventually be in some have some kind of surgery, whether no matter how big or small it is.
[00:27:56] Dr. Grant Garcia: Well, and I think we could say it's pretty impressive how well he's done so [00:28:00] far without any injuries, right? I mean, yeah, is that how many big men and again, he's got a different build, but he's how many big guys like him have gotten drafted and then just.
[00:28:12] Dr. Grant Garcia: Not done that great. Obviously, he was different. He was extra special, but there are a lot of big guys that have just kind of injury, injury, injury,
[00:28:20] Will Sanchez: Northwest Greg Oden, you know, all these guys have come and go throughout the league and that's what made them special. That's what makes them exciting to watch that.
[00:28:28] Will Sanchez: You know, that's why you buy your NBA package. You know, to see these, these incredible athletes, when we watched the Olympics, he was one of the reasons to watch, to see him out there and playing and representing his country and knowing everything that, uh, that's a part, you know, someone that could block a shot, could dunk a ball and then shoot a three.
[00:28:48] Will Sanchez: I mean, special. Right. And that's why you hope that as a fan, you know, he bounces back and that's why it was so interesting to have this conversation about this player. [00:29:00]
[00:29:00] Dr. Grant Garcia: Yeah. And I think, I think for the listeners, I think he'll bounce back. I think he will be, we just have to be, you know, you know, in the show, I'm always more cautious, right?
[00:29:07] Dr. Grant Garcia: Like there's always a potential risk here or there, but like I said before, from the studies, you know, the upper extremity players get back faster, so there's a chance that he's ready to play sooner, but it won't really matter, right. He's gonna start the next year of the season. They're not gonna push him any earlier.
[00:29:22] Will Sanchez: Yeah, no, and it's smart by them doing it. And, and, you said, exactly, you're cautious, you're optimistic, I'm the ones going What if? What if this doesn't work? Tell me the worst case scenario. I'm that guy. I'm, I'm the one that just going, Oh my, what's got the lights are flickering. We're all going to die, you know, like, so, you know, that's part of the yin and yang of our show, you know, that's why any, uh, any last thoughts as we get ready to wrap this up, um, whether it's about him or just, uh, blood clots in general, that may be informative for, uh, for our listeners.
[00:29:59] Dr. Grant Garcia: [00:30:00] I tell the patients that and listeners. So, you know, obviously this thing's really rare. If you ever have something where you have a lot of swelling and problems in an area and you've got a history of this, be aware of it. If you've had surgery, be aware of it. You just don't want it to miss it. So if you're, if your doctor's saying, Hey, this is not a big deal, which hopefully they're not.
[00:30:17] Dr. Grant Garcia: Just go get it checked out. It's pretty easy to get this. You can get an ultrasound anywhere you want. I mean, you can walk into a clinic, you can walk into an urgent care, and get the ultrasound done just to see whether or not it's there. I will tell you that it's unfortunate how many of these I've caught when someone else had said, oh, it's not a big deal.
[00:30:35] Will Sanchez: Yeah, and as you mentioned, the lung, the stroke, the heart attack, or anything like that, a lot of it can be affected, so. Alright, now that we've scared everybody, Uh, we want to thank everyone. Check us out, sports Doc Talk. We've got some great shows, we've got transcripts, we've got some great guests coming up, so we're really excited about that.
[00:30:54] Will Sanchez: And as always, we love the people that first off, always support us and give us some great [00:31:00] shout outs. So if you wanna give us a shout out, you have some show ideas, you want us to talk about certain things, check it out, sport sports.talk.com. We appreciate you Dr. Garcia. Say goodnight. Goodnight guys.
[00:31:14] Will Sanchez: Thanks.
Audio Transcript
Third Times a Charm Superbowl 2025

Third Times a Charm Superbowl 2025
[00:00:00] William Sanchez: Welcome everyone. And thank you for listening, watching, however you're enjoying Sports Doc Talk. We are really happy that you are with us. This is our Super Bowl edition. Obviously, Dr. Garcia has a incredible background. Uh, we, we had to do this. We didn't plan on doing a show, but we're like, we've got to talk a little sports.
[00:00:37] William Sanchez: We got to talk a little bit of injuries, little fandom here. So Dr. Garcia, our orthopedic surgeon and sports medicine specialist. How are you?
[00:00:46] Dr. Grant Garcia: I'm good, excited for Super Bowl, excited for, like you said, like the audience should hear, you know, we were, we've had way too many recordings in the last few weeks and we're getting requests for guests and unfortunately, our time is limited since this is [00:01:00] not our primary job.
[00:01:01] Dr. Grant Garcia: But I am good now, I'm excited and we just want to make sure we have this episode for our listeners because people are always interested in what's going on. They want to hear Will. tease me about my lack of knowledge, uh, other than orthopedics. And, uh, and then also for the injury reports, because I think that the injuries some people don't understand and or the NFL purposely sort of construed the picture a little bit for people.
[00:01:24] Dr. Grant Garcia: So we'll go through that.
[00:01:26] William Sanchez: Hey, it's Super Bowl 59. It's a rematch from Super Bowl 57. Where, uh, the Chiefs defeated the Eagles 38 to 35. If we get a matchup like that, then we're going to be in for a treat. Uh, before we get started, I am wearing my Tiki Barber Giants jersey. And I want to explain because it was pure comedy this season for the Giants.
[00:01:49] William Sanchez: I have my Wayne's World hat on. Because if you didn't laugh, you would cry, uh, just real quick. Looking back at the season, what were some of the [00:02:00] things that, uh, that stood out for you that you remembered? And I know you're a fan of the Giants. Just, I don't know, rambling along. It was a long time. If you're [00:02:10] Dr. Grant Garcia: a Giants fan, there's not much to remember.
[00:02:12] Dr. Grant Garcia: Uh, you know, you know, got, got a lot of fun stuff, like watching players for other teams run rampant when they should have been on your team, but. I think the Malik neighbors, it's probably my favorite thing just to see a player. I mean, imagine, I keep talking about it, basically, you have a player as good as him that put up the numbers that he did with four different quarterbacks, all subpar quarterbacks pretty much.
[00:02:34] Dr. Grant Garcia: So, you know, the fact is he gets a good passer. With a decent team, you know, what can he possibly do? So, and, you know, even better wide receiving crew or whatever else happens. So I, I'm hopeful we're going to see continued improvement. Uh, and so that, that's what I have to look forward to. That's kind of the only highlight from the year and Tyra, I think, uh, what's his name, Tyrod, uh, he did really well as well, [00:03:00] Tracy, Tracy, Tracy, Tracy.
[00:03:02] Dr. Grant Garcia: He did really well. I was pleased with him too. Those were the kind of like two highlights. Um, you know, minus your best players getting hurt like midseason. Uh, so that's, uh, unfortunately it's a, it's a very short episode when you talk about what happened with Jaya.
[00:03:15] William Sanchez: Yeah, definitely. Um, interesting season.
[00:03:18] William Sanchez: You know, we're fans. Um, you know, just looking back, I feel, you know, for for the fandom in Detroit, uh, Dr Bashai, right? Sharif, big Detroit Lions fans. So shout out to him. You know, he I know that he was must have been agonizing over the loss that that they suffered, uh, at the hands of Washington for being a fan of the NFC East.
[00:03:42] William Sanchez: I don't know what we're doing. We, we got one of the top teams now to, you know, you know, back two out of three years, the Eagles are in the super bowl. Now you have this superstar quarterback with Washington. I don't know what to think of when it comes to the giants and looking around, you know, heartache to all my [00:04:00] friends back in New York that are Buffalo bills fans.
[00:04:03] William Sanchez: I don't know what to say anymore. I just go, sorry, there's nothing else to say. They have gone through so many different things, so many different expectations, uh, suffering another loss. It was, uh, it's difficult. I guess the, the moral of the story is, you know, you're concerned with everyone else we suffer, but we don't want, we don't want company in our misery as giants fans, but we, we know a lot of people out there that suffered and what comes down to at the end of this game.
[00:04:31] William Sanchez: There'll be one fan base that's going to be happy and everyone else will either say we had a terrible season. We had a good season. We had a great season, but we didn't win. And that's, what's going to come down to a fun fact. We'll do a little trivia before we kick off. Uh, New Orleans has the most. Super Bowl appearances, uh, tying them with Miami with 11.
[00:04:57] William Sanchez: So have you been
[00:04:59] Dr. Grant Garcia: to New Orleans? [00:05:00] I've been there too many times for a little bit of fun and work events. Okay. So,
[00:05:06] William Sanchez: so real quick, what is your go to either meal, snack, or to do when you go to New Orleans?
[00:05:14] Dr. Grant Garcia: Well, like my travel, which you talked about and like my surgeries, I like unusual, so I like the gator sandwich.
[00:05:21] Dr. Grant Garcia: What? I really like it. I like gumbo. I love the gumbo. Gumbo's love public. There was a place we went, there was a place we went there that had like all Southern cooking and in Seattle it's like really hard to find. Yeah. So I remember having amazing gumbo, but I always search out the gator sandwich. I love gumbo.
[00:05:39] Dr. Grant Garcia: I don't want to like eat it all the time, but I want to try it. I want to say I did it. That's what I have to do without getting sick. What did you think I was going to
[00:05:48] William Sanchez: say? What is it? Just describe it real quick. What's the gator sandwich besides the gator in it? It's legitimately
[00:05:54] Dr. Grant Garcia: gator. No, so it's gator, fried gator, like in a po'boy.
[00:05:57] Dr. Grant Garcia: So it's a po'boy
[00:05:59] [00:06:00] gator.
[00:06:00] Dr. Grant Garcia: But po'boys, I like the crawfish po'boys and then obviously the beignets. Right. If you like New Orleans, you love the beignets. I'm not a huge fan of the late night bourbon street, but I love the, uh, the food there is so good. And like, I could eat gumbo pretty much every day of the week.
[00:06:15] Dr. Grant Garcia: I love gumbo.
[00:06:16] William Sanchez: Love gumbo. Love the pralines. Went there back in 2000 with a bunch of friends. We were hanging out, going for Mardi Gras and our budget pretty much had us down to, uh, Uh, an alcohol budget and a praline budget and now is it and enough gas to drive backwards. We drove down in a huge van with a bunch of us.
[00:06:36] William Sanchez: That's all the story and that's not for this crowd. So we're gonna move on. We've got some people that we're going to show some love. Dr Garcia show some love to the recovery shop.
[00:06:46] Dr. Grant Garcia: So big thanks to our sponsors recovery shop. You've heard this before. It's the more fun episode. But, you know, again, for patients, I had a patient today ask about it.
[00:06:53] Dr. Grant Garcia: They're like, Hey, you know, like I want, like, I love all this stuff you're doing, like a lot of this stuff, but what, what else can I do to get better? I [00:07:00] want like the top of the line, especially from Seattle. They come in with a lot of research, um, and they want to know the best stuff. And so the nice thing with the recovery shop is I can put, you know, normal level, top level, whatever you want.
[00:07:11] Dr. Grant Garcia: And you get to kind of order. It's a nice menu of things for your post op recovery. Um, and ranging from nutrition, which we'll talk about more at some point in the near future. Uh, to, you know, machines that can bend faster and new tech in terms of, um, different ice machines, such as a nice machine we talked about.
[00:07:27] Dr. Grant Garcia: So it's an awesome option for surgeons to offer their patients and it gives them that sort of next level stuff. And again, it's no obligation for the patients, but a lot of patients want this. They want more. And if you offer that to them, they want it. So it's a great thing. So again, reach out to Mike. Uh, they've been an awesome resource.
[00:07:44] Dr. Grant Garcia: And the patients are absolutely love it. So
[00:07:46] William Sanchez: yeah, you know, just we can't say enough good things and you summed it up perfectly. Um, dr Garcia, there's been a lot of Super Bowls. We've seen a lot of Super Bowls. Um, do you have a memorable [00:08:00] injury or occurrence that had happened in the past that really stands out for you?
[00:08:05] William Sanchez: Whether a plane player going into Super Bowl with an injury or sustaining one in the big game that you can recall there?
[00:08:13] Dr. Grant Garcia: Well, I mean, the one I keep seeing about, oh, I hate to say it's from like a malpractice reason in the sense that like seeing it, but Terrell Owens, when he, when he waived the doctors, I think he had, we, I don't know if we're going to talk about it, but the fibular, he had a fracture of his ankle and he was basically not allowed to play on it.
[00:08:31] Dr. Grant Garcia: And he had to do it right over consent that he wasn't going to sue the surgeons to release him to play in the game. And then he ended up having a phenomenal game. Um, only freak athletes as we keep saying there are regular athletes like, yeah, I'm not even maybe a regular athlete, but a regular athlete.
[00:08:47] Dr. Grant Garcia: And then there's guys like that, right? That like, even when they're 70%, they're better than most people are ready. And so the fact that he's able to do that is just mind boggling. I don't remember any serious injuries, but again, [00:09:00] I'm I'm not the great person for, you know, watching everything at full, full speed completely.
[00:09:04] Dr. Grant Garcia: But, uh, that one really rang a bell to me because that's just insane.
[00:09:09] William Sanchez: Yeah. And it's a perfect segue to this game, right? Because he's with the Philadelphia Eagles. There was a question. He questioned Donovan McNabb's toughness, right? We're going into the little bit more of the sports talk right now than the doctor talk, you know, when, when he played in that game, 122 yards, nine catches was absolutely phenomenal.
[00:09:28] William Sanchez: You know, but can you just describe what that pain threshold or what kind of setback where you're talking about that, that, that fracture and the spring [00:09:38] and
[00:09:38] William Sanchez: you're going into this game and you're playing football, let alone running around to hand touch, but then getting tackled and you know, they tackle you low and God knows there's a little extra little tweaking and twisting here and there just from a pain threshold from either something that you know, or just when your patients go through.
[00:09:57] William Sanchez: What? What are we can't? Can we put any thoughts [00:10:00] on what what's happening there to be in a position for you to play an entire game in those conditions.
[00:10:06] Dr. Grant Garcia: So I take care of a lot of people. I do lots of surgeries and postoperative pain. There's different levels and everyone's got different thresholds. You know, there's some people that they say they like pain tolerance.
[00:10:16] Dr. Grant Garcia: They really don't feel that have a high pain tolerance and they do. And then there's this level. So when you look at the body, there's different nerve receptors. The most insensitive ones are in the bone. Okay. And that's when you break a bone. That's why people are like screaming, right? Because they're like, you've seen him in the movies, you see him in the ER, like the broken bones, like one of the worst, right?
[00:10:35] Dr. Grant Garcia: Like there's kidney stones. Those are really bad. There's other things that are bad, but a broken bone really hurts. And not to mention a broken bone when you don't move hurts. So imagine what a broken bone feels like when you're walking on it. So it's like this is this is like a level 10 out of 10 that you're playing on this thing and he's running on it and getting hit.
[00:10:54] Dr. Grant Garcia: So there's no pain describable. Again, I think women take the cake in terms of being able to [00:11:00] handle pain with having pregnancies and everything.
[00:11:02] William Sanchez: Of course.
[00:11:02] Dr. Grant Garcia: And most men couldn't make it very far, we all know. Uh, but nonetheless, the, um, I would say that running on a broken, a broken ankle is, uh, right up there with, uh, one of the most kind of toughest things I've ever heard of.
[00:11:17] Dr. Grant Garcia: So that's a pretty impressive.
[00:11:19] William Sanchez: Okay, let's get to the game. Uh, let's start on the line, right? Because if, if, if this game is going to be determined, it's going to be determined by the line play. Um, we, we kind of know the recipe for Philadelphia this year has been, we are going to run the ball and kudos to them because a lot of teams kind of get away from their bread and butter, you know, what makes it really good.
[00:11:41] William Sanchez: They're not, they're not afraid of that, right? This is what they do. And for them on their offensive line, their big offensive tackle is lane Johnson, and he suffered an, uh, abdominal injury and he's been dealing with that, uh, injury, uh, for a while now. What is, [00:12:00] what are we talking about when, uh, when it says abdominal injury, because it seems a little vague.
[00:12:04] William Sanchez: So maybe you could explain that a little bit better because we go back to the way you started this show. We kind of get some information, but we don't get the whole story.
[00:12:11] Dr. Grant Garcia: Yeah. So, you know, these abdominal injuries, they're usually oblique injuries. They're hard to treat. There are people that do fix them, but they're not that common.
[00:12:19] Dr. Grant Garcia: And generally they just nag, right? Like, so imagine you have. An external external, you have different oblique muscles layers in there and they pull it off and there's like a little hole in the muscle and it hurts. Every time you're twisting or moving, it can feel it pulling. It's kind of like a hernia, but higher up and, and they're really uncomfortable.
[00:12:38] Dr. Grant Garcia: It's like a groin pull, right? We've seen like, you know, LeBron James, he talked about it took him forever to get back from a groin pull. As a swimmer, I had a couple of groin pulls. They're not fun. It's essentially like that. It's a little tear of the muscle and you want it to heal or the muscle tendon and you want it to heal back.
[00:12:52] Dr. Grant Garcia: It's like a partial hamstring tear, you know, those just nag and it's in the abdominal area. So that's what he had likely, obviously, they're not gonna tell you [00:13:00] exactly what he had. Because basically, if he can play, they don't really have to report it fully. The issue is when they get surges and they have to tell you, but again, it's also this like weird HIPAA versus NFL rules.
[00:13:12] Dr. Grant Garcia: And you know, they don't want the team to know, right? Like if it's something that you think that's going to really limit them, you don't want the team to know that he's that limited. because then they're gonna go after him for the play. Obviously, if he's limited enough that it's still safe for him to play, there is a strategy here.
[00:13:25] Dr. Grant Garcia: I mean, some of the coaches are known for really limit, really dumb, dumbing down these injuries. And there's probably borderline to like, are they even following the rules? You know,
[00:13:34] William Sanchez: um, you know, if that's something that after the season you're kinda looking at, is there anything that, is that just time and recovery or is that something that eventually you may go in there and tweak it, or it just, it depends on what, you know, what the medical records say based on that injury.
[00:13:50] Dr. Grant Garcia: I mean, this is one of those ones that I think that rest alone should help. I mean, abdominal surgery is not that common. Um, people do sports hernias and things like that, which this is something similar. [00:14:00] Um, but in general, that's probably not what they're going to do for this if he's been able to deal with it so much.
[00:14:05] Dr. Grant Garcia: Uh, so he probably will just sort of rest it off and the good news is he'll have some downtime after this. Um, but you know, these guys are tough. Like they play through a lot more than we would normally play for. And now the Super Bowl's here, right? Like the team's, you know, the team's about, has a losing season.
[00:14:19] Dr. Grant Garcia: They got like nothing to play for. You know, that's a different animal. Yeah. This is like the final game. And like every one of these players counts that we're going to talk about.
[00:14:26] William Sanchez: Yep. And then on the other side of the ball, someone that's relying on the pass rush, uh, one of the great defensive tackles, uh, in the game, uh, Chris Jones, uh, don't get confused with his brother.
[00:14:40] William Sanchez: Which is the UFC heavyweight champion, but that's a whole other, I digress. See, I go down these loopholes. He has a calf strain. So when you have a calf strain, they're saying they've been sitting them out from practice. So, and this has been kind of lingering. So I wonder what the degree of this calf strain is for you as a big man to [00:15:00] run up against somebody else that's big, push off of them, excel, throw them off.
[00:15:04] William Sanchez: run after quarterback, run after running back on every single play. What are your limitations? Or what are some of the concerns as a doctor that you're that you're treating and maybe rehabbing as you get ready for this big game?
[00:15:17] Dr. Grant Garcia: I mean, the power, obviously, right? There's power in this calf muscle. We've seen it before with other injuries, right?
[00:15:23] Dr. Grant Garcia: These calf muscles are, these don't usually end up in surgery, except that they tear their Achilles lower down. So, you know, you people, you heard of a cat problem and then they tear their Achilles later. So that is a risk in this situation, but probably not that common. These calf or we call them gastric tears.
[00:15:38] Dr. Grant Garcia: Uh, they just are such a nuisance and you know, he's probably booting He's probably treating he's getting maybe prp He's getting tons of other different all these little all the little voodoo things They could possibly do to give him to make him better. Is he and they're probably just trying do you think you put him?
[00:15:53] Dr. Grant Garcia: Yeah, put him in the boot when he's not practicing or something like that to what what is the boo? Yeah, but the issue is they get stiff if you get [00:16:00] the problem You're on is like you want to keep it loose right like you want it to not get No, you want it to heal, but if you get him too stiff and he goes back and fires, right, that'll rip it through again.
[00:16:08] Dr. Grant Garcia: So it's one of those ones that's just a pain in the butt to deal with. I mean, these, these are some of the worst injuries. I mean, these are, I've had, I've had patients take six, seven weeks more than that to recover from one of these. So these are, these are really nagging, which is why they keep them out of practice, right?
[00:16:22] Dr. Grant Garcia: Like if he's that good, he doesn't need to practice, you know, they give him treatment and then hopefully he can make it through the game.
[00:16:29] William Sanchez: Yeah. Does he need the Rebless? I'm over here doing the recovery shop here now. Does he get on the Rebless? He doesn't have to worry about it. I think he's getting even,
[00:16:37] Dr. Grant Garcia: I think he's getting above the Rebless right now.
[00:16:39] Dr. Grant Garcia: I think he's getting more treatment than you would ever imagine.
[00:16:42] William Sanchez: The full time treatment. Alright, as we get ready to move on to some other injuries. Uh, when it comes to the Super Bowl, whether it's you, the household, the wife, the kids, what are some of the things that you look forward to when you're actually sitting down and watching the game?
[00:16:58] William Sanchez: Uh, you know, [00:17:00] anthems, commercials, blah, blah, blah, blah, blah. You know, what are some of those thoughts when it comes down to it? Well, well,
[00:17:04] Dr. Grant Garcia: first off, Mike, I'll tell you right now, my wife has zero interest in the Super Bowl. So she's, I got to like. So right there, that's already, like, she just wants to see the commercials.
[00:17:13] William Sanchez: Okay. Oh, so she's there. She's, she's there.
[00:17:17] Dr. Grant Garcia: She's, she always is there. She will be there. She has zero interest in that type of wife. She is. She just shows up for the Super Bowl. Okay. So she'll show up for the Super Bowl, but she has no interest in who wins. Even if it's a giant, she doesn't. So she did. So that's the thing, the kids, they just think it's fun to hang out with dad and watch the game.
[00:17:36] Dr. Grant Garcia: And they liked the football. They used to watch, like, I have little pictures and they were babies. And they were like on my lap watching the giants. That was before that the giants would make the kids cry. Uh, now that's a different theory. Uh, but, but, [00:17:48] but to be
[00:17:49] Dr. Grant Garcia: honest with you, they really liked this year bowl because they know it's like that there's like, come on.
[00:17:54] Dr. Grant Garcia: We're just hanging out. We're having a good time. They love the commercials, but they don't get them like these to read it. Like some of these commercials are so light. [00:18:00] You know, my kids are still young. So for them, they're not funny. I love the commercials. I like the food. I like to hang out. I just like the experience, right?
[00:18:07] Dr. Grant Garcia: Like the whole thing. And usually it's actually kind of nice when I don't root for the team, because then I don't have to really focus on the game and watch the giants. I'm like fully focused. So it's like, it makes it more of a social aspect, but I think the social aspect of it is good for the whole family.
[00:18:19] Dr. Grant Garcia: So that's what we really like about it.
[00:18:21] William Sanchez: Yeah. Um, wow. Uh, my wife, I. Right there loves commercials, you know, then she'll, she'll watch, she, she watched a little bit more football this year. It's almost one of those things where, you know, the games will be on and we're doing other things. You know, but we'll have the games on the background.
[00:18:38] William Sanchez: Stop once in a while, watch the game depending, right? Because as you know, family, you have other commitments, especially on the Sunday, you're doing all these different things, right? Thursdays, you know, depends, but for her, she loves commercials. I like some of them. I'm more, I critique more gone. You spent all this money for this commercial.
[00:18:58] William Sanchez: This is, so that's where my critique is. I [00:19:00] become one of those people, right? I critique over. I think about the money you spent for this platform that you're doing. Uh, for me, I'm really looking forward to the anthem this year with John Baptiste. He's one of my favorite artists. I think he's a musical, creative, artistic genius.
[00:19:16] William Sanchez: I, I think, uh, he's absolutely incredible. So I want to see what he's going to do with it. If, uh, for fans out there on Netflix, American symphony kind of follows his, his year where, uh, he, he won for the Grammys. He performed in radio and, uh, where am I thinking? Uh, Carnegie Hall. Uh, his wife went to cancer.
[00:19:37] William Sanchez: Like, it's, it's absolutely amazing, but he's, he's one of these, uh, geniuses. So, that's, I'm looking forward to, uh, a lot of it there. Let's talk about some other key injuries. Uh, you know, speaking with music, we, I don't want to get any of the Swifties concerned, you know. No,
[00:19:55] Dr. Grant Garcia: no, no. Be careful with this one.
[00:19:57] William Sanchez: We can easily get canceled.
[00:19:59] William Sanchez: [00:20:00] Easily. So let's just be careful, but let's talk about Travis Kelsey, the all pro future hall of famer, tight end, uh, dealing with his hyperextended knee and bone bruise. He suffered in doing the practice and it said resulted in significant. Uh, does all of that makes sense to some of it go away? You can't have one without the other.
[00:20:25] William Sanchez: What are you some of your thoughts when you hear
[00:20:27] Dr. Grant Garcia: about
[00:20:27] William Sanchez: this?
[00:20:28] Dr. Grant Garcia: So this is a good one. I see this frequently with skiing. So they like land and they'll tweak their knee up or like, you know, they'll fall and they'll go hyper extension. And some people's knees go hyper more than others. He's a pretty big dude.
[00:20:38] Dr. Grant Garcia: So I highly doubt. Yeah. But, you know, he's one of those ones, that's one of those ones where, you know, when you know, when you've seen the players, they get hit and then he goes backwards and everyone gets disgusted. Yep. That's, that's like previous. So this is like one step before that. So thankfully nothing else happened because the back of the knee, the structures in the back of the knee are really stiff.
[00:20:59] Dr. Grant Garcia: There's a [00:21:00] capsule and everything else. So when he hyperextended it, he went like this. and the bones actually in the front click together, which is pretty uncommon, but you can get that and you get a bone bruise in the back in the front. And this can be just like this. The problem is you basically sprain the back of the knee.
[00:21:14] Dr. Grant Garcia: He may have sprained, you know, hamstrings and kind of tweak them a little bit. So that's why it was swelled up a lot. My assumption is that hopefully he didn't do any significant damage, and I don't think he did, or they would have done anything, uh, they're saying no structural damage. Um, so this is one of those ones you'll probably get back, you'll probably be a little bit sore, uh, but I don't think the risk long term is much for this one.
[00:21:33] William Sanchez: So, so the knee is not only, it's not only affecting the knee with that hyperextension, but it's affecting the hamstring? Because it's putting pressure or strain?
[00:21:40] Dr. Grant Garcia: Yeah, well the hamstrings come, the hamstrings, there's a knee joint like this, and the hamstrings come past the knee joint. So those hamstrings and the calf muscles, they go on either side.
[00:21:50] Dr. Grant Garcia: They protect the knee from going into the hyperextension they're firing so that they don't, they lock up. So he
[00:21:54] William Sanchez: doesn't go farther. So when it, so when it happens, he's putting a straight on that. So he [00:22:00] could, so he can actually feel that any risk of. Possibly a hamstring pull or something like that. Is there any kind of, uh, you know, damage or not damage, but you know, a strain toward that hamstring since it was affected by it, or that's not something you really think about?
[00:22:15] William Sanchez: Pretty
[00:22:16] Dr. Grant Garcia: low risk. The hamstring that we, that people usually strain are the hamstring where it attaches in the butt up higher. The lower hamstring which attaches is much less commonly torn because there's mostly tendons down there
[00:22:26] Yeah,
[00:22:26] Dr. Grant Garcia: and so that's going to be a less likely issue, but he could have inflammation right like the calf muscle Higher up is the one that the same thing is talking about the calf strain the calf muscle lower down is the achilles So either it pops It doesn't usually strain.
[00:22:40] Dr. Grant Garcia: It's hard to strain a tendon. So as a result it's pretty, it's a lot less likely that he has a sort of long-term indications from this.
[00:22:48] William Sanchez: Alright, if this eagle's offense is going, going to click, we know a big part of his Saquon Barkley, but. What has made his season so successful now [00:23:00] is the line play, but the threat of jail and hurts running as well, right?
[00:23:05] William Sanchez: So Jalen hurt is his left knee against the Rams. He's been wearing a brace. He's been playing through. We've seen him play. So he's been playing through it. Um, what are some of the concerns and restrictions with that left knee? And I guess we're going on. three weeks or close to a month now. Do you have less concern about that injury and feel like he's going to be, you know, closer to his normal self or is it something like depending on the severity, this could linger a little bit longer and all you need is to maybe not take the right hit, but turn the wrong way on a hit for you to kind of reactivate that.
[00:23:43] Dr. Grant Garcia: Yeah. So again, obviously this is the classic NFL thing. He hurt his left knee, right? Like I looked it up. There's just no way to figure out what's going on. Yeah, it's been pretty, it's been pretty sort of locked down. Um, generally, a hurt knee is like a little [00:24:00] meniscus tear, but I highly doubt that, because I don't think he would have it.
[00:24:03] Dr. Grant Garcia: enough to get by if he had torn his meniscus. The, could it be a little cartilage defect? Maybe, but you know, we all talk about this, it's probably MCL, right? He probably sprained his MCL a little bit, like DK Metcalf did, and he's probably just has this lingering sort of knee sprain thing that he's wearing that brace for, because you don't wear a brace if you have just, you know, if you have just a little bit of like inflammation in the knee, because there's no support there, right?[00:24:28] Yeah. So
[00:24:28] Dr. Grant Garcia: it's probably some sort of ligament sprain. He can play through it. I mean, the concern is obviously if he. Keeps going with it. Can you tear it more? You know, tearing the MCL more is not going to keep him out of the game unless he actually does like a big one afterwards. He could tear something else.
[00:24:42] Dr. Grant Garcia: I think the odds of him considering he's had this for so long and he's been able to play those last couple of games. I mean, everyone's trying to hit him there, right? Like it's not, it's not like it's new for the Super Bowl that he's going to get attacked in this area and he's had two extra weeks of rest.
[00:24:55] Dr. Grant Garcia: So I don't think it's going to affect him too much. But again, it's always that thing about the athlete, like [00:25:00] the big game, his knees, not perfect. Yeah. Does it slow him down, does it tick, right? Like, does he run or pass? Does he run or pass? Is that going to slow him down from the run? He's just going to think about it for an extra second before he goes.
[00:25:12] Dr. Grant Garcia: Is he going all out when you're injured? I don't care who you are. There is definitely this split second thought.
[00:25:21] William Sanchez: Yeah. And, but at the same time, we know these guys built differently. They think differently. They're, they're wired differently. And the fact that he already lost the Superbowl to the, to the chiefs, I'm thinking that he's going to be like, Okay.
[00:25:34] William Sanchez: Um, this is I gotta go for it. He's a tough guy. He's mentally tough, you know, coming from the programs that he did in college and transferring and is still staying the course. So we know mentally he's tough. So I don't be surprised. Staying with staying with Jalen Hurts. I just wanted to read a little note.
[00:25:53] William Sanchez: The last time a quarterback played the Super Bowl with 18 or fewer passing touchdowns in the regular season was Trent Delpher with [00:26:00] the Baltimore Ravens. I'm going back to now to more shame for the Giants because that's the game that the Ravens kicked the snot out of the Giants in that Super Bowl.
[00:26:09] William Sanchez: Dilfo had 12 touchdown passes that season hurts has 18 passing touchdowns, 28 total because he has the 10 rushing. So that would be an interesting stat. Um, if the Eagles win with Jalen hurts. Um, so Yeah, it was just one of those things. I was just curious. I wanted to kind of look it up. We'll wrap up two other key injuries for Kansas City.
[00:26:34] William Sanchez: Uh, Jalen Watson. Uh, he's missed the last 11 games with a broken leg, but returned for the playoffs. What are some of your thoughts about that? And, uh, just kind of describe that injury and maybe what, what you're looking for if you're the, in that room with the medical team when it comes to him.
[00:26:51] Dr. Grant Garcia: I mean, the good news about the broken leg is we've seen this before some of these basketball players.
[00:26:55] Dr. Grant Garcia: There's one while ago that broke his leg in half and had to go straight to the emergency room. They put a nail on it. So [00:27:00] generally gets a nail down it, which is kind of crazy sounding, but he's got a piece of metal inside of there that stabilize them so he can start walking on it. But the good news is generally, if you do it right, you can avoid damage to the inside of the knee, right?
[00:27:11] Dr. Grant Garcia: Like broken bones. Like, so imagine you have your bone, you have your joints, like you have your knee, you have your ankle, and then you got the long bone in the middle. You break the long bone in the middle and it heals. The ramifications are not that bad. The issue is when you start damaging the joints.
[00:27:25] Dr. Grant Garcia: Because the joints are what have the cartilage and you don't want injuries to that. So ramifications for him, he's probably going to be playing pretty well. And now he's got sort of the bionic leg. So he's going to have a metal rod in between there that protects him. I mean, occasionally they can break through the rod, but it's not that common.
[00:27:39] Dr. Grant Garcia: Um, but if I was going to get an injury that bad, this is, and I was, I knew it was going to heal. This is the one to get less, like it have damage otherwise. I mean, it's, it's morbid, but as long as you don't damage your joint, I would never want damage to my joint. The joints, the key, right? That's where the pain comes from.
[00:27:56] Dr. Grant Garcia: He heals his bone nicely, you know, he's got the rod in there. He may take that out [00:28:00] at some point, but it's not a It's a thing I see, you know, every so often people with trauma like ski injuries, and they're able to get back to everything they want to do. So again, a well done, a well done surgery will do very well with you.[00:28:11] Yeah.
[00:28:12] William Sanchez: A key injury for the Eagles, Landon Dickerson, he suffered a left knee injury. I don't know what that means. Maybe you could explain it. Suffered left knee injury, just so generic, an NFC championship game. He was playing center at the time. What, what does that mean? And is this something that you or, or We don't know what it means because it's just so this is,
[00:28:35] Dr. Grant Garcia: this is like, if he's a lineman, it's probably an MCL L again.
[00:28:39] Dr. Grant Garcia: Again, you tear your posterior corn, you tear your ACL, you tear your PCL generally your out for a bit, you know, he's gonna, probably all the lineman wear braces. It's a fun fact.
[00:28:49] William Sanchez: Yep.
[00:28:49] Dr. Grant Garcia: It's one of two things that, so the data has demonstrated braces help for only two things. Skiing injuries after ACL tears and NFL lineman and M MCL L tears.
[00:28:59] Dr. Grant Garcia: So if you see all this [00:29:00] ant those braces because it p the M. C. L. Tears. And s what he got, you know, us are so vague and they don know. Um, but you know, t what he has again. Uh, an those is generally kids t them, doesn't need surger will we brought this up b What you guys may see is all of a sudden, when this whole thing's done, they're gonna be like, Dr.
[00:29:25] Dr. Grant Garcia: Garcia and Will, they have no idea what they're talking about. Every one of those guys got surgery at the season. But, you'll know, I mean, that first week is, you know, when we were, I was looking with the Seahawks and stuff, they, at the end of the week, at the end of that week after the season's over, is like, surgery mania for the, uh, for the sports players, right?
[00:29:43] Dr. Grant Garcia: They all come in and they get cleaned up, they get fixed up. And basically then you're, then you cleaned house and then you focus on getting back to the next season.
[00:29:51] William Sanchez: It's fascinating. And I love. how everything can be just very general, right? Just like, oh, he's got a little bruise. He's got a boo boo [00:30:00] here.
[00:30:00] William Sanchez: He's got a boo boo there. You'll be all right. This hurts. That hurt. Like, what do you mean? What, what happened? Right. You know, if it was one of our kids, but like, no, what happened? Oh, just something happened. Um, before we wrap it up, key player for the Eagles, not playing. Um, one of the Really one of the captains and we'll, we'll see if he's going to retire or not, right?
[00:30:21] William Sanchez: Because he, he had a great season, but we're not sure what's going to happen. Brandon Graham tears his tricep, I don't know, maybe about six weeks ago. What kind of injury is that? And we're just talking about injuries. We know he's not going to play that type of sustained injury for the tricep. He mentioned at his locker room, he was, you know, really feeling emotional about it.
[00:30:43] William Sanchez: And he was like, I knew. what that was. So, so what, what happens there when you take a tricep? What's going on with that?
[00:30:51] Dr. Grant Garcia: Well, first of all, that's a pretty uncommon injury, but we had the player for the giants that tore it twice. And, uh, it was a few years ago, one of the, um, I think it was one of [00:31:00] our tight ends or somebody anyhow.
[00:31:02] Dr. Grant Garcia: So he, or a fullback maybe, but he basically tore his, uh, tricep, um, off the bone and that's the muscle that extends your elbow. That's what gives you that sort of contour in the back. Um, and when you tear that, it's pretty much surgery every time. I mean, unless you really have, you know, have a lot of, you're very frail, et cetera.
[00:31:19] Dr. Grant Garcia: And it's a decent recovery though. And the problem you have, it's like tearing your pec or tearing your biceps tendon. You know, these are power muscles. So this is a long recovery. And again, there is a chance that, I mean, you can get back from that. We've seen it before. It's just that, and again, upper extremity stuff like arms and stuff are much better to get back than lower extremity, [00:31:39] right?
[00:31:40] Dr. Grant Garcia: Because you're not running on them like a patella tendon rupture. We talked about, it's kind of a nightmare, but triceps up here, there's a chance we'll get back, but this is just, could be the icing on the cake. Right. But this is, this is a long recovery and we're talking about six months, nine months to recovery.
[00:31:54] Dr. Grant Garcia: And again, is he ever the same? Does he have the same power? You know, we have a good, we have been repair these really well with all this [00:32:00] fancy things. Um, but nonetheless, it's, it might not be the same, but these big muscle ruptures are a big deal.
[00:32:06] William Sanchez: All right, let's, uh, let's, what, what should we do now? Let's, let's wrap it up before we wrap it up.
[00:32:12] William Sanchez: Let's do a little trivia time. I'm going to try to make it all kind of go, go along the rounds of You know what we suffered through this year with loses Saquon and just seeing him just be the great player that we always thought he could be with the right situation and the Eagles, the way they they protect the way they open up holes just was the perfect storm for the year that Saquon had.
[00:32:42] William Sanchez: Can, do you know who has, and I could take the player's name, I could take the Super Bowl, which is impossible. I would, I would never guess the Super Bowl, or at least a team. What player had the most rushing yards in a Super Bowl game? Can [00:33:00] you think of the team, the player? And I think if, if the Chiefs are going to have, I'm sorry, if the Eagles are going to have a chance at winning the Super Bowl, Saquon may come close to Achieving this record,
[00:33:17] Dr. Grant Garcia: uh, Terrell Davis was it?
[00:33:19] Dr. Grant Garcia: Or
[00:33:20] William Sanchez: is it? Let me see. this is not it. But he, h one point. Oh, that's, th if I even got that close, good. I'll take it. He ha was timmy smith, washington the time. Um, they beat t This is where the Denver on that buffalo bills, lo Oh, to the Giants, like, you know, before they got, uh, Terrell Davis. Uh, Terrell Davis is on the list, but he did, he is not number one.
[00:33:54] William Sanchez: In fact, uh, Terrell Davis. Who's number? Well, it depends, right? They have it by [00:34:00] appearances because the most yards ever is Frankel Harris, but that's over four appearances and I'm starting to get into the woods where nobody's gonna care at this point. So I'll just leave it as this. Um, hey, let's get predictions.
[00:34:12] William Sanchez: Who's winning the game?
[00:34:15] Dr. Grant Garcia: Well, I can tell you what I want. I want a tie. So neither one of them wins. That doesn't work. You can't ask for a tie. Um, I don't know, man. The eagles are just, I know the chiefs have been lucky and they've got a lot of things in their back pocket, like referees, et cetera, whatever you want to call it.
[00:34:35] Dr. Grant Garcia: Um, but I, I don't know, the Eagles look so good. They're pretty untouchable. And unfortunately they haven't, I mean, for me, I don't want to ever root for them, but they haven't had a running back like Saquon. And it's just going to be hard to beat them because when teams struggle, they go to their ground game.
[00:34:51] Dr. Grant Garcia: And that's like their best game right now. So it's just going to be really difficult. I don't know how they're going to be stopped. I don't think anybody's minus the chaos they [00:35:00] had early on. Um, it was not that much, but they haven't been, they've been untouchable. So
[00:35:06] William Sanchez: yeah, they made the,
[00:35:08] Dr. Grant Garcia: they made the commanders look like a joke and they were amazing.
[00:35:11] Dr. Grant Garcia: I mean, no one could stop jayden daniels and they just,
[00:35:15] William Sanchez: yep, their defense is good. They're rushed is good. Um, if they stick to the plan and they don't get cute and they run the ball, the chiefs rushing defense have not been good. The only thing that the really the chiefs has been really good at a defense is Points allowed.
[00:35:32] William Sanchez: They, they, they let you run up and down all over the field. And then they get to that, you know, to that zone, the red zone or whatever you want to call it. And they've done a good job of stopping teams from scoring. I think they were ranked number two, uh, this season in scoring defense. The problem is the Eagles had the number one, uh, defense where, uh, where points allowed and one of the top rushing games, uh, in the NFL.[00:36:00]
[00:36:00] Dr. Grant Garcia: It's a one two comma. That's a problem, right? You can stop one, but you can't stop both.
[00:36:03] William Sanchez: Yeah. And the fact that the Chiefs lost Rasheed Rice, which I thought was a big, big loss for the season really hurt. I know they have some other players to step in, but he was different, you know, different looking player, different speed, uh, different weapon.
[00:36:19] William Sanchez: That said, I'm rooted for the Chiefs. All right. I just, I can't, I can't, I know everybody else would be like, they have chiefs fatigue and I saw a map. It was like, it was like Kansas city root for the chiefs, Philadelphia root for the Eagles. And then it had the rest of the country. It was like, no one cares, right?
[00:36:39] William Sanchez: They care about the game, but they just, they can't root for either team. I can't stand Nick Sirianni. He's one of those guys, but. Like I said, I'm biased. I am a Giants fan. I feel a certain way. I feel a certain way about the Eagles, the Cowboys. We're going to, uh, obviously I'm going to feel a certain way about Washington, especially the way their future looks.
[00:36:59] William Sanchez: So I am just, [00:37:00] I'm okay. I'm happy saying I'm just grumpy and I want misery. It's, it's hard. It's my part of my fandom, right? I'm completely fine with that. So go Chiefs. But my brain says, If the Eagles put it together the way they've been doing all year and just stay the course, they don't have to do anything extra.
[00:37:17] William Sanchez: Just stay the course. They're going to have a great chance of winning this game. Anyway, let's wrap it up. Let's thank everybody. Please check us out at sportsdoctalk. com. We've got episodes, we've got shows, we've got transcripts. If you don't want to listen to us, read about us. It's probably way better than listening to me jibber jabber all over the place.
[00:37:37] William Sanchez: So grab a transcript, check it out. If reading is your thing, uh, We love your emails. We love ideas about future shows. We've had people reach out to us to be guests on the show. So keep it up. Sports. talk. com. Dr. Garcia, any last words as we wrap it up?
[00:37:58] Dr. Grant Garcia: Yeah, lots of fun [00:38:00] stuff coming. We got a bunch of guests already that were going to be lined up.
[00:38:03] Dr. Grant Garcia: We're really excited. I think our issue now is just finding time to get all the guests on. Um, but we want to make sure we get back to some of those things. people like some of the c we talked about. So they in here between these and want us to talk about, le we're open to any topics. this show pivots, you nev show, next show is
[00:38:23] William Sanchez: going true.
[00:38:25] William Sanchez: We hope everyone en sunday and they have a gr Had too many drinks. We got uber. We got lift. We want everyone to be safe and happy. Even if you're miserable because the team that you root for didn't win. It's okay. We want to make sure that you're around so you could roof your team next season. Thank you, everyone.
[00:38:47] William Sanchez: Will Sanchez, Dr Garcia. We're out. Enjoy the game.
Audio Transcript
Urgent Call – Life Saving Cardiac Care with Dr. Dave Montgomery

Urgent Call – Life Saving Cardiac Care with Dr. Dave Montgomery
[00:00:00] William Sanchez: Welcome to Sports Doc Talk. Check us out at SportsDocTalk. com. I can't talk. What is going on with me? I'm a hot mess, Dr. Garcia. Welcome to the show. Our orthopedic surgeon and sports medicine specialist, I am tongue twisting Will Sanchez. Dr. Garcia, how are you? We have a great guest, but before we get to him, how are you?
[00:00:40] Dr. Grant Garcia: I'm awesome. And, uh, sticking with the thing, we have our logo in the background, heart health for Dr. Dave. He's going to love that. So anyhow, I am good. I'm super excited for this guest. Uh, you know, this is going to be, I've been waiting for something like this because again, we've talked about this so many times.
[00:00:57] Dr. Grant Garcia: Bronnie James, DeMar Hamlin. [00:01:00] And we talked about it. I talked to my friends that are cardiologists, but to have a celebrity cardiologist on with us today, that's going to go over all this is pretty awesome. And I think this is a good episode, obviously, to go over everything, you know, we had, we're going to, we had some technical difficulties with this, and this is, this is going to be important for people to see.
[00:01:18] Dr. Grant Garcia: We had to salvage this episode, right? Cause it was, and it was so valuable and honestly, everything Hopefully we'll hear and everything else be so important that we were able to save it. So I'm pumped. There's a lot of work to save this episode, but I really think that the viewers are going to appreciate it.
[00:01:34] Dr. Grant Garcia: So if it's a little different than our other one. Just bear with us. But if you're listening on, uh, if you're listening on the, um, Spotify, it probably won't be a big difference. If you're on the YouTube channel, it'll be a little different. But again, the content's the same. You're going to learn something.
[00:01:51] Dr. Grant Garcia: It's going to be more than you wanted to know about. It'll be awesome. And you might even get a little conspiracy theory on this one. Who knows?
[00:01:57] William Sanchez: Yeah, no, this, uh, just to [00:02:00] reiterate with Dr. Garcia Sand, uh, this is a great episode and that's the reason why we've gone through so much to make sure that you get the information because Dr.
[00:02:09] William Sanchez: Dave is damn awesome and his information is great and we just really appreciate him. Uh, so. As Dr. Garcia said, it's going to be a little bit different. We're going to do some, some segments. We're going to toss to what he's saying, but I think overall the information that you're going to get out of it, you're going to be really, really happy.
[00:02:29] William Sanchez: But before we do that, we know that we have some friends at the recovery shop because we talk about them all the time, all the goodies from the HR robotics and the nice machine and all the other things. But, Let's not listen to me because I'm not the doctor. I just, I use some of the stuff when I'm injured, but Dr.
[00:02:49] William Sanchez: Garcia is, this is his wheelhouse because he's going to let the patients know what they could use from the recovery shop.
[00:02:57] Dr. Grant Garcia: So thank you to our sponsors for recovery shop. You've seen it [00:03:00] before again, for surgeons that want to go take their practice, the next level, their patients are going to come in and ask them.
[00:03:06] Dr. Grant Garcia: Yes, that surgery sounds great. Your techniques sound great. I trust you. What else can you do for me, though? What you're doing is not enough. I want more. And I'm going to tell them this is your option. Right, you have paid, you have this place where you don't have to go online and search for 15 different items to help a patient get back.
[00:03:22] Dr. Grant Garcia: You don't have to go on Amazon and find them something unique that's maybe not even from the United States that they're buying. This is a way they can get the top of the line ice recovery machines. The top of the line from a vending machine standpoint. Scar creams, you name it, all stuff that you wanted your patients to have that you have solidified as a good part of your practice.
[00:03:41] Dr. Grant Garcia: And finally, if you want something that's not on there, it's really nice as a surgeon, you can add it. Again, I get, you know, this is a sponsored show, which is beneficial, but I get no cut for you signing up for them. So, again, I just really wish that all surgeons offer this because if I was a patient, I would want to know like what other options can I do, right?
[00:03:58] Dr. Grant Garcia: Like there's only the [00:04:00] insurance covered standard options and that's not good enough for a lot of my patients. Uh, so it's awesome to have this, this extra thing. So thank you guys. So, again, we're going to sidetrack back into Dr. Dave Montgomery. This is a cardiologist, founder of the Prevent Clinic, executive producer of his own podcast, TV personality.
[00:04:21] Dr. Grant Garcia: I mean, this guy's got it all and you'll see why in a minute, uh, but, you know, again, Will will go after it too, but again, this guy, I'm so excited when we get this opportunity to have him on, you're going to see so many different things. We'll talk, show you his website, his Instagram. Not a bad looking guy too.
[00:04:36] Dr. Grant Garcia: So it's going to be a great combination of things.
[00:04:38] William Sanchez: Yeah, no, it was absolutely amazing and, uh, check him out DaveMontgomery. com amongst his other things. And it was so funny. Uh, you know, we teased about it. It's like, what don't you do? And at the time we did the recording, we were having all this, you know, remember we were talking about the weather.
[00:04:55] William Sanchez: I was like, are you a weatherman? Also? He's like, I do the weather also. So he was just, he [00:05:00] was absolutely great and we appreciate his time. But to kick off the show. Especially with the NBA season off and about and one of the main things that happened on the offseason was with Bronny James and what happened to him on the court when he was at USC before he got drafted to the NBA to play with the Lakers.
[00:05:21] William Sanchez: And Dr. Dave has some great insight on that. Enough from talking about and hearing from us. Let's toss it, toss it over to Dr. Dave. The
[00:05:29] Dr. Dave Montgomery: truth
[00:05:29] William Sanchez: of
[00:05:30] Dr. Dave Montgomery: the Bronny James story is we don't really know what happened and There's a lot of sort of gray area in there, right? He's practicing, this is last year. He's practicing, and apparently collapses.
[00:05:43] Dr. Dave Montgomery: Now, so, you know, Doc, you know this. If you have one of the most common forms of fainting, we call it vasovagal syncope. Fancy words for your brain just shut the lights out because it wasn't getting enough blood. And when you have vasovagal [00:06:00] syncope, everything goes down. So the opposite of the fight or flight system is the rest or digest system.
[00:06:06] Dr. Dave Montgomery: The rest or digest, kind of think about a rest. Everything goes down, you go down, heart rate goes down, blood pressure goes down. But you also get some digestive stuff too. With the rest and digest system, your heart rate can be so slow that if I came up to you, After you passed out on the court and, and checked for a pulse, right doc?
[00:06:25] Dr. Dave Montgomery: Boy, I may not feel one for four, five, six seconds. And you don't have to necessarily have cardiac arrest. If you do that and you're not patient enough, what, what would you do? You would immediately start doing chest compressions, especially because it had been in the news. Everybody's talking about it.
[00:06:45] Dr. Dave Montgomery: You've got arenas in high level sports arenas and practice facilities like that, people are ready to go. What I think the wild card is there, just in that story, is whether or [00:07:00] not they pulled out the AED, the Automated External Defibrillator, and applied it to his chest. Now, if they did that The AEDs are pretty smart, right?
[00:07:09] Dr. Dave Montgomery: I mean, it will tell you if there is a rhythm that is incompatible with life. And it will recommend that you shock the person. So, here's the bottom line. If Bronny got shocked, he had cardiac arrest. If Bronny did not get shocked, you can't convince me that he had cardiac arrest. You just, you just can't convince me.
[00:07:32] Dr. Dave Montgomery: He didn't get cooled, we didn't hear anything. Now, listen. All of this is, is, is roughly speculation because we don't really know much. And it's his prerogative not to talk about it at all. His family's prerogative. Hey, you've got to, you know, protect the brand. I got it. But if he had truly a cardiac arrest and remember the family came out, the representative of the family said he has a diagnosable.
[00:07:58] Dr. Dave Montgomery: [00:08:00] anatomical condition and that it's treatable to the point where he'll be back to play soon. Something like that. You remember this? I, I remember jumping on Instagram as soon as I heard it. I was like, Whoa, this is good. Yeah. So I go back to, you know, the old college cardiology, like textbooks, like. Wait, what condition gives you bona fide cardiac arrest that you have an anatomical condition that is treatable to the point of cure?
[00:08:31] Dr. Dave Montgomery: Now think about it. There are some conditions, and we'll probably hit on some of those, where there, we don't have a cure yet for, for the most common form of some of these, uh, cardiac arrests, the common, the common cause. So I'm thinking to myself, well, what in the world could this be? This is like a, you know, an episode of House.
[00:08:49] Dr. Dave Montgomery: Like, what is this?
[00:08:50] Dr. Grant Garcia: And
[00:08:51] Dr. Dave Montgomery: that's why, and I grab back on those same networks. Um, and, and, and speculated, I [00:09:00] speculated that, in fact, he did not have a cardiac arrest, that he probably passed out, and maybe there, listen, doc, there's so many things, right? Well, you know, there are conditions that you're born with, you have a hole in the heart, the top chamber, bottom chamber, you know, there's electrical abnormalities, right?
[00:09:16] Dr. Dave Montgomery: There are things that you could have that are treatable that will just make you pass out. Um, and I think one of the big gaps that leaves everybody wanting to understand it is because you say, Well, boy, this is happening a lot. Happened to DeMar Hamlin top of the year, then happened to Brawny later in the year.
[00:09:37] Dr. Dave Montgomery: Like, what's really going on? And it just sort of leaves us without any information about, you know, what to do next. How do I protect my kid who's 10? I want him to play ball, but I don't want him to die. On the field of play
[00:09:51] Dr. Grant Garcia: enough of this enough of this. We finally we finally actually want to hear about what Dr.
[00:09:56] Dr. Grant Garcia: Dave does because he went straight into brawny. We know it's a hot topic. [00:10:00] You got LeBron James and his son playing together, but we haven't heard anything about what Dr. Dave actually does. It's minus my Explicit and extravagant introduction of him. But please talk about, Dr. Dave, your passions for the industry, the Prevent Clinic, the Health Mastery Cafe show, all the marketing things you do for heart disease.
[00:10:21] Dr. Grant Garcia: You know, you're a real doctor, right? You don't just play one on TV. So tell us more about that.
[00:10:27] Dr. Dave Montgomery: I'm a cardiologist. I'm a preventive, non invasive cardiologist here in Atlanta. And, um, I recently, six years ago, I guess that's not so recent, but, six years ago I branched off from a very large, um, cardiology and cardiothoracic practice to start my own.
[00:10:43] Dr. Dave Montgomery: clinic here in Atlanta called Prevent Clinic with capital P R E, like defense, prevent. We want to get there before the event happens. The events that we're really, um, focusing on are preventing people from dying from heart attack, [00:11:00] stroke, and heart failure. And we know how to do that, right? And it's not just because Dave Montgomery started a clinic.
[00:11:04] Dr. Dave Montgomery: It's like That's the biology, that's science, that's the current state of medicine. And I just decided to practice in a different way than I was able to practice in a large group and very happy about it. Our podcast is called the Health Mastery Cafe and believe it or not I started the podcast back in 2011 in Chicago, so I was still training.
[00:11:25] Dr. Dave Montgomery: Um, in my last year of training at Northwestern University in, in Chicago. And, um, I, it was, I was struck by, when I was a, a, you know, a second year resident, I was struck by hearing how heart disease is the number one killer far and away, and exceeds all of the common cancers combined. But there are two kickers here.
[00:11:53] Dr. Dave Montgomery: So everybody kind of knows that, not everybody, but most people know that. But the kickers are, we know what causes it, [00:12:00] Grant, Will, we know what causes most of the forms of heart disease that kill people. We don't know what causes many of the cancers. Here's the second thing. We know how to prevent people from dying.
[00:12:12] Dr. Dave Montgomery: So now, somebody's got to tell me, how does a condition, a set of conditions, that far and away kill more people than anything else, That we know how to prevent from killing bit. Why is that still look at? Why are we? Why am I still saying this right now to you on your podcast in 2024? And the problem to me is that we have a marketing problem.
[00:12:35] Dr. Dave Montgomery: We have first, we have a public relations problem, but that's that's the bigger problem, right? That that sort of came out in covid. You know, we really have a PR problem. But the marketing problem, what in the world is going on where we can't get the basic message out to most Americans, most people everywhere, remember heart disease is the number one killer in most of the world, and say these are the things you should do to prevent yourself from dying from heart disease.
[00:12:59] Dr. Dave Montgomery: Now I didn't [00:13:00] say we could stop everybody from developing forms of heart disease. But we know how to stop people from dying. And we know how to help people recover. And so I just decided, you know, way back then, that this, you know, just seeing patients, which I love, do it every day, um, was not enough. That, that, oh, if I can just change one person.
[00:13:20] Dr. Dave Montgomery: No! That's not enough. When are we going to say no? Changing one person's not enough. Changing large, at scale, uh, lives, that's what we really should be doing. And so I decided to go into media, and, and, boy, it was hard. Started off in print media, then I started, uh, then I went to, to radio. We'd do a live show every, you know.
[00:13:43] Dr. Dave Montgomery: Once a week, I was kind of the Dr. Oz of this radio show, so I would sneak off, Grant, I'd sneak off into the call room in the middle of the day on like a Wednesday. Like, where's Dave Fung? You know, Pagers going off, because we had Pagers back then. Pagers are going off, meep meep meep, and I'm on this 30 minute, you know, [00:14:00] call, um, taking it from the call room.
[00:14:02] Dr. Dave Montgomery: And then I started doing television, and then this podcast came along after we had some success with television. And wanting to have long form conversation, you can already tell. Talk a lot, right? I want to have long form conversations, but I wanted to do it in a way that was a little bit more approachable, a little bit more accessible, and not a whole bunch of scientific mumbo jumbo.
[00:14:21] Dr. Dave Montgomery: Like, I've got a bunch of scientific mumbo jumbo for you, but that's not what gets to people. So I started it in a cafe in Chicago. It used to be called Crew Cafe. It's no longer there. And we literally would have two microphones like this and be talking at the table, drinking whatever we were drinking.
[00:14:36] Dr. Dave Montgomery: And that's where the, the, um, the name of the podcast came out. The Health Mastery. I think in order for us to be in this body, we gotta be in this body every single day. We may as well master it. Um, and just do it in a cafe, the Health Mastery Cafe. Boom, there it was. It sounded a little wonky. People told me that was a stupid title.
[00:14:54] Dr. Dave Montgomery: I'm like, I'm sticking with it. It's like Google. Like, who loved Google when they first came up with that title? [00:15:00] Um, but that's, that's it. And so what we're trying to do now is elevate the conversations. into the current topics that people are talking about, because there's a lot of misinformation. Um, and I want to bring conversations to people where they are, without, you know, using a bunch of jargon, um, but hearing people's authentic stories.
[00:15:21] Dr. Dave Montgomery: That's a real common word now in the common parlance, right? Authentic. But that's really what drives people. It's the emotion of story. And that's what we're doing here. We're taking people's stories, their health stories, and extracting keys and tools for mastery. And that's what we do. [00:15:40] William Sanchez: So obviously, you know, Dr.
[00:15:41] William Sanchez: Dave is doing so many different things. Um, we're really excited that he was here, uh, and able to provide all this information. The next segment coming up, he really kind of gets into really his passion, right? And that's screening athletes and screening tests. And he's going to explain in depth. [00:16:00] Why these tests are so important.
[00:16:02] William Sanchez: He's going to go over a bunch of tests, but really highlight three of them. And at the same time, he's going to talk about the lack of marketing. So Dr. Garcia, when it comes to marketing in your field, how important is it? Because. Dr. Dave is going to get into that, but just, I want to know what it is for, for you as a surgeon, why marketing is so important for the patients to understand what options they have.
[00:16:24] William Sanchez: I
[00:16:25] Dr. Grant Garcia: mean, this marketing is, and you're going to hear from them, cardiologists don't do it well, orthopedic surgeons don't do well. The marketing is essential. It's not just essential to get patients into your clinic from a clinical standpoint or surgical standpoint, but it's our most important actually to get your message out.
[00:16:41] Dr. Grant Garcia: And that's what we do this for, you know, this is a unpaid thing that we do. We do this because we enjoy it and we want to get our message out. I want to teach people about these injuries. I want to teach you about these concussions. I want to teach you about these surgeries so they know they exist. They know the protocols.
[00:16:56] Dr. Grant Garcia: So if something they see doesn't seem right and they're like, listen, that does actually [00:17:00] help. I mean, that's what I get a lot of my patients coming in for. They're like, I had no idea this has been an option and that's why I do it because I want to make sure that everybody gets the best possible care.
[00:17:09] Dr. Grant Garcia: And that's exactly what Dr. Dave does as well. It's awesome.
[00:17:14] William Sanchez: Yeah. And besides the, the test he talks about the messaging of why it's important. So people could get more of information, be become knowledgeable. He hits us up with a Demar Hamlin and his thoughts on it. It's a must listen. So I'm really excited to tease what's coming up next.
[00:17:34] William Sanchez: Don't listen to us. Let's go back to Dr. Dave.
[00:17:38] Dr. Dave Montgomery: I want us to come back to the DeMar Hamlin, um, story because I've got a, another angle, but before we do that, the, the message that came out, um, I think was really clear after DeMar had his arrests and he had more than one, um, was that we should be screening our elite athletes at the collegiate level, [00:18:00] at the professional level, period.
[00:18:04] Dr. Dave Montgomery: It is too simple to do a stress test, folks. To do something called an echocardiogram, which is an ultrasound of the heart. And, um, to do a basic, you know, exam in an EKG, right? It's too simple to do that, and it casts enough of a broad net. In the cardiovascular world for that age group to be able to find the commonest forms of sudden cardiac arrest.
[00:18:30] Dr. Dave Montgomery: The most common forms of sudden cardiac arrest would be found in those three things. EKG, echocardiogram, different than the EKG, electrocardiogram. So, EKG, dots on your chest, ultrasound, echo, think sound, ultrasound, echocardiogram. and a treadmill stress test. Most of the ones, the anatomic ones, like hypertrophic cardiomyopathy, HCM, or the electrical ones, like long QT syndrome.
[00:18:56] Dr. Dave Montgomery: We've got a whole bunch of little fancy words, but many of those would be caught [00:19:00] with those exams. Now tell me somebody, please, in our elite athletes that we know are leaving high school and going to, you know, really rigorous sports programs in college, collegiate programs across the country, or from college, and no matter when they're leaving, to professional.
[00:19:17] Dr. Dave Montgomery: Tell me why we shouldn't. Does it, is it the cost? Are you kidding? I would get, listen, I don't even know who to talk to, but I could call Nike right now and boom, I've got a, I've got a title sponsor right there to make sure everybody gets screened. Like, these are not, uh, expensive exams. And it's, the, the point, uh, that you make, Grant, is because you're an elite athlete, you don't think about your health.
[00:19:44] Dr. Dave Montgomery: It's the last thing you're thinking about. Tom, how old was Tom before he said, you know, I got to stop eating this crap. I got to stop drinking this, this getting drunk, you know, the weekend before the game, you know, the week before the game, like it, it, it, it takes an evolved [00:20:00] human being to go there. And I'm not really sure because, you know, I was 22 before I was not evolved at 22 thinking about, you know, the implications for my health.
[00:20:11] Dr. Dave Montgomery: Nobody's thinking about that at that age. You are running faster than anybody on the planet. You're hitting people. I mean, it's just, it's unbelievable the kind of feats that these guys can do, guys and gals, because it's not just guys, for example. But if we don't test, you don't know. That's what I tell patients all the time.
[00:20:29] Dr. Dave Montgomery: You can feel amazing. We all have heard of stories of, of, of marathoners, triathletes. Oh my God, they were, you know, so healthy. But what happened to them? Boom. We've all heard of it. Oh, it's about to cross the finish line. And that's not a myth, by the way. That's not like folk folklore. That's real people, you know, about to cross the finish line and literally have a cardiac arrest before they cross.
[00:20:50] Dr. Dave Montgomery: We've heard of all of that before. Who's healthier than a marathoner? Nobody. So if you, there are some things, and here's the other thing I tell my patients, Grant, [00:21:00] Not everything that can harm you hurts. Not everything that can harm you hurts. Not everything that can change your life instantly will give you a symptom.
[00:21:10] Dr. Dave Montgomery: That means there's a bunch of things that are asymptomatic. And in this group of patients, this group of people, who we really are asking for so much, tell me why we shouldn't be doing it. Somebody, please. Tell me why we couldn't just spend, I don't know, a thousand dollars, twelve hundred bucks, I don't know, less.
[00:21:29] Dr. Dave Montgomery: In my lifetime, I've never seen what happened to Neymar and Hamlet. We've never seen that before. So, truthfully, it is rare, but it should just never happen. That shook the entire world. This is, this is, you know, there are some guys who were sitting on, standing on that field that saw that, that right now Are seeing a therapist.
[00:21:52] Dr. Dave Montgomery: This is far more. This is it's got far reaching implications. This is not just, Oh, yeah, we just, you know, one guy had a cardiac arrest. [00:22:00] These guys are PTSD. You know, how many games did it take them to start hitting each other the same? Like a lot. I mean, we could, we could have an entire movement afoot starting at, at, you know, sort of Collegiate bound high school athletes.
[00:22:14] Dr. Dave Montgomery: Just start with that small Group and just scream those folks because I want people to understand that although it seemed like there's a whole bunch more cardiac arrest We had Caleb White after Brawny and then then before Brawny we had DeMar Hamlin like all of that and it was in the news, but the truth of the matter is Um, kids have, you know, playing, playing sports, have cardiac arrests every year.
[00:22:37] Dr. Dave Montgomery: It's about the same, one in 100, 000. So I would get asked on the news, Hey, is it more common? No, we just had two super high profile, um, examples, super high profile, like right in the middle of a game. Are you kidding? We've never seen that before. And then, you know, the son of the king, I mean, we've never seen that.
[00:22:56] Dr. Dave Montgomery: But the numbers are about the same. I [00:23:00] will tell you that, um, one of the things that I want to say here that I, that I said, I just made a little small, um, Instagram post because there was a, a, I got a lot of questions, uh, when DeMar, Um, with Brawny, I'm sorry, when Brawny had his event, who again, we don't know what happened.
[00:23:18] Dr. Dave Montgomery: And they were saying, well, you know, why is it more common in black athletes? And it just sort of seems like that would be right, because there are a lot of different heart conditions that are more common in blacks than there are in other populations, particularly whites. This is not one of them. And there's a number of reasons to talk about this.
[00:23:39] Dr. Dave Montgomery: Number one, if we're going to start screening athletes, but you think that only a certain population of athletes is affected, what if you don't have that kind of athlete at your school? There are plenty of, uh, uh, you know, uh, schools, you know, great programs across the country, that have zero black athletes, right?
[00:23:57] Dr. Dave Montgomery: So if you think it's only black athletes, you [00:24:00] won't get an AED. You're not gonna screen any kids? Are you kidding me? What's an EKG? What do I do that for? But here's the truth. It all came from an older study when it looked at a five year period of NCAA, um, athletes. This is the only data that we had of this magnitude.
[00:24:16] Dr. Dave Montgomery: And it really was a survey study, a retrospective study. And in that study, what it showed, and I pulled it up, I'm just going to kind of pull it up here just so I can kind of quote right from it. The main graph on the study grant, Um, showed that there were, uh, uh, 45 total NCAA athletes that had, uh, deaths from cardiac arrest in this time frame.
[00:24:38] Dr. Dave Montgomery: Okay, the five year time frame. Here it is. 45 deaths, 11 of them were female. We don't really think females when we think cardiac arrest. It's a quarter of them, they're having cardiac arrest too. Of those, um, 27 of the 45 were white, 17. We're black. [00:25:00] Wait, stop. What are you talking about? It's more. Ah, I see.
[00:25:04] Dr. Dave Montgomery: You have to do a statistical manipulation. Now, I've said on my, um, my little post, uh, grant that the, the larger, uh, public, the society doesn't care about some statistical, uh, manipulation. There were more white athletes that had cardiac arrest than there were black. And we have to say, okay, well, if that's true, that means.
[00:25:26] Dr. Dave Montgomery: White athletes are having a man, but we should just start, you know, when it comes to, uh, a screening, when it comes to preventing it, we got to target everybody. The way that it happened, here's the, here's the bottom line, the way that it happened was the sample size for blacks was so much smaller than whites.
[00:25:40] Dr. Dave Montgomery: And so when they did the rate, right, the death rate, it made it seem like there were more. And the question always is when you have, um, an uneven, non, uh, controlled, randomized control where every, both sides are the same. is if I had more subjects in one side with the [00:26:00] numbers of deaths changed. So here it is.
[00:26:02] Dr. Dave Montgomery: I'm not, I don't want to get too wonky, but there were 300, 000 athletes that they looked at. They call them athlete years, but to make it simplified for, for viewers, 300, 000 athletes, let's call it. Those were 300, 000 black athletes to 17 deaths. There were 1. 6 million white athletes. to 27 deaths. So you see the rate makes it seem like that it's more likely to happen in black athletes.
[00:26:30] Dr. Dave Montgomery: They're just more white athletes that are in this study that are in the NCAA. Okay. So the question always is for people who are being statistically rigorous. What if those numbers were the same? What if there were 1. 2 million black athletes? What would the numbers be? And that's why I said, hey, listen, the, the, the reasons for cardiac arrest, the main and common reasons for cardiac arrest are not more prevalent in blacks than they are in whites.
[00:26:59] Dr. Dave Montgomery: HCM [00:27:00] is not a condition more common in blacks. We know that. Uh, um, you know, long QT is not more common in blacks. ARVD is not more common in black. You get what I'm saying? So, if we're going to be rigorous and we're going to be right about it and not just sort of have, uh, you know, a, um, uh, something for the news, right?
[00:27:21] Dr. Dave Montgomery: Because this is, this has more implications than being sexy and attractive. and pithy for your new soundbite. This is like people's lives. Like who wants to lose their child playing sports? So let's get really wise about this. I see people across all races, across everything you can imagine. Celebrities, not celebrities.
[00:27:41] Dr. Dave Montgomery: You just, you name it. Judges, it doesn't matter. I see them all. And I care about every last one of them. And so I care about their kids. We don't want these kids to die. You should be screening all the athletes that you think are going to go to that high level, whether it's collegiate or pro, and it's easy to do.
[00:27:58] Dr. Dave Montgomery: At the end of the day, we've got to say [00:28:00] cardiologists, people who study heart disease, that's the whole cabal, all of us, we just don't market well. So the reason why it's not on, you know, the radar for the owners association. meetings is because nobody's making no, listen, if we would do half of what Susan G Komen did, think about this.
[00:28:23] Dr. Dave Montgomery: I mean, you got big old defensive ends, man, pink all the way to the boom, pink, you know, underwear, like everything that's marketing. At least you, you've increased awareness of where the people who are involved in it are just so emotionally involved that they don't care about what color That's the marketing.
[00:28:42] Dr. Dave Montgomery: So let's find the Susan G. Komen's for the hard people. I, that's what I think the main things and the main reason is. That we aren't, that we don't see it more commonly now, and that we're still talking about the need for it now is because not somebody else, it's us. And until we take [00:29:00] responsibility and say we're going to do something differently about it, and then go and get some, some, some supporters and, and sponsors to make it as big as Susan G.
[00:29:09] Dr. Dave Montgomery: Komen has done, then we're going to keep having these conversations. I think that athletes get smart when they leave, right? Because I actually do. I see, uh, a lot of former athletes. I see referees, active referees, uh, across sports. Um, and, you know, they come in and, you know, sometimes I have a question. I'm like, man, you know, if we could just get your whole team, because I'm marketing, man, okay?
[00:29:34] Dr. Dave Montgomery: If we can get your whole squad to just get one of these Echoes. Wouldn't that be great? Um, I actually know people in the, in the PA. Uh, you know, the kind of, you know, help run that. Um, men and women in the, in the different player associations. And, you know, it happened to be Patience, right? Um, and I, hey, yeah, you know, when the DeMar Hamlin thing, I wrote something up, boom, slide this over.
[00:29:54] Dr. Dave Montgomery: I don't care who you slide it to, I'm just shooting my shot. I'm shooting my shot. Somebody's got to start [00:30:00] thinking about this. And before I'm done talking and yabbering my, you know, the, the, the, the time when I just hang up my jersey, my podcast and TV jersey, I will have done the best that I could to try to get the message out.
[00:30:15] Dr. Dave Montgomery: I did want to hit DeMar Hamlin if I could, because Um, I, I don't know if people remember, I, I'm, I'm, if you don't remember, I want you to go back to the video. There's a lot of different clips on YouTube. We all were asking the question, what happened to Demar? And it was, you know, just sort of one of the more popular things to say that he had what's called commotio cordis.
[00:30:43] Dr. Dave Montgomery: When you get hit in the heart at the very wrong time and you hit it at a certain phase of the EKG, if you will, the electrical activity, it can throw it into a very chaotic heart rhythm and that chaotic heart rhythm causes your heart essentially to arrest. It [00:31:00] stops beating and you have cardiac arrest.
[00:31:04] Dr. Dave Montgomery: That has to happen with a relatively direct blow to the chest and at the right time. We've seen that in lacrosse. Ssssah! Pow! Right? Hockey! Bang! Right? We've seen that before. If you get Baseball! Yes, okay? If you go back to the hit, Higgins on Hamlin. Speed it up. Go double time. Slow it down. It doesn't matter.
[00:31:33] Dr. Dave Montgomery: Watch every angle. I watched every angle before I got on the news. Every angle, he did not hit him hard enough. That's, think, go, go back and look, I wish we had a clip. He didn't hit him hard enough in the chest in order, and direct enough in the chest. There was one view, guys, that I saw. And it was from over here.
[00:31:54] Dr. Dave Montgomery: Okay. Damar, the helmet of [00:32:00] Higgins, went up and into the jaw of Damar Hamlin. Now let's stop for a second. The jaw is an extension, I don't have to tell the orthopedist, the jaw is an extension of the skull. I mean, come on, he's getting his bell rung, I don't know, a couple, five times a year. He gets his bell rung.
[00:32:21] Dr. Dave Montgomery: When he went down, do you remember what he did? He stood up. Now, Doc, he stood up. He adjusted his helmet and about two seconds later, what did he do? He went down and he didn't. He went straight down. He had lost consciousness. Now, he didn't guard himself. He didn't brace himself. His arms didn't go out and he popped his head again.
[00:32:48] Dr. Dave Montgomery: Now, I know it's not popular. I said it on a whole bunch of outlets. Until proven otherwise, he had traumatic brain injury, right? [00:33:00] He had traumatic brain injury that turned into a traumatic cardiac arrest. We've seen that before. That's not like something new that we just made up. You can have such a traumatic brain injury that you go into cardiac arrest.
[00:33:10] Dr. Dave Montgomery: That's known. And if you think about it, his heart didn't stop immediate. Camoscio Cortis, my friends, your heart is not doing a thing. It's shaking. Pop, and are you going to get up and have enough blood flow to the brain to adjust your helmet? Right? And then he was moving when they first went to him. His legs were moving.
[00:33:33] Dr. Dave Montgomery: You don't move a thing when you've got commotio cortis. Think about it. He wasn't in cardiac arrest immediately. Comotio Cordis doesn't say, let me wait for it, wait for it, boom, let me get, no. That's not how it works. And I know I'm being a little tongue in cheek, but that's not how Comotio Cordis works. So I'm sitting there as a scientist, I'm like, that's not Comotio Cordis, guys.
[00:33:58] Dr. Dave Montgomery: And then, [00:34:00] remember how long it took for the, the um, paramedic to come out and start to, right? I mean, that was a long time. Comotio cordis doesn't behave like that. It's just not biologically feasible. I mean, somebody falls from a high, you know, from a high altitude and lands on the ground, they go into cardiac arrest.
[00:34:16] Dr. Dave Montgomery: Not because the heart got smashed, because it was such a traumatic thing. You get this overload of adrenaline and all the other hormones that make your heart, and you just go into, So we know that this is a real thing. Um, I, I did want to just sort of talk about, um, how he went back into cardiac arrest. So once they got his heart back, which if you get there fast enough in commotio cordis, okay, maybe, maybe you can save him.
[00:34:43] Dr. Dave Montgomery: But to your point, Doc, listen, it's really hard to save him in commotio cordis. Um, they got him to the hospital. And he went into cardiac arrest again. If it were commotio cordis, [00:35:00] he didn't get hit again. He didn't get hit again. Why did he go back into cardiac arrest? Now, you could say there's a number of reasons.
[00:35:06] Dr. Dave Montgomery: Oh, you know, the, the, the fluids, you know, all the stuff. And, and I think that that's feasible. And maybe that's a weaker point of what we're talking about. But when he stood up and, and, and adjusted his helmet, He reminded me of Tagovailoa, when he got his bell rung a couple times, you remember that? He got up, uh, uh, yeah, right?
[00:35:26] Dr. Dave Montgomery: Yeah, I mean, he was like, he was stunned, did that, right? It's this, it was a similar kind of thing. Now, it's not sexy for the NFL to have heard that, but I also said on Tom Llamas, Listen, the NFL is doing the absolute best that they can to try to make this game as safe as possible. We've never seen that before.
[00:35:45] Dr. Dave Montgomery: Come on, it's the first time for everything. It's not like they were like, oh yeah, we don't care about the players. Nobody believes that anymore. We just have never in our lives seen that kind of hit. And guess what? You're not telling folks. Hey, got my [00:36:00] bell rung, right? If you get up and stupor around a little bit.
[00:36:02] Dr. Dave Montgomery: Okay, you got to go on, you know, concussion protocol. But I mean, there are a whole bunch more bells rung than we'll ever know. Right? I mean, think about pop Warner. You don't even talk about it when you're like this big. Um, so it could very well be that that was just the last one that his body could take.
[00:36:19] Dr. Dave Montgomery: He's like, Oh, well, you know, that's not enough. How do we know how many he's had? Through the course of two years, three years, I don't know. I'm really excited about this movement toward body imaging, full body imaging for, you know, the general population, but certainly for athletes. I'm looking forward to AI being, um, dovetailed with the current medical science and turning scans into super rapid, uh, accurate exams for stuff like HCM, ARVD, right?
[00:36:49] Dr. Dave Montgomery: I mean, some of the structural stuff that we can see. That changes people's lives. And then some of the other things, right? Right, Doc? So, you know, I mean, think about if you've got this super fast, uh, you [00:37:00] know, imaging MRI that you don't have to, you know, take somebody way off, you know, across the city to get a really high tech, uh, MRI.
[00:37:08] Dr. Dave Montgomery: And so when it comes to imaging and, and preventive testing, That's what I'm excited about. I can't wait till they get this right so that it's not such a big deal to to have your, um, your college athlete who, you know, is going to the pros to just go to one of these centers, soup, soup, soup, do the test and come out with.
[00:37:28] Dr. Dave Montgomery: Uh, you know, uh, what to do, you know, what not to do, what to eat, what not, I mean, that kind of stuff.
[00:37:33] William Sanchez: I really hope that you, the audience had a chance to learn something, to be excited about it, and really to get some information, you know, as I know for myself, whether it's the Echo exam, the EKG, the stress test, just.
[00:37:48] William Sanchez: You know, I'm getting older and we're talking about it from someone my age, but really the importance of our young athletes that are playing football, playing these sports to have these tests to [00:38:00] find out about DeMar Hamlin. We can't thank him enough. You know, what was some of the key points that that really you took away from Dr Garcia as we get ready to wrap up our show?
[00:38:09] Dr. Grant Garcia: I mean, so many first off, uh, Dr. Dave, thank you for being on here. This was awesome. I mean, just to be able to have someone of your, your caliber. The way you and the way you were able to effortlessly explain this and go through so many different scenarios. I feel like we could have done two or three hour show, but our listeners would probably get exhausted, you know, but, uh, I took away, you know, the brawny dreams thing is fascinating.
[00:38:33] Dr. Grant Garcia: Demar Hamlin. And then just just the points you make about. The ease of testing and how we are under testing because it's, it's, it's a, people don't understand that, right? Like the big glitzy stuff, the sports stuff, the orthopedic stuff that we talk about that gets in the news more frequently, right? We talk about that all the time, but this, these type of tests are actually saved lives.
[00:38:55] Dr. Grant Garcia: Like what I do, I love my job. But I don't frequently save [00:39:00] lives. You save lives, which is awesome. And so that's what the important part here is that we can save lives. It may not be that many with these sort of tests, but even one counts, right? Because anytime someone passes away from something like this, it's all over the news.
[00:39:13] Dr. Grant Garcia: We don't want that, right? We want these people to be saved. And so it's an opportunity to save lives. So thank you again. This was amazing. And thank you to all your listeners. This was well worth it for us to get, get this episode on for you. And, um, I hope you learned a bit.
[00:39:28] William Sanchez: As we wrap it up, just remind everybody, check them out.
[00:39:31] William Sanchez: Health Mastery Cafe with Dr. Dave. Um, the Prevent Clinic, you know, he's at a PreventATL. com because his clinic's at Atlanta. So if you need some more information, there it is. And as always. Check us out. Sports doc talk. com. We have our shows. We get feedback from you, the listeners and viewers, and we love it.
[00:39:55] William Sanchez: It means so much to us that allows us to do other shows. We have [00:40:00] transcripts. We have a plethora of information. Um, it's just been great. And we really appreciate you. Dr. Garcia, last words as we wrap it up.
[00:40:10] Dr. Grant Garcia: Always fun to have a guest, especially like this. So thanks guys. Thanks. I love your
[00:40:13] William Sanchez: background. Dr.
[00:40:14] William Sanchez: Garcia. I just want to say my last time out
[00:40:16] Dr. Grant Garcia: today a little ortho and a little bit of heart at the same time. So,
[00:40:20] William Sanchez: all right, we're out on that one. Thanks for listening. Bye.
[00:40:24] Dr. Grant Garcia: Take care.
Audio Transcript
Injury Insights: MLB’s Road to Recovery for 2025
Injury Insights: MLB’s Road to Recovery for 2025
[00:00:00] Will Sanchez: Welcome to Sports Doc Talk. As you can see, we have Dr. Grant Garcia. I'm Will Sanchez. Uh, Dr. Garcia, unbelievable. It's the end of the year. We're wrapping things up. And before the year was over, we wanted to make a mention, um, of some key injuries, looking at 2025, even though 2024 Major League Baseball season just ended.
[00:00:39] Will Sanchez: But with the winter meetings concluding, So many players out there. If you are Juan Soto, you just got paid, baby. So for life, he's not going
[00:00:50] Dr. Grant Garcia: to be playing anywhere else.
[00:00:52] Will Sanchez: Oh my God. That, that is, that is absolutely amazing. Gary, listen for there's over 3000 division one [00:01:00] players in the transfer portal in college.
[00:01:02] Will Sanchez: Forget football, go learn how to throw a curve ball, hit some blind drives, hit some home runs, go get paid, go get that baseball money is guaranteed. I think, I think I'm gonna start having babies again. You, you have some young ones, maybe, maybe your wife needs to hear this episode and let's, let's get some babies back on, let's get some baseball players.
[00:01:24] Will Sanchez: You're an athlete. Am I starting trouble? I don't know, but there's money out there. I'm really excited. It's a lot
[00:01:30] Dr. Grant Garcia: of money. That's a lot of money. Holy cow.
[00:01:34] Will Sanchez: Before we get to, um, these key injuries, as we look forward to 2025. Uh, for the baseball season holidays, maybe I should whisper us, maybe we should keep it quiet.
[00:01:46] Will Sanchez: Did, did you do your shopping? It's the end of the year. Did, did you take care of the shopping? The kids taking care of wife, taking care of what's going on. This is a safe place. You could tell us, you could tell us.
[00:01:58] Dr. Grant Garcia: Everybody knows that, you know, I'm too [00:02:00] busy to do that. There's no way I'd be capable of physically doing that.
[00:02:03] Dr. Grant Garcia: You know, there's a, my friend sent, my wife sent me an little Instagram ma'am, and it shows this little squirrel. That's like very excited and looking around. It says, that's what dad looks like on Christmas. Cause he's never seen the presents either
[00:02:15] Will Sanchez: messed up. Well, so I do, I do get all those companies.
[00:02:20] Dr. Grant Garcia: I do my best when I can, but unfortunately the, you know, the boss of the house is in charge and there's no way my gift would be good enough anyway, so I might as well just let the boss deal with it.
[00:02:32] Will Sanchez: A smart man. That's exactly what you should do. It's like you pick out what you want, and then I'll go, we'll all be surprised on Christmas morning.
[00:02:40] Dr. Grant Garcia: Yes, precisely. I like it because it's like for me, it's the Christmas as well. I get everything surprised. So it's very nice.
[00:02:46] Will Sanchez: Yeah. And for those that have listened to the show, if you need some travel plans, Dr.
[00:02:50] Will Sanchez: Garcia is the travel master. So you, you will coordinate all the vacations, all the travel, and the wife will take care of all the presents and make [00:03:00] sure that everyone's having a wonderful holiday as we wrap up the year. I think that's a good, uh, that's a good plan right there.
[00:03:07] Dr. Grant Garcia: Absolutely.
[00:03:08] Will Sanchez: All right, let's move on because if not, we're just going to keep going.
[00:03:10] Will Sanchez: I do this all the time. I apologize to everyone. Uh, the Dodgers have wrapped up the world series. Uh, they defeated my Yankees, which was just tough, tough, tough, tough, but you know, they've got a squad. They've deferred over a billion dollars and God knows what's going to happen going forward. But one of the star players on their team got injured and one of the star players, you know, most recognized.
[00:03:35] Will Sanchez: Players in the world. Uh, Shohei Ohtani, he had orthoscopic surgery to repair a labrum tear in his left shoulder, right now his right that he sustained during the world series, uh, while he was sliding into second base. Um, and you can explain this, right? The surgery known as was a Bankart shoulder repair involves reattaching damaged ligaments, the [00:04:00] proper position in the shoulder joint.
[00:04:02] Will Sanchez: So I hear. A very specific shoulder repair. So you got to tell me why it's called that, but also you're using ligaments to put the shoulder back in the proper position. So what happened with this injury and what does this all mean?
[00:04:18] Dr. Grant Garcia: Okay. So, uh, we talked about shoulder dislocations before, but when he slid into the, uh, the base and dislocated his shoulder, basically when you dislocate your shoulder, you're pulling the shoulder out of the joint.
[00:04:30] Dr. Grant Garcia: And there's a suction seal on it called the labrum and I draw this for so many of my patients, but imagine my hand like this. I'll try my best if I can do it. And it's probably gonna be best like this. So there's a suction seal around there called the labrum. He tore the labrum. Generally, when you dislocate your shoulder, it's out the front.
[00:04:45] Dr. Grant Garcia: So front, An inferior, so an anterior inferior tear. That front anterior tear is called a bankart tear from, you'll never guess. Dr. Banhart, he described it first. Genius. [00:05:00] So it's called a bankart repair, but basically repairing that anterior labrum. And there's various versions of this. Trevor Lawrence had a tear like this, but it was much bigger.
[00:05:11] Dr. Grant Garcia: It went all the way around. Remember them bragging, he had a seven or eight anchor repair, you know, there's been, there's been a few of these types of injuries, um, before, but this dislocation pretty much people always ask, how do you know it's torn? You don't even need an MRI to really confirm this. Cause when you have a dislocation, almost always is labrums torn.
[00:05:32] Dr. Grant Garcia: The question is whether he's had it before. Probably not. Yeah, and they did it in the first try. It's probably because now this is interesting. So this is actually the bigger point here. If he's never had dislocation before, it's his first one, right? So fixing it's almost a little bit controversial. Now, there's more.
[00:05:49] Dr. Grant Garcia: We used to tell people and I just had a patient, two patients today that I talked about this with, we used to say you can dislocate your shoulder a bunch of times, who cares? just deal with it. We've talked about this before in the season. You know, the in season [00:06:00] athlete, what do you do with them? Just look at your shoulder.
[00:06:02] Dr. Grant Garcia: But to be honest with you, we're getting more and more data to show that we should really be fixing these patients right away because the longer you wait, you get glenoid fractures like Deshaun
[00:06:11] Will Sanchez: wants and
[00:06:13] Dr. Grant Garcia: lose bone. And then this simple Bankart repair that was done is no longer an option. Um, and so I think they also what happened is it was probably as a result of the timing.
[00:06:25] Dr. Grant Garcia: I think if he dislocated his shoulder in the middle of the season or in the beginning of the season, he would not have gotten surgery, but it's that set classic like NFL thing to, you know, as you hear about the players, you're like that player wasn't injured. And then all of a sudden got surgery at the end of the season.
[00:06:38] Will Sanchez: Yeah. Yep.
[00:06:39] Dr. Grant Garcia: They probably said it wasn't worth the risk. There may have been more to the damage than we thought because it's, it's still fairly aggressive to do it, especially on the non throwing shoulder. Um, the swing in the back by February, I think is reasonable. He injured this in November. Right. Or October, end of October.
[00:06:57] Dr. Grant Garcia: Yeah. Yeah.
[00:06:57] Will Sanchez: It would, uh, yeah, it would end of [00:07:00] October. Yeah. Middle. Yeah. So
[00:07:01] Dr. Grant Garcia: we got surgery. He probably got surgery with a couple of days because he just calls his buddy Alitrosh. Yeah. You know, the one guy, the same guy did his elbow. So he's, he's going to be one, two, three, four months. I mean, usually full return for one of these, you're full return four and a half, five months.
[00:07:16] Dr. Grant Garcia: six, five and a half months. That's back to everything. So his swinging, they said February, probably March, and he'll probably be ready for the season for pitching again. It's his non pitching shoulder pitching shoulder. It will be
[00:07:29] Will Sanchez: his lead swinging shoulder. If as a left handed hitter, right. So, I mean, that is your pull.
[00:07:37] Will Sanchez: Yeah, but that doesn't. There's no concern when it comes to that.
[00:07:42] Dr. Grant Garcia: I mean, his power is going to be from the drive, right? The follow through is important. Yeah. But he's not going to dislocate his shoulder following through with the bat. Especially after one of these. This is a very bad thing for a pitcher.
[00:07:54] Dr. Grant Garcia: But thankfully it wasn't his pitching side. So,
[00:07:56] Will Sanchez: okay. So if it was, yeah, that would
[00:07:58] Dr. Grant Garcia: be, that would be kind of not, [00:08:00] that would not be good. This is coming off an
[00:08:02] Will Sanchez: injury already from pitching as well.
[00:08:05] Dr. Grant Garcia: I mean, the question you have obviously played amazing, but what is the longevity now? This is the third, this is the second surgery on his body in the last few years.
[00:08:14] Dr. Grant Garcia: Granted, obviously this is, You know, unfortunately the part of the game for some of these players, but you know, this is, this is another, another procedure you underwent, you know, it'd be back. It's not, this is not something that's, it's not a small procedure to do.
[00:08:28] Will Sanchez: So, so this type of procedure, if it was whatever the dog days of summer, right?
[00:08:34] Will Sanchez: June or July, if this would have happened and this surgery probably wouldn't have happened, they would have treated something, uh, very differently. Or Because maybe there was a, if there would have been something more severe, then you go, well, we have to go in and fix it and not just be as dismissive as, uh, we're just kind of fixing that labrum.
[00:08:55] Dr. Grant Garcia: Yeah. Like Deshaun wants a type of thing. Um, or there's something called a [00:09:00] Hillsacks legion. So he has a big one of those, or this wasn't his first one. You know, we don't know that probably his first one. I feel like we would have heard about this before. Um, And the, the mechanism was so traumatically generally when people have multiple dislocations, they don't dislocate it traumatically.
[00:09:14] Dr. Grant Garcia: It's like, Oh, I dislocated my sleep. I dislocated like putting my arm over my head. So it was probably his first one. And there was probably a little more damage than we're hearing about. And it's him. He's worth a lot of money. The Dodgers. Oh yeah. They have no interest in him being out next season.
[00:09:30] Will Sanchez: Yep.
[00:09:31] Will Sanchez: They probably made
[00:09:32] Dr. Grant Garcia: a game time decision.
[00:09:33] Will Sanchez: All right. So hopefully he'll get back. Um, unless there's some complications, if they are, we'll be back on here talking about it. So that, that, that's a plus for us then, but I don't know if that sounds a little selfish. It's a pretty
[00:09:44] Dr. Grant Garcia: low risk. It's a pretty low risk surgery and Ella trust does a good job.
[00:09:47] Dr. Grant Garcia: I, he'll be a very low chance of him not getting back.
[00:09:51] Will Sanchez: You have your Atlanta Braves logo behind you and I apologize to any Braves fans, but it seems like there you're some of your best players got hurt this past [00:10:00] season. And if you're a fan of the team, you know that firsthand. You don't need me to tell that because, uh, there were so many key injuries and, uh, that's going to be some NL East race now with Lindor and Soto and with the Mets.
[00:10:13] Will Sanchez: And then hopefully they get guys back. Like Joe humanists, uh, the land of Braves key reliever. He has surgery to repair the cartilage damage in his left knee. And he was, the surgery was performed by, you know, your buddy, Dr. Brian Cole on October 29th, 2024. He's expected to miss roughly a calendar 12 months, um, which is a big blow to, uh, the bullpen.
[00:10:41] Will Sanchez: You know, he had a fantastic ERA at two 62. So. A couple of things. October 29, 2024 is really, I mean, the season's over. So is this something, you know, when, when you hear about an injury like this and when it happened, when you're having [00:11:00] surgery, how the length of it, what do you think that process was? And we're dealing with hypotheticals here, but what do you think happened there with this picture where they realized that he had to go get this repair, the repair, the cartilage on this knee?
[00:11:15] Dr. Grant Garcia: So, I mean, this wasn't, this wasn't a spur of the moment decision. This was probably planned. Right. It's the same thing as what we talked about before is at the end of the season, you have a string of players, you know, you take care of the professional teams that Latin and that week after is like open season, right?
[00:11:32] Dr. Grant Garcia: You got to fix everybody up, get the team ready to go because it's the maximum amount of time for recovery. Uh, so this was a planned surgery, likely, um, you know, nothing we heard about and obviously he wouldn't have played so well if he had been, you know, it had been something had to get done acutely.
[00:11:48] Dr. Grant Garcia: Right. Right. So, it clearly was bothering him enough to get this done. Eight to twelve months is a long time. It's a long time. So, you're, you're looking at probably a more advanced cartilage surgery. Okay. [00:12:00] So, so yeah, break
[00:12:00] Will Sanchez: that down. What do you mean advanced?
[00:12:02] Dr. Grant Garcia: So again, the problem you have with some of these layman terms they put in here is they try to dumb it down so much, um, that unfortunately it's hard for someone like me to really diagnose it.
[00:12:11] Dr. Grant Garcia: Like, you know, the Lonzo Ball thing, we had to hear multiple rounds of injuries. Yeah, this is a bad enough that Brian Cole had to get involved. Yeah, there's some minor more minor procedures that he can do. We've talked about like bio cartilage where you can kind of micro fracture that area and you put some Yeah, some juvenile cartilage.
[00:12:29] Dr. Grant Garcia: There's some newer procedures out there that he may have done for him. Eight to 12 months in my opinion is like a cartilage transplant, which is we talked about with Lonzo ball. So, you know, maybe Dr. Cole is getting more brazen with the cartilage transplants because he now has done a few of them. He did the professional hockey player recently.
[00:12:46] Dr. Grant Garcia: Um, he just did, uh, he did Lonzo ball. And now all of a sudden, maybe this is like, I told you, what did I say in the last, Podcast. I said this could open the floodgates for more and more of these surgeries. So I wouldn't be surprised if he did something like [00:13:00] that, like a cartilage surgery. They may not announce it anymore 'cause it may not be considered hot news.
[00:13:04] Dr. Grant Garcia: Right. You know, I've had a few of 'em in the Yeah, that's in the, the NLB that's, so it's like, oh yeah, he just had a cartilage transplant. No big deal.
[00:13:11] Will Sanchez: Yeah, that's really concerning. Um, Ronald Kuia Jr. He tore his left ACL in May. Uh, he's expected to be out. You know, a couple months of the 2025 season, so that's pretty much almost a full calendar year.
[00:13:25] Will Sanchez: Second major knee surgery in three years. I mean, so what are we concerned about with his knee, with his health, um, and, and maybe what's left in that knee.
[00:13:36] Dr. Grant Garcia: That's perfect. That's a lot. Your last comment was very good. You know, you're gonna, you're gonna get your MD soon at this show. You keep going. So the, uh, So anyhow, so the, the second surgery is to me is always the word meniscus, right?
[00:13:50] Will Sanchez: Yeah,
[00:13:51] Dr. Grant Garcia: probably not cartilage damage. Generally, he gets bad enough cartilage damage. It's less common in these ACLs. When you get it, you're starting to address it or they're having a lot of pain and [00:14:00] swelling and just the cleanups don't work anymore. The ACL tear obviously needed the surgery, but my assumption is he probably had some sort of meniscus tear that they either fixed the first time or they cleaned up.
[00:14:11] Dr. Grant Garcia: So now he's had two major knee surgeries. And we're worrying, is this going to be a situation like you had with Lonzo Ball where by the time you're done with him, he's got minimum meniscus left. That being said, when you have minimum meniscus, it doesn't mean you need to be completely out of the, uh, out of the season or you're done for the, you're done for your next five years.
[00:14:32] Dr. Grant Garcia: Uh, so it's important, um, to understand that, uh, this. this meniscus injury just could be a blip. Obviously, if it goes into cartilage stuff, that's a problem. But from the meniscus standpoint, you know, we'll just have to see and hopefully we all know that when people have these A. C. L. Tears and they're reconstructed, um, the return to sport is good, but the overall longevity of the knee Is, uh, is not as good on when the [00:15:00] meniscus is gone
[00:15:03] Will Sanchez: for those who are wondering what the hell happened.
[00:15:06] Will Sanchez: I had to get my charger as I'm trying to listen to you and I disappear. So it's all, it's all very interesting. Dr. Garcia. Well, you know, the good [00:15:17] Dr. Grant Garcia: news is that I tried to keep talking until you came back.
[00:15:21] Will Sanchez: He's probably like,
[00:15:23] Dr. Grant Garcia: where did he go? I was thinking, I was like, I'm pretty sure I'm done with this. This thing, the podcast is over right now.
[00:15:30] Dr. Grant Garcia: Will's just told me it's time to leave. He just slowly exits the screen.
[00:15:35] Will Sanchez: Just see it. That's how you know, at the end of your episode here, uh, Ronald, we, we really do care about, we're really concerned about your knee. Um, as, as you can tell. So basically what
[00:15:48] Dr. Grant Garcia: we had said, Will was. Meniscus damage with an ACL, not as good of result, definitely a concern.
[00:15:55] Dr. Grant Garcia: There's been lots of data that the time that people go back, this increases the chance of [00:16:00] ACL. We want to save the meniscus at all costs. Not sure his meniscus was saved based off hearing all this stuff. And we don't want to turn into Alonzo ball situation where this turns into cartilage damage. You know, you have a really good young player here.
[00:16:11] Dr. Grant Garcia: Um, so. But again, you know, the age, the age issue with these, uh, ACLs is there's always a little secret stuff in there and you got to figure out if there's anything else wrong and how they're going to do. But generally these guys do well for a while.
[00:16:25] Will Sanchez: What would be your red flag for you? If he gets out on the field next year, starts playing, starts running or swinging.
[00:16:41] Will Sanchez: And he complains of, you know, certain pain, especially if it's not obvious if it's something that, okay, he just, you know, running the outfield or, um, you know, taking a swing and that torque in that lower body area and all of a sudden he walks up, [00:17:00] feels like, yeah, I'm, I'm, I'm kind of feeling something, you know, what's, what's, I guess, what's the next big concern for you now that he's had multiple injuries and surgeries?
[00:17:09] Dr. Grant Garcia: Yeah. I mean, I'm always thinking about his meniscus, right? If it's been trimmed or removed, you know, the ACL, you can get retears. It's just not that common, especially in baseball players. Right. We don't hear about it that frequently that you have someone. reconstruction and then retear. That's more like NFL, rugby,
[00:17:26] Will Sanchez: you
[00:17:26] Dr. Grant Garcia: know, occasionally basketball, but, um, and baseball players, I'm sure can get it, but it's just not as common.
[00:17:32] Dr. Grant Garcia: So, you know, I worry about like he starts to run and he says swelling, you know, all of a sudden you see him going on the DH more frequently, right? Like those are the things that worry me. The deficiency syndrome where basically you get some of your meniscus removed and you get into Alonzo ball situation.
[00:17:46] Dr. Grant Garcia: It's not that common. So I, I don't think he's going to have that issue, but if they fix his meniscus, well, if it's the second attempt to fix his meniscus or save any part of it, that can retear. That's a higher chance that he's going to have a retear of his meniscus. [00:18:00] If he got it fixed, then if he has part of his meniscus removed and he has a problem, it's just a much, it's just a higher percentage, 20 percent or something.
[00:18:07] Dr. Grant Garcia: So we'll see. Um, I think he's probably going to do well, but if there is issues, you know, you worry about his knee long term. I mean, the good news is obviously it depends on, he may be able to change positions if he, you know, up to that, but I think he's going to do well, uh, with just this surgery alone.
[00:18:24] Will Sanchez: Staying with the Braves. Once again, apologize. Braves, uh, Spencer Strider, you had to
[00:18:27] Dr. Grant Garcia: have him up.
[00:18:29] Will Sanchez: Yeah, no, it was just one of those things. And, and it's, it's a thing that we're just, you know, keen on certain injuries and it just kind of happens to be a lot of those players. Uh, Spencer Strider, and I'm going to kind of go back a little bit here, right?
[00:18:42] Will Sanchez: So he had Tommy John surgery in 2019. Okay. In 2024, he had elbow discomfort. Right. It began, he began to start feeling it in spring. He tried to pitch through the pain. So I want to ask you about pitching through pain, [00:19:00] especially when it comes to the elbow area. And then the MRI, uh, showed that there was damage to the UCL.
[00:19:08] Will Sanchez: And then he had surgery in April 13, 2024. He had the UCL surgery with Internal brace, you know how we like that stuff. So with all of the concerns, right, 2019 Tommy John surgery, elbow discomfort, you have the UCL surgery now with the internal brace, which is different than your traditional, uh, Tommy John surgery.
[00:19:34] Will Sanchez: And I want you to explain the difference with that. Uh, by the way, we'll always shout out the, uh, procedure by Dr. Keith Meister. That's a pretty cool name, right? Meister. Um, so let's just kind of talk about. the differences between the UCL surgery with internal brace compared to the regular Tommy John surgery.
[00:19:53] Will Sanchez: And what are some of your concerns and thoughts on it?
[00:19:57] Dr. Grant Garcia: So, um, the first part I'll make, I think for any of the doctors [00:20:00] listening is obviously I'm not sure he actually had a full reconstruction. We'll, um, we have to look at it. Cause if you have a reconstruction, you have no more UCL left there or Tommy John ligament left there.
[00:20:09] Dr. Grant Garcia: So you can't repair it. So I'd, I'd be interested to hear if that was, if maybe he had like some PRP done to it and they thought it was a procedure, um, on his UCL. So we'd have to look, we have to look into that. That's the only thing I'll say from that data that they give that you were given. Um, but, but let's go through the surgery procedures.
[00:20:26] Dr. Grant Garcia: So Tommy John obviously is the first picture that had it done. We've said this before. Yeah. We've talked about Brock Purdy. This is a really big deal and I'll explain to you why. It's not just because of the surgery is because of his status and then what had was done. So this is again, This is doctors breaking surgeons breaking in to the cutting edge material and I'm this is why I told you guys before about new tech we said does do athletes get the new tech right with Dr.
[00:20:50] Dr. Grant Garcia: Liu?
[00:20:50] Will Sanchez: Yeah, yeah, yeah.
[00:20:51] Dr. Grant Garcia: They are much slower to get the new tech because people don't want to test it out, right? Like, yeah. Carlos transplant. I told the. Guys before has been around for [00:21:00] years and we've gotten it better and better and better. And I've done hundreds of them, pro athletes, very few.
[00:21:07] Will Sanchez: And that's why you made a mention about Lonzo ball and how him having that surgery, you know, this new tech opens up the floodgates.
[00:21:15] Will Sanchez: Go ahead.
[00:21:16] Dr. Grant Garcia: So that's where we're going to go with this. So Tom John reconstruction is where you take a ligament from either the wrist, someone with the palmaris, or you take it from the hamstring, whether or not, cause some people don't have this ligament in the palmaris. It's like old cat claw. You can see it right there.
[00:21:28] Dr. Grant Garcia: Yeah. Okay. Some people don't have that. So they use the, uh, ligament in the, in the knee and then you can reconstruction. Now, we've got some newer techniques we're working on, but generally you're talking about a 12 to 18 month recovery. Okay. This newer procedure, which is maybe not even new anymore. It's almost five years old or more.
[00:21:47] Dr. Grant Garcia: Um, we repair the UCL, this tear. And again, certain tears can get this, not all of them. And then we do an internal brace, which is this, this, uh, synthetic suture. We've talked ad nauseum on this and one of Will's favorite, uh, [00:22:00] slogans, um, the internal brace as well. So the, it's a faster recovery. If it can be done, the results are the same as a UCL reconstruction, but you're back in six, seven months, kind of depends on the picture, but it's a much faster recovery.
[00:22:14] Dr. Grant Garcia: Ideally, everyone would do this. When this came out. My number of reconstructions dropped my repairs went up.
[00:22:22] Will Sanchez: Yeah,
[00:22:22] Dr. Grant Garcia: I do more repairs now that I do reconstructions and that's a good stat You should be doing that because there are so many more you can rip There's so many of these you can repair and get the patients back.
[00:22:31] Dr. Grant Garcia: So reconstruction is still has a place but it's not as high But what's really interesting for the audience to hear is that this was done on a pitcher So you hear the word pitcher all the time, but generally before the last few years They reserved this surgery for College pitchers, high school pitchers, little league, not as common pitchers and outfielders and infielders in professional baseball, but not for the pitchers.
[00:22:59] Dr. Grant Garcia: The [00:23:00] pitchers in professional baseball are the highest standard and as a
[00:23:04] Will Sanchez: result,
[00:23:05] Dr. Grant Garcia: the moneymaker. But the same point, do you want to test a surgery on a professional pitcher? Do you want to be the first guy to do a UCL internal brace on a professional pitcher and have it stretch out and tear in the first year?
[00:23:17] Dr. Grant Garcia: Right. It's just devastating. And so for, for, for years, these pitchers were the pitchers, even though other players were getting, I remember when we were taking care of the white socks, you know, six, seven, seven, eight years ago, the outfielder we did it on was like one of the few, our catcher was one of the first ones that got the UCL repair with internal brace, and that was a big deal, but they did not, they had a pitcher tear their UCL and they were like, no way.
[00:23:40] Dr. Grant Garcia: We're doing a reconstruction right now. Professional pitchers are starting to get this surgery because. The surgery works really well. There's been so much data to show that why were we doing reconstruction just because they're pitchers. If it works just as well on other players, there's no reason why a professional pitcher wouldn't work well for.
[00:23:57] Dr. Grant Garcia: So the fact that he's getting that shows that one, the [00:24:00] doctor is willing to push the envelope, which is great. And two, it's not really pushing the envelope because there's so much data out there for it. But this is what the audience should hear. This is a pretty unique thing that, right. That's the first thing I picked up when I heard this.
[00:24:11] Will Sanchez: Yeah. And, and we talked about it before. It's not just. One part of it at that level, right? It's a player, it's agent, it's ownership. It's it's, it's, there's so many factors to where everybody has to, you know, get on board and, and approve it. Um, and then obviously, you know, it'll fall under the player and who knows if there's something in the contract, you know, when they do something like that and say, well, we're, we're recommending reconstruction over repair.
[00:24:43] Will Sanchez: You know, if something happens. So I. Well, and you
[00:24:47] Dr. Grant Garcia: know, no, we're not. I mean, yeah, I know, but it's good. We couldn't, we don't want to go too crazy on this, but you know, like when they go to Ella Trosh, Ella Trosh does what he wants.
[00:24:54] Will Sanchez: Yeah. Yeah.
[00:24:55] Dr. Grant Garcia: I don't, no one tells Ella Trosh what to do, but that's not, [00:25:00] that's not who did his surgery.
[00:25:01] Dr. Grant Garcia: And that's who not to, that's not who does all these surgeries.
[00:25:03] Will Sanchez: Meister.
[00:25:04] Dr. Grant Garcia: And good. I think I, I, I, I think I know him. He's actually a good guy, but the, the point being is that if you're doing a handful of pro athletes and handful of college athletes, and you're the big name in your area, You obviously don't want to push the envelope too much, but also if an agent calls you and they want, when you take care of one of their players, they're going to be like, you should really do this, right?
[00:25:24] Dr. Grant Garcia: Like in the end, the surgeon makes the decisions, but let's be on the pros. This is the whole combination. I mean, frequently we would do the players in HSS, there would be a trainer in the room watching you do the surgery. Like, this is like how, this is how intense the situations are. It's not like, you know, you just get to do whatever you want on these professional athletes, right?
[00:25:41] Dr. Grant Garcia: You, everything's this, this discussion of doing the UCL repair was probably like six opinions in.
[00:25:48] Will Sanchez: It's, it's fascinating, but you know, with someone like Stryer and you know, some of these other pitchers and the Lonzo balls of the world, and we're starting to see, you know, people saying, okay, [00:26:00] let's, let's kind of go this route with some of this, you know, It's not new tech, but it's newer for the, for the, uh, players that's being done on, um, it'd be really interesting because when, once you start to do more, more things like that, and you open up the floodgates to, you know, do other things and present new, you know, new opportunities.
[00:26:20] Will Sanchez: So, um, it'd be really interesting to follow along that case, uh, this summer, and if everything goes well, you know, that bodes well, not for people, two, three years down the road. The season, right? I mean, if they see that this works for, for the pitcher in the season, obviously we know in, you know, people get hurt, there's gonna be a lot of injuries.
[00:26:42] Will Sanchez: And if they can say, Hey, we could get back sooner and not have that major reconstruction and it worked for this player. And we have the same agents or, you know, we're in the same major league baseball, because that's a, that's a small club. We think, you know, major league baseball, a lot of players, that's very few people that are [00:27:00] in that.
[00:27:00] Will Sanchez: So once
[00:27:02] Dr. Grant Garcia: they're all similar. Right. They know they're going to call this one. Who's your guy have, who did yours, right? Like this is, there's so much, I mean, when you have over 700 million invested in a contract for a player, you're going to make a lot of decisions to make sure that the contract keeps going.
[00:27:17] Dr. Grant Garcia: Yeah. All
[00:27:18] Will Sanchez: right. We got, I got two more players here. We're going to wrap up, uh, Walker Bueller, uh, well known pitcher, just kind of go back a little bit. 2022 Tommy John's then he had a flexor tendon repair that, uh, along with. the surgery. Um, so that was done at the same time, but it added to the recovery time.
[00:27:40] Will Sanchez: So I want you to explain why that added to recovery time. And then last year, this past season, he had hip inflammation. Right, right hip inflammation that complicated his return and then he was put on IL and he's kind of had struggles right including the reduced velocity and [00:28:00] They running out of gas getting fatigued So what are some of the things that you're hearing there as I'm explaining this this?
[00:28:10] Will Sanchez: History pattern of injuries with Walker Buehler.
[00:28:13] Dr. Grant Garcia: I mean Unfortunately, we always talk about the players that make it back, but there are players that do not make it back from these surgeries. So this could be just one of those issues. But when I hear the word flexor, that's weird. Now, was it included in the surgery?
[00:28:27] Dr. Grant Garcia: Because in order to do this surgery, you have to attach the flexors at the elbow or do you actually have a rupture of Or I don't think this, I don't want to say this, but did he have some complication during the surgery, right? When you harvest the Palmaris, did you damage another part of the wrist when you did the procedure? [00:28:44] Dr. Grant Garcia: Probably unlikely. Um, but it's very weird to have a flexor tendon tear on top of the Tommy John at the same time. So, or, or did he get it fixed and then it pulled off or when they got in there was a
[00:28:57] Will Sanchez: pair, right? But we don't know what that means between [00:29:00] repairing.
[00:29:01] Dr. Grant Garcia: Did, did he have, did he, when he tore it, did he tear his elbow?
[00:29:04] Dr. Grant Garcia: And then also his flexors. So we had to have that repaired and that took longer to come back. It just, the problem is the Tommy John takes so long to come back from that. I just don't understand how it took that much longer, or I bet he might have complications. Like if you had a flexor tendon repaired in his hand, um, they can get some stiffness in that and then it can not glide as well.
[00:29:21] Dr. Grant Garcia: So that could be another issue too. Anyhow, we won't know, but those are some, those things doesn't bug me. But that's interesting because, [00:29:29] Will Sanchez: because I was thinking about the, the, how even rehab could play a part in that, right. You know, whether if, you know, we have an elbow and we having the hand, the strength and what's not working and, you know, dealing with those things.
[00:29:43] Will Sanchez: So that, that's kind of interesting. Um, the big one for me is, uh, the phenom, the Japanese pitcher phenom, that's going to wind up going to one of these teams, an off season.[00:30:00]
[00:30:05] Dr. Grant Garcia: Will, you're muted.
[00:30:12] Will Sanchez: I don't know how that happened. There's going to be a lot of editing.
[00:30:16] Dr. Grant Garcia: No, don't edit it. Show them that we're normal. I
[00:30:19] Will Sanchez: don't know what happened. I didn't even touch anything. Anyway, so, uh, Roki Sasaki, Japanese phenom pitcher, uh, 2023. oblique injury, right? So that's always interesting. He was limited to 91 innings because of that injury.
[00:30:38] Will Sanchez: Um, that obviously affects the power and rotation and things like that. You could describe it better than me. And then 2024 right arm discomfort. I love these sayings. The discomfort and, you know, these key keywords that, you know, go, ah, there's nothing there, but, you know, right on discomfort, the issue has been a reoccurring problem and the [00:31:00] team had been cautious about the workload.
[00:31:02] Will Sanchez: So when you're having a young pitcher, right, that's about to make so much money in major league baseball, right? They're going to, he's already been posted. Uh, one of these teams are going to throw millions and millions of dollars. He's only 23 years old. But he's had an oblique injury. Now he's had this arm, uh, right arm discomfort and they've had to manage his innings pitch.
[00:31:27] Will Sanchez: What are some of the concerns there, especially for me is, uh, discomfort and the oblique, which is interesting.
[00:31:35] Dr. Grant Garcia: Yeah. I mean, oblique to me, doesn't bug me too much, but you know, the problem with those oblique injuries. It's not that it's not. They can reoccur, but also they're just hard to treat. Right. We just, there are very few people treat them.
[00:31:46] Dr. Grant Garcia: If you tear the oblique, you can get it fixed, but it's just not that common. So generally it's just something you kind of deal with. Maybe he had treatment, maybe rested it. And eventually I'm assuming,
[00:31:55] Will Sanchez: but they can linger, right? I mean, like a mid has had, um, like we've seen [00:32:00] players that they've had.
[00:32:02] Dr. Grant Garcia: Remember LeBron James is growing for like an entire season. I mean, these, these injuries let linger for months until you stop playing. Right. So he had to take a break probably to get the thing down and eventually it probably calmed down, but it's a recurrent, just strain. Right. And they're, they're torturous, but.
[00:32:20] Dr. Grant Garcia: At the same point, it's not something you need surgery most of the time. So he got over that. I'm not as worried
[00:32:24] Will Sanchez: discomfort for a 23 year old
[00:32:27] Dr. Grant Garcia: that, that could be again, is it the words or is it real? Right? We all talked about this. You've seen these amazing ways. They write up like partial sprain of the Tommy John, right?
[00:32:39] Dr. Grant Garcia: So generally arm discomfort is pretty common in baseball players, right? From even a young age, you know, I see them frequently. They come in, they think they tore the Tommy John. They didn't, you know, it's a flexor strain. So this is a recurrent flexor strain. That's fine. The problem is You know, the MRIs are only so good for seeing the UCLs or the Tommy John [00:33:00] ligament.
[00:33:00] Dr. Grant Garcia: So is he having attritional partial tearing of this and not able to see it on the MRI? I'm sure he's getting the highest quality. I'm sure they're watching him like a hound. Every team that's going to, uh, recruit him is probably going to get a new MRI on him.
[00:33:14] Will Sanchez: Oh, the medicals.
[00:33:18] Dr. Grant Garcia: Yeah. You don't want to be, he's going to have more MRIs than any of any of us have had in like a month.
[00:33:23] Dr. Grant Garcia: As he starts getting his final contract stuff because every team is going to want their own, right? So to be honest with you, he's probably going to be fine if a team signs him. They've done a lot of diligence on this, but it does bother me that, you know, now he's got two injuries. We've seen it. It's just, unfortunately it's the nature of the beast.
[00:33:42] Dr. Grant Garcia: And this is a, maybe this would be another podcast would be great. What makes a player resilient and what makes them not. It's just bad luck. Sometimes, you know, you have these players that are phenomenal and all of a sudden they just get injured. They get injured, they get injured, they get injured, and then they're just done.
[00:33:58] Will Sanchez: Yeah.
[00:33:58] Dr. Grant Garcia: I'm not saying it's the case, [00:34:00] but you have some of these players that are just like, never, they never get hurt or they just keep bouncing back. I mean, how many injuries did Tom Brady have? And he just kept popping back and he had a couple of bad ones, right? Like you just, that'd be a great topic to be like, what's the difference.
[00:34:14] Dr. Grant Garcia: And Answer is sometimes it's not. Sometimes it's surgery. They had a surgeon go as well, but sometimes it's just bad luck. I mean, you talked about Walker Bueller and his issues, right? He's had three injuries in a very short span, still not back. And the problem is the longer you're out. The harder it's to get back no matter how good you are.
[00:34:34] Will Sanchez: Yeah, that makes, that makes sense. And then you could be, uh, someone maniacal, like a Ronnie lot where you don't wanna miss a game, so you're gonna cut off your finger because it's, uh, you know, dislocated and broken and you, you're supposed to miss the rest. I just, Hey doc, Dr. Garcia. Just, just, just cut it off.
[00:34:50] Will Sanchez: I gotta, I gotta play in the Super Bowl. I just, just cut it off. I don't, it's, I, I got nine other fingers. These, they're built different. These people built different. So we talk about all [00:35:00] the time. Anyway, we'll wrap it up. I hope you get a great presence. I know we're going to do one more end of the year kind of recap on 2024, which should be a lot of fun, but for the holidays for you and your family and the little ones running around, not destroying the Christmas tree or anything like that.
[00:35:21] Will Sanchez: Or if they are just like, leave them. It's okay. Whatever you buy another one next year, just take it out. But, uh, I wish you guys the very best. Um, and, uh, I hope you enjoy the holiday. I hope you get some time off. Which I know this time of year where everybody's trying to get, get in their surgeries before they deductible start to, uh,
[00:35:40] Dr. Grant Garcia: I'm going to be operating until, uh, until January one.
[00:35:43] Dr. Grant Garcia: I've decided I'm not going to leave. I should, I'm doing this podcast for my OR.
[00:35:47] Will Sanchez: Yeah. Yeah. Yeah. You're doing that. So am I, I'm just, I'm, I'm in the next room. I'm scrubbing up. I'm getting my internal brace ready. I get all set up. [00:35:57] Dr. Grant Garcia: Well, happy holidays to your family and happy holidays to [00:36:00] all the listeners.
[00:36:01] Dr. Grant Garcia: We're going to have another end of the year episode, so it's not our final one. Um, but this was a good one just for the, for everyone to hear about it. And there's brought up a couple of good topics. I think that, you know, what are these injuries about and why do some people bounce back from injuries better than others?
[00:36:16] Dr. Grant Garcia: You know, there's a psyche thing. We've always wanted to have a psychologist on this show. And at some point we will, uh, when we can find the time to find somebody. Um, but. You know, happy holidays, everybody. Thanks again for listening again, follow us on all of our different ones. You've seen, we've had some shout outs on LinkedIn recently, um, with some topics.
[00:36:33] Dr. Grant Garcia: So this is exciting. There's a lot of momentum building. So thank you
[00:36:36] Will Sanchez: all check us out. Sports doc, talk. com for more content, uh, great information, transcripts, and, uh, we'll appreciate you. And I don't know about that. Bringing in a psychologist or something like that. I'm going to be in tears and the episode is going to get messy, but whatever.
[00:36:52] Will Sanchez: Thank you everyone. Bye guys. Audio Transcript
Spine Injuries and On Field Protocols
Spine Injuries and On Field Protocols
[00:00:00] Will Sanchez: Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon, sports medicine specialist, say that a bunch of times, Dr. Grant Garcia. Dr. Garcia, look, man, I don't know if you can see, man, I got my, I'm hanging with my gnomies because it's the holiday season. I know we're going to talk about our injury spotlight, um, but you know, we're just, we're just, we're I can't believe it's the end of the year and it's, uh, it's been a great year.
[00:00:45] Will Sanchez: I want to throw that out there. It's a, it's always a pleasure working with you and, uh, and doing these shows. So, um, how are you?
[00:00:53] Dr. Grant Garcia: I'm good. No, it's end of the year. End of the year for some people is like, Oh, Christmas is coming. End of the year for me means that. [00:01:00] I work as many days of the week as possible because the deductible season is not done until December 31st.
[00:01:06] Dr. Grant Garcia: January though is great. January is usually a lot chiller. Yeah,
[00:01:10] Will Sanchez: that's a lot chiller. So, so can you get a t shirt that says, you know, Mr. Deductible or something like that? Like just wear it in December? I don't want to
[00:01:19] Dr. Grant Garcia: make it about the deductible, but patients come in just absolutely begging to get it done.
[00:01:23] Dr. Grant Garcia: They're like, I've had my, my Farris surgeries, my family's other surgeries. Now it's. free. So I want to do it now. Nice. In January, it's not. And I'm like, okay, well, you know, unfortunately we waited all year to decide on this, but nonetheless, we got to get them done. So we're going to stay busy, but we still have time for the podcast because we have way too much fun on the show.
[00:01:45] Will Sanchez: Too much fun. Listen, I see you have your Miami Dolphins background. And wait, and before that, let's give a little love to our peeps out here. Because you know, when we're trying to recovery, where do you need to go? The recovery shop. [00:02:00] Dr. Garcia, tell us about the recovery shop.
[00:02:03] Dr. Grant Garcia: Big thanks to our sponsors.
[00:02:05] Dr. Grant Garcia: We've had this, you know, repeatedly on here. They've been great sponsors of the show and I love talking about them. I mean, it keeps coming up my patients, right? So your patients, they get high quality surgery. They want, they expect the best. And they, after surgery, they're like, what else can I do? Right?
[00:02:19] Dr. Grant Garcia: Like I got this surgery. You talked about all these fancy things. You've talked on this show, internal bracing, you name it, but I want to make sure that I have the best recovery. So yeah. On there we have, uh, nutrition supplementation, which is all over the internet and one of the hottest topics. We have the Nice Machine.
[00:02:36] Dr. Grant Garcia: We have new braces. We have the ReBliss for some of the patients who are having a more complicated knee surgery. That's pretty
[00:02:41] Will Sanchez: cool.
[00:02:42] Dr. Grant Garcia: Yeah, and the patients can get this and it's a, it's easy. The patients have been thrilled with it. I mean, we have patients that had issues with snowstorm deliveries and they made sure that they overnighted these products for them.
[00:02:52] Dr. Grant Garcia: Um, and my patients love it. Again, there's no cut from me for you signing up for this. The key here is just to give information for [00:03:00] surgeons or patients. If you did a surgery done and you want something like this, talk to your surgeon about using this opportunity because it's a really nice opportunity.
[00:03:07] Dr. Grant Garcia: It's beneficial for all parties. Um, And again, the goal is for the patients to get the best. And sometimes it's hard to get the best just insurance alone. So this opportunity is great. Reach out to Mike at recovery shop. com. He's all over the website. A fantastic group to work with a strongly recommended for any surgeon who wants to, to offer patients a little bit extra.
[00:03:28] Dr. Grant Garcia: So thanks guys.
[00:03:29] Will Sanchez: Yeah. Once again, Mike B at shop dash recovery. com for more information. And uh, that's what we're doing here today, right? We're providing everyone with a little bit more information. We were watching, um, you know, NFL Sunday, right? NFL football. There's only so many weeks left. It's a sport that we love.
[00:03:48] Will Sanchez: that we're into, but we also know it's a sport that is dangerous, that we have severe injuries in there. And, uh, unfortunately, once again, a Miami [00:04:00] Dolphin has sustained a concussion. Mike DuBose, um, you know, catching the pass across the middle, getting hit and pretty much laying there. Obviously, um, There was a lot of concern.
[00:04:14] Will Sanchez: And as the doctors that go out there and we think about these head injuries, right? And you're like, okay, well, he got hurt. There's a head injury. Um, unless it's super, super serious. We usually don't see the cart or stretcher being, you know, called out, you know, they go into the blue tents. then eventually maybe get, you know, back into the locker room, things like that.
[00:04:37] Will Sanchez: But for this situation, that wasn't the case. So they came out and they brought out the spine, uh, the boarding. So while we, we wanted to talk about the importance of spine boarding in these situations. Um, so while we start with there and Dr. Garcia, just explain a little bit, like what's that procedure, right?
[00:04:56] Will Sanchez: You, you have to play it there. You have concern [00:05:00] and. we don't really think about spine boarding when we think of concussions. So tell us a little bit about what happened and how did they get there?
[00:05:09] Dr. Grant Garcia: Yeah. So, I mean, you can watch the videos. It was, uh, it was pretty atrocious looking in terms of the hit. You see the head cock back and then you see him go down and you see a posture position and then you see very limited movement of the arms.
[00:05:21] Dr. Grant Garcia: Now, again, this is just what they showing, right? They pull away from the athlete once they're injured. Yeah, and then the medical team comes in. So we're not really getting to see that much from someone who's recently had to spine board a patient on the field. I can tell you that you don't just start pulling the spine board out just for fun.
[00:05:39] Dr. Grant Garcia: It's a pretty serious situation you're concerned about. I will tell you this is like, it's When in doubt, spineboard. Okay, so that's the number one thing I'm going to tell you. It's just like when you learn in lifeguarding, right? I was a lifeguard when I was a kid. You know, if you're concerned about, again, they were probably, they were not initially concerned about a head injury.
[00:05:57] Dr. Grant Garcia: I'm sure they were, but that's not why they [00:06:00] spineboarded him. They spineboard him because they're worried about a neck injury. And they worry about a spine injury. So the board is for the spine to keep it straight. So really what the key is, is if you think there's damage to the spine, either the bones or the spinal cord, which we've all talked about, those are the worst possible football injuries we can think of.
[00:06:19] Dr. Grant Garcia: Um, you don't want any movement of that spine. So you need this board to be on there and then you need to be able to find a way to strap them on there. Now, this sounds really simple. Right. You slide the board on, move them. It's not so simple to move a 240, 250 pound human being who has completely gone limp or is not moving, whether or not they have a real injury and actually get them on the board.
[00:06:42] Dr. Grant Garcia: So there's actually a procedure and you've seen, I will give you examples. So I take care of a high school team, right? Mercer on high school. I've been there now for six years. We've had injuries on the field. And in one game, I had a spine board, two players. No joke. [00:07:00] It's a traumatic thing for the players.
[00:07:01] Dr. Grant Garcia: It's very traumatic for the, for the field. Obviously the worst is for the player. The
[00:07:06] Will Sanchez: parents also, right? The parents. For
[00:07:08] Dr. Grant Garcia: the parents, for the other players and for the stands. I mean, as soon as I spine bore these patients, there was concern to the players that died. There was concerns of the players, you know, they paralyzed and So, but you have to do it, right?
[00:07:22] Dr. Grant Garcia: Because you're concerned about it. So in both those cases, the players were not moving their legs or said they had severe back pain and they couldn't move. So you have to spineboard them. So that's the same thing that happened here. Thankfully in mine, both players were okay. And I will tell you that probably a majority of time that we spineboard the player, the player, a person is okay.
[00:07:41] Dr. Grant Garcia: Um, but there are definitely instances where it's not. We've seen this on the news. You've, we've talked about this before with players getting paralyzed, but here, They thought there was something wrong with the cervical spine and so they got a spine board. The key is you don't, you imagine when you're rolling somebody, their whole thing is they're going to hold collapse, right?
[00:07:58] Dr. Grant Garcia: So you got to keep them on. [00:08:00] But now there's the catches here. He's also got a helmet on. So how do you get the helmet on without bending the neck? Or extending the neck. Okay. That's the first part. So they have to take off the face shield, which they did, right? That's they can see, make sure he's breathing.
[00:08:14] Dr. Grant Garcia: Sometimes it would take off the guard and the actual helmet. And sometimes you have to sneak in there. The other thing is you want to keep the airway open. So if they're worried, he can't breathe. They're going to have to elevate the chin so that he can breathe and put a mask on him. And I know they brought out the oxygen for this as well.
[00:08:29] Dr. Grant Garcia: So this is not a joke with there. This is not an exercise. Yeah. Yeah. And,
[00:08:32] Will Sanchez: and they also hooked them up to EKG. So he was hooked up to EKG and, um, I, I'm obviously do not have the experience you do. Um, I do have my certification WFR and the wilderness, uh, certification and talking about how, um. You're stabilizing.
[00:08:51] Will Sanchez: You have that person right behind the head behind them and stabilizing the neck. And they're like, do not let go [00:09:00] of that head. You're and you are
[00:09:01] Dr. Grant Garcia: like in charge.
[00:09:02] Will Sanchez: Yeah.
[00:09:03] Dr. Grant Garcia: Like you are the most important person. So our average number of people for a spine boarding is five. So when I did it, we had five EMTs and two surgeons there.
[00:09:11] Dr. Grant Garcia: It turns out my buddy, Dr. Wayne, while I was also on the field, we had to do it together. Um, but you know, You get in there, players either not conscious and or players can't speak right and or players as they have numbness and tingling or back pain. The first thing you do is check it out. The second thing you do is if you're really worried, you're going to put them on the spine board and you're going to take them away to the hospital.
[00:09:34] Dr. Grant Garcia: And the reason is you want to get that CT scan, the cat scan of their neck and spine to double check for any breaks. If they have to do an urgent MRI, they will many times on the way to the hospital, the decrease in anxiety for the player, the calm situation of being on the spine board and or the amount of time from the injury.
[00:09:54] Dr. Grant Garcia: Most of the time, the real symptoms will either subside or still be there, right? So that's the biggest [00:10:00] concern. There were some other things that you mentioned when you initially texted me yesterday about this injury that were, that's pretty alarming for the people watching. It's cutting off all the pads.
[00:10:10] Dr. Grant Garcia: Right? You don't get to see that that often either. Like, how often do you see a player leave with no shirt on? Right. I thought it
[00:10:16] Will Sanchez: was something else. I was like, Oh my God, are we, you know, we dealing with something, a Demar Hamlin situation, right? And you know, and you know, I'm going to tease an episode that's going to be out in about another month.
[00:10:28] Will Sanchez: So with us and Dr. Dave and Dr. Dave was concerned not only about the heart, but maybe this was more of a traumatic injury to the brain. Anyway, I digress a little bit.
[00:10:39] Dr. Grant Garcia: You don't digress though, because you're right, this is some, this is a similar situation. He had an EKG tested, maybe for arrhythmia issues when he got hit.
[00:10:48] Dr. Grant Garcia: Similar thing to tomorrow. He had, he had the spot. So the reason they cut off the pads is so we can check the back of the neck and it can check the back of the player because you want it. [00:11:00] The first thing you do is you, the back of the spine has a lot of points on it and you want to feel those points because if any of those are tender, there's a concern that something called a burst fracture, which is not good, but basically it means That the spine is like a hole in it, right?
[00:11:13] Dr. Grant Garcia: So your cord can go through there and then surrounds by bone. When you have a burst fracture or crack, you can have a crack and it can go into the spinal cord or it can be unstable and that can cause a shift, which would cause spinal cord damage. So that's how we're checking for that. And so all those things are important.
[00:11:29] Dr. Grant Garcia: So when I did one of these players, he kept complaining that I was hurting his back when I was touching him and I'm not touching the muscles. I'm touching right on the bones. That to me is spine board. Don't, you know, get them over there. Do all this stuff like so they probably checked his hands. They probably checked himself and he's like, I can't feel my fingers, right?
[00:11:44] Dr. Grant Garcia: Cause he had just gotten hit. So he's just totally out of it. Yeah, he may not even been conscious. He may have not been able to say anything. He may have been limp and completely knocked out. That's what, that's what
[00:11:54] Will Sanchez: it looks like. He did not look, there was that slight movement, but it looked like, you know, [00:12:00] that could be also from the falling and he [00:12:03] Dr. Grant Garcia: basically got, he basically got KO'd boxing style and that's essentially what happened.
[00:12:08] Dr. Grant Garcia: Um, and so, you know, they don't know what to do with this right now. So this is split second decision. And I think that the, the, the part that I really like about this is that this was the safest bet to do. And when in doubt, you do that. So you've done your, so let's say you've taken your helmet off. Now you're starting to get off the head.
[00:12:23] Dr. Grant Garcia: Now you do, again, the hardest part is the roll, right? You have five people, you need to roll a 250 pound monster. I mean, the kid I did was about the same size as him. So I don't understand. It's, it's not easy. You roll them off, you slide the pads out, you're getting the back feeling, and then you're putting them back on the board.
[00:12:38] Dr. Grant Garcia: And then you got to slide them onto the board. Now, again, none of this, you want any movement of the spine. So it's a lot harder than it sounds, and it's good to have a concerted effort, but it's amazing when you get a team that, you know, we had four EMTs, so they were just like, boom, boom, boom, boom, boom, and they took over in terms of how to move, like these guys just do this all the time, and they're really good at it, and [00:13:00] that's essentially what they're, I mean, the team position wasn't leading the spine boarding.
[00:13:04] Dr. Grant Garcia: That was the ATCs on the field and the EMPs that were there, uh, to do that. So,
[00:13:09] Will Sanchez: yeah, the team physician would go with them. Is that something, you know, when he gets in the ambulance or is his responsibility to stay with the team and somebody else from the team goes with them and reports back of what's happening?
[00:13:24] Will Sanchez: What's normally that's,
[00:13:25] Dr. Grant Garcia: that's an excellent question because that is brought up a lot. And that's really hard when you start to be a team physician, you don't really understand like where your place is, right? Like as a doctor, if I'm on, if I'm like doing surgery, I would never like leave my patient, right?
[00:13:38] Dr. Grant Garcia: And go somewhere else. But at the same point, You have to because your job is to come after that plays done. He's got 52 other guys,
[00:13:46] Will Sanchez: right?
[00:13:48] Dr. Grant Garcia: Yeah. Or you, and you have all the entire field you have to take care of. So as a team physician, what you do is you pass it off. So you're basically the EMTs go there.
[00:13:56] Dr. Grant Garcia: And I, and like the same thing happened to me when I'm in the high school game. [00:14:00] Right? Like I'm like, okay, send the player to the hospital. And then I will, if there's an update, they'll have my number. They can call me. Usually the trainers will update me as to what's going on. But once they're kind of at the hospital, they've got the appropriate emergency room care.
[00:14:12] Dr. Grant Garcia: So the same thing happened there. They probably called, had the hospital get ready. Then he went straight to the emergency room. He probably had all the testing done. And it sounds like he's doing really well. So this is really good news. Obviously wheel brought up at the beginning, head injury. But if we had had this discussion last night, that's not what we've been talking about because this is new information, um, from the last 24 hours.
[00:14:33] Dr. Grant Garcia: But it's important for you guys to the, the listeners to hear this. Cause this is not just. Orthopedics is his team position. Um, at any surgeon or person, resident ATC that takes care of the team position, you need to know how to spine board and you need to know the threshold to do it. Um, like I said, I've been covering these games for six years plus fellowship plus residency, and I've only had a spine board a couple of times, [00:15:00] but when it happens, it's, You gotta make the decision, you gotta be becoming more,
[00:15:04] Will Sanchez: it's becoming more of the norm because you know, we, we see it more now.
[00:15:10] Will Sanchez: So I wonder what's the standard? What are those conversations? We know, especially at the high levels, I'm pretty sure in NFL College High School, you're involved with high school, have these conversations, especially in the off season of going into a new season saying, hey. When we have these type of injuries, we're always going to caution on the safer side because we're seeing, you know, players treated in this manner.
[00:15:34] Will Sanchez: You know, it's not going back to like the Dennis Bird days where they're just laying there and it seems like people are not sure what to do. And, you know, now it seems like there's a plan, you know, what's that checkpoint system, right? You mentioned, do you have feel in your hands? Do you know what, what's that process when you go in there and you're saying, Oh, wait a minute.
[00:15:54] Will Sanchez: I see one sign. And let's, let's do this.
[00:15:58] Dr. Grant Garcia: Yeah. So obviously there's [00:16:00] the big red flags, which we talked about. There's the consciousness, things like that. So obviously those have not changed, right? Like what you look for has not changed in the last 20 years. But what has changed is technology, information, social media, right?
[00:16:13] Dr. Grant Garcia: Like, yeah. If there's a delayed response on the field, that doesn't look good for anybody, right? It's just, it's just serious there. We don't know. I don't think of, and again, I, I hope obviously this is just my opinion or what I've seen. So this is definitely not 100. This definitely hasn't been fact checked,
[00:16:28] Will Sanchez: but
[00:16:28] Dr. Grant Garcia: I haven't seen an increase in.
[00:16:30] Dr. Grant Garcia: Issues with delayed responses from the NFL, right? We haven't seen a part of players that have had like that have died. They weren't taken care of. I mean, if anything, we talked about to Mary Hamlin is like a stroke of a stroke of pure amazement that they were able to get on the field that fast and take care of that.
[00:16:45] Dr. Grant Garcia: So, and nothing but accolades for all the, the secondary, uh, you know, uh, the EMTs and everything else in the ATCs on the field. So what I have seen is probably an increased response time, like you said. So there's just more speed to get there. Yeah. And probably [00:17:00] from Damir Hamlin and other, we talked about this with Dr.
[00:17:02] Dr. Grant Garcia: Joe Liu, you know, the entire team probably has extra checks. And I would imagine from some of these more serious injuries, Bronny, Damar Hamlin, and other players that we've seen, that there are probably an increase in what they're going to start doing stuff. And they're, you know. We've seen really bad injuries and note and everybody knows that like sometimes response time is really important with any of these things So we've just probably seen and we're also now looking for it more will but I would say that I do I do think that they have that the checklist for these injuries has probably increased and there is with Litigation increasing with NFL lawsuits, which we saw talked about with dr.
[00:17:40] Dr. Grant Garcia: Liu.
[00:17:41] Yeah,
[00:17:41] Dr. Grant Garcia: you know But there is no doubt in my mind that all of that has helped persuade people to do things a little bit more aggressively
[00:17:49] Will Sanchez: caution, caution, caution, caution, right? I mean, it's, uh, you know, just making sure that, you know, if you're going to side anyway, in any [00:18:00] direction, you're siding in an area that's just being extra cautious, right?
[00:18:03] Dr. Grant Garcia: Well, if there's ever a doubt. You spying board, there's just no, there's, there's no one, I mean, I had, I had to, I had to send, I had a patient. I thought I had broken their neck on one of my teams and tons of pain in the back of the neck. The dad was an orthopedic surgeon. I don't think he was very happy to me that I sent his son to the emergency room to get a CT scan, but I didn't really care.
[00:18:27] Dr. Grant Garcia: Right. Because I'm like, I don't really care what the dad thinks. I don't care what anybody else thinks. It's going to be a nuisance. They're going to get called at two in the morning because they have their CT scan of their son back. But to me, all I care about is that I'm making sure that the person has that the player is fine.
[00:18:40] Dr. Grant Garcia: And they ended up being fine, which was great. Um, what is the number? We don't one miss over a hundred non misses is well worth it still. So again, I'm not spying, boarding everyone on the field. Like I told you before, it's very rare that I have to do it, but there was enough that you had these. You had these team physicians calling for it.[00:19:00]
[00:19:00] Dr. Grant Garcia: And yeah, I mean, we could, we could go at nauseam with this, but again, it's the importance here is understanding that this was clearly more serious. They expected it to be more serious and thank goodness it's not. And hopefully he has a full recovery and this goes into concussion protocol. And in a few weeks, he's back to playing.
[00:19:17] Will Sanchez: Yeah. And for me, it's, it's the evolution. That's what stands out for me because I was like, wait a minute, this was head trauma, right? It wasn't, I can't feel my legs. Or anything like that. So just seeing the evolution of, of how, uh, players are being treated and taken care of, and you, you know, illustrate it perfectly, especially what has happened since DeMar Hamlin.
[00:19:42] Will Sanchez: And I can imagine those conversations you're starting the day after. With every team physician, you know, with those types of scenarios, it's just being overly cautious and just being careful and making sure that, um, because that's the scariest thing that anything could happen to the NFL, right? Is having a [00:20:00] player, God forbid, die on the field.
[00:20:03] Will Sanchez: And, uh, and all of a sudden now, Oh, you know, Moms and dads all over the place is saying, well, go make one Soto money and go play baseball and get off the football field. Um, and just real quick, you know, you mentioned that, you know, you do work with Mercer Island. Um, at one point I was, uh, one of the coaches with Franklin high school, and we had a player that got absolutely demolished kickoff.
[00:20:28] Will Sanchez: Return. Um, and we had to call the ambulance. They had to get spine boarded. And they wound up going to Harborview. All of us. I can't imagine the parents and everyone else in the stands, as you mentioned, but from the coaching staff, we were playing against hail from the coaching staff. I just wanted the game to be over.
[00:20:51] Dr. Grant Garcia: Well, they canceled our game. The game got forfeited when we did it.
[00:20:54] Will Sanchez: Yeah. It was so
[00:20:55] Dr. Grant Garcia: traumatic for people that the entire game was forfeited.
[00:20:58] Will Sanchez: Yeah. And [00:21:00] I kind of wish that we would have done the same thing, right? I'm not, I wasn't a head coach, but it's one of those things like, all I want to do is get out of there, get in my car, And then myself and the head coach, we went to the hospital, checked in on them, got the update, the parents were there, you know, like, and by the, and then once we were all done, we were like, I was looking at the coach.
[00:21:20] Will Sanchez: I was like, let's, let's go get a slice of pizza and a beer. I need a, I need to say, I can't go home right now. I need a second. So it's just, it is just so scary to see anyone so vulnerable. Um, so, you know, one of the reasons also that we were kind of talking about this as well.
[00:21:39] Dr. Grant Garcia: No, and it's good. I mean, it's just important for people to understand that I'm glad I was taken seriously.
[00:21:44] Dr. Grant Garcia: This is an, this is important people understand when you see the spine board come out, it's again, the, the, the goal of this episode I think is, and again, we're not going to run on too much longer, but the goal of the episode is to show people that people are, it's when you see a spine board, it doesn't mean there's a, some catastrophic thing.
[00:21:59] Dr. Grant Garcia: You know, I don't, [00:22:00] we want to, we don't want to cause more trauma to people when they see this spine board come out, but I want you also to hear that it's. It's expected that you should feel trauma like to see the spine board is very traumatic like the traumatic response I got when I got home. My wife is telling me I saw the Instagram posts about what happened at your game.
[00:22:17] Dr. Grant Garcia: What happened? And I hadn't even been home yet. It was like one hour, right? And it was a lot of traumatic and they canceled the game and everything else. So that's totally expected response. But at the same point is it's also doctors and, and EMTs just doing their job because we want to be safe. So a lot of times it isn't as big a deal.
[00:22:34] Dr. Grant Garcia: Um, but to understand that, you know, you, the number one thing you should think about is obviously the safety of the player and to, you know, Just making sure that it's good to know that people are on the field that want to make sure the player gets the safest, most lowest risk potential, um, scenario. Yeah.
[00:22:51] Will Sanchez: Look at this picture over here. Look at that. Sports Do talk.com. All sports, all orthopedics all the time. [00:23:00] Check out our website. You got the Look at this guy right here. Look at that picture. I mean, what a hand. I'm gonna change
[00:23:05] that to your picture. I got that. The greatest picture ever in the, in the logo one.
[00:23:10] Will Sanchez: Check out our past episodes, our transcripts. Um, we'll always want to hear from you. So if you have some suggestions for shows, we've had a couple of people request certain shows and we make sure that we give our listeners, uh, what they want, especially, you know, being informative. So we, uh, we want to hear from you, but please check out the website.
[00:23:31] Will Sanchez: Check out our podcast. We have audio podcasts, video podcasts on YouTube. We're on every stream and platform, Spotify, iHeart. Apple, you name it. We're there. You're probably sick of us at that point, but we really appreciate you because you know what? I'm hanging with my Nomi's right here and this is my Nomi right here with me. [00:23:51] Will Sanchez: Dr. Grant Garcia. Uh, happy holidays. Uh, you're all squared away for the holidays and ready to go. Except for the 18 surgeries you're doing [00:24:00] in the next two days. Is that, that, that, uh,
[00:24:02] Dr. Grant Garcia: yeah, we're, we're good. I, I, listen, I ha that's why I have a great wife because I can do my job and she's going to. Take care of all the stuff. [00:24:10] Dr. Grant Garcia: She's going to take over everything that's actually important and I'm just going to focus on my doing my stuff. So, and you know, I appreciate all your listeners, uh, happy holidays. This is going to be the last episode of the, of the new year, but we've got a lot more to come and I'm really looking forward to next year.
[00:24:26] Dr. Grant Garcia: Um, and we've sound, we've seen a lot of changes in this. This podcast, you know, we've got these injury updates, we've got guest appearances. It's been awesome. And I think the viewers like all of it. So, I mean, I just heard about his tongue. Well, I heard a couple of patients even this week asking about the podcast and things that they had seen about it.
[00:24:41] Dr. Grant Garcia: So we keep doing this so you guys can be informed. This is fun for us. This is not our full time job. Uh, so this is just something we, this is something we just record late at night.
[00:24:51] Will Sanchez: Yeah. It's spooky. Anyway, happy holidays, everyone. We want to wish everyone a, uh, Merry Christmas, uh, Hanukkah, [00:25:00] however you celebrate with your loved ones, happy new year and, uh, be merry and be safe.
[00:25:05] Will Sanchez: Uh, Dr. Garcia, I appreciate our relationship, our friendship and our, uh, partnership. So let's keep it going.
[00:25:13] Dr. Grant Garcia: My Nomi.
[00:25:14] Will Sanchez: My no me. Bye peoples. Audio Transcript
Revolutionizing Orthopedics: The future of biointegrative implants with Brennan Marilla
Revolutionizing Orthopedics: The future of biointegrative implants with Brennan Marilla
[00:00:00] Will Sanchez: Welcome to sports doc talk. I don't know. I got this vertical thing going on. Hold on. Let's go. Here we go. That's our look. Will Sanchez along with Dr. Grant Garcia, our orthopedic surgeon, sports specialist. How are you Dr. Garcia?
[00:00:33] Dr. Grant Garcia: I'm good. I'm good. It's a good day. And, uh, you guys have, we got a new logo in the back.
[00:00:38] Dr. Grant Garcia: So we're going to learn a little bit about this. You never know what's going to be up there.
[00:00:42] Will Sanchez: Dr. Garcia is constantly changing his background. We started out with a promise in early September rooting for the Giants, having the Giants background. And apparently Dr. Garcia has put the kibosh on the Giants with the background.
[00:00:56] Will Sanchez: So now he's going with different backgrounds for all our shows. [00:01:00] It's still not working. I'm not sure what we need to do next. Maybe I need to change the blue light to a red light or yellow light or green light. Oh, you know what? I should have done green light for today's show because we have a phenomenal guest.
[00:01:15] Will Sanchez: But before we get to our guests, this kind of, uh, give a little housekeeping here and give a little shout out to our sponsors, the recovery shop. Garcia, this is your bread and butter. Take it away.
[00:01:26] Dr. Grant Garcia: All right. Well, again, this is, it's awesome. I've I talked to Mike and those guys and they said that they've had some people contact from the show interested.
[00:01:33] Dr. Grant Garcia: I had a surgeon that sent me a patient that asked to use this because the patients love it. So the idea behind recovery shop is any of your performance things that you want after surgery. People kept asking, I want more. You're doing all the cutting edge tools, but what else can I have? What else can you get me to get me better?
[00:01:50] Dr. Grant Garcia: Um, and we've seen some of these different products on the show with the Nice Machine, the Nutrition Supplementation, the Rebliss, you name it. So now my patients can go to this sort [00:02:00] of page that's mine and get whatever they need in terms of that for the recovery. So if you are a surgeon, you're interested in this or you're a surgeon, you're about to get surgery and you want your surgeon to offer this, I'll reach out to them and Mike likes and be contacted directly.
[00:02:13] Dr. Grant Garcia: So it's easier for you again I got no say in this other than the sponsorship. So just use this direct line Um, and hopefully you enjoy it for your patients and i've been super happy. So
[00:02:23] Will Sanchez: yeah, that's it's great for everyone and We're going to tease our own website at sports. talk. com. You can find transcripts.
[00:02:32] Will Sanchez: You can find previous shows. You could go to YouTube, check us out your favorite, uh, listening podcast platform, whether it's Spotify, Apple, you name it. So I am doing a shameless plug, maybe not so shameless plug of our show and all the great guests that we've had on, uh, Are you tired of listening to me talk at this point?
[00:02:51] Will Sanchez: Should we tease who's about to come on our segment and what they do?
[00:02:56] Dr. Grant Garcia: Yeah, I think we mix it up each time. So let's do a little quick intro for the, [00:03:00] uh, the viewers, uh, and also the listeners to hear what's up next.
[00:03:04] Will Sanchez: All right, here we go. The future of sports medicine is a biologic based. We owe
[00:03:10] it to our patients to bring the most up to date technology that'll make their recovery easier and also allow for them to heal faster.
[00:03:19] It's forming a new bone within 24 months. It integrates so there's no trace left behind. We've gotten away from using truly artificial means and restoring the body to its native structures. Osseofiber is going to revolutionize sports medicine.
[00:03:36] Will Sanchez: Dr. Garcia, we're really excited to have our guests. We have Brennan Marilla and I know the last name.
[00:03:43] Will Sanchez: I know how to say it. Let's go. Brendan Marella. Thank you so much. He's our chief commercial and operating officer at Osseo. Thank you for taking some time and to join us tonight. We appreciate it.
[00:03:56] Brennan Marilla: Thanks guys. Appreciate it. Thanks for playing that video. That video always gets [00:04:00] me pumped up every time I see it.
[00:04:01] Brennan Marilla: So, uh, hope you enjoyed it.
[00:04:03] Will Sanchez: It's a great video. Um, before we get into all the, all the toys that Dr. Garcia likes to use and obviously, uh, what you're providing, um, just for our listeners and viewers, we reached out to you a couple of weeks ago. We were trying to plan an earlier show and unfortunately, like so many others affected by The hurricane season, you were affected with the hurricane that came through hitting the Tampa and Orlando region.
[00:04:32] Will Sanchez: Uh, first and foremost, before we get to the show, how are you, how's your family doing, , what's going on? Because that was some scary, scary stuff.
[00:04:41] Brennan Marilla: Yeah. Well, hey, thanks for asking. Uh, this is, this is a rental home. We're in and I'm grateful to be in this house and I've got my, I've got my two adult children with me too.
[00:04:51] Brennan Marilla: So it's, we're back to a family of four because my kids also had their places flooded. Uh, but we had a, we have a house on a barrier Island here
[00:05:00] in the, uh, kind of the Sarasota area. And, uh, unfortunately, Helene, um, uh, Helene, uh, flooded our house. So we had about two feet of water throughout the entire house.
[00:05:10] Brennan Marilla: So, uh, while we were in the process of removing, you know, all of our furniture and all of our things, and ripping out the drywall and the insulation, you know, kind of there's a race against time for. You want to get it out before the mold sets, uh, in the middle of all that we had to evacuate because Milton was coming and, uh, unbelievable, you know, so it was kind of a one, two punch.
[00:05:32] Brennan Marilla: It's been kind of a wild, uh, wild month for us. Uh, but I think we're starting to kind of get our feet out, feet under us now. And, uh, you know, life is starting to get back to normal, but we're starting the long rebuild process now, but everybody's safe and, uh, you know, the area, the community has been great.
[00:05:49] Brennan Marilla: And I think, uh, We'll be back soon.
[00:05:52] Will Sanchez: Do you have them do, do, do you have the kids now doing chores? Are, are they raking leaves, throwing out the garbage, loading up the [00:06:00] dishwasher? Like are you, are you taking advantage of the full labor that maybe is, uh, happening in the house or now they're too grown and they can't be told what to do?
[00:06:08] Will Sanchez: What's going on there?
[00:06:09] Brennan Marilla: Yeah. No, I'm cracking the whip, just like the good old days.
[00:06:12] Dr. Grant Garcia: smart man.
[00:06:14] Brennan Marilla: Yeah, they're living rent free right now, so. Uh, you know, now I have to just kind of negotiate things, you know, like I need you to do this. I need you to do that. I, I'll, you won't have to pay utilities if you take the trash out.
[00:06:25] Brennan Marilla: So when they get, when they become adults, you have to do a little bit more negotiating cutting deals versus just telling them to go to their room.
[00:06:33] Dr. Grant Garcia: So we're learning, I'm learning so much from this. Well, anyhow, I'm glad you're safe. Everything's good. Uh, we're really excited to have you on her. I know it's been a lot going on in your life, but this product you guys have heard about it before on our show, right?
[00:06:46] Dr. Grant Garcia: This idea of harder than, you know, some of the other competitors on the market turns into bone faster, uh, and replacing metal. And honestly, this is just what patients have been asking for. I mean, I know that the couple of shows I put out with I put out before had [00:07:00] questions about this. We finally have someone who's an expert on it.
[00:07:03] Dr. Grant Garcia: I've used the product. I use it a lot. I'm really pleased with it. But obviously, you know, we have experience here with one of the man himself. So, Can you, we can talk about a little bit about your background and kind of why you got an Osseo before we go after the product, because it's going to be really awesome.
[00:07:17] Dr. Grant Garcia: We start talking about it, but as well knows we're gone once we start going after it, because it's going to be so much stuff we're going to have questions on.
[00:07:24] Brennan Marilla: All right. What do we, what are we talking about first? I'm ready to go. Well, I love
[00:07:30] Will Sanchez: the title on the website. If you go to Osseo. io. It's great. It says don't settle for metal.
[00:07:37] Will Sanchez: It's the first thing that you see on the website. And right there, it is so simple. It is so catchy. And all of a sudden, if you don't know what's happening or what it's about, just those three words alone already kind of puts you on the path saying, Oh, wait a minute, this is something different. So tell us a little bit about, uh, how you got involved with the company first, before [00:08:00] you get into the product itself.
[00:08:01] Brennan Marilla: Yeah, sure. So I've been in med tech about 30 years. Most of my career has actually been in cardiovascular, actually peripheral vascular and aortic disease. Spent a lot of most of my career at big companies. I've done some small companies, some big companies. I was at Medtronic for many years at Covidian.
[00:08:16] Brennan Marilla: Um, you know, one thing I learned from coming from the peripheral vascular space is that the mantra in that space is in terms of opening arteries, things like that, instead of leaving Instead of putting stents in like they used to, the market is moving towards, uh, like shockwave ultrasound or drug coated balloons.
[00:08:34] Brennan Marilla: The mantra is leave nothing behind. And the body leave nothing permanent behind. So, uh, when, uh, when Brian Verrier, who's our CEO, who I've worked with, uh, for many years at a few other companies told me he was thinking about taking this job as the CEO and, uh, I was at a different company. We had just sold that company.
[00:08:57] Brennan Marilla: Uh, and he called me and said, you know, I'm thinking [00:09:00] about doing some different things. There's this company Osseo. Um, would you take a look at it? I just want some advice on whether I should take this job or a different job. And I said, sure, I'd love to see it. And he sat down with me and showed me kind of the management presentation and some early animal studies and the idea of osteofiber.
[00:09:17] Brennan Marilla: And I said, God, I think that sounds like one of the most compelling things I've ever heard. I, the value proposition is, is obvious. I mean, you could explain to your next door neighbor, Hey, wouldn't you love to have orthopedic surgery? And instead of. a metal implant, you have an implant that turns into your own bone.
[00:09:34] Brennan Marilla: Uh, you know, immediately they're like, of course I would want that. You know, so we, I thought, geez, there's a huge, uh, unmet need here. It's very compelling to patients, to surgeons, even payers. Um, and, uh, you know, it's a five, 10 K path. It's very disruptive versus being something that's incremental. And I said, you know, you ought to take that job.
[00:09:56] Brennan Marilla: And by the way, if you take that job and you raise some money, why don't you bring me on? [00:10:00] Uh, and let's do this together because I think this sounds really, really interesting. The other thing that caught my attention was that, um, again, I was new to orthopedics seven years ago when we, when we kind of got Osseo off the ground, the United States.
[00:10:13] Brennan Marilla: Um, but, uh, I just thought it was interesting that all of, you know, most of the large companies, uh, have tried this over the years. They've tried to come up with non permanent implants because it's, it's, the need is obvious. Uh, the benefits are fairly obvious. But no one's really been able to quite crack the code on a non permanent implant that's weight bearing that is really strong and also is very biocompatible.
[00:10:40] Brennan Marilla: Um, and so that's why I thought Osseo could really be very disruptive. across multiple sectors of orthopedics.
[00:10:50] Dr. Grant Garcia: I want to chime in there. So we'll to you have, and obviously I wanted you guys on the show. I've been pretty excited about the product since I first saw it myself. [00:11:00] I would say, well, you have now have two people on this show and I'm assuming Will's going to be that way in a minute that when I heard about this idea, I said, that's, I've never heard of anything like that.
[00:11:09] Dr. Grant Garcia: And then when I used it, I felt the same way. So the disruption you have here to the listeners or to will is metal is very strong, right? Like we think of metal is like kind of what, almost, I hate to say the gold standard, right? Like when you're putting something in, you would never put in a plastic, you know, you put in plastic screws and drywall, but you wouldn't put a plastic screw into wood, right?
[00:11:32] Dr. Grant Garcia: I mean, it just not, now we can talk about this thing, but you wouldn't do that originally. You think it's break, it's not strong enough. And there's no products that we see out here for drywall stuff that we see that is often. In the bone, in the, in the body, it's the same way. And so people are just like this idea that every time we use a product, that's sort of supposed to dissolve or turn into bone before I've seen this.
[00:11:52] Dr. Grant Garcia: They would crack
[00:11:53] Brennan Marilla: right? Hard,
[00:11:54] Dr. Grant Garcia: hard bone. It cracks. Sure. So the first time I put this into something that was hard, I was [00:12:00] expecting it to crack. And instead it worked just as well in terms of strength as the metal, which we're going to go to in a second. There are various different types of screws that are not metal.
[00:12:11] Dr. Grant Garcia: And I have not seen one yet that turns into bone as well, but it's also as hard, which is just an extremely unique pattern. And I think that Brendan's going to go into this, but for the people to see this, it's like, there's so many different products out there, but there's, this one seemed to figure it out.
[00:12:28] Dr. Grant Garcia: And so that I think is what the uniqueness of the product is. And that's why I want people to hear about it. And I'll, we'll explain more of this in a minute as to why this is so important. Sorry, keep going, Brendan.
[00:12:37] Brennan Marilla: No. So what we tried to do is we, we wanted to create a new category. Uh, called bio integrative implants.
[00:12:44] Brennan Marilla: Um, we didn't, we especially didn't want to call this a bio resorbable or a biocomposite. That's not what it is. We, these are made differently. And Brendan,
[00:12:53] Dr. Grant Garcia: will you explain everybody why you didn't want to call that?
[00:12:56] Brennan Marilla: There's just a lot of baggage and a lot of negative baggage with bioresorbables [00:13:00] for a couple of reasons.
[00:13:00] Brennan Marilla: One is they're primarily just. Polymer based implants. Um, biocomposites introduced a little bit of minerals, some resin to kind of give it a little bit more, um, uh, structure, but they're still, it's still kind of powder. So basically traditional bioresorbables, uh, that have not been widely adopted, uh, in, in orthopedics.
[00:13:22] Brennan Marilla: And that's why metal is still still around 150 years later. Everybody's tried this and haven't really, haven't really been able to succeed is because polymer is very, it's not strong enough. If you drill it in, if you, if you nail it in, if you screw it in, um, you know, the, sometimes the, they'll, they're very brittle and they'll break or after you, uh, after you fixate bone, they might not be weight bearing, uh, they might break.
[00:13:47] Brennan Marilla: And, but if you get them in successfully, What happens is, um, these big polymer, these polymer implants can have these acidic breakdowns two, three, four years down the road. And when that happens, [00:14:00] patient feels inflammation, pain, uh, you guys see cystic formation, bone void, things like that. Uh, also the other issue is that if you want to do a revision surgery, whether it's metal or even peak, it's in your way.
[00:14:14] Brennan Marilla: Uh, and so we thought that, you know, if you. Um, if you have a technology that turns into bone, there's, there's nothing in your way if you need to go back in for any reason. Um, so we make these differently than the non permanent implants of the past. And that's why we call these bio integrators because that's really kind of the nature of how it works.
[00:14:35] Dr. Grant Garcia: We'll put that slide back up. I think that was important. The one we just had. So to chime in on this, he, what he hit on his thing, the cysts and the cracking for the biocomposite is a big concern. And. And the idea behind plastic, you're still leaving behind something that you've got to take out. And some of the plastics you can drill through, but some you can't.
[00:14:56] Dr. Grant Garcia: And this is a big problem. Alright, Will, so here's an example. Nick Chubb, we just had the [00:15:00] discussion. He had a revision surgery, right? There's a low chance that the surgeon used a biocomposite screw for him. So they probably used either a metal screw. Or a plastic screw, a peak screw. So when they did the second ACL for him, they had to either take them out.
[00:15:17] Dr. Grant Garcia: And by the way, everybody knows no one looks good taking out hardware. And so you're talking about stripping a screw pulling out. I do a ton of revision ACLs. I do a ton of revision surgeries. I mean, I just had a patient today. She's doing awesome. You could see she's got, I took out all these metal from the ones you had before.
[00:15:33] Dr. Grant Garcia: They just got track marks all over the inside of her bone. And I had to worry about those when I'm doing the surgery. Is it going to get in my way? Is my going to get by fixation? So there's still these things. And if they have a biocomposite, the CIS formation is actually worse. Taking out a screw and having a hole is a, is frustrating and certain surgeons can figure out different ways of doing it, but the cyst is a nightmare.
[00:15:53] Dr. Grant Garcia: And so you, the fact is you leave no trace doing a second surgery or doing a third surgery, which we [00:16:00] never want to do, but it's like probably something I do twice a week or three times a week. Yeah. It makes my life so much easier. And so that's another point of it as well. So else, sorry. Can you describe the, the strength prat, the strength graph and the regeneration graph you have here?
[00:16:15] Brennan Marilla: Yeah. So the, um, the graph on the right is just kind of, uh, an illustration of kind of what we set out to do was, you know, the kind of the Holy grail of, of, uh, materials, fixation materials and orthopedics should be that they're natural. Um, they, they leave nothing behind, leave no trace, but they're also strong.
[00:16:36] Brennan Marilla: So if you kind of look at that chart, you've got strength on one axis and you've got kind of natural bone regeneration on the other axis. Um, you can see where we're twice as strong as peak or about five times as strong as a traditional bioresorbable. Uh, and, um, and we also have that natural bone regeneration happening.
[00:16:53] Brennan Marilla: So that upper right hand corner is kind of where you want to be in terms of orthopedic fixation materials in the future.
[00:17:00] Dr. Grant Garcia: All right, well, let's go to that next slide. By
[00:17:01] Brennan Marilla: the way, Um, you mentioned Harbor Removal Surgery, uh, obviously there's a huge cost benefit here too. Um, obviously patients don't want a second surgery, especially, uh, children, which is why we have a pediatric label for most of our products now.
[00:17:16] Brennan Marilla: Um, but Harbor Removal Surgery is one of the most common surgeries in the United States. Of any surgery and that's and you also started foot
[00:17:24] Dr. Grant Garcia: and ankle, which is the most common, right? So as a knee surgeon, I take out plates. I take out I I don't do many metal in you're talking about surgeons Still love this product not being a metal guy.
[00:17:34] Dr. Grant Garcia: I'm an anti metal surgeon if I could do it I mean I have to do metal occasionally But i'm anti metal and I tell my patients I try not to do metal But even that that type of surgeon that does anti metal this product is very very unique still Right, so, you know you're comparing to metal and that's actually the most common thing we see You Um, but even people that don't always use metal, there's still a huge benefit of this, right?
[00:17:54] Dr. Grant Garcia: It's just that you're, you, we're always, metal is the gold standard for hardness. Um, but taking out [00:18:00] removal of hardware is very common. And in foot and ankle, I have a bunch of really good partners. I would tell you that 30 percent of their surgeries are removing the hardware they put in the foot.
[00:18:08] Brennan Marilla: Exactly.
[00:18:09] Brennan Marilla: It was really important to us that we bring you guys, the surgeon community, um, a technology that would not have, would not have trade offs so that you could get the benefit, the patient benefit. You could get the benefit of leaving nothing behind and preserving your landscape without feeling like you're trading off strength.
[00:18:29] Brennan Marilla: Or ease of use. And we've worked very, very hard at that. So the way we get our strength is, is this, this chart here, this, this, um, kind of illustration here. Um, we take basically minerals found in bones, silica, calcium, magnesium, et cetera. Um, Iran, our founder, uh, figured out how to take, uh, these minerals and how to, um, engineer them into these long, continuous fibers.
[00:18:55] Brennan Marilla: like fiber optic cable and then he layers them in different directions. You layer [00:19:00] them in different directions, uh, and you create like this matrix infrastructure and that gives you unbelievable strength. Um, it gives you a lot of body, a lot of structure and a lot of strength. And as a matter of fact, we make our, our implant, if you know, if we make a screw different differently than we make a staple or an anchor, we can just take these fibers and we orient them in different ways.
[00:19:21] Brennan Marilla: to dial in different mechanical properties. But each time we do that, we definitely continue to overlap and weave them. So they're really, really strong. Um, what that does is it gives you really, it gives you. Uh, strength higher than cortical bone at time, zero through six months and beyond. And then, and then over time, what happens is bone attaches to this immediately.
[00:19:42] Brennan Marilla: We saw in our animal studies at two weeks tra trabecular bone formation on the implant. Bone thinks this is bone and then it starts to infiltrate the implant. It's a little porous bone cells infiltrate the implant and then over time it just mineralizes and just regenerates and just becomes bone. [00:20:00] So at about in all of our animal studies and in our human studies as well, but in the animal studies where you can look at histology.
[00:20:06] Brennan Marilla: At two years, there's no evidence there was ever an implant.
[00:20:10] Dr. Grant Garcia: And well, this is a really, I want to explain to you what you said for the listeners. Cause obviously the surgeons get it. Med device company, people might hear this and understand some of it, but we'll cortical bones, the outside of the bone. Okay.
[00:20:22] Dr. Grant Garcia: And I think, can you go to the next slide? Is that the one with the bones? So I can show them. Yes. Right here, guys. Okay. So cortical bone is the surrounding bone. You guys see the bottom, that sheep study that's cortical bone. That's the hard stuff. So like, and I don't want to gross too many viewers out when you're drilling, you're hit cortical bone.
[00:20:39] Dr. Grant Garcia: You're like, that's hard. It's like really solid. And then you go through the counsellors bones, like where the bone marrow is. That's like, well, if you ever eat bone marrow, it's super soft and gushy. And can sell us bone is like very soft. So there's really not much there. And then you go to cortical bone.
[00:20:53] Dr. Grant Garcia: So the idea is that this is the hardest bone you want is cortical. Like we always are looking for cortical purchase. It's like in a [00:21:00] wall, right? You have, you're looking for the stud. That's absolutely right. But what's cool about this product is that it basically, what we're finding and you're going to see us in a second is that that's the screws are essentially turning the entire tract into cortical bone.
[00:21:15] Dr. Grant Garcia: So you're actually getting, you're actually making the bone harder in certain spaces. Which is pretty crazy to think about. So the idea is that in some of these cases, they're actually able to heal bone. You're going to see that from the knee bar study. And the idea is like helping with union, right? So if you've got two, you split that bone in half right there.
[00:21:32] Dr. Grant Garcia: Imagine you've got two, the shell casings are good, but when you, when you put it back together, you still have the soft stuff in the middle. And that can take a little while to heal. So the idea that we're still working on is if we put that screw through the middle in a metal one, there's nothing's going to grow, right?
[00:21:45] Dr. Grant Garcia: It's just going to grow around it, but not in the middle. So you're going to have a part that's not actually healed. If this turns into solid bone, are you actually going to turn this? This bone into like a three part thing. So now you're going to have a piece of cortical going through the middle, which is kind of a crazy concept.
[00:21:59] Dr. Grant Garcia: You're [00:22:00] essentially get, you essentially could make people's bones harder, which is really fricking wild. I don't know, Brennan, if you were going to talk about that, but that idea to me was, that's one of the things we're working on is the future. Right.
[00:22:11] Brennan Marilla: Yeah. That's interesting. You know, the, uh, over time it'll end up, it'll end up like it was never there.
[00:22:18] Brennan Marilla: Uh, and so, um, you know, you don't have to worry about any of these kind of like, uh, uh, extra articular structures and like that on the, on the, on the bottom there, that's a, that's a plate study that we did, um, years ago. Uh, a little feasibility study, the sheep tibia, and what's interesting about the study is you look, we put a plate on top, you can see in the kind of the 13 week on the far left, and then over time, it looked like bone kind of tense up to the side of it, and then it all remodels back down to the cortical surface.
[00:22:48] Brennan Marilla: So for us, for, for us, you know, we are working towards a plate technology. Um, but the staple that we launched, we launched a staple a year ago. We just launched a small staple that has a lot [00:23:00] of foot and ankle applications, a little hand and wrist. They do a lot of Aikens with these little nines and 11s.
[00:23:04] Brennan Marilla: But, um, but this was, uh, this, this helped us with the FDA in terms of getting this, the first non permanent staple in the world to market, because people wondered, we knew what happened in bone. We wanted to know what happens on bone. And this is what happens on bone. It completely remodels down to the cortical surface
[00:23:21] Dr. Grant Garcia: and that's incredible to create
[00:23:22] Brennan Marilla: a speed bump.
[00:23:23] Brennan Marilla: You don't have to worry about, uh,
[00:23:25] Dr. Grant Garcia: uh, overgrowth
[00:23:26] Will Sanchez: looking out. Yeah. Brendan. Um, what was this seems, you know, we we've had so many shows, um, With different technology, um, you know, different, you know, medical advances from the beginning, right? You got the phone call, the company, things like that. But what was the process to talk to the doctors to see what worked?
[00:23:52] Will Sanchez: What didn't work? What did that look like? What was the studies? How many people did you guys talk to? Um, was it just, you know, [00:24:00] United States was expansive. Did you, you know, what, what was the research? I'm just curious to. To come up with the concept and just hear from the different, um, whether it's orthopedic surgeons or anyone else saying we need something else besides metal.
[00:24:16] Will Sanchez: And what did that look like as far as trying to figure that out and get, and get into the point where you're at now, because obviously like all the, all this technology is start somewhere. Yeah.
[00:24:25] Brennan Marilla: You're talking about developing the technology or developing the go to market plan. Well, no, just, just, yeah, no,
[00:24:32] Will Sanchez: just really just kind of just having the conversations, you know, how did those conversations start with other doctors and realizing that, you know, there was a market for something like this and how do we get to the point where we can get away from metal?
[00:24:45] Brennan Marilla: Yeah. I mean, look, I, I think like I said earlier, the, uh, um, the market had already been kind of validated. The need had been validated. Everybody's been trying to bring, you know, uh, non permanent implants, the market that can be mainstream. I mean, we wanted this to be. the [00:25:00] first credible replacement to metal implants and other permanent implants like peak.
[00:25:05] Brennan Marilla: Um, Iran price bloom is our founder. He deserves all the credit for this. Uh, I call him the Elon Musk of orthopedic fixation materials. He's a very talented biomedical engineer, uh, studied at Columbia university, uh, orthopedic research department. His thesis was the interaction of metal and bone. He became very obsessed with the fact that, uh, there's so much innovation in orthopedics.
[00:25:27] Brennan Marilla: I mean, there's a lot of innovation in this part of med tech, but fixation materials is not one of them. And, uh, and they're, and they're problematic for all the reasons that we know, of course it works and, you know, and using it for a hundred plus years. But you know, why, why are we going to put somebody.
[00:25:44] Brennan Marilla: On mars in the next 10 15 years and we're still using metal implants. It's kind of ridiculous. So he was obsessed with it and and uh, and was able to Uh bring this concept to life and uh You know, we got some smart, you [00:26:00] know early, um advisors around us. Uh, we were able to raise money Um, we were able to get some seed money from the israeli government because the technology center is based in israel Okay, and um, and we were able to get it off the ground Get it off the ground and, and get it into some successful animal studies.
[00:26:18] Brennan Marilla: Um, when we just, when we started, um, our, when we kind of got our plans together to go to market United States, when we, you know, in about 2017 is when we, uh, opened up the Boston headquarters and started hiring people in United States. And, um, and at that point we began to go out and try to understand the perceptions of the market around non permanent implants.
[00:26:43] Brennan Marilla: And what we found was what we, what we thought we would find, which is everybody loves the idea. There's not a single surgeon that just says, yeah, that's not a good idea. Like, why are you even thinking about this? That's, that's not even the, you know, kind of validating the need we don't need to do. We have to prove that this is [00:27:00] different from prior attempts.
[00:27:01] Hmm.
[00:27:02] Brennan Marilla: And so we had to get out and we had to understand what were, you know, what did they like and dislike about, you know, the, the other, um, the other non permanent implants that had been on the market are still in the market, including the biocomposite market, which is still very, that that's been a successful part of non permanent implants is shoulder biocomposite acres.
[00:27:21] Brennan Marilla: Um, but otherwise anything weight bearing has not been typically. Um, so we went, we had to go out and try to understand, you know, uh, how would the market view this, how would, how do we need to explain it? And we just decided to go out and just be as transparent as we possibly could with how we make it all the animal studies.
[00:27:39] Brennan Marilla: Um, we wanted to be a very scientific company. Uh, we wanted that to be part of our brand personalities to be, to be very scientific and innovative. And, um, and we also decided to brand the category differently with, which is biointegrative. And that has been a term that I think has been very sticky for us because once you have a chance to explain this, um, [00:28:00] to a surgeon or even to a patient.
[00:28:03] Brennan Marilla: Uh, it just makes a lot of sense and people want to evaluate it and try it. So
[00:28:09] Dr. Grant Garcia: the, uh, I think we'll also, you're trying to get at the way these surgeons think again, I'm obviously just one of them. There's many of them. Um, all the stuff that Brennan saying is really good. Right. And we listened to that, but obviously the same thing is it's got to perform.
[00:28:24] Dr. Grant Garcia: When you actually do it, so when I did my first trial, so we can hear this, I picked the hardest scenario because I was like, if it doesn't mess up on this, then we're good. Right? So I eat the tibia, which is the tibial bone. And so I do certain surgeries that require the fixation of the tibia. And I have tried a lot of anchors.
[00:28:42] Dr. Grant Garcia: And I've had a lot of reps upset when they crack when I'm doing them. And I remember the first time I put one of these in, I put it in and it just kept squeaking, which means, as you know, squeaking in the wall means like, there's only two ways this is going. It's going to snap in half
[00:28:57] Will Sanchez: and I'm not
[00:28:57] Dr. Grant Garcia: going to be done using it or it's going to go all the way [00:29:00] down and it's going to work.
[00:29:01] Dr. Grant Garcia: So I remember doing it and went all the way down. I look over at the rep and I said, how did you guys do that? I was sure this thing was going to crack because I heard it squeaking the entire time. And then the next time I did it, I was like, let me make this even harder. So, you know, you're supposed to tap up screw.
[00:29:15] Dr. Grant Garcia: He's like, just the reps, like do only a little bit. And I was like, dude, that's going to break for sure. And I did the exact same thing, but I'm like, if this breaks, it's no big deal. Right. The cool part about these implants is, you know, again, doesn't happen, but if they crack, you can just drill it out and do it again.
[00:29:30] Dr. Grant Garcia: It's not like when you have a wall, you have a whole hole, you can't use it again. So I tried it again and it squeaked even more. And I'm like, this is definitely going to break. And sure enough, it didn't. And I looked at him, I was like, where can I get more of these? This is awesome. So that's all honestly, will, I hate to tell you that you can, Brendan can talk all day about all the data he says.
[00:29:48] Dr. Grant Garcia: And that's really great. And that helps me feel good to tell my patients about it. But in the end, it's got to perform. It's just like these athletes, right? Like all day you can train, but if you can't shoot the hoops, there's no point in even being on the court. So [00:30:00] anyhow, go to the next slide. This is, this is really good.
[00:30:06] Dr. Grant Garcia: So you can see where they're at. I mean, Brennan, you can see where we're going to ask about what are your, what are the service lines you're looking at? And we want to make sure we get to all this stuff cause we could go all day with this. We,
[00:30:17] Brennan Marilla: we see this as a platform technology, uh, and you could make, you can make endless number of implants across all the, all the sectors of orthopedics.
[00:30:26] Brennan Marilla: Um, I mean, you know, uh, you know, Iran, our founder, he wanted to go into spine first. Okay. We were like, well, maybe let's, let's pick a different space. Uh, first that's, that's a little bit of the wild, wild West right now. He is,
[00:30:38] Dr. Grant Garcia: but he is the Elon Musk. So he's just,
[00:30:41] Brennan Marilla: listen, we think there are many great applications of spine, but we said, you know, why don't we start with a foot and ankle and we started in foot and ankle for a few reasons.
[00:30:49] Brennan Marilla: One is we thought that was maybe where the biggest unmet need existed because you're walking on these implants, people feel them in their feet, even when you have a successful union, a
[00:30:59] Dr. Grant Garcia: lot of removal of [00:31:00] hardwares is probably the
[00:31:01] Brennan Marilla: very high hardware removal rate. Um, and there just wasn't a lot of, uh, non permanent implants available for that market.
[00:31:11] Brennan Marilla: So we went to that market first and we've had a lot of success in that market. We've, you know, we're over 40, 000 implantations now. Um, And, and that just in a few years. And so this is our current portfolio. Um, thanks for pulling this up. You know, we started off with, we started off with something really easy.
[00:31:29] Brennan Marilla: We thought, geez, a hammer toe implant would be really a easy place to start. Uh, it's also an interesting study because we did our first in human study was, it was in hammer toe. And not because we wanted to really, we were super interested in hammer toe. It's just that we wanted to show biointegration and safety and efficacy.
[00:31:48] Brennan Marilla: And, um, that implant fills up a lot of that, uh, intramedullary space. So it's actually a really good test. But anyway, so we start off with a hammer toe. Uh, we introduced these nails, these nails, think about rebar, [00:32:00] uh, anywhere where you need stability or strength, uh, if you need to add fixation. Um, these nails, these trimmable nails are super interesting to use really strong.
[00:32:09] Brennan Marilla: You can hang 350 off the end of one of these nails and you can trim them. You can customize them. Um, and then we introduced screws. Uh, we then followed with, uh, the suture anchors that you've, you, that you've used Dr Garcia, uh, then this, then the, uh, different staples. And then we have a new product that we literally launched a few weeks ago, which is the fully threaded trimmable nail, or it's kind of like a fully threaded screw, but we have a really interesting way to, uh, to trim them and then to, um, resharpen the tip.
[00:32:45] Brennan Marilla: So it's a, it's, it solves the scourge of the end of the industry that one of the biggest problems in the industry is. Inventory management. Imagine one length screw, essentially it's a nail and you trim it. And then, um, [00:33:00] you've got a little pencil sharpener there and you, you basically have a driver that's adjustable and you would just adjust the driver to the length of the, of the nail after you cut it.
[00:33:10] Brennan Marilla: And then you just resharpen the tip. And then you, you put it in, you can drive it in really easily. You don't even have to tell you
[00:33:17] Dr. Grant Garcia: don't have to tell you is you can use, you can have one long nail and put in three small screws with it. Is that what you're saying?
[00:33:22] Brennan Marilla: No, you can have one long nail. Oh, so on the, on the trimmable now, just the normal, just the typical nails, the ones we've had for a while.
[00:33:29] Brennan Marilla: You can cut those in half or in three pieces and you can get two or three implants out of those nails. The, the fully threaded nail. Uh, I think that may be difficult to do. I think you're going to get one implant out of that nail. You're just going to be able to trim it to length.
[00:33:44] Dr. Grant Garcia: Yes. So you're only having one side of the table.
[00:33:47] Dr. Grant Garcia: So you're not having to have like 10. So, well, the other issue you have with these implants is obviously stock, right? Like I'm lucky I've got a pretty good stock area, but like I can't carry every single size. So what he's saying is it comes in and you have one size fits [00:34:00] all, and then you can adjust it and customize it.
[00:34:02] Dr. Grant Garcia: So it means everything's a lot easier.
[00:34:04] Will Sanchez: I love that wording. The pencil sharpener is like, okay, you know, it's a three inches long. We need to get it down to two and a half. Well, we're just going to, you know, just, uh, Use the, the trimable nail and get it down to two and a half where I need it. And there you go.
[00:34:18] Will Sanchez: There's the exact size that you need for whatever the size of the bone or the area that you're going in. Because as we know, every person is built differently. Everyone is a little bit longer or shorter or things like that. So, uh, that's a, that's a great concept. Uh, what, what was the mindset behind that was to just realizing that there was a need and finding a tool would.
[00:34:42] Will Sanchez: You know, satisfy that?
[00:34:45] Brennan Marilla: Well, yeah. I mean, uh, our, our, our compression screws are, are, uh, partially thread at compression screws. They're really strong, but they're, um, not as sharp as metal. So you, you do have to tap them in hard bone, especially. Um. With the [00:35:00] fully threaded nail, you don't have to tap because the driver extends through the, uh, along the nail.
[00:35:07] Brennan Marilla: So you don't have all the torque in the head. And also it gives you better visibility when you're placing the implant because the driver, you can see the tip of the driver at the very end of the implant.
[00:35:15] Dr. Grant Garcia: Yes. Well, that's a good point you brought up. You can't see them on x ray either. So after you're done, you have to be able to find it.
[00:35:20] Dr. Grant Garcia: So this is why they did the beat, beat the trick on there. Yeah.
[00:35:23] Brennan Marilla: Yeah. So we actually used instrumentation to solve a few of the, uh, maybe some of the minor objections we had with our original screw. And we think this is the platform moving forward and the compression you get is amazing. And the squeaking, the surgeons love the squeak.
[00:35:37] Brennan Marilla: Uh, and I actually, I think this is a great TTO product for, uh, for, for sports medicine. Surgeons a great product for. using for TTOs and some of the other applications. But, um, we're going to have four and a half. We have five and a half. So we're going to launch next month. And we also have a hand and wrist.
[00:35:54] Brennan Marilla: So we have a kit for foot and ankle and sports medicine. Other, you know, kind of, kind of a universal kit. [00:36:00] Uh, and then we have one that's specific to hand and wrist for, so they can use these as metacarpal nails. So you asked like in terms of what sectors we're in, we're in foot and ankle. Um, we've been in foot and ankle for five years.
[00:36:11] Brennan Marilla: We've been in sports medicine for about a year. We're having great success in sports medicine right now. And then we're just, we're kind of entering hand and wrist. We've done, been doing hand and wrist cases, but this is our first like specific hand and wrist product. Is the, trimmable nail with the hand and wrist kit.
[00:36:26] Brennan Marilla: Go For metacarpal surgery, um, which obviously you don't, you hate to, you hate to revise those with metal on the way, uh, and patients don't want metal in their hands. So, you know, we think this is a winner for that application to really excited about this product and we'll continue to make all, we'll make smaller diameters and we'll make larger diameters.
[00:36:45] Brennan Marilla: We want to make big seven O's for big hind foot surgeries, hip, things like that.
[00:36:50] Dr. Grant Garcia: Yeah. Will, I want to tell you one more thing. So this product, again, I had the older trim old nail. I remember they showed me and they brought it in. They were like, okay. So they gave it to me. And this is all part of the intro [00:37:00] cock with the surgeon.
[00:37:00] Dr. Grant Garcia: And they said, and I've had this before where it hasn't gone well, not with you guys, but other companies. And they said, break it. And I was like, Okay. So he goes, break it, bend it. You're strong. You think you're strong, break it. And you're talking about, you know, it's this, I don't even know. It's as long as this chapstick.
[00:37:15] Dr. Grant Garcia: Right. But if it's thin, it's, this is only 4. 5 millimeters. That's not very thin. That's not very thick. And they were like, break it with your hands. So I'm like squeezing and it's, it's literally not moving. And I'm trying, I'm put on the table and I'm trying to break it. You can't break it on the table. So right then and there, you're like, okay, what's going on here with this?
[00:37:32] Dr. Grant Garcia: Not only is it not breaking, the threads are not shaving off. So that's a pretty impressive product. I remember specifically doing that cause I was 99 percent sure it was going to crack in half.
[00:37:44] Brennan Marilla: I'm glad it didn't. I wouldn't expect it. But
[00:37:48] Dr. Grant Garcia: you know what though, that's how you guys, that's how you guys get people to believe it because I remember, well the thing about this product is it's budding what we're [00:38:00] so used to.
[00:38:00] Dr. Grant Garcia: We're reached a really integrative, uh, Materials being soft and really strong materials not being integrative. So it's just, it's, it's so different that it just takes a lot of people to figure it out and a lot of time with people and it takes us for someone like me, it just takes me, I got to see this to believe it, right?
[00:38:22] Dr. Grant Garcia: I got to try this. I got to test how strong it is. Then I got to see how the patients do. And again, I've seen plenty of studies on this. I know the product works well. I'm not concerned about this in terms of. Recovery from the patients or cystic changes. I feel really good about it. But the, the hardness to me was the hardest part for me to, to bear.
[00:38:39] Dr. Grant Garcia: And I needed to test it out on the hardest stuff. And I've been pretty impressed. I
[00:38:44] Will Sanchez: just wanted to ask you, you've been with the company now for a while. What was that? Wow. Moment for you when you were like, obviously the, you know, you were all in, you believed in the product, but from seeing the products, you know, we saw the timeline right up till [00:39:00] now.
[00:39:01] Will Sanchez: What was that wow moment for you saying, okay, we got, we got something incredible on our hands and the future is just sky's the limit.
[00:39:10] Brennan Marilla: Gosh, that's a tough question. There's been a lot of wow moments. Um, uh, I'll give you a recent one and I'll maybe try to back up and give you some of the early ones. I think a recent one is getting the pediatric label from the FDA, uh, being able to treat children down to two years old.
[00:39:26] Brennan Marilla: Um, that was a big vote of confidence by the agency, um, in our, in our technology. Um, and, uh, and, and having surgeons across different specialties that have treated, um, pediatric, uh, pediatric patients tell us success stories, show us x rays. Um, we've been able to interview some of the parents and some of the children.
[00:39:51] Brennan Marilla: That's a major wow factor because when I first thought, when we all first thought about this opportunity, you know, should we, should we do Osseo or not? Um, we always thought [00:40:00] that pediatric avoiding a second surgery for a child that falls off a bike or breaks their ankle. Uh, is, is, uh, that's kind of the Holy grail.
[00:40:12] Brennan Marilla: That's why you get out of bed in the morning. It's not just the money. It's not the resume. It's not all the other benefits that, you know, all the other motivators that are kind of exist in jobs. It was. Gosh, that's just a really, that's just a really cool thing to be able to do is to put these and put these in children, have them just turn into their own bone and they have to, they don't have to go back for a second surgery and go through all that pain and, and you know, all the, all the hassle of having to do that.
[00:40:40] Brennan Marilla: So, so that's been very exciting for us as of late early on. I think it was just having surgeons use the product, um, having them, um, be so impressed with the strength of it. But, but more importantly, having them tell us three months, six months, a year, two years later, they're like, God, my patients are doing so well.
[00:40:58] Brennan Marilla: And no one's complaining. [00:41:00] Like no one comes back and says, Oh, I, you know, I've got this, you know, my, I've got all the swelling now, a year out. I mean, we just didn't hear that. And so that was, And then that's a foot and ankle
[00:41:09] Dr. Grant Garcia: thing too, what you brought up, Brendan. I mean, they picked. And they all say they pick foot and ankle because the market was underserved, but they also pick foot and ankle because like I said, I tried it on the tibia, the foot and ankle stuff.
[00:41:20] Dr. Grant Garcia: If the hardware is not going to work with foot and ankle, it's not going to work anywhere else. It's the hardest place to heal. It's the smallest place. It's the place that can patients complain by far the most of hardware, right? You guys, the easiest thing for you guys would have been to start with sports.
[00:41:36] Dr. Grant Garcia: Right. The sports has a lot of innovative, but there's not as much stuff. You pick the hardest one. I mean, spine would have been, spine would have been a hard one, but it wouldn't be the same because the patients have a lot of other stuff going on. Right? Like you pick the one where like, my mom's had multiple foot surgeries before.
[00:41:50] Dr. Grant Garcia: I know how hard it is to recover. Right. Then done plenty of foot surgeries at HSS. And you picked a very difficult one. And the fact is that that market was so successful that you moved on to [00:42:00] other ones should tell people how this product's doing.
[00:42:02] Brennan Marilla: You know, one thing that, one thing that kind of, I was thinking about as we were thinking about entering foot and ankle was seeing all the competitors in foot and ankle, or they were like, I don't know, they were like 25 or more companies that make.
[00:42:14] Brennan Marilla: Make hardware, uh, for foot and ankle. And I thought, geez, that's a really red ocean. Um, but in some ways it told you that first of all, these are all great competitors. There's a lot of phenomenal startups and big companies that are, that, that compete in foot and ankle. But when it, when you have that many companies making hardware, you wonder how does the market support that many companies?
[00:42:35] Brennan Marilla: Uh, and I've thought, you know, maybe it's because they're just not very differentiated and there's nothing that's really come in. That's replaced all of it. And that would take many years to really knock out all these, all these other, uh, uh, products. But, but when the, when a market's that noisy, you just say to yourself, geez, maybe if there was one great product, you wouldn't have to have 30 different companies with hardware.
[00:42:57] Brennan Marilla: Maybe that's not the right way to think about it, but why just, we thought that [00:43:00] that was both a, uh, a sign that's very competitive. So it's going to be difficult, which, you know, which it is. But it's also, um, because there's little differentiation, that's an opportunity. It's not also
[00:43:13] Dr. Grant Garcia: not someone dominating, right?
[00:43:15] Dr. Grant Garcia: It's like you're saying, like, when there's 200 answers for something, clearly, maybe you don't have the answer yet. Right? Like if there was, if it was, if someone had the right thing that worked every time, The other companies wouldn't be able to compete.
[00:43:27] Brennan Marilla: Exactly.
[00:43:27] Dr. Grant Garcia: Right. They'd be out right now. All my screws a little different than this screw.
[00:43:31] Dr. Grant Garcia: My plate's a little different than this plate. You know, it's all the repetitive same stuff so they can take their market shares and spread them out. So we'll, it's, it's, as a matter of fact, the more competitors you have, the better it's a, it's a kind of a backwards thing to think about. But I, what you're saying is perfect.
[00:43:44] Will Sanchez: Well the competitors are starting to, you know, spread thin because top 10 innovations. Best Technology Award, Best Practices Award, Global Excellence Award, Best Orthopedic Medical Device Company. Your [00:44:00] award winning technology is on display and is getting recognized. Uh, so competitors, I know it's very competitive field, but you guys are definitely leading the way.
[00:44:10] Will Sanchez: And, uh, I'll let you get back on topic as we always tend to steer in different directions there. Um, let me get back that, uh, That beautiful slide there, but congratulations. I mean, the, the, the awards, the recognition, um, it's gotta be exciting when, when you get that, you know, notification when the company, uh, when the founder gets recognized like that.
[00:44:36] Will Sanchez: So, uh, it's gotta be, it's gotta be a special thing just to validate all the work that you guys are doing.
[00:44:41] Dr. Grant Garcia: Will, let's show that foot and ankle side for the sake of time. I want to keep going. There we go. Show them that. And Brendan, you tell this. Why is it such a big deal?
[00:44:48] Brennan Marilla: Yeah. Again, um, not, not that anybody's watching your show to, to, to look at hammer toe studies.
[00:44:54] Brennan Marilla: Uh, there's more, I'm sure there's more. You never
[00:44:57] Dr. Grant Garcia: know. You never know.
[00:44:58] Brennan Marilla: There's might be more [00:45:00] exciting things to talk about, although it's a, it's, it's a, it's a highly prevalent issue and it's important issue for people. Um, so we did that, we, you know, that was our first product. So we did our first in human study.
[00:45:10] Brennan Marilla: Using a hammer toe implant and not because we were not not because we the market needed another hammer to implant or another hammer hammer to implant paper, but it was a great first study for us because we were looking really at safety biointegration and A hammer toe implant actually fills up quite a bit of an intramedullary canal.
[00:45:31] Brennan Marilla: So it's actually a really good test You really put it to the test and you can see here on x ray. You can see it two years You can't see it on x ray You It's in that second toe there. There's no joint
[00:45:43] Dr. Grant Garcia: left, guys. You can see there's no joint left. It just looks like a big long bone.
[00:45:47] Brennan Marilla: Yeah, it's a big fusion.
[00:45:48] Brennan Marilla: Nice fusion there. That's what you want to see when you get your hammer toe, uh, uh, fixed. And then on the right side is an, is, is a MRI. And you can see there's no fluid accumulation. And the implant is gone at two years. Um, [00:46:00] so that was the basis for, you know, our, some of our first publications. That came out first human publications.
[00:46:05] Brennan Marilla: And, uh, these were really important. And by the way, we got great, we got great fusion rates for, uh, for hammer toe implant.
[00:46:12] Dr. Grant Garcia: 96%. Well, if I did anything in my life, 96 percent would be good. So let's go to the next study. Let's go to the next study for him to show 100 [00:46:19] Brennan Marilla: percent patient satisfaction. That was, that was one of the most important metric we actually did.
[00:46:22] Brennan Marilla: That was an end point in the study was patient, uh, uh, satisfaction. We had a hundred percent patient satisfaction and, and usually patients aren't too happy with hammer toes. It's just a tough procedure. We thought that was a, we thought that was really, really good.
[00:46:35] Dr. Grant Garcia: All this is really good. I know you want to go this.
[00:46:37] Dr. Grant Garcia: I want you to touch on that last one. The biocomposite comparison. And I want to show people the difference because you, people say when I have a biocomposite anchor, I've got an anchor that's turns into bone. It turns in right away, right? I want you to show this 24 month thing.
[00:46:53] Brennan Marilla: Yeah. So, um, I believe one of your mentors, Brian Cole, uh, Brian Cole did this study with us [00:47:00] and, uh, we did this at the vet school at Colorado state and, um, we compared osteofiber to, um, A couple of the leading biocomposite anchors in the market and, uh, we were looking at a couple of things, uh, strength on strength at implantation.
[00:47:16] Brennan Marilla: Uh, we did really well there. And then on biointegration and, um, what we saw at two years, we're essentially completely biointegrated that point. Um, and what we saw with the biocomposite anchors is they really haven't broken down very much at that point. There really is not a lot of degradation that's happened.
[00:47:34] Brennan Marilla: Um, there's a lot of anchor left. And, uh, so at two years we didn't see much of a, uh,
[00:47:40] Dr. Grant Garcia: yeah. So when we, when people are selling some of these things, they're telling you. My biocomposite anchor, you want to use it because it turns into bone. And the idea is that more surgeons are, know this, and we all know this, that like, yeah, it might turn into more bone than a plastic one, right?
[00:47:55] Dr. Grant Garcia: Cause that's not going to go anywhere. That's inert, but it's not going to turn into bone as fast as you [00:48:00] think. And they can leave behind reactions, which is why he keeps saying it did not react because the common thought process is reaction happens with these. It's cystic changes. I mean, look at that.
[00:48:10] Dr. Grant Garcia: That's still not integrated. It. You see them too, Will? I mean, you don't have, you have an MD from the show, but outside of that, that's, but you know what I mean, Will, can you see the differences in that?
[00:48:19] Will Sanchez: Oh yeah, 100%. You can definitely see it. You can tell the difference, tell the graph.
[00:48:24] Brennan Marilla: One of the other things that's really cool about this study, um, we looked at graph cellularity.
[00:48:29] Brennan Marilla: So we wanted to see, you know, the biologics around the kind of the anchor graph interface. And we had a statistically significant Significantly better, uh, higher graft cellularity versus the, uh, control. Um, so we thought that was really interesting. So it heals really, really nicely. In addition to the strength, um, this, this heals really, really well.
[00:48:51] Dr. Grant Garcia: All right, let's go to the next one and see if there's anything on there. That's the, so this is, this is pretty cool. This knee bar thing is what I talked to you guys about [00:49:00] when I said, if you put it through something, it can kind of like heal it because actually it might promote healing because of the way it's structured.
[00:49:07] Dr. Grant Garcia: Right. Is that part of the thought process?
[00:49:08] Brennan Marilla: Yeah, yeah. Again, this is, we're, we're evaluating this in a clinical study right now. Um, looking at our trimmable nails that are already on the market, indicated for fracture fixation. Uh, looking at, um, uh, looking at, looking in the knee at, uh, at treating insufficiency fractures.
[00:49:28] Brennan Marilla: And is the, is the raftering, you know, basically is the kind of the scaffolding from this, um, from these nails. Is that having an effect and is the kind of the bone regeneration around that implant having an effect to reduce edema and pain? Um, again, this is, this is, uh, we're, we're doing a study. Um, uh, we're seeing very, very promising results.
[00:49:52] Brennan Marilla: Uh, uh, I know, uh, Dr. Cole's a manuscript that's, uh, you know, hopefully we'll get a publication soon. There's something that's, uh, [00:50:00] you know, in process right now on the, on the feasibility. Yeah. The, the, the initial feasibility. And, uh, this looks very promising. Uh, we're still learning, we're still trying to perfect the technique.
[00:50:09] Brennan Marilla: Um, but, um, but we're very excited about the, the potential for. this application, um, and it's interesting
[00:50:19] Dr. Grant Garcia: for them. It's interesting to see this stuff. I mean, this stuff is pretty impressive because we've all tried this. Well, so in this, this stuff you're seeing here, this edema, this is what pain it comes from.
[00:50:29] Dr. Grant Garcia: And so I'll do, you know, if they have this, it's either, you know, you either have to do eventually it's bad enough. You do an knee replacement. So if you can turn the, you see there, the one on the right, you see all of them, you see the white stuff going to no white. That's a really good thing. That's a really, really good.
[00:50:44] Dr. Grant Garcia: That means that person doesn't have pain anymore. Generally. Speaking. So this is the idea that you can do this without having to do a lot of other stuff. Cause some of the stuff on the market now is, you know, you blow it up with calcium and that actually really hurts, right? Versus something that's a screw that they're not going to feel.
[00:50:59] Dr. Grant Garcia: I mean, people don't [00:51:00] generally feel screws when you put them in after the first few months, they have achiness from the screw later on, sometimes with the change in weather. But the idea that you're putting this screw in, it's not a very painful process after the first few weeks. Uh, but the idea is that it heals in, which is pretty cool.
[00:51:15] Brennan Marilla: And will you asked about the wow factor? This has been a big wow factor for us. Um, um, and, uh, you know, we've been, uh, uh, a little stealthy with this because we wanted to make sure we had good scientific evidence before we really went out and, uh, and, and, you know, pursued this. Um, but, uh, the wow factor is definitely there.
[00:51:36] Brennan Marilla: The patients are really happy about their result and the surgeons are really happy. Really excited about what they're seeing so far. Um, more to come on this.
[00:51:46] Will Sanchez: Yeah. And, uh,
[00:51:48] Dr. Grant Garcia: maybe another episode.
[00:51:49] Will Sanchez: The, the, the wow factor is really the next slide that's coming up. Right. And even if you're not sure exactly all the things you talked about.
[00:51:58] Will Sanchez: It's clear as day when you [00:52:00] look at the results from the examples of metal to what Asio, the comparison, I mean, the pictures speak a thousand words. Uh, I have a buddy that broke his fibula and tibula jogging, a nasty accident. He has a rod and he had metal screws put in. And they didn't get taken out. So he still has them and he has a bunch of complications at times he could feel them.
[00:52:25] Will Sanchez: So having metal in his body at, you know, 53 years old and getting older in New York city with the heat, humidity, cold, we didn't, we didn't even talk about how the weather makes the body feel right. We, you know, just dealing with all of those elements, especially on the East coast where you have the extreme temperatures.
[00:52:45] Will Sanchez: I mean, he talks about it. So. Seeing this right here and seeing this slide and example, uh, metal compared to Osseo, the picture says a thousand words.
[00:52:55] Brennan Marilla: We treated a, uh, we actually have a video on our website. You can look at it. There's a, it [00:53:00] was a Kentucky Derby jockey, uh, out of Louisville, Kentucky. Really great guy.
[00:53:03] Brennan Marilla: And he had metal, he had a lot of metal from a lot, you know, a lot of accidents, these jockeys get. You know, throwing off his horses a lot and he had a lot of metal in his foot and his ankle. And, uh, in, in the, in the winter that gets so cold, he would go back down to Louisiana and train down there because he couldn't stand, uh, how his foot felt.
[00:53:20] Brennan Marilla: So he actually had the hardware removed and, and, and they replaced it with osteofiber and he's, it's, it's been a game changer for him. So we made a video with him. It's, it's, it was really inspirational. Um, you know, what's the other thing that, that, uh, that that's been really fun is to, um, we've been advertising on meta, the different meta platforms.
[00:53:38] Brennan Marilla: Um, around elective proce bunions, hammer toe proce patients research and sho say on the sidelines beca of surgery. And so we've awareness to the patient reception we've gotten ha We have about 350 surgeons Um, [00:54:00] and, uh, and we, this, so far this year, we've had over a hundred thousand patients click our ads and then go to our locator, a hundred thousand.
[00:54:10] Brennan Marilla: Uh, and we're not even spending that much money on advertising. I mean, we're a small company. We're not, we're not spending like millions of dollars on this. So, uh, we're getting a really strong interest, a really strong patient demand, and they're asking for it. They're going to their surgeon and saying, I want osteofiber.
[00:54:25] Brennan Marilla: And, and I've seen them, by the way, I'm seeing patients now in chat rooms and they're like resource groups that are online, these Facebook bunion groups and things like that, and they're in there and they're talking about osteofiber. And it's really, really, uh, really great to see that because the more patients are educated about this, the more they can go in as an informed consumer and say, Hey, is this right for me?
[00:54:48] Brennan Marilla: And if it is, you know, I want it. And, and they rave about it. So that's been a strategy of ours to educate, educate patients about this and certain sports medicine applications might be tough. [00:55:00] to advertise because I don't, people really shop for, okay, what kind of an anchor am I going to get when I have rotator cuff surgery and things like that.
[00:55:06] Brennan Marilla: But there are definitely, there are definitely opportunities there that we're also exploring in terms of some of those applications that are more relevant to your practice. Um, Dr. Garcia.
[00:55:16] Dr. Grant Garcia: Well, you know, I would, I would, I would counter you, Brennan, and tell you that patients come in asking for everything that I do.
[00:55:22] Dr. Grant Garcia: They asked for the every possible thing you could think of. They're like, I want this type of surgery. And we'll, we've talked about this before with a lot of the other companies, you know, they come in asking for specific things. I mean, today in the office, I had three or four specific requests for specific surgeries, specific implants.
[00:55:39] Dr. Grant Garcia: So they're really educated. We're in Seattle. They're like doing, you know, I bet you half my patients are already on your chat blog and they're going to be going on there now to figure out what this thing is and ask for it. So I would say that this is, this happens everywhere and any surgeon that does a practice where they require, where they're reliant on patients to look them up and find things and come to their website and things like that.
[00:55:59] Dr. Grant Garcia: This is a [00:56:00] great opportunity from a marketing standpoint for a good product that differentiates itself and to be able to offer this for your patients because they're going to ask for it. And these surgeons say they don't ever ask for it. I don't know you're talking about. You know, I just do my surgery the way you do it.
[00:56:12] Dr. Grant Garcia: Well, that's okay. You can be left in the dust if you want. Uh, but it's important that you understand that this is, this is coming, whether you like it or not, this is an excellent product and patients are going to ask for it, Brennan, even with your small amount of marketing.
[00:56:25] Will Sanchez: And if you're going to ask for it, you know what to say already, right?
[00:56:29] Will Sanchez: Don't settle for metal. Don't
[00:56:30] Brennan Marilla: settle for metal.
[00:56:31] Will Sanchez: Don't say
[00:56:32] Brennan Marilla: nature remains, baby. Leave nothing behind.
[00:56:34] Will Sanchez: Leave nothing behind. It's right on the website. It's amazing. I love it. I'm all for it. Whoever, whoever put that up there, the problem is now, well, it's going
[00:56:44] Dr. Grant Garcia: to repeat it like over the next five
[00:56:46] Will Sanchez: podcasts, every show, it's going to be like a little Easter egg.
[00:56:51] Will Sanchez: Yeah, that's great, man. Don't settle for metal.
[00:56:53] Brennan Marilla: There's a great foot and ankle surgeon in Baltimore, Stuart Miller, all the foot and ankle surgeon knows Stuart Miller. And he used to say when we first [00:57:00] introduced Osco to him, he used to say, I just want to set it and forget it. You set it and forget it. I just want to, I just want to treat that pain.
[00:57:07] Brennan Marilla: I want to just put that implant in there and not have to worry about it again. Set it and forget it. So I always, always remember that one.
[00:57:12] Will Sanchez: It's like an infomercial.
[00:57:13] Brennan Marilla: I
[00:57:13] Will Sanchez: love
[00:57:14] Brennan Marilla: it.
[00:57:16] Dr. Grant Garcia: So we'll we're at, we're now out of time.
[00:57:19] Will Sanchez: We are out of time. Let's say goodbye to Brennan. Brennan, thank you so much for your time.
[00:57:24] Will Sanchez: Um, I mean, we've talked about it. Check out asio. io. I mean, the webpage is amazing. I mean, it's good. We don't need to say anything. I mean, the awards say, speak for themselves. Um, we wish you and your family, uh, you know, just speedy recovery for the house, for the home, getting back, kicking the kids out, or if not putting them to work, whatever it is.
[00:57:46] Will Sanchez: Um, we just wish the best for you and your family and I'm hoping that this is a positive, right? To get the, get the family back under the roof and, you know, spend some quality time. And I know you kicked them out of the room because you were doing this show, so we really [00:58:00] appreciate it. That was, that was really fun.
[00:58:01] Brennan Marilla: I keep telling myself that, well, that's good. That's a good, it's a good positive outlook. So no, we're happy to be together. And, um, listen guys, if you, if you buy a house in a flood zone, just make sure it's really, really high. Okay. Just that's my, that's my lesson. Let me serve as a warning to others. Okay.
[00:58:19] Will Sanchez: All right. Or have some kayaks or something. All right.
[00:58:26] Brennan Marilla: All right. so much. Appreciate it. Talking to you. Enjoy the opportunity. And uh, Dr. Garcia, I'm so, so happy. Your patients are doing so well with this technology. So thanks again, guys. Great to meet you. Well,
[00:58:38] Will Sanchez: thank you. Likewise. Dr. Garcia. That was Brennan Marilla.
[00:58:42] Will Sanchez: I mean, providing information, right. And talking about tech and we emphasize a lot on the tech. And I mean, Osseo speaks for itself. Uh, the don't settle for metal. I'm going to say it all the time. Don't settle for metal. I'm gonna drive you [00:59:00] crazy. All right. Enough of that. Will Sanchez, Dr. Grant Garcia. Do you want to, anything to, before you wrap it up, Dr.
[00:59:05] Will Sanchez: Garcia?
[00:59:06] Dr. Grant Garcia: I don't know. Check it out. This book. Product's awesome. Check out the stuff they're doing. I hope that people are informed again. It's all orthopedics, all sports, all the time. Obviously we talked about it with some other specialties, but it was good. Follow us. We're almost running out of time. Cause they're not going to like it.
[00:59:19] Dr. Grant Garcia: If we go over an hour. Thank you.
[00:59:22] Will Sanchez: All right, people don't settle for metal.
Audio Transcript
Dr. Joseph Liu: Professional Team Coverage, What it Takes
Dr. Joseph Liu: Professional Team Coverage, What it Takes
[00:00:00] Will Sanchez:Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic surgeon in sports medicine specialist, Dr. Grant Garcia, uh, Dr. Garcia, before we get started and before we welcome our guests today, um, what's going on with your background? The last couple of weeks we've had the New York Giants, we're already hyped up, you know, for the season and Danny Dimes.
[00:00:38] Will Sanchez: And this is our year. We're going to make it.
[00:00:43] Dr. Grant Garcia: Not a good showing last week and we had to change it. I still cheer for them, but I can't represent right now. Got to represent what's doing well. The podcast. That's much better. That's a great picture, by the way, of Will. I got to work on mine, but that's an excellent picture. [00:01:00] That's the best rendition I've seen.
[00:01:01] Will Sanchez: I got, yeah, I got my little haircut kind of going on. Surprisingly,
[00:01:05] Dr. Grant Garcia: surprisingly, he looks even better in real life than the picture.
[00:01:09] Will Sanchez: Anyway, um, You know, it's perfect, right? Because our guests has been working with sports, works right in your field, you know, you know him really well.
But before we get to him, let's kind of give a shout out to our sponsors, the recovery shop, Dr.
[00:01:26] Will Sanchez: Garcia. You know, we talked about them before we even started working with them, but Tell us a little bit about why the recovery shop just works so well.
[00:01:35] Dr. Grant Garcia: Yeah. So we, you know, we've said this on all the episodes, but really the recovery shop for me has been awesome for my patients, right? There's certain things they can't get and I can get them to the recovery shop.
[00:01:45] Dr. Grant Garcia: And so instead of going online and having to look up, you know, which products they want, braces, more advanced ice things, the re bliss, other scar creams. It's now all available for my patients on their recovery shop. And each one of us surgeons has their own landing page. So my [00:02:00] patients feel comfortable with the stuff that I've pre approved.
[00:02:02] Dr. Grant Garcia: And I review all those things and do it. It's been rave reviews from the patients just because of the ease of it. And then they can, you know, they're always coming to me like, I want nutrition supplements. We have those from the show on there. Uh, I want to have the Reblesses on there. I want the Nice Machine.
[00:02:16] Dr. Grant Garcia: It's on there. All those things are all together and they can order them whatever they want. And a lot of times with the complicated surgeries we do, they want to be going to the next level. And it's not just the surgery. It's not just the rehab. They want the extras. And so this provides it for them. So, again, I get no cut from this, you know, go on there, go to, go to the recovery shop, uh, talk to them, uh, see if they're interested for surgeons is an awesome outlet to offer your patients the next level and stuff, especially there when they're asking for more.
[00:02:44] Dr. Grant Garcia: So without further ado, we got to get to the, to our awesome guests tonight. All right.
[00:02:50] Will Sanchez: Bring in our orthopedic surgeon, uh, Dr. Lu, Joseph Lu, uh, thank you for taking some time to be with us. And it's funny. Dr. Garcia mentioned something about the [00:03:00] Rebless and we'll get to that later on because I saw a really cool video of you checking out the Rebless.
[00:03:06] Will Sanchez: Well, we'll get back to that first and foremost, you know, it's, it's all about the company you keep. And obviously you're friends with Dr. Garcia. How in the hell do you guys have a relationship? Tell us a little bit how this relationship started. And, uh, and we'll take it from there.
[00:03:22] Dr. Joseph Liu: Well, Will and Grant, thank you so much for having me on the show.
[00:03:26] Dr. Joseph Liu: Um, just like you said, I've known Grant for Basically forever. Um, he and I were co residents, meaning we were the same year. We entered at the same time, uh, in residency at New York, in New York City at the Hospital for Special Surgery, which is basically the number one orthopedic hospital in the nation.
[00:03:42] Dr. Joseph Liu: And if that wasn't enough, we spent five years together there. Uh, we actually spent an additional year of subspecialty training when we traveled to Rush, uh, in Chicago together and did our one year sports medicine fellowship at the Midwest Orthopedics at Rush. So, you know, it's been a long time and we've been friends ever since.
[00:03:58] Will Sanchez: Dr. Garcia, before you [00:04:00] jump in, this is an important question here. You spent all this time in New York, uh, I'm originally from New York. In fact, I, my broken wrist was treated at the hospital for special surgery, but. Where was the hangout spot? All right. We're in the city. You guys are working together and spend all this time.
[00:04:18] Will Sanchez: Where's the watering hole? What was the spot? Are we hanging out on Second Avenue? We're going to fifth. We're going to Madison and we're going midtown uptown. Where was that? What was that
[00:04:27] Dr. Grant Garcia: Mexican restaurant that we always went to? It was so good.
[00:04:31] Dr. Joseph Liu: It was on second and 70th. I just remember the sangria. Okay.
[00:04:34] Dr. Joseph Liu: Okay. Okay. So this
[00:04:36] Dr. Grant Garcia: place, this place, this place will, we, the HSS, if you don't know, they try to track the best residents. And so by doing that, they subsidize housing. So we basically have our own building. And so we get like insane rent, uh, to go there. So it's like a, it's a no brainer when you want to go to New York and plus working at this place.
[00:04:53] Dr. Grant Garcia: So Joe and I all live in the same building for five years. So he like, we got, you know, not only do you work with the person, but you live in the same building as them. [00:05:00] And they see all your outside stuff, all your personal stuff. So there's no, there's all the dirty, the dirty things are released at that point.
[00:05:07] Dr. Grant Garcia: But on the way, literally we only have to walk two blocks and this is dangerous cantina between the two that has like the best sangria ever. And literally every time you walk home, you see some sort of one of the residents or fellows or whatever at the place. So, and I remember we would go there way too frequently.
[00:05:25] Dr. Grant Garcia: Uh, but it was an awesome hangout spot. Good. I think it was, it was Mexican. I'm almost positive. There's so many ones in New York, but that one was like dangerous cause you literally could smell it as you walk by or like your friends are like trying to hand you a margarita on your way home from the residency.
[00:05:40] Dr. Grant Garcia: Not the way in, obviously would never do that on call. Well, the
[00:05:43] Dr. Joseph Liu: worst is when you're covering the night shift and everyone's coming home and they're meeting up at this, uh, you know, corner tapas or sangria bar and you have to go in for the night shift and you can't, you know, take anything with you. And you're the only one in the hospital that evening.
[00:05:58] Dr. Joseph Liu: And so then you're just jealous for the rest of the [00:06:00] night, missing out. I don't think the audience wants to know about the night
[00:06:03] Dr. Grant Garcia: shift. The night shift, I don't wish the night shift upon anybody. Up is down, down is up. The only person that can handle the night shift was Dr. Joe Lu here. He's a master of that.
[00:06:14] Dr. Grant Garcia: He could do no sleep. You run around the hospital on fire is amazing. Well, that's hanging
[00:06:19] Will Sanchez: out at the cantina, right? I know. Grant was hanging out at the cantina. That's after six months. I was
[00:06:23] Dr. Grant Garcia: smart. I was smart. I was at the cantina. He was working. That's the way it rolls. Well,
[00:06:28] Will Sanchez: I'm glad the patients heard that.
[00:06:29] Will Sanchez: So they, they know that they were always safe, but they were in good hands with Dr. Liu. So that's good.
[00:06:35] Dr. Grant Garcia: So I wanted to introduce Dr. Liu, because obviously. You know, he had amazing training, HSS rush. He went to UCSF and then Stanford for undergrad. So he's clearly a slacker, uh, on the show. Um, but on top of that, you know, he's currently works with, uh, USC.
[00:06:52] Dr. Grant Garcia: He's done the USC athletes been on the field team physician. Um, and also works with the Sacramento, right? Sacramento Kings LA [00:07:00] LA Kings, LA Kings. And does the hockey team, but the hockey team is unique because we haven't talked about hockey, professional hockey coverage. It's a totally different animal than the football players.
[00:07:11] Dr. Grant Garcia: And we're going to go into this later, but there's also the side of the business, which is taking care of the players, the grit, the glitzy part. But then there's the other side. We talked about the last episode or two episodes with Tua and what happens with the clearance of him. So Dr. Liu is going to kind of, kind of refer to us as on that as well.
[00:07:28] Dr. Grant Garcia: But Joe, kind of talk about your practice, you know, what you do, uh, and then, you know, go from there and we'll keep jumping around.
[00:07:37] Dr. Joseph Liu: Yeah, so, you know, I'm an academic sports medicine surgeon at Keck Medicine of USC. Uh, I work with residents. I have sports medicine fellows that we train on a yearly basis as well.
[00:07:48] Dr. Joseph Liu: Um, I also do some, um, work at L. A. General Hospital as well, where you take care of, like, level one trauma or trauma associated sports medicine care. Lots of knee dislocations and multi ligament, you know, knee dislocations and things [00:08:00] like that. Um, and then I'll, you know, as an adjunct, because we're part of the USC faculty, we take care of the sports team.
[00:08:05] Dr. Joseph Liu: So USC Athletics, the USC football's almost like a professional team. Their yearly budget is You know, basically the same as a professional sports team, except for the salaries and with NIL, that's also a changing story as well. And then we also work with the Los Angeles Kings. And I think it's a great mix of taking care of, um, you know, patients from all walks of life.
[00:08:26] Dr. Joseph Liu: You have. You know, patients who are in, you know, kind of lower socioeconomic status at the LA General, where you get to take care of people that are very in need of care, and sometimes don't have great access to care. And then you have the flip side of things, where you take care of professional athletes, uh, collegiate athletes, where, You know, they're getting the, um, they're getting immediate care, you know, day zero care, and they're trying to, you're trying to get them back to sport immediately, you know, a lost day on a lost hour is, is too much for them.
[00:08:52] Dr. Joseph Liu: So they're trying to get back immediately. And I think that's the dichotomy between taking care of professional sports versus taking care of patients in [00:09:00] our office who come in and see us on a kind of outpatient basis.
[00:09:03] Dr. Grant Garcia: Uh, Joe, two questions that came from that, obviously questions from you introducing yourself, the NIL, right?
[00:09:09] Dr. Grant Garcia: We talked, we've heard about this. Have you noticed a difference in the USC team since the NIL was instituted? Is there any difference in the players, the way they're acting or the way you have to treat them differently? Right? Because before you take care of players, something happens. They don't really have a contract yet.
[00:09:24] Dr. Grant Garcia: Now they're worth millions of dollars. They're essentially pro athletes, right? So it's a different, it's a different, did you notice anything different when that happened? I mean, it's kind of been three or 10 years.
[00:09:33] Dr. Joseph Liu: I think the first thing that I noticed number one is that I think it came with the transfer portal.
[00:09:38] Dr. Joseph Liu: So the transfer portal changes as well as the NIL kind of occurred, not simultaneously, but around the same time period. And I think the combination of the two really changed the way we view. Um, or not necessarily the medical staff still treats them the same, but the way the players kind of try to, uh, kind of see their career.
[00:09:57] Dr. Joseph Liu: And that's part of it is their tenure at any [00:10:00] one university, USC included may not be that long, right? So you, what happened is when I started in most of the time, when you recruit someone, you're recruiting someone in the past for their entire collegiate career. They might have one transfer and it used to be where you had to wait a year before you were eligible.
[00:10:14] Dr. Joseph Liu: So transfers were a lot more, taken a lot more. Um, they just gave it a lot more thought. Nowadays, if you're not doing well or performing well, you might get injured. You might register early because you can transfer immediately and get asked either to another school or get a better contract through the NIL and you don't lose a year of eligibility.
[00:10:33] Dr. Joseph Liu: So I think the combination of the NIL money as well as the transfer policies have now made it so that players are, um, Are more apt to not be free agents. It college seems like a more of a little bit more like a free agency these days than it has in the past. I think that's probably the biggest change.
[00:10:52] Will Sanchez: Yeah, 100%. And, um, there's been articles coming out, especially lately, as far as. [00:11:00] What's going to be the next step. And so I want to ask you that question. And it's a really, it's a little bit of a vague question because we're alluding to the fact that these kids are now becoming professionals, right? And as we know, college sports and, and amateur sports, we are getting so far away from that at this point that we can, I can see the landscape changing all together where it, whether it's going to be a.
[00:11:27] Will Sanchez: Professional minor league or whatever it is. Um, are you starting to see that on your level in even as month to month, day to day, as we get closer and closer and seeing these changes that you're noticing that you're having a lot more influence, whether it's the coach or staff. Player player agent, you know, things like that, where there's a higher level of concern, especially when it comes to someone being injured.
[00:11:58] Will Sanchez: And, and I know it's a weird question [00:12:00] because as you mentioned earlier, you're going to treat each individual, give them the same care, but it doesn't mean that you had the same amount of stress. So I'm wondering if you're starting to see that or your staff or just across the board, maybe not yourself directly, but indirectly with your peers as well.
[00:12:17] Dr. Joseph Liu: I think that's a great question. And I think what you're alluding to is the fact that there is just more at stake here for these athletes, even at the collegiate level, right? Whereas before, um, maybe that transition was more at the professional level or CoachingBadminton. com because there wasn't as money as much money at stake.
[00:12:36] Dr. Joseph Liu: Um, there may have been a little bit more leeway to get these athletes back into, you know, back to playing status or you just had a little bit more time because there was kind of a little bit less at stake because you weren't trying to get them back for that season. So otherwise they would have transferred out or something like that.
[00:12:51] Dr. Joseph Liu: You had kind of more time to develop them. Um, but I do think that in this day and age, whether it's Just the competitive of collegiate [00:13:00] sports at every level has become greater. There's more money involved. There are just more, um, minds kind of in, in, uh, started behind every athlete. And so whether it's the parents that are more involved or there's an agent, or there is the, the kind of the posse behind these players that all have to be, you know, all want to be involved in, in their care and all have, there are people that they want to give their opinion.
[00:13:25] Dr. Joseph Liu: Um, I think that's part of it. Um, I think it's the second thing is we're probably more apt to, if someone's not doing well, to have second, you know, earlier opinions from other experts, whether it's from our partners or, or either from partners within USC or even partners within the town or even partners across the United States, where we send them to a specialist that is just known to treat all of the, you know, these athletes with this specific problem.
[00:13:50] Dr. Joseph Liu: Um, there's no expense spared because, you know, probably Neil
[00:13:53] Dr. Grant Garcia: Alatrosh. Right. We talked about this way too many times. Well, yeah.
[00:13:58] Will Sanchez: Yeah. That's interesting [00:14:00] to hear about that collaboration. So, you know, are you seeing your, uh, you know, to use an old term, your Rolodex kind of opening up and saying, well, we know how to treat this, but we're going to, you know, collaborate with a different group where they specific hand injury or Thumb injury for quarterback.
[00:14:16] Will Sanchez: That's just not healing. Right. And you know that, you know, someone across the country has a little bit more experience. So are you starting to see a wider pool of, or an openness to collaborate with your peers, uh, across the board? Because there's so much at stake.
[00:14:32] Dr. Joseph Liu: I think that's absolutely the case. And I don't think that's necessarily, I think, uh, USC athletics is very much like that, where we're very open to collaboration with the experts across the nation.
[00:14:45] Dr. Joseph Liu: Um, and it's always a case by case basis. Right? I think if it's something that's very, um, uh, you know, standard in terms of an injury, such as an ACL tear, uh, you know, shoulder dislocation very commonly treated, then, you know, certainly [00:15:00] keeping, keeping it within, sorry, keeping it in house is very reasonable.
[00:15:04] Dr. Joseph Liu: And if it's a very esoteric injury, so for example, we had, there was a foot injury that we recently sent out. Um, or, you know, there've been a couple of foot injuries that we've sent out to Dr. Anderson, who's one of the premier foot and ankle specialists across the nation. Um, you know, he's known to get these athletes back in a timely fashion.
[00:15:20] Dr. Joseph Liu: You know, there, there was, there are certain circumstances that require us to basically collaborate with these experts across the nation.
[00:15:27] Dr. Grant Garcia: Well, and do you ever, I mean, when we taking care of the pro teams as well, you know, you had a lot of these players, did they ever ask to go outside? Or whether, because they, they have agents now, right?
[00:15:36] Dr. Grant Garcia: With NIL, are they doing agents? And so a lot of times the agents will just float them. There'll be like, we're going to get another opinion, right? Whether or not you choose to, because now there's so much more money at stake. I mean, that's the one people don't realize. Like you could be a team doc. I mean, many of these team doctors don't operate on the players, right?
[00:15:52] Dr. Grant Garcia: The big players, they go wherever they want. They just pick and choose and they fly around the country. I remember seeing a few of the. Seahawks in my office. And it was just like, I [00:16:00] was opinion number six, right. And they'd already seen like they'd already, but they'd already had like the entire United States they'd seen and they were asking other opinions.
[00:16:07] Dr. Grant Garcia: And it was all the agent, the team was not, was not validating that, but that's not their, you know, the team doesn't make that decision. Unfortunately, in the end maybe a different for the college stuff. No, I think
[00:16:17] Dr. Joseph Liu: as a result of, you know, the NIL Monday, NIL money, I think these athletes have more people in their circle, whether it's their agent or.
[00:16:26] Dr. Joseph Liu: Um, family, friends or whoever, and they have all have their own connections. That's kind of how they get into the circle. Right. And they may have their opinions or you need to see X, Y, you know, this person to get their opinion because they know best and, you know, it kind of depends on who's talking in the athlete's ear.
[00:16:41] Dr. Joseph Liu: I'm not, I don't think an 18 year old who comes into college definitely knows, you know, the nuance ins and out of them, but if they get connected with an agent, there's enough money on the line, there's going to be someone who's talking in their ear that. Basically may recommend someone who they would see.
[00:16:55] Dr. Joseph Liu: And I think that's okay in sports, you know, and I think in medicine, it's, it's okay to get several [00:17:00] opinions. And I think when there's more consensus, then I think these athletes often, uh, have more confidence in their care as well.
[00:17:07] Dr. Grant Garcia: And I think the thing that people need to understand when they're hearing this is that As much as everyone thinks it's so great to operate a professional athlete, right?
[00:17:14] Dr. Grant Garcia: It sounds so cool Right. Like everybody always asks me that they're like, who do you operate? And obviously you don't tell them you can't say anything, but like, who do you put professionals? Do you operate? Have you operated on her? Who you fixed? They don't realize like, that's like, that's absolutely torture.
[00:17:26] Dr. Grant Garcia: Right. That's like calling the agent. They have to perform well, they don't perform well. And you're not one of the bigger top five sports guys in the country. You know, you're, it's your fault. Right. And there's the med legal, which we'll get into in a second as well. So like I, you know, we all welcome multiple opinions and there are certain guys that can just take on the risk.
[00:17:43] Dr. Grant Garcia: Neil Elitrosh somehow is the golden hands, right? He can operate all these players. He, I'm sure he's got issues with legal stuff dealing with it. No matter who you are, you have the James Andrews, you have Anderson. Um, you know, you have all check at HSS. Uh, you have all these guys that basically they, they're [00:18:00] basically, their practice and their whole setup is tuned to take care of these athletes and they can handle that volume, right?
[00:18:05] Dr. Grant Garcia: Cause if, if Neil Elitrosh does surgery on a professional athlete, right? And he doesn't get back, They're not going to blame Neil Altraz. They might, but he'll be like, I've done other, I've done 50 other guys like you and they all got back. So it's not my fault. If one, no offense to one of us, but if we do, we do one of the top players, they don't get back.
[00:18:22] Dr. Grant Garcia: They might be like, well, their Garcia hasn't done that many pro athletes. Maybe we didn't do a good job.
[00:18:27] Dr. Joseph Liu: Yeah. I think in the, uh, in the professional world, in terms of surgery, there are a select number of trusted surgeons that are the standard in terms of getting athletes back to sport, even if it's the same surgery that any of us would offer them, right?
[00:18:41] Dr. Joseph Liu: Um, that being said, it's, you know, that's their reputation. It's their history. Um, it's their, um, relationships with the agents and the players themselves kind of through the leagues that they've worked with. And I think that's confidence and trust that's built through You know, several decades of experience.
[00:18:57] Dr. Joseph Liu: And, you know, I think that's why there are a few, you know, [00:19:00] just a few surgeons that are out there that are, you know, in the echelon.
[00:19:04] Dr. Grant Garcia: It's a, this is this topic we could keep talking about all day. I mean, it's the, the thing people interesting that they don't understand is you're right. It's it 99, 95 percent of the time.
[00:19:15] Dr. Grant Garcia: Cause I mean, you and I both worked at rush HSS. We got bulls, white socks, U. S. Open giants, you name it. And we can talk about that experience, but you know, these are really good surgeons, but the surgeries that we do or the surgeries that I've seen by other doctors, Are just as good in many respects. And sometimes they use newer nuances.
[00:19:35] Dr. Grant Garcia: 'cause sometimes we've talked this in the pros, but they don't always get the like most up-to-date stuff 'cause people aren't willing to mess around with them. Right. Well like there's newer ACL techniques and if, like, I just saw an article that they pulled all these professional athletes and all, all these professional, uh, NFL doctors and they all would do the same ACL that we've done for the last 20 years.
[00:19:54] Dr. Grant Garcia: They wouldn't add anything extra to it. They would just do the exact same basic ACL. Now it's worked. It's time [00:20:00] tested. But the fact is that there was no innovation added to that. Meanwhile, I'm out there and Joe's out there doing things that are like 10 steps ahead because we don't have to be worried about the norm.
[00:20:11] Dr. Grant Garcia: Right. We want the best for the patients with best for the newest data. We've read 15 papers over the last two years showing how much better it is to add this stuff. But in that professional athletes, they can't, you can't start experimenting. I mean, that's why the Lonzo ball meniscus Carlos transplant is so crazy if he gets back, but there's only one person that could do it.
[00:20:27] Dr. Grant Garcia: And get away with it. And we all know that's Brian Cole, uh, outside of that is not possible. So hopefully it gets back. That'd be a whole nother topic to talk about. But Joe, on that topic, can you talk about your experience? I mean, everyone's heard me talk about HSS and rush, obviously awesome experience, you do the same stuff.
[00:20:47] Dr. Grant Garcia: And then like how that helped you or what you felt like going into the USC and then taking care of the hockey team. And like, kind of get the ins and outs of that briefly, you know, I think people love hearing that stuff because behind the scenes, they just see us running around on the field [00:21:00] and they don't really know what goes on, right?
[00:21:01] Dr. Grant Garcia: They don't understand the behind the scenes stuff.
[00:21:04] Dr. Joseph Liu: Uh, yeah. So are you talking about, you know, just my experience training at HSS and Russian? Yeah. And
[00:21:10] Dr. Grant Garcia: you know what, taking care of the pro athletes, what you, what you saw, what you, You know what, briefly what you did, you know, those kinds of things. And then how did it translate into your sort of taking care of the hockey teams, the USC, because we'll kind of jump in basically trying to talk about being a team doctor and all the stuff that you had to go through and like how you got prepared for it.
[00:21:27] Dr. Grant Garcia: Right. Cause not everybody gets the experience that we get in those first six years is vital. There's a reason there's a high HSS in Russia, some of the highest amount of professional team doctors in the country because they, they breed that, right. They want that.
[00:21:41] Dr. Joseph Liu: Yeah. I mean, I think. Number one is just HSS is just the mecca of orthopedics and sports medicine, right?
[00:21:48] Dr. Joseph Liu: We have, you know, some of the godfathers of sports medicine there that have, you know, so Dr. Warren is taking care of the, or previously taking care of the, uh, the giants for the last 40 or 50, you know, 40 years. And, you know, now [00:22:00] he's passed it on to Dr. Scott Rodeo, uh, who's, you know, been the head team physician for a number of years recently, and just watching them, uh, you know, getting, um, you know, watching them take care of patients on and off the field in the office.
[00:22:13] Dr. Joseph Liu: Uh, in the training room. I think that is a very unique experience. It's not necessarily available to all of the residents across the nation, right? You basically can only get that in very special, you know, specialized training facilities. Uh, I think also just the volume and the complexity of care that was taken, you know, done at special surgery, which is an orthopedic only hospital.
[00:22:33] Dr. Joseph Liu: Uh, working with, uh, basically every subspecialty, there's a giant in that field and, you know, probably not just one of them or a couple of them are, you know, at special surgery. That's kind of how unique it was. Uh, and then going to, you know, rush in Chicago, I think, you know, being involved in the White Sox and the Bulls and watching Dr.
[00:22:50] Dr. Joseph Liu: Brian Cole take care of the Bulls and see, you know, seeing how he managed those, you know, both in season and out of season players. I think that's the critical thing, right? I think the difference in taking care of professional [00:23:00] athletes is depending on where they are, the type of injury. Where they are in the season that you're it's going to be managed differently And I think there's only one way to see that you can't see that in the office Unless you're taking care of that style of patient If you just take care of, you know, someone like myself walking into the office, they're going to just give me physical therapy and see you in six weeks, right?
[00:23:19] Dr. Joseph Liu: But when you're taking care of professional athletes, you're trying to timeline and try to get them back to, you know, tomorrow, the next week, you're going to get, you're going to see them on a daily or, you know, uh, on a daily basis, occasionally to try to get them back to kind of see how they are. They might be day to day in terms of their status.
[00:23:34] Dr. Joseph Liu: And I think that's not something you can experience unless you're in the training room in the dugout. Uh, at the games, you know, seeing these injuries real time, uh, assessing them right at the time of injury, seeing them in the office the next day, seeing, you know, seeing the combination of their imaging, as well as their symptoms basically evolve over the next couple of days.
[00:23:53] Dr. Joseph Liu: I think that's the difference in terms of professional athletes. It's the speed at which you have to treat these injuries and trying to get [00:24:00] them back in the quickest way possible because days off are considered. Um, You know, they're, they're taboo, right? You, they're, they're playing for their next contract.
[00:24:09] Dr. Joseph Liu: They're playing in a contract year. Those are so, those considerations are so different. And so as a result, those are the things that aren't taught in normal orthopedic residency or education. They're not taught in normal medical education. You know, we're just, you know, in normal medical education, just taught to take care of the patient, try to get them back.
[00:24:26] Dr. Joseph Liu: But there's not really, um, that urgency. Um, that changes the way, you know, things are done in professional sports. I will say the other thing that I learned, and I don't know if you guys talked about it previously, is there is, uh, probably a little bit more reticence to, or sorry, more, um, incentive to do surgery on an earlier basis sometimes, so there's some things that potentially in the lay person you might treat nonoperatively.
[00:24:49] Dr. Joseph Liu: Because there's probably a more variable outcome or sorry timeline for healing. So for example a fracture that we might treat, you know A broken bone that we might treat non operatively in in the professional [00:25:00] athlete You're more likely to operate on them because once their wounds healed you have a much faster more reliable healing Uh timeline and you can get them back faster.
[00:25:08] Dr. Joseph Liu: And so as a result, uh Those indications are slightly different than what we would indicate for potentially someone who's just a community, uh, you know, someone coming into our office, basically.
[00:25:20] Dr. Grant Garcia: I think that's like literally the best points ever. I mean, Will, you should hear this because this is from like a layman standpoint.
[00:25:25] Dr. Grant Garcia: This kind of like blows people's minds. It's like we don't treat them differently, but you have to, right? You just have to like we try not to, but like sometimes I mean, Joe, what Joe's saying is right. Like certain things you treat them more aggressively. Right. Like a clavicle fracture, they go straight to ORIF, right?
[00:25:41] Dr. Grant Garcia: Because they want to get them back. And that means fix plating it. You know, there's a lot of things. But there's also some surgeries where we treat them less aggressively. Like cartilage, right? We wouldn't do a cartilage transplant on a professional athlete, obviously, until Alonzo Ball. But generally, we're going to do, they're going to do microfracture and things that like, would be considered like a huge no no now in my [00:26:00] practice.
[00:26:01] Dr. Grant Garcia: Right. But we change our methods for each doctor. I remember seeing one of the players and he had a terrible cartilage lesion with me from a condyle. And that will would be like, I'd be like, yeah, this needs like a pretty big cartilage procedure. And I, and I basically, the player was in a contract year and I had to tell him, you know, we're just going to do some stem cells or we're going to do some PRP and try to get you through the season, but like a lame person will walk in, I've been like, don't run.
[00:26:27] Dr. Grant Garcia: Don't walk. We're going to go to surgery in like six months. Like this is not good for you. So you just have like, everything's just different perspective and you don't, and then you can't be taught that you need to see other guys that other guys and gals that do this to learn how to do it that way. I mean, the in season out of season thing you mentioned.
[00:26:46] Dr. Grant Garcia: Joe was, is so vital. And there was no textbook for that. And even just even now treating just like high school and college athletes, they come in. I'm like, when's your season over with? I mean, even the martial arts high school kids, it's like, do you treat the dislocation in the [00:27:00] middle of the season? Do you treat at the end of the season?
[00:27:02] Dr. Grant Garcia: What surgery do you, you can tell them, okay, maybe you're gonna get a basic surgery now, but if you wait till the season, it's going to be bigger. Like everything you said was just on par. I don't know if Will has any questions about that, but it's like, I don't think we've talked about this on the show.
[00:27:13] Dr. Grant Garcia: We've had like over 40 episodes. But this is, this is amazing. This is exactly what we were hoping to get out of Dr. Liu today.
[00:27:20] Will Sanchez: This is more of a curiosity question just because, um, just from watching games and kind of seeing the speed and the movement of the reaction of the doctors on the field. We just saw Aiden Hutchison have a, you know, just pretty much breaking his leg.
[00:27:37] Will Sanchez: Instantaneously people are coming out, you know, getting his leg in a cast. Um, and in less than 24 hours, he already has surgery. So when you're working with the LA Kings, what's the protocol for someone like yourself or a team of physicians on game day? Like how many people need to be there, be ready just in case something happens.
[00:27:59] Will Sanchez: [00:28:00] What's the protocol of an injury of that magnitude happens that Yeah, we're hitting the ice. We've got four of us on standby. We have automatically this hospital ready to go. The aim, like just to kind of get a behind the scenes because when you watch it and if you're paying attention, it happens really, really fast and we've seen it with, you know, especially in the NFL where it, every second matters, right?
[00:28:27] Will Sanchez: Whether it's a DeMar Hamlin or anything else. So what's your protocol for game day? What does that look like behind the scenes? Yeah.
[00:28:34] Dr. Joseph Liu: Uh, that's a great question and um, I think the most important thing is there are more doctors than you can imagine that are That starts with that it starts with who your personnel is I think that's a character preparation so Uh at in in the nhl you're required to have an orthopedic surgeon who is the kind of head team physician there then you need to have um An er doctor typically our er doctor is in a general surgeon as well as er [00:29:00] trained.
[00:29:00] Dr. Joseph Liu: They're kind of combined, you know They have there are um, you know They're kind of code co trained. They, we have a dentist there for, you know, cause we get a lot of, uh, facial or, or mouth injuries. Oh, yeah, yeah, yeah. E and T doctor or a plastic surgeon who takes care of a lot of facial lacks or, uh, we have an ophthalmologist for eye injuries.
[00:29:17] Dr. Joseph Liu: Uh, we obviously have a general medicine doctor there for concussions. Um, uh, those are probably the, uh, those are the most common ones that we have in hockey. Uh, for football, we also have on staff neurosurgery that's involved as well. Uh, I know the NHL ha oh, sorry, NFL has their own kind of independent neurologist, uh, that's available to deal with depression, but that's not required at the collegiate level.
[00:29:39] Dr. Joseph Liu: Um, and then, um, So in terms of what's available on game day, we have paramedics are basically right off the ice, right? So you in, in USC football, they're just kind of right in the, in the tunnel that leads to the stadium. And then on the, uh, in for, um, for the NHL, they're just right off the ice. And we basically have, you know, uh, hospitals that we [00:30:00] know that, you know, we go to for certain problems.
[00:30:03] Dr. Joseph Liu: So if it's a cardiac event, they're going to go to a certain hospital. They're going to, if there is a traumatic injury, they're Uh, whether it's, uh, like a broken bone or something like that, we have another, it's a separate hospital for that. And so we know the contact and we go over the contact with, uh, the opposing team before game.
[00:30:19] Dr. Joseph Liu: So there's this pre game kind of huddle to make sure that everyone's on the same page. Uh, if there's like a cervical spine, a neck injury, we know how they like to basically position and get the patient uh, athlete off the, uh, off the rink to make sure they're transported safely. I see. I think these are, you know, it's all in the preparation more than so that when something like this happens, we can react on a moment's notice.
[00:30:38] Dr. Joseph Liu: And we're not, we're just following protocol at that point. We're just going to say, okay, this happened. We're going to do X, Y, and Z, and we're going to get them to the right location.
[00:30:45] Dr. Grant Garcia: And I want to bring up a point because I actually was, my friend was asking me this lot two weeks ago. He said, what's the craziest thing you had in your residency or fellowship?
[00:30:54] Dr. Grant Garcia: And you remember the White Sox player that had the aneurysm? And, and will [00:31:00] the, He's, I can't remember the guy's name. I just looked it up. He'll survived. White Sox player had an aneurysm on the mound. So he ruptured a blood vessel in his brain.
[00:31:09] Will Sanchez: Do you hit by a ball or was it just something that was building up
[00:31:12] Dr. Grant Garcia: sporadic?
[00:31:13] Dr. Grant Garcia: I mean, I don't know if there's a history of him. What he had is, but he probably had something brewing at some point, but he's just passed out and normally you'd like die from that and they somehow got him actually one of our co fellows with the doctors there, got him to the hospital. They got him taken care of and he survived.
[00:31:30] Dr. Grant Garcia: And he wasn't brain damaged. I mean, throw out a first pitch a few years. And that was on when dark, that's when Joe Lou and I were both at rush. We actually were not on that game, but we could have been. Um, and it was, I heard it was quite a traumatic experience for everybody there in the field. I mean, there's also the side of this is like, I mean, you're at the NHL and you get that carotid artery injury.
[00:31:49] Dr. Grant Garcia: That's no joke, man. So it's like most of the time, a lot of these games you deal with small things, but I mean, how many times Joe, we've had a couple and I will, we haven't even talked about this, but like we've [00:32:00] had a couple where we're like, we, the residents are called in. Because we're at HSS and we had to fix one of the Giants that broke his leg at like Saturday night, right?
[00:32:08] Dr. Grant Garcia: They're like, you're not even working and they're like, you get like a ring on your phone. It's like, we need you in the OR. You know, thankfully you're sober, so you run to the OR to help them out because you're not on call. And you need to go see, you know, whatever. I'm not at the cantina
[00:32:20] Will Sanchez: on 2nd Avenue and 70th.
[00:32:21] Will Sanchez: No,
[00:32:22] Dr. Grant Garcia: you're not in the cantina when you get the call to go fix the Giants. But, um, it happens. I mean, probably most, I think the most traumatic stuff is generally football, but there, we can pick a story from any one of those, but it's a, there's a lot of stuff that goes on behind the scenes. I think that's an excellent question.
[00:32:38] Dr. Grant Garcia: And it's really interesting for the, cause you just see that on the field. And all of a sudden you get a news report, right? You don't see the like hours of work behind the scenes. And I mean, how many times you prepare for this stuff and nothing happens. Right. So you got to be on alert. It's yeah.
[00:32:53] Dr. Joseph Liu: I mean, it, it can happen.
[00:32:55] Dr. Joseph Liu: Obviously the games are the most high profile, but it can happen anytime. Right. There's some players, [00:33:00] you know, who basically had a cardiac issue, you know, in practice and how to get them to the hospital, you know, And so those are things that, you know, at the most high profile situations are the games where other stuff is going on, and that's why protocol is really important.
[00:33:17] Dr. Joseph Liu: This can happen not just to the professional athlete, this can happen to anyone. And I say, so I think, you know, having these protocols at these locations that we, um, Uh, take care of. I think it's really critical and knowing who your resources are. I think that's another part of it. No one can ever do this alone, right?
[00:33:32] Dr. Joseph Liu: No, you know, there's, we're, we're all sub specialists in our own field. We know how to take care of what we know how to do very well. And we're going to rely on. Um, partners to take care of the, you know, things that they're specialized about. And so having a team that's in place beforehand, like I said, the preparation and having the right team available and having those protocols in place is going to keep our athletes safe.
[00:33:55] Dr. Grant Garcia: So I want to, I want to Change pace a little bit. This is always going to be, this is [00:34:00] always the hardest part of our jobs, but it's important for the viewers to hear this because we brought it up with the two, a conversation, but the med legality of team coverage, it is no joke. And the sexy thing of saying you're the team doc for this or the team doc for this, that's all great, right?
[00:34:19] Dr. Grant Garcia: Patients want to see you. You've got clout. You're solid. You know, that's, that's, that's, that is the highest level of marketing you can have as be a professional athlete, team physician, right? Like any, any, any sports guy coming out, that's the first thing they're thinking about doing, especially when you come from places like we did, right.
[00:34:34] Dr. Grant Garcia: They're just like, when are you gonna take care of the professional team? The problem is it doesn't always go the way you like. And sometimes you get issues. And we talked about the most recent one. And I want to know your opinion, but this is, this is for the viewers. This is the largest lawsuit in the history of the NFL, right?
[00:34:52] Dr. Grant Garcia: And one doctor, Dr. James Bradley, who's a great guy, great surgeon, Pittsburgh Steelers, but took care of this player. [00:35:00] And they sued him for, what, 29 million dollars, which is insane. And Rothman, who took care of the Eagles, which no longer does, got sued for, I don't know, I can't remember, 12 or 19. And they didn't even actually take care of him, they just did the rehab.
[00:35:13] Dr. Grant Garcia: So the fact that the lawsuit was dropped on them as well is absolutely insane. And this is going to change the market for teams. I mean, the teams can't even get coverage now because they're workers comp injuries. They can't even get coverage for some of these teams. Have you noticed, did you guys talk about that when it came out?
[00:35:29] Dr. Grant Garcia: Like I remember every surgeon, all my partners were talking about it. When it came out and they're like, did you hear about this? Did you hear about this? Like it's a big deal
[00:35:38] Dr. Joseph Liu: Yeah, so i'm not sure it's trickled down to the collegiate level yet Um, but we did have a specific meeting about it at the nhl team physician society And so what happened was?
[00:35:50] Dr. Joseph Liu: Um, this was, you know, like Grant said, the largest settlement that's ever been, um, you know, kind of doled out for a malpractice suit. And not [00:36:00] only was it the size, it was not, it was about future earnings, right? So there, in, in very, in certain states, there are short reform for painting suffering that's limited to a certain number.
[00:36:09] Dr. Joseph Liu: Uh, but there is no limit on future event, future earnings. And so that's basically why the number became so high, right? Um, and they just,
[00:36:18] Dr. Grant Garcia: and one second for the listeners, that's why professional athletes are the hardest, the hardest issue for malpractice because the word future earnings is killer because most insurance is like, no offense, but like if a standard person got injured, their future earnings are not going to be a hundred million dollars.
[00:36:33] Dr. Grant Garcia: Right. So, and most policies won't go that high. So that's the, sorry, keep going, but that's the reason why the future earnings is a huge deal.
[00:36:40] Dr. Joseph Liu: And so just like Grant was saying, our typical policies for just taking care of patients, right, is usually like a 1 policy. That's for just taking care of normal patients.
[00:36:51] Dr. Joseph Liu: And that, you know, that includes pain and suffering and, you know, any sort of negligence, that type of thing, malpractice associated payouts, you know, bodily harm, [00:37:00] um, that type of thing. But that's you, like Grant was saying, that takes into account what, you know, normal people are going to make in their lifetime.
[00:37:07] Dr. Joseph Liu: And so that's usually why that policy won't be maxed out. But in the professional level, there's typically not a secondary coverage that you're taking just because you're a professional, you know, a team physician. And so what, because this settlement was so high, there's never been in the history of a policy that's been that high for one individual surgeon.
[00:37:26] Dr. Joseph Liu: And so the fact that they personally had Dr. Bradley, um, uh, liable for, you know, 29 million himself was, you know, astronomical. That's crazy, right? There's no policy that's going to cover him. And then the secondarily, when the health system, you know, from Rothman was, you know, Uh, you know, on the hook for another 1 3rd, you know, basically another 1 3rd of that settlement, you know, that's how they got in trouble as well because I don't think I think the apartments themselves had to, um, they didn't, I don't think they had necessarily had secondary insurance that was that high that could cover that.
[00:37:56] Dr. Grant Garcia: Well, that's not a good day when you asked to write a check of that size and you didn't [00:38:00] even have to take care of the person.
[00:38:01] Will Sanchez: Yeah, 14. 3, right? So, um, that was their stake in what they owed. What does that do to a doctor? It, when you get sued at that level at 29. 2 million or whatever it is personally, What does that do to you?
[00:38:19] Will Sanchez: How does that affect not only obviously your wallet, but as far as you working with an institution, another hospital, like what are the ramifications at that level is it's, well, this doctor's legit. So it's just bad luck and we can move forward or do people hesitate saying. Hey, we cannot afford bringing, you know, to bring him in and have a lawsuit on our hands at that size.
[00:38:45] Will Sanchez: Can you, can you even answer that?
[00:38:48] Dr. Joseph Liu: I mean, I obviously I don't have personal experience with that number, but this is what I would imagine. There's two parts about it. Number one is. Are you insurable? [00:39:00] Right? Will insurances be with that type of settlement against you continue to cover your malpractice? Or are they willing to cover your malpractice insurance going forward?
[00:39:11] Dr. Joseph Liu: Because you have a suit of this type. size. You
[00:39:14] Will Sanchez: set the standard already, right? I mean, if you have, somebody has the same injury and something goes wrong, well, they already paid out at this. So that's where I'm starting my,
[00:39:24] Dr. Grant Garcia: well, that's a whole nother topic. Well, that's the, that's the worst part of this whole situation, which we haven't talked about.
[00:39:30] Dr. Joseph Liu: You know, just going forward, as you keep taking care of patients, you're in theory, in the eyes of the, in these insurance companies, you're much higher risk because you have this, Against your record whether you're at fault or not, right? And so this is just a statistic that you can no longer get rid of it's like kind of like getting uh, you know, a Something on your record tattoo or something like that Like that exactly that's exactly correct Um, I think the second thing is the mental aspect of it, right?
[00:40:00] Dr. Joseph Liu: Are you willing to take on you have the confidence? To take on that stress of getting someone back it at that level. That's a good It's not necessarily that you're not confident in your own surgical skills, right? But are you confident to treat them because they're going to potentially come back and bite you in the butt again, right?
[00:40:20] Dr. Joseph Liu: Meaning that are will they? If they have a bad outcome, are you always going to think what if they have a bad outcome? You treat them differently because of that. I think that is the thing that I can't answer because obviously I've never been in that mental space, but I would certainly think about that.
[00:40:36] Dr. Joseph Liu: And that's what I, I think that's what team physicians have to start thinking about. At the professional level, at the NIA level, when that much money is involved, right? Do, are these athletes going to suddenly turn around and start saying, because did you, whatever you did stopped me from these future earnings, therefore I'm going to sue you now, right?
[00:40:54] Dr. Joseph Liu: And I think that's really critical to think about. That maybe in the past we didn't think about because we were so focused on [00:41:00] the other side, the glamorous side. This is the, the very, You know, kind of the, the dirt of the, the, uh, team position side for sure.
[00:41:07] Dr. Grant Garcia: This is so important for the listeners to hear and to hear Dr.
[00:41:11] Dr. Grant Garcia: Liu's thing, because when you're a team, when you're a sports surgeon and you have some sort of clout in your community, the number one thing people ask is, are you taking care of a professional sports team? It's not how are you doing? You busy in practice? It's how are you taking care of your professional sports team?
[00:41:26] Dr. Grant Garcia: So there's a lot of motivation to do it. But the downside is there are too many surgeons I know who did sports teams who got so burnt out from the medical legal stuff or so scared that they were going to get sued by a player and lose all of their earnings for one thing. And by the way, The lawsuit, the lawsuit against this guy was not a mistake.
[00:41:50] Dr. Grant Garcia: It was actually a legitimate reason. It just somehow was able to find a way to win this lawsuit with a trauma surgeon that I went against an orthopedic surgeon. It's actually like absolutely some of these lawsuits, facial [00:42:00] professional athletes, they were on, you know, the problem you have, this guy's on, you know, guys on a contract year, he gets hurt, will can't 20 million contract if it hadn't been for you.
[00:42:10] Dr. Grant Garcia: Right. And you have a
[00:42:13] Will Sanchez: champion that goes to validate him, right? You know, I mean,
[00:42:18] Dr. Grant Garcia: because they're the because they know all about
[00:42:20] Will Sanchez: it and said he was a great player that can't get back on the field. So you have this Philadelphia Eagles Super Bowl champion that has a statue in front of the stadium saying, if it wasn't for you, He would be earning money and be back on the field.
[00:42:35] Will Sanchez: So there's a whole other aspect of it because now, now you're getting into public opinion, you're getting into fandom. I mean, we just talked to him. We started the show talking about the giants, right? So you're, you're, you're pulling on all of these emotional strings. And then you're having a decision made by a judge and now you have these ramifications.
[00:42:58] Will Sanchez: So I think going back to what you were [00:43:00] originally talking about, what happens to the Eagles? What happens to, uh, will we see a norm where eventually teams kind of take a step back because of something like this? Is there anything that you can foresee or guess that could sway a certain way?
[00:43:17] Dr. Grant Garcia: I don't think this is going to go over very well, this comment, but I'm going to say it anyways, because that's what we do here.
[00:43:22] Dr. Grant Garcia: Unfortunately, there are way too many of us young surgeons that turn into little lemmings. And we want to have the team coverage because you want to be busy when you come out and you're in private practice. I've had this experience and you open up your doors and you're, you're six months in and all of a sudden nobody's there.
[00:43:39] Dr. Grant Garcia: You got to pay the bills and you're stressed.
[00:43:42] right?
[00:43:42] Dr. Grant Garcia: Or you're two years in or three years in. And thankfully I was able to build my practice very quickly in Seattle. So for fewer years in that stress reduced. But to be honest with you, I had the same stress and I had this opportunity for potential professional athletics and I'm so glad I did not do it.
[00:43:58] Dr. Grant Garcia: But it was there and it would have [00:44:00] been very glorious to have opportunity. And Joe knows this, but you know, everyone we ever talked to, whenever we talk about how things are going, if they got onto a professional sports team, that's the number one thing they tell us. Guess what? I'm doing the trailblazers.
[00:44:11] Dr. Grant Garcia: Guess what? This team does this so that I think that's never going to go away. And unfortunately it means that young. Physicians and surgeons are going to be put up as lemmings and then eventually have some sort of burnout from something else. I don't know if Joe feels the same way, but, um, it's sad, but you know what?
[00:44:28] Dr. Grant Garcia: For some people, they really need that to boost their practice. And so I'm not faulting them for it. I just think it's, I wish there was a safer method and I wish there was more tort reform, but you know, we could go on and on about this. I don't know what you think, Joe.
[00:44:40] Dr. Joseph Liu: Yeah. So that's definitely the case.
[00:44:42] Dr. Joseph Liu: So, um, as long as they're surgeons that are willing to become team physicians, this problem is solved. We're all we don't have the leverage basically if that's what you're I think that's what you're pointing to is At this level from the team position level that you don't have leverage against this type of possibility, right?
[00:44:59] Dr. Joseph Liu: You certainly want [00:45:00] um You know our surgeons society is to kind of police themselves to make sure that surgeons are At an appropriate level to take care of these athletes and you're doing the right thing And I think that's also you know, just to point out that you had talked about previously who is kind of testifying on this athlete's behalf and drawing, you know, tugging on their heartstrings and things like that.
[00:45:20] Dr. Joseph Liu: The biggest issue is that, you know, in these medical legal cases, as you're trying to, you know, Basically, you're trying to basically convince these, the jury who are, you know, typically lay people, not medical people on purpose, right. Kind of the nuances of these surgeries. Right. And I think this is a very nuanced situation in terms of what Dr.
[00:45:39] Dr. Joseph Liu: Bradley decided to do in the, at the time of surgery that, you know, the lay person doesn't necessarily understand. And I think that's the complexity of surgery and sports medicine, especially at the highest level is that it's not just. One or the other there's not one right answer and often it's a judgment call of what you see at the time of surgery in the context of the what you see [00:46:00] in the rest of you know the athlete's you know body or the joint or whatever we're operating on it's not just the one thing that they're talking about right and so I think that's very hard to describe to the lay person and so a trial by peers is You know, not perfect because of the fact that the people that are actually sitting on the jury don't have the education to make such a, um, you know, the call to say someone's truly liable or negligent in this situation.
[00:46:26] Dr. Joseph Liu: And I think that's what's required in malpractice, right? These, you know, is the, is the negligence portion.
[00:46:31] Dr. Grant Garcia: And the problem you have too, is the experts. that they find they have trouble getting the good experts, right? Nobody's going to go against James Bradley if they think what he did was legitimate, right?
[00:46:41] Dr. Grant Garcia: Like you've gotten calls with Joe. I've gotten calls to be an expert witness against a sports surgeon that did something legitimate. I mean, I got a call six months ago. The surgeon did very little, definitely not enough to get sued. And I was like, I'm not testifying against them. That was completely legitimate.
[00:46:58] Dr. Grant Garcia: But of course, you know, [00:47:00] like they're going to find somebody eventually, right? And that's the problem. So it's a whole nother ballgame. I, we could keep going on this. I got a few more minutes. I got what I do, but I want you do your follow up question. Then we're going to go to NHL. I want to NHL's decision.
[00:47:13] Dr. Grant Garcia: So you do your follow up question. And then cause we're going to go all night. Will we do this all the time?
[00:47:17] Will Sanchez: I definitely go all night. So can you see a world where the contracts change? Between player and team, where, where the team is protective when it comes to, uh, the medical treatment and also maybe combining that with insurance policies, which we've seen, but I don't know if every player has them.
[00:47:42] Will Sanchez: So with the insurance policies covering the player and also the contracts that the player signed with the team, as long as you know, if you're going using our. Physicians or facilities or something like that, where maybe something is put in place where everyone is getting [00:48:00] something out of it, if something goes wrong, where someone's not getting smeared, if something happens, players are insured, can you envision something like that?
[00:48:08] Will Sanchez: I know there's certain things in place and some players have it, but I don't know if that's across the board.
[00:48:14] Dr. Joseph Liu: Um, so I think this might get at Grant's point that we're going to talk about very shortly, but I think. You obviously want players to earn their money, right? And so as all of these sports become more and more popular, they're just more and more money involved.
[00:48:27] Dr. Joseph Liu: And that's why these numbers are just going up and up, right? Our contracts nowadays for. You know, all of these sports are two, three times 10 X, what they were 10, 20 years ago. But it's also
[00:48:39] Dr. Grant Garcia: 10 X compared to the average population, right? They've gone up exponentially higher than all of us. Normal earners, right?
[00:48:46] Dr. Grant Garcia: We just, there's no way that we can't match the exponential growth of them. So that's a problem too, but keep going.
[00:48:51] Dr. Joseph Liu: So basically, and I'll bring this up a little early, um, is that, you know, when the NHL team positions were started to talk about this dilemma and, you know, [00:49:00] who should be coverage covering it, you know, they, they started to talk to the players association as well as the league.
[00:49:05] Dr. Joseph Liu: And I think what they came up with is that in, um, that probably the, the person that makes them, or the entity that makes the most sense to cover or provide kind of the secondary coverage is the league itself, right? Because that's where all the money's funneled through. Uh, and so if the league, you know, and that allows team positions to do what they are supposed to do, which is take care of players in the best way possible, not think about these consequences.
[00:49:28] Dr. Joseph Liu: And so if you have this larger entity that kind of obviously wants the best for their, you know, wants the players to do well and be healthy because that's their, you know, that's their product. Right. And wants their team positions to be available to keep taking care of. Um, players and not be afraid of kind of the possibility of these lawsuits occurring, then all of these leagues that have, have all this revenue that's then ultimately divided amongst the teams and the players, if they are the entity that covers them, then that's going to be the one, the entity that has the most amount of money that can cover them, right?
[00:49:58] Dr. Joseph Liu: So whether the, you know, I [00:50:00] think ultimately if they're, we're able to, they're able to come up with an agreement with all of the, you know, team positions, the team position society, as well as the players association and say, okay, well, you know, the league is going to head, you know, kind of. lead this kind of secondary insurance policies above and beyond what they carry normally, right?
[00:50:16] Dr. Joseph Liu: You don't need it for, you know, normal malpractice. You need the secondary insurance for basically, you know, out of this world settlements like, you know, the most, right, exactly.
[00:50:25] Dr. Grant Garcia: So this is amazing. What Joe just brought up as many point and the people, when they listen to this, These NFL teams literally have dead money and every year because they trade a player that's atrociously playing and they paid them so much money.
[00:50:40] Dr. Grant Garcia: 29 million dollars is like a rounding error for some of these teams. But meanwhile, you have James Bradley and Rothman that literally are like, sunken because of this lawsuit. And if the NFL literally could do this, it would be a game changer for all team positions and they could really take care of their players.
[00:50:58] Dr. Grant Garcia: And it would be no, this would be very little [00:51:00] burden, to be honest with you. I mean, the largest lawsuit ever is that big. I mean, that's like one year salary for one of these players. I mean, it's not like
[00:51:07] Will Sanchez: it's less than a year salary for Daniel Jones. Enough said, and
[00:51:12] Dr. Grant Garcia: that's, that's, that's saying a lot. So my point being is that what Joe is getting at is that is the future.
[00:51:20] Dr. Grant Garcia: And the only way you're going to get the best surgeons and the best people to take care of the players and they can do their best. And it's not going to incentivize us to do a poor job. It's going to send us to do a better job because when my number one concern, when I was offered to do more professional teams and I wasn't going to be fully employed and it was going to be a contractual relationship is that if I touch the player, I'm going to get sued.
[00:51:40] Dr. Grant Garcia: If there's a problem and I'm not protected in Washington state, we have employment laws that actually protect this situation. So if you're a team physician, but you're in fully employed with the sports team, supposedly you cannot be. sued by the sports team. So this would not happen in Washington state, which is interesting.
[00:51:55] Dr. Grant Garcia: And so we have very strict employment laws. Now, again, it may have changed recently. [00:52:00] That's something that's not in most of these states. It's clearly not in Philadelphia. Philadelphia is the largest Joe knows. This is the largest per capita of lawyers in the country, right? You just, you just, you run into a lawyer when you walked on the street.
[00:52:12] Dr. Grant Garcia: I mean, that's just, this is just the way it goes when I trained it, uh, in Penn. But this isn't, this is just really important. People understand there is a solution for this. Um, I just think the greed of the NFL needs to be fixed and uh, you can see this right now. I mean, it just protect your players, let them get the best possible treatment.
[00:52:31] Dr. Grant Garcia: And every team physician's thinking this when they're thinking of the player, they're worried about this. It doesn't matter who they are. I've, we've talked to, we've had seen so many amazing surgeons we've worked with and this is one of their concerns. I mean, it's right, Joe. It's medical legal. Everyone's concerned.
[00:52:45] Dr. Grant Garcia: No one wants to talk about it.
[00:52:47] Dr. Joseph Liu: Yeah. I mean, I think you're just, you're covering your eyes and you're covering your ears and hoping for the best, right? When you're taking care of these players, obviously, I think, you know, ultimately all of these leagues that, you [00:53:00] know, have all the revenue. They're the ones that have the deepest pockets to be able to cover these.
[00:53:04] Dr. Joseph Liu: And it's going to be up to, you know, the negotiating power of these teams. physician societies, as well as, you know, and as long as the players, I think associations are also on the same page. I think there will be enough leverage to hopefully get these kind of, um, entities to cover, cover the, uh, cover the physicians.
[00:53:20] Dr. Grant Garcia: Well, I think maybe the hope of this NHL thing is that it shows the other teams that they could do it. Um, and. I hate to say you keep saying the word deep pockets, but this isn't very deep. I mean, it's like I said, this is the rounding errors for NFL. Like there, how, how often will, and Joe, are there's, is there money that's like these teams when they, they get rid of a quarterback mid season, right.
[00:53:41] Dr. Grant Garcia: Who's done terrible. And it's got like 29 to 30 million of dead money. And we're talking about like a lawsuit here against the, one of their team physicians. For a, for a one single instance, that was likely not even negligence, right? It was, there's, from what I've understood about it, this is, this is, again, we know this is [00:54:00] extreme situation, but many of these are like player just can't play and they didn't get back to what they wanted to do.
[00:54:05] Dr. Grant Garcia: And so it's really important for people to understand that this is not a huge financial burden for these teams. And it's just, it destroys physicians who are doing teams and you don't get the best people, in my opinion, don't get people that you don't, you don't get the cream and you don't get your full pick, right?
[00:54:21] Dr. Grant Garcia: It's just, it's just the way it is, or you get people and they're scared. So it's just, it's a, it's a sad state. But again, we're not here to depress the viewers. We're just here to give them information.
[00:54:32] Will Sanchez: I see. You got five minutes because you just, you don't let Dr. Lou talk and you're jumping in all over the place.
[00:54:38] Will Sanchez: I'm so excited. I'm so
[00:54:39] Dr. Grant Garcia: excited to talk about this.
[00:54:42] Will Sanchez: It's all right. I stole a lot of your time, man. It was my bad. Listen, uh, how do you work your, uh, work life balance, uh, Dr. Liu? Just, uh, you know, you're busy, USC, and Kings, and, you know, dealing with Dr. Garcia. That's taking up all your time. What are you doing for, uh, for fun?
[00:54:59] Will Sanchez: And what's your work [00:55:00] life balance like? Just so, uh, just so we know here.
[00:55:02] Dr. Joseph Liu: Yeah, I think that's really critical for our longevity in any career. Uh, and, uh, I think now that I've come, uh, uh, Grant is gonna make fun of me because I used to be the most, uh, frugal person that he knows, and he might still be the most frugal person he's ever known in his life.
[00:55:17] Dr. Grant Garcia: He definitely is. This kid, this guy could retire. He's so frugal.
[00:55:21] Dr. Joseph Liu: But, I think, uh, you know, just finding, uh, Time on a daily basis to keep yourself, to keep my body healthy, as well as my mind healthy, working out, going to the gym, I think travel, you know, broadening your horizons, I think, you know, spending all your time working, I think that's, if it's, obviously, I think it does give someone purpose, but I think, um, going outside, learning about new things, I think learning about new cultures, uh, diversity, that kind of thing.
[00:55:47] Dr. Joseph Liu: I think that's the way to stay grounded in the fact that, you know, there's more than to life than just work. There's more to life than just taking care of sports. There's more to life than just doing surgery. Um, I think getting to know [00:56:00] new people, I think that's always exciting. I think that's, you know, but in a, in a situation that's not medicine, right?
[00:56:04] Dr. Joseph Liu: I think that's the interesting part, right? Um, that's what gives me joy. I think travel does that because you're, Uh, instantaneously going to go to a different place, uh, a walk of life that you may not have, um, You know, been able, been exposed to in the past. And I think, uh, you know, my girlfriend is loves to travel.
[00:56:21] Dr. Joseph Liu: She, you know, she's hit more countries and she she's gone through more passport books. As you're
[00:56:26] Dr. Grant Garcia: hearing the girlfriend changed him. Thank you.
[00:56:30] Will Sanchez: Have you gotten the, gotten the travel itinerary from Dr. Garcia? Right. And you know about this.
[00:56:38] Dr. Grant Garcia: Thankfully we're running out of time. So Joe can't tell me.
[00:56:41] Dr. Joseph Liu: I should be a separate podcast.
[00:56:43] Dr. Joseph Liu: If it hasn't already been featured.
[00:56:45] Dr. Grant Garcia: It's a, well, first off, I just want to tell everybody the, one of the best parts of my job as orthopedic surgeon is also the colleagues that I met and my friends and Joe's one of my best friends [00:57:00] and it's awesome. To be able to talk about random stuff, work stuff, anything.
[00:57:05] Dr. Grant Garcia: And honestly, I have a lot of work life balance, but the decompression, when I have a tough case or when stresses like not hopefully this level come up, I have someone like Joe that I can call and I would tell you, I've bounced, he's heard me talk way too many times and I've, he's bounced stuff off me. Um, and that's really the key to longevity.
[00:57:24] Dr. Grant Garcia: In practice and taking care of people, uh, because as much as we want to be perfectionists, nothing's perfect in life and we can bounce things off. And I am better because of friends like Joe and I hope that Joe's better because they're friends like me. And so that's what this really is important for the podcast too.
[00:57:40] Dr. Grant Garcia: Obviously we talked a lot about medical legal, but we both fricking love our jobs, right? But I like my job too, because I have people like Joe that I can talk to and I feel really good about my decision to do this thing. So thank you, Joe.
[00:57:53] Dr. Joseph Liu: No, thanks, Grant. I, I definitely want to echo Grant's sentiments about, you know, even though we're, a lot of us are [00:58:00] taking care of patients one on one, I think number one, it's, you know, our collaborative experiences from our training, you know, training, training with the best of the best and the greatest in orthopedics and sports medicine.
[00:58:11] Dr. Joseph Liu: And then it's not a community. You know, once you're in, so, you know, practice on your own, you don't finish learning, right? I think it's a lifelong learning experience. You continue to talk to friends and colleagues, uh, about difficult cases. Um, and you know, I I'm still learning every day with every patient.
[00:58:30] Dr. Joseph Liu: Um, I think that's the most, the best thing about orthopedic surgery, about sports medicine, is that not everyone is exactly the same, and everyone has their own story, and you can treat them, you know, you just need to treat them with kindness, and, uh, you know, understand that Okay to have a team behind you to give them the best possible care.
[00:58:51] Dr. Grant Garcia: Thank you so much, Dr. Liu. We really, really appreciate you coming on and normally we could keep talking, but we're going to go past an hour and Instagram does not like an [00:59:00] hour.
[00:59:02] Will Sanchez: Hey, we just want to, we want to thank everybody. We want to thank your time. Check us out at sports. talk. com. We have episodes, transcripts, you name it.
[00:59:10] Will Sanchez: Uh, we're going to get, uh, Dr. Grant Garcia's, uh, travel itinerary. It will be bigger than war and peace. Uh, so just be prepared. We'll see if we could do a cliff note version and we have to get a Dr. Lou talking about, you know, all of the travel shared here and, uh, everything that Dr. Garcia has done. Thank you, Dr.
[00:59:32] Will Sanchez: Lou. Thank you. Thank you, Dr. Garcia. our favorite orthopedic sports medicine specialist. And we, as always, we want to thank the listeners. Say goodbye, everyone. Thank you. Bye.
Audio Transcript
Lonzo Ball returns to the 2024 NBA season after cartilage surgery
Lonzo Ball returns to the 2024 NBA season after cartilage surgery
[00:00:00] Will Sanchez: Welcome to Sports Doc Talk. I've got our orthopedic surgeon, sports medicine specialist, Dr. Grant Garcia, Will Sanchez, Dr. Garcia. I mean, your background says it all. It's incredible. MBA time. I got to be honest with you. I'm a Knicks fan. I'm a little triggered from all the Jordan and Pippen beatings, but I'm going to, I'm going to excuse.
[00:00:39] Will Sanchez: I know you've worked with them in the past and I know you have some affiliations, so I'm gonna let it go. But before I ramble on and get excited about our show, how are you? And are you a bulls fan?
[00:00:51] Dr. Grant Garcia: I'm not a bulls fan. So first off, I don't want to throw off the viewers. We're going to, we're starting to do some stuff.
[00:00:56] Dr. Grant Garcia: You never know what's going to be on my background. So today we're going to talk about. [00:01:00] Obviously took care of the bulls. You know, working with them was awesome. Um, but the player we're gonna talk about today, which we'll go after in a minute is Lonzo ball, who is currently going to be starting with the bulls.
[00:01:11] Dr. Grant Garcia: Let's say three days, right? Thursday, I think is the start of the season.
[00:01:15] Will Sanchez: Yeah. So, um, that'll show will be the morning of, uh, the start of the season for them. So we're really excited about this 20, 24, uh, 2025, like I said, I'm a Knicks fan, so I'm hoping for good things this upcoming season, but for the business that you're in and what we like to talk about, um, This is right up your alley.
[00:01:35] Will Sanchez: We talked about it in the show previously, but before we get into that, because we're going to talk about recovery and this is kind of what we do. Let's talk about the recovery shop. Take it away.
[00:01:47] Dr. Grant Garcia: So again, thanks for our sponsors. Uh, we've heard this before, but this is what's essential for these big surgeries.
[00:01:53] Dr. Grant Garcia: You get these big surgeries, patients like professional athletes, regular athletes, college athletes. They were like, what do I, can I do? I need [00:02:00] what you're doing is good. But I need more. Yeah. Right? So what can we offer? So as a surgeon, we can have a place like this as a landing page and the surgeons can offer their patients that they go there or they get a call from the recovery shop offering these services and they can buy a bunch of these different things that they want.
[00:02:16] Dr. Grant Garcia: Different advanced ice machines, advanced recovery machines. You know, we got scar creams, uh, we got special bending machines. I mean, pretty much anything you want, you can put on there. I mean, that's the nice thing about this. It's not like you have to stick with something and it's something you value. So if it's something different that you want, you can talk to them.
[00:02:33] Dr. Grant Garcia: They can do it again. Obviously there are sponsors, but I get no affiliation if you sign up. Um, so just, you know, check it out, contact them as a surgeon. It's always good to have this. armamentarium because the patients are going to ask for it. Don't pretend like they don't, you know, you unfortunately have way too many visits where the patients come in, they go, what else can I do?
[00:02:49] Dr. Grant Garcia: And you'll say, well, you got this or this, you know, we can offer nutrition. So it's been an awesome outlets for my, for my patients.
[00:02:57] Will Sanchez: Yeah. And let's get kind of get started about, uh, [00:03:00] today's show. You know, we, uh, we talked about it last year. just the concern, right? And you know, when we're talking about Lonzo ball, you know, when we heard about his injury, um, he's had, I believe three arthro arthroscopic surgeries since the 2021 2022 season, which would be 2022.
[00:03:18] Will Sanchez: I believe the last time he stepped on the court was January, 2022. So he's finally been cleared after the torn meniscus, which has happened twice the surgeries. You know, we talked about it. Very concerning. This is something that most likely this player, even at such a young age in his twenties, may never play again.
[00:03:45] Will Sanchez: But now there's the chance he stepped on the court for the first time during preseason. He got a chance to play. Um, why don't you tell our listeners and viewers more about the injury that leading up to it and the procedure that he had, because, [00:04:00] um, like I said, we both discussed it and we didn't think that this was something that he may come back from.
[00:04:05] Dr. Grant Garcia: So first off this episode, I'm really excited about, uh, many reasons. First reason was when we did this initial show, you can go back and listen to it. We did not know that he had his meniscus replaced because it was never announced. We said we had an entire show, one of our hottest shows on the internet about cartilage transplants.
[00:04:26] Dr. Grant Garcia: Yeah. And we talked all about cartilage transplants, the recovery and everything else. And then all of a sudden, like six months ago, it came out that he had a meniscus transplant and a cartilage transplant. Which is a humongous surgery and that's near and dear to my heart. And there's a couple of reasons.
[00:04:42] Dr. Grant Garcia: One, this is my, this is my absolute favorite surgery to do. This is my absolute favorite surgery to take care of patients. This is a highly niche practice. There are a few very few people in each state that do this. So this is a very cool that I can talk about this in an NBA player. And [00:05:00] finally, The most cool part of this is the person that taught me how to do meniscus and cartilage transplants, who did this on Lonzo Ball, is the person that did it to it.
[00:05:10] Dr. Grant Garcia: Dr. Brian Cole, the godfather of cartilage and meniscus transplants. So, and, happens to also be the Bulls team doctor. So this is a, Awesome conglomeration of everything that I've worked for, for since I've been here to talk about this and to be able to show off this, this really cool procedure, you know, patients know about this, they come in asking about it, but, and we tell them it's for recreational athletes, professionals have never gotten it before.
[00:05:35] Dr. Grant Garcia: A cartilage transplant, but the meniscus transplant is even the next level. And so now we're about to see an NBA player who's already played preseason play in his first professional NBA game. The first player in history to have this type of procedure. I think he's the first player with a cartilage transplant and the first player with a meniscus.
[00:05:51] Dr. Grant Garcia: And they decided to go after both at the same time. And we can explain that in a minute why they did that. But this is a humongous deal. It's a technical surgery. [00:06:00] And it has obviously its own risks, just like any other surgery, but let's roll through the slides for the, for the viewers. They can understand what he did.
[00:06:09] Dr. Grant Garcia: Now I have inside information. Not only do I do this procedure, but I've done this procedure with the person that did the surgery on him. So I can tell you, this is exactly how he did it. So this is really cool. So on the left hand side, you see the black and we'll please chime in because for the viewers, I I'm going to, I'm geeking out right now.
[00:06:27] Will Sanchez: Yeah, I know. I'm just giving you a little room to breathe and stuff. Cause I've got some follow up questions, but go ahead, man. You're like a little kid in a candy store. I know.
[00:06:36] Dr. Grant Garcia: Okay. Thank you so much for the opportunity. So the. So the meniscus transplant you see here on the left. So what we do is this is called a If you're not
[00:06:44] Will Sanchez: watching this, and it's a great way to promote our YouTube page.
[00:06:48] Will Sanchez: Uh, Dr. Garcia has got a smile ear to ear. I mean, he may hurt his cheeks from smiling so much. I'm sorry to interrupt. A mental
[00:06:56] Dr. Grant Garcia: break. I got a mental break after this. I'm too excited. So, and we [00:07:00] got to keep this short because it's supposed to be a blast episode. As you know, we do a good job of that.
[00:07:03] Will Sanchez: Yeah.
[00:07:03] Dr. Grant Garcia: Okay. So, so first off, this is the meniscus transplant. So you can see here, now this is a lateral one. I'm pretty sure he had a medial one. That's more common with the issue he had, but nonetheless, gets his meniscus removed a few times. All of a sudden gets a hole in the meniscus or a hole in the cartilage, as we talked about.
[00:07:19] Dr. Grant Garcia: And then all of a sudden has no meniscus left either. The problem you have and what some surgeons do is they say, Hey, the meniscus is really hard. The meniscus is the hardest part of this whole surgery. So let's say the surgeon skips that, right? That's not good because now you've lost the cushion. You need to get all three things fixed.
[00:07:34] Dr. Grant Garcia: The cushion, you need the tibial plateau and you need the cartilage to be good. The tibial plateau is usually not the issue, which is the bottom part of the tibia right here below where the transplant is. Then you have the meniscus transplant and then you have the cartilage portion. So if you fix the hole, you fix the meniscus and the plateau is good.
[00:07:49] Dr. Grant Garcia: Then you have a good knee again. And right. And that's where the pain goes away and allows you to get back to activities. So the way he did this, as you see here, this is like a keyhole. It's actually crazy. It's just like woodworking. So [00:08:00] you cut that hole in, um, And then you slide the meniscus in like that, but you don't see here.
[00:08:04] Dr. Grant Garcia: And I didn't want, I couldn't find any images that were not gross for the viewers. So I apologize, but you attach it with stitches. Now that looks like it's really simple, but this is one of the most technically challenging surgeries that we do in orthopedic sports medicine because of all the nuances and little complications that can occur when you do this.
[00:08:21] Dr. Grant Garcia: So you do all that. And then on the same time, On the right hand side and this surgeries happen at the same time. This is not something you do separately and you come back. So you, I mean, Dr. Brian Cole is amazingly skilled at this and he's very efficient in the operating room. You take a piece of cartilage from someone else that has passed away.
[00:08:38] Dr. Grant Garcia: Generally someone younger. It's unfortunate to talk about it like that, but you that's the way it is. They just recently passed away three to four weeks. So it has to be fresh. And when you get it, you do some things, prepare it, and you actually core it out just like a bone dowel. So, so you see here, it's a bone plug, and you push that thing right back in.
[00:08:55] Dr. Grant Garcia: You generally don't need any screws or anything else. It literally just press fits. It's designed in the system to do [00:09:00] that. And those two things together are going to instantaneously give the patient a better joint surface. And then you're talking about a long recovery. I mean, Lonzo Ball's recovery was more extended than I would do for a regular athlete.
[00:09:12] Dr. Grant Garcia: I think they
[00:09:12] Will Sanchez: said it was 18 months or something like that. I mean, that sounds unreal to have a recovery that long for the surgeon. Go ahead.
[00:09:21] Dr. Grant Garcia: But you know what? He had bone edema. He had other issues going on. What's bone edema
[00:09:25] Will Sanchez: for those? I don't know.
[00:09:27] Dr. Grant Garcia: Obviously, he's starting to get like basically that means the bone is not happy, right?
[00:09:30] Dr. Grant Garcia: He has no meniscus. He has no cartilage and he's on that pre arthritis stage So if they don't do something soon, this is going to go really poorly, which is why he had so much pain, right? There are athletes i've taken care of nfl athletes Nba athletes that have had early arthritis or arthritis in their knees and they're fine, right?
[00:09:46] Dr. Grant Garcia: It hurts but they can push through it Lonzo ball clearly had something else going on the swelling the constant pain that he had but His knee didn't react very well to losing that meniscus and it doesn't happen to everybody. Um, he's just lucky that everything else [00:10:00] was in his favor. Good ACL, good everything else.
[00:10:02] Dr. Grant Garcia: So he basically had this special surgery, which again is incredibly unique. It's not unique in general, probably do. I mean, I think Dr. Brian Cole probably does 60 of these a year. He probably does a hundred cartilage transplants a year. You know, I do 20 of these a year with cartilage about 45. So it's not uncommon that we do them.
[00:10:23] Dr. Grant Garcia: I do one every couple of weeks, uh, but to do it in a professional athlete is, uh, is the next level. So this 18,
[00:10:30] Will Sanchez: I'm going to interrupt you as we go along. Why is that something that becomes a risk and why you normally wouldn't do it on an athlete like this?
[00:10:40] Dr. Grant Garcia: So first off, very few people have the. Have the cojones to go after the, be the first one, right?
[00:10:45] Dr. Grant Garcia: No one wants to be the first one with a surgery like this. If it fails, right? Like let's say Alonzo ball goes out in two weeks. And again, I hope not. I don't think it's going to happen. He's obviously been checked a million times. I'm sure he's had way too many MRIs to make sure everything's looking good.[00:11:00]
[00:11:00] Dr. Grant Garcia: Uh, and I'm sure Cole's seen him. I'm sure other people have seen him and make sure that he's cleared and ready to go. Right. There's no way the Bulls are letting him put in an experimental NBA thing and then go after it. Right. The surgeon experimental, but it's the first time done on an NBA player. Yeah.
[00:11:13] Dr. Grant Garcia: So the idea is that like that's, that's the big problem here, right? That's what we have to worry about. Like, what else, what else is going to happen? So what can happen is you can tear your meniscus again, right? The meniscus, even though, so that meniscus transplant is from somebody else. It's a cadaver as well.
[00:11:30] Dr. Grant Garcia: Now, those are frozen. And the cartilage is fresh. So the cartilage sustains itself better. Those less likely damage themselves. So other professional athletes have gotten cartilage transplants. There was a hockey player that just recently got it from Brian Cole. There's a few other athletes that have had the cartilage transplant.
[00:11:45] Dr. Grant Garcia: Those are way more durable. Those are way more solid. Like I do those and I kind of set and forget. I mean, people can have issues with them, but it's just not as often. The meniscus, the meniscus has three zones. There's the zone with the blood supply. That's the very far back [00:12:00] zone. Then there's the middle zone and there's the white zone, which is the edge.
[00:12:03] Dr. Grant Garcia: And you can see that here when the meniscus transplant heals. And it's pretty crazy. I just scoped someone last week that had a meniscus transplant. You can't tell all the sutures have dissolved. Everything looks like it's a regular meniscus. I grab, sometimes I grab a nurse in the room and I say, Hey, what is this real or not real meniscus?
[00:12:18] Dr. Grant Garcia: And they can't tell. So they look the same, which is amazing because it's been from somebody else. The, that little layer, the layer without the blood supply never gets integrated into the rest of the body. And so there's a risk of tearing again. It's a little more brittle. It's a little more fragile than maybe the one you were born with.
[00:12:35] Dr. Grant Garcia: You know, obviously nothing's as good as what we were born with.
[00:12:38] Will Sanchez: Yeah. But.
[00:12:39] Dr. Grant Garcia: And it depends on you. Well,
[00:12:40] Will Sanchez: can I assume that depending on the age of, of where you're getting this transplant from can also be a factor as far as let's say, you know, like Lonzo balls is 26 years old, you know, and if you got a replacement from someone that was in their twenties, you know, maybe that is a little bit more stable and stronger compared to [00:13:00] someone that's older.
[00:13:00] Will Sanchez: Can that be a part of making the decision making when you're selecting a transplant? That specific, um, you know, part of the body for the transplant.
[00:13:10] Dr. Grant Garcia: That's an excellent point. So the answer is we rarely would put something older than 30 to 30 years old in a knee like his. I'm sure he got something younger than him.
[00:13:21] Dr. Grant Garcia: He got a patient younger than him. It's just, that's unfortunate. Unfortunately, there's way too many, Bad things that happen out there. And we have a lot of these transplants to do. And again, I don't want to go into the ethics and, you know, stressfulness of the situation of getting donors. Um, but yeah, it's real.
[00:13:37] Dr. Grant Garcia: I mean, it's, we all know what happens. Listen, I
[00:13:40] Will Sanchez: I'm a donor. Gaffa bits. You know, when my time comes, if there's anything still working, please take it. And it's really
[00:13:48] Dr. Grant Garcia: nice too. Like what you can do and you do these, my patients will write letters to the family. that donated. And so you can actually, I've done my, I mean, I did one of my best friend's wives and she got [00:14:00] a cadaver ligament for her ACL and she wrote a really nice note to the family.
[00:14:03] Dr. Grant Garcia: And actually they, that's really cool. I get it frequently. My patients do it cause I do a lot of these. Um, and it's a really cool thing you can do. Uh, and again, I'm sure it makes the family feel better that they went to, went to a good cause and made a patient feel better and made someone feel better. So.
[00:14:17] Dr. Grant Garcia: Anyhow, on that, on, on back to the topic, the recovery 18 months is pretty long, but not for, uh, athlete of his level, you know, these, the average return to sport on these is about 10 months to a year. Um, and I have my patients, you know, the thing is, what's crazy about these is he probably felt pretty fricking good by about 8, 10 weeks, you know, there don't usually feel, they feel a difference in their knee very quickly.
[00:14:41] Dr. Grant Garcia: Despite how big of a surgery this is, but he probably had to reduce that bone inflammation. He probably had to reduce all that stuff and he had to strengthen his knee. And also because he's an NBA athlete, I'm sure they were just going super slow with him. I mean, one of the things that
[00:14:57] Will Sanchez: they mentioned was, Oh, one of the articles I read was [00:15:00] that he had to relearn to walk.
[00:15:03] Will Sanchez: Now, why would that be something that happens? Is it the procedure? It is it the way you want it to heal a certain way. So even though you're saying you're going to feel a certain way, eight to 10 weeks that you want to make sure that you're not advancing. So why is that?
[00:15:20] Dr. Grant Garcia: I'm so glad you're on here. Well, this is great.
[00:15:22] Dr. Grant Garcia: These are the questions that I don't, I just assume people know. So this is excellent. So when you get a meniscus transplant, you cannot put weight on it. For up to six weeks or so. So the first four, again, it depends on the surgeon. It depends on the procedure you do. It depends on your comfort level, but generally four weeks of no weight on this.
[00:15:41] Dr. Grant Garcia: So, and then two weeks of sort of partial weight, I think Cole's very similar. So by six weeks, you're walking pretty normally, maybe more aggressive walking by seven, eight weeks. Right. So that's the, that's the thing here is he had to relearn to walk. One, he probably was limping or having pain frequently.
[00:15:58] Will Sanchez: Yeah.
[00:15:58] Dr. Grant Garcia: And two, and generally his pain [00:16:00] pins are not doing very well when they start beforehand. And then he had to learn to walk again. And then he probably was walking abnormally. Because he was probably hurting right enough. They shut down so many times. Um, I mean, he basically, I don't think he was probably normal with his knee for two to three years before this.
[00:16:18] Will Sanchez: And, and who knows if he was normal or what we, you know, quote unquote normal because he had already had an injury prior to the one that set them back to where he's at right now, uh, with that meniscus injury or the meniscus tear, uh, prior. So, um, and also we've talked about it, right? You're laid up, you're losing strength, you're losing muscle.
[00:16:41] Will Sanchez: Um, just everything that kind of goes into it, right. We've had different discussions now to saying that this is something that they use, but you know, we've talked about peptides. We've had different conversations with different people, amino acids. How do we, you know, get certain things. So, you know, it'd be great to know what was the goodie bag, right.
[00:16:59] Will Sanchez: If we're [00:17:00] going into Halloween, right. to look into our bag of goodies and what did the doctors put in there to try to help him even though it's such a long process to get them going as fast as they can.
[00:17:11] Dr. Grant Garcia: A hundred percent. I'm sure there was more than you could possibly imagine. I mean, I've, I've had to take care of some of these bulls players and the screening tests we do for them, you would, they're not normal, you know, you're getting like checked for literally everything, right?
[00:17:24] Dr. Grant Garcia: They're getting, they're getting way more information. They've got, Cutting edge technology above what we have. Like we've shown before, you know, guardian caps, uh, Q collar, plenty of other technology that makes it to the NBA much faster than we would make. Right. They don't, there's no insurance costs. They don't care about that.
[00:17:41] Dr. Grant Garcia: They've unlimited supply of money and they're like, whatever it takes, let's do it. It's cutting edge. It's not going to hurt. The player and it's going to give him a leg up. Let's do it. So you, yeah, no, they're, I mean, they're, they look like, unfortunately, the NBA training rooms look like a science experiment because they've got all these different little potions and things there that you, that we [00:18:00] don't even have, we don't even access to yet.
[00:18:02] Will Sanchez: We've talked about recovery plenty of times, right? H robotics, rebel list, things like that. What would be something that they would use for Lonzo in this healing procedure?
[00:18:14] Dr. Grant Garcia: So this is what I use as the rebus for. This exact surgery. So this procedure. So basically he gets this surgery and I'm not sure if Cole used just our standard bending machine or he used, I mean, he didn't use the rebless, but another machine of some similar thing, we start using that right away.
[00:18:30] Dr. Grant Garcia: And that we used to use those bending machines for everything, ACL, you name it, but that's also a little more old school. But now with these machines, you want the patient to get bending because as he bends, he, he, he, he, He puts fluid through his knee. It's like lubrication and it gets the things moving and he wants to put a little bit of Bend on it because it actually pushes that meniscus out To the capsule where you want it to heal to and with the transplant it keeps it flush, right?
[00:18:55] Dr. Grant Garcia: So he's checking up before he finished the surgery He's gonna re scope at the knee be like that all [00:19:00] looks perfect Everything nothing's moved since I've bent the knee and then he's gonna let him bend his knee to try to get him back because you Want him in like week one or two to have very little pain and to be really moving that knee really well You Like by week six, you want them to let them loose.
[00:19:12] Dr. Grant Garcia: And you're going to say, go to full motion and you want them walking smooth, glide, no issues.
[00:19:18] Will Sanchez: All right, so it's not Lonzo's leg, right? So I'm gonna take Lonzo's leg out of it. Dr. Garcia has just had this operation done. What's the normal, and I know everyone is different, so just for our listeners to take it with a grain of salt, what's the normal progress for the bend?
[00:19:34] Will Sanchez: So if the, if the leg is straight, completely horizontal, you know, That week, first week, two weeks, whatever it is, what's the degrees that you start to implement? And if everything is on on par and going the way you want it as a doctor, when do we get to that 90 degrees, uh, in that timeframe?
[00:19:54] Dr. Grant Garcia: So it's actually fairly quickly with these, which is pretty impressive.
[00:19:58] Dr. Grant Garcia: I mean, I would say [00:20:00] I start them. I let them go all the way to 90. If they can in the first, Week now most people can't the first week if they get swelling everyone's different like you said But I let them go to 90 and I want them to keep going to 90 Repetitively because as you know after a surgery, especially a big surgery your swelling is going to keep coming back So you can't you gotta if you set it and forget it and then you stop doing it.
[00:20:20] Dr. Grant Garcia: It's going to lose motion again So you have the motion? Of the knee and the motion of the shoulder, but really mainly the knee for these surgeries is so important It's so important that that's why we give people these machines You So they can do bending. I mean, my patients talk about falling asleep in the machine.
[00:20:35] Dr. Grant Garcia: So they're just falling asleep and they get six to eight hours of just bending their knee while they're sleeping. And that's a really, really good thing for the knee. There's no damage caused by this. If you're worried about damage, then you did the, the surgery was not, uh, up to par. Um, so it's, uh, it's really important to have that aspect.
[00:20:53] Dr. Grant Garcia: So it's a good question. So then progress for me outside of the bending, you know, walking [00:21:00] fairly normally at six weeks, seven weeks. That's when you start to be like, Hey, how are you feeling really? That like up to three months is when you start to really notice a difference in your knee. Um, three months doing some elliptical ish stuff.
[00:21:12] Dr. Grant Garcia: Running, it's going to be like five, six months. Now again, this is, this could have been delayed more with Lonzo ball and then you have sort of the high impact stuff, seven, eight months, full return, 10 months to a year, but eight to 18 months is not considered abnormal. I mean, I've had patients that have taken 14, 16 months, even just from the transplant to get back.
[00:21:33] Dr. Grant Garcia: So that's what I tell people. The return to sport data is 10 months, but not everybody's the same and a high level cutting basketball player is different than my. patients who want to hike Mount Rainier or one of the
[00:21:46] Will Sanchez: biggest concern with this surgery for the basketball player, right? We're talking about one explosion to the basket or that quick cut, quick shift.
[00:21:56] Will Sanchez: You know, he's a point guard. I'm not sure how much they're gonna play him to the point [00:22:00] guard, which means you're you're stopping, starting, accelerating, coming off the pick and roll, things like that. So what are your concerns when you're thinking about uh, you know, your lateral to horizontal movements. If you're looking at this player, your patient, you're going, okay, this is what I want to see when he's doing, you know, X movement.
[00:22:19] Dr. Grant Garcia: Yeah. So, I mean, that is by far the most, I mean, you have a, you have a young 20 year old NBA level basketball player. Who's going to be playing all out. I mean, he's going to be scared that first six months. I don't think you're going to see him at his number one. There's just no way because he's going to be too concerned about damaging this.
[00:22:35] Dr. Grant Garcia: It's been two years. We've talked to us before. There's a massive mental aspect to this. And I mean, this is a guy that his, his livelihood is required, you know, him, him to be able to continue on and do in the NBA and do stuff he loves, but also get paid. He's got to be able to play well. And now he also has to worry about his knee because he's now the first one ever in the NBA to have this.
[00:22:57] Dr. Grant Garcia: That being said, this isn't a, this is not a [00:23:00] surgery that is experimental. This has been around. I mean, um, Brian, Dr. Brian Cole has done this for like 15 or more years. Right. He's done over 800 to a thousand, right? This is not a, he, no offense to Lonzo ball, but he probably did this as like he had his morning coffee and then he walked and he did lots of well, that's type of guy that Brian Cole is.
[00:23:19] Dr. Grant Garcia: So this is not something that we should be stressed about the quality of the surgery, just that it's unknown. And um, I mean there's plenty of athletes I've done this on that had done really well, but never professional obviously, or you know, but that cutting maneuver is, is a concern. And that's what I'm watching out for.
[00:23:37] Dr. Grant Garcia: You may get into this, but the two biggest things we worry about with this, the number one, and I hate to say it, retear of the meniscus transplant because, and it can happen. It's like 10, 15 percent in the first year, it can be up to it. So 75 percent of these transplants are still intact at 10 years. The problem you have is you have some, that's in general, right?
[00:23:58] Dr. Grant Garcia: So my, my 40 year old patients, I [00:24:00] do this on, And they're not going back to cut high level cutting sports. Yeah. So he may not last as long with this new meniscus, but again, if we get him three or four more years in the NBA, that'd be amazing.
[00:24:13] Will Sanchez: That's a, that's, that'd be interesting. I I'm, I'm looking forward to, obviously I'm, I'm, I'm a sports fan, basketball fan.
[00:24:20] Will Sanchez: I want to. see what his minutes restriction will look like, you know, especially in the beginning. Um, you know, obviously the league is always talked about, especially the players nowadays with the back to back games. I would be shocked to see him in any back to back games. Um, but it'll be, it'll be interesting to see what the progress is from when, you know, and maybe at the end of the season, you know, we're talking about the NBA finals, maybe some key injuries or NBA playoffs.
[00:24:48] Will Sanchez: You know, we could kind of look back at the, this injury and, you know, whether the bulls are in the playoffs or not, uh, they have a young team and we'll see kind of what happens with them, but kind of say, Hey, got through the [00:25:00] season. Hopefully we're saying got through the season, went from, you know, six minutes of game, no back to backs by the season, he was up to 22 minutes a game or something like that, able to contribute.
[00:25:11] Will Sanchez: Looks like things like that. And I know we're, we're starting to go along here, but, um, where are you feeling as a doctor? What's that over the hump, right? Because you already said there's always a chance of tear, right? And it almost seems like you you'll be surprised if there wasn't, especially with this high impact.
[00:25:33] Will Sanchez: But I mean, if I did this,
[00:25:34] Dr. Grant Garcia: I'd be nervous all season, right? If I was, if I was, if, Brian Cole, I know, is able to, he's a cool, calm guy. I love him. He's awesome. But, and there's, I don't think he's nearly as stressed as I am watching Lonzo Ball play. Just because I know the level of the surgery and the level of two years of recovery and obviously being the first one.
[00:25:52] Dr. Grant Garcia: Yeah. Um,
[00:25:54] Will Sanchez: but there's not a point there where you go, well, he's up to 20 minutes. He's, he's, he's reacted. Well, obviously I [00:26:00] can't imagine how many times he's being checked in, right? You know, at this level that you're, you know, you know, dr cole's checking in on him. How you feeling? What's going on? Okay, let's, let's get your ice and You know, this is what I want you to do when you come off the court and, and after the game and before the game, like this whole process, I can't even imagine, uh, what goes into it.
[00:26:20] Will Sanchez: So there, there's no point of it where you go, all right, anything can happen. But overall, I'm kind of feeling pretty good where we're at. And, you know, everything else is just kind of, you know, we'll, we'll see.
[00:26:30] Dr. Grant Garcia: Well, so I think to me is he's had a long discussion with the agent. I'm sure family, uh, Alonzo Cole had discussion with many other different surgeons too, to make sure this call was the right call.
[00:26:41] Dr. Grant Garcia: And I think it is because this has not been done before and it's needs to be done. I mean, you have players, you have, this is, this is a, this is a humongous first start. And I think that there is not, I think, I think that as the games go along, there's gonna be less and less stress. And you're going to see that if this works, Lonzo is going to be playing better than he's [00:27:00] probably played in a while because
[00:27:02] Will Sanchez: when
[00:27:02] Dr. Grant Garcia: patients get this, like my, my, this is one of my highest.
[00:27:06] Dr. Grant Garcia: The reason I like the surgery, I already told you it's extremely challenging. It's a really niche thing that very few people do, but when you do it right and well, the results are mind boggling. I mean, you get patients that are miserable with pain, swelling, frustration, and you can make them feel stable.
[00:27:24] Dr. Grant Garcia: They have this thing they call stability, which is very weird because they're not actually unstable, right? They have normal ACLs. And you can make their pain go away and they feel like the fullness of their knee feels better, right? It's like a car and they're like you're driving you feel like something's missing like the belt's not working, right?
[00:27:38] Dr. Grant Garcia: You can just feel it clutching you feel something weird going on. Yeah, when they get this they go My kneel my knee feels different. It feels strong. It feels stable. It feels not swelling. It's not painful These are weird comments that you don't hear when you do other surgeries. Like I do lots of other procedures I Thank you.
[00:27:56] Dr. Grant Garcia: I feel better. My pain's better, but they'd like they'd like they can like put their mouth on it. They can put their [00:28:00] words to it and they can say this is what this is.
[00:28:02] Will Sanchez: Yeah.
[00:28:02] Dr. Grant Garcia: And if he gets that if he gets that and again, it happens more frequently than then it doesn't happen Um, that'll be so cool. I think we're gonna see some impressive things and I think that You know, we're talking about 10, 12 games of the season.
[00:28:15] Dr. Grant Garcia: He's following the restrictions slowly improving. We're going to see some pretty impressive things. And I'm confident in this procedure. I hope he does really well. And even worst case, I'll let the viewers live this even worst case. If he does get a small tear at the end of the season or something that gets cleaned up, it doesn't mean that it's a failure.
[00:28:29] Dr. Grant Garcia: Right. Because he's still going to have a lot of his meniscus left. He's still gonna have that cartilage transplant, hopefully. So even a small hiccup, it doesn't mean that you're failed, right? Most of these cleanup procedures, you still keep going. So I know we go all day with this, but I'm really excited about this.
[00:28:42] Dr. Grant Garcia: Obviously, I think that it's really cool for the listeners to understand this. The last piece I'm going to tell the listeners, be prepared. This is not going to be the last person that gets this surgery. If this works in the next year, Because there are so many other athletes that need this done that no doctor wants to do this surgery on them because they're terrified.
[00:28:59] Dr. Grant Garcia: So because [00:29:00] they don't want to be, have this fail, right? This is a higher complication rate than an ACL. This has a higher complication rate than a meniscus cleanup, right? It's got all of the things. But if this works and gets back a player that has, there's, this is, this is career ending. You're going to see, uh, not a flood, but this is, this is going to be something you're going to see every year in the news after this.
[00:29:19] Dr. Grant Garcia: I, again, I could be wrong, but we'll see.
[00:29:23] Will Sanchez: It'll be, uh, it'll be great to watch. Um, you know, just as we wrap it up, we think about injuries and what's happening on the court and, you know, you've had injuries, I've had injuries and probably every, you know, everyone that's listened is not. Just the injury of what you're doing.
[00:29:40] Will Sanchez: It's laying in bed. It's trying to sleep. It's trying to be comfortable. It's just being uncomfortable and having this, this issue with whatever it is, whether it's your knee or elbow or neck or whatever. So just having some, something there that can be Kind of will make him feel better and even sleeping, right?[00:30:00]
[00:30:00] Will Sanchez: Maybe getting your full eight, nine hours to sleep and everything else. It's got to be beneficial, uh, for, you know, physically and mentally. So we, we hope that everything goes well and we know what it is to just be in pain, right? And that's one of the reasons that we talk about the show, you know, being in pain is not fun, not just walking, but even doing nothing, you can be in constant pain.
[00:30:23] Dr. Grant Garcia: Well, and again, for this one, It's not, he probably wasn't in pain constantly. The people, these, most of my patients are athletes, right? They're like, it hurts when I run, it hurts when I do sports. And that's what we're here for a sport surgeon. I want to fix you so you can do sports again.
[00:30:35] Will Sanchez: Yeah.
[00:30:36] Dr. Grant Garcia: Um, but you know, also wanted to let them know the lesson, let the listeners know, thanks again for all the requests I had.
[00:30:41] Dr. Grant Garcia: I've had three patients in the last three weeks asked me when the show was going to happen. And I didn't tell them I was going to do it. So people are waiting for this Lonzo ball show to hear about it. So I've been excited. The start of
[00:30:52] Will Sanchez: the
[00:30:52] Dr. Grant Garcia: NBA season. Right.
[00:30:54] Will Sanchez: Well, opening night, we had to, we had to come back to this.
[00:30:59] Dr. Grant Garcia: Thank [00:31:00] you to the listeners for. Continuing to encourage us to do stuff like this, because this is what this what's all about. Want to teach people about this surgery. You know, people come to me like this is so new. I'm like, it's not new, but you just haven't heard about it. So we're going to inform you and learn.
[00:31:14] Dr. Grant Garcia: So thanks again.
[00:31:16] Will Sanchez: Yep. And please check us out at sports. talk. com because that's where you can put in your requests for other shows and anything else you want to listen to. You could check out our previous shows transcripts. You get tired of listening to us babble, but you love the information. Check out the transcripts of the show.
[00:31:33] Will Sanchez: We have everything there. So, uh, we appreciate you guys and, uh, let's go next. Let's see if we could finally win one. It's been damn too long. It's been since 73 and I don't want to have to talk about John Starks anymore, missing all those shots. I'm not going
[00:31:50] Dr. Grant Garcia: to, I can't root for the bulls, but I'm going to say go Lonzo.
[00:31:52] Dr. Grant Garcia: No,
[00:31:54] Will Sanchez: no, we, we always root for our guys recovering, uh, things like that. So Dr. Garcia, this is
[00:32:00] great, man. Thank you so much. You have a good one. Bye.
Audio Transcript
Nick Chubb Returns From A Challenging Injury and Surgery
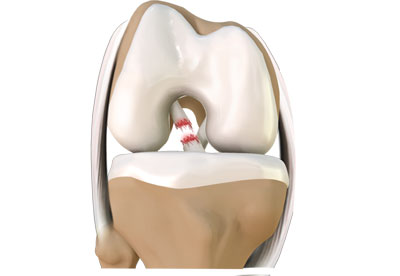
Will Sanchez: Welcome to Sports Doc Talk. We have our orthopedic surgeon and sports medicine specialist with a Sunday night edition that's going to come out Monday because we were really excited to follow up on a show that we have done uh, wow, just last fall talking about Nick Chubb. As we conclude week NFL, can you believe that we're almost halfway through Through this NFL season, I felt like we just started talking about the NFL season, the upcoming NFL season and, uh, and here we are.
Dr. Grant Garcia:Oh, and you can see my, my logos changed. Unfortunately, the Giants are, uh, So we're Cleveland, but, uh, we're going to be starting. I can't represent right now. So we decided to put this up in [00:01:00] honor of So this is, this is the new sports stock talk for the next year. We're going to keep trying to do logos.
[00:01:07] Dr. Grant Garcia: You're going to guess my logo is coming up for each show.
[00:01:09] Will Sanchez: Oh, maybe we should do that. Right. What's the, what's the logo of the next show? Um, you know, geez, we had this, this show last year, right. And we mentioned the, the Nick chop injury. I believe it was Sunday night. football. I think it was Sunday night football.
[00:01:25] Will Sanchez: I forget why we were watching them and it was just a nasty, nasty leg injury with the helmet to the knee and the leg moving in places that you just don't want to, you know, see it move. Uh, for those that didn't see the injury, I'm pretty sure you could find it on YouTube and anywhere else going back to that run.
[00:01:47] Will Sanchez: And we talked about it right away. You were like, this is, this is a tough one, right? With the damage to the medial collateral ligament, the medial capsule and the meniscus. Um, before we update where he's at today, [00:02:00] let's go back to that, you know, that injury and kind of recap what that injury entails.
[00:02:08] Dr. Grant Garcia: Yeah, so I remember when we were talking about the, when the first show happened, it was just so nasty and actually I would tell, I would tell you that this is lucky compared to what I thought it was just because it looked like a full knee dislocation.
[00:02:19] Dr. Grant Garcia: So he tore the MCL, which commonly happens with these ACLs, but as we remember, he had an ACL done already. This is now a second surgery. Go back to college. Yes, exactly. And so it's never the same, right? It's not like a fresh situation we're going into. So this is not a guy that tore his ACL for the first time.
[00:02:37] Dr. Grant Garcia: This is a second ACL tear. This is an MCL tear. And what was not mentioned is the bone grafting, right? So he supposedly had some bone grafting done because the tunnels were not perfect. Like we had talked about this. He might need that. And then it turns out he ended up needing that. So he got his September surgery.
[00:02:53] Dr. Grant Garcia: He got his MCL fixed. He got his meniscus fixed and that's what they did to obviously help out with some of the trauma, [00:03:00] right? Cause all the surgery at once might be traumatic. He got some bone grafting and then basically September, October, November, three months. As soon as they could do it, they did the second surgery.
[00:03:10] Dr. Grant Garcia: They talked about using some smaller scopes to try to help with inflammation and they gave him a new ACL. Uh, and they use some special screw options to try to help integrate the bone. And we can talk about the future of those at some point. And maybe in a future show, who knows, we don't want to hint too much on upcoming guests.
[00:03:28] Dr. Grant Garcia: Um, but. They use some biocomposite screws. So these are screws that turn into bone. And so the idea is that just leave no trace, right? Everything will be natural when he's done and hopefully give him the best, uh, option to recover. And also it fills any of those old tunnels of graft. Um, so pretty bad injury, revision ACL, new MCL or new MCL repair and meniscus repair.
[00:03:51] Dr. Grant Garcia: I mean, this is, this is not ideal. But we have seen players come back from this, but you know, 390 something days after [00:04:00] the injury. We can pull that up. Um, that's the impressive. Uh, and I mean, 11 carries a touchdown in 22 yards. Not too shabby for an NFL player, especially coming back from injury. This level.
[00:04:12] Dr. Grant Garcia: We're going to see this. We've talked about this well with our other players that have gotten injured the first day, the first week, the first month. It's not the same. Right. They, it takes them a while to get back and we've seen the return to sport data for different players and running backs are not ideal, right?
[00:04:28] Dr. Grant Garcia: Quarterbacks different, which is Dan Jones, which we, we can't really talk about too much anymore now. Uh, but, uh, you know, for him. This is, uh, this is impressive that he's back out there doing what he loves to do. Um, and big shout out to Dr. James Vu's, who is the team doctor for Cleveland. And one of my friends also, uh, Jacob Kelsey, who, who probably was assisting or some part of that surgery as well.
[00:04:53] Dr. Grant Garcia: So, uh, you know, I know these guys, they're really good surgeons and, um, just to be able to get a guy back like this is [00:05:00] awesome. And again, it's a team. Right. We've talked about this way too many times. We'll have something coming up soon. Maybe about Lonzo ball, something about the recovery for other athletes.
[00:05:10] Dr. Grant Garcia: It's everything, right? Everything matters. It's not, you know, the surgery is incredibly important. The techniques you use are incredibly important, but it's the entire, it's setting expectations is telling Nick Chubb 150 times. You're not going to go out there and run 200 yards and plow through everybody.
[00:05:27] Dr. Grant Garcia: Your first game. It's just not going to happen.
[00:05:30] Will Sanchez: Yeah, I, I'm curious, right? So obviously the injury was just, you know, as you mentioned, it was really nasty, right? When we first saw it and, you know, we decided to do the show and we, in fact, we touched upon a couple of other injuries. I'll bring up an injury, um, you know, going forward that we talked about, but, um, Were they, are there any benefits with going back in and having that type of injury and fixing kind of what was [00:06:00] done, whatever it was five or six years prior, right?
[00:06:03] Will Sanchez: We have new technology, right? We're always talking about new tech and new toys and, and things like that. And maybe it was something that whether the knee was going to eventually go or whatever case, maybe But is there any benefit to going back in, kind of redoing what was done, taking out the old, putting in the new, getting the knee, maybe even stronger.
[00:06:25] Will Sanchez: Right. We think about re injuring. And when I hear re injure, I go, you're weakening, you're re weakening something. Is there any positive that could come out of that?
[00:06:36] Dr. Grant Garcia: So a lot, I mean, if you're in a concern that there's going to be, remember the tunnels that we had before are no longer bone, right? They're tendon.
[00:06:44] Dr. Grant Garcia: So they don't, they never fill with bone again. So they can be windshield wiper. And so the tunnels are too big. or not perfect spots or they've, they've changed over time. You want to have that ACL at the exact spots, right? So it stops the knee from going forward. And so I do a lot of these [00:07:00] revision situations.
[00:07:00] Dr. Grant Garcia: If it's not a situation where you're exactly happy with it, you want to redo the whole thing
[00:07:05] Will Sanchez: because
[00:07:05] Dr. Grant Garcia: it's not very hard to redo. And with a guy like Nick Chubb. So like a standard athlete, three to four months is what I'd wait between the two surgeries. But understanding that like he has, he can wear a special brace, they'll protect him from not injuring his ACL, but still let him work.
[00:07:19] Dr. Grant Garcia: Some of my patients, they kind of, they don't always listen as well as someone like Nick Chubb would because they don't have all the resources, right? So I worry, the only thing you worry about between those two times is does he injure himself because now he doesn't have an ACL, right? He had no ACL for almost three months.
[00:07:34] Will Sanchez: That's what that
[00:07:35] Dr. Grant Garcia: is. And he doesn't, you don't need it for walking. You don't even really need it for running. Um, and a guy like him, I bet you that his exam would be hard to tell if you actually tore his ACL at the beginning. Cause look at his legs. He can overpower you. Like some of these guys, you can't even tell you need them to be sort of like almost paralyzed for a second before you can get the exam.
[00:07:53] Dr. Grant Garcia: Um, we've talked about players like Heinz Ward, right? For the Steelers, there's been players that have had no ACL and still been able to get away with [00:08:00] it. So these guys are really strong and they can, they can beat the system in certain respects. Uh, so like it is, it is definitely an advantage to what they did.
[00:08:07] Dr. Grant Garcia: And they added new technology. I'm sure they added internal brace. I know who's just talking about the nanoscope that they use, the special mini scope, that's an Arthrex product. Um, they, they used, they use the most cutting edge technology for him and they probably use some things we haven't even heard of, uh, because they have everything there.
[00:08:23] Dr. Grant Garcia: Like I said, this is, they're going to, they're going to pull out all expenses for the Cleveland Browns. Um, and the, uh, the, the. With the hospital system that he got done at. So
[00:08:31] Will Sanchez: I was going to ask you about that when you talked about the holes, if they would go internal brace or fertilize ACL or any of the other things that we've talked about before to maybe fill in some of those gaps to make it stronger and for it to operate.
[00:08:44] Will Sanchez: I bet they did
[00:08:45] Dr. Grant Garcia: everything. I bet they did everything. I mean, you're talking about, they're talking about the smaller scope they used. They probably use some sort of stem cell PRP option to help the ACL integrate. We talked about this with revision ACLs on our, you guys look back. If you want to go see how this [00:09:00] happens.
[00:09:00] Dr. Grant Garcia: We talked about this on our bio biologics and ACL surgeries. One of our, one of our more popular episodes, they did a lot of things to try to get him back faster. Now, again, 398 days is not faster, but for the type of injury had, that isn't faster. I thought,
[00:09:14] Will Sanchez: I thought it could be his career, let alone, you know, being back.
[00:09:18] Will Sanchez: Yeah. This is,
[00:09:18] Dr. Grant Garcia: this is, this is a, this is a, I mean, 3 98 days is an average for some of these NFL players. Yeah, yeah, right. Who just getting race regularly.
[00:09:25] Will Sanchez: He got, he got hurt, I believe it was week two of the 2023 season, and now we're in week seven of the 2024 season and he's out on the field. I mean, that is.
[00:09:35] Will Sanchez: mind boggling when you look at the type of injury that he had the violent nature of the collision. This is not a knee that just kind of, you know, buckled on his own. This was a man running into your knee and making it go in a direction that is not supposed to go right. Just to kind of give context to it.
[00:09:54] Will Sanchez: So, uh, fast forwarding, what are your concerns, um, going forward? [00:10:00] He had, he went out on the field, he got contact, you know, he, he huddled, he, you know, he gotta take it to the ground. So, you know, what is this week looking like for him that you would, if you had to guess? You know, as far as his recovery.
[00:10:16] Will Sanchez: afterwards and then just kind of getting ready, um, for each game as he goes forward for each season. If you're treating him as a doctor, knowing the type of injury and the type of sport, what are some of the key things that you're looking out for, uh, for this upcoming season for Nick chuck? [00:10:33] Dr. Grant Garcia: I mean, the first thing I'm doing is just symmetrical strength and activity.
[00:10:36] Dr. Grant Garcia: I'm just making sure that after the game, he still looks like he's walking normally, he's active normally, right? Like making sure that he still stays symmetrical, right? His goal is like, you got to work both sides. You're going to try to shut down any inflammation. He's going to, he's going to swell like heck.
[00:10:49] Dr. Grant Garcia: I'm sure his knees swollen more than average right now, because you just, he just put it through a ringer that he's hasn't, you know, as much as you practice what you do, do in the game. The game's totally different animal. Right. He's going to, [00:11:00] his adrenaline is going to kick in. Um, and then finally, you just want to make sure he recovers down.
[00:11:04] Dr. Grant Garcia: You get that swelling down as soon as possible. Um, and then I think the last part, which I'm sure they're doing at the Browns is a mental health coach. Like he's got to get in with the mental health coach, but like, how did that feel? Right. Like you had a devastating career, any injury and you just play it again.
[00:11:19] Dr. Grant Garcia: Like, how are you feeling? Like, do you feel good about this? Are you ready to go back for the next game? Did you have any hesitancy, like going through a play by play virtual in his head, like how it went, that's what I would do. Yeah. Um,
[00:11:31] Will Sanchez: Yeah. And he, he was emotional leading up to the week. The, the fan base, you know, cheered for him.
[00:11:38] Will Sanchez: Um, you know, his teammates came up to him afterwards when he scored and, you know, gave him that, you know, the pat on the butt and everything else. So, uh, I'm pretty sure, and I love that you brought that up, right? The mental aspect, because it looked like the teammates rallying around wasn't rallying around because of the injury was rallying around with the person saying, okay, you did it.
[00:11:58] Will Sanchez: Yeah. And him having kind of [00:12:00] that expression of gratitude and maybe some relief. So it's really, uh, I'm really glad that you brought that up his teammate. Unfortunately, Deshaun Watson, and this is why I kind of go back to the original show, because we've talked about his shoulder displaced fracture in the glenoid and I don't know, I'm, I'm out of my depths over here with some of these wording, you're doing
[00:12:21] Dr. Grant Garcia: great.
[00:12:21] Dr. Grant Garcia: You're doing great.
[00:12:23] Will Sanchez: You know, we talked about the severity of that injury. Um, I looked at the replay today and we're doing a show on Sunday night. Um, and it looked like his Achilles popped. It's exactly what you want. You have the closeup on the, on the Achilles. He steps to go forward and you see the muscle go like, you know, and he hits the ground.
[00:12:44] Will Sanchez: So, uh, it looks like back to back seasons, uh, for Deshaun Watson, for him being out. So. It's just, uh, Cleveland Browns, not good for the quarterback and, uh, of their team, but great news for Nick Chubb being [00:13:00] back on the field and, you know, resuming a career where last year I wouldn't have been surprised if you said, yeah, he's done that.
[00:13:08] Will Sanchez: That knee is just not going to cooperate on the level of being an NFL player. He can walk again, he'll do this, but to perform at that level and squat 600 pounds and. Run over 300 pound lineman them days are over. So it's a, it's a great story. Any last thoughts before we wrap it up?
[00:13:29] Dr. Grant Garcia: Yeah, I mean, thanks to listeners.
[00:13:30] Dr. Grant Garcia: Uh, this obviously is kind of an important injury to talk about, uh, just cause it was so devastating. We had the previous episode and do some followup on this. So hopefully they enjoyed this, learned a little bit more and, uh, awesome job. Congratulations, Nick Chubb for getting back and we may have some more update injuries coming up soon.
[00:13:47] Dr. Grant Garcia: So thanks for listening. Take care guys. Bye bye. Audio Transcript
Tua Tagovailoa’s Injury Confronting the NFL’s Ongoing Dilemma
Will Sanchez: Welcome to Sports Doc Talk. I'm Will Sanchez, along with our orthopedic sports medicine specialist, the doctor. Oh, by the way, before we get started and we're it's always a great topic that we're gonna have here but before we get started. Congratulations on getting recognized, especially in the Latino community.
So just tell our fans real quick because apparently you're getting recognized weekly right now because you're so done. Let me tell us a little bit about that, that that honor that you've just been given.
Dr. Grant Garcia: So I was honored to get Castle Connelly, which is actually one of the ones when I first started, I really was excited to get, you don't really know you're going to get it until they email [00:01:00] you.
And then Castle Connelly does a Latino and Hispanic section. They have different sections for different diverse backgrounds. So they selected me for top doctor for Latinos as well. So it was cool. I think my dad was pumped about that. I think my post, but Yes, my dad was born in Brazil. He came over here when he was nine.
He was, he learned how to learn English. He ended up doing really well. And now I'm here. So my mom's from Jersey, so she didn't have to do the same type of stuff nonetheless, and grew up a Giants fan. So this is why. We still root for them.
Will Sanchez: Yeah. Congratulations, man. It's you're achieving a lot and just to get recognized like that and see what you're doing.
It's important. It's great for Latinos to see the possibilities. And being rep, having representation in every field is important, so it matters. And not only is a great honor for you, but it's a great honor for someone else that recognizes that. Anyway, enough. [00:02:00] No more compliments.
I'm completely done with it. I'm blushing. We got to move on. Let's go. I'm blushed. Let's make it
Dr. Grant Garcia: cut.
Will Sanchez: Yeah, your cheeks are a little red, man. It might be all that little sun. The sun's going away. We're about to get the clouds and rain, so no more sun for us. I
Dr. Grant Garcia: know. I know.
Will Sanchez: We were talking about it.
And once again another scary site, right? And this time it was less traumatic. We're talking about to a tongue of Iola suffering another concussion just to give you a recap. Last year he didn't have a concussion that we were aware of, but the year prior against Miami.
I'm sorry against Buffalo. He sustained an injury in Miami where he was hit. He got up. He stumbled. We all clearly saw that this injury he sustained had everything that you would deem to be a concussion. The doctors approved him to play the following week against the Bengals. Since then, After the Bengal injury, which was a nasty [00:03:00] injury when he was sacked and flung to the turf, laid out there.
For those that don't know, he suffered what's called fencing, and I'm going to tee you up in a second for you to explain what fencing is. And now once again, he has suffered another concussion, three concussions on the biggest stages, one on the Sunday afternoon game, Another one on a Monday night game and then again on another prime time event where the world kind of watches since NFL rules our universe here in the United States.
First off, describe what fencing is and to what was the first thought you had when you saw that to a sustained another concussion, a third concussion that we're aware of in this short time frame.
Dr. Grant Garcia: So Yeah, first off fencing you whenever you get traumatic injuries or traumatic brain injuries, it goes back to your prenatal state.
And so when you're getting hit, this idea of fencing is you flinging back the arms, everything's just like abnormal motion. Actually, like the fencing position, [00:04:00] like when you fence in the Olympics, it's the idea of what it looks like. It's not good. And we had this. Entire podcast a year and a half ago.
You guys can listen to our episode about this exact same injury. And so when does it happen again? And all of a sudden now the articles are coming out about concussions. It just has to come up again. We have to have the conversation because this is not just a hot topic because it's a hot topic because it's a good player.
It's a hot topic because we're just, we're seeing a bad injury and a difficult situation for someone like to as to what to do. You have the media spoken people that are saying retire, retire, but you also, you have no idea what's going on behind closed doors, right? We're just seeing a bit.
We're seeing just the tip of the iceberg. And we've seen the shows, movies, concussion. We've talked about this. We've seen We've had Dr. David Smith on here talking about ways to reduce traumatic brain injury in these sort of events. And now we're having another thing come up, and it was on the stage, and it's not like he got up and he was dizzy.
He went into [00:05:00] fencing position again. Which is just, this is just not a good thing.
Will Sanchez: Yeah. For me, it was really scary because if you look at the hit and for those that haven't seen it, just go back to playing against Buffalo he's rushing for a first down. He's trying to get close to the end zone.
He runs into, of all people, DeMar Hamlin, which we've talked about, this sustained a life threatening injury on the field in Cincinnati. Also just a little over a year ago and the contact was not extreme. And that's really what kind of made me go. This is not good. This wasn't a defensive player coming at him and coming with the crown of his head, banging his head or anything like that to actually ran into the Mars chest, which, that's scary itself because that's how he sustained this injury just was running, ducked into it, ran into his chest and collapse.
Demar, it was the most, the [00:06:00] softest tackle pretty much is almost like he's just. cradling him as he's running into him to tackle him. And the fact that he had this concussion and his body had that reaction, went into this fencing state. And that for me was scary because I'm saying if he got hurt like this on a tackle play, that when you look at the NFL, it is a non violent type of tackle play.
Where do we go from here when it comes to this man and this injury?
Dr. Grant Garcia: The problem you're going to have too is who's going to clear him, right? They'll find somebody but like you've been seeing I was just bringing up my partners You've been seeing these massive lawsuits in the nfl, right?
There was the one for the philadelphia eagles so bad The lawsuit was so bad that the philadelphia eagles got dropped by rothman institute. Like that just doesn't happen Like on the news, they say we are no longer going to cover the Philadelphia Eagles and they had to find the scrambled and found an old doctor that did them.
I'm sure doctors great, but it's not Rothman Institute. [00:07:00] And so for those that
Will Sanchez: don't know, I'm sorry to interrupt for those that don't know, can you explain that Rothman Institute, Rothman
Dr. Grant Garcia: Institute, Rothman Institute is one of the biggest orthopedic places. I train eight spousal special surgery.
You have Rothman down there in the Philadelphia area, but now they basically run the whole West East coast. And they are, their main hub is in Philadelphia, actually across the street from where I went to the med school in Penn. And they're known for just being really big powerhouse orthopedics.
And they've got A number of teams. I think they did the flyers they used to do the Eagles, and they have really good surgeons. They're really good guys and they got a massive lawsuit. We're not here to talk about medical legal of football, but they got a massive lawsuit and they dropped the Eagles and they announced it on NF on the ESPN and all these other shows that they're dropping because of that lawsuit, because it was the largest lawsuit in the history of the NFL.
And so now if you see this situation where you have a player that got two injuries, another concussion. You clear him. He goes back out there and gets another one. All of a [00:08:00] sudden he can't, he has no cognitive ability. Some of the things have happened, again, I don't want to predict this, but the brain is scary.
We have no idea which way it goes. You see these, you boxers get hit repeated times. They're going to hit more than obviously this. Clear him to go back and then he has another instance, another week or two, and now he's like out for another season. The, they find some way to let him go, get him pushed off.
The dolphins are screwed in this situation. Anyways, we saw well, they played last week. Yeah,
Will Sanchez: they look
Dr. Grant Garcia: terrible. This is a really difficult situation. And if he doesn't, and if he doesn't retire himself, if he hasn't, he has to get medically retired for him to have all that money. And it's a lot of money, like 120 million I think is on the table.
So this is a really difficult situation because you have, Medical legal side from the doctors. You have that dolphins, which I know they care about him. So I'm not going to hear to talk about NFL being a bad person, but at the same point, they want to win. So they want to maximize stuff. And this is just difficult.
This is a business. [00:09:00] It's as if this is just a difficult situation. And now you have players. We used to see Steve Young just get smashed every single game, right? And just right. Concussion after concussion, bread, barb, concussion. It's no longer that way. We know the risks. We've seen it way too many times.
We've got, we've seen shows about this. There's, we're not going to bring up too much today, you've got the league of the Niles article, the PBS special that we just watched. This is a, this isn't ending. This is not going away. We are looking for new things. And as we've seen, there is so much technology out there and we still can't stop it.
You, we brought this up to a did, I think I had showed you, he was practicing jujitsu classes to learn how to fall and hit the turf better. That's a really great thing that they talked about, fricking way that's going to stop him from getting, if he's got baseline. This wasn't a hit. Like you said, this wasn't a traumatic thing.
He didn't smash his brick. I don't care how well you learn how to fall. If you get hit blindside, it doesn't matter who you're the best athlete in the world. You're not [00:10:00] going to see it coming. It's all about, when you do jiu jitsu, right? I have a lot of take care of jitsu people.
They're, they see their opponent. They know what their opponent's gonna do. It's MMA too. You see what they're doing to do. They may be fast, they may do something, but they're coming at you. They're not blindsiding you in the ring. Yeah. It's a totally different thing. I think we can do whatever, we'll talk about some preventative measures, but again, we keep seeing upgraded helmets, upgraded protocols, and there's a reason for that because we still haven't gotten the answer.
Will Sanchez: Yeah. I'm going to be selfish here and I want to be clear and let our listeners know, right? I'm going to give you a selfish point, right? And this is my selfish take on this, his injury and the way he's. the way he has suffered this injury in front of everyone has almost become not fair. It's not fair to his teammates.
It's not fair to his opponents, and it's [00:11:00] not fair to the fans that every time This man draws back to pass or starts running that you are going to think about his safety. And that is what has happened when I've watched him play. When he started taking off running, I felt like the announcers were almost saying slide, the fact that Demar Hamlin did not take a shot on him.
That you're running, you got a quarterback and usually is Hey, the game, let's take them up. You didn't see that if we're his teammates. So now whether it's blocking Lyman blocking or him getting sack the coaching staff, whatever it is, his teammates have to look at this player back there saying, I hope today is not the day his opponents that are trained to be violent.
In this sport are saying, I hope I'm not the one and for fans saying, I hope I'm not going to witness anything [00:12:00] on the field that is going to be lasting. And we've seen different injuries. We've seen bad injuries. We've seen Derek Dennis bird, Corey stinger. We've seen men paralyzed on the field and what that does.
We saw what happened with the more Hamlin and everyone just being emotional, but. Almost to the point now, if two is back under center, there is no way as a football fan that you're not watching that game saying, I hope that we don't see something today. But
Dr. Grant Garcia: It's true. I think he's going to be back.
I think someone's going to clear them. They'll find a neurologist to clear them. That's the NFL. But, and I don't think he's going to retire. Yeah, I just don't see it. They just it's just not a good situation. Know we, I think we, I think I brought it up to you, but, there have been players that have retired.
Before we had the original one, that's the Luke Cooke [00:13:00] Cooke's league or whatever you he's the one that just
Will Sanchez: recently retired.
Dr. Grant Garcia: Yep.
Will Sanchez: Linebacker, same thing, but a lot of injuries had concussions, probably borderline hall of famer. If you're a Panthers fan you're saying definitely hall of famer.
A guy that made it to the league out of, I believe it was Boston college and became the captain of the team and went to a Superbowl with Cam Newton. Yeah. And. Same thing, had to leave the game due to those injuries. And we saw some bad ones. You mentioned the Eagles, Lane Johnson, starting left tackle for the Eagles concussion, right?
Devante Smith and nasty concussion where he was hit from behind and his helmet came flying off. And he experienced some of that fencing as well. Scary stuff. So the fact that you mentioned the Philadelphia Eagles, now they've got two major injuries right now. The Devante Smith, that was really serious.
He's not a big guy. I'm, he's lucky if he's buck 90. He is a skinny Y receiver and [00:14:00] you wish him the best. I wanted to put up there for those that are watching and not just listening. I'm putting up the five phases for the NFL concussion protocol and I'll just go through them real quick.
And then I want to ask you about this protocol and also whether you have a similar protocol since you are a team doctor as well. And maybe some of the symptoms that you see and what you expect from before you clear player. So phase one symptom limited activities, light aerobic exercise phase 20 minutes of running stationary bike under supervision.
Phase three football specific exercise like non contact drills, strength training, cone drills, phase four club based non contact training. So that's participation, running, throwing, catching, still non contact. And then phase five is pretty much full participation in practice without, with [00:15:00] any restrictions.
If any of the player's symptoms return at any point during any of the phases, they will return to the previous phase of the protocol. Can you talk about that a little bit?
Dr. Grant Garcia: Yeah. So this is important. And I think we brought this up. We've had a few concussion episodes just cause it's such a hot topic, even though it's not,
It's an orthopedic thing, but it's not really we don't see these every day as an orthopedic surgeon, especially sports surgeon. But if you take care of teams and players, you're going to have to know how to deal with this, right? Cause it's it's just the nature of the beast. There's an neurologist on the field during the high school games.
Sometimes the college games, there's no neurologist NFL. Yes, but different animal. Yeah. So the, those phases, those one through five, it used to be, I think actually seven. So it was always hard. And it may not have been NFL level that had the seven, but you can see that each one of those steps is really important.
And they're monitoring for symptoms. You always say I don't know if they're gonna clear the protocol, right? So they go phase one, phase two, phase three. All of a sudden, player get some symptoms, lose a day, go backwards. And that's [00:16:00] why you have Injury on Sunday really starts on Monday, right?
They may not be cleared, right? But if they have five days, they can be like Friday, you hear Friday, Saturday, oh, they cleared the protocol. And I don't know, I would, I want to say they're strict, but I don't know how it works. If the guy had very minimal symptoms, they call them out of the game.
They go phase one, two and two days in one day. I don't, it's just this, the problem is this is a really fancy little page, but how does it, this is not always the case. It's not exact science. The other thing is, what about like training in hot facilities versus cold facilities and how are you going to have symptoms, ready to get a concussion, but you also have to have a little bit of heat, and do stuff, but you gotta be careful about like when you're skipping these phases.
This is a guideline, it's important to have it, we're much more stringent on it in high school and college because, there's just less to lose by missing a game. Like I just, my players get hurt, they're out. And they're not out. They're not back until I feel really strongly. They're going to be safe, right?
It just doesn't matter. It just, I know they all play for the [00:17:00] championship. They're all, I want all the kids to do well, but I sure as heck don't want another kid to, if I saw a kid fence, I would never let him, I would never, that would be done for the season. So this is just not worth it. And the NFL is a different animal.
Yeah. He's got millions of dollars on the line. He's an adult. He's got an agent, right? Like they, this is, there's not just, this is not right. It's, we always talk about this. We treat everybody the same, but unfortunately the pros, it's just a different ball game. Yeah. It's just way too much money, way too much on the line and they're adults, right? My kids on the field, they're my kind of got a kid got hurt. He's got 15 years old. They got to ask the parents for permission to do something, right? Like It's just different different strokes, but anyhow,
Will Sanchez: and we talk about all the time they're built different, right? I cannot do what they do. I cannot get into that mindset.
And for them to always have that winning mindset of, I can do this at the highest level where 99. 9 percent of the people [00:18:00] that play the sport can't reach. I they cannot reach that level. So you have to be built different, so that's another part of it where they're, that's one of the things it's, who is the ultimate competitor?
I'm going to get out there. I, my team, imagine him sitting on the couch, watching that game against the Seahawks going. I can't help my teammate. They look like a bunch of scrubs out there. If I was out there, we could probably win this game. I could get the ball to Tyreek Hill. I can do these things.
I could go in there and support my brotherhood, and we've seen them compete at every level. And you talk about it all the time. These professional athletes are built different. And in all of the elements that you're talking about, what makes it so hard between the business, the mindset getting cleared, being an adult.
I can't imagine, being that team doctor or multi at this point, I'm assuming he's going to go to multiple specialists and doctors for them [00:19:00] to say. You passed my face. I'm clearing you. What about the next guy?
Dr. Grant Garcia: Exactly. For the sake of our short segment, we're trying to do is do a good job of, sorry, we should talk about this next thing because this is cool.
Cause I actually did not know much about this. We'll bring it up. So you guys have all been seeing, if you watch, I just watched the Giants game replays on highlights and you see a couple of the Cleveland Browns, which we beat, which is very exciting. The, these coffee caps and you're like, what the heck are these things?
So these are guardian helmet caps. And Guardian is the company. And these are actually, so they're now mandated in the NFL for practices. They're not actually that expensive. At least I looked them up. It didn't seem like they're that expensive. Now what's interesting is I hadn't seen these in the high school level.
No one talked about them and maybe they're using it in practice, but you've seen the practice. They had all those weird helmets and things like that. These are the new thing.
Will Sanchez: Yeah.
Dr. Grant Garcia: And if you can pull the timeline up, it's interesting to show this. So in 2017, they won this sort of NFL tech award.[00:20:00] They had validated and it turned out that they found that it was a 50 percent reduction in concussions. Now the problem here, obviously, and I don't want to be knocking this because I think this is like anything, anything that can help is always good, right? There's nothing. I'm not going to, I'm not going to pooh any technology.
That's great. But obviously what's the definition of concussion. We saw this with Dr. David Smith, right? It's very broad. There's not like a diagnosis. If someone has an ACL tear, there's very few people that are going to have a, like surgery, they can't figure that out, right? It's an ACL tear, you examine it and you get an MRI and it says ACL tear, right? Simple concussion. You do a testing system. We've gone over so many different testing systems, right? Those are pretty good, but these are still like, check boxes and try to do your best. There's no brain MRI. It's going to tell you there's a brain MRI for traumatic brain injury, but you don't want to get to that level.
You can start seeing it as I think Dr. David Smith said, if you can start seeing an MRI, you're beyond a problem.
Will Sanchez: So
Dr. Grant Garcia: we have to be aware of that. And then, so now they found this is so [00:21:00] in 2018 is validated the increase of use and all of a sudden, boom, 2022 mandated by the NFL for certain players.
So it was the offensive lineman, defensive lineman, tight ends and linebackers. Okay, but listen to this, listen to what we're going to say about the positions. 2023 expanded it to include preseason, regular season, postseason contact practices. So then they added running backs and fullbacks and then 2024 and this is where it's crazy.
They expanded it again. O line, D line, linebacker, defensive back. We'll go down the list. The only one, one of the only ones not on there. quarterback. So that's interesting. We'll talk that, that jumps segues right into our thing. And now you're seeing they're allowed as of this year. That's why you're starting to see them.
They're allowed to wear the guardian caps on their head, on their helmet, as long as the team logo is on there. So this is just super interesting because you're just seeing a piece of, again, we talk about this, we talk about orthopedic sports all the time, but we love technology. And so this is just something else and it's [00:22:00] simple, right?
It's a really simple thing. But if we can reduce these concussive symptoms. Anything helps now again, there was something else about maybe if they have a new helmet option, they don't need that, players are into this, they're trying to use it. You seen this, you see a player maybe has this on and the cue collar, which you guys can look at our old episodes, but this piece of tech is pretty interesting.
Will Sanchez: Yeah, it definitely is. And and I think you're bringing up a really good point as far as the technology, because, and I apologize, I don't know his name, but one of the head guys at the NFL, their doctor, their head doctor that kind of, does the rounds. He said that they've looked at 12 new helmets, six of them are being approved going forward.
And then one of the questions brought up was. This guardian cap and they're saying you're just putting the helmet on top of a helmet, and they go, yeah, we understand that, but this is what we have right now. We don't have [00:23:00] the amount of testing time, which then leads back to the conversations we have prior when it comes to technology yeah, they're utilizing it, but there's still, it's still not, approved and we're starting to see the groundwork.
And that was some of the things that they were simulated We, we are looking at stuff, but we have not had enough time from testing for it to finally get approved. So this is where we're at right now, but they realize that there's a huge emphasis on trying to figure this out. And we've talked about it before, right?
Do you have something new? And we've had guests talking about new tech. How long, right? We talk when winter was on, right? Winter innovations. How long does it take? From concept and testing to finally getting approval and going out there. What are we looking at? 10 years less, what's the normal.
Dr. Grant Garcia: Yeah, 10 years.
But that's the crazy part is this is the 2017 to 2024 use in the [00:24:00] NFL is actually fast, but they don't need like FDA, right? They don't need to make sure it's safe, right? Because it's padding, right? It's not it's a different thing. And it's not approved for patients. It's a different to pay for proof for NFL players in sports, right? So they just want to show, but they just want to show that efficacy for the NFL to approve it. But it doesn't need to be like mainstream. It's not going through insurance. It's not a medical device. Yeah. So it's just different. But yes, 10 years is from start to finish. Obviously there's different things.
We've talked about this before. We're not going to go into here. There's faster pathways, but from very basic idea, brand new idea to that 10 years is a pretty good timeline and that's a long ways to wait. It's a long way for anybody to wait for anything. Yeah, no, this is but this is, they're just trying to, this is a damn that is.
This is a dam and they're plugging the holes in the dam and this plus the two, a thing, it just. Just not good for them, [00:25:00] right? They're trying everything they can in the guardian caps. No offense. They look a little ridiculous, but nonetheless, if they work, that's awesome, but it just shows then makes you question why are we what's one of the helmets?
Like, why do they need this? If they have the helmets?
Will Sanchez: Yeah. And that's exactly what it is that they eventually need to figure out. It's almost like the NHL, they used to play without helmets and then it took forever for them to approve it. And then not only that for the players to buy in, as we see, you can wear it, but only a few players are wearing it. We showed a picture of Jonathan Taylor or Julius peppers or something like that. Not everyone is wearing it. And then based on some of the conversations we've had, Four prior with our doctors, they're going, yeah, the helmet's never going to treat it because your brain is going to squish around.
Anyway, it's still going to move. The helmet is not keeping the brain in place, so you're still going to have some issues. So it's fascinating. I think that's why we wanted to talk about, because it brings up conversation. It's not just what's happening with [00:26:00] two, but what's happening with all these players and with the sport and their biggest concern, and if you're concerned with your business.
You're going, Oh my God, this is happening. Everyone's seeing it and little, and mommy's not gonna let little Johnny play football and we're going to have a crisis of football players on our hands. 20 years from now.
Dr. Grant Garcia: Yeah. But the other thing you want to say is I think as orthopedic surgeons, we were so hyper focused on everything except for this.
And you can't, if you guys are not watching, it's I'm talking about my face or my head. Yeah. So you basically, we don't focus on it. Meanwhile, this is one of the things we've seen the most tech, right? We had the Bluetooth. Conversation stuff. We talked about the helmets. We've talked about multiple renditions of different helmets.
You've talked about areas, the Q collar to reduce, to increase the pressure inside the brain so that you're less sloshing of the brain when you get hit. We're still scrounging for options and this is, and there's no surgery to fix these problems. There's no pill, there's no medicine. [00:27:00] We are literally just using the same device, the helmet and modifying it.
Helmets. They look cool, but they don't look that much different than the helmets from 10 years ago, right? Did they? I don't really see much. I know there's a lot of technology, so I'm not belittling anything in the technology. But the fact is, now that we have to add these caps. That are like basically just like mittens on top of there to try to hopefully help prevent this situation It just shows the situation that we're in right but at the same point, I think it's awesome The side thing this to be I don't want to be a debbie downer because we're talking about concussions and you know all this stuff
Will Sanchez: Love also, let's be clear right?
This is what makes it hard right? These are tough conversations And this is a sport that we like to watch. You have a New York giants background, right? I've got, like we, we talk sports, right? That's our show, right? It's orthopedics and sports, and this is what we do. And this is what we love.
But at the same time, we can have real conversations and this is exactly what that is. And it's a little maddening [00:28:00] at the same time. Dr. Grant Garcia: And also I want the listeners when they're watching the games to be like, oh, that's the guardian Catholic. That makes sense, right? Like, why are they doing that?
Like, why is that guy wearing that thing on his head? That's what I said when I saw it the first time and you've seen him at practice and now when all of a sudden we're doing research on Tua and I watch an article on my feed, I see something about the guardian caps and it makes sense now and you read about it, but it's actually pretty interesting because I didn't realize his route for that long and the history is really interesting, but you know what I'm going to wonder?
Do you think they're going to be adding the QB to the mandated practice thing?
Will Sanchez: Yeah. Yeah. Let's see. Yeah. Yeah. Yeah. I know. I'm going to get a text from you and be like, Hey, guess what? Same, the same way we look for the, I look for the Q collar, right? We've had, we've talked about the Q collar. I recognize it.
The second I see somebody wearing it in the NFL game or college, I go, oh, he's wearing a cu collar. So just recognize that still. My, my favorite tech is the urinal with the player. I know it's you,
Dr. Grant Garcia: you want, you're upset because you missed out on the [00:29:00] patent on that one. I know you're upset about That was a good stuff.
Podcast is people learn. Every aspect of sports technology right now, they're seeing, you watch a show and you go, Oh, like they talked about Aaron Rogers speed bridge. You know what that is? You talked about, now you see the guardian caps. Now you see the Q collar. Now you see the new helmets. Maybe someone miked up, all those things.
Heads up displays, things like that, like where we're going. And so now we can give you what's the latest tech and how it relates to the medical field. And so anyhow, we did our, we did a good job of staying under 30 minutes, like we always do.
Will Sanchez: But yeah,
Dr. Grant Garcia: it's good.
Will Sanchez: By the way, that heads up helmet that we did a show on for deaf football players has finally been approved.
So they had approved it for one game when we first had this discussion. They just recently, maybe a week, two weeks ago, somewhere along that timeline approved it for full time use. So that's another thing with technology and it got more to come and good for those players now [00:30:00] to level the field a little bit.
When it comes to them enjoying the game, they love to play. So anyway, enough of that. Congratulations once again on your award. It's always great talking with you is always great.
Having these. Real discussions and we've got more shows, headed our way. Thank you Everyone
Dr. Grant Garcia: always good. All right. Peace out. Bye
Audio Transcript
2024 NFL Season: Injuries and Comebacks
Will Sanchez: You know, that's our jam. Welcome to sports doc. Talk will Sanchez here with our residential New York giants fan, Dr. Grant Garcia. I think he's an orthopedic surgeon and sports medicine specialist as well. But today to kick off the 2024 NFL season, we are giants fans in the house. Uh, hopefully we don't lose any of our.
[00:00:26] Will Sanchez: Regular fans, but I think hopefully they'll, uh, they'll excuse it. Dr. Garcia, man. Uh, first welcome. And then how excited you to finally have some football coming around.
[00:00:41] Dr. Grant Garcia: So excited. It's a, I'm not, I watch some sports, but my wife will say, you know, I do a lot of other stuff too busy in my life, but when it comes to football season, especially for the Giants, I find time.
[00:00:51] Dr. Grant Garcia: So I'm super excited. Uh, and plus, you know, Being a sports surgeon, this is where all the crazy stuff happens. You get to see crazy comebacks, [00:01:00] which we'll talk about today. Um, you learn about all the innovative stuff. I mean, really, when you talk about the cutting edge sports medicine, it's all to get players like these NFL players back in the game.
[00:01:12] Dr. Grant Garcia: And so, you know, it's really exciting. I love, I love football. It's my favorite sport.
[00:01:18] Will Sanchez: Yeah, listen, we're excited. And just to kind of let the, our listeners or viewers, um, know, you know, this is our 2024 NFL season. We're thinking about key injuries from last year coming into this year. Uh, comeback players, eventually I'm going to ask you, who's your comeback player of the year if you had to guess, uh, so we'll kind of get into all of that, uh, later on.
[00:01:40] Will Sanchez: September 5th, we kick off the season. I mean, Two teams, right? Possibly two MVP candidates in Patrick Mahomes and Lamar Jackson, Ravens chiefs, the defending super bowl champion. I mean, Derek Henry is now with the Ravens. He's left the [00:02:00] Titans. There's so many storylines, so many reasons to get excited. But for us, we're going to talk about the players getting ready for this year, but.
[00:02:09] Will Sanchez: I am super excited to kick off the NFL season, especially with that doozy on Thursday night. And as always, we like to give a shout out to our sponsor, the recovery shop. We know it's our favorite, not even our favorite, the patient's favorite, Dr. Garcia's favorite. When it comes to all the stuff that you need from the recovery shop, and I'll kick it over to Dr.
[00:02:31] Will Sanchez: Garcia because he uses them all the time for his patients.
[00:02:38] Dr. Grant Garcia: You know, I love this place. And again, you know, obviously they're sponsors, so we bring them up every episode, but it's great that people can hear about this. And I was just talking to my friend in the car who's works in California. He's going to plan on start using this.
[00:02:49] Dr. Grant Garcia: Cause he's like, Hey, how do I get this innovative stuff? Right? Like my normal products, I can't cover it. They're not covered. I can't get them into my patient. My patients want the newest stuff. And so the recovery shop allows you. [00:03:00] And what's really cool about it too, is if, you know, we have someone on this episode and they talk about something new I can offer at the recovery shop for patients.
[00:03:06] Dr. Grant Garcia: So it's all built into that one section. So it's really nice for surgeons to be able to offer patients. The newest stuff that may not be from the, the medical realm, but sort of the tech realm. Yeah. Um, on top of that, it's all, it's all together vetted for you. It makes it really easy. And the patients have raved.
[00:03:24] Dr. Grant Garcia: I mean, we're not gonna go again on this episode about how much we love the Nice machine, but you know, the ability to offer all those products like that, or the res or something else. The res, yeah, that's a good one in one place. And really I do, I do feel like. It improves the recovery for my patients. So check it out if you're a surgeon you can offer this to Uh contact myself, uh the website check out the website here Um at shop recovery.
[00:03:50] Dr. Grant Garcia: net and you'll see it on our links also. So thanks again guys
[00:03:54] Will Sanchez: Yeah. And that's a great one. And before we move on from that, you know, we started talking about this way [00:04:00] beforehand. So check out our previous shows. We talk about the next machine. We talk about the rebless. We talk about this, you know, these futuristic, you know, get better, heal better, something's better for your nutrition.
[00:04:14] Will Sanchez: We've gone in depth about these machines. So now we finally have a platform that we can also make a reference to. But if you want to hear more about that. Go back, check our shows. We always have great write ups. We have trans, uh, uh, transcripts. So check us out at sports doc dot, uh, talk. com. It's a mouthful right there, as you can tell, but I'm really excited, uh, about all of that, but we're excited about.
[00:04:37] Will Sanchez: This season, before we get into that, I just have a question. I know you do work with the high school kids. Are you picking up, uh, once again, working with the football team and working with the high school kids, give us a little update, uh, for the 2024 season for Dr. Garcia, uh, this upcoming football season.
[00:04:56] Dr. Grant Garcia: Yeah, so I, uh, you know, previously we took care of pro [00:05:00] teams and we've had opportunities for those things, but, and those are fun. We've talked about them before, but, uh, I have a special connection with Mercer Island High School, uh, and that's where I currently live on Mercer Island and I went to high school there too.
[00:05:13] Dr. Grant Garcia: So when I came back, that was, I wanted to take care of the team that used to be, I used to be with my, my wife also went to high school there. Wow. We went, yeah, no, listen, I'm told you I'm going to drop a little bit each time. So we went to high school there and I remember she was in the band and we used to go to the games and hang out and I had my Letterman jacket on and now I get to be the team doc for them.
[00:05:36] Dr. Grant Garcia: And I take care of the players. Now, of course, when they come into the office, they're like, you didn't go to Mercer on your way to old. I'm like, dude, I'm not that old yet. And so, you know, but it's so much fun. And so, yeah, I'm super excited, you know, myself, and actually, uh, you've had Dr. Wayne while in here.
[00:05:52] Dr. Grant Garcia: He's also going to be helping out, uh, because he does the, we all basically help. Like I do most of the sports. I did the triage and [00:06:00] then, you know, foot and ankle. We had one of the coaches tears Achilles. You never, you know, who fixed them. Yeah. Yep. Dr. Anthony. Yeah. Dr. Wayne. Wow. When they have the hand injury.
[00:06:10] Dr. Grant Garcia: So, you know, we have a whole list of docs that can help out the team. It's really awesome. And I'm on the field with them and I have a lot of fun and I get to see everybody went to high school with sometimes, uh, in the stands with their kids. So it's a super awesome experience. It's so fun to get back. So, yeah, I mean, I'm, I'm so excited.
[00:06:26] Will Sanchez: It's so amazing to think about that. Right. And it's just kind of a reminder for all of us as we do our part within our communities that, you know, you leave school, you go off to college, you, you live a life and then all of a sudden you're, you know, you're coming back, uh, um, you know, three 60 and, you know, back where you started, but now you're giving back, uh, to the community.
[00:06:46] Will Sanchez: Um, you mentioned Dr. Yee and, you know, it's, it's one of those things when it comes to Dr. If you see in them. And you're not there to see him as a doctor. It's great to see him, but if not, it usually means that something has gone [00:07:00] wrong. And, uh, if we look back to September 11th, 2023, uh, four plays in as the jets.
[00:07:09] Will Sanchez: Came out to kick off the season and they were taking on the Buffalo Bills and they were at MetLife Stadium and the stadium was going crazy. It was jam packed and they had the, the, the light show, the fireworks and their brand new toy comes running out of the tunnel with the American flag in his right hand, leading out the cheer and the crowd and the fans are going.
[00:07:37] Will Sanchez: Absolutely bonkers. And you're saying, oh my Lord, what a way to kick off the 2023 season. And for all my friends back in New York that are Jets fans, not so much my Giants fans, they are as excited as can be going back to maybe last time with Vinny Testaverde was with Bill Parcells and Curtis Martin saying, we have a [00:08:00] chance four plays into the season.
[00:08:04] Will Sanchez: runs out of the pocket and Dr. Garcia, what happens next?
[00:08:10] Dr. Grant Garcia: Achilles tear. Emilia calls his buddy, Dr. Elitraj, which we've heard all those things about and is on the opera room table in a few days. And unfortunately the rest of this history, except for the Recurrent news articles talking about speed bridge and how quick he was going to get back.
[00:08:27] Dr. Grant Garcia: So, you know, I think, uh, we'll see how the season goes. You know, we've, uh, this is obviously not, we've had this talk a few times. We had the Olympic talk recently. We had a whole separate section when he injured it. We talked about this. You've gone over your recovery too, with Dr. Yee. So we've had all these discussions on Achilles, but this is now again, quarterbacks are different, right?
[00:08:49] Dr. Grant Garcia: This isn't, uh, Simone Biles having to go jump around and do back flips. Or front flips or her own new tricks, you know This is a guy that can sit in the pocket and do his throwing, you know He's never [00:09:00] been known for his high level mobility. Um, But what's important I think for this episode which you can bring up and we're not going to go again We try to talk about orthopedic sports all the time yeah, but I do want to bring up a little data because this is really interesting because like Even as orthopedic surgeon I can fire off my opinion, right?
[00:09:16] Dr. Grant Garcia: My opinion is this is not a good injury My opinion he's not going to recover and patients, you know, that stuff that you know, they understand I got experience I see these things But the data doesn't lie. And so it's really interesting to see the data because we're so used to seeing like the one or two athletes that get back.
[00:09:31] Dr. Grant Garcia: But what about the guys in the practice squad? What about the guys on the, you know, that are not the starters? How do they get back from these injuries? Because really, they're the ones that, you know, we talked about before, like, an injured LeBron James is better than most of the players on the court, right?
[00:09:46] Dr. Grant Garcia: But an injured professional player is no longer a good player. Right. So how long does it take them to get back and can they get back? And this may segue into our discussion of our controversial quarterback, [00:10:00] Daniel Jones and his ACL tear. Um, but you know, there's two articles we'll talk about. So the first article is really easy to kind of go over, but basically it looks at return to play.
[00:10:11] Dr. Grant Garcia: So return to football in the NFL for wide receivers. Now it's not Dan Jones, a quarterback, but I looked these up because for this show, I was like, well, I want to know, cause I know Will and I are going to talk about what do we think Dan Jones is going to get back? What's his performance going to be like?
[00:10:23] Dr. Grant Garcia: And I was like, well, the other, I'm sure someone's looked at this, right? Like you want to know this data. So the wide receivers was interesting. A wide receiver. Achilles, patella, and ACL are, are the greatest effect on the career. And actually they do have a decrease in success after one year of surgery.
[00:10:42] Dr. Grant Garcia: And what's interesting, so we always talk about the one year mark, but I always tell patients, remember we talked about this, Will, other than the Adrian Peterson absurdity, which we saw. Yeah. Most players are not better the first year they're back and they're not at their full level. And it takes, I mean, Saquon Barkley, right?
[00:10:57] Dr. Grant Garcia: Obviously we, you know, it's kind of a dirty word now for New York. [00:11:00] Um, but, but, uh, you know, they found that, you know, this, it takes a section year and sometimes they don't get back. And of the four major sports, NFL players, so the hockey, football, basketball and baseball, the NFL, the shortest injury, the shortest careers afterwards in the highest decrease in performance after ACL injuries.
[00:11:22] Dr. Grant Garcia: So it's just something for people to be aware of. But if you're a New York Giants fan, you'll like the second article, second article, same guy, Burgess et al. And he, they found that there is no significant decrease in performance for AC reconstruction for quarterbacks. So that is a good thing for us to hear.
[00:11:41] Dr. Grant Garcia: And maybe the mental side of things, but not for the physical. So running backs, wide receivers, we added running backs, decreased performance, but for some reason, quarterbacks do not have a decrease in performance afterwards. And it's probably because. What's their main use of their bodies is their arms, right?
[00:11:56] Dr. Grant Garcia: I mean, they have to aim, they have to have core, but they're not doing the same [00:12:00] thing. A running back wide receiver, you want that explosive speed. You know, we've seen Odell Beckham Jr. Two ACLs, you know, it's, it's, uh, they're not as good the second time. And it takes longer. And you know, these guys are freak athletes.
[00:12:12] Dr. Grant Garcia: So
[00:12:13] Will Sanchez: yeah. And just to let, you know, let our listeners know, these are studies going back, uh, they reviewed it from 88 to 2017. So it's a, uh, large chunk of data, uh, that they were able to make a reference to for, for the numbers that Dr. Garcia just, um, explain. Go ahead, Dr. Garcia, you're going to say something.
[00:12:35] Dr. Grant Garcia: Well, we're going to make this even more complicated because you know, I like to do this. But if you think about this, we didn't have the new ACL techniques we do. I just read an article yesterday and Will's going to get too excited when I tell him that. So I'm going to say it quickly and hopefully we can move on from the topic.
[00:12:50] Will Sanchez: We're going to move on.
[00:12:51] Dr. Grant Garcia: Adding internal brace, any of your, any of your ACL constructions or hamstring, which is they have here, private teleten, [00:13:00] which they got in quad. So all three of the graphs from, and these are pro players are getting, they're getting Grafts from their own body, decreased tear rate, decreased, uh, increased speed, uh, sort of recovery and decreased the stretching of the graft.
[00:13:13] Dr. Grant Garcia: And so, you know, probably one of the reasons these people don't get back as much is part of it is also, is there some natural laxity? Do they re tear it? And those type of things. So maybe the data we might see in the next, you know, 10 years is actually, there isn't a decrease. So we have technology. So you gotta be careful.
[00:13:30] Dr. Grant Garcia: It's just like when you look at anything, I just told you all this data, but now we're not in 2017, are we? We're in 2024
[00:13:37] Will Sanchez: with new, with new technology, new concepts. Uh, our previous show, we were talking, um, with, um, with the gentleman from Arthrex and about how fast the technology is moving. Advancing. So it was like, okay, this works.
[00:13:54] Will Sanchez: Yes. But how can we make it better? Right. Just so yeah, 2024 [00:14:00] and 2028 and 2030, you know, we're probably looking at a whole slew of other things because as we know, we can see it in our regular, you know, day to day technology is moving so fast right now that the numbers are changing, um, at extreme rate, probably like we've never seen before.
[00:14:19] Dr. Grant Garcia: Well, and look at the, look at the, uh, look at the people now. I mean, we used to have Ember, Tommy John, you could never throw again. Now I'm talking about designing a new technique and how it's going to make people get better and how we're going to add the internal brace and how we're going to add different techniques and we're developing new things so that we can do the technique faster and more efficiently reduce revisions.
[00:14:38] Dr. Grant Garcia: You get us, if you get a first time, Tommy John reconstruction, you fail it. We now have better techniques for a second one. You've heard of people, you've heard of baseball players coming back after a second Tommy John. And so we, that was unheard of, right? None of this is, I mean, we could do a whole show.
[00:14:52] Dr. Grant Garcia: This might be a good one. We'll later on what we, what we do now that we like what players can get back. Now they never were able to come back. [00:15:00] I mean, a patella tendon rupture like Victor Cruz had or other players. Yeah. We've had that show a long time ago that was done. I mean, you were done, you were never coming back.
[00:15:10] Dr. Grant Garcia: Yeah. We have all this fancy gear, biologics. Awesome recovery stuff. You know, we've talked about nice machine talk about blood flow restriction. Uh, There are ways that we can do things now Now the human body is still the human body and we have to be there and you have to have the right surgeons Which nowadays, you know, if you're an athlete, you can go anywhere in the world, right?
[00:15:31] Dr. Grant Garcia: Like it's not like you got to like ride a horse and buggy to go find the next guy. Like you hop on your private jet and you go and get, you hope you go and get fixed up by the person you think is going to do the best job. So, you know, it's a, it's a different game than it used to be, but it's a, it's pretty cool too, because as at a sports fans or as a surgeon that likes to watch sports as well, it's exciting to see at, it's terrible to see an athlete get injured and never come back because.
[00:15:56] Dr. Grant Garcia: You know, the ones we're watching out for are the stars, right? It's really sad when [00:16:00] you lose that level. Of athleticism, obviously there's retirement from injuries and everything else, but it's pretty cool. Like, I mean, the, where we're going is hopefully we can see these players play longer, um, and play better, which is, which is awesome
[00:16:13] Will Sanchez: before we move on from Aaron Rogers, I kind of want to bring it up, right?
[00:16:16] Will Sanchez: So there's, there's two things I want to bring up his injury happened week one, September, right? Right now we have, uh, Kirk cousins that had the same injury week eight. Now. We'll find out if Kirk, he's not on the P, uh, the pup list and we'll kind of get into that later on, you know, but what are your concerns as a surgeon week one to week eight?
[00:16:43] Will Sanchez: So now we're talking two months later. Right. Coming back at the same time. Right. So you're starting off at the same time with week one in 2024. And then you're also comparing. So one of them is a time assisted and another one is age assisted since he's [00:17:00] younger than Aaron Rogers. So. Trying to see what's the way I want to kind of word this.
[00:17:05] Will Sanchez: If you had to pick one or the other, when it comes to healing fast and being ready for the start of the season, are you more concerned about the age? Or are you more concerned that one of them had recovery two months earlier?
[00:17:19] Dr. Grant Garcia: So no offense, Dr. Eltrod, he's amazing. So I'm sure his surgery was bomb proof, but I would choose the younger age to be more likely to, I'd be more motivated by the younger age.
[00:17:30] Dr. Grant Garcia: I just hate to say it, you know, Even a few years is a big difference. And Aaron Rogers looks old, Kirk Cousins still looks young and you know, people, people's bodies are different, right? Like I get in, I get into people's bodies and I do a lot of ACLs and ligament surgeries on these patients that between 20 to 40.
[00:17:48] Dr. Grant Garcia: And sometimes I get into a 35 year old knee and I say, this is not a 35 year old. This is a 40, 45 year old knee. And sometimes I get in and go, holy cow, this 35 year old's got bone of a 20 year old. Right? [00:18:00] And you can kind of, you know, you don't always tell, but you can kind of tell, you know, that the age is a little bit, is more showing on there.
[00:18:07] Dr. Grant Garcia: And so it does concern me that, you know, is, and also, I don't know, maybe is, is there other things at play too? Are they taking weird supplements? Are they weird dieting things they're doing? You know, I don't know all the background to that. Yeah. Um, but you know, I know that, I know that both of them probably got amazing surgeries.
[00:18:25] Dr. Grant Garcia: Yeah. Yeah. Um, but if I had to choose one, even with a little bit of a difference in the timeline, uh, I would choose, uh, Kirk Cousins.
[00:18:33] Will Sanchez: Got you. Got you. And then, you know, we always, we always want to remind our listeners that, you know, this is, we're always talking about what, what we think, but without dr Garcia actually going into the knee and you made a reference to that and being there to see the ins and outs.
[00:18:49] Will Sanchez: It's, you know, it's never a verbatim 100 percent but it's kind of like the guest because I was curious, right? Because those are two factors, right? Time versus age. I [00:19:00] know my injury later on, right? Was way different than when I've been injured earlier on. And, um, we know that we, we say it all the time, athletes are freaks, especially the way they, uh, they heal and perform.
[00:19:12] Will Sanchez: And we know that Aaron Rogers will not lose his fastball. But it will be really interesting to see a 40-year-old body start to take hits. From the season, so I don't wanna scare any of the Jets fans. We're gonna kind of move on because they've had enough suffering over the years. We might [00:19:29] Dr. Grant Garcia: get some, we might get some nasty comments on our podcast.
[00:19:31] Dr. Grant Garcia: Yeah, yeah, yeah. Some Angry Jets fans,
[00:19:33] Will Sanchez: um, you know, and the quarterback and the team that we're rooting for. We expecting a, a, a, probably a, a rough year, um, as far as wins and losses. So we're just kind of brace ourselves for that. But Daniel Jones is coming back, uh, from his injury. Why don't you talk about that injury a little bit and then we will, uh, we'll take it from there.
[00:19:52] Dr. Grant Garcia: So he suffered an ACL tear. We've talked about ACL tear ad nauseum on this show. It's obviously a very hot topic ever. It's so [00:20:00] common. I mean, we could go through the, we went through the, in this preparation for this player's, uh, injury list. You know, we basically, I kind of had to say, let's not talk about any more ACLs on here.
[00:20:08] Dr. Grant Garcia: Right. Cause we've done it so many times, but it's a big topic. So I don't know what else he had done. I'm assuming just ACL, they didn't say anything else on meniscus or anything else related, but we don't know. Um, but obviously he's out for the season now. He's back. Uh, you know, the question is Dan Jones, you know, you may, you like him or you hate him, right?
[00:20:25] Dr. Grant Garcia: There's nobody, there's no in between. There isn't. Yeah. Um, but he was known for his speed, right? He was fast. Like that's, I mean, give him that. He's one of the fastest. He was like one of the, he had the fifth and most in rushing and he was, he's one of the fastest quarterbacks, uh, in the NFL. Um, and he's tall and he is big.
[00:20:44] Dr. Grant Garcia: So, and he's bulked up, which is nice.
[00:20:46] Will Sanchez: He's a big guy. Yeah, but can you
[00:20:48] Dr. Grant Garcia: take, but can you take those same hits, right? Like,
[00:20:51] Will Sanchez: or should
[00:20:52] Dr. Grant Garcia: he, he's not a pocket player. Don't get me started on a pocket player. No, no, but he's not a pocket player, right? He's not, he [00:21:00] relied last year, the last few years on his ability to get out of the pocket and run and avoid tackles because he had such a bad offensive line.
[00:21:07] Dr. Grant Garcia: Right. So it's just, I don't know. I hope he can, but you know, there's that rust too of getting, you know, your ACL torn, right? He's got to come back from that. Oh, the one thing that he has dealt with is he's dealt with so much adversity and so much negative publicity and negative comments about him that I don't really know if this is going to make a difference for him.
[00:21:26] Dr. Grant Garcia: I think some of the players that have been the best themselves, the whole five years of their 10 years of their career, and then they injured their knees and they're worried they're gonna really get back, I think there's more of a mental aspect. I just don't. I honestly think he's too tough to even be stressed about it.
[00:21:39] Dr. Grant Garcia: To be honest with you, he's put up with so much stuff, more than most quarterbacks would ever have to do in their position,
[00:21:44] Will Sanchez: especially in New York. One of the reasons I brought up, um, Daniel Jones, besides, you know, the whole jets giants thing and, and everything else, but it's, my concern is The neck injuries and we talked about it briefly before we, uh, hit record on [00:22:00] the show.
[00:22:00] Will Sanchez: Um, he's had a few neck injuries he's had at different times. You know, I think going back to 2019, he suffered an injury and then, uh, last year before he got hurt, he had a neck injury. This, and then he hurt it again. They said it was unrelated. Um, so I am concerned. Not so much from the knee aspect and maybe you as a surgeon going, I'm concerned about the knee, but I'm also concerned about the neck, uh, injury.
[00:22:26] Will Sanchez: And, you know, I'm showing here for those that are listening and not watching us on YouTube Packers running back, AJ Dillon, which is their star running back. He's on the season ending IR he's done for the 2024, uh, seizing with a. Stinger injury and stinger is always kind of like, it's always a funny thing because I go, well, that doesn't sound like a big deal.
[00:22:49] Will Sanchez: It sounds like you got like a little pitch, something or other, and you're going to be fine in a week or two, but apparently it is. Can you talk about, you know, what kind of injury that is? And it sounds like. That's serious [00:23:00] enough that without taking a snap in the 2024 season, getting hurt in at a joint practice that you are already done for the year.
[00:23:11] Dr. Grant Garcia: So let's go through this. So first of, I'll talk about the Dan Jones thing. So anytime the word is repetitive neck injury, I get worried. And what the heck puts you out for a couple months? It's probably something cervical, which is in neck and it's probably in the disc and he could be getting some bulges and they're concerned about it.
[00:23:29] Dr. Grant Garcia: And maybe it's pinching a nerve. I don't really know. And they were super cryptic about it. I mean, he said he had a neck injury, but he's had this repeatedly three or four times. Yeah, that's not, that's not a neck spasm. That's something where they're worried about the health of his, him. And if he gets another hit, could he like get paralyzed type of thing?
[00:23:45] Dr. Grant Garcia: In my opinion. Okay. Yeah, I don't think it's that bad, but I think that there's something else going on. They're not telling us and that's that's okay That's what that's the nature of football and the nature of the show is we get to do a little guessing Um with the stinger, so usually a stinger is when [00:24:00] you get hit on one side It's unilateral.
[00:24:02] Dr. Grant Garcia: So one side you get hit on the side and it goes into your brachial plexus So you imagine i'm not going to get too much in anatomy But imagine you can try to show here imagine you have your neck and all the nerves come off and they go into like your upper chest Area down to the shoulder and they, they branch off like this.
[00:24:17] Dr. Grant Garcia: And when you stretch them, you get your whole arm. Just like, like you feel like a sting, like that's why I call it a stinger. Yeah. Okay. And that's like, remember you guys ever hit your funny bone? Yeah. Imagine the whole arm. The whole arm is where it happens. It happens and it goes away, right? And it's usually a single, like unilateral.
[00:24:34] Dr. Grant Garcia: We say you get a unilateral stinger. You're good. Like 10 minutes rest, make sure they're all normal and then they go. So that's why I don't understand about this. I think that they're trying to dumb down the injury. You get a bilateral stinger. That's when you basically likely had some real bad neck injury.
[00:24:48] Dr. Grant Garcia: Like you're like a disc in your cervical spine, which we've talked about with Dr. Schaefer before on this up on the show. And that does concern me because I don't even know if that's considered a real stinger, right? Like I think they're just doing, you know, they say like [00:25:00] knee contusion or knee sprain or meniscus meniscus contusion, because they're trying to dumb it down.
[00:25:06] Dr. Grant Garcia: Yeah. And what they're trying to do is try to play it off as not that big a deal. But the fact is, if you're out for the season with this, that is not good. So I think, you know, I don't know what he had. I'm surprised he's not getting surgery when he goes out like that. Um, but there are some notable neck injuries that have happened in the NFL.
[00:25:21] Dr. Grant Garcia: Obviously, the most prominent one is Peyton Manning. He had multiple neck surgeries. Uh, he had a spinal fusion, so they actually fused. We talked about disc arthroplasty, a replacement with Dr. Schaefer. Yeah, that's where they actually, and that's, that probably would have been, he probably would have had that now, but this was, this was a while ago, 2011.
[00:25:41] Dr. Grant Garcia: So now the new stuff, which we talked about again, remember if you look at all the performance of these surgeries and 10 years later, it's probably a different surgery, right?
[00:25:50] Will Sanchez: Yep.
[00:25:51] Dr. Grant Garcia: So
[00:25:52] Will Sanchez: yeah, we had a great discussion with dr Andre Schaefer. Um, you know, with, and he was showing us all the cool little gadgets and you know, everything else [00:26:00] that they're using, uh, in that cervical area.
[00:26:02] Will Sanchez: So, and we go back to 2011, that's a long time. We just started off the show saying it, things are moving fast, let alone going back to 2011. You know, what, what kind of recovery with Peyton Manning and he was getting a little bit older at that point too, but what kind of recovery would he have had because we know his super bowl season I mean, he could barely move and barely throw the ball because he was just so jacked up.
[00:26:25] Dr. Grant Garcia: Yeah, I mean, we think we talked about this a while ago, but at some point, he couldn't even feel his arm. He was just throwing with no triceps. Cause one of his nerves was out. So, I mean, it's just, just craziness, but you know what I said, LeBron James, Peyton Manning, when they're missing something, they're still really good.
[00:26:42] Dr. Grant Garcia: Yeah. Also helps have a good team with you. And then David Wilson's one of our, the favorite guys used to see him do backflips on the field. And I remember he was kind of a freak and they talked about the next big thing. And unfortunately after like a year or two, It's something called spinal stenosis. So it's where you're, I'll go into [00:27:00] basically briefly, but you basically have like your, your whole spine.
[00:27:02] Dr. Grant Garcia: This is like really straight and it's like not made to bend well. And if you get hit, it can be like instant paralysis. So if you have that, it's automatic retirement, which is what he had. And it actually can be happening commonly in football players. Uh, so it's a pretty scary thing. So when they diagnosed that with him, he was out.
[00:27:18] Will Sanchez: Yep. He was, uh, he was a promising, uh, running back also kick returner. Uh, we thought he was going to be another compliment along with Ahmad Bradshaw and, and, you know, some of the other guys that were on that Giants team. And I believe he was a either first or second round draft pick, maybe out of Virginia.
[00:27:35] Will Sanchez: Anyway, at this point, I'm probably just guessing here. Uh, no, I remember he used to do
[00:27:39] Dr. Grant Garcia: the best show. Is that, remember that little. Intro. They had him. He was catching rabbits in the field or something crazy. They showed how I got so fast. That's what you do. Well, you and I can do that. We should do rabbit catching.
[00:27:49] Dr. Grant Garcia: We'll get ourselves.
[00:27:50] Will Sanchez: I can't catch a spider right now. I ain't going nowhere. That's it. I'm going to see how fast I can catch the remote out of, out of somebody's hand on the couch. [00:28:00] That that's, that's the speed that we're at right now. But, uh, you know, stick, you know, listen, we're talking about catastrophic injuries to the running back.
[00:28:07] Will Sanchez: Um, there was. I don't recall last year and obviously the year before that we had the scariness that happened in Cincinnati on the field. But as far as devastating injuries, um, what happened to Nick Chubb on that game and we, we reached out immediately. You know, uh, when we were texting each other saying, Oh my God, did, did you just see what happened?
[00:28:35] Will Sanchez: Um, to, uh, Nick Chubb on, um, when he was playing against the Steelers where that leg bent in ways that, you know, You, you just, you just didn't want to see, you know, we, and I have a picture not of the injury. 'cause I just didn't even, I saw it and I just didn't wanna put it up there. But, you know, he, and, and I want you to break this down because it said damage to the medial to, to the MCL, the medial [00:29:00] capsule and meniscus.
[00:29:01] Will Sanchez: And then he had a second surgery on November 14th to repair a torn ACL. And I know some of this and, and this is why I'm gonna have you kind of break down this. Knee, what happened to the knee, what they did, and also the fact that they went back and fixed a previous ACL surgery, going back to Georgia, where he had a really nasty injury.
[00:29:23] Will Sanchez: I believe it was on the sideline where his knee bent in a way that it wasn't supposed to. And when they went back in, they said, well, we're going to fix, we're going to fix that also, and redo the entire thing, not just kind of leave it the way it was. When you hear about all of this and going in and doing first off multiple surgeries, it's not just one area of the knee and and how you're fixing certain things to connecting to others and whatever peptides or whatever else he's taken in order to recover.
[00:29:55] Will Sanchez: Just I don't even have a question. What's your initial thoughts when you hear [00:30:00] about all this?
[00:30:01] Dr. Grant Garcia: So I remember, I remember this show and we saw the knee dislocate. Right. And when you told me he was going to get a small surgery or he got a small surgery, I was like, there's no fricking way. Like, and, and the problem you have is I know Dr.
[00:30:16] Dr. Grant Garcia: Vose is awesome. I think he went to same place, HSS. And then I know the other team doctor, uh, who's a friend of mine went to residency with me. Um, They're both great surgeons, great guys. But I think this press release was a little, the press release they talked about his knee was a little soft and they tried not to dumb it down what he had.
[00:30:34] Dr. Grant Garcia: I mean, this is a nasty injury and you know, they did it in two parts. And one of the reasons they didn't two parts, which not everybody does it that way, but they didn't do parts to reduce the stiffness, right? Cause it's, you hit up, imagine like. If you repair only part of it, the knee, then it got to have time to calm down.
[00:30:50] Dr. Grant Garcia: They use the smaller scope and nanoscope is actually an Arthrex products. A big like thing is like, can we make this incision smaller? I'll be honest with you. It's a great product, but [00:31:00] I'm not sure that this made a difference in his swelling, but I know that it's kind of a fancy thing they like to talk about.
[00:31:05] Dr. Grant Garcia: The most minimally invasive opt and we can talk about this at some point. Yeah. And then they went back and they did, you know, they use special screws. for healing of the ACL. And somehow his PCL didn't get torn. So I'm I think this I think there was more to the story. but obviously this guy is a freak, right?
[00:31:23] Dr. Grant Garcia: So they obviously had to redo it. I think we had talked originally did some bone tunnel grafting because you know, the problem you have is once you have an ACL, if you, if it's not in a good spot or weakens out, you might need to get bone graft done, which we had talked about. Remember you and I were talking about this cause we were like, how are they not bone graft?
[00:31:40] Dr. Grant Garcia: And then all of a sudden you found it. They went in there and they didn't realize how bad it was. And then they ended up doing a bone grafting or something crazy. So Unfortunately, guys, with this one, I don't think that the article is correct. And I think there's missing some things. It's just way too simple sounding for what we saw on the TV.
[00:31:57] Dr. Grant Garcia: It was absolutely nasty. But [00:32:00] what's more important, I think, is if they finished the second surgery and they felt that they had a solid repair of everything and reconstruction, then. I think that, you know, hopefully a guy like that can come back, but I think his career is limited. Um, I don't think we're going to see the same Nick Chubb, but we will see, and that's the whole point of this show, right?
[00:32:18] Dr. Grant Garcia: To prove me wrong. Maybe there's, you know, the newer technology they used is going to get him back and things that we've never been able to see. But I mean, I just read an article on this, multiple ligament injuries. So ACL, MCL, multiple injuries actually get back the same amount as a regular ACL. Now, the problem is it's not a revision.
[00:32:36] Dr. Grant Garcia: Which is a different animal, right? A second time. And we all know second time for anything's not good. So, you know, we'll see. I think my hat off to Dr. Booz, if this, if Nick Chubbs comes back and does it just a similar season to what he had before, I will be, I will eat my words and I will be very impressed.
[00:32:53] Dr. Grant Garcia: So good luck.
[00:32:55] Will Sanchez: Yeah, I mean, listen, we don't need him to be the way he was because you, you know, [00:33:00] you, uh, we're very clear, you know, you usually don't come back to the way you were at least initially right away. But if he could get back on the field, take a couple of hits, the leg responds. Well, that fear because I'm, I'm assuming.
[00:33:15] Will Sanchez: That there, I know for myself, there will be that fear factor, right? Because this was a tackle. This was Minka Fitzpatrick coming in to tackle him. He didn't want to deal with the big man, went low, right. And then the leg didn't give out, stayed right where it was. And the knee went right. One way the leg went the other, and you know, the rest is, uh, a nasty, nasty, uh, history there.
[00:33:39] Will Sanchez: So if he can get back on, on the field and, you know, and big picture is yeah, you're, you're able to walk around as, as you get older. Right. And we're hoping that we have advances in arthritis and things like that. Right. Because we always try to think about not just today, but tomorrow, uh, like all the normal folks like us, you know, that just having some [00:34:00] quality of life there, but, uh, it's, it's absolutely amazing.
[00:34:05] Will Sanchez: And, and I, I remember when we were talking about this, I said, what happens if something's pinching something else and they have to go in right away? You know, did, did they, Put things back in place and let it calm down. Or is that something that was instantaneously that they had to go in? But perfect scenario is to let it calm down first, right?
[00:34:26] Will Sanchez: Stabilize it and then go in.
[00:34:29] Dr. Grant Garcia: So it depends on the way it is. I mean, if it was torn artery or something like we've seen those crazy ones in some of these, there was that one player for the Browns that had to have the artery. he dislocated his knee an emergency, right? Like yo lose his leg. I don't thin case.
[00:34:43] Dr. Grant Garcia: Obviously they chec as soon as they can. So, idea to let the body calm discussion we can have at kind of like the idea of So as a sports surgeon, someone comes in and they tear their knee like this, like multiple ligaments, there is some [00:35:00] discussion. This is a debate on all these. I mean, I was just talking at one of the meetings for Arthrex and I showed a case and they're like, wow, you did all four of those things at once.
[00:35:06] Dr. Grant Garcia: And I'm like, yeah, my team can do it. I did it. But some of the guys were like, I would have done in two parts like they did here. Yeah, and I did one part, let it calm down, do the second part, um, and come back and there is that, you know, there's, but then you always have to talk to the patient, like, are you okay with two surgeries?
[00:35:20] Dr. Grant Garcia: Right? Like Nick Chubb trusted his surgeon and he's a, you know, he's the professional player and they did whatever they thought was the best plan for him. Yeah. But the key is, yeah, I mean, there is some thoughts to, should you do these things in part? And when you have an urgent surgery, you can do whatever you want, right?
[00:35:35] Dr. Grant Garcia: Like the person's not going to go find some other surgeon that says, I'm going to do it together, right? It's not, it's not like there's, there's a little different factor when it's something that's, that you can go walk around and find different people for it. Um, but what's important to know is, yeah, I mean, their thought process here is less stiffness.
[00:35:50] Dr. Grant Garcia: So you do the first surgery. Sooner. Fix the ligaments on the outside, not inside the knee, and then do a little check to see what everything else is gone. And then the second surgery come [00:36:00] back and do the inside part when it's not as stiff. And that's exactly what probably was done here. That way you Is that stiffness?
[00:36:05] Will Sanchez: Is that better? You would think that you work inside out, but you're saying it is better to work outside in with something you decide to do two surgeries.
[00:36:14] Dr. Grant Garcia: This is a great question. So assuming you're not grafting anything, like you're not, you don't need to do this in two parts 'cause you're waiting for something to heal.
[00:36:20] Dr. Grant Garcia: Right. Like when you're grafting the bone, it means the tunnels in the ACL were not good. And if you put a new ACL and imagine like, imagine if like I put a hole out of the ground and there's a massive hole right there. Right. And then you want to put like something smaller in like a stake, but it's going to wiggle around.
[00:36:34] Dr. Grant Garcia: Right. Yep. So the only way to fix that is to fill the hole with good grass again, let it grow back and then stick it back in. Does that make sense? Yep. So that would be the, a reason that you do two parts and you'd want to wait. That's not related to stiffness, but when you want someone to not get stiff, you want their knee to get moving.
[00:36:50] Dr. Grant Garcia: Like what we tell people is you want your pre motion to be what your post motion is. So if he's stuck, I get to, he gets injured and I can't bend his knee past 20 degrees. [00:37:00] Then you don't want to go in there and do surgery. Cause they'll get stuck like that. But you can do the outside ligament spine, which are the MCL and the LCL.
[00:37:06] Dr. Grant Garcia: And then you can still be able to give his motion back. Cause you're not messing with the inside of the knee. It's like, it's kind of like a bomb went off in there and you don't want to get in there. So
[00:37:13] Will Sanchez: he started rehab after the first surgery, maybe using a rebless, a shout out to our sponsor there.
[00:37:19] Will Sanchez: Maybe that would be awesome. I don't know. Maybe, maybe grabbing a rebless and getting the, getting it. The nice machine probably. Get some stuff going on, starting to PT, uh, you know, as soon as possible before getting ready for the next surgery. Right. Now, something that we've discussed in the past with some of our other guests, right, starting that physical therapy, uh, prior, you know, obviously he did not know that he was going to sustain this.
[00:37:44] Will Sanchez: So you're not rehabbing prior to the surgery, but as soon as that first surgery is done and, you know, we're just, you know, we're just kind of guessing here as far as what may have happened. Um, I just kind of want to go back and I'm, I'm trying not to get stuck here [00:38:00] with these conversations and move on.
[00:38:03] Will Sanchez: But how do you determine the severity of the knee and knowing that you got to go in that maybe it's impinging on something? Is that, are you sending this to the MRI to get an MRI right away to see if it's on a nerve or, or on something? That can cause permanent damage or what, what's the process? Or can you tell right away?
[00:38:24] Will Sanchez: What's the, what, what are the steps there for you to go? Oh, this is, we, we cannot let this calm down. We have to go in ASAP.
[00:38:31] Dr. Grant Garcia: Great. So let's, we'll, we'll change around the knowledge base there. So that's perfect. So. Impinging on nerves pretty uncommon with these. The one you can do when you dislocate your knees, you can stretch the nerve on the outside of your leg and that causes a foot drop.
[00:38:42] Dr. Grant Garcia: You may have seen people occasionally that have like their foot drops and they've got to wear a brace to keep their foot up. It's called a, uh, and that's the perineal nerve on the outside. So if you dislocate your knee, that can go out. Generally, we're not going in to fix that because once it's stretched, you just want it to come back, right?
[00:38:57] Dr. Grant Garcia: You're not, it's not like usually it's cut. And unfortunately [00:39:00] those are a lot more permanent. Like when that happens, there's not really much we can do to save it. Right. We can do grafting and everything else, but usually you give it like 10 months to a year before it CO goes, but the artery is a different animal, right?
[00:39:11] Dr. Grant Garcia: The artery is the bad one. So that's the one that they got Chicago bears player had basically that's in the knee dislocates. It comes out. And the thing in the back gets torn. It's the artery. So we don't get an MRI on those. You get a CT scan. That's a, that's a bunch of x rays and then you run dye in there called a CT angio and you run dye down the artery and with a CT scan, you can do it really fast.
[00:39:32] Dr. Grant Garcia: Like they can do it in like 20 minutes. And so that's what you would do on top of checking the blood pressures. It's kind of crazy. It's called ABIs to check the blood pressure in the foot and the blood pressure in their arm. And you tell there's a difference, right? Cause if there's not, if there's a tear in the artery, the blood pressure is going to be lower in the foot.
[00:39:49] Will Sanchez: Yeah, it makes sense. So that's
[00:39:50] Dr. Grant Garcia: how they do it. So you check that originally you check pulses and then you go straight to the CT angio and then you're in the operating room that night, uh, if that, if that happens with the artery, so if the dye is leaking, [00:40:00]
[00:40:00] Will Sanchez: right, if the dye is leaking, then you, you know that you've, you've got, we've got trouble buzz.
[00:40:05] Will Sanchez: Yeah.
[00:40:06] Dr. Grant Garcia: Yeah. And you'll just see, I mean, like the, and then do your giants, like how you do right here. It's like, goes like this. And then you just see, you just see the stop. And there's nothing below it. It just out. And that's, that's a medical emergency. And that's when you get a vascular surgeon in there, they bypass it.
[00:40:20] Dr. Grant Garcia: And usually, unfortunately, they're probably not coming back and you can lose your leg, uh, if you don't do that, but hopefully we don't see many of those. And that's not what happened here. So
[00:40:30] Will Sanchez: have you had to experience anything close to that or something like that?
[00:40:36] Dr. Grant Garcia: I have seen, I have seen one of each. Um, I have seen the one where it was not caught and the person lost their leg. [00:40:46] Dr. Grant Garcia: And I have seen one where it was caught and it was fixed. So, uh, you don't want to be on the second, the first one. That's not a good day. Unfortunately, the person was under the influence and didn't wake up for like [00:41:00] 24 hours. And so that was a problem when they dislocated it. So that's nasty. But I don't want to gross the viewers out too much.
[00:41:06] Dr. Grant Garcia: No, it's it's
[00:41:07] Will Sanchez: it's it's what we do here. You know? Yeah. So
[00:41:09] Dr. Grant Garcia: if that happens to you and you're worried about it, get someone to see you quickly. But thankfully, it's just not that common.
[00:41:15] Will Sanchez: It's very, very rare. Wow, that's, uh, that's scary stuff, but it's good to kind of understand what the process is because, you know, when you see an injury like that, you assume the worst, right?
[00:41:25] Will Sanchez: Anyone that saw that injury, any fan that saw that, you, you go, what did, it lost his leg. He's never going to play again. That, that's just, you know, when, when players on the field cringe. That's usually a sign for me going. Oh, that's not good. You know, just that's my sitting at home when I see the players going.
[00:41:45] Will Sanchez: Oh, my God. When Lawrence Taylor is jumping up and waving over the medical staff that because of what has happened to Joe Theismann or what has happened to Alex Smith, when we see players react a certain way, you know, whatever has happened because these guys [00:42:00] have seen probably the it. the nastiest of injuries on the field, but when they react a certain way, you go, okay, that whatever's, whatever's happening right now, that's, that's not good.
[00:42:11] Will Sanchez: Anyway. Well, the Cleveland Browns have had it, uh, had a, had a rough year last year. And we probably could say that, uh, going back to probably the, the Bernie Kosar days, those are probably the last good days, uh, for the Cleveland Browns fans. But their superstar quarterback to Sean Watson. Um, he had a rough season last year before he got hurt in his shoulder.
[00:42:33] Will Sanchez: Um, multiple injuries. Tough guy. In fact, he he displaced this fracture that he had. I'm gonna let you break it down and kept playing throughout that game. With that injury just to kind of display the toughness of these, uh, of these athletes, but talk about this, uh, this displaced, uh, shoulder that he has.
[00:42:54] Will Sanchez: And, you know, the rumors about possible additional procedures he may have [00:43:00] had and the rotator cuff, he, he injured his rotator cuff week three before the broken bone in the shoulders. And they, you know, once again, uh, James Voss and, uh, Uh, Ella Trash was also was, uh, a part of this, uh, these decisions. So if you could talk about this injury.
[00:43:18] Dr. Grant Garcia: So we had another, this is another one of our special episodes last summer, hit all three of them. Yeah. So Dr. Ella Trash is obviously involved in all of these, I think. Um, anyhow, so, uh, he broke off, well, we don't know the full story. We actually got a couple, we didn't end up working out, but we got a couple articles, we got a couple of reporters from, I remember the Browns that reached out to us and wanted to talk about this.
[00:43:41] Dr. Grant Garcia: Cause after our, after our podcast, they were a little bit surprised to hear that we had some other thoughts. Yeah. Yeah. And you know, that was interesting to me that people were interested that much in the topic that the actual people that cover the Browns were asking about it. What's really interesting to me is we talked about this.
[00:43:57] Dr. Grant Garcia: If he broke a piece of his shoulder off, usually within a couple of [00:44:00] weeks of the heels, right? These heels so fast because, and if you have to heal in the wrong spot, they heal fast. And the fact you played through it is very impressive. Again, this is the classic example. I just don't know the whole story because it doesn't make sense to me.
[00:44:12] Dr. Grant Garcia: And I do this surgery. I mean, I, I do some fancy techniques to fix things like this. You want to fix these within three weeks, four weeks of their stock. But I heard a rumor. And again, I don't know if it's true is that maybe it was not fixable and something else was done actually to reconstruct the bone in the front of his shoulder, which would be absolutely insane.
[00:44:30] Dr. Grant Garcia: If that was truly done in NFL player. You know, we've seen the first carlet transplant being done. We've seen the first meniscus transplant being done in high level athletes. So I had heard that there was some possibility there was a reconstruction with something called an ankle bone or a distal tibial allograft.
[00:44:45] Dr. Grant Garcia: And again, I have no confirming data. This is what happened to his shoulder. But it does seems weird to me that when you break off the golf tee and it heals in the wrong spot, you can't rebreak it and bring it back up. It's stuck there. Is
[00:44:58] Will Sanchez: that shoulder? Is that closer [00:45:00] to the clavicle? Like where, where is this for, for those that don't understand exactly what you're discussing?
[00:45:07] Will Sanchez: Can you get, can we get a visual, um, of where this injury may have occurred in his shoulder?
[00:45:15] Dr. Grant Garcia: All right, let me do my best. So the black box is the. Golf tee, and that's the socket, right? Okay, I got you. Sockets like this. I
[00:45:26] Will Sanchez: got you, I got you. So
[00:45:26] Dr. Grant Garcia: imagine, imagine if I took off 25 percent of this and broke this off.
[00:45:32] Will Sanchez: No, that's not good. Now when I do
[00:45:33] Dr. Grant Garcia: this, it slips out, right? It slips, it slips out faster. But when you break a piece of plastic like this. If you maybe, maybe right away, you can glue it, but maybe after a couple of weeks, it heals the wrong spot. You can't get that piece up again. It's done. Like if it's there, you're not going to re break it and shift it up.
[00:45:49] Dr. Grant Garcia: It's just not going to happen. What you have to do is replace it with something else. And so I had heard potentially that he had something replaced there. Um, but that was never told on the, uh, [00:46:00] on the information of that. And if he got something, Is his
[00:46:03] Will Sanchez: rotator cuff had played a part in maybe, you know, something, you know, I think the rotator
[00:46:08] Dr. Grant Garcia: cuff tore when he dislocated his shoulder because that's a, that's a, like now generally only happens in people over 40.
[00:46:15] Dr. Grant Garcia: So if you're over 40, you dislocate your shoulder. You have a very high chance of tearing the rotator cuff. And I've fixed patients like that before. Or a 350 pound
[00:46:22] Will Sanchez: man landing on you, on your shoulder. That is
[00:46:24] Dr. Grant Garcia: a new indicator. That might be a new reason to have a 350 pound man lands on you. Then you're more likely to tear your rotator cuff.
[00:46:31] Dr. Grant Garcia: Okay. Okay. So, so again, more of the story is here. Like the good news is that these patients, if it's stabilized, actually do really well. I mean, it sounds like a nasty injury, But like, if you can stabilize his shoulder, I actually think he'll get back pretty well. Like I'm not worried. I'm not as worried about the Sean Watson as about the other ones we've talked.
[00:46:50] Dr. Grant Garcia: Now we'll see again, it's my prediction. Yeah, poorly. And the Browns are screwed, but you know, I, I think that, I think that whatever you had done [00:47:00] is probably going to keep them stable. And if Ella Trash was doing anything, he'll work his magic. And, uh, I think we're going to see another, another miraculous recovery from Dr.
[00:47:09] Dr. Grant Garcia: Ella Josh's surgery skills.
[00:47:12] Will Sanchez: So they determined the injury will require immediate surgical repair to avoid further structural damage. You made a reference that if you, if it sits around for a few weeks, you could have that permanently damaged. Is there anything that kind of, you know, has the light bulb go off in your head where you're like, this was an immediate surgery, um, that they had to perform once they kind of found out what was going on that they determined the head physician along with, uh, Dr.
[00:47:40] Will Sanchez: Al Trash.
[00:47:42] Dr. Grant Garcia: Well, so, I mean, as soon as you see that glenoid fracture, I mean, I have one of these coming up and then you're just like, oh, that's not a good thing, right? Like, once the bone's broken on the shoulder socket and he feels like his shoulder's shifted out of place, he'll just destroy his shoulder.
[00:47:55] Dr. Grant Garcia: He won't be able to throw. So that's why they wanted to fix it. Right. Cause like in a [00:48:00] normal human, doing normal activities, they can't tolerate this, right? It's slipping out. He's obviously not a normal human. He's super athletic, but he's also putting his shoulder at I mean, having to throw the ball and throw it, the velocities of the accuracy he does.
[00:48:14] Dr. Grant Garcia: And already having a, just a not perfect socket or base for the arm is not a good thing. And so, you know, you could see that. This was a, I think this was actually more of a surgery to help longevity rather than just for the acute situation. Does that make sense? Like it could have, like, if he could, like, if they wanted, they were probably worried it's gonna do more damage and they just put a lot of money in their investment.
[00:48:35] Dr. Grant Garcia: This was to save their investment.
[00:48:39] Will Sanchez: Yeah. I mean, you, you think about the torque, you think about the speed, the accuracy, you think about people landing on it. Um, they said, you know, he is a mobile quarterback. Um, he does run around. It would be interesting to see if that, you know, if they had that conversation with the coaches saying, Hey, you've got to find a way to coach them out of this a little bit.
[00:48:58] Will Sanchez: You know, some of the things that we'd [00:49:00] like to see Daniel maybe do a little bit less. So it all around. I don't have the player's name. I know they looked into their backup quarterbacks, making sure that their backup quarterbacks are kind of legit and ready to go as well. If without knowing everything that's happening, if everything goes smoothly, what's the, what's the timeline here?
[00:49:25] Will Sanchez: You know, for having, this was week 10, so two and a half months, October, November, I guess right before December, I'm guessing I'm not looking at the calendar, just thinking about the timeline or close to December, um, that he suffered this injury. We're now kicking off the NFL season, uh, the first week of September.
[00:49:47] Will Sanchez: You know, is that timeline concerning for someone that works on shoulders and, and things like that, uh, and for your thought process, or you're like, well, once that's done, they done X, Y, Z, they've done the rehab. [00:50:00] It's just a matter of going out there, getting contact and seeing how it holds.
[00:50:05] Dr. Grant Garcia: So what's crazy is with the shoulder stuff.
[00:50:07] Dr. Grant Garcia: Minus the baseball players and maybe quarterback might be a little different. Generally, we're talking about five months. I mean, I've had linebackers with these injuries come back in four and a half months, so it's crazy if done well, uh, as long as the bone heals, if they had to do a bone healing procedure or whatever, you know, you're talking about five and a half months and you're letting them rip.
[00:50:25] Dr. Grant Garcia: So it's different than a knee. So I think he'll be back. Like I said, I mean, I wouldn't wish any of these injuries on anybody, but I think if he had his, if, if, again, I don't know what happened, this glenoid fracture thing is still super crazy to me that it was injured months, weeks before, and they found him and they had to think through an urgent surgery.
[00:50:44] Dr. Grant Garcia: So I have no idea exactly what they found, but I can suspect what they did. But, you know, based off whatever they did, I'm assuming that they feel pretty good about it and I'm assuming that he, you know, hopefully we'll get back.
[00:50:56] Will Sanchez: AFC North has been, uh, Been getting, taking their [00:51:00] lumps, obviously one of the MVP kind of, uh, you know, one of these, one of these guys probably going to win the MVPs between, you know, Joe Burrow and, uh, Lamar and Patrick Mahomes.
[00:51:15] Will Sanchez: But, you know, once again, uh, Burrow ending his season, torn ligament, wrist. I mean, he had a real rough season where he had an earlier injury, uh, to start off the year with a cap injury. And then, you know, he had this torn ligament, any concern with the wrist area, uh, for Joe Burrow going into this season, besides, you know, he hasn't played much football, you know, the last year, um, as far as taking hits, spinning the ball, gripping the ball.
[00:51:43] Will Sanchez: Right. I mean, I think gripping is one of the concerns. And I think if we had a Dr. Whale here, we'd be talking about that. What are your thoughts on that?
[00:51:52] Dr. Grant Garcia: Yeah, I mean, I'm worried about that. With ligament stuff like this where you're not doing a reconstruction, you're just basically repairing it. I think if he doesn't get [00:52:00] anything stuck, I think he'll actually be pretty good.
[00:52:02] Dr. Grant Garcia: I think it's more the But that's just me, again, I'm not a hand surgeon, so I do less of these. But, I tend to see, I tend to be less stressed about something like this. You know, I'm more worried about, I'm more worried about the knee stuff and the damage and the revision situations. You know, unfortunately the knees take the longest.
[00:52:19] Dr. Grant Garcia: This is a good one though. So we'll move on. I want, this is a good one.
[00:52:21] Will Sanchez: Yeah. Yeah. Anthony Richardson
[00:52:23] Dr. Grant Garcia: thing.
[00:52:23] Will Sanchez: Yeah. Anthony Richardson, you know, I wanted to get to that because we've been yip yapping away. And, uh, as time is ticking over here, let's get to Anthony Richardson's with his AC joint sprain. And once again, we hear sprain or I hear spray and I go, well, that doesn't sound like it's too concerning.
[00:52:39] Will Sanchez: But, uh, grade three, uh, what, what's your biggest concern with this? Also, once again, it's the throwing arm.
[00:52:46] Dr. Grant Garcia: Yes. So this is controversial topic. Good. You picked a good job. You always do a good job with this. Well, so AC joint injury, acromion clavicular. So acromion is this, it's a shoulder separation, right?
[00:52:56] Dr. Grant Garcia: You've heard the word shoulder separation. Yep. It's a really common in [00:53:00] bikers football, direct blow on the shoulder. The thing about this is for every grade, there's six grades, but we almost never see the fours. Those are like with some weird, you know, the cloud was stuck underneath. It's just almost, I've never, I think I've seen one of my whole life.
[00:53:15] Dr. Grant Garcia: Um, but the threes and the fives, the ones you worry about, because those are the ones that might need surgery. One, two is like a little bit. Three is where it comes up a little bit more than five is where it's like way up. If he had had a five he would have automatically gotten surgery. Uh, but because he's a three The three is where it's on the fence And so the data shows that if you have a three That half those patients don't need any surgery.
[00:53:39] Dr. Grant Garcia: They'll get back on their own And I have one of the Mercer on football players. I just did this with and I was able to treat him without surgery, but some people come back and I've had this at like two months, three months, four months, and they still feel bad. They can't throw. They have like popping and it's unstable.
[00:53:53] Dr. Grant Garcia: And what they've seen now is it's actually maybe more like a three a and a three B. The A's can get back and the B's don't because there's actually [00:54:00] a component that's, we think about AC joint injuries, the chromium goes up, right? That's how we measure it. But we don't think about it. Remember, Our body doesn't work in one plane.
[00:54:09] Dr. Grant Garcia: It works in two planes. So the concern is that some of these eight, these grade threes actually have this stability and this, and when you have both, then you might not get back. My assumption is he just had this one, right? Or they would have probably done surgery on him, but we've done studies on this.
[00:54:25] Dr. Grant Garcia: Looking at baseball players is a really common baseball injury. And you ask about the team doctors and it was crazy because only half of them said they would ever do surgery on this. The other half said never would do surgery on a grade three. I will do surgery on somebody, but again, the studies show that you want to try no surgery first.
[00:54:41] Dr. Grant Garcia: So the surgery timeline, the recovery timeline for this is about one to two weeks for every grade. It's like an MCL without surgery without surgery. So six weeks.
[00:54:50] Will Sanchez: So, so you, you should, you should have the needed information for you to think about your next step within the two week period.
[00:54:59] Dr. Grant Garcia: Usually I [00:55:00] tell them six to eight weeks, you know, now with him, he's going to give you monitored more closely.
[00:55:04] Dr. Grant Garcia: But like I tell, like I told the football player and the office is going back and play, I said, you know, go back and play for the season if you can, and if it starts feeling unstable, you can't do it. We got to pull you out. We're going to do surgery on you. And if you can tolerate it and it's bad at the end of the season, then we do it at the end.
[00:55:20] Dr. Grant Garcia: So what he may do is he may, but again, you can see these bikers, they come in cause we have all this biking around, we're surrounding around the area, you know, the bikers have both of them. They look like little horns, right? They got AC joint injuries on both sides and they've been no surgery on it. So it's really depends on the patient and how they feel.
[00:55:35] Dr. Grant Garcia: But it's that, it's that shucking anterior posterior. So front backwards. And that's why we're starting to see these, like that, the, that the grading system we have may be too old school, right? Like it's just, it doesn't give us cause we reason we make grades and I'm going, I know we're almost over. We make grading systems so we can, we can determine.
[00:55:53] Dr. Grant Garcia: We can say, okay, that grade twos need this something, this grade three needs this something. Does that make sense? That's what we grade these things. [00:56:00] And we, so we can describe them more easily. Right. So like, we know grade one takes this long grade two, and we can just like, by having that documentation, it makes it faster.
[00:56:07] Dr. Grant Garcia: It's like a, it's like a, it's a, um, conversion chart for surgeons. You think it's time to
[00:56:12] Will Sanchez: reassess these grades for these type of injuries? Possibly without starting trouble.
[00:56:18] Dr. Grant Garcia: I think, well, no, we're talking about it. Well, you're going to start some trouble. I love it. No, no, no. You're absolutely right. And there are people looking at it.
[00:56:24] Dr. Grant Garcia: There was a paper about this recently that wanted to regrade some of these because we don't have a good system and this, this grade three, like the number of ones that create these come my office and I go, listen, you might need surgery, you might not. The only ones I benefit from are the ones that come in at like two or three months.
[00:56:40] Dr. Grant Garcia: They have a grade three and they're not happy because those are the ones I know need surgery, right? Like they've already declared themselves, but these acute ones, a lot of times you don't need surgery, but it's tough because they get different opinions and some people say you need it. So this is one of those ones.
[00:56:52] Dr. Grant Garcia: It's a gray box. This is a great topic.
[00:56:55] Will Sanchez: Any concerns for him this season as we get ready to wrap up? [00:57:00] I could talk about this for another two hours. Anyway, go ahead.
[00:57:04] Dr. Grant Garcia: I know you could. I know you could. You open up Pandora's box every time he asks you about an injury. Um, concerns for him are, I hope he doesn't have the bee.
[00:57:13] Dr. Grant Garcia: I hope he got the A. I'm assuming he does. He wouldn't have got surgery already. So, so we might, they don't damage the inside. All right. So, so once he
[00:57:21] Will Sanchez: starts playing football, gets hit, we're going to find out if, if something needs to be done. So there is a question Mark about his 2024 season. Um, you know, until we see what happens, right.
[00:57:36] Will Sanchez: Is that comfortable enough to say there?
[00:57:38] Dr. Grant Garcia: Yeah, I have a good feeling about it. I feel like you, I feel like they would have pulled the trigger already. I have a good feeling about it. So,
[00:57:45] Will Sanchez: all right. We had a bunch of other stuff to talk about, but we're not, we're going to end on some trivia to kick off the season.
[00:57:51] Will Sanchez: All right. Three players have won the NFL comeback player of the year award and a super bowl. Can [00:58:00] you name one of those three players? JJ Watt.
[00:58:04] Will Sanchez: Nope. One more.
[00:58:06] Will Sanchez: Tom Brady. Tom Brady is one of three players. He won the comeback player of the year in 2009 and then won the Super Bowl that same year. Peyton Manning won it in 2012 and then, uh, won the Super Bowl. And Rob Gronkowski also was a part of that. So hip, hip, hooray. I'm excited about the G. I got my Tiki Barber jersey on.
[00:58:32] Will Sanchez: Can't see it there. Tiki bar right now. You got your giants. I'm really excited. I got to put my
[00:58:36] Dr. Grant Garcia: brand.
[00:58:38] Will Sanchez: Yeah. And hey, we're going to update our, our listeners throughout the year. We think it's important, these injuries and top players. So being the look lock lookout, we're going to do some short, quick hitters.
[00:58:51] Will Sanchez: I hope we'll keep it short, but probably not. And, uh, keep all of our fans, uh, Ready to go for this season, man. I [00:59:00] appreciate you. Dr. Garcia is always good to chat with you and we look forward to our upcoming shows. Check us out at sports doc talk. com where we have plenty of content and transcripts. Say goodbye.
[00:59:13] Will Sanchez: Dr. Garcia.
[00:59:15] Will Sanchez: Bye bye.
[00:59:17] Dr. Grant Garcia: Thank you guys. Audio Transcript
The Key Behind Arthrex Innovation

Will Sanchez:Welcome to Sports Doc Talk. Dr. Garcia, once again, it's great to see you. I think I've heard this music way too much because I've got like a little bop going on. Why am I bopping to this music? This is a terrible sign. Maybe we're doing too many shows because I'm thinking about it in my sleep. Before we continue, we have a great show, great guests, but before we get to them, Dr.
[00:00:40] Will Sanchez: Garcia, how are you doing today?
[00:00:43] Dr. Grant Garcia: I'm good. I'm really good. You know, I'm excited for the show. Something different. Put a little spin on it. Each time you never know who's going to be on here.
[00:00:49] Will Sanchez: That's right. And as always, we always like to give a shout out. Where's our little shout out here? Let's give a shout out to The Recovery Shop.
[00:00:59] Will Sanchez: This [00:01:00] episode is sponsored by The Recovery Shop. Orthopedic surgeons like Dr. Garcia and patients alike love the recovery shop for its curated selection of physician approved post operative recovery products from braces to nutrition. We've had the nice machine, you name it, you, you, we have it all for you on
[00:01:20] Dr. Grant Garcia: there.
[00:01:21] Dr. Grant Garcia: The Rebless is on there too. The
[00:01:23] Will Sanchez: Rebless, so many cool things. Um, and obviously we know why Dr. Garcia loves it because it's easy. He can. Pushes patients that way. And, uh, it's just great for everyone. So, uh, check us out at the recovery shop and Dr. Garcia. Um, you excited about today's guests?
[00:01:43] Dr. Grant Garcia: I am. I'm excited.
[00:01:44] Dr. Grant Garcia: One more thing on the recovery shop. Again, we've brought it up many times. You know, this is, this is awesome for the patients, right? Like we want, you want something new, you know, if we hear something new today or on rehab, I can call them and say, Hey, listen, put that on the website. So my patients can find it easily, right?
[00:01:59] Dr. Grant Garcia: You're [00:02:00] not going to Amazon. You're not going to other proprietary websites where you don't know the quality. These are all been pre vetted by myself and working with these top guys in the recovery shop. And it's great for surgeons kind of have your own little hub, right? It adds a little personalization to it.
[00:02:14] Dr. Grant Garcia: The patients really like it. And honestly, the products which Will's tried, I've tried, they really worked. Will didn't want to give
[00:02:21] Will Sanchez: it back. And we had a grant on from the nice recovery. And I told him, I said, The best part about having the nice recovery and it is the way it worked wonders. And especially for my wife that I was laid up and she didn't have to run around getting me ice packs all the time.
[00:02:41] Will Sanchez: And I was able to use machine. But when I actually had to send it back, I was very disappointed. Let's not go down this rabbit hole. We know I'm going to stop. We got to move on. We got such. No, we always do this. Listen, we've got a great show
[00:02:55] Dr. Grant Garcia: is gonna be short. As you know, our show is always short.
[00:02:57] Will Sanchez: Oh, shut up, man.
[00:02:58] Will Sanchez: We're not doing that. Come on. You know [00:03:00] how that works. Come on. Let's bring in, where is he? Where's where's Austin? Austin. Austin Robinson working with Arthrex in Seattle and before Austin, I apologize because I'm jumping the gun here and I'm yip yapping away, I just want to let. The viewers and listeners know, right?
[00:03:18] Will Sanchez: We have nothing to do with Arthrex, any kind of financial standpoint or anything like that. Okay. We're talking about Arthrex and we're bringing you on because the product is so good and it's not only just beneficial for. are surgeons, but I could care less about that because I'm not a surgeon. I'm a patient.
[00:03:39] Will Sanchez: And when you've got cool tools to play with, it makes my recovery a whole lot better than everyone else out there. That's a patient. And for someone that actually has some gear in my leg, I'm very thankful. So. Austin, welcome to the show. Oh, Garcia, interrupt me because I'm talking too much. No, you're doing great.
[00:03:59] Auston Robinson: [00:04:00] Thank you for having me. It's a pleasure to be here.
[00:04:02] Dr. Grant Garcia: So I can choose Austin again. I'll bring that up again. This is, there's no monetization from Arthrex on this. I'm a consultant for them. I work for them. I help with product development and other things and videos, but nothing to do with this. The reason I bring someone like Austin on is first off, Austin, how long have you known each other?
[00:04:16] Dr. Grant Garcia: I think five, six years.
[00:04:18] Auston Robinson: Yeah.
[00:04:18] Dr. Grant Garcia: And we talk about internal brace, Will, don't get started yet. Wait, wait. And we talk about a sale repair. We talk about all this innovative stuff. Can you hear me talk about, you know, I visited here, we went here, we did this and that all sounds great, but that doesn't, it doesn't happen like that.
[00:04:35] Dr. Grant Garcia: You don't just go to those places. You don't just get those new products. There has to be someone behind the scenes. And when you're doing the type of complex surgeries that I'm doing in my surgery center, or you're looking to constantly be on what they have, and we'll go to Arthrex as alpha beta launches.
[00:04:49] Dr. Grant Garcia: So we get, will the products before other surgeons get them? How does that happen? Well, it happens through someone like Austin, right? And you, you you pair up to get those, they get those things [00:05:00] earlier, so you can try them, you can use them in safe manner. And there's so many different things that Austin's team offers, As a subunit of Arthrex and then the major corporate will get into too.
[00:05:12] Dr. Grant Garcia: Like, what is the benefits of this? Um, and what can surgeons learn from it? And this is, you know, a lot of different industry does this, but you know, they have a specific way of doing it for sports. And I remember, I won't get too much more Austin. Sorry. I don't want to take up time, but I remember when I was in residency, I know, I know, but I was wondering like, how did they get in?
[00:05:32] Dr. Grant Garcia: How are they able to get involved in so many things? And it's the. It's not just the products. It's not just the glitz and the screen in the background, which we'll get into in a minute. It's the, it's the whole thing. It's the videos. It's a teaching. It's a focus on the entire, the entire unit and making sure that surgeons are integral part in helping out, uh, with this sort of company.
[00:05:53] Dr. Grant Garcia: And it's, it's pretty awesome. So anyhow, without further ado, Austin is the owner and agency [00:06:00] owner of the Seattle Pacific Northwest. And he has been, he has done way too many jobs in the past. And he is now, he is now, he's a good friend of mine. We talk way too much. My wife's jealous of Austin. I talked to him more, I think, unfortunately, as
[00:06:11] Auston Robinson: well.
[00:06:13] Dr. Grant Garcia: So anyhow, well, thank you for coming on and we'll, do you want to pop his little bio up there as little.
[00:06:18] Will Sanchez: Yeah, I'll throw it up there. And, uh, in Austin, just real quick, man, how, how did you get involved with, uh, Arthur X?
[00:06:26] Auston Robinson: That's a great question. Uh, and thank you for having me. It's a distinct, distinct privilege to be on the program.
[00:06:31] Auston Robinson: This is a prestigious show. to catch every episode. It's always fun to hear. So it's a unique experience to be featured with you all and be part of the conversation. Obviously, Dr. Garcia, thank you so much for your approach to patient care, because it really aligns with Reinhold's vision at Arthrex of helping surgeons treat their patients better and helping people get better.
[00:06:50] Auston Robinson: Um, and you, you do that at the cutting edge. You're the tip of the spear in so many different modalities, but I, I found my way to Arthrex. I was working for a competitor as, as often as the story [00:07:00] Uh, in the medical device world. And, uh, uh, my previous boss, Bobby Adams, who was very influential in my life and career, uh, gave me an opportunity to, to embrace Arthrex is, is a lesser known fact about Arthrex, but something that is, uh, some, you know, feature that we take great pride in is Arthrex is one of the largest medical education companies in the world, if not the largest.
[00:07:21] Auston Robinson: And, um, he hired me into a role that was a burgeoning new department called. our local medical education department and, uh, just kind of progressively made my way through the, uh, the different levels of the organization and have been privileged and honored to be given the opportunity to, uh, take the helm with Arthuric Seattle.
[00:07:40] Auston Robinson: Uh, we have a tremendous team as I just play a very small part, but it's a really, uh, fun opportunity to be a part of it.
[00:07:46] Dr. Grant Garcia: I'm laughing. He doesn't play a small part. He's the man. This is the man. He's takes, he's a strong leader. It's amazing. All the different people that talk about how good a leader you are, Austin, but I'm not going to, I'm not making, so you can at least walk out of the room, [00:08:00] not have your head explode.
[00:08:01] Dr. Grant Garcia: So, yeah, I'm
[00:08:02] Auston Robinson: going to get my wife and see if she can listen in just to, you know,
[00:08:07] Dr. Grant Garcia: so the, so I guess this is, this is a good way to start when people hear, I think. When some patients hear industry, they think that's awesome. Like they see arthritis, you know, patients come in all the time asking me for, I want the tight rope.
[00:08:20] Dr. Grant Garcia: I want the internal brace. I want, you know, a swivel lock. I want the thing Aaron Rodgers had. I want the thing that, you know, Neil Alatrosh did to that other guy, that other NFL player, right. They ask for those things. So they have a, they have a reasonable perspective. I think the idea of industry and surgeon type of thing is not really a negatively influenced at this standpoint, but from a surgeon standpoint is a different.
[00:08:41] Dr. Grant Garcia: Uh, thought process and especially early on, you know, some, I think some places think of like, Oh, if you talk to industry or industry talks to you, you know, this is like, you shouldn't get involved. You shouldn't help out. And even early on for me when I was in practice. It was surprising to me working with you guys and I worked with, you know, [00:09:00] Arthrex a lot because they do, I do sports and that's like one of your biggest things, right?
[00:09:03] Dr. Grant Garcia: Like you're, you guys are, it's mega. And what I realized pretty quickly was like, it's not just about the implants. It's about what do you want to get better at? What do I want to improve on? How do I want to help my patients get better? And it was, it's weird because it, for me, it felt more like. family situation and understanding, like, what is the whole that we want to improve on?
[00:09:24] Dr. Grant Garcia: Like, if I, I go to Austin all the time, I'm like, what's new? What can I, what can you show me that's new? And I don't have to, you know, stive the internet, right? He's going to help me give me the catalog of things that I can look at and also being fair with pricing, which is, which is awesome. And so I think, what, how do you navigate that with surgeons that are skeptical of the idea of, Industry, right?
[00:09:44] Dr. Grant Garcia: It's a, it's alarming, especially new surgeons. You know, you have older surgeons that are like, you know, I don't, I'm not involved. I don't really care. I'll just do whatever. Um, and we all know that situation. We've talked about that before, but these newer guys, social media, they're hitting that. They want to prove themselves.
[00:09:57] Dr. Grant Garcia: They're gunning. How do you deal with that situation [00:10:00] where they're nervous about industry involvement?
[00:10:03] Auston Robinson: Yeah, that's a great question. Uh, and it's a great opportunity to just live up to our mission statement of helping you all treat your patients better. We, we, uh, you know, obviously we're a business. We're, we're trying to do well in, in that regard, but ultimately I think what, what drew me to Arthrex and what makes it so unique is that the patient is still the center focus.
[00:10:23] Auston Robinson: Reinhold has done an incredible job. ever since he started in 81 to keep the company private. So there's no shareholders that he has to appeal to. There's no quarterly statements that have to be emphasized, uh, or profits that have to be justified or decisions that need to be justified. And there's a lot of decisions that he makes.
[00:10:42] Auston Robinson: that don't make good financial sense. Uh, I wouldn't say a lot. He's been very successful, but there are there are certain instances where he will invest a tremendous amount of money into building a device or a tool to make the job of the surgeon easier so that you're not having to worry about that. You can keep your [00:11:00] mind focused on that patient's outcome, and we try to live up to that through our commitment to medical education locally.
[00:11:07] Auston Robinson: Every agency in the country is as if not one, several, uh, local cadaver labs that allow their surgeons to practice and rehearse and bring their team in. And that's a, you know, no cost to them, uh, accessory to their practice that they can use to continue to leverage their training into advancing their skills.
[00:11:27] Auston Robinson: So, uh,
[00:11:29] Dr. Grant Garcia: this is important for, I'm sorry, I'll send me interrupt you, but I want to hear this. I want the young surgeons. I want will to understand this because we'll always I went to the lab and I practiced it. And then I tried it and then I was able to take it to the patient and do a good job. And we had a Savito on, he was talking about that as well.
[00:11:44] Dr. Grant Garcia: Oh yeah. And a lot of the companies, and again, I'm not between any of the companies. I've worked with a lot of them. They're all, all of them have their different benefits of working with them. If I want to try something, I can call Austin. He's like, Hey, I'll get you a lab. We'll do it in the cadaver. We'll practice it.
[00:11:58] Dr. Grant Garcia: And I mean, awesome. We've come up with new [00:12:00] techniques. I mean, I would tell you, I would tell the patients that how many times I've been in the lab. It's way too many, right? I know that I grabbed my coffee. I know exactly where I'm supposed to go, right? But the thing is, that's how you get better, right? Like you don't want, we don't want to practice on a patient, right?
[00:12:13] Dr. Grant Garcia: Like we have like, We have nuances we can change in the operating room, but if it's something big, I mean, I remember starting practice. Well, like I called, uh, my rep who was, who's working with Austin at the time. And I was like, I want to try these two new surgeries. I'm about to bring to Seattle. Like, can we go and start before I started practice?
[00:12:29] Dr. Grant Garcia: That was. I'm now almost six years. It's crazy and basically was practicing in the lab to get ready for my patients and it makes me better Faster and more efficient and you know, it's crazy, too And again, you know, I don't know what the arthritis to think about this But like we've practiced that plus adding techniques right like new things not just the arthrix thing, right?
[00:12:48] Dr. Grant Garcia: So austin's all about What can you do to get better? Right? Like if I'm going to do five different things during a surgery and four are going to be arthrics and one is going to be non arthrics, that's okay with these guys because they want, they care about what the patient outcomes. And I think [00:13:00] that's, what's really hard for some of this newer surgeons to see is it's that like, you don't always have to be doing everything from one place.
[00:13:07] Dr. Grant Garcia: And what's the focus for them is like that you do good surgery, right? Because a good surgery you're like i'm gonna do that exact same technique and use the exact same instrumentation the same next time I don't know if you have any questions, but I will but it's just it's just
[00:13:18] Auston Robinson: yeah
[00:13:19] Dr. Grant Garcia: people don't understand It's so hard to get a cadaver lab at many of these companies.
[00:13:22] Dr. Grant Garcia: I've tried i've been like I want to do this in the lab And unfortunately, I'm spoiled because I have the access to Austin because we're friends and he's able to help me out. Um, and the Arthritics guys, I can get a lab whenever I want, you know, they're always available. It's such an incredible resource and it's so rare.
[00:13:36] Will Sanchez: Yeah, I wanted to ask you, like, how do you, how do you elaborate on the patient's Transcribed outcomes and satisfactions. Um, how do you measure that, you know, for making informed decisions for the product? So, you know, based on a reaction from the, from the patient, what, how do you give that feedback, um, that, you know, whatever that decision making is?[00:14:00]
[00:14:00] Auston Robinson: Uh, from my perspective, we rely heavily on people like dr Garcia. You know, um, he treats the patients and, you know, it's been very compelling. As you mentioned, ACL repair earlier, there's a variety of techniques out there. I am biased, but I feel like we have the best technique and the best product for that, you know, procedure.
[00:14:20] Auston Robinson: But we rely heavily on our on our surgeons to say, Hey, this needs to be improved. You know, this was a struggle. This was finicky. This was Uh, and Reinhold, he, that's how he started the company and that's how he's maintained the flow of information at the company is surgeons are in the, in the pilot seat where, you know, we're in the background trying to make sure that we can give the surgeons the tools that they can use to most optimally treat their patients.
[00:14:45] Auston Robinson: So when they say, you know, You know, this, it's, it's rare. I would say, Dr Garcia, you might, might agree with me. It's rare for Arthrex to produce something that is flawed. They do such a great job thinking it through because they have so many surgeons offering guidance and feedback. But in the [00:15:00] instance that there is a refinement that could be put in place, offered or interjected.
[00:15:04] Auston Robinson: Uh, we, the surgeons bring it and, and there's always, it's amazing. You go down to our headquarters in Naples, there's always people in the labs trying to refine the practice of surgical orthopedic surgery and spine surgery and laparoscopic surgery. Uh, it's incredible.
[00:15:20] Dr. Grant Garcia: Well, I don't want to have to there. I think you should, we shouldn't change the word from flawed, right?
[00:15:24] Dr. Grant Garcia: You have, when we had like, well, we've talked about this, there are these special anchors and they're so minuscule and they're so amazing for shoulder or labrum repairs. Right. Um, And then not less fiber attacks, right? And they've been changed four times in the last three years. And it's not because they're bad.
[00:15:38] Dr. Grant Garcia: It's not because they were flawed. It's like, Oh, some other person figured out how to make it even better. So I think what Austin is also trying to say is that there is a lot of change. I mean, you could have a product and you get like that swivel lock. You show there's been renditions. There's different changes of it.
[00:15:51] Dr. Grant Garcia: There's all these different things. And the reason being is not because the last product was flawed. They need to fix this, right? Occasionally there are products like that. [00:16:00] What's really interesting too, is that they have a lot of background input. There's alpha and beta, like I mentioned. And so before the product hits mainstream, they'll have surgeons and Austin's really big on this, have surgeons evaluate the products and they listen to it.
[00:16:14] Dr. Grant Garcia: I mean, every time I do a beta testing, I'm sending notes and the reps, you know, Rachel, we can talk about her at some point. She's amazing. Um, but you know, she's writing notes about what's going on the technique. Garcia didn't like this. He liked this part. This was good. And half the time you want to be, and obviously I'm, I have a lot of discussion where I say, Oh, maybe I did this wrong.
[00:16:32] Dr. Grant Garcia: And a lot of times it is the surgeon, the technique, we did it by holding the hands or something, but they're really good about making sure that they, they teach us the right way to do it. And if there's a, if there's something that we're concerned about, it's not, you know, most surgeons unfortunately will, and you may, may or may not know this.
[00:16:47] Dr. Grant Garcia: They like to blame others, which is not good. Um, for something that's not going right, and we all know that it's that we all have error in us, um, and it's never a bad thing if you have a little, you know, if you're putting the anchor and it didn't go exactly what you [00:17:00] wanted, it's not a catastrophic issue, but what we have, what we understand now is that, unfortunately, every surgeon's, surgeon's learning curve is different, and what arthritis really does is they don't want, they want to eliminate the learning curve, and that's really, really hard to do.
[00:17:16] Dr. Grant Garcia: And I found that out by working with Arthrex over the last five years that I'm like, well, I do this a lot, but like, maybe the surgeon next door doesn't do a lot of those. And so I'm like, I don't understand why you can't figure that. Or I do something. I'm like, I don't understand. I don't understand this thing.
[00:17:29] Dr. Grant Garcia: And they're like, you know, you tell them an idea and they're like, that's way too complicated. And you're like that. We're just talking about like an anchor, right? It's a little swivel. You pull it out, you pop the button, you know, this is straightforward. They're like, no, that might like, we're talking about a design right now.
[00:17:42] Dr. Grant Garcia: And I was told that they can't do two loops because sometimes they cut the wrong loop, right? Like you're like, that doesn't make any sense to me, but they're so keen on making sure that the surgeons. That the surgeons happy with the product and the product works flawlessly every single time. And that's really, really hard to [00:18:00] find the industry.
[00:18:01] Dr. Grant Garcia: Well, like, it's just amazing that they're like, I want someone that does one of these and does 10, 000 of these to be just as good every time to put it in. And that's extremely hard to do. That's way harder than you'd ever imagined.
[00:18:12] Auston Robinson: Uh, if I can interject, I know I'm just a passenger on this journey together, but that is, it seems like a perfect opportunity.
[00:18:19] Auston Robinson: If I can make a shameless plug for our people. Because I think a big part of that, too, is the technology is there. You're obviously a gifted surgeon, uh, and and surgeons are very well trained, but to have the support of, uh, you know, a competent rep in the background that knows the technology is prepared to do their job well, which, you know, You mentioned Rachel, Rachel Robinson.
[00:18:40] Auston Robinson: She's our rep that covers your, your, uh, surgery center. And she's super stellar. She's a rockstar and she wants to make sure that she doesn't let the patient on the table down or you down. And internally, I think that's another differentiator arthritis does really well is we have our own medical education director, a gentleman by the name of Bram Shamas, who's a brilliant [00:19:00] guy and devotes a lot of his time and energy to making sure that when we have a rep going to an OR, They know what they're doing and, you know, we all have room to improve.
[00:19:08] Auston Robinson: We're all continuing to grow on our journey. But, uh, you know, we, we invest heavily in those resources to make sure that we're not sending somebody into that procedure that can't assist, especially when, uh, something goes wrong. Right. And, and that's a, that's an
[00:19:24] Dr. Grant Garcia: incredible point. I don't think, Will, we do enough discussion of everybody else behind the scenes, right?
[00:19:30] Dr. Grant Garcia: Because it's impossible. Like, you've been productions. Like, you can't, you know, every camera person, every lighting person, you can't talk about it. I'm not trying to dumb down the reps or anybody else into like a, you know, a light or a camera or, um, but what's incredible about the reps on Arthrex, in my opinion, Is that there that you even get some people that are new and they're really, really intent on learning, right?
[00:19:51] Dr. Grant Garcia: I mean, we'll, I will tell you, and Austin may think we have some of the hardest surgeries we do in the state and our operating room, very complex, high volume, [00:20:00] really intense. Like I'm, I remember the best and we'll make me think this is funny, but inside information, I was always told that my OR is the most giggles.
[00:20:09] Dr. Grant Garcia: And the most stressful at the same time,
[00:20:12] Auston Robinson: because we're
[00:20:12] Dr. Grant Garcia: doing such complex procedures, but we're also having a good time. And so that to me is the key, but the fact that a rep can come into that situation, and they're prepared for it, and they have notes, I mean, Rachel, I, I don't want to make it about Rachel, because I know that she's going to blush when she hears this, but You know, I asked her about something I did and she's like, Oh, you did this like six months ago.
[00:20:30] Dr. Grant Garcia: You did this way. And I was like, how did you remember that? And right. Well, she's writing notes. So it's not like I am, I may steer the ship, but I have lots of people that help me out. Like my outcome in the end for the patient is because of Rachel, because of my scrub techs, because of my PAs, because of.
[00:20:47] Dr. Grant Garcia: My, my scheduler, like this is a combination. This is a team effort to get there. And if you don't, they are the final finish line, right? Like if you, when I'm doing something, if your rep's [00:21:00] not good and all of a sudden I do something that doesn't work, how do I decide? I've never seen it. Right. Like Rachel and I have been together most of the time, but she works with other surgeons or other reps do too.
[00:21:10] Dr. Grant Garcia: And if they, they actually have more experience than the surgeon does combined well, because they're going every day to the operating room. And so they know their product and they go, this doesn't work, do this. And early on, that was huge for me. I mean, I had Kyle, he's awesome. And he was like, he told me that something went wrong and he's like, this is how you fix it.
[00:21:25] Dr. Grant Garcia: I'm like, I had never even heard of that. And I'd been at HSS where these guys are using Arthrex products left and right, left and right. And you learn something new. And the cool part is they, if you keep an environment where you're like, Hey, just teach me because I want to learn too. And that's really, I think.
[00:21:40] Dr. Grant Garcia: The one thing you guys do a really good job of, you build a relationship. So the surgeons are willing to be taught, right? Like there's other companies and I will not name names where I don't want to be taught by anybody. Because to me, I don't feel like there's a lot of, there's the same caliber of what I'm getting, which is why to me, the relationship is so important, um, because of the consistency [00:22:00] and because of the personalities.
[00:22:02] Dr. Grant Garcia: I mean, Will and ROR, they're like our, The reps there for Arthur to come in. They're like best friends. Everyone's like, Hey, Rachel, thanks. Good morning. Let's get going. You ready for today? And she's like, Oh yeah. And they put so much effort in well, it's hustle all day long hustle. And that is a, that is a hard thing to do.
[00:22:16] Dr. Grant Garcia: And that's something that's built by the brand. Um, and You know, I think Austin, one thing I think that people would say is, and we'll might be able to test to this, but you know, one thing that one knock, I think people talk about arthritis, that the products are expensive, right? There, they maybe are more expensive than some of the other brands for the patients listening and for the surgeons is that unfortunately, when you have, you usually pay for what you get, right?
[00:22:41] Dr. Grant Garcia: So if you don't have the higher quality stuff or the higher quality thing, you don't get the rep in the room that knows what's going on. You don't get the medical videos to teach you how to do it. And we'll, I don't know what your thoughts are, but I think that if I offered you, and again, there's nothing wrong with a Honda or Toyota or a BMW or a, you know, [00:23:00] a Mercedes, I think, you know, which one you might choose.
[00:23:02] Dr. Grant Garcia: It's just, it's just the difference.
[00:23:05] Will Sanchez: It's funny. You're talking about this and, um, it reminded me, and this is, I'm really going off the beaten path here, uh, episode of the King of Queens, right. And, um, he wants to surprise his wife with a LASIK surgery. So he's like, all right, we, you know, for your birthday, we're going to get you the LASIK surgery, you're going to no more glasses.
[00:23:27] Will Sanchez: So, you know, he goes to take the surgery and she wakes up the next day. It's blurry. The day after that, it's blurry. Finally, she's at her birthday party. She can't see anything. And then, you know, one of the friends comes by and it's like, Hey, I heard you had the surgery is like, yeah, blah, blah, blah. Did, did you go to my guy?
[00:23:46] Will Sanchez: She was like, what are you talking about? Yeah, this guy is like, no, I went to this guy and she found out that her husband got cheap and kind of got like a Groupon 50 percent off of one eye or the other and wound up having to go back to the original guy to get it [00:24:00] fixed. So in a weird way, you know, like I said, I'm going off the beaten path.
[00:24:05] Will Sanchez: You're not off. You pay for what you get. In this case, he got cheap on it. Didn't get what the necessary tools. And the result was a very angry wife that did not celebrate a birthday. So
[00:24:19] Dr. Grant Garcia: it's one way to think about
[00:24:20] Will Sanchez: it.
[00:24:20] Dr. Grant Garcia: Thankfully, I mean, again, there are a lot of other product companies that have make good products, but I think what we're trying to get at here is that you have this consistent quality, which to me is really important.
[00:24:31] Dr. Grant Garcia: And I'm, my patients are looking for it. My patients are like, did you put metal in me? That's the one thing that's just put metal in me. What type of anchors did you use? Like I get the Boeing engineers, I get the Microsoft, I get the Facebook and they've done all the research, right? They've seen the Olympics and they saw the two players that got back after Arthrex and they're asking me, am I going to do it?
[00:24:50] Dr. Grant Garcia: We'll ask this, am I going to do a speed bridge? Right. So if you don't offer that option, what are you going to do? Right. You got to stay up with the times. And so to me, it's the patients [00:25:00] have gotten smart and that's what helped build, honestly, for surgeons listening. One of my, one of my biggest polling points is that I, is that I offer some of these products because the patients want it.
[00:25:09] Dr. Grant Garcia: I mean, it's just a no brainer patients want their ACL repaired, and if you can do a good job on it, you have an awesome product that you can support. It makes it easier. And it's a heck of a lot easier for me to. Offer the surgery for the patients when I feel like consistently I'm not giving up something right like if I knew something would save me money And it was inferior.
[00:25:27] Dr. Grant Garcia: I would absolutely never ever use it in a patient and I might and I talked about this with my partners and everybody else. It's like, why are you using this thing versus this? I'm like, I think it's better. And if I didn't think it's better, and that's the best part about Austin and why our relationship works out.
[00:25:41] Dr. Grant Garcia: If I don't think it's better, Austin's like, then don't use it like Austin's in sales. But I can tell you right now, if Austin sells me something that's expensive and crappy, sorry to put on the, on the call, he knows I'm done. I'm not going to ever trust him on that product. And so he, that's what's really good about them too.
[00:25:56] Dr. Grant Garcia: It's not overselling, right? We're in sales, [00:26:00] trust me, it's a business and that's the way it works. But at the same point, it's amazing to focus, you know, with corporate Arthrex, but also this relationship we have with Arthrex and Pacific Northwest. Austin's team is that it's, I mean, you can describe this better, but you guys really, you don't, that's not your goal.
[00:26:18] Dr. Grant Garcia: Like you're not, your primary goal is not, you know, we have to find a way to get involved in everything possible. It's more like, what do you, what do you need? What's going on here? What's the problem here? What's your issue here?
[00:26:29] Auston Robinson: Absolutely. I mean, you know, that's a another unique approach that I think Arthrex senior leadership has understood and done very well for a long time.
[00:26:37] Auston Robinson: They look at solutions for problems, right? You know, we're we're a partner and we're a symbiotic partnership between the two of us. You treat the patients. How can we make your job easier? How can we make sure that if that's my mother on the table, she has the best, most optimized outcome possible. And I, you know, I, I appreciate the fact that you, uh, recognize the value [00:27:00] there, because I think that's a really important part of what we do.
[00:27:03] Auston Robinson: Um, and you know, it's, it's not dissimilar to, uh, Surgeons reputations in the community, right? I mean, the value that you provide to a patient, the experience that you provide to the patient, uh, is not the only distinguishing factor that sets you apart, but it's certainly something that attracts patients to you from the word of mouth reputation that you've developed, uh, along with your, your exceptional skills.
[00:27:26] Auston Robinson: But we, you know, for us, it's very similar. We can come in and try to hammer you over the head with what we want you to use. But I'm not an orthopedic surgeon. Uh, you know, I understand it at a lower level, but I do know that we can offer solutions to problems and make the patient's outcomes better with the technology.
[00:27:44] Auston Robinson: So we want to introduce those things. We want to make sure people are aware and raise the awareness level. And Arthrex has done incredibly well at that as well with things like in terms of the living up to the You know, commitment to education with our orthopedia website, Reinholds invested immense amounts of [00:28:00] money into that resource that is not even branded Arthrex.
[00:28:03] Auston Robinson: It's just a resource for people to learn around the world on, uh, surgical techniques and biomechanics. Dr. Chris Adams, our global director of medical education, who's a Burkhart fellow orthopedic trained surgeon, very successful guy has committed a ton of hours with an impressive team to, Build out those resources where they, they go through the anatomy, then the biomechanics, then the clinical relevancy and, and so on and so forth.
[00:28:28] Auston Robinson: Uh, you know, you, you've seen that, that, uh, website, but it's an incredible commitment, you know, and, and they back it up with their actions, which is a really fun thing to be a part of.
[00:28:37] Dr. Grant Garcia: And I think before I talk about the thing behind me, um, I think we should tell people too, you know, people want to know they've seen posts of like, I fly to Naples, right?
[00:28:46] Dr. Grant Garcia: It's a far distance. And obviously there is some level of competition when I fly, but at the same point, it's still time away from work, time away from my family. So what's the reason for doing it? Well, the reason for doing it and the reason that, you know, any surgeon who's interested should [00:29:00] learn about it or see the headquarters or even go downtown to, uh, you know, Uh, you know, Kirkland to see it is the really the teaching and what's gone into the resources to allow us to do this.
[00:29:10] Dr. Grant Garcia: I mean, if you want to show the headquarters, I mean, it's just absolutely gorgeous. Well, it's, it's got, you know, pick a ball courts, its own hotel, its own restaurant. Like this is talking about, like, this is like, this is better than going to Vegas for an orthopedic surgeon. Trust me. And the, uh, and the labs.
[00:29:27] Dr. Grant Garcia: I mean, you, you might see eventually, well, a video where I'm in an operating room, it's not even the operating room. It's just like an operating. They've built up just for videos to show people like in an operating room. And they've got a studio, one of like seven in the country, and that's called studio X and that's behind me.
[00:29:42] Dr. Grant Garcia: And what it is, they can turn into anything they want, any environment, and they can film commercials there locally. It's pretty sick. But what they really do use it for is to teach. Other surgeons and to teach patients and I think they have you guys have you know You've we've talked about my videos on my website I've got so many 200 [00:30:00] 300 and part of that is honestly just mimicking stuff that arthrax has done Because it works so well for me to learn right like all of us want to learn and the surgical videos are so important But the, I mean, the amount of money that, that Reinholtz invested in it is, this is not like, there's no reason to have done that much money.
[00:30:17] Dr. Grant Garcia: He just did it because he's, he wants to show everybody and he wants to have the best video products, right? There's no reason to have 25 K videos for your products from us, from a monetary standpoint, right? It doesn't make a difference in my opinion to show that. And to make, you don't make more money off that.
[00:30:34] Dr. Grant Garcia: He's just doing it because he wants people to have the best and if he wants to, she wants to show his stuff in the best possible format, would you agree? And that's what you were talking about. You know, he doesn't always, it's not always about the dollar or it's not about the stockholder. It's about, it's about, well, how can I show that?
[00:30:49] Dr. Grant Garcia: How can I have the best? And how can I give everybody the best experience?
[00:30:52] Auston Robinson: Absolutely. Yeah. You know, not to sound cliche, but it's been described as a nexus of innovation. And, you know, as, uh, [00:31:00] as, uh, interesting as that may sound, it really lives up to its reputation. Reinholds designed it to be such so that, You know, people have a place in the country where they can go and inevitably you bump into another surgeon from, you know, another part of the country and they're talking about challenges or world, right?
[00:31:18] Auston Robinson: Yeah, we come across Europeans and South Americans and people from Asia Pacific region and they're experiencing the same challenges, same anatomy, same injuries. And you can rub elbows together and say, Hey, how can we make this better? And then Reinhold says, you know, to the to the degree of having rapid prototyping and, uh, you know, visually enabling technologies to improve the patient's experiences.
[00:31:42] Auston Robinson: And I can say without hesitation, He, you know, in, in even the personal conversations, he's so devoted and committed to the experience of improving the patient, uh, patient's experience, the patient's outcome and supporting the surgeon in a way that they have the resources and they see that as an extension [00:32:00] of their practice to be successful.
[00:32:02] Auston Robinson: It's, it's really a remarkable thing.
[00:32:05] Dr. Grant Garcia: So well, how many times, oh, sorry. One second. Ask a question. Well, how many times have you seen a company? As big as Arthrex and everybody knows the CEO by first and last name and where you go to a random event, let's say you have. Walmart and you go to a Walmart function and the Walmart CEO is hanging out there.
[00:32:25] Dr. Grant Garcia: Let's say you have like a McDonald's and the McDonald's CEO is out there. Again, not belittling anything that Arthrex does, but I don't want to get to the proprietary of other companies, but it's one of the few companies where the CEO is constantly there and involved. And that's what's, I think that's really what makes a difference, right?
[00:32:39] Dr. Grant Garcia: You know, I mean, I'm out there, Will, I'm out there for something. And all of a sudden he shows up at breakfast and he's like, Hey Grant. Hey Garcia. And I'm like, this is the CEO of Arthrex. And you know, he's just, he, he knows everybody. He just has that. And he asks, starts asking questions. What do you think about this?
[00:32:53] Dr. Grant Garcia: What do you think about this? I'm just like, holy cow. This is a lot of information. This is the guy who's the CEO of the company. So, I mean, it's just the [00:33:00] involvement and that makes you feel really good, right? Like, well, if you work for working for, if you're working for someplace, you never knew your boss, you never knew anybody else, and you just basically did your job and you kind of sat down and you kind of sat there, it's hard, right?
[00:33:12] Dr. Grant Garcia: But to see all those people involved and so committed is it's pretty. It's pretty impressive. It shows the mentality. [00:33:19] Will Sanchez: Yeah. And that shows that it's organizational culture, right? So obviously I've never met this individual, but what has been discussed and how his policy is, that is what he's promoting breeding and encouraging.
[00:33:34] Will Sanchez: Right. Is that culture. So he's setting the standard. So then. Everyone else could follow along. And that's why you have folks like Austin and some other people that will be a part of your community, because that's the culture that he's fostering. So on my culture there, anyway, so we talked about technology.
[00:33:54] Will Sanchez: We talked about innovation and it's 2024. And what is the hot [00:34:00] topic that's happening right now? That. Is the super advancement in technology, right? The, the industrial revolution of this, uh, decade in a century is going to be AI. So how is AI machine learning virtual reality? How are they starting to think about that?
[00:34:19] Will Sanchez: To apply that to not only the tech you have now. but future tech going down the road?
[00:34:27] Auston Robinson: That's a great question. Uh, and it's an exciting frontier to be a part of. Arthrex is always looking at ways to enhance, you know, the offerings that they provide the surgeons for the patients. And one of those areas that they can use machine learning is, uh, you know, we, we, in our shoulder arthroplasty, uh, portfolio, we have a tool that is, uh, uh, tool that is accessible to all surgeons.
[00:34:48] Auston Robinson: It's the, uh, we call it a VIP targeting system, but it's based off of the patient's native anatomy through CT, uh, examination, digitization. And so, uh, with machine learning, they [00:35:00] can look at this array of, uh, CT images of different shoulders and identify based on the patient's anatomy and the morphology of their scapula and the humerus and the chromium, there's an optimal position of the products and the implants.
[00:35:15] Auston Robinson: in, during the surgical intervention. And that is a game changer because you don't have to wonder, is this screw going to go through and hit a nerve? Is this a base plate going to be too far lateral? The machine learning, uh, based on the formulas and the weights and inputs that they include in the algorithms allow you to have a much more precise determination.
[00:35:32] Auston Robinson: And now they can start to, and we're, I think we're still exploring this, but can start to upload or include. other patient specific considerations like, uh, other other components of their health and their their genetic background, things like that to make more specific decision making that allows for the surgeon to not have to wonder as much.
[00:35:55] Auston Robinson: Not that they're I don't think the surgeons are necessarily wondering often, but [00:36:00] it reduces and eliminates some of that. uh, gray area in, in terms of implant position and implant sizing selections. That's just one unique way I think, uh, Arthrex is doing it. They're looking at, you know, different ways that they can, uh, visualize or the surgeon can visualize intraoperatively the anatomy, say for a spine and some of the revolutionary, uh, designs that Arthrex has partnered with some really, uh, exceptional surgeons in the spine world to better.
[00:36:28] Auston Robinson: visualize and identify patient's anatomy when they're suffering from extreme pain. Okay, just
[00:36:34] Will Sanchez: to follow up on that, uh, can you see a world where Arthrex is not only leading a technology with, um, what's, what you're doing now for surgical outcomes, but also in a preventive way with having this AI information about the anatomy and seeing where there may be certain situation because, you know, they've ruptured their Achilles twice and they know their tendons [00:37:00] a certain way where, where maybe, and maybe I'm going, you know, to keep
[00:37:04] Dr. Grant Garcia: going, keep going, we see
[00:37:07] Will Sanchez: this arthrax preventative, uh, innovation headed.
[00:37:12] Will Sanchez: down the road.
[00:37:14] Dr. Grant Garcia: So I'm going to help a little bit and then I'll let him jump in. Sorry, but this is amazing. Will. Arthrex's focus is not on putting a hundred implants into a patient and revision, revision, revision. Arthrex's, Arthrex's goal by adding such as the, and Will don't get too excited yet, internal brace, adding biologics, adding all these things is so that you don't have to come and do the surgery again.
[00:37:36] Dr. Grant Garcia: And whether it will be more cost effective, that's the key here is. No more second surgery. And that's why I use a lot of my Arthrex products. Because I don't want to do another surgery on a patient. I want to give them the internal brace. The regular ACL. If I need to add biologics, do what I will. With the ACL repair, we're working on more biologics, tissue engineering, biomaterials, you name it.
[00:37:58] Auston Robinson: Wound
[00:37:59] Dr. Grant Garcia: healing, [00:38:00] jumpstart, amniotic patches, well, we could go all day on this stuff. That is the number one thing they want they want to find ways to prevent the second surgery preventing original surgery There's biologics. There's all these different things too that they have again. I digress Awesome.
[00:38:18] Dr. Grant Garcia: Keep going. Sorry.
[00:38:19] Auston Robinson: No that no, that's great insight. Dr. Garcia. I appreciate it. But yes Will, your question, can I envision a world where Arthrex is leading the way in that space, uh, with the leadership that we have, uh, in the organization and the teams that we have abroad, I can envision, uh, leading in any space, but especially in the, the area of preventative medicine, uh, you know, we have among the companies that are in orthopedics and in, in the industry, the broadest portfolio of, uh, biologics.
[00:38:49] Auston Robinson: implements that are our customers are exposed to, uh, to consider the entire algorithm of care, if you will, in how they treat the patient prior to [00:39:00] degeneration of tissue or cartilage during the procedure and then also postoperatively. So biologics, I know, uh, internally, our leadership is So strongly supportive of that direction that they're implementing those things in their own bodies on a regular basis, you know, to prevent arthritis, prevent tendinopathies, different things like that, uh, in a way that is, it just shows the commitment to the development in the, into the space.
[00:39:29] Auston Robinson: And I think that that's something that Arthrex is going to, I can't speak for Arthrex, uh, in terms of, you know, organizational, uh, strategic initiatives. But from my perspective and from what I've heard, I would say that they're absolutely geared up to do whatever they can to make it so that the patient doesn't have to, uh, you know, have the problems that they're potentially going to have.
[00:39:49] Auston Robinson: And that's that's, you know, if the patient's at the forefront or in focus in a topic and there's a way to get better, Arthrex is going to at least from my perspective, continue to do [00:40:00] what they can and invest in developing ways to mitigate the risk for the patient.
[00:40:05] Will Sanchez: The key word that you said, you said a lot of important things.
[00:40:09] Will Sanchez: But when you said arthritis and there's so many people that suffer through that, um, and getting closer to, uh, relief. One of many different ways, uh, that, that should be excited for everyone along with, uh, all the other things that you talked about with, uh, you know, preventive medicine. So it's really exciting.
[00:40:28] Dr. Grant Garcia: Well, and one more thing, I think what Austin brought up, but that's really important. It's very rare in a company. Is the size of Arthrex is a little bit alarming to some surgeons and overall when you hear about it, but the size is what gives them their domination because they have crosstalk between the groups.
[00:40:43] Dr. Grant Garcia: Like I'm, when I work in on something with ACL repair and I'm like, Hey, I want to add biologics. I want my patients to even have a better healing rate. I'm not satisfied with. 90%. I'm not satisfied with 96 percent healing rates. I want 100. I want 99. They're looking at, and again, we can pull up the tight [00:41:00] rope, uh, which I love talking about, uh, in there, but they're like, let's get the biologics team involved.
[00:41:06] Dr. Grant Garcia: Or Austin's like, let me look at the portfolio. And because they have so much in their portfolio, um, this thing in three or four years, as amazing as it's going to hear. And obviously the whole knee team's going to hear me say this is probably going to be even obsolete for Arthrex soon. Cause it's just, it's so good, but we can make it even better, right?
[00:41:23] Dr. Grant Garcia: We can add biologics to it. Can we get the healing up? Right? Like maybe this technique is going to stay there, but there's going to be something added to it. Like we're, we're not even close. Uh, you know, we're not even, we're not even close to the end of this sort of rain of continuing to improve. Would you agree?
[00:41:39] Auston Robinson: Absolutely. I think, you know, as long as there's injuries, we're going to continue to pursue with vigor, better ways to treat them. Right. And in optimizing the patient's outcome, as long as there's a patient on the table, uh, we can get, we can continue to get better. And again, I can't speak to Arthrex corporate strategic initiatives as an agency representative in, in the [00:42:00] little, uh, state of Washington, but, uh, from what I know, from what I see, I would absolutely, uh, expect that if they're, uh, If there's an opportunity, they're thinking of a way to make it better.
[00:42:10] Auston Robinson: The thing in a way to make the patient get back to activity quicker, to get back to sport quicker, to get back to work quicker for the patients that, you know, a lot of these surgeries require a lot of downtime, you know, I think of, you know, somebody that's a single parent can't afford to take six weeks laying down because they have back pain.
[00:42:28] Auston Robinson: So, You, you know, the, we could go way off topic on that, that issue. But I, as an example, I was getting a haircut a couple of weeks ago. And, um, my barber is a female. She said, I'm really struggling with this pain in my leg and said, have you seen a spine surgeon? And she said, I have, they've done some injections.
[00:42:46] Auston Robinson: Now they want me to get surgery. They say I need a decompression. And I talked to her about, you know, our arthritis has recently made a foray into endoscopic spine surgery. And instead of doing a large two centimeter incision, you can do it through a scope, [00:43:00] eight millimeter incision. And she started. Dr.
[00:43:02] Auston Robinson: Schaefer, Dr. Schaefer. Well,
[00:43:04] Dr. Grant Garcia: that's what we have. We just had him on talking about arthritic stuff.
[00:43:07] Auston Robinson: Yep. Incredible surgeon. And, and, uh, similar to you cut from a similar cloth and in terms of, uh, you know, an affinity for innovation and how to optimize the patient's outcome. But she broke down. She said, I'm a single mom.
[00:43:19] Auston Robinson: And they told me I would have to take six weeks off of work. I can't afford to take six weeks off. And I said, talk to, yeah, I recommended Dr. Schaefer, gave her, uh, your practice's number and the website. And I said, people are getting, you know, endoscopic spine decompressions and they're walking out of the ASC.
[00:43:36] Auston Robinson: They're, they're back to work two days later. It's incredible what's going on. And, and, you know, that that's cool from a technology standpoint, but man, it's really impactful from a patient outcomes perspective.
[00:43:48] Dr. Grant Garcia: Well, and I think, I think what you brought up is really important. Some patients don't understand the technology sometimes, and that's why we have this show.
[00:43:55] Dr. Grant Garcia: Just tell people about the new technology. That's why I had as soon as Andre got in practice [00:44:00] with us to talk about endoscopic spine because I don't think and it's sad because what you said is calming. I mean, I literally just had Multiple patients I saw today in the clinic and the lady was like, I can't believe my ACL is going to be walking out of there and I'm gonna be moving this quickly and I'm gonna, you know, my, or my UCL, I can start throwing the baseball so soon.
[00:44:17] Dr. Grant Garcia: I thought that it would take longer. Like, my last one did not or the other surgeon told me this and I'm like, listen, the technology we have, I can let you rip. Right. We can, we can do it right. This, you have an internal brace in that ACL. You can go harder on it. Like, it doesn't mean that we're going to be too aggressive in room.
[00:44:33] Dr. Grant Garcia: I mean, we just had an ACL repair patient and she was worried cause she had seen other protocols and they were slow. And she's like, I don't, I'm worried about tearing this. And I'm like, listen, this new ACL repair is way stronger. I feel much better letting you go. And it just, you could just see her face just calm down.
[00:44:51] Dr. Grant Garcia: Oh my gosh. I'm not going to tear this right away. I know you're not, I trust it. That's why I do so many of these. And so I think we'll can attest to this, but [00:45:00] having that basic technology and we can bring it up, we can talk about internal brace for a few minutes. Well, if you'd like to bring it up, but it's just part of me.
[00:45:07] Dr. Grant Garcia: Yeah. Talk about that. Honestly, Austin, you, you, you, uh, you're, you're, you know, you're the master of all things. But how is the internal brace concept? changed your entire perception of things.
[00:45:24] Auston Robinson: It's incredible. I mean, you know, when you look at the incidents of of retail rates and a lot of these, we've, you know, Gordon McKay back in, uh, you know, the late early 20 teens, mid 20 teens really put some interesting work.
[00:45:39] Auston Robinson: A surgeon out of Scotland into the lateral ankle and Pat Smith and yourself and so many have really kind of been willing to give this a shot for their patients. And I think the data has shown that there is a tremendous value added to the procedure for the patient if it's incorporated. Um, you know, it started out as [00:46:00] a as a supplement for A.
[00:46:02] Auston Robinson: T. F. L. Ligament repair or, or, uh, you know, it's called a brochure procedure. Uh, and you have these patients that are, are frequently rolling their ankles. Cause I think Dr. Muffuli published, 10 year data that showed that they, the, the native tissue repair stretches out over time. So is there a way to strengthen this?
[00:46:20] Auston Robinson: So the patients don't, as you mentioned earlier, don't need a second surgery, don't need a revision to this. And it's, it worked so well. People started to think innovative surgeons started to think maybe this could be applied in other ligamentous. uh, areas of repair and reconstruction. And now we see, you know, people using these and we see second looks where a patient gets into a car accident and they hit their tibia on the dashboard and their femur slides way forward.
[00:46:46] Auston Robinson: And all of a sudden, uh, the tight rope or excuse me, the internal brace ruptures, but their ligaments intact. So we preserved them from needing an entire new reconstruction.
[00:46:57] Dr. Grant Garcia: I have personally had that. Where a patient I scoped [00:47:00] him and I saw the internal brace it, uh, had torn and the ligament was still intact or you go in there and you scope them for another reason.
[00:47:07] Dr. Grant Garcia: You see the internal braces grown into the A. C. L. It's just incredible.
[00:47:11] Auston Robinson: I mean, you know, the seventies people didn't work hard seatbelts, right? And then they were invented and somebody quickly realized we should put these in every vehicle. And it's very similar to the the advent of the internal brace where why you know Maybe it's not relevant to every procedure But why wouldn't you do it if you can give the patient a more optimal outcome with that backstop in the in the construct
[00:47:37] Dr. Grant Garcia: This is a good question I get this a lot from patients and will may have this question too since he has part internal brace in his body the uh, the I would say this question You Is it going to damage my ligaments?
[00:47:50] Dr. Grant Garcia: But I mean in your perspective I have I tell them I put in More I put in over that I've put in thousands of these and it actually grows into [00:48:00] ligaments Is that what you guys have seen like what is your experience with this? I mean that doesn't to me. It's very inert It's collagen impregnated, right?
[00:48:06] Auston Robinson: That's right. It's, it's synovializes with the ligamentous repair, uh, and healing process. And we've put millions of strands of fiber tape into human bodies since the early 2000s. And that reaction rate is, is, uh, insignificant. And so it's an incredibly safe, inert product that is there as a support for the construct that gives the patient the opportunity to prevent re tear of their ligament.
[00:48:31] Auston Robinson: Uh, you know, and it's a great adjunct to what's being done biologically there. Uh, because we all, I mean, you can speak to the science far better than I can, but as those graphs reincorporate, we know that they kind of turn into a jelly before they really reconstitute as a ligamentous tissue. So in that season of reconstitution, having something there that can offer a little bit of mechanical support.
[00:48:54] Auston Robinson: Makes a lot of sense. And, and I think the data shows that.
[00:48:58] Will Sanchez: Got a quick question here. Um, as [00:49:00] we get ready for, um, the NFL season that's coming up and just looking across the board, um, where around the world, football is the number one sport here. It's NFL. Can you see, um, a place where owners, and this is.
[00:49:19] Will Sanchez: Probably just personal thought, not trying to label the company's, uh, thought process behind us, but where these owners in these big industries could possibly start to incorporate some of these things in their, uh, players. For example, we see every offensive and defensive lineman pretty much wear knee braces, right?
[00:49:39] Will Sanchez: We know that between knees and ankle damages in the sport of football, um, It takes time away from the pitch and, you know, these billion dollars, you know, worth of revenue that come through. Um, especially if it's deemed safe, is it something that you can see, or is this kind of a [00:50:00] little farfetched as far as what, you know, we may see in the future of sport, protecting their investment and maybe not exactly the internal brace, but maybe there's some future tech alone.
[00:50:11] Will Sanchez: No,
[00:50:11] Dr. Grant Garcia: I think this is a great point. I think what. You're asking for is that's what they do. The arthritis teaches the team doctors. I mean, you have a team physician meeting. For all the team surgeons in the country that come to it and they learn about techniques that the other team positions are doing. And so it becomes a standard of care in the NFL, right?
[00:50:30] Dr. Grant Garcia: I mean, that's pretty much what that meeting is for. It's an incredible meeting. Um, and you can talk more about it briefly, but. Will, you're that's already happening. You just don't know about.
[00:50:41] Auston Robinson: Yeah, I think we, you know, we see more and more stories of high profile athletes that, you know, to your point of protecting the investment, uh, from the, the team's perspective, it makes sense, right?
[00:50:52] Auston Robinson: I mean, anecdotally, I've heard, uh, team doctors say that there's even been big linemen that, that have had a history of rolling their ankles, [00:51:00] asking for the internal brace prophylactically, uh, just as a preventative measure. Um, no, I don't think any surgeon in good conscious, uh, in good conscience to do that.
[00:51:09] Auston Robinson: Uh, you know, but the concept is there, uh, you know, be for the same reason you're asking the question. It makes a ton of sense to reinforce some of those, uh, injury prone anatomic location.
[00:51:22] Will Sanchez: And maybe this is the question that we're talking about leading into, you know, future tech, right? Because maybe it's not set up exactly the way it is now, but maybe as we go ahead and look five, 10 years from now and seeing a product that Is safe that can help, uh, players, you know, maybe this is something along the lines where there's Arthrex or anyone else that, you know, they're protecting this huge investment because we were seeing common injuries, injuries in certain sport, um, to protect.
[00:51:50] Will Sanchez: And, uh, it'll be interesting to see what happens. So as we always, I think you're on
[00:51:54] Dr. Grant Garcia: to a new show idea, by the way, this is phenomenal, this has been talked about in ACL [00:52:00] repair, there is, there was some theory. That if you didn't, if you didn't, uh, so an ACL repair, sometimes you do an extra ligament called the extra articular, um, tinnitus with called an IT band, or you can do an ALL reconstruction.
[00:52:13] Dr. Grant Garcia: There's some thoughts about doing that second ligament, but just doing internal brace, if someone hasn't told their ACL, but it's a high prone. And actually, I don't even know if there's a public study. I thought there was on this. It seemed like, I don't know how the IRB would approve it. Um, but some players have been considering doing that to prevent getting their ACL torn.
[00:52:31] Dr. Grant Garcia: Um, so you're onto this. And I. Don't know how it will ever ethically get approved or how anybody would ever undergo it, but there are some athletes that want the edge and an ACL tear is devastating or an ankle sprain. We've seen hundreds of those in the NFL, you know, Saquon, obviously not, no longer giants.
[00:52:47] Dr. Grant Garcia: We don't want to talk about it too much, but you know, roll, roll this ankle. Will and I are both giants fans, by the way. So, uh, I do think. [00:53:00] That it'll be prophylactic or though what we've seen now is surgery happens sooner. right? We have better instruments. So the old way of like, let's wait 20 times before you get surgery.
[00:53:10] Dr. Grant Garcia: Now it's like you're getting surgery right now. Like it's way better this new way, right? My homes are not homes. And there was other player that got an internal brace for his MPFL, his dislocating kneecap. And it was way earlier than he should have. And he ended up doing great because it's much faster recovery than standard reconstruction, right?
[00:53:26] Dr. Grant Garcia: Those are the type of things I will. So prophylactic before the injury happens or prophylactic before the standard would happen for surgery. Yeah. And therefore, you reduce the issues later on. So everything you're talking about is spot on. Well, you're, you should do it.
[00:53:40] Auston Robinson: Yeah, that's right.
[00:53:42] Will Sanchez: All right, Garcia, we, we need to wrap it up here.
[00:53:44] Will Sanchez: Um, but before we go, um, Austin, if you could control all of it, what would you like to see? Five years from now, 10 years from now, um, as far as a [00:54:00] revolutionary tool or something biometric to help the patient and surgeon collaborate to, uh, take this to a whole other level, you've got the power, you're the God of Arthrex and all this little toys, what would Austin do with this power?
[00:54:17] Auston Robinson: I'd love to come up with something unique, but I'm sure, uh, Reinhold's already thought of it. Uh, yeah, I, I, uh, I think that, you know, we would love to see things in from my perspective, you know, with the patient being the center of our focus, anything that we could do to anticipate the injury, like if there is a device that could be used to test the quality of of ligaments and tendons and look at their, their native tensile strength.
[00:54:42] Auston Robinson: Uh, before the sports injury occurs or, uh, if we could test the, uh, annular tissue of the, of the vertebral disc in, in determine whether or not their disc was going to rupture and go in and, uh, somehow with minimally or ultra minimally and basically, uh, Prevent that from [00:55:00] happening, I think would be remarkable technology, and I don't see why it's not gonna be something that we see in the in the near future, with all the development going on in the tech space and the merging of tech into into medicine.
[00:55:12] Auston Robinson: And, you know, you see different ads for a I being able to detect detect the breast tumor years before it actually develops those kinds of things that is going to Be a game changer for families around the world. Uh, and I think it would be a lot of fun to see Arthur X be a part of that because selfishly I'd love to be a part of it as well.
[00:55:31] Dr. Grant Garcia: I love that. And I think that's going to be the future. Right? You know, AI learning on MRIs. They're like, your disc is about to herniate. Go see the surgeon, 20 minute endoscopic procedure, little tiny patch, little internal brace on the disc will make him happy. And you know, the surgery takes 15 minutes.
[00:55:47] Dr. Grant Garcia: There's no recovery time because you never got hurt in the first place, right? You're almost got hurt, but didn't get fully hurt. And now you never going to tear that disc again. Right? Like that's, that's, that's what it's at. Well,
[00:55:58] Will Sanchez: Austin, thank [00:56:00] you so much for taking time. Uh, this was extremely informative and we really appreciate you, uh, being a part of the show.
[00:56:07] Will Sanchez: So, uh, thank you. I know Garcia talks to you all the time, but, uh, it was my pleasure to have you on. So thank you. Garcia. Thank you for the Austin.
[00:56:16] Auston Robinson: I really appreciate you having me. It's a real privilege. I'll talk to you
[00:56:18] Dr. Grant Garcia: tomorrow, Austin.
[00:56:19] Auston Robinson: I'll look forward to it.
[00:56:23] Will Sanchez: Dr. Garcia, man, Austin Robinson, that was awesome.
[00:56:26] Will Sanchez: Um, you talk too much. Look, we're almost at an hour. It's all your fault. We're just going to blame you for everything. I don't know. I know.
[00:56:33] Dr. Grant Garcia: It's because you give me too many layups, man. It's great. Unfortunately, I like all the guests too much. That's the problem. We need to pick some guests that are, I don't want nothing to do with.
[00:56:41] Dr. Grant Garcia: Then we won't chat. Yeah.
[00:56:42] Will Sanchez: Yeah, that won't be any fun. And we'll just be staring at each other and just comparing backgrounds. But listen, a lot of great information, right? You know, we, we talked about training, you know, a VIP targeting system, machine learning, preventative medicine, biomaterials, tissue, engineering, largest [00:57:00] portfolio,
[00:57:00] Auston Robinson: Austin
[00:57:02] Will Sanchez: has, I loved his answer on future tech.
[00:57:06] Will Sanchez: I mean, that is exactly, it is not a pie in the sky kind of answer. This is a legit answer where we all go. Yeah, that sounds great. Sign me up. I'll take one of those. And, um, you know, let me know when something's bad is going to happen in my body, right? Because that's what we want to get to. Right. And whether it's, I know, I know I'm going, here I go.
[00:57:28] Will Sanchez: I'm doing a one 80 here. Right. You go get a colonoscopy because you're trying to be prevented, right? You, you go through, you, you do certain things to make sure that you're going to be okay, and you're catching it early. That's exactly what we're talking about is having some tech besides the wonderful things that they do now is eventually, hopefully getting to that point as well.
[00:57:49] Will Sanchez: We can do better. Well,
[00:57:50] Dr. Grant Garcia: we can always do better, right? That's the one thing of the show. If you, I tell everyone this, if I'm doing the same thing I did five years ago, then I shouldn't be doing it because [00:58:00] you're not innovating. So preventative medicine is huge and preventive orthopedics is actually not talked about that often because I hate to say it.
[00:58:07] Dr. Grant Garcia: We like surgery. So, but if I could find a way to prevent people from having injuries and being fearful of injuring themselves and get to all the sports they love. I think that's honestly the best thing. And that is, I really appreciate Austin coming on and all the viewers listening. And I know we need to wrap it up cause we're on a minute and 40 seconds before we get kicked off.
[00:58:26] Will Sanchez: We're not going to kicked off, but we got to stay under the 60 minute. And I love the thing that you guys talked about in the beginning saying, yes, this works. But we can make it work better. And it's been changed two, three, four times, not because it didn't work or it failed is because you found a way to like, this works great, but if we do this, we can make it work better.
[00:58:47] Will Sanchez: So I, you know, that's something that I took out of it, that conversation as well, and that's something that. Everyone should be excited about. It's not, not only that this is, you know, we're doing something that's great and we utilize in the tool. That's great. But [00:59:00] how can we make it better? And I think that was the common theme throughout all this.
[00:59:04] Will Sanchez: How can we make it better? Dr. Garcia, we're going to wrap it up. We've got NFL and everybody's excited. I don't know how I'm feeling about the Giants. We'll talk about that the next show, but we're going to talk about key players coming back from injury, major injuries, how that affects the upcoming NFL season.
[00:59:21] Will Sanchez: And then somewhere along the lines, we'll probably take about two minutes and cry in our bowl about the upcoming Giants season. But as always, Dr. Garcia, our sports medicine orthopedic specialists, thank you for being with us. You rock as always. Um,
[00:59:42] Dr. Grant Garcia: Thank you, Will. Always good. Great episode. Thanks, guys. Audio Transcript
Mike Trout’s Second Meniscus Surgery Discussed
Will Sanchez:Welcome to Sports Doc Talk. This is our 15 minute edition. I'm keeping my fingers crossed that we're going to hit that 15 minute or less. We're not going to. We can do it. I'm Will Sanchez along with orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia. Our top doctor, you know, him, we love him.
[00:00:38] Will Sanchez: He's got this cool, funky background going on, man. This is very like, wow, look at that. This is a Stanley Kubrick kind of thing going on, man. How
[00:00:46] Dr. Grant Garcia: are you? I'm good. This, this is a nice fun. I, you texted me this weekend. You said to this, you talked about this, uh, Mike trout injury. And I was like, you know what?
[00:00:53] Dr. Grant Garcia: It's time. This is our first. 15 minute segment. All the other ones have been [00:01:00] audio, so this is the first blast, um, and we're hoping for this season, uh, to do a few more of these, because I think that our listeners like these a lot, like, because it's more, it's more cutting edge, it's more, uh, recent, um, and this, this is the first time we've done this.
[00:01:15] Dr. Grant Garcia: meniscus stuff we're going to talk about is just keeps coming up. It's just nonstop with these. We just talked about an Olympic episode literally last week.
[00:01:24] Will Sanchez: Yeah. Yeah. And, and listen, it, when you have an injury to a first ballot hall of famer and Mike Trout, uh, someone that his career path was, you know, up there with some of the greatest players ever, except for the last five years now, where he's been pretty much robbed of a complete baseball season.
[00:01:45] Will Sanchez: And we'll show you the stats later on, uh, due to injuries. So just to recap on April 29th, Mike Trout, uh, was playing in a game. Uh, felt a little something in his knee, [00:02:00] went, ran the bases, played the outfield. Um, you know, came, came in, was like, yeah, I think I'm good. Didn't, no concerns. He goes home and, and I want you to kind of chime in on this.
[00:02:13] Will Sanchez: He goes home. goes to bed and it's like, Oh, something is not feeling right. I'm ha he's having pain. He, he's going through pain at night, wakes up in the morning, calls the doctors, like, Hey, I'm having some issues with, with my knee. Um, you know, maybe we should just go check it out just in case he wasn't thinking of anything because of the way that he was able to complete the game.
[00:02:38] Will Sanchez: Finds out when April 29th that he's, he tore his meniscus before we go further. What happened to Mike Trout? Is it just the adrenaline that kind of kept them going through or things didn't settle in? What happened when he got home at night, laid down, and when he was trying to sleep, all of a sudden this pain started coming off.
[00:02:59] Dr. Grant Garcia: So [00:03:00] one, you know, obviously you don't know the tear pattern. We didn't see the MRI. We talked about there's various tear patterns, right? You got these meniscus, it's C shaped.
[00:03:07] Will Sanchez: Yeah,
[00:03:07] Dr. Grant Garcia: you can have a radial tear. That's a big split. Probably not that usually that's a massive pop. And then you're like literally unable to walk, which is what we thought was happened to the Olympian.
[00:03:16] Dr. Grant Garcia: Right. Big crack. Yeah. This is a different thing. Uh, but again, we don't want to give away too much of it, but obviously it was repairable. So it was some tear pattern, maybe in the back of the meniscus where there's better blood supply. When you get a tear right there, uh, and usually it's a tear, it's a, it's a, he's probably from when he was batting or rounding the bases, right?
[00:03:36] Dr. Grant Garcia: Like it's a, it's a plant shift. And one thing that can increase the risk of this is probably the cleats, um, when he's batting, right? Cause you're, you're, you're plant the foot and then you're, you're cranking the knee. And if there's any pre, you know, they can have, you know, guys like this that are playing all the time, they can have these little small meniscus tears.
[00:03:54] Dr. Grant Garcia: We used to see, we took care of the giants, uh, and the mats and stuff. We'd have Monday morning kind of MRI [00:04:00] review and you get to see some crazy stuff in MRIs for players that are like still actively playing.
[00:04:04] Will Sanchez: Yeah.
[00:04:05] Dr. Grant Garcia: Right. So he may have had some small capsular tear that you couldn't really recognize, twisted, had some pain and maybe had a little tweak and he's like, Hey, I'm fine.
[00:04:12] Dr. Grant Garcia: I'm going to deal with it.
[00:04:13] Will Sanchez: Yeah. Yeah.
[00:04:13] Dr. Grant Garcia: Then he gets home. And what happens is these tend to ache and like my patients who have these special capsular tears or tears in the back where the blood supply, they say at night they have to put pillows between their legs and anytime they twist or move, it hurts a lot more and it probably started swelling up on it.
[00:04:30] Dr. Grant Garcia: So like, that's what he probably felt. And that's only me reading between the lines from experience from him at being in a fixable repair and just from the fact that the fact that it acted more at night and these, these tear patterns that he got these tend to be ones that people can kind of go up and down with, right?
[00:04:46] Dr. Grant Garcia: Like sometimes they know, but he's my trout. So he's getting MRI right away. Like some of these patients that come in, they're like, they've had it for two months. They've never really, they know they're just kind of like dealing with it.
[00:04:54] Will Sanchez: Yeah, so he has surgery on May 3rd, right? So we go back to April 29th.
[00:04:59] Will Sanchez: This is when he felt [00:05:00] that whatever happened to his knee, obviously we know that it was a torn meniscus, goes in May 3rd, uh, begins rehab assignment at AAA Salt Lake on July 24th. Before that, On the Thursday, they said that the MRI was clean and it was expected to start running shortly. And then he goes rehab assignment, plays two innings, leaves the game due to knee discomfort, right?
[00:05:27] Will Sanchez: And then they necessitated a follow up MRI, which revealed a new tear separate from the first one. And they're saying it's unclear. that how he tore his second or how he suffered a second tear. So I'm not going full, uh, conspiracy theory or what, but what is it? What, what, when you hear these things, what, what could have happened?
[00:05:54] Will Sanchez: Uh, because obviously this man is the franchise and the face of baseball. One of the faces [00:06:00] of baseball, the franchise for the angels, they wouldn't. I would assume that they're not going to risk his health based on them rushing him. So what happened? What do you think happened? The fact that he has an MRI, he has a meniscus tear and now suffers another one, uh, a month and a half later after surgery.
[00:06:20] Dr. Grant Garcia: Yeah, so again, obviously we don't hold me to this, right? We, or hold me to it, but you know how this works. We're predicting a surgery. Hold on. I'm writing down
[00:06:28] Will Sanchez: notes to hold you to it. Hold on a second. Write it
[00:06:30] Dr. Grant Garcia: down. Write it down. Maybe you'll find out in like six months. I had no idea what I was talking about.
[00:06:34] Dr. Grant Garcia: That's okay. That's how we do the show.
[00:06:36] Will Sanchez: So
[00:06:36] Dr. Grant Garcia: the uh, and again, thankfully my ego is not too soft. So I think I can handle it. So, you know, so the um, that's right. So basically he gets a fix. So you already know that the tear is a special type of tear, right? There's only certain tears we can fix. Some of these baseball players, school players, they get tears that are kind of just trashed meniscus, and you can't fix those, right?
[00:06:55] Dr. Grant Garcia: Probably not a root tear, probably not one of the more complex radial tears we talked about. He would have been out for a lot [00:07:00] longer, five, six months. So, I'm, I'm reading between the lines, right? He had a rate, he had a tear of the meniscus, and you guys see here, medial or lateral, generally they're medial, but I don't know which side his was.
[00:07:10] Dr. Grant Garcia: Medial means it's on the inside of the knee. You can see there. And then there's usually it's around the capsule. So the meniscus has blood supply in three zones, white, white, which means there's no blood supply. Those almost always get removed middle, which is red, white, occasionally fix those. And we're starting to push the envelope on fixing those, which you've talked about on previous episodes and younger patients.
[00:07:28] Dr. Grant Garcia: We fix them more. Um, and then red, red, which is right next to the blood supply. Those you want to fix as much as possible. Cause if you don't fix it. You remove a lot of meniscus and we've seen already we've talked about this a number of times on this on this show That removing that much meniscus is not good for people if you have to do it You know people ask like in their 50s like you're removing my meniscus.
[00:07:51] Dr. Grant Garcia: Why are you doing that? Well, I can't fix it then right it doesn't heal the same as it does in someone like mike trout who's still young uh active and healthy, um [00:08:00] And really the meniscus under, you know, 40, 30 years old. We just want to fix his man. He's
[00:08:04] Will Sanchez: 32 years old. Just to kind of give you the age group.
[00:08:07] Will Sanchez: He turned 32 years old. In fact, uh, it is, I think it's almost his birthday, August 7th. 33
[00:08:18] Dr. Grant Garcia: years old. Unfortunately, happy birthday to him. So anyhow, so the, um, so basically he gets this fixed and it's probably a capsular tear. He probably gets it fixed. There's different ways of doing this, right? There's stitches.
[00:08:29] Dr. Grant Garcia: You can do stitches from just two little poke holes. He can have a bunch of stitches in his knee and someone catches him out the back and he tie him in the back. And that's kind of like the more aggressive kind of gold standard method. So what happens is he gets that done and he gets his three month recovery.
[00:08:42] Dr. Grant Garcia: That's what makes me assume it was probably one of those, right? Cause it's only three months.
[00:08:46] Will Sanchez: Yeah.
[00:08:46] Dr. Grant Garcia: He starts running on it. He gets a clean MRI. The problem you have with the MRIs on these meniscus is you can't, I've been on my own meniscus and sometimes you think they MRIs are clean or you go in there for another reason, right?
[00:08:57] Dr. Grant Garcia: You rescope their knee cause they're having some other issue [00:09:00] or like a year or two later something else gets hurt, right? And you rescope them and then you go in there and you see like your meniscus repair is like mostly healed. There's still the stitches in there, but there's a line like where like imagine like your meniscus tear is like a full slit, right?
[00:09:13] Dr. Grant Garcia: It's the whole thickness of my fingers. Only like this much, only like this much healed, right? So you still have a layer that's a tear on the top, but on the MRI, it looks like it's a full connected tear repair. Cause what happens is scar tissue is really hard to pick up on these MRIs sometimes. So they always say like some of the reports, like I look at them as myself, but the reports say, Possible tear, but maybe due to surgery.
[00:09:38] Dr. Grant Garcia: So it may just be healing. Cause people always want to know, did it heal? So they think it healed, they let them go back out and he re tears it, or he ripped through the stitches. And that's what I think happened. He, the, the stitches we placed, you place that they're stress risers. And if it doesn't heal, those stretches are now holes in the meniscus and they can tug on them.
[00:09:58] Dr. Grant Garcia: And to be honest with you, I've had this happen to [00:10:00] me. You know, I do a lot of meniscus repairs and every once while you get in and the meniscus didn't heal. And now you've got this sort of rope. in the meniscus. And if it doesn't heal and scar in, it can act as like a knife and it can cut through. It's not anybody's fault.
[00:10:13] Dr. Grant Garcia: It's just the fact that didn't heal. And now he created a new tear.
[00:10:17] Will Sanchez: So that's why it was a
[00:10:18] Dr. Grant Garcia: separate area.
[00:10:19] Will Sanchez: I want to read a quote from him, right? Because to me, this is a warning sign or a concerning sign. And for you, it's probably nothing because you're like, yeah, I hear this all the time. He says, since my initial surgery on May 3rd to repair my meniscus, my rehabilitation proved longer and more.
[00:10:34] Will Sanchez: difficult than anticipated. But if you talk about the three month timeline, he came back right before the three month timeline. So if you're saying that you're, it was a difficult process and maybe it's just because these guys are super, super human. So it, you know, the fact that you don't recover as fast as you expect, you know, that all of a sudden there's a warning sign for the player, but when he says something like that, I don't know.
[00:10:59] Will Sanchez: Are [00:11:00] you concerned or is this something that it was just maybe bad luck for, you know, either didn't heal properly or he popped that, uh, that stitch and he suffered that tear?
[00:11:11] Dr. Grant Garcia: This is a classic sign that, again, first off, don't know the situation and he's also, you know, he's frustrated. You'll show a stat how many times he's been injured, right?
[00:11:23] Will Sanchez: Yeah. So to
[00:11:23] Dr. Grant Garcia: him, it's like any days down, he's like, this is so long, right? Like my, you know, I have this, I have, I'll see four patients, the same ACL surgery done within a few weeks of each other. Same surgeon, same technique. And one will be like, Oh, this process was terrible. It was so long. I'm like stressed.
[00:11:38] Dr. Grant Garcia: I don't want to do it again. Second one's like, thank you so much. You saved my knee. All of them look the same, but they all have different complaints, right? So you don't know the ones when I get these revision situations where something happens or I see someone that's had this and they'll say they go to get a second opinion, right?
[00:11:54] Dr. Grant Garcia: And they're like, my knee never felt right after the surgery. That's the ones you were kind of like, okay, that's a little bit [00:12:00] fishy. I don't think it's fishy with the angels. I think they probably did everything they're supposed to do. And also it's really easy for, I don't know when he quoted this, but it's really easy for Mike Trout to say My recovery wasn't as good as I wanted when he reto his meniscus.
[00:12:11] Dr. Grant Garcia: Oh, after
[00:12:12] Will Sanchez: the fact? Yeah, if it's after that, yeah. Like it's just
[00:12:14] Dr. Grant Garcia: total bias. So you know, you don't know. But, and also like we know Patience and Mike t Trout's no different. I mean, this is guy, this guy's smart, but he is not a rocket scientist. Like I'm sure the surgeon told him how long it was gonna be and he just was like.
[00:12:28] Dr. Grant Garcia: Whatever you want to do, doc, just fix me.
[00:12:31] Will Sanchez: Right.
[00:12:31] Dr. Grant Garcia: And sometimes they don't listen and they're sitting there like at two months. They're like, why is my knee still swollen? I'm like, I told you it's going to take a long time.
[00:12:37] Will Sanchez: So when it comes to the recovery process, right? Tear now retear 14 seasons in the major league baseball.
[00:12:49] Will Sanchez: He's going into his 15th season. just just turning 33 years old, so not old as far as age and even baseball. You kind of should be in your [00:13:00] prime, but he really started his career at an early age, which was really fast tracking him to this Hall of Fame resume. Uh, uh, What's the recovery process and then what are some of the concerns now?
[00:13:13] Will Sanchez: Obviously he's out for the whole season. So you'll have the rest of this year going into the winter and then coming back for spring. Are there any concerns at this point, uh, for as, as a doctor there, or is it something like, Hey, it's just. Shit happens, you know, go through the recovery process, you know, go through your PT, start over, get stronger and you know, we should see you back on the field or is it something where you go, all right, now we've got into that knee.
[00:13:44] Will Sanchez: What have we lost? Right? You're not looking at the knee. It's a process. What has been lost already from the surgeries to maybe impact not only his recovery process, but possibly continuing his career because he hasn't [00:14:00] played a full season in quite some time.
[00:14:04] Dr. Grant Garcia: And you can show the stats there. So basically, so to answer your question, this is really concerning.
[00:14:10] Dr. Grant Garcia: I mean, usually I tell them if, if, if someone good did a surgery, which I think it was, Um, the odds of it being fixable again are pretty low and going and trying it again on a guy like this might be a bad idea, right? Cause you're going to look pretty bad if he fails again in like three, in three months, right?
[00:14:28] Dr. Grant Garcia: We know about, it was a, one of the guys, uh, it was a guy that, you know, retore his triceps, sent him for the giants. And then he tore it again after, you know, playing it was out again for another six months. Right. Like he just doesn't, this is unfortunately get a little bit scary. I don't want to say this word, but it's sounding like Lonzo ball, right?
[00:14:45] Dr. Grant Garcia: They know like meniscus reminiscence. Now again, the first was a repair, but the second was likely a removal and we know where that went. And so that is the, that's obviously worst case scenario. But I, I, I don't think the amount of time that he [00:15:00] has to recover really matters to be honest with you.
[00:15:02] Will Sanchez: Yeah.
[00:15:02] Dr. Grant Garcia: It's what the health of the cartilage is and how much meniscus gets removed. If his cartilage is healthy, which we don't know. Probably is maybe hopefully. Um, cause he's still young, then he's going to be in a better situation. And if it's a medial meniscus, which what we showed on the board, medial meniscus, they do way better.
[00:15:23] Dr. Grant Garcia: If it's a lateral meniscus removed, they do a lot worse. And I mean, I've had a, I took care of an NFL guy that retired at 32. This guy was incredibly athletic. Had two lateral meniscus removals came to my office with a knee that was like knock me like this Terrible arthritis at 32, right? So that's what happens on the lateral side medials tend to last a lot longer So if he gets his medial meniscus removed At this point he may make it, you know He'll probably make it for the next few years of his rest of his career Um, and then obviously eventually may have issues in the long run But again, a lot of these athletes have that it doesn't it's not from this actual injury per se Um [00:16:00] But, but again, the problem is if he has all of a sudden he loses meniscus and he starts getting a cartilage hole, then we're looking at the same issue, you know, is he going to get a micro fracture, which we mentioned before, is he going to get a cartilage procedure?
[00:16:12] Dr. Grant Garcia: Is that even going to be possible for him? I hope not. We've got to see the worst case scenario with Lonzo Ball needing a really big surgery, like a Hail Mary surgery for a professional athlete. But those are the risks. If they do a repair, I'd be shocked. And then recovery wise, generally depends on the type of tear you repair.
[00:16:32] Dr. Grant Garcia: But usually, you know, two weeks of crutches, one week, no weight, one week, partial brace for six weeks with that sort of three to four month recovery. But everyone's different, right? Like Mike Trout's getting the best
[00:16:43] Will Sanchez: PT.
[00:16:45] Dr. Grant Garcia: Some patients takes five, six months. So it just depends on the level of what he's having.
[00:16:49] Dr. Grant Garcia: If he just gets a cleanup or, you know, that usual clean, you know, people go say they clean the knee, right. Did the little, the little cleanup of the knee, you know, that's probably six, six, eight weeks. So he doesn't [00:17:00] need all that time to get back. So we'll know how he's doing probably in the off season or towards the playoffs or pre.
[00:17:06] Dr. Grant Garcia: Um, but also depends like if he's out for the season, right. Cause you have August. I mean, September, October, they're out.
[00:17:12] Will Sanchez: Yeah, no, he's done. He's done for the year. And obviously it's a smart move. Um, let's wrap it up here because we've gone over our 15 minutes. So we got to change our 15 minute segment to 1723.
[00:17:26] Will Sanchez: But, um, I have to ask it any advancements right now when it comes to meniscus. Um, you know, recovery or surgery, things like that. We always like to talk about, you know, future stuff and all the cool toys that are out there. Is there anything that, um, that you can kind of throw out there that might be beneficial or depending on really kind of what's going on.
[00:17:49] Will Sanchez: And just to clarify with everyone that's listening or watching, it's hard to, we're talking about the injury itself. It's hard to know exactly what it is unless it Dr. Garcia was in [00:18:00] there looking at the knee. So I just want to kind of throw that out there as well.
[00:18:03] Dr. Grant Garcia: Well, and also for layman terms, right?
[00:18:05] Dr. Grant Garcia: Like everyone's here's the word meniscus tear. They all seem the same for me as a meniscus specialist. I go, if I go in like tomorrow, I'm doing three different types of meniscus tears repairs, right? They're all three different. Yeah, so for it's a very large gamut of that and I'm getting into the minutiae of it, but so advancements This is very similar to the ACL biologics.
[00:18:26] Dr. Grant Garcia: So the one advancement is we do the microfracture I told you about originally on the show poke holes where there's ACL PCL and with stem cells I'm assuming the surgeon did that there's been some studies on PRP So we take PRP injecting the knee after the meniscus repair hopefully help it One of the slick thing you can do is you can take blood turn into a vibrant clot and try to sneak that into the meniscus repair that you're doing it again.
[00:18:48] Dr. Grant Garcia: This is assuming that he's getting a meniscus repair. So you want to get that. Also, what matters is it kind of crazy, but you just have to do a good job of repairing it, right? Like you can't skimp. So this is getting the [00:19:00] details, but if you fix them, it's a meniscus. The meniscus fibers are radial. So they're circular.
[00:19:05] Dr. Grant Garcia: Does it make sense? Yep. Circular. So if you fix it horizontally, so I'm trying to do my best here to show you. If you fix it horizontally, you'll, you can go right through the meniscus. You see that if you fix it vertically, you cinch the meniscus and it won't tear out when you fix it. So when you do your repair, you wanna try to get your repair sutures like this rather than like this.
[00:19:26] Dr. Grant Garcia: I mean, you have to sometimes do that, but like this way stronger in the meniscus. So sutures, so all those things. Vertical,
[00:19:31] Will Sanchez: not horizontal, right? Because vertical. See, member, think about this vertical you got,
[00:19:36] Dr. Grant Garcia: I'm coming at you. Like this scissors vertical. You don't want vertical. There you go. I'm not, um. He might, that's gonna scare, that's gonna scare everybody now.
[00:19:44] Dr. Grant Garcia: Anyhow, so the, uh, so else, so the, uh, and then there's, and then there's Bone Mar Aspir. I'm sure he is getting everything. I'm sure he is doing that. I'm sure he is getting more stuff. And, and there's like collagen gels they're talking about. Again, this is the, when you figure out the solution on how you [00:20:00] can take an 80% success surgery.
[00:20:02] Dr. Grant Garcia: You know, without an ACL tear, this is a pretty, there is, there are people that do not do as well when you, if he tore his ACL at the same time, the success rate would go way up, right? So it's the, the issue is without the ACL, uh, is the problem here. And so we're looking at everything. I said, PRP, fibrin clot.
[00:20:20] Dr. Grant Garcia: I mean, I'm working on some of this stuff right now with other things and how we can make our ACL repairs better. So the biologics is a huge topic on this. We're just not there yet. But we're getting, we're going to be there hopefully soon in the next few years. So we'll see.
[00:20:33] Will Sanchez: Great job, Dr. Garcia. We hope that the three time AL MVP gets back on the field next season and, uh, is able to perform for all the fans out there that enjoy watching them.
[00:20:46] Will Sanchez: Because as you know, careers come and go pretty quickly. Uh, Dr. Garcia, say bye to the fans. Peace out guys. Remember vertical, vertical, not horizontal, and don't have Edward Scissorhands nightmares. [00:21:00] Peace.
Audio Transcript
We Are The Champions – 2024 Olympic Edition

Will Sanchez: Dr. Garcia, welcome. I want to welcome everyone to Sports Doc Talk. I'm Will Sanchez along with our orthopedic sports medicine surgeon, top doctor, you name it. It's great. I'm already rambling. We said, Oh, there's not going to be an hour. It's not going to be an hour, but I'm rambling. We're going to talk Olympics and Olympic injuries, and we're going to get into all of this stuff, but we have our gold medalist top doctor right now winning it every single year.
[00:00:45] Will Sanchez: Dr. Grant Garcia. I know I'm blowing smoke right now, but listen, it's summertime. We have the Olympics before we get into all that. How are you doing? How are the kids doing? Does everyone having a good time this summer?
[00:00:57] Dr.Grant Garcia: Yeah. Summer's awesome. You know, usually [00:01:00] summer's not super busy, but this year for some reason, everyone's enjoying sports.
[00:01:03] Dr.Grant Garcia: I think it may be the pre Olympics chaos that happens. Um, and now we're gonna have that post Olympic chaos. You know, everyone's gonna start signing up for swimming. And track and field. That's right. You know, soccer. Uh, you know, we get, the swim team gets like triple the volume after they finish, see the Olympics and you see Michael Phelps and now you see all the new swimmers going on there.
[00:01:24] Dr.Grant Garcia: So it'll be cool. But yeah, summer has been good. We finally got some eighties now it's back down to 66. I don't know what's going on, but we'll figure it out. Somebody will figure it out.
[00:01:32] Will Sanchez: It's only a couple of days. The Seattle dude, we're such complainers.
[00:01:37] Dr.Grant Garcia: We waited months for this.
[00:01:39] Will Sanchez: Yes, we did. And listen, before we go on, let's give a quick shout out to the recovery shop.
[00:01:44] Will Sanchez: Uh, Dr. Garcia, I'll tee you up for that one there. Talk a little bit about the recovery shop.
[00:01:50] Dr.Grant Garcia: So these are our sponsors, uh, big thank you to them. Uh, I love this stuff. You guys, you know, reach out to me, reach out to the recovery shop link above. Um, this is really good [00:02:00] for the patients. Your patients are asking me, I had someone today came in asking me, what can they do after, after their surgery?
[00:02:05] Dr.Grant Garcia: What extras can we, do we offer? You know, they've been hearing about the standard stuff, but like, you know, the nice machine, uh, recovering nutrition, uh, you know, the reboost machine, all those things they off, you can, we can offer them that, you know, you normally can't get, uh, and this allows you as a surgeon to offer them to your patients kind of in a one big bundled, you know, option.
[00:02:24] Dr.Grant Garcia: They can see it all there. And what's really nice to is just got kind of tired of telling people, you know, go to Amazon, buy this brace, buy this aftermarket thing. Instead, I can vet it. We can put it up there and it can be really helpful for the patients. So for patients, you can reach out and find out who's dealing with the recovery shop.
[00:02:39] Dr.Grant Garcia: But really, for surgeons, it's really the key is because it allows your patients to get everything quick access and good quality items. Uh, so I strongly recommend, uh, feel free. You can reach out to me on my website, on the sports doc doc website, or reach out directly to recovery shop. Again, there's no, you know, benefit to us if you go from any of those links.
[00:02:56] Dr.Grant Garcia: Uh, so do whatever works for you. Uh, but hopefully, uh, it'll be work for you. [00:03:00] So. Thanks guys.
[00:03:01] Will Sanchez: Yeah. And for those that are listening to this, uh, shop recovery. net, or you can find it on our website at sports stock talk. And what's great about that. And we're going to let this go in a second, but you mentioned it, right?
[00:03:12] Will Sanchez: We've been talking about the nice machine. We've been talking about rebless for, I don't know, for the last year, probably longer. So this just kind of, you know, just validates all the things that we've been talking about. And, uh, the benefit is, um, the patients. So we just want to give a. Quick shout out to the recovery shop and thank 'em for, uh, being a partner with us.
[00:03:33] Will Sanchez: And more importantly, uh, they're there to assist the recovery of the patient. Listen, it's Olympic time, baby. The Olympics have started the, I I hope no one in my job is listening, right? So I bet I had a really busy week. I had a bunch of shows. We did all these shows, and then I've been working from home and I gotta say, I got the Peacock app going.
[00:03:55] Will Sanchez: I've got, it's called the gold, the gold channels, like the red zone, the gold [00:04:00] zone, and they had the red zone guys on there doing this, like the octo box. And we've got gymnastics and volleyball and I'm going bananas over here. And I'm trying not to spill the beans because of in the chat with the team, they're going to know that I'm watching the Olympics, but I've been so excited about the Olympics.
[00:04:19] Will Sanchez: Have you had a chance to watch any Olympics going on?
[00:04:22] Dr.Grant Garcia: I watched a little bit of them, but I need to do this. I clearly am working too hard. I need to get on your ring . You do. Even though I know you work so hard, I gotta get the gold box, whatever it is, with the, we're doing, do Peacock. It's a great idea. I watched
[00:04:34] Will Sanchez: the Peacock app, man.
[00:04:35] Will Sanchez: I, I got it last year for the football season. They, they tried to trick us into watching the playoff game and then I got a great deal and I was like, ah, whatever. I'll pick it up. And now, I mean. All of the games are on it. So totally worth it. And by the way, you know, you know how we do, right? We usually do some stats, especially when it's just you and I, right?
[00:04:53] Will Sanchez: When we have our gas, don't worry about it. We're not doing trivia yet. We're [00:05:00] not doing trivia yet, but we'll give you the stat, right? So, um, the 2024 summer Olympics in Paris, right? They have the surfing competition in Tahiti, which is 9, 750 miles away from the host city, which makes it the farthest distance between Olympic and event and the host city.
[00:05:23] Will Sanchez: So for those that don't know where Tahiti is, it's in the French Polynesia and it's super far. So you're watching the Olympic at night and then you've got surfing going on during the day. Uh, there's been some really cool photos out there. And I think I'm really jealous because I don't want to surf because I'm not messing with those waves, but I can get a chair and some sand and a cooler, uh, maybe a little sunblock and a sand castle somewhere.
[00:05:48] Will Sanchez: That's probably my speed right there. So when I look at everybody at the beach, that's kind of where I'm wishing I was. [00:05:53] Dr.Grant Garcia: I think you would enjoy it. We were just in, we went to that spot about a year and a half ago. Uh, but you know what [00:06:00] that way, you know, that area is called something of skulls. Not really sure that that what they didn't say.
[00:06:07] Dr.Grant Garcia: I just read an article on it is the, uh, I actually have a few stats today. I'm going to school you. So the last time they had an Olympics and there was an event that far away was equestrian in Australia because they can't have such a long quarantine. So they can't have the horses actively in Australia doing the competition.
[00:06:27] Dr.Grant Garcia: So they did it in. somewhere I think in Scotland or in Londoners or in England somewhere. Yeah. And so that was the last time this has happened. But what's super cool is, you know, just the ability that they're doing this so far away. Um, but the waves are so dangerous there that like people have died.
[00:06:44] Dr.Grant Garcia: There's multiple deaths on this wave that we're doing. So this is, this is just insanity. Um, but you know, they, it's a, that place is beautiful and I hope they get a little, we know we might be finding some of those athletes stuck in Bora Bora for a little while. Unfortunately.
[00:06:58] Will Sanchez: Yeah, yeah. Quote unquote, [00:07:00] unfortunate.
[00:07:00] Will Sanchez: And listen, here we go. We're going off the beaten path already. For those that don't know, Dr. Garcia is a maniac when it comes to planning his vacations. So we need to find a section at sports doc, talk. com where Dr. Garcia can share. He has an itinerary plan out my next vacation. I'm just going to tee Dr.
[00:07:23] Will Sanchez: Garcia up because he's going to tell me where to go. When to go, whatever we need to do. So I'm pretty sure you should at least post the Tahiti one because you probably have a 23 page document there for your travels. So can we get that on the website?
[00:07:39] Dr.Grant Garcia: Dude, seriously, you're rigged. That's my best kept secret.
[00:07:42] Dr.Grant Garcia: Nobody knows about this. I'm shouting it out. It's tremendous. Totally unlocked it. Yeah. My partners steal my spreadsheets for my trips. You know, my friends steal my spreadsheet for my trips. But listen, the audience needs to know, I vacation like I do my surgeries. I only go, I go all out [00:08:00] making sure I do the best possible job.
[00:08:02] Dr.Grant Garcia: And I don't, there's no chill mode. It's everything, everything we plan, plan to the T, make it perfect. Um, and it's fun. We like to do it wild. I like to not, I'm not, you've already seen, we've seen my surgeries. We like to do, you know, there's not a lot of repetition. So anyhow, so that'd be another show. You already got enough information out of me on that one.
[00:08:21] Will Sanchez: No, no, we're, we're, we're. That show will probably be a four hour show. We'll do four parts on all of the, the planning that goes into it real quick before we move on. See this, this we're off the tangent. Where are we? 10 minutes in eight minutes in a, does your wife love it? Or is she like, okay, this is your over planning.
[00:08:40] Will Sanchez: Like there's a delicate balance. What's, what's the deal? Because I know when we try to plan things out, there's a delicate balance. We're like, okay, we just, we overloaded. that the schedule or we under load it. What's that? What's that key balance? And how does your wife feel about the way you go about planning these trips?
[00:08:58] Dr.Grant Garcia: So I usually catch [00:09:00] her off guard. That's the key. So she's tired at night. She's had too much of the kids and I'm like, Hey honey, do you want to go to Vietnam? And she'll be like, yeah, yeah, sure, sure. And I'll be like, she said yes. And then she wakes up and the trip's fully booked for her. So that is a positive.
[00:09:16] Dr.Grant Garcia: We've started doing conversations before, like a few weeks before. So she knows where we're going. Cause a lot of times she's landed and she's like, I don't really know where this is. Like, you know, there's certain places that we have, what's the next step we're going. So. You know, most people, it's the, it's funny, you know, that's the, because of my job, they think that I'm like, not the vacation guy.
[00:09:33] Dr.Grant Garcia: So it's the, it's the exact opposite in our family. Like she likes it, but she's obviously stressed. She's be honest with you. Her job's harder than mine with the two little rascals. So, you know, it's the, it's fun, but yeah, we do, we have, it's a good time and she likes it, it's just, it becomes intense sometimes you're tired after the vacation, but then the memories are worth it.
[00:09:51] Dr.Grant Garcia: So.
[00:09:51] Will Sanchez: All right. Well, you're apparently you're the Olympic champion of planning. Speaking of another Olympic champion, that is, I mean, she's to [00:10:00] me and you know, I'm going to ask you who is your top Olympian? Uh, for me, I have Jesse Owens as one of the top Olympians ever because of not only him winning, but at the time that it happened, uh, where he did it, uh, the circumstances that like, to me, it just, I put it under a much bigger umbrella and I have a couple of others that fall under my, these are my goats.
[00:10:28] Will Sanchez: But before I continue with that, who, who is your goat when it comes to Olympic games and what you've experienced in your life?
[00:10:38] Dr.Grant Garcia: So again, um, Uh, there are a lot of ones that stand out, but I, I, I mean, I'm kind of biased, man. I'm a swimmer. So you know where I'm going with this.
[00:10:47] Will Sanchez: Yes, I do. You got
[00:10:48] Dr.Grant Garcia: Michael Phelps.
[00:10:49] Dr.Grant Garcia: I mean, to have a swimmer that's, I mean, I was literally watching, you know, in prep for this show, we were looking up different injuries and trying to see previous injuries and they show first pitches and it's [00:11:00] like Michael Phelps, like all talking about Michael Phelps, you know, he, how can you rock a ponytail and be so cool still?
[00:11:05] Dr.Grant Garcia: Yeah. It's just so impressive. It looks good. You saw him out there, right? But that's what, but that's what I'm saying. It's not that common that you can do that. And he pulls it off because he's Michael Phelps. I mean, he's the most famous swimmer and probably one of the most currently most famous athletes that's not professional, like professional swimmer, but he's not like LeBron James, right?
[00:11:24] Dr.Grant Garcia: He doesn't play in the NBA. Yeah, he's not still active. He's at every Olympics hosting. Uh, and he's, I mean, they said that, you know, there was a huge article on this insane, basically, like. The U S is, is, is thirsty for another Michael Phelps to make the Olympics cool again. I mean, he's good. There are a lot of good athletes out there, but he just was a different, it was a different animal, right?
[00:11:45] Dr.Grant Garcia: There's the, I can't remember the guys, the French guy's name, but they're like, yeah, we have a new Olympic, we have a new Michael Phelps and he doesn't swim for the U S I'm like, that was like the worst possible line you could do, you know?
[00:11:56] Will Sanchez: Swimmer. I mean, you know, the, it, it all goes [00:12:00] through waves of the dominance, but you know, um, another person that is.
[00:12:05] Will Sanchez: and by far she is the best know, when you look at th Mary Lou Renton's, I mean out of the water and that
[00:12:19] Will Sanchez: When you're doing tricks in the air that no one else has done and you have so many things named after you, uh, that alone puts you in a whole other category. Um, she's often running and by the time we air this show, she's going to be competing, I believe, in six different events. She did sustain a calf injury during her warm ups at the Paris Olympics.
[00:12:45] Will Sanchez: Um, what are some of the concerns? When it comes to an elite athlete that is loading that muscle, you know, what's something that's really concerning to you when you hear calf injury? Because when [00:13:00] I hear calf injury, I get worried about a whole bunch of other things, not just maybe I'm having some tightness or some soreness.
[00:13:07] Will Sanchez: What are some of your concerns?
[00:13:09] Dr.Grant Garcia: Well, I mean, you're going to see this a lot in this episode. We talk about All the spectrums, right? Um, calf injuries are nasty. I mean, they're one of the most annoying nagging injuries. I mean, we've talked about hamstrings before we talked about quad injuries, uh, and you don't get as much in upper extremity, you know, gymnast, maybe, but you know, they don't get nearly the same injuries you'd think.
[00:13:29] Dr.Grant Garcia: And they get a lot of these lower extremity because they're, because they're having to land at such high velocity, right? Like, I mean, if you look at the height they're going from and they're landing and then they land in an end point. Right. So that's like to drop that and not blow your, you know, blow out your Achilles as you land, which we'll talk about happens, uh, is pretty impressive.
[00:13:48] Dr.Grant Garcia: And so the patients that I take care of that have these calf injuries, they're usually not surgical. I mean, we've talked about many football players. This has come up a few times on here talking about these calf injuries, but they're just really, [00:14:00] really good. really nagging and they hurt. They hurt a lot.
[00:14:04] Dr.Grant Garcia: I mean the most of my patients are coming in with a calf injury. They're limping, they're walking weird. Now again, I'm assuming she wasn't had didn't have a really bad strain. I mean, I know she's tough, but probably a grade one. And again, for the audience, there's usually three grades of these tears. You know, again, there's grade one, which is just a little sprain grade two, probably hematoma, maybe.
[00:14:24] Dr.Grant Garcia: which is some blood, maybe a more of a split. And then you have like a full on rip tear, probably not a grade three, probably a grade one. Again, also depends on where it is, right? We could, you know, we're not going to show that other picture in a minute, but basically you have the muscle, then you have the muscle tendinous junction and you have the tendon.
[00:14:40] Dr.Grant Garcia: The tendon is the Achilles tendon. So you can see how this all links together. Yeah. But you can see when they wrapped her, You know, they wrap her so tight that basically she's not even contracting the muscle and what they're trying to do with that is to get it so the muscle stays in put so that when she's landing, it's basically not contracting, but she then loses her spring force.
[00:14:59] Dr.Grant Garcia: The crazy [00:15:00] thing
[00:15:00] Will Sanchez: she does not lose her spring force. And what it's wrapped up. And it doesn't affect her. Uh, it, she's absolutely amazing. I I'm sorry to cut you off there. I think
[00:15:11] Dr.Grant Garcia: that she's probably good enough to do it with one foot. That's why. Yeah. You know what I mean? Well, we've talked about this before, right?
[00:15:17] Dr.Grant Garcia: Like it's like. Um, some of my patients ask me about professional athletes and they're like, well, what, how did, what did they get? I'm like, well, just so you know, like I've seen some of these athletes surgeries and like a lot of the surgeons are great. We've talked about Neil Altrosh, amazing surgeon, right?
[00:15:30] Dr.Grant Garcia: Like it's insane article. We have to hold an episode just on that article. We just read in the New York or was it New York times or something incredible, but basically these elite athletes. Even if they don't get a great surgery, and I'm not saying they do always, I'm not saying that they don't, but if they don't get a great surgery or they don't get a great, uh, treatment, they still can perform better than average.
[00:15:50] Dr.Grant Garcia: I mean, when I take care of these high level athletes, and if let's say sometimes you come in and you know, these have percentage success, right? They're just don't [00:16:00] have that same issue. It's just not the same because they're able to overpower whatever they need and they're able to do it. There's a reason that they're elite.
[00:16:06] Dr.Grant Garcia: And you're talking about the most elite. person. Right. So what does it take to get that level? And then the problem is that she's not even what that take to get that level. She's significantly above the rest of the world, right? She has tricks named after her. She's going for another trick that we've never seen before, right?
[00:16:24] Dr.Grant Garcia: That's that she's going to rename, name another one of her tricks. Um, And so she doesn't even need to be at a hundred percent to win.
[00:16:33] Will Sanchez: Let me ask you about this. Right. And once again, we are recording this. If we were going to go live, we would need to get this out in the next three hours and 27 minutes because, uh, Paris is, it will start rocking and rolling at midnight, uh, Pacific time, uh, when they go.
[00:16:53] Will Sanchez: So this is going to be, you know, a little bit later and halfway through the Olympics when we released this, but Her [00:17:00] dates and the reason I'm bringing this up is what's your concern? If you're the personal trainer and you're like, I'm in charge of the most important calf at the Olympics for gymnastics, July 30th, women's teams final, August 1st, women's all around final, August 3rd, women's vault final.
[00:17:21] Will Sanchez: The fourth uneven bar, the fifth balance beam finals and the fifth floor exercise finals. That is six. Events within five days or six days and the last day she has two Major events with the balance beam and the floor exercise final What are you doing to keep that calf? not only when she's going to perform but before https: otter.
[00:17:53] Will Sanchez: ai[00:18:00]
[00:18:00] Will Sanchez: monumental beating within that time frame.
[00:18:03] Dr.Grant Garcia: I mean, you're doing everything right. They might even have to be thrown in PRP. They might have been throwing some stem cells in her during the time they may be doing something called shockwave. We've had a few of the players that come in. We had a couple high level soccer players.
[00:18:16] Dr.Grant Garcia: A couple of high level basketball players. We do the Seahawks and they come in and they get this thing called shockwave. And so they do it like when they get like, when they have injuries like this and it sort of breaks up the scar tissue and kind of relieve some tension there. So she may be doing something like that.
[00:18:29] Dr.Grant Garcia: There's probably things I've never even heard of that. She's getting treatment on there in Europe and remember she's in Europe, right? So they probably have some other things that they don't even have here in the U S that they can offer her. I mean, she's getting smashed with treatment right now. I mean, there's just no way that she's just sitting around doing nothing.
[00:18:44] Dr.Grant Garcia: And also you're, you're forgetting to mention, which again, you, you're bringing up the most important parts, but she's warming up also, right? Like she's just not going cold Turkey and doing those things. And she's going to keep herself warm every day. She's going to do routines every day. You know, she may be chilling out more than average because she's injured and she doesn't [00:19:00] want to get more injured and she wants to save it for the actual events.
[00:19:03] Dr.Grant Garcia: But I mean, those are not, those are still like a few days away. Right. Like we're not talking about like, this is going to be over in a day or two. Right. You're talking about six events over a period of time. So yeah, I mean, it's, they're doing everything possible and they're probably consulting, they're probably calling.
[00:19:19] Dr.Grant Garcia: They probably have all these people involved in this. This is not a single person. um, treatment option. Yeah. And there, and there has probably been so many people involved in this, which is always a really important to understand like these, even you have these team physicians, they're, they're top of their game.
[00:19:34] Dr.Grant Garcia: You know, I took, took care of a player that had seen Ella trash and then flew to see somebody else. And, you know, it's just amazing to hear their stories when they're like, Oh, well this guy operated me, but I flew to see three other people because he's like, I want you to get trekked by three people before I do your surgery.
[00:19:47] Dr.Grant Garcia: Like these are the best docs in the, world, if not country. Um, and they're still getting these extra opinions because all of us want to make sure we do the right thing for the player or for the patient.
[00:19:58] Will Sanchez: Um, last thing before I move [00:20:00] on, you know, we've heard a lot of different things right before it was, you know, um, the rest and the ice and things like that.
[00:20:08] Will Sanchez: And it seems like we're getting more information now about compression and maybe going away from some of the ice treatments when it comes to, let's say it's a grade one calf strain. What is that treatment? Is it focusing on compression or it's just besides everything else that you mentioned, but just, you know, what, what say maybe go to when she's at the hotel, she's already had her treatment, but they still want her to quote unquote treat it while she's.
[00:20:36] Will Sanchez: Relax at the hotel room at the end of the day. What is she doing there?
[00:20:40] Dr.Grant Garcia: I mean, there's, they're probably doing massage, they're probably doing graft and they're probably doing 24 seven
[00:20:46] Will Sanchez: everybody. It's, it's not a, you know, I don't think, I
[00:20:48] Dr.Grant Garcia: mean, I just don't think she's sitting there icing her leg. I mean, the problem is that ice is really good for like a sore knee, right?
[00:20:53] Dr.Grant Garcia: Like swelling, intraarticular swelling. Uh, I, I, as a, [00:21:00] a layman athlete, recreational athlete, you know, despite being an orthopedic surgeon, I would ice my leg, but that's just, cause I, you know, I don't have Even with all the stuff that I see and do, I don't have access to the treatments that she has, nor do I have the time to go get that stuff.
[00:21:15] Dr.Grant Garcia: And so as a result, I would just do the basic bread and butter, but that's not what she's getting. I mean, she's probably having, she probably has her own nice machine in the room. You know, she's probably getting something we haven't even heard about, you know, there's more than shout out to grant. I mean, I just think, uh, I, we can't fathom the type of stuff that she's probably having right now, but you know what?
[00:21:36] Dr.Grant Garcia: The best part is maybe we're completely wrong and maybe she's just so good. Yeah. That she's getting treatment and she's surprised
[00:21:43] Will Sanchez: by she's a, she's, she's a,
[00:21:45] Dr.Grant Garcia: maybe all this stuff. She's maybe she, maybe she watches the show and she says, these guys are such, we have, I've gotten no treatment and I'm just going to win regardless.
[00:21:55] Dr.Grant Garcia: I'm rocking my PlayStation. That's the fun part of the show where predictions are wrong. Yeah. Do our best. [00:22:00] We tell everyone, but it's, it's, uh, but you know, like LeBron James though, like he probably got like a hyperbaric chamber he brought with him. So I know he's getting treatment.
[00:22:08] Will Sanchez: And he likes his red wine as well.
[00:22:10] Will Sanchez: So maybe it's a little combination there between getting his treatment and a and a off day with a nice, uh, nice glass of red wine. We'll, we'll stick with the gymnastics. Uh, unfortunately these are serious injuries with Sky Blakely and Kayla, uh, Dello, uh, with their. Achilles injury, really rough. Um, I mean, Achilles injuries, right?
[00:22:33] Will Sanchez: That that's all we have to pretty much say, uh, during the U S Olympic uh, gymnastics trials for, uh, for Kayla, you know, I mean, you guys are seeing this,
[00:22:43] Dr.Grant Garcia: it's like the, when you think of Achilles injuries, you know, in no offense to the world, but we have, you know, it's usually. 30, 40, like we don't, the high level athlete injuries are a different animal, right?
[00:22:56] Dr.Grant Garcia: Yeah, they're just, you know, you've seen Aaron Rodgers, but Aaron [00:23:00] Rodgers wasn't 25 when he got his injury, right? There's NFL players that get it, but to see two 20
[00:23:05] Will Sanchez: years old. And we're talking about high level athlete.
[00:23:08] Dr.Grant Garcia: These are really young. Not that common to see this injury, um, in every day. I mean, we see people in their mid twenties to thirties tear there, but it's usually that like high twenties.
[00:23:22] Dr.Grant Garcia: We always call it the weekend warrior, right? Like the dad or it's more men. Actually, this is different. Obviously we're talking about two female athletes here, but it's usually higher precipitants of men because. They tend to do stupider things. That's me. Tend to wasn't directed at you. Will, but
[00:23:37] Will Sanchez: yes, it was 100%.
[00:23:39] Will Sanchez: Just because you're nice about it does not mean it wasn't directed weekend warriors doing dumb things and busting their, this is all
[00:23:47] Dr.Grant Garcia: about, I'm just trying to make fun of you the entire time without anybody knowing on the show. So I, uh, so, you know, so it's generally the population's generally I said, it's weekend warrior.
[00:23:57] Dr.Grant Garcia: Like I've had friends like that, you know, in the late thirties, early [00:24:00] forties, tear their Uh, Achilles and then talk about repair, which we will in a second. Um, but to have young, I mean, one of them was what, 16. Or something or like it, she's 20 years old and the other one, I can't remember how old she was, but these are not very old.
[00:24:15] Dr.Grant Garcia: Anyhow, so these are young, young athletes, but what, remember what we said before, this is like jumping off a building, right? Like they're going, look at the height that they go. Like we, we never get to experience that. Like you would never fall at that speed. And it's also a rotational component, right? And then they have to immediately stop on a dime.
[00:24:33] Dr.Grant Garcia: And that's usually what happens. It's that abrupt halt. That's what gets any of our things. Like if you think about. We see biceps tenon tears, you know, it's not like the guy is just lifting and obviously let's go. It's just all of a sudden goes into an isometric, which means that your muscle has to hold that same strength without moving and your tendon gives out because it's either your tendon or your bone snaps.
[00:24:55] Dr.Grant Garcia: Now, if they were younger and they were like in [00:25:00] 16, 14, they're 19 and 20
[00:25:03] Will Sanchez: just to let that's 19 and 20.
[00:25:05] Dr.Grant Garcia: That's we're talking about really young. This is a pretty devastating injury. And we've talked about this before on the show. We've seen examples of this. Um, and you know, you can see this is, this is a long road.
[00:25:17] Dr.Grant Garcia: I mean, they're out for a year and are they the same? I mean, they're going to have to rely on that power spike land. Uh, you know, maneuvers with this type of Achilles is just, it's a really devastating injury. And, but again, the nice cool thing we've seen now is it used to be, you know, we saw many baseball players that are earlier on, you know, 10, 15 years ago, get this and it would take them two years to come back and they never be the same.
[00:25:44] Dr.Grant Garcia: And now we've seen some players come back from it and they've done well, you know, and we'll see how Aaron Rodgers begin. Aaron Rodgers is not, he's a great player, but he's not the antithesis of like. A hurdler or a gymnast, right? Like he could sit in the pocket. He was never [00:26:00] known as a high, high impact player, right?
[00:26:03] Dr.Grant Garcia: Like going for big runs, doing dives, jumping and things like that. So like, he doesn't need to be, I mean, you saw him, he was at four, like six weeks, he's throwing the ball better than most quarterbacks can do. Right. He doesn't really need that Achilles to do the things that he does compared to these. He's gotta move in the pocket.
[00:26:19] Dr.Grant Garcia: Yeah, exactly. So Will's gonna show this. I know the audience. I don't want him to be too grossed out, but it's kind of interesting to see like kind of the old and the new way. Um, really briefly, just so the audience can see what it's, yeah. So I'm gonna show, show this.
[00:26:31] Will Sanchez: So give everybody heads up. I'm going to show an Achilles rupture.
[00:26:34] Will Sanchez: It's a little gross. If you're not used to it for Dr. Garcia, he has this with some peas in a salad. It's fine with him because he lives it every day. Uh, for those that are listening on our podcast, please is a great segue to check out our YouTube page. Cause if you want to see our faces and get grossed out by the next slide, then please, uh, check us out.
[00:26:54] Will Sanchez: So let's talk about this, uh, Achilles rupture here.
[00:26:58] Dr.Grant Garcia: All right. So again, [00:27:00] audience can see. So these are two the same. These are surgeries. So if someone tells you they got their Achilles repaired, this is actually the same surgery. You can obviously see there's a difference here. We've had Dr. Anthony on here.
[00:27:13] Dr.Grant Garcia: Will's undergone one of these. Thankfully, Will's undergone the one on the right. If you're looking at the screen, um, but so the one is an open repair. And again, that's a little more of an accentuated repair, but that's what the Achilles looks like when it snaps. And you can see that the white is the tendinous portion, and then it's sewed back together and you want to make sure you're sewing it.
[00:27:31] Dr.Grant Garcia: So you don't have a lot of knots on the outside or anything else, right? And the issue with this is obviously wound infections and things like that on the right. And now they don't have the little holes on the bottom for the speed bridge, but this is what Aaron Rogers got. And again, usually it kind of goes, this is a good one here.
[00:27:46] Dr.Grant Garcia: Usually you might go a little bit lower with your incision. You might go different orientations, but again, it's small, percutaneous, and then you just fix it down to that bone. That's kind of the newest hottest way of doing it. And that's the speed bridge you guys keep hearing about. Down into
[00:27:59] Will Sanchez: the [00:28:00] heel area, right?
[00:28:01] Will Sanchez: That's what, you know, As far as when you say the bone and the suture is connecting that
[00:28:05] Dr.Grant Garcia: like blue mark, as you can see, that's where the heel bone is going to be going roughly. And the reason is you can see here, 10 attendance, great. But what the Arthrex team and other people have figured out is that, you know, usually it actually tears a little bit lower and when it tears lower.
[00:28:21] Dr.Grant Garcia: The tendon that's connected to the heel bone, which is the lowest part. And again, I'm sorry, I can't show you because I can't point. Um, it, uh, it's really not good quality. And what we've seen is there are people that can be treated without surgery. There are people that are older or people that are really patient or okay with maybe not the high impact power plays.
[00:28:39] Dr.Grant Garcia: And so they keep their, they keep their ankle like this and then slowly over time. Now, again, for an athlete, if it was me, I'd get it fixed. Right. I want to get back faster. I want to, I don't, I can't sit in the OR for 10 weeks in a boot and be okay with it. And so you want to go a bit, you want to go back quicker.
[00:28:54] Dr.Grant Garcia: And so by having this sort of enhanced bridge and then being able to fix it to bone, it's stronger. Like if you can get bone to tendon [00:29:00] healing, it's always better than the tendon to tendon. Dr. Justin Marchegiani, M. D.: Less scarring. Evan Brand, M. D.: Faster recovery. Dr. Justin Marchegiani, the whole purpose of this is.
[00:29:06] Dr.Grant Garcia: So, you know, so they're probably undergoing that. I'm hoping they're undergoing the right one which is the percutaneous. I can sure bet that they'retheyone of them's probably gonna be seeing Dr. Elitrosh sometime soon. Dr. Justin Marchegiani, You know, we've already seen he's the master of everything. Iwe need to have an entire episode on him.
[00:29:20] Dr.Grant Garcia: Uh Dr. Marchegiani, M. D.: But anyhow, so thesethat's what's gonna be going to go in. It's gonna be a long recovery. And, you know, there's going to be their different ups and downs, but, you know, hopefully they're still young and hopefully we can see them again in four years and, uh, Los Angeles, right?
[00:29:34] Will Sanchez: Yeah. And, you know, before we move on, as we mentioned, right, 19 and 20, um, you know, one of them, uh, Kayla.
[00:29:44] Will Sanchez: Was part of the championship team last year and pretty sure was expecting to go and compete with her teammates and try to bring home a gold for the US gymnast uh, uh, gymnastics [00:30:00] team, you know, and. We talk about injuries. We talk about knees and Achilles and things like that. But what that mental preparation, some of the concerns are when you have these young athletes that this is possibly their career, even though they're young, we know that gymnastics is Obviously, Simone is 27.
[00:30:20] Will Sanchez: She's different. She's, you know, she's LeBron, you know, she's, she's, she's on a whole other out of our galaxy. But for a lot of these, you know, athletes, their careers, you know, end at an early age and, you know, if as a doctor, as someone that, you know, knows this, what are some of your concerns with the mental status?
[00:30:42] Will Sanchez: And what is something that you can do or encourage the patient to do when you know that They're going to be rough days. You are laid up, you're a mobile, you're watching on TV, your dreams, you know, you're not, you know, sitting there for a week or two, you're going, this is a [00:31:00] long recovery. What are some of your concerns as a doctor?
[00:31:04] Will Sanchez: And if you had to share with some of our listeners, what do you recommend if you're. Struggling mentally with something like this.
[00:31:13] Dr.Grant Garcia: I mean, we're going to need to have an entire episode on this. This is a great topic. I think the mental health of recovery is humongous and it's completely not talked about.
[00:31:23] Dr.Grant Garcia: If you watch our previous episodes, this probably comes up frequently and I made it. It wasn't a joke, but I made a point that I'm basically two thirds surgeon and one third therapist, even though my wife thinks that's funny because she would say you're not a very good therapist, but nonetheless, yeah, she's biased.
[00:31:40] Dr.Grant Garcia: She's biased. That's true. So anyhow, so there's a lot of therapy, right? I
[00:31:44] Will Sanchez: don't want to get in trouble here, but anyway, no,
[00:31:45] Dr.Grant Garcia: no, we're good. We're good. So she's, so basically, you know, there is, this is just, this is, I'm just dealing with everyday athletes, right? I mean, we had paid, we had some young kids today that came in that have, Meniscus tears we're gonna have to do surgery on and tell them, [00:32:00] you know, you're out five months, right?
[00:32:02] Dr.Grant Garcia: Like everything that you wanted to do done. You're stopping. Yeah baseball player Tommy John. You're done You're you know, that's a junior season you had it's out. You're not doing it It stinks, right? You're telling the parents, you're telling the kids and there's, and it's just, you know, the surgery, that's the easy part, right?
[00:32:20] Dr.Grant Garcia: Like you go to sleep, you wake up, let me do my job. And then you start the recovery and you have pain for a few weeks and then you get back. And that's, I'm not trying to belittle the pain and the recovery, but that's the, I mean, will, you know, you've gone to this, I've undergone surgery, like the surgery part sucks, but like, that's not the, that's not the hardest part.
[00:32:37] Dr.Grant Garcia: It's the mental part. Right. And so, and, and we're talking about like, Just being annoyed because we can't go play basketball or play with our friends. These are the people that have been training for this particular thing and they can no longer do it. And they're not pro athletes where they can be out for a year and still get paid.
[00:32:53] Dr.Grant Garcia: Right. Like, I mean, they're professionals, but they're not the same as these NFL players that don't have guarantees on their contracts and every, or these [00:33:00] MBA or whatever, and so they're going to need mental health coaches. I mean, we've seen it in shows. We've seen it in, um, you heard it on there. I mean, Simone Biles.
[00:33:09] Dr.Grant Garcia: Right? Mental health, the tipsies, all these other things, mental health is huge. And almost every athlete now has a psych, a sports psychologist that's available to them. And if you are doing athletics and you're having trouble with things, I would strongly, I mean, listen, this is not a athlete only issue.
[00:33:30] Dr.Grant Garcia: Right? Like there was a huge article on this for surgeons. I mean, we're put under in stream stresses sometimes in the, or you're dealing with athletes like this, you're trying to fix, you want to get them back. And if they don't get back, you feel sad. You're upset about it. Even though the success rate of some of these surgeries is 80%.
[00:33:46] Dr.Grant Garcia: That means 20 percent of the players that you operate on will not get back and there's absolutely nothing you can do about it, right? Nothing you can do about it. So it's the same thing with these, you know, they have to, and I think that this is important. I think that it's [00:34:00] completely underappreciated.
[00:34:02] Dr.Grant Garcia: And until recent with some of these athletes that have come out and said, you know, they have these mental illnesses use. No one wants to talk about it. It was considered sort of, which is sick to say is weak. If you came out and said you had the mental issues, if you said that you were having a tough time, but you know the worst part about this is it happens to everybody.
[00:34:19] Dr.Grant Garcia: It happens to, I mean it happens for the surgeons. It happens to everybody. You feeling feeling like you got to do better. You could do better on the next one, right? I don't remember. I don't remember like half my successes, right? Like I operate a lot of people. I take care of people. I'll don't, I can tell you right now, I remember every single one of the failures and you just, that's the same way they're going to be there.
[00:34:40] Dr.Grant Garcia: They're not going to remember the 15 competitions they won. They remember the time that they were sitting there on the couch with their Achilles recovery. And so I don't know, it's a long winded answer because obviously this is a little more personal clearly. Um, but the, uh, I think it's tough. Sports psychologist is important.
[00:34:56] Will Sanchez: Yeah. I think that's the big part because, um, [00:35:00] Right? Your surgery ends. You're like, all right, I'm going to rock this. I'm going to be gung ho about it. I'm going to get him. I can't write. And you, you just, especially if that you had that mindset, I'm just going to just go after it. Time is a mofo. You know, and you're like that for a couple of weeks, all of a sudden you start to feel it right.
[00:35:22] Will Sanchez: And you start to, you know, you're going through, even as you're doing things to try to benefit, eventually you're sitting there and you're like, man, this is, this is rough because sometimes not even yourself, but you, you see that it's affecting the people around you, right. If you know, if you have responsibilities, if you know, like for myself, when I got hurt, I see my wife doing all this stuff and, you know, and I can't do certain things and, and things like that.
[00:35:44] Will Sanchez: And all of this. Extra stress is falling on other people, and that's a whole other thing besides what you're personally going through. So, without going into, you know, so much as we already have, I think the point is that whether you're an [00:36:00] athlete or someone just getting surgery tomorrow morning, Be aware of that, you know, and, you know, reach out, get a support system, especially if it's a long term injury, because you're going to have some ups and downs and you want to have a support system there to kind of help you through that no matter how strong you are.
[00:36:19] Will Sanchez: I
[00:36:21] Dr.Grant Garcia: think, and I don't want to go any more because I think we're going to, I think, well, I've just added another topic for one of our podcasts. I wrote it right here. Look,
[00:36:27] Will Sanchez: people that are home, I wrote on my yellow pad. It says Mental health therapist as one of our next shows. So, so yeah, this will be a good show.
[00:36:36] Will Sanchez: I
[00:36:36] Dr.Grant Garcia: think the audience is going to love this one, but basically be honest with yourself. That's one to understand that everybody feels that way. You know, that's one thing I like to do in the office being like the girl before you was just upset. You know, the guy before you was upset that he had to go through this, like it, you're not alone, right?
[00:36:51] Dr.Grant Garcia: You're not even alone today. Right. Which is good. Um, and then I think the biggest thing you understand is that like, [00:37:00] is that you will get, you will get there if you persevere. And you have to be okay with different things. You've got to be able to have the options in your head, but it's hard. I mean, like you said, you're in isolation, despite, despite what you want to do.
[00:37:11] Dr.Grant Garcia: But, you know, we'll move on. This is going to be a great topic for another time. I think we could talk an entire hour on this, if not more. Um, and maybe you find a really good mental health sports psychologist to come on the show at some point, we will get,
[00:37:23] Will Sanchez: we will get one on. And, uh, anyone listening, I want to come join the show and be a part of our show.
[00:37:30] Will Sanchez: Check us out, sports. talk. com. We have on our website, not only all of our podcasts, but great information, Dr. Garcia provides, we have transcripts of the show. So if you get tired of listening to my voice, you can just read what we're talking about. And more importantly, if you want to be a part of the show, on our webpage.
[00:37:52] Will Sanchez: You can reach out to us and if it all works out, we would love to have you. We've been blessed with some great guests already. [00:38:00] We're going to move on. We're going to go to your fun spot, your warm spot. ACL injuries. It's like ACL and shoulder injuries are like Dr. Garcia's favorite. I don't know. Maybe they're all his favorite here, but let's talk about secretly.
[00:38:13] Dr.Grant Garcia: They're all my favorite secretly. I do not discriminate against injuries. Everybody's
[00:38:17] Will Sanchez: allowed. Cameron Brinks. ACL injury. Uh, she tore ACL just a month before the Paris Olympics. Um, really a blow to her, uh, team. And I mean, And maybe we'll get into this in a second here, having this ACL injury coming out of Stanford, graduating one of the best players in college rebounds points blocks.
[00:38:45] Will Sanchez: She was one by far, right? Everyone talks about Caitlin Clark and Angel Reese, Cameron Brink. Was a superb college athlete. It was going to have a tremendous rookie year for the Sparks. Um, let's talk about this ACL injury [00:39:00] and what this involves. We're talking about another young athlete here. What does this ACL injury involve?
[00:39:08] Will Sanchez: Just talk about that as, and then we'll get into the recovery process.
[00:39:11] Dr.Grant Garcia: Yeah. I mean, We've all heard about this with all these players. I mean, ACL keeps coming up on this thing. We talk about all the different surgery options she has and everything else. But again, she tears her ACL. You can see there. It's one of the most commonly torn ligaments.
[00:39:25] Dr.Grant Garcia: You it's the one you hear about all in the news, um, with these athletes. So she's going to tear this. She's going to be out, you know, seven, eight months. Uh, she'll get a, probably a reconstruction and there's other fancy things we talked about, but not an athlete at this level, uh, yet. Um, yeah. And again, the interesting thing though, is it's women's basketball.
[00:39:43] Dr.Grant Garcia: So we haven't brought that up as much. We've had a lot of NFL players we've talked about. Um, and what, what people don't understand and what I see actually a higher amount is female athletes coming in with ACL tears. So female athletes are two to eight times higher. men. [00:40:00] And that's really important for people to understand because I do a lot of ACLs and I would tell you that this is very true and it's, it's really high in basketball, but the highest in soccer.
[00:40:12] Dr.Grant Garcia: And so a lot of soccer. So when soccer season comes, unfortunately it's a lot of, and it's young girls too. I mean, Cameron Brink, despite her being in the, uh, the WNBA is she's still young, right? She's just a rookie young girl. Yeah. Yeah. So again, And it's because of the way that it's not because they're female male, but it's because of the way they land, they landed more valgus.
[00:40:33] Dr.Grant Garcia: They have some rotation. They tend to have smaller notches, which means that's what the area where the ACL sits, it kind of impinges. And also women tend to be more at lack. So they tend to have more flexibility. And so that means that their ligaments are a little bit looser, um, but allows them to do other things, right?
[00:40:48] Dr.Grant Garcia: There are a lot more. Flexible. They can do things like that. But again, and it, and for Cameron Brink, who's so tall, um, it could have put her at more risk. But again, it's also just bad luck, right? Like people ask me all [00:41:00] the time. They're like, well, why did this happen? I mean, I have so many, a couple of my friends that were like insanely good skiers.
[00:41:05] Dr.Grant Garcia: They made it through their entire career. No ACL tear. Then they're 35. And Whistler and they fall and they tear their ACL. And they're like, why did that happen? I'm like, listen, it's just bad luck. So a lot of times we just can't explain why it happens.
[00:41:21] Will Sanchez: So the anatomy, the hormonal and the biomechanics of the woman athlete is slightly different than the male.
[00:41:30] Will Sanchez: And that does play a part, or at least the, the numbers or the stats or studies show that they tend to be higher in female when it comes to ACL injuries compared to male. Okay. Did I say that right?
[00:41:42] Dr.Grant Garcia: Yes. Yes. And what we also know is that because that information is important, it's important that teams and understand that you can also prevent these.
[00:41:51] Dr.Grant Garcia: So by doing prehab or by doing pre, you know, injury workouts, by learning, teaching females to not fall into so much valgus, [00:42:00] there's different things you can do to prevent it. Now, obviously someone like Cameron Brink has probably been doing that, right? Like there's no way that you get to that level and they're not preparing her to avoid her from getting injured.
[00:42:08] Dr.Grant Garcia: But nonetheless, for this is a This all of our shows segway into something different, right? Like we start off with the topic and then sometimes we go off the deep end and sometimes we go in
[00:42:18] Will Sanchez: a different direction.
[00:42:20] Dr.Grant Garcia: So any else? So as you're a swimmer,
[00:42:22] Will Sanchez: we go off the deep end.
[00:42:23] Dr.Grant Garcia: Dude, no pun intended. That's right.
[00:42:25] Dr.Grant Garcia: Uh, but anyway, all
[00:42:28] Will Sanchez: right. Very different. I think it's the only sport and I'm not, I'm not putting much thought to it. So someone's definitely going to correct me on this. Right. But college basketball. Depending how deep you go in right now, I was thinking about this with Caitlin Clark, but now even talking about this with Cameron, she played all the way through into the playoffs, March Madness, finished, got drafted and play [00:43:00] professional basketball.
[00:43:01] Will Sanchez: In a month, maybe five weeks. It's the same thing with Cameron, right? Played in the, in the tournament, had a full season going back to the beginning of the college basketball season, got a month off, probably less because it probably went right into practicing. You know, you, you get out of the tournament, you get drafted, you go right to your team.
[00:43:24] Will Sanchez: And then the game start up two weeks later or something like that. Um, right after the draft or, you know, a couple of weeks later after the draft, does that amount of playing and like I say, it could always go back to just bad luck, but the fatigue for a starting basketball player where you are clearly the best player in.
[00:43:45] Will Sanchez: Iowa for Caitlin Clark or Stanford like Cameron, where you are both have the bulk of the minutes and playing the most because that gives your teams the best opportunity to win. Having all of that basketball is going on. [00:44:00] Could that add to something like this happen? Or do we go back to, well, you're just kind of shit out of luck a little bit.
[00:44:09] Dr.Grant Garcia: I would say maybe I used to, would have to say yes. You know, the more low, the more, the quicker turnaround is there, but we're not talking about days. We're talking about weeks, right? Like you, most of us, like if you sit around on the couch for two weeks, like your body actually is worse, right? So I don't know if that quick turnaround is, I don't think in my opinion, I don't think that that's the reasoning.
[00:44:29] Dr.Grant Garcia: I think that the higher amount of games puts her at a higher risk to potentially tear their ACL. Right. And so they had more games in that season, but again, you know, Caitlin Clark didn't do it. So like, it doesn't mean that like, just, I don't know, there's a stat on that to show that that's causing that. I think if they're right,
[00:44:45] Will Sanchez: Cameron, uh, Caitlin Clark's a guard, we're talking about a, a, a taller, a center, right.
[00:44:52] Will Sanchez: Um, and you know, it all plays, but I like the point that you're bringing up a great point. It's the number of games, right? Please think about [00:45:00] it. If you think about her college career, I don't know what she did in the high school or AAU or anything like that, but by far at least her college career, she's played the most amount of games in a calendar year because she didn't end her bad, her college basketball season and then have that break or whatever she would do afterwards before the next fall, she went right into a WNBA season.
[00:45:25] Dr.Grant Garcia: That's true. And again, also the best players usually. Drive their teams to win. So they're usually probably finishing in the March madness also. So anyhow, I don't think it's, I don't think that's the exact reasoning. Um, it's always load management is always important. Uh, it depends on probably the players too.
[00:45:41] Dr.Grant Garcia: We've seen that too with football, right? Like running backs are more low management, wide receivers, other guys, you're not as worried about. So.
[00:45:48] Will Sanchez: All right, let's, uh, let's move on to a couple of the athletes, man. We just, I think we're just full of great news, right? Just talking about all of these injuries for these great athletes.
[00:45:58] Will Sanchez: So we apologize if [00:46:00] it seems a little bit morbid, but this is what we do. We talk about injuries and not only, you know, I mean,
[00:46:05] Dr.Grant Garcia: you don't need it. You don't need me to tell you about who won the gold medals. You go on the news.
[00:46:08] Will Sanchez: Yeah. And when you hear about the injuries, then
[00:46:10] Dr.Grant Garcia: you can come to us.
[00:46:11] Will Sanchez: Exactly. And we're still talking about the Olympics.
[00:46:13] Will Sanchez: Let's go. Uh, Shalise Jones and Alicia Monsoon. They had meniscus tears, uh, in their knee. Can you talk about the difference between a meniscus tear and tearing your ACL?
[00:46:26] Dr.Grant Garcia: Yeah. So can you pull that picture up again? That was good. So, uh, you know, different recoveries, different prognoses, they can come in. So first off, we've talked about this a few times, probably on some of the earlier episodes.
[00:46:39] Dr.Grant Garcia: So it might be good for us to rehash this again. Yeah. Problem you have is a lot of times with the injury report, you don't get information on the meniscus. Right, so they'll say patient the Cameron Brink tore ACL, but did she tear something else in that in the meniscus? And if she did that puts her at higher risk for other issues.
[00:46:53] Dr.Grant Garcia: You can see here that's the meniscus is the two cushions of the knee and then the ACL is in the middle. The ACL gets a lot of [00:47:00] publicity. It's kind of the sexy ligament. It's the most commonly torn one, but honestly the meniscus is way more common. If I would say like, even the last two weeks, I've probably seen like seven ACL tears and I've probably seen like 15 meniscus tears because the meniscus tears is more.
[00:47:14] Dr.Grant Garcia: The most common surgery we do is a meniscus surgery. So it's just way more common. Um,
[00:47:20] Will Sanchez: so that's a real quick scope for Shalise Jones, which is another gymnast. Her having this meniscus tear is this. Better or worse than the injuries that her other gymnastics, uh, teammates have suffered through.
[00:47:34] Dr.Grant Garcia: So that is a loaded question, which may go off on a tangent and I know we're running outta time, so we'll never
[00:47:39] Will Sanchez: run outta time.
[00:47:39] Will Sanchez: It depends on
[00:47:40] Dr.Grant Garcia: where the tear is. It depends on what type of tear it is. I run, run outta time
[00:47:44] Will Sanchez: already. Okay. I ires, sorry. It's because
[00:47:46] Dr.Grant Garcia: you and me do this. This is Okay. So, and then we'll talk about this, this crack that monsoon felt. 'cause this is a really interesting Oh, so basically. You have friends that have had meniscus tears.
[00:47:55] Dr.Grant Garcia: They go in there, they do a little cleanup. Yeah, that's fine. Those are sort of like the simple tears, little pair of [00:48:00] tears, little radial tears, but the tear that you're even seeing here, this is a radial tear. Those are kind of nasty. Cause when you take one of those out, that's equivalent to removing the entire meniscus and that's when you run into problems.
[00:48:11] Dr.Grant Garcia: Right. And we're going to go on one of these that's had problems. Alonzo Ball. This is exactly what happened to Alonzo Ball. Meniscus tear, cleaned up, which we're going to go into this in one second on Monsoon in one of the articles they talked about. And then, again, a problem. And then guess what happened?
[00:48:27] Dr.Grant Garcia: He developed a cartilage hole. And he had no meniscus left. So what was he end up getting? Which we have not talked about as the meniscus transplant, but he got a meniscus transplant and a cartilage transplant, which the meniscus was not announced until recently. They just mentioned the cartilage portion, which is a game changer for their whole procedure.
[00:48:44] Dr.Grant Garcia: And so, yes, it's uncommon, right? Lonzo Ball's the first NBA player to get this. It's one of those risks you have. So if you get a nasty one, it doesn't heal, and you get problems, they go down faster. Generally, the ACL. Players, if you can get [00:49:00] the ACL stabilized, they don't get that risk of arthritis as much.
[00:49:04] Dr.Grant Garcia: The meniscus one is a much worse thing if it goes. So basically, if it goes well for both, you're good. ACLs go well more often. The meniscus can heal. But the long term of the meniscus sometimes is increased arthritis a little bit more than the ACL. Does that make sense? That was trying to be as best I can.
[00:49:21] Dr.Grant Garcia: And again, it depends on what you have to do.
[00:49:24] Will Sanchez: That makes sense. And then for Alicia Monsoon, 2021 Olympian in the 10, 000 meters, she felt a quote unquote, I'm doing air quotes. If you're not watching, she felt a crack in her knee doing a run, which then turned out to be a medial. meniscus tear. So once you talk about the differences, that's when you hear that red
[00:49:46] Dr.Grant Garcia: thing
[00:49:46] Will Sanchez: cracked there.
[00:49:47] Will Sanchez: So what does that? That's not a
[00:49:48] Dr.Grant Garcia: good sign. So that's not good. That's not a good one. You don't want to hear that word. So crack generally means a pop and generally with meniscus tears. There's ones that are little, they get a little tears, a little frame and that's the ones that get [00:50:00] cleanups or they're usually small.
[00:50:01] Dr.Grant Garcia: A cracker pop is usually a big radial tear, which is right there. Radial tear means Like, it looks like someone cut with a scissors like this right across the meniscus. Okay. And generally those are not good and those need to be fixed. And the reason you fix them, which I just mentioned earlier, is if you don't fix them, the only way to take care of them is to remove the entire meniscus.
[00:50:23] Dr.Grant Garcia: And that is not ideal. It happens. We take, I see patients all the time. They've had, they put internal brace in [00:50:28] Will Sanchez: there. What are they doing with that meniscus?
[00:50:31] Dr.Grant Garcia: So we have to fix it. So you would let you do essentially an internal brace. You know, you do, you fix it and it's called, it's actually kind of a fancy thing.
[00:50:39] Dr.Grant Garcia: You do like a rip stop. It looks like a little checker pattern. I got on some one days we'll pull up one of the things and show how we fix one of these, but it's not simple. Not everybody does it like this. Um, but you want to save the meniscus if you can, but again, it's not always a successful procedure, but let's mention something that her coach mentioned when they asked about this, right?
[00:50:58] Dr.Grant Garcia: You said [00:51:00] she looked at quicker fixes, but it would have led to significant problems down the road. So we committed to the long term flow recovery, right? So when you hear that, there's, there's two things here, six month recovery. That's not a meniscus cleanup. Right. That's it. That is a minute. That is a meniscus repair, and they looked at quicker fixes.
[00:51:21] Dr.Grant Garcia: So a lot of the players in the professional sports get quick fixes. So quick fix is the meniscus cleanup. You've seen a player knee cleanup, knee wash, something like that. And they're like back in six weeks. Those are meniscus cleanups. The problem is it leads to significant where we've been knowing this and it's getting more and more obvious that when you have these really bad tears, like a radial tear, you don't owe, it's not best for the athlete to just remove it.
[00:51:46] Dr.Grant Garcia: Right. And we used to do that a lot earlier on. Yeah. Thankfully not in my time, but even before that, um, and the problems down the road are the worst case scenario, which is what you saw from Lonzo ball. That is the worst case scenario. Well, actually, that's not the worst case [00:52:00] scenario. The worst case scenario is some of the NFL players I've seen after the NFL that retire at 27 that have bone on arthritis, right?
[00:52:07] Dr.Grant Garcia: That's the worst case. Yeah, because we still
[00:52:09] Will Sanchez: haven't figured out the arthritis portion of that. That's the medical science that that's the golden goose, right? If we ever figure out how to eliminate that arthritis.
[00:52:20] Dr.Grant Garcia: Well, that's also what we do. I mean, that is the golden goose and we're getting, we're getting a little bit better and we can go and add another tangent.
[00:52:26] Dr.Grant Garcia: But the, the thing is that like, they're one of my specialties. If you see, um, what I do and there's, this is becoming a more common, it's still not that common and why people like to hear this stuff. And I talk about time, it's called cartilage restoration. So how do we restore the cartilage or how do we save the cartilage?
[00:52:43] Dr.Grant Garcia: So the number one way to save the cartilage is if you look on all my posts, there's a hashtag save the meniscus. There's a reason we do that. Right save the meniscus here is so important So that's why she they they're vowing that she saves the meniscus And the crazy thing is these young patients can do really well.
[00:52:58] Dr.Grant Garcia: I mean, I just I just told [00:53:00] the 15 year old today that I don't know if I can fix her meniscus, but if I can fix, but even if it looks like it needs to be fixed, I'm going to fix it because I'm going to see what happens because with a 15 year old, the blood supply is so good. 26 year olds are kind of the same, right?
[00:53:13] Dr.Grant Garcia: I would rather throw a Hail Mary pass and know that it's a 60 percent success rate because if I don't try it, it's 0%.
[00:53:21] Will Sanchez: Yeah, you already know the outcome. Yeah. And, and how old was this patient? Young woman.
[00:53:28] Dr.Grant Garcia: Mine was 15 a day, but this page we're talking about months and she's 26. I mean, they're still young.
[00:53:32] Dr.Grant Garcia: 10,
[00:53:33] Will Sanchez: 000 meters. This is what she competes in. Did you see something like that? You know, you go, well, let's, let's just kind of fix things and depending on how you heal and if everything goes right, then we could discuss whether, you know, you're going back to running these distances again. Well, [00:53:50] Dr.Grant Garcia: and they can do these other things.
[00:53:51] Dr.Grant Garcia: I mean, now you can do ultrasounds. You can do these, they have these special in office scopes you can do. You basically put a tiny needle in with the camera and they can actually see if it healed. Like there's other things they can [00:54:00] do before they release her if they really want to do that. You know, it doesn't, they're going to do every check on her, on her before they feel comfortable with letting her rip.
[00:54:08] Dr.Grant Garcia: Um, but we've seen with these newer techniques, we can get these things to heal. It's just you, the number one thing is getting to it quickly. Right. The longer you wait, the more it stretches out. And the more that once everything stretches out, it's like, imagine like a water sack, like a balloon. Once you blow it up for so long, it won't always contract back.
[00:54:25] Dr.Grant Garcia: So you want to get that thing back. And usually I say six weeks, sometimes even sooner. Like if someone comes to my office and I have an opening, I do it in a week or two. Like it's just, you just got to get it done. I got you. So. That's, that's what happened here. So we're, we're, we're almost out of time,
[00:54:38] Will Sanchez: right?
[00:54:39] Will Sanchez: It's good news. A long recovery, but Derek Rose had something like this. Uh, Roger Federer for you, a tennis fans had something like this. And, um, obviously, uh, Federer is one of the great tennis players of all time. And Derek Rose came back to become a, a contributing NBA player. Never back to the MVP [00:55:00] status.
[00:55:00] Will Sanchez: Uh, But you know, if you can have an entire career in the NBA, uh, to me, that's a pretty good thing. We can go on and on, but we're going to start wrapping it up, um, because we talk too much again. We said,
[00:55:16] Dr.Grant Garcia: I told you before the show, I said 30 minutes and this is what happened. I know it. I knew it. All right.
[00:55:21] Will Sanchez: All right, we're talking Olympics, Dr. Garcia. You ready for a trivia question? Oh, here we go. All right, I think you're gonna get this. You're gonna be close, right? So, um, Paris, this is the third time that Paris has hosted the Summer Olympics. There is one other city that has hosted the Olympics three times.
[00:55:47] Will Sanchez: What city would have hosted the Summer Olympics three times? Now it's Paris and this other city that have done it three times.
[00:55:55] Dr.Grant Garcia: London.
[00:55:57] Will Sanchez: London is the answer. [00:56:00]
[00:56:00] Dr.Grant Garcia: 1908. First time ever. First time ever. Everyone's got to hear this. First time ever I got it correct.
[00:56:05] Will Sanchez: 1908, 1948, and then in, uh, 20, uh, 2010. So you have stumped the trivia question.
[00:56:17] Will Sanchez: That was our Olympic question. And maybe it's another four years before you get it right again. So
[00:56:24] Dr.Grant Garcia: it's going to be, that's right. I'm going to have to do, we're almost, we're at, we're at three years right now. So I got, I got one more year and then I get a pass, then we're good.
[00:56:31] Will Sanchez: Uh, we just want to remind everybody, please check us out at sports.
[00:56:34] Will Sanchez: talk. com. We really appreciate everyone. Check us out in your favorite listening podcast, uh, with his, uh, Apple and Spotify and I heart, and you name it. We're on there. The same jibber jabber. If you're listening to us, check out our YouTube page. Uh, we really appreciate once again, shout out to recovery shop.
[00:56:55] Will Sanchez: We, uh, we really appreciate them. And for all the surgeons who are interested in [00:57:00] participating, uh, feel free to reach out to the recovery shop. Uh, the link is on our website. The link is on dr Garcia's website, or you can check out their website at shop recovery. net. I don't know. What else? Did I leave anything else out, Dr.
[00:57:15] Will Sanchez: Garcia?
[00:57:16] Dr.Grant Garcia: No, I mean, I know we were slow in the summer, but just, you know, we have a lot more in store for everybody. So thanks for listening. Thanks for watching. Uh, enjoy the Olympics. And, um, What are you going
[00:57:28] Will Sanchez: to watch? What's the one go to? What's your go to? What about your wife? What did she got to go to?
[00:57:33] Will Sanchez: She's like, leave me alone. Get out of my way.
[00:57:35] Dr.Grant Garcia: We swimming. I'm a swimmer. I like the swimming and I, I'm going to watch the Olympics. The gymnastics.
[00:57:41] Will Sanchez: Oh, I gotta, I gotta watch Simone. Uh, it is Abso absolutely amazing. Oh,
[00:57:46] Dr.Grant Garcia: by the way, for you rugby. I like the kayaking. I like the kayaking. We're gonna get off topic, but I like the, I don't want to go any further with this, but I like the kayaking.
[00:57:53] Dr.Grant Garcia: That's so cool. We, we got two
[00:57:54] Will Sanchez: minutes to go further. We love the kayak. Kayaking is awesome. Um, rugby fans, uh, [00:58:00] the women and like I said, I have no idea what the results would be by the time we listened to the show, but the women. Rugby team have made the medal round is the first time the men or women have ever made the medal round for rugby to shout out to a sport that doesn't get enough love.
[00:58:17] Will Sanchez: Um, I figured that you were going to watch the breakdancing competition, but maybe you'll just stick to swimming their
[00:58:23] Dr.Grant Garcia: skateboarding. Who knows?
[00:58:25] Will Sanchez: Thank you, Dr. Garcia. I appreciate it, man. Have a good one. And by the way, we've got Arthrex folks coming in. We got some really cool tools and stuff that we're going to talk about.
[00:58:36] Will Sanchez: We're going to get ready for our kickoff season 2020. NFL season. We're going to talk Chubb. We'll talk Aaron Rodgers. We got Joe Burrow coming back. We've got an exciting fall season coming ahead. So we're really excited. We're going to have guests, you name it. We'll talk about it and we'll do our thing.
[00:58:57] Will Sanchez: Will Sanchez, Dr. Garcia, thank you very much. [00:59:00] Say bye to the audience, Dr. Garcia.
[00:59:03] Dr.Grant Garcia: Bye guys. Thanks for listening. Audio Transcript

Will Sanchez: Oh, Dr. Garcia, it's good to see you. Welcome to Sports Doc Talk. I'm Will Sanchez along with Dr. Grant Garcia. As always, we are really excited about today's show. We're always happy that you're joining us and be sure to check us out on YouTube and your friends. Favorite listening platform. Dr. Garcia, how are you?
[00:00:38] Dr.Grant Garcia: I'm good. I'm really excited for our guests today. Grant Kastner is going to be awesome. Talk about some innovative technology before we introduce him and talk about this amazing product is going to show us we have a really nice sponsorship we want to talk about. So today this episode sponsored you by recovery shop.
[00:00:57] Dr.Grant Garcia: And really, you know, this has been awesome for me. [00:01:00] I use this for my patients. And the problem is that, you know, when you get surgery, a lot of patients are like, Hey, what else can I do? What can I do to get better? What can I do to recover faster? I heard about all these braces and these creams and these patches and cooling products.
[00:01:13] Dr.Grant Garcia: We'll talk about one of those today. Recovery drinks, nutrition. We've had nutrition supplements on. You've had a lot of these people on here and the problem is that in the office, the patients are asking me tons of different questions. They'd ask me, where do I get them? Can you go on Amazon and help me find them?
[00:01:27] Dr.Grant Garcia: You know, a lot of things and it's just so time consuming. So I started partnering with this place called the recovery shop. And what it is, is it offers. The surgeon's ability to offer their patients all of these products I'm talking about, they can get pretty much anyone you want aftermarket and they're, you know, really high quality and it works together to help your patients find it all in one spot, and then they can, you know, buy those things for their surgery as they see fit.
[00:01:50] Dr.Grant Garcia: And it's really been a game changer for my patients. They really love the products they are offered. They're a lot more trusting than having to go through a bunch of Amazon reviews. And you know, I really [00:02:00] encourage it. So if any surgeons are interested, again, this is signed up for the surgeons for their, their patients to get them better.
[00:02:06] Dr.Grant Garcia: Feel free to reach out. I have a link on my website or you can visit the website link here for recovery shop. And yeah, thank you again, guys. Shop
[00:02:15] Will Sanchez: recovery. net. So be sure to check it out. Dr. Garcia, let's let's talk a little bit about our guests today and what our listeners and viewers are in for. [00:02:26] Dr.Grant Garcia: Well, you're in for a real treat. This is a product used by both the hosts of this, and it has been a game changer and basically started for us in. December, early December. And we have patient number one here who wants to show his experience.
[00:02:41] Will Sanchez: Yeah, it's a, it's, it was absolutely amazing. And you know, for those have listened to the show.
[00:02:46] Will Sanchez: Thanksgiving morning, I tore my Achilles. I went in for surgery. And then in December, I've got my nice, I love it. Nice package. Let's look back to December, 2023, [00:03:00] when I received that package. Hey, welcome everyone. I got a great package here from Nice Recovery System, a great company out there in Colorado.
[00:03:08] Will Sanchez: I want to thank. Grant Kashner: for sending this to me. This is really going to help me with my healing process, a cold and compression therapy system. Got a cool little boots, got all these great accessories, exactly whatever you need. So I'm really looking forward to utilizing this. I am 11 days out of.
[00:03:27] Will Sanchez: surgery. I ruptured my Achilles tendon. Thankfully for, for me Dr. Anthony Yee from orthopedic specialist of Seattle's did the procedure. In fact, he did the speed bridge procedure, which you might have had heard from our previous shows. So as soon as I can get out of this cast, start getting this compression therapy system working.
[00:03:47] Will Sanchez: I'm looking forward to getting healed and I'll keep everyone updated on my process. And what a product it was. I'm really excited to talk about it. And anyone that's thinking about it, that's a [00:04:00] patient that has gone through healing. This was absolutely incredible. And we're really excited to have Dr.
[00:04:05] Will Sanchez: Dr. Grant cash. Everybody's a doctor. He's so
[00:04:09] Dr.Grant Garcia: excited. Grant to have you on here. He can't even contain himself.
[00:04:13] Grant Kashner:: No, no. Thank you guys. I appreciate it. And yeah, that's certainly a great video. I've been through it myself being under the knife three times. So a patient as well as you know, luckily the first employee and yeah, been kind of worn all the hats as far as you know, getting to where we are today.
[00:04:28] Grant Kashner:: So thank you guys for having me. I'm excited to be here.
[00:04:31] Dr.Grant Garcia: Awesome. Before I tell my experience, Grant, once you tell them about we keep telling everybody about this nice machine, we'll show a secret little video. But why don't you tell everybody what it does? Because while we'll did amazing job, we still don't really know what it does.
[00:04:44] Grant Kashner:: Sure. So at the kind of the most basic definition, it's kind of the best pain control device on the market, right? It does cold and compression without the need for ice. So we use a thermoelectric technology. Where it gets the the water to a targeted [00:05:00] temperature in between kind of a 4 degree temperature range from 59 to 42 degrees.
[00:05:05] Grant Kashner:: And stays at a constant you know, temperature once it reaches that. So it's just kind of the best, you know, for lack of better term mousetrap on the market. Newest technology and kind of the most portable package for the patient.
[00:05:17] Dr.Grant Garcia: Yeah, this is awesome. So for those patients out there, so I I've gone through surgery.
[00:05:22] Dr.Grant Garcia: I've tried the old ice machines and my wife, I can tell you when I had to get this done, she was. Not pleased with having to change the ice bags every couple hours. We found every trick possible. We tried Frozen peas we tried frozen stuff and thrown in the water because that we literally could not produce enough ice To cool it down and I'm a sucker for ice.
[00:05:43] Dr.Grant Garcia: I ice my shoulder if it hurts. So when We started meeting up with Grant and we first were able to offer this product cause we were the first in the one of the first in the state to have this option for our Washington state patients. I was like, well, Grant, I love this. This is awesome. It sounds cool.
[00:05:57] Dr.Grant Garcia: But like. Let's try it first, right? [00:06:00] Cause I want to make sure that if I try, I always tell Will this, like my patients get offered innovative technology. I want to feel confident. And if I'm going to sell the product to my patients to get really excited about it, I want to make sure it is a difference. So the minute I grant got me one, he sent it to my house.
[00:06:13] Dr.Grant Garcia: I put it on. It was a huge difference. I mean, we're talking about. The cooling system has five cooling depths. I always, I'm a max kind of guy. So I went to five right away. Probably not always the best thing when you're post surgery, but you know, five up there, you don't ever refill it with ice, which is so fricking awesome. [00:06:29] Dr.Grant Garcia: Just a little bit of water. And the compression was really a big difference. And I think Will's nodding his head because he felt the huge difference as well. I mean, even I'm a guy that throws ice bags on my shoulders after I work out sometimes. And this was better than that. And my wife looks at it and goes, Oh, I really wish we had that for your surgery.
[00:06:45] Dr.Grant Garcia: That would have been a much better thing. And then it was funny because I had my father in law over. Who had surgery on his shoulder and he tried it and he was like, this is, what is this thing? This is awesome. And then I also had one of my good friends and she's pretty particular on things. She's actually was one of our [00:07:00] podcast recommenders early on.
[00:07:02] Dr.Grant Garcia: And she tried on her shoulder after she had sold the surgery and she was like, I'm sold. I wish I had this for mine. So right then and there, I knew we were onto something good. And it's a, it's kind of taken off after that. So thank you again, grant for getting, introducing us to this awesome product.
[00:07:15] Dr.Grant Garcia: And the patient experience has been off the hook. You know, they're, They're so happy. I don't want to take too much thunder, but we had to, we have patients. The crazy part of my job is I get patients with two knees, right? And so a year ago I did a couple of patients with their knees and then they wanted their other side done.
[00:07:30] Dr.Grant Garcia: And I got to literally have the head to head experience and patients when they tried it, they were like, why didn't you give me this before? I'm like, dude, listen, I wish I had the technology earlier, but we didn't. So anyhow, it's a, I really appreciate it. This is awesome. I'm so excited to have you on here and I want the viewers to be able to understand this better.
[00:07:48] Grant Kashner:: No thank you, and you kind of hit the nail on the head. It's we, we, I didn't, I didn't know this coming into the business, and I would've thought, you know, I would've, you know, definitely not thought this was the, the train of thought. We have patients that actually call us [00:08:00] and you know, they're, they're looking at doctors or, you know, surgeons in certain areas, and the ones that offer the nice machine.
[00:08:07] Grant Kashner:: They're considering going to them versus the ones that don't. And you know, we obviously have to tell them, you know, go to the surgeon that is the highest recommended that does the surgery that you need. Right. And then we will, we'll, we'll, you know, obviously we're about the the post-op process after, but that was something that we saw too, was just how much it really does affect the patient experience post-op in a very dramatic way.
[00:08:29] Grant Kashner:: So I'm glad you guys kind of see the same thing.
[00:08:31] Will Sanchez: Yeah, let me jump in real quick. It is not only great for the patient, it is great for your marriage. And dr Garcia alluded to that, that I was, this is not, this is, this is your saving relationships and marriages and partnerships. So thank you. Because the fact that I put it's what I felt was like an ounce or two ounce and I, and I'll let you describe [00:09:00] it of water into this machine and it's running for about a month.
[00:09:05] Will Sanchez: And, and I'm like, how is this possible? And I'm utilizing this at least once an hour, throwing this on, wrapping it up, putting the compression, getting the cold in there, utilizing this. My wife is sitting there with the remote. Like, well, all I got to do is just get food for this man. I don't have to get. An ice bag every hour and running to the [00:09:26] Dr.Grant Garcia: torture, torture, you're
[00:09:29] Will Sanchez: saving relationship.
[00:09:31] Will Sanchez: Forget about the patients. The technology is amazing. But the fact is that the fact that our wives still love us after disrupting their lives for months. I can't thank you and everyone there at nice. Thank you for saving our relationships. Well, I will come in today.
[00:09:49] Grant Kashner:: Yeah. We're going to add a, you know, marital bliss as well.
[00:09:53] Grant Kashner:: I
[00:09:56] Dr.Grant Garcia: love it. I love it. And y'all one more last shout out. So [00:10:00] I, my partner just had a big knee surgery. And he comes to me and he's like, Hey man, my knee's pretty stiff. And I've been doing the ice compression with the ice buckets and it's, it's, I don't know. I'm just still stiff. And I'm like, dude, did you hear about this thing I'm offering?
[00:10:12] Dr.Grant Garcia: He's like, what are you talking about? Right. And so I was like, Hey, I call Grant. He ships it to him next day. Such a, such a move, man. I really appreciate it. And he, he literally, this is my partner is amazing, but he doesn't really say much. Like he's chill and he's not going to like complain. He hasn't complained about anything.
[00:10:28] Dr.Grant Garcia: I had to literally ask him how he's doing. He's operated like a day, a month, a week and a half after like a massive surgery. I mean, this guy's tough. And he comes to me, he goes, All I wrote was nice, nice exclamation Mark. And he comes in the next day and he was like, dude, that was awesome. That is so much better.
[00:10:43] Dr.Grant Garcia: I can't believe it. So thanks again. I mean, it's been nonstop. People are nonstop impressed with the product. So it's I, I feel bad for other people that aren't able to offer it. But again, it's not that hard. And we'll get into like, you know, anybody can offer this option. This is not something that because I [00:11:00] do, you know, You know, I work with recovery shop and I work with you guys and stuff like that, that, you know, I have elite product access to it.
[00:11:06] Dr.Grant Garcia: No, there's the whole point of this show is to show people that anybody can have it. And patients want it. And it's the same thing we talked about before from a marketing standpoint. I mean, I hate to say it guys, but you know, when you're a surgeon, like patients come to me because I offer innovative stuff.
[00:11:19] Dr.Grant Garcia: Like it doesn't, I try to do a good job. I think I've got a decent reputation, but really like you said, people are calling, they're calling Arthrex, they're calling other companies and they're like, who should we go to? Right. And that's brings patient referrals and it's not like you should sign up for this or, you know, it's not, it's not a subscription or anything, but it's not like you should do something because it helps that.
[00:11:37] Dr.Grant Garcia: But if it's from a marketing standpoint and it's good for your patients, this is a win, win, win, right? Everybody wins. And that's always the key here in a, in a type of relationship. So any go, thanks again, Grant. This is awesome. Do you want to I want to kind of. Stop talking a little bit less and let you talk some more. [00:11:53] Dr.Grant Garcia: 'cause obviously I want everybody to hear about this. We don't
[00:11:55] Will Sanchez: even need grant cash. Grant, just hang out. Let us talk for you. In [00:12:00] fact, you don't just sit back. You got nice hat on. You got, this is great. He looks good. He's killing. And just go like that because we're doing all the talking for you. But , I appreciate it.
[00:12:13] Will Sanchez: We can tell you we are terrible
[00:12:14] Dr.Grant Garcia: on this.
[00:12:15] Will Sanchez: We are terrible. Hey, why don't you tell us a little bit about the company and how it started and the founder, let's kind of get down to the roots and what was the inspiration to, to start to look into this technology and how it developed from day one to where you're at right now?
[00:12:34] Grant Kashner:: Sure. No, and it's actually a really cool story. So our founder and CEO, Michael Ross, he you know, for Just, you know, again, not not the, you know, kind of kind of a buzzword. He term was a serial entrepreneur right in his career. A few different businesses move to Boulder to kind of figure out his next move.
[00:12:53] Grant Kashner:: Right? While he was in Boulder, he decided to take up ski racing right at the young age of 46 years old. So. If you [00:13:00] guys know about downhill ski racing you're going about 85 miles an hour turning, you know at about 45 degrees, you know every, let's call it, you know, few hundred yards. So I'm, I'm, I'm sure you know what happens next to a 46-year-old, you know.
[00:13:15] Grant Kashner:: Man, and he he destroyed one of his knees blew his IT band off, tibial plateau every ligament and was essentially you know, ski and ski out to the Steadman Clinic in Vail. So he had a series of surgeries done by Tom Hackett. At at Steadman and then used it, used our competitive product, which is a game ready.
[00:13:36] Grant Kashner:: And I know you're not supposed to say your competitors, but they did a great job you know, kind of seeding the market with a really good product. And then honestly just didn't ever product innovate. So Michael used this product, realized that there, you know, was just inefficiencies and there was better technology on the market.
[00:13:52] Grant Kashner:: So. Just being, you know, hard headed and kind of spiteful started engineering a better product and about two [00:14:00] years later brought a pretty good working prototype to the Stedman clinic showed Dr. Hackett as well as Dr. Philipp on, and they were, you know, jumped all over it. Technology wise similar, you know, you, Dr.
[00:14:11] Grant Kashner:: Garcia, they also love kind of the innovative technology and wanted to, you know, stand behind, especially an American made product, right. We're even then we set up, you know, American manufacturing in Boulder through a contract manufacturer. And then now we make everything in house. So long story short from there, he went to working on the FDA.
[00:14:32] Grant Kashner:: And then somehow, you know, I called him when I had a couple other things going on, just on some kind of, you know, advice and the timing worked out and this was in April of 2016. So I hopped on board and it truly was you know, a garage company, but he didn't have a garage. So it was in his home office.
[00:14:49] Grant Kashner:: So and then from there, about two months later, they were he was actually getting married. So we had to find an office building. So that kind of started the whole business was we had three units [00:15:00] produced. And we had to find an office, so it's been yeah, you know, every kind of building block figuring out this business.
[00:15:08] Grant Kashner:: I don't know if you guys are, you know, no, no, a lot about the, kind of the, the very niche kind of DME market, but it's it's a very interesting world as far as, you know, no insurance and figuring out kind of delivery service and product and, you know, just how to, how to How to bring a good solution to the market.
[00:15:26] Grant Kashner:: Right. And I feel like, you know, eight years later we finally have have arrived. So, you know, overnight success just takes, you know, about, you know, eight to 10 years.
[00:15:38] Dr.Grant Garcia: Well, this is, it's interesting for the viewers to hear that last part you said about, you know, the difficulty of the DME market. What they're not realizing is that like you don't have like a nice rep on the ground.
[00:15:48] Dr.Grant Garcia: Right. Like, it's not like, you know, you hear guys here about these products, like, you know, there's amazing arthritis products. There's lots of other ones we've talked about, you know, when we get those things, those are in, those are surgeries, like they're getting delivered before [00:16:00] we got a ton in house.
[00:16:01] Dr.Grant Garcia: Like I could do pretty much any surgery I want in house. It's all there. I got a little bag and I can grab whatever I need. This has to be shipped from all over. And so it's got to be shipped with quality and it's got to be functional. But I think the one really important thing about the product is that it's despite how tech, how smart is and technology driven it is, it's actually pretty easy to use and like you just don't need instruction manuals, which is really good for the patients because everyone, you know, and we have a lot of smart patients, but the technology can be a challenge, especially when you start doing, you know, in the total knee population as you get a little bit older, you know, they're not a big fan of using their phone or remotes or things like that.
[00:16:36] Dr.Grant Garcia: So again, It's a little less than my patient population, but overall, you know, there's so many outlets for this. And so it's amazing to have a technology that's simple, but effective. What what other institutions, I know you guys do a lot of Stedman. Are there any other places you guys have worked with around the country or you're kind of like I know you guys do a lot with HSS now too.
[00:16:54] Dr.Grant Garcia: Any other place for the viewers to kind of hear places you've worked with? Cause again, you're a lot bigger company than you were from three machines now. [00:17:00]
[00:17:00] Grant Kashner:: Yeah. Yeah. Yeah. So our roots are obviously in our backyard in Colorado, right. Where Michael got his you know, kind of, kind of got, got his, you know, fixed and kind of on this track.
[00:17:10] Grant Kashner:: So Stedman is the big, you know, kind of start from there. You know a lot of docs kind of train there and then go other places. Right. So we do a big volume of business in TCO. So in Minnesota, right. A lot of activity there. I think we're partnering
[00:17:25] Dr.Grant Garcia: with them now. We're Pelto. We're part of the alliance.
[00:17:28] Dr.Grant Garcia: So that's cool.
[00:17:29] Grant Kashner:: So yeah a very big presence there. Obviously HSS is another, you know, very big kind of stronghold for us. We do a good volume of work in resurgence in the Atlanta market as well. So yep. And then we have been growing significantly in the Carroll Clinic and the Dallas market.
[00:17:48] Grant Kashner:: You know. Kind of rapidly as we, and you know, Dr. Garcia, you kind of hit it on the head, right? It's you need good stewards of the product, right? We're the manufacturer and you know, we, we want to [00:18:00] choose with good people to represent us in the market because people, people remember the doc and they remember the product, right?
[00:18:06] Grant Kashner:: They don't really remember the people in between that because it's who fixed them and then what helped them after getting fixed, right? So it's really important to have good people that represent the product because If they don't deliver it or they don't service the patient or they don't, you know, communicate with the patient or communicate with the doc and the physician and the staff, then the patient experience just isn't like doesn't follow the quality of the product.
[00:18:32] Grant Kashner:: So the main, you know, a lot of the driver of our growth is also choosing really good partners to represent the product in certain markets. And that's kind of what goes hand in hand, right? We have a really good network, a really good product, and then we choose really good partners that service the product stewards to the patient.
[00:18:49] Dr.Grant Garcia: And I don't want to jet out of this topic, but one thing for the people that are listening is one, and this is a kind of a full circle episode. So, you know, one of the, one of the good ones you guys have is recovery shop. [00:19:00] So we work with them. And if, you know, a surgeon's part of recovery shop, they can get that product to their patients really easily.
[00:19:07] Dr.Grant Garcia: And it's been, they've been amazing. And again, I don't want to overdo it. Cause we already talked about them as a sponsorship, but for people to know, like this all is intertwined, right? How does this work? It's not like, you know, as good as grant is he can't deliver them all himself. So he's got to have someone help him.
[00:19:21] Dr.Grant Garcia: And so they've done an amazing job. And, and anybody knows that you can know when you partner like this, it's really nice to know that, like. You said like grants team is amazing, but also adding another amazing team like the recovery shop guys together allows us to automatically, you know, I patients are getting these things flown in all the time, you know, and if there's any issue, like sometimes patients will forget and they'll get it like the last minute and they get it to him overnight.
[00:19:42] Dr.Grant Garcia: Like this. It's not always easy in the winter snowstorms, but you know, we get the service has been amazing. And again, I'm in Seattle. It's not very easy to, We have the hardest place to go. I mean, it's one of the farthest distances from anywhere in the country. And patients have been really pleased.
[00:19:56] Dr.Grant Garcia: We've been doing this for, you know, six months. So anyhow, so [00:20:00] that's good for patients to know, like, how it works. Kind of behind the scenes. And it's easy, again. If, and again, what's, so what's the, so let's say a patient's listening to this, right? Or a doc's listening to it. Can a, can a patient, How does a patient, like let's say a patient wants to get one of these machines can they work through you guys or do they talk, can you talk to your surgeon?
[00:20:18] Dr.Grant Garcia: What do you guys recommend? What's the easiest thing? So
[00:20:21] Grant Kashner:: kind of it works both ways, right? What I always say is there needs to be an actionable event for which is a patient getting injured, right? Then, then what happens is that actionable event drives to a physician who writes a script for that, Patient right to obviously get surgery and then, you know, be fixed.
[00:20:39] Grant Kashner:: So it really drives from the patient side, right? The patient need. So that's really patients can get ahold of us and then physicians as well, right? We get a lot of surgeons that kind of, you know, see what you're doing, Dr. Garcia, right. And see what, you know, the guys at HSS are doing and see what the guys that, you know, resurgents are doing and see what, you know, kind of [00:21:00] the big clinics that really run very efficiently and very, you know professionally are doing and, and obviously want to copy it.
[00:21:06] Grant Kashner:: So mostly yeah, if patients want to rent it, they can, they can get in contact with us. We will get them in contact with the recovery shop who will service them. You know, immediately. That's another reason why we do such good work with them as I can send them a patient referral. And I know within 30 minutes, that patient's going to be contacted and you know, just have We'll have a very good service experience.
[00:21:33] Dr.Grant Garcia: That's important for them. And also for the patients, you mentioned something that's really important and it's, it's kind of confusing to think about it, but this is a rental guys. And I'll tell you why that's such a good idea because it sounds weird, right? You're renting a system and then you're giving it back.
[00:21:47] Dr.Grant Garcia: Right. But the, I own an ice machine and it's in my garage and I can't get rid of it. And, and I'm a Seattle guy, you know, we're [00:22:00] environmentally friendly here. And I've got a huge plastic thing sitting in my garage, and I know all my other patients have a huge plastic thing sitting in their garage. And so, they never get used again, or they get used once, or my friends take it from me and borrow it.
[00:22:16] Dr.Grant Garcia: And now you can rent something and you only get it for a couple weeks and then you can give it back. Which is great. And then it's reused. Essentially it's recycling, right? Which is awesome because you don't need this for, this is not a 10, 12, 14 week product, right? You know, for me, most of my patients are renting three weeks, four weeks.
[00:22:33] Dr.Grant Garcia: What do you think on average people for you guys are doing usually?
[00:22:37] Grant Kashner:: It all depends on case, right? So you know, for me that I had you know an ACL revision with an let, right. I was more in that eight. Kind of a six, eight week bracket. 'cause I was pushing it pretty hard in the rehab. Right. I'd say primarily most people are in that three week, right?
[00:22:55] Grant Kashner:: Four week, maybe five week range. And then scopes, you know, a [00:23:00] couple really what happens is the first two weeks are the pain control. Then once they start getting into pt, right. Just depending on how aggravated that kind of joint gets. Kind of deems how, you know, how [00:23:11] Will Sanchez: much,
[00:23:11] Grant Kashner:: how much they're going to need it.
[00:23:13] Grant Kashner:: But, but generally it's usually about two to four weeks. And just to add one thing to your point, Dr. Garcia, every patient gets a brand new wrap. So each wrap is a single patient use. I just wanted to clarify that. So that's
[00:23:27] Dr.Grant Garcia: important to remember. Yeah, no, no, no,
[00:23:29] Grant Kashner:: no. You get a brand new wrap super high quality four layer.
[00:23:34] Grant Kashner:: You know, air, water, and then the outside, you know, yep, exactly. So they're all ergonomically designed per joint or per site. And yeah, we keep expanding the wrap line. Well, I saw your video with our old ankle wrap, but we just brought on a new ankle wrap, which I was like, no, I wanted to get you that one, but [00:23:53] Dr.Grant Garcia: we'll get them up.
[00:23:54] Dr.Grant Garcia: We've got to give them an upgrade.
[00:23:55] Will Sanchez: Up. I want to say this. Listen, I don't know what these, these folks here are [00:24:00] talking about. Three weeks, four weeks, six weeks. I did not want to give it back. Okay. Because it was just like something was feeling a certain way. I had swelling. You know, you still kind of recover.
[00:24:13] Will Sanchez: You kind of go, I did not wanna give it back. I got my FedEx sticker to send it back, and I was just. Real sad face is putting in the bubble wrap and it just really folding it nicely. I was like saying goodbye to a friend. And then the first time I needed to use ice, I was angry. I was like these SOBs and I had to send it back. [00:24:37] Will Sanchez: So listen, yeah, send it back, utilize it. But the problem is once you get used to it and you utilize it and it's so simple and so effective that you don't want to give this back. So I don't, you know, I'm, I'm, I'm going off on a tangent here, but I was really angry when I had to send it back and disappointed my wife came with me to FedEx and to drop it off.
[00:24:58] Will Sanchez: So,
[00:24:59] Dr.Grant Garcia: so your, your wife's gonna [00:25:00] have to go with you cause it's a marital thing. Remember, right? With this nice
[00:25:02] Will Sanchez: machine.
[00:25:03] Dr.Grant Garcia: And then, and when you give it back, you're going to be sad. But when you get it, you're going to be happy. It's kind of a, it's a, this is a good, I like this part. So, yeah, I mean, basically what you're, what you guys can hear is that, you know, this, and the nice thing too, is like, Grant will say, when you work with these companies, the recovery, or, you know, just directly with you guys, If someone wants to keep it, they can, you know, they just extend the rental.
[00:25:24] Dr.Grant Garcia: It's not something you have to return, you know, and then re rent it or something like that. And what's cool is you guys keep coming out with new wraps, right? The, I like for my patients, the knee, we started doing a lot of straight wraps. Can you show the straight one over there? But then, you know, grants, like we have something even better.
[00:25:40] Dr.Grant Garcia: We have an articulating wrap. I think this is what separates you guys even more from the other companies too. Would you say, I mean, you have so many more options and it's customizable. I mean, you have a hip wrap. That's crazy. Right. Like I tried a few of these and they're really impressive. And [00:25:54] Grant Kashner:: that's kind of what what our company is built on, right.
[00:25:56] Grant Kashner:: Is innovation around, you know, we kind of saw [00:26:00] what Michael's really good at is seeing what our competition does and doesn't do well, right.
And they don't, they don't. They don't product innovate and they don't keep the, you know, the, the, the, the products moving forward. So the unit that we first produced in 2015, while it looks the same has probably, you know, 15 or so upgrades internally and slight, you know, slightly externally as well.
[00:26:25] Grant Kashner:: That we just want to keep upgrading the technology. Like we just put a brushless pump in there from a brushed pump. Right. Because the technology in the market is up, you know, is, is updated from eight years ago. And the wraps, that's another big area that we look at, right. We are bringing out ones that, you know, people aren't even really considering an amputee wrap, right.
[00:26:46] Grant Kashner:: A glove. We have an integrated. Solution with Aspen on their on their, on their bracing line where we can integrate cold into bracing. Right? We have a new ankle boot that fits into a boot Walker. So we're really [00:27:00] trying to to cover everything. Right? We have a new elbow specific come into the market as well.
[00:27:05] Grant Kashner:: That covers the distal bicep. So, like, we're really trying to look at, kind of the complicated stuff that not a lot of companies can cover. And really, really have good solutions for it.
[00:27:15] Dr.Grant Garcia: I think that's really important. What you just said, Grant, I think it's important. You said like the, sorry, well, I just say, make sure patients hear that.
[00:27:23] Dr.Grant Garcia: Like this is this product going to keep getting better too, which is awesome. And it's made for everybody. It's not like, Some things like the, you get two pads, right? It's like a back and that's it. And trust me, I had back and I was using a knee pad because there was no lumbar. There was no lumbar stuff.
[00:27:39] Dr.Grant Garcia: So yeah, I know it's, it's amazing. So anyhow, so keep going. Well, I'm sorry to interrupt.
[00:27:43] Will Sanchez: No, not at all. What you're saying is absolutely makes sense. I just wanted to kind of put up there and talk about what this is and just kind of describe it a little bit more for those that haven't used it. Right. So I alluded to that in the beginning, right?
[00:27:56] Will Sanchez: So you have this Pretty much it looks like a box. We've shown [00:28:00] it if, but if you're listening, just want to give you a description is a blue box. It has an led screen. You can set compression, no compression, how cold from one to five. So it gives you a lot of options, but going back to the no ice. What is, or how many ounces of water are you adding to the tank and what is the timeline depending on how, how long you use it, that you can keep, keep that on before you have to even add more water to it.
[00:28:31] Grant Kashner:: Sure. So great question. And we have a couple parts of the machine that aren't really, you know, pumped out there like that. And one being the water, right? It's nine ounces of water fits in the tank. Each wrap holds about, or, you know, let me use milliliters. Cause it kind of just converts a little bit easier.
[00:28:47] Grant Kashner:: 350 milliliters are in the tank, right? Each wrap holds about a hundred to 150 milliliters. So that's actually what we cool. And the other kind of. is extra, right? It's a [00:29:00] So essentially, unless th of, you know, kind of eva know, there's a couple of of the connector every on might have to put a coupl 2 3 months, just dependin hot it is outside, you kn Yeah, apart from that, the machine will actually tell you when it's too low.
[00:29:23] Grant Kashner:: And, you know, there are some, you know some machines in clinic that they probably, you know, because it's at a nice, in a nice cool area and, you know, it's been connected to the same wrap for, you know, forever. It's probably, they probably haven't put any water in it in, you know, a year or two. So.
[00:29:39] Dr.Grant Garcia: That's just amazing. That's amazing. That's just, I mean, that's just ridiculous. I, like, I felt bad keeping the water in there for like three days. Yeah, no, it's change it, but it's amazing what it can do.
[00:29:50] Grant Kashner:: And and for patients really the biggest thing, and I kind of touched on this, is it's the kinda the best pain control mechanism, right?
[00:29:56] Grant Kashner:: And it stays at a constant temperature. Now we have preset [00:30:00] programs on this and. Again, it's not one of those things that we pump out there, but if you know about it, then, you know, then the patients love it. So our preset timing programs have a 10 cycle memory. So that meaning we have you know, a 30 on 30 offsetting, which gets the patient 10 hours of runtime, 30 minutes on 30 minutes off without them having to touch the unit.
[00:30:20] Grant Kashner:: So for pain control at night, it's a game changer. Because usually to, you know, to heal, you need to sleep. Right. And if you can't sleep because of pain, you're usually grabbing for opiates, right? Because that helps you kind of leave the pain and sleep because this runs at that 10 hours of 30 on 30 off, your pain control mechanism is consistent, right?
[00:30:42] Grant Kashner:: And it's there every time so that you're not grabbing that three a. m. Right. Or, you know, you know, tapping your wife and saying, honey, yeah, go, go get me some ice. Fill this up. Exactly. Or
[00:30:55] Dr.Grant Garcia: pills or pills. So That's a huge thing. I [00:31:00] think that the opioid sparing is all over man, and it's a big deal, right? We've already we don't want to I don't want to go into the opioid pandemic and all the craziness But it's a big deal and for patients.
[00:31:12] Dr.Grant Garcia: I have so many patients that come in They're like I won't want to use a single opioid I'm like, well, I totally get it and I want to find every way possible. You know, I'm looking at all different alternatives. We're always looking for new technology to reduce that, but it's tough for these huge surges we're doing.
[00:31:26] Dr.Grant Garcia: I mean, the patients that benefit the most from the nice machine are the biggest surgeries. I mean, everyone benefits, but like my bigger, my more complex surgeries get a huge, huge, huge benefit from it. And I basically tell them it's just almost a non factor that they should get it right. But opioid use is humongous.
[00:31:43] Dr.Grant Garcia: And the fact is ice is so harmless and this machine's harmless. You know, again, I maxed out, I do ice bags and I've gotten some shoulder burns before on ice bags. And I had the nice machine cranked up. It felt just, it's crazy. It felt just as cold as the ice bag, but I didn't get a single concern about that.[00:32:00]
[00:32:00] Dr.Grant Garcia: Like I never, my wife at first was like, take it easy. Cause she knows I go all out with the ice and and, and I, I cranked that thing up to five and it felt just as good and just as relieving. But. Without the concern for the burn. And so that's why this 30 on 30 off.
[00:32:13] Will Sanchez: That's a big selling point right there.
[00:32:15] Will Sanchez: I think what you said right there, because sometimes we'll cheat it also, and maybe not use ice, but one of those ice packs that are kind of gel and that.
is a different type of cold. And if they, you apply that to the skin, you're having other issues, other complications. So that's another great thing to consider because for the same reason we're talking about either one, I can't make ice fast enough.
[00:32:42] Will Sanchez: I don't have the space in my freezer to buy an ice bag. Maybe I have some gel ice gel things that maybe I'm using something like that. If I use it, you know, I don't use it properly. I can cause skin irritations and things like that. So I think it's another way to kind of promote the technology and the benefit [00:33:00] of using the nice recovery system.
[00:33:02] Grant Kashner:: You actually just brought up a really good point that I don't think a lot of consumers or people know kind of about thermo kind of regulation on the skin. Right. So. If it's too cold, right? Meaning it's below 38 degrees, so the, so the nice goes to 42 degrees for a very specific reason, right? It's the coldest that you can get before you start to vasso constrict on the patient, right?
[00:33:25] Grant Kashner:: Which again, doesn't create blood flow, doesn't create the best healing environment, right? There's, there's a lot of reasons why you don't want it too cold. All the news, all the newest studies out of actually Nicholas Institute of sports medicine and technology in New York city, they actually did a bunch of trauma studies and saw the perfect temperature and the perfect kind of millimeters of mercury or compression level that created the, the, the best healing mechanism for the patient.
[00:33:52] Grant Kashner:: Right. And it's actually about 49 Fahrenheit. And about 15 millimeters of mercury or about our low [00:34:00] of squeeze. Right. And Dr. Garcia, to your point, everybody, especially athletes and just kind of high, you know kind of high motor individuals. We all, we want it cold, cold, cold, cold, cold, and squeeze, squeeze, squeeze, squeeze.
[00:34:12] Grant Kashner:: Right. But I
[00:34:14] Dr.Grant Garcia: put max on everything. So I'm just going to explain. I am definitely that person.
[00:34:18] Grant Kashner:: No, but it actually, all the. And we actually are hearing this now. It's funny how when we first came in, it was like, people were like, it's not getting cold enough. Right? And now everybody's like, no, we actually, it's perfect.
[00:34:28] Grant Kashner:: You guys, you know, it's kind of the best overall healing setting. So to your point, it's, you know, it's skin safe, it's, you know electronically controlled, right? By software on the, on the temperature. And, yeah, it really is for those big surgeries. I've had a couple absolutely massive ones just from being injured, you know, doing extreme sports.
[00:34:49] Grant Kashner:: It was I was shipping it around when I was flying to meetings and everything. I was overnighting it to hotels because it literally was the most important piece of equipment. And I was [00:35:00] like, you know, I was like, thank God I worked for this company because I'd be, I'd be running the, I, I mean, I, I would have bought one by now.
[00:35:07] Dr.Grant Garcia: Yeah. Well, I mean, it's, and also, but it's important for the listeners to know, I, I wouldn't recommend like taking this on all your trips with you. Cause it isn't, it isn't super small, but it's actually pretty easy. It's so light. I mean, how many pounds is it? You said nine pounds.
[00:35:22] Grant Kashner:: Yeah. And it comes in a carry case, which you can carry on.
[00:35:25] Grant Kashner:: Don't check it. Right. Just carry it on as a second carry on, if
[00:35:29] Dr.Grant Garcia: you need to. Yeah, it's not bad. I mean, the thing is, I've you guys ever carried one of those ice buckets? It's like so heavy, filled with water and ice. So, I mean, this full is still not even that heavy. So it's great for people, especially, you know, any type person can bring it around and carry it.
[00:35:45] Dr.Grant Garcia: Well, and pro sports, right?
[00:35:47] Grant Kashner:: So everything else is pretty big. So we do really well with pro sports because and college and high school because there's no ice in the dorms. It's really hard to find ice on the road, on the, in the hotels, on the team [00:36:00] bus. On the team plane. So we do really well with any, you know, teams that are traveling or people that are traveling that you know, kind of are needed, are, are needed.
[00:36:12] Grant Kashner:: The technology on the road as well.
[00:36:14] Dr.Grant Garcia: That's an awesome point. Remember I would do the training room for, you know, giants and the Mets, et cetera. And like, there was just like ice flying off the handles there. And like every guy wanted ice, but I can imagine that like, that's kind of the old way of doing things.
[00:36:29] Dr.Grant Garcia: You know, you get a couple of these machines and you know, the major leagues. or the NFL and it's so much easier just to throw it on and you can run it so much longer, you know, like the, you know, they, these pictures they'll come out and they got like an ice here, ice here and it's, and it's just not, it's not efficient.
[00:36:45] Dr.Grant Garcia: Right. And if they're, they can't do that on the plane, cause it's going to melt. Well, and that option,
[00:36:50] Grant Kashner:: it's really important to get the relief when you're needed, right? Like even, even a quick 20 minute session without having to, you know, fumble with ice, especially if you're. [00:37:00] Let's say you're on the road, you're moving around, right?
[00:37:03] Grant Kashner:: You're kind of six, eight weeks, 10 weeks out. Right. And that thing gets inflamed. Just having that machine there and the confidence that you can just hit a session quickly and not have to worry about it was the biggest confidence booster as well. Mentally coming back from an injury. And I think that's slept on a lot too.
[00:37:20] Grant Kashner:: And kind of forgotten is like kind of the mental battles that go along with injuries. And the pain and the, you know, the, will I get back to doing what I want to do and be where I want to be? And you know, alleviating the pain and at least getting, you know, range of motion and starting the PT process and having the, the post op process a little bit smoother is a major game changer as far as the mental, you know that's something that also really isn't talked about in the surgery.
[00:37:46] Grant Kashner:: It's always like no opiates, make sure you're doing this, but it's also like, Hey. you're, you know, that, that after surgery, you're feeling good about, you know, kind of getting back to where you want to be.
[00:37:58] Dr.Grant Garcia: Oh yeah. I mean, I, I tell [00:38:00] patients now I've gotten so used to the, I'm like probably 35 percent therapist now in the, right.
[00:38:06] Dr.Grant Garcia: Like I do a lot of surgeries, but I'm it's therapist. I mean, I tell patient, I'm like, you're going to be back in seven months, but this is not going to be back for at least a year. It's hard. And I think But one thing that's really nice about this option, just like so many other stuff we talked about is it gives patients the confidence that you're really invested in their, you know, their non opioid presence, recovering faster, because like, a lot of these patients, they come in and I try to, I got a lot of stuff on my website and everything else, and so they, you know, they know that I'm thinking about other things, but it's good for them to be like, you know, a lot of people get in the surgery and they're like, all the surgeon cares about is surgery.
[00:38:40] Dr.Grant Garcia: I am going to operate, I am going to fix you, I am a machine, and then you're going to be done with me. Right, that's the concern, that's the fear of like half my, I mean I do so many second opinions because of the fear of machine. It's a huge problem and listen, I'm not going to lie. I love surgery. Okay.
[00:38:59] Dr.Grant Garcia: I love [00:39:00] fixing people. But at the same point I really like people when I fix somebody, I want them to feel totally safe and confident and I want them to feel that they're getting the best care possible and that I'm not just another person churning out a patient in the office. I'm there to, I want to see them the whole way.
[00:39:14] Dr.Grant Garcia: You know, I have patients come by. Every week, someone goes, are you going to see me after surgery? And I'm like, did someone tell you that that wasn't going to happen? I was like, I see everyone as much as I can because I want to make sure you're doing well, right? And this is one of those things. I want to make sure patients do as well as possible.
[00:39:29] Dr.Grant Garcia: So offer the most innovative technology in the operating room, offer the best prehab, and then offer the best stuff postoperatively. And this is one of these options for them. And it's, it's important for me because less opioids, they have less pain. They have the less, they have less marital issues. They have less comfort, you know, all these things, right?
[00:39:48] Dr.Grant Garcia: Well,
[00:39:50] Will Sanchez: Oh yeah, I've got a two part question for you. Are you doing anything for kids sizes? Has there been any studies that, [00:40:00] you know, you say, okay, well, we're working on kids sizes and also this is the age that's appropriate. Like, so have you gone down that road yet?
[00:40:08] Grant Kashner:: It's actually a really good question.
[00:40:10] Grant Kashner:: And we, we, we, we have, to some extent, we've started down that path. And it's kind of stemmed from a couple of things. One is our HSS peds department. Right. We get a lot of, you know, unfortunate, you know, but, but, but fortunately for us, we can start to get ahead of it, right. And we can bring out products that really fit that age.
[00:40:31] Grant Kashner:: Mostly it's about 12 and up. Right. It's. But it's the smaller and, and not even peds. It's just kind of, you know, smaller people and even smaller, old, you know, ladies in general. And, and mostly the shoulders, right? We can, we can, we can fit a leg, we can fit a knee, we can fit an ankle. It's the shoulders and the hips that are the kind of the biggest target areas for us.
[00:40:53] Grant Kashner:: And that's really something that shoulders primarily we are focused on first, then hips, [00:41:00] everything else we can kind of maneuver right now with our current wraps. But we like to kind of, again, gauge the need. We love to work with, you know surgeons and facilities and, you know, orthopods that say, Hey, What about this?
[00:41:15] Grant Kashner:: Right. And something we haven't thought about or looked at, right. We, we can produce it and we can produce it pretty quickly. Or if we need to make changes, right, we have it, we have the process dialed so that that's a big, going to be a big focus of ours. Moving forward as a, a big peds line. It's exciting.
[00:41:31] Grant Kashner:: And
[00:41:31] Dr.Grant Garcia: that's so important. What you just said. I think the, for the surgeons listening and for the patients, you know, this is not just a product, like a machine that just pumps cold, this is more. This is the sales experience. This is the concierge aspect. If you have a problem, you can call them. This is working with surgeons who know what they're doing, working with the partnerships like recovery shop, but finally feedback, right?
[00:41:56] Dr.Grant Garcia: I've done so many, we've done so many company discussions [00:42:00] on this thing. And you tell somebody something and it just goes in one ear and comes out the other. And the fact is like, what you're saying is like, we listen to feedback. You know, the HSP is guys, that's where I trained. Right. They do so much peds and I, in my practice now I do 12 and up as well.
[00:42:14] Dr.Grant Garcia: And so for those patients, you know, you don't want to feel like they're underserved and this is not, this is a good way a kid could use. This is not a dangerous product. It's just more of the size fitting, right? Like anybody can use this. There's nothing, there's nothing kids have, I kind of have ice on their bodies and kids do stupid things with regular things.
[00:42:30] Dr.Grant Garcia: So this is not a dangerous product. Trust me, I have kids. So this idea, it will knows this too, but anyhow, the, the, the point being is that It's nice to hear that you guys are like, we just keep hearing this more innovation and this product, this, something, this is simple, right? It's a, it's a box that's got amazing technology in it that makes things cold and compresses, which is a phenomenal, but it's more than just that.
[00:42:51] Dr.Grant Garcia: It's like so many other things that are important that people don't think about, right? Like, what about a small arm? What about an elbow?
[00:42:57] Will Sanchez: Those are
[00:42:57] Dr.Grant Garcia: coming, right? Those, all those things you guys keep continuing [00:43:00] to improve. And it's just, it's just awesome. And, and we're looking forward to, you know, the, the next year or two and seeing what more is to come.
[00:43:07] Dr.Grant Garcia: Oh yeah, we got a lot under the hood. But we'll
[00:43:10] Grant Kashner:: add something to your kind of point you said before, right? It's, you know, you're, you're also a therapist, right? You fix the patients mentally, physically, all of that. And we hear that frequently on our side too, is that, you know, if you call us, you're going to talk to a human.
[00:43:25] Grant Kashner:: Right. You know, you, you know Dr. Garcia, you can text me and I'm gonna reply quickly. Right. It's like, and, and, and patients have that same experience, right? It's 'cause we, well we've been patients ourselves first, right? It's founder and CEO owned from an injury. So that really matriculates through the entire company where.
[00:43:45] Grant Kashner:: We understand the patient experience through and through, and you really feel that in the company and the products and how we treat people. And, you know, it kind of just perpetuates the whole company. And that's why we, you know, really, really like working with surgeons like you, dr. Garcia, [00:44:00] because, you know, we align so well.
[00:44:02] Grant Kashner:: Just in our basic ethos and the way we do business and the way we, you know, want to treat people. And that's really important to us from a medical, you know, I know we're a medical device manufacturer, but just as a, you know, a company and as, you know, as a person as well we like to work with good people and treat people well.
[00:44:19] Dr.Grant Garcia: I mean, I wouldn't call, you know, the thing I want to take your listeners see is, is we talk about a lot of different device things, but the mentality here, that one reason I like working with. Them so much. I think the patients like it is I do feel like it's a patient first mentality And that's a challenge to find all the time as will and I've talked about in the market.
[00:44:35] Dr.Grant Garcia: You know the ability like You know, you're coming out with all you don't have to make all those things A lot of these companies just make three pads, right? There's no reason you need to make a baby elbow pad No. Right. There's no reason for it. You still sell a lot of stuff and you do well financially, but that's not big deal. [00:44:50] Dr.Grant Garcia: Like, that's not the part, part the purpose for you. Mm-Hmm. The purpose is you, is you want people to feel good about it and do well, and that's why you have a product like that. That's why you guys worry about the, [00:45:00] the temperature you can do and you don't wanna max out here and you want to educate and things like this, the podcast so people can understand what it's all about.
[00:45:08] Dr.Grant Garcia: Right. It's not just a little box that does compression. There's more to it. There's so much that goes behind it. And to, you know, to hear there's constantly being updated. It just makes people feel good. Right? Like you don't want something that's been stagnant. You don't want old technology. Patients don't want that.
[00:45:21] Dr.Grant Garcia: At least the ones that I deal with. And they want to know they're getting something that's updated and better, and that's what they get. Do you, do you want to last, I guess, one more topic and then we can go and maybe quick future stuff. Do you, for any doctors interested. And using this, what do you recommend?
[00:45:36] Dr.Grant Garcia: I know we've talked about the recovery shop. That's an awesome outlet. So again, guys, check it out. And they work really well with the nice team. If someone wants to get involved and make sure they offer this product, cause I have a feeling after this episode, we're going to get a few. What do you recommend?
[00:45:50] Grant Kashner:: So I would say let's, we love to obviously get the product and like you guys, right? Let your, your experience. I want to put the product in your hands, make sure it works well for [00:46:00] them. They love it. Their patients love it. Their staff loves it. Right from there. We can figure out the details about the rental piece and how we figure out, you know, how we get it delivered.
[00:46:09] Grant Kashner:: That's usually what I like to start with is. Either, you know, contact me, go through our website and let's get you a demo. So will you wanna [00:46:16] Dr.Grant Garcia: put the website up one more time? There you go guys. Yep. You have a,
[00:46:19] Grant Kashner:: A form on there you can fill out. And again we like to start with a demo. Just to make sure you know, you like our company, you like our product, right?
[00:46:27] Grant Kashner:: We we align well, and then from there we can figure out kind of all the details in the middle.
[00:46:33] Dr.Grant Garcia: I like to say if you guys, if you guys liked it from the podcast, make sure you drop the podcast in your likes. So that grant knows, you know, you heard it on here so you have some background information.
[00:46:42] Dr.Grant Garcia: So again, you heard it from us here. Go to the nice recovery if you're interested and let 'em know what what you want to know. 'cause so I think practice and Dr always
[00:46:50] Grant Kashner:: go through you and you can connect us. You know, we, you know how to get ahold of me, whatever works as well. So yeah, whatever works. [00:46:56] Grant Kashner:: That's awesome.
[00:46:56] Dr.Grant Garcia: Yeah, you guys can reach out to us at wws sports do com. Doc. com. If you're [00:47:00] curious again, all outlets, we like to make sure I listen, I'm a competitive guy, but if every single person in the whole world got, got access to all this stuff, that's all I care about to me. I care. Number one, that your patients get this and they have access to this.
[00:47:14] Dr.Grant Garcia: I get no benefit from selling nice machines. All right. I'm getting no cut from this. I just think it's such a good idea. And like, I care way more about all this technology, you know, 99 percent of the stuff I talk about a hundred percent, I get no cut on it, but all I care about is that the patients get it.
[00:47:28] Dr.Grant Garcia: Do better. And they hear about this stuff and that, you know, either they come to me and offer it, or they go to somebody else that can offer it again. I'm not here to ask you that the only person that offers in the world is someone like me. There's tons of people that can offer it and anybody can. And so it's really important for people to know that.
[00:47:43] Grant Kashner:: Well, no, and I, I appreciate what you guys are doing here and sorry. Well, you can, but. I always tell people, right? It's the information's free, right? The, the app, you know, the the implementation is where it costs you. Right. But you guys do such a good job of being subject matter experts on [00:48:00] the information side of this niche that we're in that for patients, for surgeons, for, it just adds to your brand and your, you know, your expertise, right?
[00:48:10] Grant Kashner:: It's like, you know, about all the other elements of surgery around it. So obviously you probably have studied exactly what you do very well too. Right. So that's where I think, you know, apart from, you know, there's no monetary benefit, but you're the, the, I look at it and I say, wow, you know, from a patient standpoint, that would be a surgeon that I'd want to go to, and I've had five orthopedic surgeries myself, unfortunately.
[00:48:37] Grant Kashner:: So I look at the docs that are really pushing it because I'm like, They're really looking at all the elements for the patient, not just cutting, right? They're really looking at the holistic approach, underst, and that is so important in today's day with. With surgery and with the patient, you know, with, with the patient satisfaction.
[00:48:56] Grant Kashner:: So that's all I'll say on that. You guys are doing a great job. [00:49:00]
[00:49:00] Dr.Grant Garcia: We got to keep this. I knew we were going to go to an hour. Will, every time you say we're not going to go to an hour, we're going to go to our, we got to have one more last quick thing. We got to get Grant out of here. Show us the new technology coming really briefly.
[00:49:11] Dr.Grant Garcia: And then we got to go.
[00:49:13] Grant Kashner:: Okay. So this is coming soon. It's our first retail product. Quickly. The on the most efficient way. To, to cool. To cool. Your core temperature is through special nerve endings, which are in your, the palms of your hand, the bottom of your feet, and the back of your neck, right? So long story short the only reason that your muscles fail.
[00:49:36] Grant Kashner:: Right during workouts or, you know, running, sprinting, lifting, everything is because of heat, right? They get too hot and the heat causes them to fail. So if you've ever done a set of bench press and you feel that pump out feeling, it's because ATP is, it is not being delivered to the muscle anymore because it's too much heat being delivered.
[00:49:55] Grant Kashner:: So that being said, what this does, it's called the rock, right? It's a [00:50:00] palm cooling device. And again, there's so much around palm cooling on Huberman, Rogan you know, Dr. Craig Heller out of Stanford across the board, everybody, you know, all the girls basketball teams in the final four, the Duke men's basketball team, baseball team, everybody's using palm cooling because of the performance benefits.
[00:50:17] Grant Kashner:: So traditionally on the market, there hasn't been a good delivery of the product, right? So what we do really well is we deliver precise colds. In a very slick and innovative product that does it very well. So the, the rock does that it gets to a targeted temperature and stays there and the performance gains around it are insane to say the least.
[00:50:39] Grant Kashner:: So everyone we've given it to, it's been. We're, we're, we're, we're, you know, we're trying to keep it behind the curtain before we do a full launch on it, but you guys are the first, not anymore. Now to actually see, I know you, you're the first ones to actually see the product, so
[00:50:55] Will Sanchez: there you go off and running there. Before we before we wrap it [00:51:00] up and, we want to promote and go check out nice recovery dot com. And if you do go to the webpage, please check this page out and try to explain to everyone what is going on here. With all of the dogs before you grant. What is happening on your web page for those that can't see it, the entire team, including Grant and Michael Ross, the founder, they all have this beautiful dog in their hands and this is their picture, their team picture, their individual picture.
[00:51:36] Will Sanchez: Whose idea was this? How did this come about? I have to know before we let you go.
[00:51:41] Grant Kashner:: So we no, it's great. Right. We, Michael, our founder, right. He's he, he loves to, you know, kind of do things, you know, kind of a unique and special, you know, kind of way. Right. And he doesn't like to do things stuffy and didn't, you know, he wanted to put team pictures on there in a way that really [00:52:00] represented our company well, and he got a puppy.
[00:52:02] Grant Kashner:: And the puppy is obviously as, you know, as cute as it gets. So we had a round of pictures with the puppy. And yeah, it's been a big we actually hear a lot about the pictures. So I think, you know, we're a boulder company, so we're very into our animals. You know, we have, we have, We have dogs in the office frequently.
[00:52:21] Grant Kashner:: So it just kind of fits our brand and we want it to come off as like, you know, it's like, we're a patient we're, we're, we're not a stuffy medical device company. Right. We'll, we'll actually talk to you like a human. We'll ask what you're like, what surgery you haven't done. Right. What's, what's going on?
[00:52:36] Grant Kashner:: Do you have somebody taking care of you? What do you have somebody, you know, like, like we actually care about the, like. You know, the the details. So having a puppy kind of, you know, I guess shows that we have at least a softer side and we're not you know, a traditional medical device company. We, we love
[00:52:52] Will Sanchez: it.
[00:52:52] Will Sanchez: And we thank you so much. Grant Kastner CCO at nice recovery system. Thank you for taking some time and being a part [00:53:00] of the show. We really appreciate it.
[00:53:02] Grant Kashner:: Yeah. Thank you guys. This was this was great. So I, I really appreciate you guys having me on.
[00:53:08] Will Sanchez: Dr. Garcia. What can we say, man? It was absolutely fantastic.
[00:53:13] Will Sanchez: Having Grant on and we're listen, man, we, we, well, we say we do it less than an hour, we got to get to less than an hour, but there's so many great things to talk about. We have so many great guests that is hard to, and you know, it's just one of those things, but we both love the product. This was easy.
[00:53:31] Will Sanchez: This was like. No homework needed for this show.
[00:53:34] Dr.Grant Garcia: So much homework on these shows, but not this one. This was,
[00:53:38] Will Sanchez: this was an absolute layup. I don't know how we coordinated with all the green that's going on. That's not Celtics fans.
[00:53:44] Dr.Grant Garcia: We're not Celtics fans,
[00:53:45] Will Sanchez: Celtics fans. And as we wrap it up, man, we always like to let everybody know, check us out at sports.
[00:53:51] Will Sanchez: talk. com. You have Dr. Garcia's face there with a nice little purple tie represent his, his colors. But more [00:54:00] importantly, we have our podcast.
We have our transcripts of the show. We have absolutely everything. He mentioned that you can find information on the nice recovery. com. All of that stuff. So, I mean, who better to explain it?
[00:54:13] Will Sanchez: Last words, Dr. Garcia, because I'm going to jibber jabber all over the place. How do you want to wrap up this show as we say goodbye?
[00:54:20] Dr.Grant Garcia: Well, first off, it was awesome guests. And as usual, we got close to an hour and it was just too much fun. The product's awesome. You can find everything, like you said, on our website and you hit, there's a link that goes to my main website and you can find the recovery shop.
[00:54:35] Dr.Grant Garcia: You can find my accelerated recovery stuff and we'll have this podcast. For the nice, in addition, you can find ways to access it and, you know,purchase it and find their website. We have, we want to make this easy for patients. We want to make it easy for surgeons. They want to get involved. Again, no cut from us.
[00:54:50] Dr.Grant Garcia: The key here is just so you get the best possible options and you hear about the products. Again, all orthopedics, all sports, all the time. That's what I want our patients to have and hear the most [00:55:00] cutting edge technology. So thank you.
[00:55:02] Will Sanchez: Yeah. And think twice before you give the nice recovery nice package.
[00:55:05] Will Sanchez: I, I should have just kept it and just avoided his phone calls. That would have been the smart way to do it. Now I'm all disappointed. Thank you, boys and girls and everyone else. We had a great show. Thank you for listening to sports doc talk. Thank you to our guests, Grant Cashner there and nice recovery.
[00:55:23] Will Sanchez: And we'll catch you next time. Bye. Dr. Garcia. Audio Transcript
ACL Injury, Surgery and Biologics

[00:00:00]Welcome everyone and thanks for listening or if you're watching on YouTube. Thanks for watching and listening to Sports Doc Talk. I'm Will Sanchez along with Dr. Grant Garcia. Dr. Garcia, what is this? It's just a party of two. Normally we've been having all these great guests and uh, and today we get a chance to uh, Catch up, do a one on one and really kind of do a topic that is near and dear to your heart.
[00:00:30] How are you, Dr. Garcia? I'm good. I'm, you know, we've had, like you said, so many good guests, but you know, it's time for us just to hang out. You know, we haven't done this in a while. You used to do this pretty much all the time. Uh, and we've had some phenomenal guests. Um, and you know, people were getting tired of just hearing me and you talk all the time, but I FaceTime.
[00:00:49] So this is good. Uh, this actually, this topic, Um, while near and dear to my heart and we get lots of patients asking about it, it was actually a patient [00:01:00] request. So we had someone go through the website. You've seen we've had a couple of those we've presented on recently since we've had the new sports stock talk website and you know, the patients actually, uh, it's actually a patient of mine, um, but they went separately through the website to ask this question and I thought it was really good because.
[00:01:17] Especially the patients for me, you know, we see a lot of local patients. We have patients that drive three or four hours and then we have patients and this patient is actually from out of the state. And so they'll come from out of the state and they want, they want something different, right? Like, you know, They don't want to fly up for surgery and say, Hey, listen, I want to go fly to you.
[00:01:34] You know, you do, you do a decent ACL or whatever, but they want to know like, is there anything else you can do? And in some cases there is sometimes there isn't, but they, you know, they want to ask those questions, right? Cause they haven't, they feel like there's more out there. They've done research, they've done Dr.
[00:01:48] Google, which we know is never the best thing. Um, but it does help in some, it does help in some aspects because I think the problem you have is you don't always know what you don't know. And you don't know what the surgeon doesn't want [00:02:00] you to know, or you don't know what's available and what options are.
[00:02:03] We've already seen different ways of doing ACLs. We've seen different ways of doing ACL repairs. I mean, even in the city of Seattle, if you went to three different doctors, two of them may never even bring up the word repair. And so it's important for people to have all these information. It's also why it's important for second opinions.
[00:02:16] But I think the point here is biologics is in its infancy. And it also matters about how you ask the right questions. So the thought is, you know, they've heard about the repairs, they've heard about bear, they've heard about ACLs injuries. They've read about this thing called bio ACL, which we'll get into in a minute.
[00:02:33] And we've actually talked about on the show, just a different name. Um, You've heard about bone marrow, you've heard about PRP. So we're gonna talk about like, how does it all integrate together and kind of work our way down from the basics to more complex. Um, and hopefully the listeners will learn a little bit on the way.
[00:02:48] Yeah, it's, uh, like we said, it's right up your alley and, uh, you know, talking about, uh, you know, our ACL injury surgery and biologics, uh, event. And as we get it right before we get into that though, I'm kind of backtracking a [00:03:00] little bit here. You know, we're six months into the new year and we had, uh, you know, uh, Dr.
[00:03:06] Acevedo and Bashai and, uh, uh, Dr. Jazieri and, and, you know, with his peptides and different techniques and, uh, whether it's Leah Winter, which was at the end of 2023 before we started 2024, uh, just kind of reflecting, uh, already just the tremendous amount of shows and, and we have some great guests lined up.
[00:03:29] As we, you know, Oh my God, head into the summer. And next thing you know, it'll be fall again. And the kids are off to another grade and, but I'm getting ahead of myself. So let me just kind of slow down a little bit, but I think it's just a great reflection to just to thank the audience members, to thank our guests.
[00:03:45] That have listened, watched, and been a part of the show that have reached out that want to have these conversations. And we just want to thank you. And whether you're watching us on YouTube, check us out on Spotify or Apple or any of your favorite platforms. So I'm just giving a [00:04:00] quick, you know, tip of the hat.
[00:04:01] And if you're watching right now, I'm tipping my little hat right over to, to all the fans and guests. And just thank them, uh, anything that you want to add there before we get into talking about ACLs without surgery and all this good stuff. Yeah. So, I mean, it's just. Yeah, the guests have been phenomenal.
[00:04:18] We have more to come. You know, I think one thing we've heard, I've heard a lot from actually from other orthopedic surgeons I've talked to, or other people in the industry, medical device companies, et cetera. What they like, I think most about the podcast, which we didn't think about originally was, While it's all sports, all orthopedics, that doesn't always mean surgery.
[00:04:37] We're talking about innovation, nutrition, talking about how other people deal with interpersonal stuff. I mean, Acevedo and Bechet are two of some of the best surgeons I know, and they didn't spend most of their time not even talking about the surgeries. We talked about how you prep for surgery, all the behind the scenes stuff.
[00:04:53] I mean, this show is keeping it real. You've heard so much stuff that you will not hear on many places and [00:05:00] getting to hear how it works behind the scenes. We had the tech. You know, the tech show, obviously with us, you know, that people don't even hear about that stuff, right? You may be here to the cocktail party.
[00:05:09] If you happen to run in and be, be with a surgeon, they've had a few drinks. Maybe they'll tell you the truth. Um, but you know, the, the thing is it's, it's a really exciting, um, and there's more to come and you're going to see other things that you're not expecting. Right. Other guests that are, maybe you're not surgeons.
[00:05:24] Right. That are going to come in and they're going to have topics that are, that are important for orthopedics or sports, but maybe not always surgery involved. So anyhow, we're getting off topic again, like we always do. And we're trying to keep, that's okay. It's part of what we do, but going back, Hey, check out the tech trends unveiled.
[00:05:39] That was a great episode. And let's give a shout out to Dr. Schaefer. Right? He was another guest that we had on. Just so many. So if we forgot anybody, just, we're always thinking about you. But right now we just, you know, kind of jumping around, but let's talk about this ACL injuries, surgeries and biologics.
[00:05:57] And the first thing, when you sent your notes over to [00:06:00] me was like you, like you mentioned, to start the show. This was a request. This was someone that wanted more information about it. So when we talk about A. C. L. Injuries that heal without surgery, um, can you start with, like, primary repair? Like, what does that entail?
[00:06:17] When you when you think about Or, or when you're discussing primary repair when it comes to these ACL injuries. Perfect. So we'll go one step back further. So there's a lot of hype. You may have seen the articles. You're looking at your Apple news and you see ACL repaired without surgery. Magic, right?
[00:06:34] They'll get like 200 MRIs. It's usually a European, European study and no offense to the Europeans, but you know, they, they, they tend to have, it tends to be, I know a different different data sets, at least for some of these things. Um, and it's in a journal you've never heard of. And they're saying, hey, they repaired all these ACLs.
[00:06:52] You gotta be really careful about this because it's someone that does a lot of ACL repairs now. Um, you know, when I get in there, I pretty much I've never been in one where I get in [00:07:00] there and all of a sudden the ACLs completely stuck to the wall and I don't have to do anything to just kind of attach it like we talked about with the tightrope and it goes back there.
[00:07:07] I mean, I was had one last week and I said, there's absolutely no way this would heal on its own. You know, these ACLs, they were tracked. Imagine like recoil, right? There's a springiness to the ligament. And so when they tear, they recoil. So while they're still stuck on the wall of the, the femur, they're pulled back.
[00:07:23] And when you stretch them out and retighten them, it's amazing to see how they go right back into the orientation of when you see a normal ACL. Because we do a lot of surgeries on people that have normal ACLs for other reasons, since we, we know what it looks like anatomically to be normal. And so you got to be really careful because the idea of it healing is not the case now maybe in patients with partial ACLs.
[00:07:44] So that's a different topic and we're not going to go too much into it. But partial ACLs or sprains are actually fairly common too. We see probably, I would say maybe out of one out of every ten ACLs I see is a sprain. Now again, I'm seeing more surgical ACLs. It's a bias to come to the surgeon with a [00:08:00] surgery ACL, but people that sprain their ACLs, we see a lot, especially my team, you know, Tim, the teams I cover and everything, because they're coming to me regardless of whether it needs surgery, um, these partial ACLs where it's like either a partial bundle or it's just a little bit of a stretch, you know, those are ones that sometimes can get away without surgery.
[00:08:18] And I tell patients maybe 30, 40 percent of patients may need surgery at some point and sometimes it's lower, you know, you never know, it depends on the amount of injury and that's where biologics, you know, such as potentially PRP, which is where we take your blood and spin it down or bone marrow. We take bone marrow out, maybe helpful again.
[00:08:36] We don't have a lot of data on it. They've looked at ACLs and PRPs for sprains and the data does show that some studies show there may be some slight benefit. And others show nothing at all. So it's something to be aware of now doing PRP when you acutely injure it. There's no downside. We'll talk about these biologics.
[00:08:54] There's no downside to biologics except for the cost. And not covered by insurance. Like me just really, it's the platelet [00:09:00] rich plasma, which is the PRP. So if anyone's listening, doesn't know what dr Garcia is mentioning, uh, like myself, as I'm, you know, I'm just a, uh, doctor on the radio here, but platelet rich.
[00:09:13] plasma. Um, for the PRP people out there. So I'm sorry to interrupt Dr Garcia. Go ahead. No, that's perfect. And that's a good segue. You get, it's important to mention that. So anyway, so the PRP or the platelet rich plasma, the bone marrow aspirate, which is from your bone marrow, like your hip, your knee, you know, we can take it from all different places.
[00:09:29] And the idea is in the acute phase, you give that to somebody and maybe to help them heal. Now, like I said before, data's mixed. So that's the, that's the idea. That's on the non surgical, maybe biologics options. And that's something that people can try again. There's no downside except for the cost. So, you know, depends on the place you go.
[00:09:46] But there's a cost these things and they're not covered by insurance. So if you have to be aware of that, you know, that does change the aspect and that's important to bring up. It's just like the Tech trends, you know, all these sexy biologics we're going to talk about. They are not covered by [00:10:00] insurance and it's different than like implants.
[00:10:02] So like if you have an implant, it's all bundled in the price, right? So you can basically like sometimes it's more expensive and it's something that won't, it can't be done because it's just too expensive. The surgery won't cover it. Your insurance won't cover it. And there's no way to get around that with biologics.
[00:10:18] It's never covered by insurance and there's no way to get around it getting covered by insurance because basically, They're expensive to do. And so the patient has to be on the patient's own as to do it. So understanding all this stuff sounds really great when it comes to the biologic side, but people who ever get these are paying out of pocket extra for them.
[00:10:36] Real quick. Is that something also that the insurance can, uh, find a way to excuse saying, You don't really need this or you might not need this. We can treat this differently. It may not be at the level of biologics, but you know, fine. We can put a bandaid on it. It might not be the, the, you know, nice H wrap band to hold it together, but [00:11:00] it's still as effective.
[00:11:01] Is that their way of kind of working around, you know, uh, paying for some of these things? Yeah. So the, the, we still use codes, like I told you before. Yeah. Uh, for these, these biologics as a PRP code, there's a bone marrow asper code, but they're considered experimental and Don't get scared by the word experimental because it doesn't mean you're being experimenting on and no one's ever done this before It just means that's the insurance company's way of saying we're never paying for this There's not enough And and the good news for you is you can actually pay for it because in some of these things Yeah, we've talked about some of the implants They're so expensive that an insurance company will never pay for them by contractual rules.
[00:11:38] You're not allowed to pay extra So then you're just, you're just stuck. You just don't know. You just never get it versus this. At least you can get off. There's no contractual rules that you can do it. So that's the one thing. And it's, they're really safe. I mean, there's no downside. Like I said, to most of these things, except for the cost.
[00:11:54] We're getting sidetracked on that, but just to have patients hear this, uh, you know, that's how it works. Um, [00:12:00] but basically talk about repair. So, you know, we talked about this before and you could bring it up, you know, my favorite, which is the tight rope repair, um, for ACL. So, uh, Let's say you decide you want biologics or you're like, Hey, I want to biologics and I need my ACL fixed.
[00:12:14] Well, obviously in one of the, the, the, our, um, our request was how do you save proprioception? So the idea behind the repair, we've brought about this about a million times now in this podcast is that if you save the ACL, these patients, they, I'll tell you, I done a lot of these, I'm up to like 40 or more.
[00:12:31] And we just, we just flew down to San Diego to teach about this. So, you know, this is a hot topic. We fix them with this device. And they, if you know, when it goes on to heal their, they can, their knee feels better because of the proprioceptive things are saved, right? When we do a reconstruction and we're removing all of that, or a lot of it, as much as the doctor tells you to try to save as much, you can't really do a good ACL reconstruction by keeping the entire ACL there.
[00:12:57] So the idea is you're saving some of the proprioceptive receptors, [00:13:00] which is important for certain people. Um, if it heals and then, you know, there's less, less stuff that comes out. You're not making a big a bone tunnels. And there's less pain. You know, the patients are doing a lot. They're doing, they're feeling different.
[00:13:14] That being said, not everybody's a candidate, like I brought up before. I would say, I do a lot of ACLs, so I'm probably done, you know, if I'm doing probably one every six or seven, now my indications keep getting a little bit broader as I get better. Do more of these and I see, okay, this group is doing really well.
[00:13:29] I'm going to broaden a bit more. This group is doing really well. And I'm going to keep going slowly, so I do this appropriately. Because again, I told patients before, I'm not here to experiment, but I want to give them the cutting edge stuff. So, what people don't understand is they always ask, you know, they ask for biologics with this too.
[00:13:45] They're like, hey, what else can I do? Like, ACL repair, that's great. Like, that's old news. Right. We're onto new, new stuff. What's the newest thing you can do or what they don't realize. And you can bring up this little, the little pick device is that whenever time we do a repair, whether it's a bear, an ACL repair with the tight [00:14:00] rope, a combination of both, we'll get into that in a second.
[00:14:03] We use this device. This is a, this is a power pick. There's other ways of doing this too. And basically what we do is we make little holes. in the bone where the ACL and the PCL sit. And we actually do this for meniscus tears as well. And this brings bone marrow in. So it's actually covered by insurance, this procedure.
[00:14:19] So that actually is nice for patients because they're not paying out of pocket for the PRP, which is the platelet rich plasma or the bone marrow. And there are people that are looking at whether we can add more biologics. Can we add bone marrow, which you, you know, don't always get from just this alone that's concentrated or platelet rich plasma that's concentrated.
[00:14:36] And it's the same thing they've looked at with meniscus tears. Again, it's hard to show a big difference because this micro fracture thing causes improved healing as it is. So that's already, it's hard to show something that's as effective as this and biologics being better. Does that make sense? Yeah, I guess my question is, um, this tool is creating [00:15:00] the holes, right?
[00:15:01] And then what do you mean that it's promoting bone marrow? So you'll see, and we don't have a video to show you, but when I do this, you see a fat bone marrow coming out as you're doing it. And by creating a hole, now it's going in and then doing it's own, it's coming out. Coming out. Okay. So you're essentially going out into the knee and what it does actually simulates an ACL tear.
[00:15:24] Because we've seen when you, when you tear your meniscus and then you tear your ACL at the same time and you do the surgery at the same time, they heal way higher rates than if it just meniscus alone. So you want to simulate this ACL tear, um, and even if you don't, when you do a reconstruction or a new repair, you're not making as big of tunnels, you're not doing as much trauma, and so as a result, you want to still simulate this ACL tear.
[00:15:49] Fluid stuff coming in. So people will heal. So how does that risk your recovery by doing this procedure? Like you're, you're adding this, um, [00:16:00] uh, you know, lack of better word, kind of like simulating this injury in order to promote healing. That's a perfect exam. So I tell patients sometimes they'll have a little bit more swelling in the first few weeks, but.
[00:16:13] We also have tricks to reduce the swelling that we give patients medicine called TXA. So. It's negligible. The problem is, you know, if I have a something that's going to increase your success rates by 25 percent for a meniscus Yeah It's pretty hard for me not wanting to do that regardless if you feel swollen for two more weeks, right?
[00:16:30] Like any patient any person would say I would want that I want to heal better with the first time you try it then dealing with swelling for two or three weeks So that's really the that's the downside of doing this Uh, it's pretty low. Um, but people are looking at this. I mean, we're, we're looking at this.
[00:16:47] I work with, you know, I work with the Arthrex company. You've probably seen a lot of my stuff. Uh, you know, we're looking at finding ways to add more biologics. They're talking about putting collagen patches on to help the ACL heal. And so we're, they, we're [00:17:00] getting there. And one of the ones that does this is bear, you know, let's bring that up to like, we've talked about this before
[00:17:08] the thing, the thing with the bear here is people don't get is that they think the bear is the entire surgery. And we just posted our newest video. We actually use the Arthrex ACL tight rope. And then all we do at the end is slide the bear down there and add it. So the way that was FDA approved as a different type of technique, and we continue to improve this.
[00:17:29] If you look online, there's like 20 now videos out. All these are the top guys doing bear ACLs and each one of them does something different. So it's just wild because the idea of bear is literally just the implant. All it is, is the collagen implant soaked in whole blood. And put into the knee and then everything else they don't really like it's really not a step for doing that.
[00:17:48] Like the old technique, the FDA approved us great, but it's not as strong in my opinion. And so that's why I started doing the tightrope with them. And then I'll add the bear like I just did one a few weeks ago. And so what we're seeing with [00:18:00] that is that you're hopefully going to have, you know, you, you get the ACL to hold up to the wall.
[00:18:04] And then the bear implant, which is this collagen with, uh, you know, The whole blog, people are actually using PRP sometimes. And there, as soon as you know how this works, as soon as it hits the market, you have all these like smart surgeons that are like trying to figure out a better way to make it better.
[00:18:21] And they're all trying to tinker a little bit cause they want to find the golden ticket. Like which one's going to be even better than what's currently out there. Right. Yeah. And it's. I hate to say the word off label because not really because there's really not a label for how you should do this. Like there's a technique guide, but the FDA doesn't say you have to do it this way.
[00:18:36] They just want you to make sure you, you have to do a certain things that are, that are allowed, which is like, you know, soak the blood, put in the knee, lay the groundwork down. And then it's up to if you're going to be a little creative or what works for you. And then I'm going to oversimplify it for people that are listening to the show.
[00:18:50] They may not really understand. Think of you having a hole in the wall. Right? And then you're creating this compound, right? And it was stucco and you're [00:19:00] you're covering the hole to in order for it then to harden and heal correctly. And this is kind of what this bear implant, this bridge enhanced ACL repair is kind of happening.
[00:19:13] Obviously, I'm dumbing it down here, uh, and not to, to take anything away from it, but it's just kind of gives you a visual idea of what this, this compound or silly putty or whatever you want to call it, that's kind of holding everything together so it can heal correctly. Right? Am I wrong in that assessment there?
[00:19:32] You're pretty good on that. I mean, we brought this up before, but like the MCI, which is the ligament on the outside of your knee almost never needs surgery. And so what they're doing is trying to turn this into an MCL tear. So ACLs used to never heal. That's the thought process. And now we're doing more repairs.
[00:19:46] The bear's out. People are doing more bears. And the idea is that basically it causes clot that guides it to keel in a very, you know, we've heard of the word college and impregnated. Everything's college and impregnated. Right. The what about UCL internal [00:20:00] brace? We talked about this from the, from Brock Purdy and the throwing collagen impregnated suture.
[00:20:05] Well, in this, the FDA didn't have the internal brace. So now I do an internal brace. I do a tightrope and then I add the bear at the end brace. The thing you're trying ask your, the thing you're trying to ask yourself is, wait a second, you're doing an ACL tightrope, which is identical to the other surgery you're talking about, and all you do for the bear is just add the bear.
[00:20:24] And the answer is yes. So the problem is there's no head to head studies at this point because is it the bear? Is it both? What's ha what is causing this improvement, healing, or peer patients doing well? So, so there's no study right now saying, um, And this is all right. I'm going off track. I apologize. I like it.
[00:20:45] No, this is good. I'm talking too much. I want to hear your question. When you do a surgery and you say, okay, I did the bear. I did the tight rope. I did, you know, whatever I'm doing. And then I say, I did these [00:21:00] three different techniques for this. That's not going into, uh, some kind of database that they get, then you can have, you know, the recovery time, the patient, this, this was what happened and it goes into a national database where everybody's now kind of keeping track and or some kind of form.
[00:21:17] Is there nothing out there like that? Where I, instead of the FDA just kind of doing their own studies, but you know, the surgeons themselves. They are putting in the combination. Well, I only did the bear and I did the tight rope or I only did the tight rope for this one. And then you're seeing those comparisons based on the severity of the injury.
[00:21:37] Oh man, you were open up a can of worms. I love it. Well put. No, it's great. So, um, first off, those studies are expensive, right? So who's going to pay for them, right? Like, are you going to have the search? Google docs. It's not, no, because you got to get permission for the patient, right? Like, it's not like I can just throw in HIPAA.
[00:21:55] Yeah, technically. I mean, uh, technically a study where no [00:22:00] patient's information is given out is, is okay. But what about within your office, right? Or, or your doctors or still has to be approved. So to be approved, I can't start logging a spreadsheet, like a whole, like a, there's like a committee that has to like, look at this and I'm going to talk to the committee.
[00:22:16] Can you take me to your next conference? I've got a couple. I will. I will. So, so basically we're going to try not to get too off topic here, but basically the idea is it costs a lot of money to keep systems to do that. And we're getting there. Bayer has their own reps, the people that bring the implant and they ask questions about the surgery, like when did the Powell was the patient, when they get injured, how they choose you.
[00:22:36] They ask all those questions. They keep track of it. And every six months I get a message from them with the entire national information in it. It's all confidential at this point because they're, they got what they want to publish it and make it, you know, peer reviewed and, you know, fully, fully reviewed and checked out, but yes, the answer is, it's really hard to do all these in certain places.
[00:22:53] I'm prior practice, so I don't have a lot of research assistance, you know, and I don't have fellows, but a lot of places I've worked, HSS. And, [00:23:00] uh, rush their machine so they would have someone in the hour like writing everything down patient when they signed 15 consent forms. One of them is the IRB. So they're illegally allowed to were allowed to keep their information and follow it.
[00:23:11] Um, so yeah, I mean, you can and you can track it retro. You can track it afterwards. There's different. We can look up codes and stuff of patients. And I've done that before. And then you can call them a two or three years later and see how they're doing. So we're going to get there. We're just not there yet.
[00:23:26] And this stuff so new. Um, but you're going to see more things coming out of the pipeline, but imagine surgery comes out, you need at least one, two years, if not three years after the surgery, because you gotta make sure enough of the surgeries have been done. So we're just not there yet, but this comparative study is a really interesting one, and it's something that some of the companies are thinking about.
[00:23:42] So, one of the things they've been doing with the bear, It's actually grinding it down into the, because you may have seen it's like this big honking piece of collagen and then you put stuff on it and then it starts to get gooey and you put it in the knee. Some guys are grinding it down, soaking it with stuff and then just squirting it in the knee.
[00:23:59] So it doesn't, [00:24:00] there's, we're finding other ways to deliver it to you and that's another like, You know, maybe off label, but that's a biologic thing is like, is this just the, is it just the, it doesn't have to be the actual implant size. It's just the stuff in the knee that you can get in there. Okay. And it's always going to be kind of like a silly putty, right?
[00:24:16] You're never going to throw it into like a, uh, a NutriBullet and grind it up and then sprinkle it in there and do some kind of concoction. You never know. You never know. And, and, and one of these questions we always have is, can we do, well, how do we keep it in there? So the word collagen, like a lot of these different things we talk about.
[00:24:33] They're, they have a, they have something that brings it in. It's a conduit. So that's the idea behind this collagen thing is it can soak up the blood and then it starts to create clot formation. Um, and yeah, everything's about conduits. Like if you just push stuff in the knee, it just like floats around and disappears, right?
[00:24:49] Like the idea is like, that's great, but with some of these things you want a delivery system. And so that's where this becomes challenging because then you start talking about manipulating biologics. And then that technically is [00:25:00] FDA. Oh geez. Put some balloons on there. That's exciting. So manipulating, you want to be careful.
[00:25:06] So you gotta, you gotta stay with it. And I think you got to stay with the new limits. I definitely think they put the balloon. Anyhow. So we, uh, so that's, that's it for the ACL repair and biologics. Oh, that was perfect. Let's see if we can do it. Will it work? I'll try one more time. Air quotes. It's not working.
[00:25:25] No. Maybe we'll get better. I think everything is better. We should end every segment with balloons. So I think that is perfect. No, it's, uh, it's fascinating to think about that. And it was interesting because, you know, you obviously made the point that you needed to stay, not just put it in there, but to stay, because, uh, you know, my first visualization of when I was making the joke about, you know, grinding it up and Nutribullet is like, you know, if you ever had a wound and you put salt, In the wound, you see it bubble up, right?
[00:25:58] And it starts to, you know, [00:26:00] obviously it's painful and things like that, but it bubbles up and kind of kills everything. You see everything kind of happening. I was just having this vision of you sprinkling this, this concoction into, you know, the knee and, uh, And who knows what works. But anyway, we get, we get sidetracked.
[00:26:15] Um, let's, let's move on. And I know we were talking about the key components, benefits of the Bayer implants and ACL. And, uh, you wanted to jump into, uh, ACL grafts and things like that. Yeah. I mean, so, you know, one of the guys, uh, the listener patient is he's already had an ACL done. So he's wants to know more about the graft options, right.
[00:26:35] Cause the repair is sexy, but You know, there's a lot of ACLs that are done and people have an injury again and they want to know what to do after it, right? Or there's people that can't get their ACL repaired, right? Like, the idea of the ACL repair is very sexy, it's very cool, but it's not for everybody.
[00:26:47] I mean, it's like less than 10 percent of patients. And so it's just most patients are never going to have that option. Dr. Justin Marchegiani Wow, I did not realize that, why is that? Dr. Brandon Miller There's some people pushing the envelope, but it's [00:27:00] really the certain pattern of tear. It's got to be torn off the femur.
[00:27:03] Um, if you look at it, you know, I can't remember the exact data, but it's like maybe 10, 20%. And maybe we should be repairing a few more of these and we're starting to get better at it. But, you know, I'm a surgeon that pushes the limit. I do probably the most repairs in Seattle. Uh, if not the whole area, um, I teach on this and I'm still not comfortable trying to repair all these ACLs.
[00:27:22] It's just, we're not there yet. But you have a program of rehabilitation anyway, also. Yes. And I'm a proponent of all these things. I'm a proponent of reconstructions. I'm a proponent of all these things. It's just, it's important for the listeners to understand. So, I think the important thing you should understand is it's not just like adding biologics and doing, so let's move on to the ACL reconstruction because that's actually the more common thing.
[00:27:43] So, you know, let's say your surgeon doesn't want to repair it or it's not a repairable tear. Well, majority of them get reconstructions and when you get a reconstruction, there's three things you got to figure out a way to improve if you want to, if you want to get someone back faster. So like all of this is like, people do this, people are worried [00:28:00] about their graft healing, like the grafts will heal.
[00:28:05] It's just a question of how long it takes. And so that's the thing that people, I think people are worried. They think that if they're going to get biologics, that they're going to basically, they're going to heal way better than anybody else. And then they're not, they're going to get back faster or they're going to get back, uh, and have a stronger ACL.
[00:28:20] That's not the case here. There's some things we'll talk about that may add some structural integrity to it, which we've mentioned before, but really it's about speed, right? Like if I could do an ACL on you, the reason people want the ACL repair is it's faster recovery. Not the bear. You've got to follow the protocol, but the repair tight rope, people are back faster.
[00:28:37] And so that's why they choose it. I mean, it's, I literally I'll offer it. It's like 95 percent of people. So this fertilized ACL is a perfect point, but you want the graft to heal to the bone faster. So it depends on the graft option. You've got patella tendon, which is bone. So that'll heal versus other tenant options, which is what the fertilized ACL is.
[00:28:55] And then member, you're taking a tendon out, which is a tendon is a bone to [00:29:00] muscle attachment. So you've got the hamstring tendon, you have the quad tendon. There's a few other options too, but you're putting in, you wanna make it into a ligament. So a ligament is where it's attached to bone on both sides.
[00:29:12] And so it's gotta go a process where it goes ligamentization, where it basically turns into a ligament, and then you wanna make sure it doesn't tear as it's getting bigger and better. And so the idea is if you can make it heal faster and you can make it remodel faster. And you can keep it safe and stable.
[00:29:30] Then you've come up with the perfect solution. And so the idea behind this fertilize HCL, which we've heard about it, you actually interviewed, we talked about it and then actually was a couple of years ago and then Chad Lavender reached out to you, you had a whole topic with him. And so, you know, maybe we'll have you be a great guest to have on at some point.
[00:29:48] Now, yeah, Adam Marshall, you know, he's, yeah, he's, uh, And, and he's a sports guy too, so it'll be interesting. Uh, you know, maybe he might be a good one for the fall as we get into football [00:30:00] season. He'll be excited for college fall for sure. I think I added him to the list. This would be great. Yeah. So typical ACL nine months to a year to get back.
[00:30:07] And so what, uh, Dr. Lavender, Chad Lavender has done is something called the fertilized ACL. And actually my, um, my, uh, patient asked about this. It's called. For Arthrex company itself, it's called bio ACL. It's the same basic principle. And so what they do is they take PRP or your own blood and they put it with, you know, uh, allograft bones called mineral bones.
[00:30:29] So the hope, the key is to hopefully it's a conduit. So it's like soaks it up and then they inject it into the tunnels. And then they can take some of your own bones. So they have this, this device that as you shave, it sucks bone up and it filters it. Imagine like a, um, a pool filter. And so the bones all mixed up there.
[00:30:45] It's your own bone with some other bone and then the PRP, and then you can inject it in the tunnels and the whole, and what he is trying to show is that patients will get the bone to bone healing bone to tendon healing faster. And then potentially the ligament [00:31:00] is faster and so therefore they can get back faster.
[00:31:02] So he has looked at some studies and shown some patients that have gotten back at six months with this. Now the caveat, which if you look at the studies, and I know we've done some of these, is he's had some trials where he's had really good results, but some of the trials, not all the patients came back for the follow up.
[00:31:22] And so you've got to be a little careful, right? Because Who's the most likely patient not to come back to a follow up?
[00:31:31] I don't know, would it be a young person? Probably someone who's not happy. Right? If you're gonna get called, and all of a sudden, in two years. So I'm not, it's not that his data is not accurate. I totally, I, I think it's awesome what he's doing. I'm, I'm all for it, and I think it's legitimate. But the, the, the, the, the You know, if you, when you start losing followup at two to three years, you have to be say, Hey, listen, is this, is this, uh, is, are all of these patients, did you lose followup because they left the state and that's totally legitimate?
[00:31:58] And that happens all the time. Like [00:32:00] there's, it's really hard to find if you're doing surgeon and people and they're flying in for surgery, that they're going to call you back or listen to the pickup, right? That doesn't mean that you just have to have a little bit of a healthy bias. Or healthy skepticism and say, Hey, listen, this is pretty awesome what they're doing.
[00:32:14] They are getting patients back. I mean, I've seen promos for this, uh, you know, it's pretty impressive. And these patients, you know, we talked about this, they're, they're returned to sport function. They're 80 percent of normal compared to 35 percent for regular ACL. They're functional tests. Um, yeah. They're 80 percent of the 30%, um, and their CT scans, which is cat scan, where you look at bone, show that they had less tunnel widening and they're already starting to form bone around the quad tendon.
[00:32:39] Now, again, this is only for one type of ACL, which is quad, which is where you take a piece of your quad. It's not for patella tendon and it's not for hamstring, which are actually way more commonly done ACLs. And so it's something to be aware of too. It's only been tested on one type of ACL. So there's a lot of caveats to this, but it's really cool because he's addressed everything that we're concerned about [00:33:00] and he's pushing the envelope because no one's willing to do this.
[00:33:03] I mean, he's just, he's, he's letting these guys rip. I mean, he's releasing them to full activity at six months. And that's terrifying because if you have a kid tear their ACL at six months after you let them go inadvertently is that's that's really traumatizing, right? And he's a surgeon. I mean, as a prior practice surgeon, I don't know if I get away with that.
[00:33:24] Like I'd have to, I have to see some data before I did it. Just cause, you know, patients would immediately tell everyone, you know, my surgeon let me go at five months and they'd say, he's crazy. Right. And like the ACL repair, I had to slowly integrate it in. And I had to see how the first patient did second patient.
[00:33:38] Okay. I'm going to let more and more do it. And he obviously has gone for the gusto. So I have only utmost respect for someone like that. It's something that patients would be aware of. So this is a biologic option. So we do your ACL, we add either bone marrow or PRP, one or the other. And then we do this putty, which helps grow it in faster.
[00:33:57] Okay. And it's a little bit technically challenging too, um, [00:34:00] and the idea is you do it all but doesn't go inside the knee, right? Just stays in the tunnels. So you know, and there's, and there's a certain way they do it too. It's a, it's a different technique than some of us do for the ACL. So you've got to do everything exactly as a study or you're technically not following it.
[00:34:12] The protocol. Yeah. Does that make sense? Yeah. So it's a, it's, it's really good. I mean, it'd be nice that this needs to be expanded basically. It needs to be expanded for other surgeons because I haven't seen, when I was looking up for this show, I looked up fertilized ACL or bio ACL and he's the only one that's published about it.
[00:34:27] And so it would really be nice to see someone else who didn't invent the technique showing good study results as well. So there's a lot more work to be done, but this is something really interesting for patients and it's definitely a viable option. I think it's totally legitimate. I just want to see more information.
[00:34:41] Yeah. I mean, it's, uh, it's really interesting. Uh, and just to think about, you know, we were thinking about this, uh, this mix that we've been talking about for now, uh, for a while now. And how does that evolve? Yeah. Right. Does that keep evolving to, you know, finding the right [00:35:00] mixture and, you know, whether it's, you know, holding, not holding soft or harder, you know, like how that affects certain things, but obviously, um, you know, you do test on cadavers and things like that.
[00:35:12] Is there a way to kind of expanding on this quote unquote kind of silly putty that you're utilizing, uh, to fill in the gaps on, you know, just cadavers or do eventually you need to have. You know, real folks to get real data, uh, going forward. If you're doing different mixtures, kind of a little bit on conversation right now.
[00:35:33] Yeah. I mean, the nice thing about this is that none of these things are dangerous. They're doing other than like, you know, the idea of dangerous is like, you know, something that's not approved for patients, but all this stuff, like the putty, the PRP, you know, Yeah. Uh, everything I talked about, we put that in me all the time.
[00:35:46] I just, I did two of these today. Like I added putty and I added PRP and patience today. Like it's a little, I got to say putty too. You're going to be saying putty to everybody. No, but it's called, we actually call it. I go open the putty. It looks like putty. It looks like putty. [00:36:00] So all of these things we're already doing in the knee all the time.
[00:36:04] And so what he did is found a concoction that works for him. He kept it regimented. He documented it. And then he looked to push it to the next level. And he did everything right. MRIs, CT scans. Watch the players getting ready. The one thing that you got to understand though is they probably had really good physical therapy and probably therapists that were willing to let them rip.
[00:36:24] Right? That is incredibly important. You stole my thunder, I was about to say that. No, keep going. You know what I'm talking about. I was going to ask you, I was like, wait a minute, this all tells me in order for him to say, Hey, six months, go. What kind of physical therapy are they getting? Is it once a week or they're in there, you know, mandatory?
[00:36:42] How many days, right? So that's the even bigger conversation now besides the surgery is right. Because we talk about it, right? You know, hand in hand, your physical therapist, the homework, when you go home, how much are you working? How much are you doing? You know, what's the requirement? If you have this type of surgery, you want to get back at six [00:37:00] months while you're seeing your physical therapist three times a week.
[00:37:02] So, you know, these are, you know, mandatory. You know, questions that you would like to, to, uh, to know besides the procedure, what's really going into it. What's the Molotov cocktail in order for you to have success. I think it's a perfect point. And I mean, remember I do ACL repairs. My patients still come in slow sometimes because PTs are so nervous, they've never seen this protocol before.
[00:37:24] So like, these are probably finely tuned for the clinical trial. Right. They saw the same therapists who did all of these. And so that's where you got to be careful. Can you extrapolate this general population? I mean, if I'm operating on, I have a patient, she, she flew in from Montana for an ACL repair.
[00:37:39] Like I have no way of dealing with her physical therapist in Montana, right? I, we have patients that come in. I can't, I can't. I have to have a surgery that will, that they can follow my protocol, but they're still nervous. I mean, even some of my regular ACLs, if I'm more advanced than some other surgeons, or I do something differently, they still want to keep it their own way because they're nervous.
[00:37:59][00:38:00] So they also, they don't want to be responsible. They feel responsible. The person tears their ACL to at six months to a year. Are you doing video calls for out of state folks after a post op? I usually will just do phone calls. Uh, the video I find doesn't add a lot of value except for just looking each other in the camera.
[00:38:17] And it's really hard because I can't just FaceTime them because of the HIPAA. So I have to use like a program. And so then if you have to schedule it, we used to do video calls during the pandemic and we've stopped because it's really hard to schedule stuff for patients cause they, they want to be called at a certain time.
[00:38:34] But if you have time in the middle, they, so we just do phone calls out of state. And it works perfectly fine. If patient wants a video call, I'm happy to arrange it. But usually, I mean, most of the time you're just talking to the doctor. Gotcha. Gotcha. All right. Let's move on because I'll sidetrack you continuously here.
[00:38:49] Yeah. So let's put up that slide to look at the growth factor. So we talked about, this is with reconstruction. The fertilized acetyl is the best example we have for biologics. So it's important again, we brought this up and we can throw this [00:39:00] off in a second. Everything we're looking at is called autologous, which means it's from your own body.
[00:39:04] There's allogeneic, which is from somebody else. Uh, and those are just two doctors, you know, lay, uh, medical terms. And again, you got to be careful here. You want to make sure, again, the FDA doesn't really regulate whether you use these things. It just, as long as you don't manipulate them. And that's the biggest thing we talked about.
[00:39:20] You don't want to over manipulate these, um, and manipulation means like doing stuff beyond the machines process, like trying to add other factors in that no one talked about. You didn't consent them for that. And again, we don't do that. And a lot of people, I don't know anybody that does, but it's just important for people to understand.
[00:39:35] So everything we're talking about is your own body. Um, there are people that do stem cells from amniotic fluid and things like that. We are not talking about that today. There is not a lot of data on that stuff. So you just gotta be careful and it's incredibly expensive. So I want you to that next in the next slide.
[00:39:52] So again, this is a, this is a really good, I always have to quote the studies from this. This is Rodriguez and Merkineck all 2021. Um, but this is [00:40:00] really good for patients to see this. These are reconstructions and these are the growth factors that they're currently looking at. So they're looking at growth factors, stem cells we talked about, bone marrow, aspirate.
[00:40:08] autologous tissue, pharmaceuticals, and there's different types of things. So go to the next slide. You'll see what we're kind of going at. So these are everything that people are currently looking at. And so if you want to ask what biologic you're looking at, we're looking at everything. BMP, BMP growth factors are, is basically that putty we talked about.
[00:40:27] So can they add that and make people's ligaments heal harder to bone? Yeah. There's a bunch of other ones. Fibroblastic growth factor. I'm just going to go on and on and on and on. This TGF beta is really important and there's been some studies that can you add it back and help people heal their ACLs better.
[00:40:43] Um, so, you know, again, this is going to get a little boring, so I don't want, you know, you people ask about biologics, but then there's a lot of information in the background because you can't just throw in these potions. You got to look at the data, see if it's safe. VEGF is one that we hear about. The problem with VEGF is it increases blood flow.
[00:40:58] So is that, you know, [00:41:00] we see VEGF actually in cancers. So you want to make sure you're not just throwing that into people and causing more vascularity in an area. And then you've seen PRP. This fibrin clot's really interesting. So the idea behind it is, uh, it's, you actually make these clots. But again, it's the idea is can you put the fibrin clot or have PRP in some sort of gel form and then bring it, bring it in the knee?
[00:41:21] It's a conduit, right? If you just inject PRP. Into the knee. It might help with some anti inflammatory properties like for arthritis, but is it going to stay where you want it to stay? So you have to have a conduit to get it in there and the fibrin clots nice because that's that's a thicker Modality, so it's important for people to hear this and understand, you know, what each of these things means I think we probably can get off that.
[00:41:46] That's, that's good. I don't want to get, I don't want anybody to start yawning on us. No, no, it's good. And if anyone's listening on the podcast, please check us out on our YouTube page. We have some slides, we have some information. [00:42:00] Uh, the negative is that you're going to see our faces, but besides that, we've got some really good information here.
[00:42:05] So, uh, please check out our YouTube page. All right. Let's talk about this PRP there. Go ahead, buddy. When we talk about the PRP, um, I want to go back one more thing though. I go back up to the other slide real quick. So there's the DBM putty you keep bringing up. So the idea they've looked at this and they looked at this with how does it combine with graphs from animals because a lot of these studies are in animals.
[00:42:27] They looked at different factors, you know, can you add the PRP and then add, you know, collagen scaffold and can you apply it? And they've seen in models of rats and rabbits that if you add this DBM putty, it increases the tendon to bone healing. So again, the key is to soup up the healing so that your tendon that's in the tunnels closes off with bone quickly.
[00:42:51] One reason that's good is because you can hopefully stress it sooner. But the second reason is some of these grafts like a quad or a hamstring, they're [00:43:00] soft tissue so they can windshield wiper. It doesn't happen usually with In the short period, but one reason if you get the tunnels healed faster, there's less likely chance that they'll get bigger.
[00:43:09] And when they get bigger, you can imagine what happens when they get bigger. They can get looser, right? Looser. And so you don't want that again, not that common if done well, but you know, if there's an, if the tunnels are off and you don't have them healing fast enough, they can cause a little wiggle factor.
[00:43:26] What do you mean by tight, like tighten quickly? Like, what is that timeline? You know, when, when these are kind of like, you know, hardening and, you know, it's getting set in place. What's the timeline from when. You're operating, are we talking a week, two weeks, two months? Like what's the process there for that healing for to get heart?
[00:43:46] It depends on the person, six months to a year and maybe more. And so that's why people aren't ready to go back yet. And sometimes we don't know. I mean, we're not getting MRIs and CT scans at everybody. I mean, like you're ready to go back. Does that make sense? Yeah. And so that's something to be [00:44:00] aware of.
[00:44:00] So the idea is like, can you give them this thing so you boost them and then you let them go back faster knowing that they've healed faster or assuming, but you know, we deal with fractures all the time. I told you I do these osteotomy sort of realignments. Last week I saw three patients back. They were all within five years of each other.
[00:44:16] One patient was 20, was 50 percent healed, one patient was 80 percent healed, and one patient was completely healed. Exact same surgery, exact same surgeon, within like 3 weeks apart. And what were the age of the patients? 45, 50, 52. Okay, we're not this is I'm talking about like literally everything the same.
[00:44:38] So we don't know how can we make one better than the other, but maybe that patient that was a slow healer, if we had known that we would have added some stuff. So can we make them all the same? Can we get these patients back? That's another thing to be concerned about. Obviously, you know, Chad Lavender's patients were really young, right?
[00:44:53] But the average age of an ACL tear now is like 27 to 29. And that's, I would say that's pretty common. Like I do a lot of young [00:45:00] kids. But I also do patient, I do do patients in their 30s, 40s, 50s, uh, that have ACLs that want to get back because there's lots of data they do well too. And so it's important to understand that as patients get older, they don't heal as fast.
[00:45:13] And so would this fertilize ACL work on 40 year olds? I don't know. Would they be able to get back in six months? Would they even care if they get back in six months? Because everyone can say that I really want to get back in six months, but like these patients from Marshall, they're, you know, high level athletes, right?
[00:45:29] Like three or four months for a pro athlete's great, but does it really make a difference? for a recreational athlete. Like everyone wants to be back faster, but does it really make a difference now? You know, I'm sorry, keep going while you're doing it. And I'll add my last piece. No, no. Yeah. Because I'm about to ask you something about when it comes to the age, right?
[00:45:49] So I'm just going to jump the gun. So try to remember what you were going to say. You know, we're talking about the ages and we talk about the Biologics, especially of each individual, [00:46:00] right? And if you're a baseball fan, one of the biggest stars in baseball got hurt again, uh, Ronald Acuna. And, uh, he is, he tore his ACL and his left knee on May 26, right.
[00:46:12] Before that in 2021 tore his right ACL. So now he's torn his left ACL in 2021. He tore his right ACL 2018. He sprained his left ACL. Um, so between when he was 20 years old and now that he's 26 years old, he's had two ACLs. and a sprain, both ACLs on each leg knee. So, you know, you know, is it, is it something that because of the ACL, maybe other things weaken, or it's just sometimes just your body and the way you hold up and are able to just deal with the rigors of life, right?
[00:46:54] Every body type is different. And that's why I'm kind of bringing this in when you're talking about the comparison, the [00:47:00] 45 to 50 to 53 year old, same procedure, same everything else. different results. Is that an example or is it a little bit more to it? No, it's example. There's some patients that just are higher risk, right?
[00:47:12] Like, I mean, I did two, two ACLs today and both patients had ACL done on the other side. So it's just, some people are higher risk. I mean, once you tear your first ACL, the second ACL is 6 percent risk on the other side, just from the idea that you've already had one ACL. Um, it's actually higher risk to re tear your ACL on the other side than it is to re tear the ACL you just had done.
[00:47:39] So it's, think about that. Yeah. So the, and that's what happened with him, right? Like it's just, these, some people are at higher risk and there's anatomy issues. There's, you know, it's higher in females. It's the way they land. And again, he's male, but it's the same type of thing. The, you know, One of the patients today was male, um, that had had other side done.
[00:47:58] So it's just [00:48:00] people are at higher risks and we want, it's a key is, can we identify those risks? I mean, we, we're going to do as much as we can and we'll, you know, I'd like to finish up this part. Um, we're doing as much as we can to prevent people from having retairs. And there's lots of things we talked about, you know, adding the internal brace.
[00:48:14] Can we add biologics? Can we do some fertilized option, um, to help them not have that issue? What, uh, It band tinnitus is like, can we add all these other things so that they don't have that happen again? And now we're getting digressing, but the idea here is what you're hearing about is. And what patients want is, I don't want to do this again.
[00:48:33] I want to do it once, I want to do it right, and I want to make it perfect. Well, it's never going to be perfect, but can we make it right? And can we give you a better shot than you currently have? Which is what we're doing here. Oh, I did it! The balloons! So, it must be the, it must be this or something doing that.
[00:48:50] So, can we, can we I think your daughters are sitting in another room with your wife and they've got some kind of remote control or something clicking on the [00:49:00] button, the balloon button. Oh. Yes. So anyway, so that's the idea behind this is can we give you let people like up? Um, so with the PRP, you can bring that up.
[00:49:10] We'll go through that quickly. Uh, they looked at, they looked at this for adding, you know, PRP again, this take your own blood and then this is injecting the knee and in a surgery, you'd add it into the ACL and there's different conduits that you can use this through. We've talked about this, adding putty, adding collagen, you name it.
[00:49:29] And so, they showed in this one study that there were like 109 knees, 101 patients. So they obviously, some people were bilateral. It's a Burtis et al. Uh, and they had a lower retail rate for the younger patients that had the PRP college and matrix added. Um, now began one study. So be, you know, be aware of this, but there is a, there is a study showing that there is improvement.
[00:49:53] There's also a study showing that that maybe these people, uh, this is Vogren et al. [00:50:00] And some of these people that got the PRP, a different study, uh, that they maybe had higher blood flow into the ACL graft. So again, you're getting the ligament, turning the ligament faster, hopefully. And then again, sort of like a VEGF, which is that blood flow thing I told you about, but obviously a different type of material.
[00:50:19] And some of these are gels. So they're PRP that's in a gel. You can see that that's actually what, that's what PRP looks like. It's a, Maybe usually not that exact color. So, uh, but it's usually around that color. And then can you put that into a gel? So it just stays there and resorbs. Like it's like a, um, a time release capsule, right?
[00:50:36] Like you've seen medicines that are quick acting, but you want, in this case you want something that's slow release. So this is another, another option. There is some data on it. It's just not really good. And I, I don't routinely offer this to my patients. You know, there's, If patients really wanted it, I tell them, you know, I'm happy to do it, but obviously it is also an added cost.
[00:50:55] Uh, so, you know, we're not, we're not there yet, but it's just some interesting information. [00:51:00] Let's briefly bring up the BioBrace. I think it's important to see it. Um, I don't want to overdo this. So this is a relatively new implant. Um, it was designed for a lot of things. You can see rotator cuffs here. Uh, you have this idea.
[00:51:14] So the idea behind this is to. Uh, it's another collagen reinforcement or microfilament. And then basically what it is, is it's, it's got a strength modulus to it. So it's like an internal brace type of thing, but it's supposed to reabsorb with the tissue and people are doing ACLs with this. And actually my patient or what do you mean reabsorb with the tissue?
[00:51:33] What does that mean? It's supposed to grow in with the tissue and add some structural basis to it. I got you. So it stays in. I got you. Where it has really been helpful is in hamstrings. So in hamstrings, people take their hamstring tendons. They're generally smaller. Then the average ACL we do and in under 25, we've seen less and less people recommending doing them.
[00:51:52] So the idea that we used to do is if the tampering wasn't big enough, we would add cadaver tendon to right. So make it bulkier. [00:52:00] But now what people are doing is they're adding this bio brace to it to make it thicker. The problem is obviously it's expensive, so it's not everyone might not be able to get it.
[00:52:09] Um, but the idea is that there's good strength and you know, they've been seeing that if you, the goal is if you can get these hamstring tendons, like imagine we're going to get too off topic, but basically if you take a tendon, imagine the width you want the width of a tendon, the width of your tendon, your ACL to be bigger than eight millimeters.
[00:52:28] But if you take a small girl or a small woman, um, a lot of times it's smaller than that. It's seven millimeters. So how do you make it bulkier? Well, this is a, this is a biologic that you can add with some soaking of other Biologics and you can add it right into the ACL. And there's some idea that we don't haven't seen enough.
[00:52:44] Most of the articles on there are not actually, um, studies, but basically they're showing techniques how to do it. So we're not there yet, but there is some future hope for this potential option for patients. Are you adding anything to this implant? Like, are you, [00:53:00] you know, coding this in something or coding it where, you know, putting a PRP on it before you put it like it, or is it just kind of going in there?
[00:53:09] Is this something that you can add to it as well before, uh, putting this in? Yes. I mean, you can add, um, You can add like PRP, you can add bone marrow, and a lot of times you just basically integrate it into the graph. So there's certain suturing techniques you can use as well. Um, you don't really need to add much for this because it's really its own thing.
[00:53:30] Uh, and so again, we're, it's, it's, the idea is can we, How does this going to enhance the strength of our graft? And especially one of the highest risks, the highest risk you are tearing your ACLs between three and six months. And so by adding this, can we prevent that from happening? Right? Again, this is not that common.
[00:53:48] I mean, I can't think of anybody on my half my head and my patients that's torn their graph at three to six months, but like, The reason is they're also not going crazy, right? But, but Chad Lavender's patients are [00:54:00] going nuts at three to six months. So that's the other issue. So can they go faster? And then therefore they've got this backup tissue.
[00:54:06] So we are, we're, we're attacking these things in really good ways and we're going to get there, but we're just not there yet. Um, I think let's kind of skip over this last one for the sake of time. But basically the last thing is allografts. So we've talked a lot about your own tissue, right? Like there's hamstring, there's quad, there's teletenin, but some patients, It's not an option.
[00:54:28] They either had, I mean, I had a girl that's just 24. She had three failed ACLs. They took every single piece of her tissue. So she's got nothing left. So what are you going to do? Well, how can I make it better? Well, there's some studies in this in sheep, but again, using cadaver tendons, combining the BMAC bone marrow aspirate and the PRP.
[00:54:47] And they did see some improved incorporation. Again, just the, just the sheep study. Um, and there's some ideas also looking at, can you add this sort of, this is bone marrow seen from the hip, you get from the knee. Now here [00:55:00] is AVN. So they're injecting it into the knee to kind of help it heal, but you can see other ways you can do it.
[00:55:05] This is, we can take it from the crest here. This is in the back. Um, and the idea is that they've seen that hopefully maybe the tunnels won't get as wide with these tendon, these, uh, these cadaver graphs. Again, it depends on the type of cadaver graph to use. I use, um, Exclusively patella tendon. So it comes with bone on both sides.
[00:55:22] So the idea is behind that is there's no concern for this windshield wiper. Remember I told you about that where it goes back and forth, back and forth. But a lot of people don't use that type of cadaver graft. They use something else that's got tendon on both sides. So if you have that, you have to get it to heal faster.
[00:55:38] And how do you do that? Maybe you add something like this. So there's a lot of You've got to think about when you talk about this and be careful you're not comparing apples to oranges, right? So this was done on probably soft tissue, which is what we talked about that I don't use for allograft. So it may not be compatible for someone like me and the way I'm doing it may be [00:56:00] different or may heal better or worse.
[00:56:01] You know, we don't know. Um, I've had good results with it, but it's important to understand that everything is a little bit different and there's, there's so many caveats to this. But also ACL is a real, we'll go into this. We'll just talk about this very briefly, but ACL is a really good surgery. It's definitely not perfect, but there's some of my happiest patients and they get back to things they want to do.
[00:56:21] Again, not perfect. There are patients don't get back to the sports they want to do, but it's just, it's also really popular surgery because it's really common. One of the most common surgeries I do is ACLs, but it's just hard. You got to be careful, right? Like you'd never want to do a surgery for an ACL kid.
[00:56:36] And then make them worse, right? Like that's the whole most horrible thing you can possibly do because these are not like, it's like you get your second and third and your fourth within a couple years. Like that's not a good thing for you. Like, it's not like you just go redo an ACL l and it's no big deal, right?
[00:56:50] Like it is a big deal. No, it's not cool. Even though it's obviously life threatening. It's not, it's not cool. Those none of it is. So let's talk about this last topic. So we've gone in a lot of biologics. [00:57:00] We've talked about a ton. I mean, this could be like a three hour show of your scene. Well, we, we got two and a half minutes left.
[00:57:05] Well let, let's talk about the last piece. It's all well and good. But one of the concerns is like, how, how do you get, why are things not healing as fast? Well, some studies have shown that basically, the reason things don't heal as fast sometimes is there's an indolent infection. So like, people will tell you like, my graft failed at like a year.
[00:57:23] And thankfully I haven't had those issues, but that can happen. I've heard about it. And one thought is that maybe the graft, the certain thing you put in had a little bit of infection in it, but not bad enough to cause a real infection, right? Like it's a subclinical, like you don't notice it. And as a result that the graft failed or over time after two to three years, all of a sudden you get an MRI and then ACL is gone.
[00:57:43] Like, how did that happen? The patient never felt a pop. So it did dissolve from the infection. So what we're doing now for every single ACL I do, allograft, you name it, I wrap the ACL in something called vancomycin, which is an antibiotic. And there's been studies that show it drops the infection [00:58:00] rate to literally zero.
[00:58:01] And I'll knock on one. I have not had one. An infection after an ACL is an absolute devastation and you never want that. So the thought process is not only in like, it's great to prevent the big one, right? Like, I never want that to happen. Yeah, it's pretty uncommon. But these indolent infections, there are some thoughts that are way more common.
[00:58:20] And so Ken, And it improved their healing just by wrapping their ACL antibiotics. Yeah. So that you left a big one for the end. I mean, that's, I know that's amazing. I think the problem here is that patients are so worried about getting their ACL better. They don't realize they're already doing a lot of things.
[00:58:44] And so the problem I think is, Is I just told you a lot of really sexy awesome stuff, but then we've got to start executing on it, right? Like we've got it once the data comes out. You got to push it, right? Like if my bear patients are getting the same surgery as my [00:59:00] acl tyro, but my acl tyro patients are allowed to go back at five months and my bears are making them wait till nine months because the fda protocol Am I doing the right thing for my patients with the B.
[00:59:09] E. A. R.? Yeah, it's uh, if you're gonna tell people that you're reducing the chance of infections and that after this is one thing less to worry about, that's a big one because that's obviously a main concern. Oh, it's that time. Dr. Garcia, we're going to wrap it up here. This was a great episode. So happy and check us out at sports doc talk.
[00:59:36] com. We've got a lot more information, a lot more stuff going on. We really appreciate everyone listening to the show.
Thank you very much.
Thank you.Audio Transcript
Surgical Nutrition: Amino Acids and Peptides with Dr. Jazayeri

Will Sanchez: [00:00:00] Welcome to the show. Welcome to sports doc talk. I'm Will Sanchez along with Dr. Grant Garcia. Dr. Garcia, we have a fantastic show. We have an incredible guest, but before we get to him, let's just remind everybody, check us out at sports. talk. com. We're on YouTube and Odyssey and Spotify and Apple and all of the goodies.
[00:00:28] Will Sanchez: And be sure to check out our website where we have previous shows and we have transcripts. We have so much information that we provide, especially from you, Dr. Garcia. I've rambled on for over a minute. Let's welcome you in, man. How are you, Dr. Garcia?
[00:00:45] Dr. Grant Garcia: I'm great. This is awesome. I'm so excited. It's always so fun when we get to, you know, we've had, we get a lot of guests on here and we've had different doctors and everything else, but it's so fun to see a topic that comes up or your patients ask about, [00:01:00] and then you find like the best expert for it.
[00:01:03] Dr. Grant Garcia: And plus, A normal, cool orthopedic surgeon. So this is going to be super fun. I'm a little worried that we're likely going to try to go over an hour. So we'll keep me in check because I have a feeling this is going to be one of those times. I've already had a pre conversation with Reza, and I'm not sure we're going to be able to make it.
[00:01:20] Dr. Grant Garcia: under an hour. Do not go off the deep end, okay? So I'm just letting you know. I've never done that before, Will, right? I've never done that before. No, no, no. So let me introduce, before you put them on, let me introduce. So when in, uh, in the office and you know, Will, you brought this up a couple of shows ago, but in the office patrons keep asking me about supplementation.
[00:01:39] Dr. Grant Garcia: They're asking about post recovery. We're going to go into that. This is, we have first good topic on nutrition, but they're asking me about how they can get better after my ACL surgeries and my cuff surgeries, my big surgeon meniscus cartilage transplants, where they get significant atrophy and it takes them nine, 12 months to fully recover.
[00:01:55] Dr. Grant Garcia: And they're, and these are Seattle patients. They're looking up everything and they want to know the best of the best. Like, how do I get to the next [00:02:00] level? And for a long time, we had very little. We're starting to get more things through different things we'll talk about.
[00:02:05] Dr. Reza Jazayeri: Yeah.
[00:02:05] Dr. Grant Garcia: But one of the number one things is nutrition.
[00:02:07] Dr. Grant Garcia: And then you're seeing on LinkedIn, people are talking about nutrition. How do we get people better, faster? And this is not just knee replacements, patients with hip fractures, you know, patients that are elderly that need to gain their muscle back. This is athletes. And I mean, I see athletes All the time that we operate on and they come in and their their leg looks like half the size and they felt they only had surgery like three or four weeks ago.
[00:02:25] Dr. Grant Garcia: Right? So how do we get them stim faster? And patients are like, how do I get my quads back faster? And one of these things is nutrition. And Uh, Dr. Jazayeri, who we're going to have on in a second, we have a big article called J AOS. And so it's one of like the number one journal we all look at. And he wrote the, he was the lead in this article about amino acids.
[00:02:43] Dr. Grant Garcia: So immediately after seeing this, having seen his content online, I reached out to him and he was, um, awesome to come on our show today and tell us a little bit more about this and understand like what's so hot about this. We're at an infancy right now. We're going to see more and more of this coming up and people are looking how they can get their patients back faster.
[00:02:59] Dr. Grant Garcia: And [00:03:00] this is one of those things. And he started this awesome company. So I'm really excited to have them on. Let's bring them on
[00:03:04] Dr. Reza Jazayeri: guys. Thanks for that intro. I totally agree. This is an exciting topic for all of us. And, uh, Like I was sharing with you Grant earlier, I'm, I'm a fan of you and the stuff that you're doing.
[00:03:16] Dr. Reza Jazayeri: So it's just kind of great to be able to, um, share ideas and especially this one. I think it's, it's, it's something that people are interested in. We're interested in, and we're, like you said, we're, we're at the infancy. So, um, uh, I think it's our challenge and our kind of responsibility to kind of know.
[00:03:35] Dr. Reza Jazayeri: this material because our patients are demanding it. And I think it's a part of now our practice to understand this, if we can have this dialogue.
[00:03:43] Dr. Grant Garcia: Yeah. And it's important to, you know, uh, res is a sports surgeon down in California. He does the same stuff I do. He's curl and Joe fellowship. Awesome. One of the top sports fellowships in the country.
[00:03:53] Dr. Grant Garcia: So, you know, he gets these things and he and I have the same mindset of like, how can we get these patients that are athletes back faster? And [00:04:00] And you're getting the same patients in downtown in California, you know, they they're active patients They're like, I don't want to sit around for two days. I don't want to sit around for two weeks, right?
[00:04:07] Dr. Grant Garcia: And so you developed this thing So I guess tell us more about the practice and the interest you have and then we'll get into the nitty gritty too
[00:04:15] Dr. Reza Jazayeri: Yeah. Yeah, you know, um, I think we're all a product of where we trained kind of who we are And then also where we practice and our patients around us. Right.
[00:04:24] Dr. Reza Jazayeri: And so I'm like a block down from Gold's gym, Venice. Right. So my patients are, I have a sports practice, like do you like you, but I also do a lot of shoulder and arthroplasty and revisions. And I'm the guy in my practice who like, no one wants to touch the stuff. And then they're like, just give it to rise a heel, do it.
[00:04:41] Dr. Reza Jazayeri: And I'm like, okay, you know, I'm happy to do it. Right. So I have almost like a sports trauma practice. And I say trauma because peck ruptures, biceps tears, hamstring ruptures. You know, these are these athletes who are on a different level and who are coming in with much higher expectations for [00:05:00] me. So throughout the years of my practice, I have Learn to kind of now have higher expectations of my patients to say, Hey, if you expect me to do this, then I need you to optimize yourself.
[00:05:11] Dr. Reza Jazayeri: And I think that's where I started to realize, look, you and I can sit here and talk about ACL graphs and screws or buttons or suspension or flip cutter or this and that. That's already kind of tapped out what we ask our patients to do. How can they optimize themselves? What are they bringing to the table?
[00:05:32] Dr. Reza Jazayeri: How can they be a better fit patient to have a better success? This is where I think we can make a big impact on their outcomes. So this is how I got into the nutritional piece.
[00:05:43] Dr. Grant Garcia: Well, and I think you're making a point point, you know, patients are like, why can't I get back? You know, why is, why is the ACL surgery you guys did 10 years ago, still at nine to 10 month recovery now?
[00:05:52] Dr. Grant Garcia: Why is the shoulder surgery, the rotator cuff, that one, or the pec ruptures? I mean, those are massive tears. Why do they still take so long to recover? [00:06:00] And the problem is that patients, and I think you're perfect point. When I think that we should really emphasize this and will, you can hear this too, but you got to flip it around on them because it's not just my surgery.
[00:06:10] Dr. Grant Garcia: Like your work, right? You do an hour, a half of work. They're doing hours and hours of stuff. And so they're expecting your work. to get them back as quickly as possible. But if you don't do the extra stuff, I always tell them the PT and the recovery stuff, that's actually way more important than even the surgery, right?
[00:06:26] Dr. Grant Garcia: Because you know, there's, there's so many different things you can ways you can fix it, right? It doesn't really mean they're not all perfect and they're not all the best, but the other stuff is important.
[00:06:33] Dr. Reza Jazayeri: You know, basically when these patients are coming in, they're already at a disadvantage because they took a hit.
[00:06:40] Dr. Reza Jazayeri: And what happens to the patients after an ACL injury or any kind of injury, actually, the muscle starts to change its physiology. It becomes kind of resistant to growth and there's both neurological and physiological changes. So, you know, I have this philosophy of the [00:07:00] surgical athlete. So I treat all my patients like an athlete training for an event and that event is their surgery.
[00:07:06] Dr. Reza Jazayeri: So I tell him, look, we got to prep you up for this. We got to get you ready. So all my A. C. L. S. Get prehab, they get B. F. R. I get him into exercising before the surgery. I check The nutritional status before surgery, we do all these things to prime them up. How are
[00:07:22] Dr. Grant Garcia: you checking their, sorry, interrupt. How are you checking their nutritional status?
[00:07:25] Dr. Grant Garcia: What are you doing?
[00:07:26] Dr. Reza Jazayeri: So albumin is, uh, uh, uh, uh, albumin and prealbumin, um, are good ones to check. And we can get into that a little bit more. That, that really ends up being a factor in, in the, in the elderly group. But it's interesting. You'll also pick it up in younger patients, especially revisions.
[00:07:44] Dr. Reza Jazayeri: infections. Um, and you know, I'm in California, so I'm getting a lot of these vegetarians and vegans and don't get me wrong, I'm, I'm, I'm vegetarian myself, except when I'm eating steak, you know, but, but, but the reality is these patients don't heal the same way. They just don't
[00:08:00] because they're not getting the substrates.
[00:08:02] Dr. Reza Jazayeri: And so when you check these variables, you're actually better off holding off on surgery for a little bit, optimizing them, getting them ready. So when they, you know, when they enter the operating room, they have all the necessary variables. Besides just the implant that we do in order to get them to heal faster.
[00:08:18] Dr. Reza Jazayeri: So kind of what this graph is showing here is that this decrease in mobilization is is a problem because they have muscle loss. And so if you can kind of mitigate that by improving prehab, you build the resilience. And this is what we'll talk about when nutrition comes in to also improve their muscle resilience.
[00:08:36] Dr. Reza Jazayeri: So This hit that they take, everybody gets this, by the way, this is the best case scenario, guys, this is a healthy athlete, you get someone to do a joint arthroplasty, that line is much lower, much further down, and then the one with the hip fracture, 30 percent die in a year, so, We have a lot of work to do in this kind of opportune time where the body's really breaking down its own tissue.
[00:08:59] Dr. Reza Jazayeri: [00:09:00] And this is where, you know, the, the, the strategies through, you know, nutrition and amino acids come in to really effectively mitigate that drop that you see right there.
[00:09:09] Dr. Grant Garcia: I see a lot more of this too. If I do a lot of meniscus cartilage transplants, struggling in the cartilage patients, they're struggling for like a year, two years, three years.
[00:09:18] Dr. Grant Garcia: So then they do their surgery. And the problem you have is like, I mean, I had patients today, they're nine months out, they have no pain, but they're still feeling like they're, they're tell us got not tracking right or something because their quads been shut down for like 10 years,
[00:09:30] Dr. Reza Jazayeri: you know, before surgery.
[00:09:32] Dr. Reza Jazayeri: Um, and then after surgery, and then the amount of atrophy that we've seen, the quadriceps is really profound. And if you look at, we let most of our athletes, they want to get back by a year. Sometimes they're pushing to get back even earlier. But if you really critically look at the literature on ACLs, for example, at one year, not many patients are at 100%.
[00:09:52] Dr. Reza Jazayeri: Actually, most are about 75 percent other contralateral side. And so a lot of them are not getting back to where they want. And it's [00:10:00] closer to a year and a half to two years before, after an auto, after an autograph, they were able to get back to higher nineties. And so interestingly, we see the most we rupture rates in the first 12 months in the early phase.
[00:10:14] Dr. Reza Jazayeri: And so that's where I think Improving on the muscle side is just as important as getting the graft to heal.
[00:10:22] Dr. Grant Garcia: And we always talk about this in ACLs, right? When we do an ACL, your patients are always like, they're like, I make them so focused on their number. And obviously that's, there's a lot of other things contributing, but like quad strength is so essential for the testing.
[00:10:34] Dr. Grant Garcia: Right. And there's the 90 percent factor we look for and they're just harped on it. But if, but it's like, it becomes a situation where if they're like 75%, they feel like they let me down at 10 months. Right. And I'm like, listen, it doesn't not. And they all want to be, the problem is you get like 80, we brought this up.
[00:10:48] Dr. Grant Garcia: You got the Adrian Peterson who probably went back too early, but this is a freak of nature. Right. And he goes back at six months. So they assume everyone should be back at that Sam. Well,
[00:10:58] Dr. Reza Jazayeri: Well, he was probably on [00:11:00] some supplements that helped him.
[00:11:01] Dr. Grant Garcia: There we go.
[00:11:02] Will Sanchez: No, no, no, no. There we go. I like the way you say supplements.
[00:11:06] Dr. Grant Garcia: Perfect segue. I
[00:11:08] Will Sanchez: think Aaron Rodgers was on some supplements also after his Speedbridge, uh, surgery.
[00:11:14] Dr. Reza Jazayeri: That's, um, actually I can't say yes and I can't say no, but I can tell you that Everyone, uh, you know, uh, uh, curling job, for example, who, who, um, you know, they're very familiar with, with, with the amino acid supplement and it's, it's at their DMV.
[00:11:29] Dr. Reza Jazayeri: So we, you know, we, that's something that, you know, we're using and professional athletes and, uh, it's, it's being supported by, you can read between
[00:11:37] Dr. Grant Garcia: the lines. Well, Neil ElAttrache is at curling job. And they're on DME for that. So therefore you can read between the lines. We're
[00:11:43] Dr. Reza Jazayeri: very fortunate. Dr. Ellis has been a supporter of accelerated recovery.
[00:11:47] Dr. Reza Jazayeri: It's, it's, it's, it's been great. Yeah. Um, so I think that's what, so, you know, one thing to kind of recognize is look, everyone's going to have a hit, but it's mitigating that hit. And if you don't drop, then you don't have to [00:12:00] fight to get back up. And the older you get, the harder it is. And I'll just tell you this, it takes 12 weeks of strength training to put on.
[00:12:10] Dr. Reza Jazayeri: what you lose in two weeks of immobilization. So it's a it's a big difference in how fast you lose and how hard it is to gain. And so if you can prevent the loss, that's the win right there.
[00:12:23] Will Sanchez: Yeah, I just want to jump in real quick. Um, obviously you're, you know, we're not talking about the Achilles, but just because it happened to me, I had surgery on December 1st and, um, just sitting around for a couple of weeks was just absolutely brutal.
[00:12:38] Will Sanchez: And then so much muscle loss, uh, you know, calves, so much skinnier and, you know, just doing the work now, calf raises, seated calf raises, trying to do, you know, single leg stuff. But, You know, as you said, because I sat around for, you know, a month and a half. Um, before putting, you know, weight bearing and little by little, I'm [00:13:00] still nowhere close to where I was when I was running, playing, jumping, and moving.
[00:13:05] Will Sanchez: So just, it resonated with me when you said, you know, in two weeks. You're already gonna have this sustained muscle loss, let alone sitting around, um, you know, for a month and change, almost two months, and then slowly starting to, you know, get, become active again. And also having those, you know, those restrictions in your mind as well, saying, well, you know, can I do this?
[00:13:29] Will Sanchez: What can I do? Am I going to hurt myself? Because, you know, same thing you're talking about re injuring, you know, it's, you know, You guys tell me, but the re injury part could happen when those first six months, right? So that's kind of like in the back of your mind as well. So there's so much that a patient thinks about and it's great to hear that you're saying, Hey, this pre op preparation should be a part of You know what you do and obviously, you know, you can talk about when the situation doesn't call for when you [00:14:00] have to go in because it's an emergency and you don't have the flexibility to do that.
[00:14:04] Will Sanchez: Yeah. What are those situations where you can't, you know, prepare your patient in advance for surgery? Is this something that stands out?
[00:14:12] Dr. Reza Jazayeri: Oh, yeah. I mean, you know, I was telling you earlier. Some of my practice is like sports trauma where they're coming in with an immediate tear or rupture. It's not, it's not so elective, right?
[00:14:21] Dr. Reza Jazayeri: So those cases, um, then you, you, you don't have that opportunity to pre have them. So it's even more important to, to really start the weight bearing. So, so weight bearing is something that is something where we can really help patients with preventing muscle loss. And so, uh, this is where, look, everything ties in.
[00:14:40] Dr. Reza Jazayeri: There's no magic bullet, right? But, but if you have a very strong construct that you feel confident in that, that, that, that, that implant then gives you the ability to wait there earlier. Okay. And so then if you can wait there earlier because of your implant, then you can have less muscle loss. And if you can bring on the [00:15:00] supplementation along with exercise and then tack on like BFR, okay.
[00:15:05] Dr. Reza Jazayeri: Then you see how you got this Domino effect of multiple things meshing so you can't just say it was just this one thing It's really this comprehensive approach and then don't forget. It's the mindset too You have your pictures are going to have this fear of getting back. So You know, I never want to say hey, I got this.
[00:15:23] Dr. Reza Jazayeri: There's this magic bullet it's really understanding all of it, but not leaving anything on the table because you don't want to shortchange the surgery that you did by just missing out on these key variables.
[00:15:34] Will Sanchez: I got I got a quick follow up. Um, how important is it for your P. T. Person to be on board with what your your mindset is for your patient?
[00:15:45] Will Sanchez: post op. And how does that normally work? Because there's different variables like, hey, you know, pick one of these places you go and I'll see you in six months, you know, how hands on are
[00:15:58] Dr. Reza Jazayeri: you? So the [00:16:00] time that the physical therapist spends with the, with that patient is way more than they spend with me.
[00:16:05] Dr. Reza Jazayeri: And so the reality is, the better that relationship is, the better that patient is going to do. And so for me, my, my ideal ACL patient, for example, is they have their physical therapist that I know at the prehab. So they're already working with them. So it's not like, you know, Samantha comes out of her A. C.
[00:16:23] Dr. Reza Jazayeri: L. And says, Who am I going to go to? And then, you know, find somebody. And then they're like, Okay, hi, Samantha. Nice to meet you. It's no, no, no. How did the surgery go? We've been working for a few weeks together. I know where you're at. So you have the report. So for me, the physical therapy piece is extremely important and the literature has already shown prehabilitation before, you know, these kind of surgeries actually does enhance the recovery process.
[00:16:44] Dr. Reza Jazayeri: So, um, That's a very they're all important but that particular relationship is something that I try to foster
[00:16:52] Dr. Grant Garcia: So let's talk about really quick She'll pull up the amino acids peptides because people keep asking about it and they're using interchangeably But they're not and you were mentioning before, you know [00:17:00] ones and one we can have potentially one.
[00:17:02] Dr. Grant Garcia: We're not there yet um Perfect. Yeah, so there's amino acids. So kind of run through this real quick with us. Okay,
[00:17:09] Dr. Reza Jazayeri: okay, so You know, what you see on here is when our body is going through surgery, it's a very unique time. The requirement for these building blocks is extremely elevated. It's about 80 percent more.
[00:17:26] Dr. Reza Jazayeri: Why is that? Because, well, let's back up and say, okay, what are amino acids? So think about the vocabulary that we have with our alphabets, right? We got 26 letters and we can use these 26 letters to create sentences and paragraphs and tell the whole story. Okay, And you're only doing that with 26. So amino acids, our entire body has only 20 amino acids, but these 20 amino acids can similarly be kind of coupled to have a particular [00:18:00] function.
[00:18:00] Dr. Reza Jazayeri: Okay. And so these 20 amino acids come together to form all the precursors that we need for muscle and for bone mineralization and collagen synthesis. So this is where your body is really requiring these amino acids. to produce these things that we are really looking for in a orthopedic surgical recovery.
[00:18:21] Dr. Reza Jazayeri: Those are the three variables, in addition to all the enzymes and immunity for, uh, for fighting off infection. And so there's this demand that's really elevated. What happens is when you don't have those available. When you and I were cavemen, you broke down your, you broke your leg and you fell. Well, you have fat sores.
[00:18:43] Dr. Reza Jazayeri: Everyone knows fat is there for, so you don't starve. You don't have a reserve for skeletal, for, for amino acids that's hanging around. That's your muscle. So you actually start to harvest, you break down your own muscle to provide these key amino acids. So this is what happens when people lose weight [00:19:00] after surgery.
[00:19:01] Dr. Reza Jazayeri: fat. They actually just l because you broke down yo to provide these really k you need for all these di And guess what happens af have much appetite. People want to eat. And guess wh before surgery. You tell is. So this is why now yo such a change. So our protocol now with with with the accelerated recovery program, we do carb loading, right?
[00:19:27] Dr. Reza Jazayeri: I mean, think what a marathon runner with a jujitsu fighter go into their fight fasted. They're gonna do terrible, right? And so if you go into, but so guess what? When you go into surgery after overnight fast, our livers have about 120. Maybe if you're really well trained, maybe 150 grams of glycogen after overnight fast, it's almost gone.
[00:19:47] Dr. Reza Jazayeri: By the time you hit surgery, You don't have much. So your body says, okay, no problem. I'm just going to go to my muscle, break it down. Gluconeogenesis breaking you, you know, make new glucose from muscle. And so essentially you're [00:20:00] harvesting your own tissue. This is why now we're providing the amino acids and the carbohydrates.
[00:20:06] Dr. Reza Jazayeri: So your body is kind of prepared for the surgery and you're not wasting your own tissue. So that's kind of the essence of it.
[00:20:13] Dr. Grant Garcia: So you get to your, I saw your thing. So you got the pre, uh, That's the carb loading, right? And then the post supplementation is the essential amino acids. So the important thing is for the listeners to the essential amino acids, you can't get those.
[00:20:25] Dr. Grant Garcia: You have to, you have to, those are from diet. Um, and they're hard to get sometimes,
[00:20:30] Dr. Reza Jazayeri: right? So of these 20 amino acids that we have, nine of them are called essential. Essential means they need to come from the outside source. Your body can't make them. And the only place it could, Get it from is again, breaking down your own tissue.
[00:20:43] Dr. Reza Jazayeri: And it's the essential amino acids that have the same profile as your skeletal muscle tissue. That's why they're really essential. And so you, so this is why you really break those down during this time of stress burns injury. And that's where. these amino acids at the the [00:21:00] right time is given t it needs.
[00:21:03] Dr. Reza Jazayeri: So it doesn't b tissue. We actually start before. And this is what when you give patients am week before, Hans driver They did biopsy studies at the time of total knee arthroplasty. They took muscle tissue at the time of surgery on these patients who were supplemented for a week prior, and they found that regenerative tissue in the, in the muscle, they're called satellite cells, usually stem cells.
[00:21:29] Dr. Reza Jazayeri: They actually got higher in number. Which then led to having a quicker recovery? So it's really fascinating to see there's a sailor mechanism And the rationale for why you're supplementing
[00:21:41] Dr. Grant Garcia: so, you know Give an example of like do you have examples of this for the and I know you work with a lot of athletes We've seen on your profile.
[00:21:46] Dr. Grant Garcia: You've got the ce certification right ce or something you can or you can talk about it Sure
[00:21:51] Dr. Reza Jazayeri: Sure.
[00:21:52] Dr. Grant Garcia: Yeah. So, I mean, yeah. What have you seen from athletes? What is your experience? You're obviously clearly involved in curl and job with their stuff, uh, doing and other things like, [00:22:00] what's that, what's your sort of data or information you have on that?
[00:22:03] Dr. Reza Jazayeri: So basically, you know, in, in, in order for any athlete. Whether it's professional football collegiate level, you know, and all the international in order for them to take a supplement, it has to be NSF or sports certified. NSF for sport does an extremely good job and making sure everything is pure. and they they check it in multiple levels to make sure that these athletes are not getting anything that's banned.
[00:22:29] Dr. Reza Jazayeri: There's no contaminants. And it's kind of the we went to the FDA said, Hey, what's the best, safest thing that we can do for our athletes? And it's the NSF for sport. So if you don't see an NSF for sport on the supplement, um, It's probably hasn't gone. It hasn't gone through the testing and the professional athlete can't take it.
[00:22:45] Dr. Reza Jazayeri: So, so that's that's any supplement that an athlete takes has to be NSF for sport. Um, so well, and that's
[00:22:52] Dr. Grant Garcia: a concern to write. You see on the news. These people that said they took something. They didn't know what it was. And all of a sudden now it's a banned substance. So that's important for people to hear that as well.[00:23:00]
[00:23:00] Dr. Grant Garcia: Sorry. Keep going.
[00:23:00] Dr. Reza Jazayeri: No, no. So that's that's really important. So that's why it's for us. It's been really exciting that we've been sharing the supplement with, you know, NFL Major League Baseball. All the professional teams have been really Excited to have this. And one, the discussions I have with their nutritionist and their dieticians, they're like, oh my God.
[00:23:15] Dr. Reza Jazayeri: Finally someone who took all these different supplements that we've been kind of thinking about and put it together with the right dose and, and, and is providing it at the right time. So this is where, this is where kind of my practice was able to. Look, because I live in Venice and I'm, and I'm around these athletes and these bodybuilders, they're, they're coming in with so much knowledge that this is the stuff that you and I never got in residence here in medical school, right?
[00:23:38] Dr. Reza Jazayeri: So I have to actually take a sabbatical on this because they're coming in with all this stuff and I have to re educate myself to understand, wow, there is, because this stuff, look, when I see a patient who's completely supplemented, we can talk about the whole regimen that some of these guys are doing and what we're working on.
[00:23:53] Dr. Reza Jazayeri: It's day and night. Their recovery is so much faster. They have less muscle loss and they're able to get back. Now it's our, [00:24:00] it's on us now to do the good academic science and the research to show safety and efficacy, but there's a huge gap. But I can tell you on that side, these guys have been doing this for a long time, and they have.
[00:24:11] Dr. Reza Jazayeri: High success rate with it.
[00:24:13] Dr. Grant Garcia: Well, and also will, we talked about this before on the number of things, like what it takes, right? We had a website on what it takes for these pro athletes and why, like, and I've said, this is a kind of a joke aside, but everyone can hear this on here. Why, you know, like if you do a good surgeon, a pro athlete, they'll still do well.
[00:24:26] Dr. Grant Garcia: If you do a great surgeon, a pro athlete, they'll still do well. And why one, they're freaks in nature to, you know, like, but they also, they have all these extra tricks in their bag. Like you said, for Adrian Peterson. They're pre supplemented, they're post supplemented, they're getting, they have nutritionists working with them.
[00:24:40] Dr. Grant Garcia: And this is just one component that Will and I did never talk about. And it's been ignored on a lot of these different things discussing about it because we don't understand it. I don't get any nutrition training, you know. To me, this concept is, I've always known it was better for patients, But it's just really hard to stay up to date on everything.
[00:24:58] Dr. Grant Garcia: You would take a sabbatical to learn about [00:25:00] this. You're, you're involved with bodybuilders, you know, these bodybuilders are like, I mix all my things together. They have their potions and with their creatine, other things that they mix together that we don't see on a daily basis, you know, I'm not taking 45 supplements.
[00:25:11] Dr. Reza Jazayeri: Yeah, well, if it weren't for that and sitting with these guys and going to the lab and, you know, um, spending time with them and seeing what works, I wouldn't have got this experience myself. It would just meet me also, you know, being here. And then the other, the other part of this is, look, if, if these athletes, um, are not given this whole, um, this whole aspect of you need the surgery.
[00:25:36] Dr. Reza Jazayeri: We also need the safety. And this is where we come in. Right? And I think a lot of surgeons, the concern that I've been hearing from some of the athletes is my other surgeons don't want to hear about it. They just poopoo it or they just turn the other way. I don't think that's necessarily the best approach for us because just the same way we talked about having good engagement with your patients and physical therapists, you want to be able to have a good rapport with [00:26:00] your athletes and with all your patients.
[00:26:02] Dr. Reza Jazayeri: And if your patients are asking, you don't want to say, I don't know. Yeah. Go to someone else. This is where it's important for us and I think we need to actually lean into this and, and study it for ourselves and get more information that, and that's where we're gonna really have this cohesive approach.
[00:26:17] Dr. Grant Garcia: Re this happens all the time in practice. I had three patients a day that told the surgeon that they tell my surgeons don't work. My Macy's don't work. My Carly's transplants don't work. I do ACL repairs now with the new tight rope. I've been, they've been rocking it and they say it doesn't work. You know, I just gave a lecture down and talking about it.
[00:26:33] Dr. Grant Garcia: And people are just like, they didn't even seen this thing before. You know, you're so used to this. You get the same thing and your supplementation thing. I have no doubt that 75 percent of the surgeons poo poo it because they have no idea what's going on. And I always my my favorite response to this is if they don't ever try it or do it and they say no, then there doesn't their opinion doesn't count.
[00:26:52] Dr. Grant Garcia: And it's the exact same thing. Their surgeries, they say they've never done it before, so it doesn't work.
[00:26:55] Dr. Reza Jazayeri: Yeah, and I think this is just, uh, what we expect with, with medicine. Things take time, you [00:27:00] know, from actual, from actual being, you know, from, from ussing it into a lab, into research, and then finally being common practice.
[00:27:07] Dr. Reza Jazayeri: There, there's such a, there's such a delay in that. Uh, but now I think with technology and science, uh, we're, this is, this is definitely exploding.
[00:27:16] Dr. Grant Garcia: And you've seen it all the time. I mean, you, you're a big article on JOS. Obviously I'd seen your stuff online. I'd seen the guys you worked with. I know Acevedo, he's done some stuff with you guys and you obviously have a lot of neat people that you've worked with, a lot of good doctors on your website that you've advised with.
[00:27:29] Dr. Grant Garcia: So it's not like you have a bunch of schmucks out there working with you. No, we're very fortunate.
[00:27:33] Dr. Reza Jazayeri: Yeah. You know, and we have a couple of Clinical studies coming up with Johns Hopkins, looking at total knees with NYU. We're doing a hip fracture study and, uh, also a ACL study looking at this stuff. But these things take time as you know, writing IRBs, getting patients enrolled, you know, understanding, you know, how to best approach these.
[00:27:50] Dr. Reza Jazayeri: These are very tough studies to do. There's so many confounding factors. I mean, look. You know, uh, I do a double row repair, uh, on my rotator cuff repair, but it, it's, you know, you can find a lot of studies that say, [00:28:00] Hey, just do a single row doesn't make a difference. So something we know biomechanically totally works.
[00:28:04] Dr. Reza Jazayeri: Okay. And then you do the same thing in a patient. And then our, our data. Because the way we study it doesn't show it, right? And so people can poo poo it. But, but, but we, we still have this kind of understanding on a biomechanical side. This is the problem with our research and actually, you know, getting to that next step, the confounding factors.
[00:28:25] Dr. Grant Garcia: Well, also you need power, right? Like, I mean, for instance, I do a lot of surgeries. How many post op wound infections do I have? I don't have that many cause I'm doing scopes, right? But you get one, you wish you had supplemented them, right? So it's, it's, it's, it's, it's going to be, it's hard to get the numbers like you're talking about for the data.
[00:28:40] Dr. Grant Garcia: And I totally agree with you. I mean, you're gonna get people that are going to poo poo you cause you don't have 45, 000 patients in your study to show your supplementation works for certain aspects, but the same point. You have to realize like at a visit at six weeks, if I come into my patients, I mean, I have these other things I'm doing already now for post op recovery in terms of some other machines.
[00:28:57] Dr. Grant Garcia: I'm using different ice machines and things like that. I [00:29:00] noticed already patients are feeling better and that makes me feel good. And anecdotally, I can say that I feel like it works well, but I don't have the research back like you do for certain, some of these certain things, but it helps me to feel better that I can give my patients some enhancement, which is why it's awesome that I can offer this.
[00:29:15] Dr. Reza Jazayeri: Yeah, you know, I'll tell you right now, the joint arthroplasty and the hip fracture literature is really is really good. And it's there. So there's, you know, there was a recent systematic review of randomness control trials looking at totally arthroplasty and amino acid supplementation. And it's clear, you know, if you provide this one week before and two weeks after.
[00:29:33] Dr. Reza Jazayeri: You have an impact on their outcomes. And so, you know, you can extract. And so why they pick total knees because need total knees. We're gonna be doing so many of them in the future. Right? And so those are right. High volume. And so that's where the focus on the industry has been right. But because I started as a sports guy looking at a C.
[00:29:48] Dr. Reza Jazayeri: L. S. Um, that's how I first got into and I see the benefit there. You know, there may be the delta is gonna be maybe different for someone who's gonna have fracture versus someone who's having a C. L. You know, you're not gonna [00:30:00] die from an A. C. L. You may just get back later or, you know, you may retear hip fractures.
[00:30:04] Dr. Reza Jazayeri: These patients have significant morbidity and and the sarcopenia, the muscle loss leads to a lot of complications. So I think we can help everybody, but they're all going to be helped differently. So getting an athlete back is very valuable to them, but also preventing a hip fracture death and getting them out of the hospital on the other is also valuable for the system as a whole.
[00:30:27] Dr. Grant Garcia: And I want to do one thing that's going to, this is going to resonate with the patients, because this is what always, they always ask me. I'm like, you know, I do a PRP on somebody and they're like, well, what's the downside? What's the downside of supplementing patients?
[00:30:37] Dr. Reza Jazayeri: Zero, absolutely not. Zero. I mean, look, look, everybody, no matter what, is going to have a catabolic hit because of surgery.
[00:30:47] Dr. Reza Jazayeri: Your body is just going through the stressful response. And in order for you to be able to keep up with that, you're just going to harvest your own tissue, your own muscle. And so that was an evolutionary kind of, set for our [00:31:00] muscle to have this reserve to be able to kind of deal with this catabolic stress.
[00:31:04] Dr. Reza Jazayeri: But now if we can provide that, so I'll tell you, one of the really cool things that we're working on is we're doing intro up amino acids. Okay. There's good literature on that now when total hits, how do you do that? So you, you, you know, five years ago you weren't hanging a bag of TXA, were you? But you now
[00:31:23] Dr. Grant Garcia: I do it all day.
[00:31:24] Dr. Grant Garcia: My, my scrub check is TXA all day is his slogan.
[00:31:27] Dr. Reza Jazayeri: Okay. There you go. Okay. So for my shoulder arthroplasties, I do one in the, uh, in the beginning, one at the end. Right. And, and so
[00:31:33] Dr. Grant Garcia: every time. Every time.
[00:31:34] Dr. Reza Jazayeri: Right, right. And so before we, our shoulder arthroplasties by reverses, they would see in the hospital, two, three days wait for the drain to go down.
[00:31:41] Dr. Reza Jazayeri: And this, I'm getting an outpatient. I haven't kept the patient in hospital for arthroplasty. Maybe I had like a periprosthetic you know, it was a big deal, but otherwise they all go home. Right? So the same way you hang a bag of TXA, you hang a bag of amino acids now and we have that. And so, and so we're doing with some of the spine guys in New [00:32:00] York who are doing like really rapid recovery.
[00:32:02] Dr. Reza Jazayeri: Our advanced protocol we haven't even put this up yet, but I'm giving you a little teaser What what's coming is we have a latest and greatest
[00:32:08] Dr. Grant Garcia: here on this podcast. You're gonna hear all the earliest stuff
[00:32:11] Dr. Reza Jazayeri: Yeah, so we're doing intra up amino acid infusion And so what you see is when you and I are sitting here right now, we're making and we're breaking muscle It's it's like a it's like a dynamic just like bone right making breaking making breaking And so if, if you look at what happens during surgery, you, you break down a lot more and you're not making as much.
[00:32:30] Dr. Reza Jazayeri: So the net is you lose after the two hours of surgery, when you give intra op amino acid infusion, you stay exactly like you are now. So you're able to mitigate that drop. And so essentially you leave the surgery and you haven't had the muscle loss. So the impact of that will lead to, you know, faster recovery.
[00:32:48] Dr. Reza Jazayeri: So now this, we need to show the clinical side of it, but the intra op muscle synthesis and breakdown. The data is already there. That was a 2021 study.
[00:32:56] Dr. Grant Garcia: A lot of people that watch this show, orthopedic surgeons [00:33:00] who are going to tell their patients, they're going to see this and they're going to say, well, I want to get this product or whatever.
[00:33:03] Dr. Grant Garcia: And we'll go through this product really quickly in a minute. Um, but so what are you telling, like, is there a, so for me and my patient, right, I got my meniscus mastectomy patients and I have my, you know, my biceps tedious patients, the simple kind of recovery ones. But then I have my bigger stuff, like my ACL meniscus, Carlos transplant, we're talking about like three hours of surgery, a lot of work, a lot of atrophy, non weight bearing Carlos transplants, you name it.
[00:33:26] Dr. Grant Garcia: So are those the ones that you would focus on first if you're kind of trying to start this practice Hundred percent and trying to start the nutrition?
[00:33:32] Dr. Reza Jazayeri: Yeah. I, I, so we have kind of this, um, if, if you, on the website we have this kind of the high demand patients and we've broken up into two categories. We got the, we got the high risk, which are the infections, diabetic smokers, revisions, you know, the elderly patient, um, massive rotator cuff tear, right?
[00:33:48] Dr. Reza Jazayeri: You got, you got that group. Those are the kind of high risk patients. And then on the other side, you got the high demand patients. Those are essentially our athletes, our patients trying to get back faster. So I think, [00:34:00] you know, those are the two, um, patients that really are, are looking for, or would really benefit from it.
[00:34:06] Dr. Reza Jazayeri: And you can arise,
[00:34:07] Dr. Grant Garcia: you can have sometimes they can cross. I mean, I've got some patients that are crazy high demand. I've had three failed surgeries too. And that's also important. And those are the ones that are higher.
[00:34:14] Dr. Reza Jazayeri: That's a no brainer. That's a no. So, you know, in my conversation with my patients, you know, we all go through our discussion with our patients and one thing that comes up regardless of who you are, what.
[00:34:23] Dr. Reza Jazayeri: is patients always ask ab right? So tell me about are you doing whatever yo long am I gonna be in a s
[00:34:34] Dr. Reza Jazayeri: add this to my conversation. I say, look, in order to improve your recovery, we try to optimize your nutrition by using a supplement that provides you what you need for improved healing. That's it. You know, and, and, uh, and then, you know, really the, the company really takes over as far as there's a whole, it's like a concierge type service where they explain this to the patients.
[00:34:53] Dr. Reza Jazayeri: We have a whole, well, it's on the muscle sensor calculator. So if I, if I could do it for you right now, I would, you can go online and you could put in your [00:35:00] body weight, your sex, your age for you. And then it would give you a meal plan. So again, it's not just about the supplement. It's not just about the physical therapy.
[00:35:08] Dr. Reza Jazayeri: It's also where you're actually consuming. So we provide all these resources for patients who would otherwise have to go to some nutritionists or something. Does that come with
[00:35:16] Dr. Grant Garcia: your, is that, uh, okay, let's pause there. I want to talk about your company. Cause no one even said anything. We haven't even shown a picture of it and we're getting distracted, but I want to focus.
[00:35:27] Dr. Grant Garcia: So. That topic. So tell us about this company and then tell us about what comes with it. So you got your, your supplementation, but also the background stuff that you were just getting into.
[00:35:36] Dr. Reza Jazayeri: Sure. So, you know, I'll tell you how this kind of started actually. So I might, so my personal background before med school, I was in skeletal metabolism, and so I was, you know, That was pretty mad.
[00:35:46] Dr. Reza Jazayeri: So I was like kind of doing biopsies on rats anyway, and understanding how muscle works. And that was before meds, you know, so I kind of had this in my well,
[00:35:54] Dr. Grant Garcia: he was a natural surgeon. He was biopsy muscles before.
[00:35:58] Dr. Reza Jazayeri: So, so I [00:36:00] had this in the back of my mind, but then a few years back, I had a patient who came to see me for a revision ACL and he did an osteotomy.
[00:36:05] Dr. Reza Jazayeri: He came back and he's like, doc, my leg is finally stable, but I lost all my muscle. What do you have for me? And so, you know, I live in an area where the primary care docs, you know, they talk about anabolics, they talk about growth hormone, they talk about peptides and they talk about, you know, supplementation.
[00:36:21] Dr. Reza Jazayeri: And so when I talked about supplementation, he's like, well, doc, you know, are you, do you know about the, all the amino acids stuff that we're, that we're using for NASA? And I said, Oh, whoa, what do you know? And so that, so that blew my mind. So I called him back and we brought him on essentially. We are really, really late to the game.
[00:36:39] Dr. Reza Jazayeri: The guys who've been really studying this. NASA got onto this a long time ago because they had to study what can they do in order to prevent the like the really rapid muscle loss that happens when you go to outer space. And so in order to be able to prevent muscle loss, you can't take a bunch of food with you.
[00:36:56] Dr. Reza Jazayeri: But they identified what were the key amino acids that you can [00:37:00] consume to prevent muscle loss. This is where all the studies actually started from. Okay. It came from muscle loss studies in order to prevent that degeneration that you see in outer space. And then that got extrapolated now to a lot of the stuff that we're doing now.
[00:37:16] Dr. Reza Jazayeri: So that's how the company actually started. So, you know, this was, this is how it kind of got started. And then when I kind of tapped into this, that's when I kind of really dove into this. I looked at, you know, we looked at burn patients, right? Burn patients are supplemented with these amino acids and they're getting better faster.
[00:37:32] Dr. Reza Jazayeri: And I realized, wait a minute, What is a burn have to do with orthopedics? What's collagen? Collagen synthesis. They have the same underlying pathophysiology, right? You want to increase blood flow. Well, how do you increase blood flow? We're doing it for guess what? Angina supplements. There's supplements for erectile dysfunction.
[00:37:48] Dr. Reza Jazayeri: You know, there's supplements for a lot of different things in the body. And similarly, they're being used for burns as well. So when I looked at that, I said, wait a minute, if we can improve blood flow to an area, well, guess what? They're using these [00:38:00] supplements for diabetic wound ulcers, right? So to me, when I started to look at all these supplements are being used in different subspecialties in AIDS patients, in wasting disorders, and I'm like, this is actually ideal for an orthopedic surgeon, because these are the issues that we're dealing with muscle loss.
[00:38:17] Dr. Reza Jazayeri: And and wound healing and bringing more blood flow and giving the key amino acids at the right dose To be able to enhance these processes
[00:38:25] Dr. Grant Garcia: and i'll say a little tidbit and this is just off topic But when I I had a major surgery a couple years ago And the first thing I was looking at supplementation and I went on and got some collagen powders and did all the stuff I could But obviously didn't have this stuff Available and I would have jumped on it right away.
[00:38:39] Dr. Grant Garcia: I mean, but obviously I, but it's still knowing that I had to do all that extra stuff myself, legwork, figure it all out. And I wasn't really doing a lot of evidence based medicine. I just wanted to give myself the best possible option. And so why wouldn't I do that for my patients? And now that I have a much easier option, not just saying, you know, I used it in my surgery.
[00:38:58] Dr. Grant Garcia: So therefore you should [00:39:00] use it more like we have evidence based, but it's just interesting to hear this because I'm just like those patients in Seattle that come in and they're like, I want everything. Like, I want to get back. The fastest I don't have any time like I, I need to be back on my feet in the operating room in four weeks or I was going to be freaking out.
[00:39:15] Dr. Grant Garcia: I'm private practice. Like I had to be back and I don't have time. And again, I'm not a pro athlete, but we have a pretty aggressive job and we don't get to use these. That's right. Have anything. That's right. That's right.
[00:39:26] Dr. Reza Jazayeri: So, so, so that, so that's, this, this was what was born out of, of kind of, you know, that, that one patient that really stimulated, it.
[00:39:33] Dr. Reza Jazayeri: you know, think about this. And I've already been recommending supplements and working with some of the guys here. But then I said, you know what? I didn't trust the supplement out there. That was the problem. So then understanding who to work with, getting the NSF for certification, knowing exactly the right dose, basing on literature that you and I are comfortable with.
[00:39:49] Dr. Reza Jazayeri: This was like 56 years in the process to finally have this conversation with, you know, and gathering data. And it's and it's interesting now to see The orthopedic community is now looking at this [00:40:00] more initially because of the hip fractures and the elderly patients because muscle loss in them. So sarcopenia is a big issue, but now we can extrapolate it and implement it for, you know, our, all our patients actually.
[00:40:12] Dr. Grant Garcia: And I think it's important for patients again, to remind them there is no downside to this. It's, it is going, if anything, it gives you even a few weeks better recovery, in my opinion, it's worth it. If it was my surgery, I would do it no matter what. And just the problem is you need to be able to have the access to it, right?
[00:40:28] Dr. Grant Garcia: And you need to have the understanding of it. And this is really, it's really key. And I'm excited that we're all, we're having you on the show and everyone can hear about this. Um, cause now I can reference this talk, right? It's, you know, it's like you said, you just tell them I'm going to supplement you after surgery because To be honest, we can have this whole 43 minute talk.
[00:40:44] Dr. Grant Garcia: If you had this talk to every single person, you would have no time left in your day.
[00:40:47] Dr. Reza Jazayeri: Well, so you, you just took the words out of my mouth. I was just going to tell you. So when I realized putting this together, because I don't, we don't have the time to do this. What I, what I wanted to create was the pain point, not just for the patients, but also for our practice.
[00:40:59] Dr. Reza Jazayeri: I [00:41:00] don't have the time to have this kind of discussion, even though I really, really want to, okay. It just doesn't exist. So we created a kind of a concierge service for any patient who signs up for this, has access to. someone will call them bac explain to them what it i list is dietary support t there's a lot of look pat Covid.
[00:41:19] Dr. Reza Jazayeri: They're much more consume, what they can do We don't have the time, but if we have a good resource that we can provide them, this is how we can make a positive impact.
[00:41:33] Will Sanchez: I think that's awesome. That's awesome. What's the process for, for your patients, uh, for you to determine, um, what is the right combination for each patient?
[00:41:42] Will Sanchez: Is it lab work? Uh, you know, what, what, what goes into it? Blood work? What, what happens for you to make that determination? This
[00:41:49] Dr. Reza Jazayeri: is a, so great question. So because. The body goes through this catabolic stress and the requirements are elevated for these [00:42:00] key amino acids that are needed for muscle and bone and collagen synthesis.
[00:42:04] Dr. Reza Jazayeri: You can apply this to any orthopedic surgery. Actually, to be honest with you, we're getting a lot of interest and a lot of positive feedback from bariatric surgeons and plastic surgeons. We even have a one of the guys who's really been using this a lot as a breast reconstruction surgeon, right? Same issue, right?
[00:42:18] Dr. Reza Jazayeri: Patients, those patients, Or or after cancer, chemo, radiation have breasts and then now they're really mal malnourished. They need everything they can. So this, so this actually has simplified it, right? That's the other thing that's really important. If you're gonna do something that's gonna work, it also has to be simplified, right?
[00:42:36] Dr. Reza Jazayeri: So this is simplified. This is one week before, two weeks after. and it's been dose where a 14 year old ACL can take it. Also, your 82 year old grandmother can take it. So under
[00:42:46] Dr. Grant Garcia: 18 can have this too.
[00:42:48] Dr. Reza Jazayeri: Yeah, the only issue is if you're under 70, um, they're, you know, we decrease the packets usually take two packets a day for someone who's under [00:43:00] 70.
[00:43:00] Dr. Reza Jazayeri: They just don't need that. Uh, we just because I'll just pee it out. It's like there's there's zero issues with toxicity on this. These are amino acids that are free form. You know, you consume them. Otherwise they go through the unit.
[00:43:11] Dr. Grant Garcia: So they'll do this and they'll get how many packets with
[00:43:14] Dr. Reza Jazayeri: this? So it's three.
[00:43:16] Dr. Reza Jazayeri: So they get three boxes. and each box has 14. So they do two of the two a day for, uh, for three weeks. So that's all, that's all, you know, that patients have to think about is a three week supplementation one week before and two weeks after. I have some patients who feel better afterwards. They like the energy.
[00:43:34] Dr. Reza Jazayeri: They, you know, we, we, you know, we, we hear all these different things where you're doing ACL and someone, but they're like, Hey, my upper body strength is better. My mood is better. My energy is better. So they're, they're actually not coming back. And we have a patient that's Like a subscription where they stay on it as a daily, but you really want to hit them for that opportune time that we can be showed on that graph is, is that, is that, is that critical time?
[00:43:53] Dr. Reza Jazayeri: The one week before in order to build the resilience to build up the amino acid pool. And then the two weeks after when [00:44:00] they're most catabolic, if you can, if there's one time to hit them, it's that three week window. And
[00:44:06] Dr. Grant Garcia: if you can't get it, let's say you were saying, So two weeks after most important, but if possible, three weeks is recommended.
[00:44:12] Dr. Reza Jazayeri: Yes. So when I see my patients, I usually see my patients about a week and a half to two weeks before. And then there's a QR code that they just scan and then the company just ships it to them. And I think you work with, uh, um, recovery shop. Yeah. So we're on multiple platforms. Recovery shop is one of them.
[00:44:28] Dr. Reza Jazayeri: They're great because the patient just scans your QR code and then they drop ship it to them. Um, some surgeons like to have it at their place, like a curling joke. It's at their DME. So they see Dr so and so and they walk down and they pick up their box and they go home with it. So there's different ways of doing it and we have kind of a mix for different facilities.
[00:44:46] Dr. Grant Garcia: Yeah, for me, I mean, my longterm plan with it, obviously, and I'll tell patients, they're going to, this is going to be offered probably very soon. It's already in the works since we've been talking. Uh, but it's part of this enhanced recovery protocol, right? So you get a, we'll talk about the next, next episodes.
[00:44:59] Dr. Grant Garcia: Can we talk about the nice [00:45:00] machine? And the episode after that, we'll talk about the other machines we have and other options. And so it's all part of this bundle where it's like the enhanced bundle, right? You get the recovery, you get the machines, things that you just can't normally get. That's
[00:45:11] Dr. Reza Jazayeri: actually what we're seeing.
[00:45:12] Dr. Reza Jazayeri: Like, um, Some of the guys at HSS are also using, um, the recovery shop and it's, they have these bundles that they do. And then, so they put XR in their, in their like ACL or their total knee or total shoulder bundle, you know? And, and so it's no
[00:45:27] Dr. Grant Garcia: coincidence. I went to HSS, so I got to
[00:45:31] Dr. Reza Jazayeri: Are you getting
[00:45:32] Will Sanchez: folks that, that kind of want something like this, uh, even post op and saying, man, I'm feeling really good.
[00:45:38] Will Sanchez: I'm starting to work out. I really need to kind of elevate myself, you know, as someone that's like I said, we discussed earlier recovering that I still am struggling with that. Absolutely. You have a patient like myself saying, please, I, I, I need, I need a boost. How do, how do they go about that?
[00:45:55] Dr. Reza Jazayeri: So, so interestingly, you know, when, you know, we, we, we, we have [00:46:00] done this on multiple, um, kind of demographics.
[00:46:03] Dr. Reza Jazayeri: Um, and you know, obviously we're talking about the surgical patients and they need a higher dose of that. But I'll tell you what's really fascinating with these really extreme athletes. they're willing to put their bodies through some ridiculous things. Okay. And, and the amount of stress that they put through their bodies as like one of these crazy bodybuilders, their demand is actually not that different than what we want in our patients who are coming out of orthopedic surgical recovery.
[00:46:30] Dr. Reza Jazayeri: Right? So they want muscle synthesis, they want collagen enhancement, right? They don't, they don't want, they don't want to, um, They want to be able to get back to their sport and where we're seeing this used a lot right now. So one of our, um, one of our teams that's using this, you know, for Major League Baseball, um, they.
[00:46:48] Dr. Reza Jazayeri: won the championship last year. Okay. But, um, they are using it as a, almost like a preventative. And I'll tell you something really interesting. A lot of the science that we have on this [00:47:00] didn't come from orthopedics. It came from the, the scientists were have been studying this on athletes. So something that athletes get, I've heard of DOMS, delayed onset muscle soreness.
[00:47:09] Dr. Reza Jazayeri: When you work out, you're sore. Yes. Uh, okay. But if you, if you look at it in an objective way, there's something called EIDM, exercise induced muscle damage. What that basically means is if you train really, really hard, you break down your muscle tissue. And just like when you get a heart attack, you can check troponin levels.
[00:47:24] Dr. Reza Jazayeri: You can say, Oh, someone had a little heart attack or a big heart attack. Based on how much to form well up where you can check how much you damaged the muscle tissue by the intensity of your workout and you can objectively look at that by the creatine kinase level. And so creatine
[00:47:39] Dr. Grant Garcia: like next level, like the people that go do CrossFit too much and they can get like go to the hospital, right?
[00:47:43] Dr. Grant Garcia: Exactly. So much damage.
[00:47:45] Dr. Reza Jazayeri: Exactly. And so you can use these amino acids and these amino acids, you know, we talked about the essential amino acids. Those are the nine that are essential. There's something called branch chain amino acids. Those are the BCAAs. You may see that. Those BCAAs, those are the
[00:48:00] three of those essential amino acids.
[00:48:02] Dr. Reza Jazayeri: They're still essential, but the three of them have these branched chain. Those have been shown, particularly in the exercise world, to reduce that exercise induced muscle damage by creatine kinase levels. So a lot of the athletes, a lot of the, um, strength coaches and the major league baseball nutrition and dietitians are aware of the science and so they use this for enhancing their athletic recovery.
[00:48:25] Dr. Reza Jazayeri: Okay. And recovery is really the key now for enhancing performance because no longer are our athletes limited by how much they can work. They're limited by how fast they can recover. And that's where we're seeing the difference, okay? Because if you have nine months to train for something, and if you work out really hard, but you're sore for four days before your next ability to train and build on that previous gain, you've only had so many sessions.
[00:48:51] Dr. Reza Jazayeri: But if you can shorten that training period by having improved recovery, Then in that nine month period, you've really tacked on a lot more [00:49:00] training, effective training sessions. That's where these athletes are using it. So it's your point, Hey, you know, who else can use this or benefit from this?
[00:49:07] Dr. Reza Jazayeri: Especially if they've this for years. Well, this sounds like a
[00:49:11] Will Sanchez: game changer, especially when it comes to sports, because, you know, this is, you know, You know, I'm a huge sports fan. I've worked in sports forever. Um, you know, this was the conversation when you had, when you talked about a Barry Bonds and a Mark McGuire and certain athletes that were affiliated with the steroid era.
[00:49:27] Will Sanchez: And, you know, say it's not going to help you hit a ball. It was the recovery, right? That's that these athletes were looking for. And if there's something like this, not just for the athlete, but for, but that's
[00:49:38] Dr. Grant Garcia: legal and not steroids.
[00:49:42] Will Sanchez: It's the recovery process, whether it's athletes or ourselves, that we can feel better quicker.
[00:49:47] Will Sanchez: We can go to the gym three, four times a week, and our recovery time is better. Just maybe having something like that in the future, and it's all working naturally with the amino acids that belong in our body, that's a part of [00:50:00] it. That's just, it's like the, the, the fountain of youth, the holy grail.
[00:50:05] Dr. Reza Jazayeri: Well, I'll tell you, you know.
[00:50:07] Dr. Reza Jazayeri: Nutrition and what you put in your body is, is, is really key. I mean, mm-Hmm. not to get too deep into the science of it, but literally the amino acids that were tagged in some of these studies that you consumed, you can biopsy them outta your muscles in, uh, in, in about a day. And so our body is, is turning over about.
[00:50:25] Dr. Reza Jazayeri: All of us right now are in one day, we're turning over about 300 grams of protein. We're making, we're breaking, we're making, we're breaking. If you eat maybe a hundred grams of protein a day, that means 200 of it is being recycled. So there's a huge turnover. And so during the time of surgery where you're breaking down so much, you just can't keep up.
[00:50:43] Dr. Reza Jazayeri: So you lose it. So this is very simple. We can take something very complicated, really simplified to say, look, during this time of surgery, when you got this huge hit, just give your body the exact amino acids it needs. To then prevent that loss. And that's where we're seeing that improvements. Exciting.
[00:50:59] Dr. Grant Garcia: Well, I don't want Reza, [00:51:00] you, we could talk, as I mentioned before, so basically
[00:51:03] Dr. Reza Jazayeri: tell us
[00:51:05] Dr. Grant Garcia: about
[00:51:06] Dr. Reza Jazayeri: the future
[00:51:07] Dr. Grant Garcia: horizons of it. And then we can wrap it up.
[00:51:11] Dr. Reza Jazayeri: Yeah. So one thing we didn't really get into, we talked about amino acids, but peptides are a little bit different. Peptides are usually injectable. Okay. And, and that's a, and that's a little bit different than, than, I mean, so I mean as you can orally consume, you can get them, you know, uh, at, at, at your GNC or whatever, but, but peptides are a little bit different peptides is when two amino acids come together.
[00:51:36] Dr. Reza Jazayeri: Okay. When they get linked, so what's a peptide that we're all familiar with? Insulin, for example, insulin is a peptide. We use it all the time. Oxytocin is another peptide that we can constantly, these, um, uh, the GPL one agonists, these are all peptides. These are for diabetes. So peptides are being used. For, for since 1920, since they were identified.
[00:51:58] Dr. Reza Jazayeri: The one that is be, [00:52:00] be being used in the, in the recovery world, that's still not FDA approved, but being used by a lot of these athletes, for example, um, is B PC 1 57. That's what maybe some of your patients asking salt tissue repair one, right? Yeah. And that one I'll tell you. If it weren't for me seeing, and by the way, I sent you guys a couple of art.
[00:52:18] Dr. Reza Jazayeri: I sent you an, uh, the articles, these references. So you have a grant. If you want to put it up for your patient, this was done in, this is, these studies were done mostly on, I have to say this on rats and on animals. So they're not on humans yet. Okay. But there's so much literature, MCL study, MCL tears, Achilles tendon tears.
[00:52:33] Dr. Reza Jazayeri: They take these, uh, these animals and they, you know, basically cause this injury and then they take this BPC, which is, Body protection compound. This is a peptide that lives in our guts already. Why in our gut it's so important for recovery because we're constantly needing to keep everything outside because from our, from our mouth, through our butt, essentially, that's the GI system and is constantly regenerating.
[00:52:56] Dr. Reza Jazayeri: So this BPC com peptide [00:53:00] increases, angiogenesis, increases vascularity, and helps with FibroGen. production. This is why it's used in all sort of colitis. It's been used in all these G. I. Issues. These athletes now have been injecting it for years now, and I see them because they come back and they look very different.
[00:53:20] Dr. Reza Jazayeri: So that's what that's the next step that we're looking into is, is can we safely study this? The problem with these peptides? The reason the FDA is saying no is because anytime you say we're increasing angiogenesis and you and I are excited because we're like, wait a minute, that's why I do a micro fracture.
[00:53:35] Dr. Reza Jazayeri: That's why I do PRP. That's why I do all the stuff that I'm doing. You can increase baby cancer and that's where everyone says, okay, I'm gonna hold off And so we're trying to find a happy means to hey, look if someone's having surgery and for six weeks They got a third rotator cuff repair that we can't get to heal and we're seeing Biological histological studies on these rats showing improved tendon healing Incredible studies done, but [00:54:00] we still haven't been able to translate it into the human.
[00:54:02] Dr. Reza Jazayeri: So I think this is where we're going to see the next of where these peptides safely being studied where some of the Um researchers are we're looking at setting a usc
[00:54:10] Will Sanchez: And can you give a quick warning because when I look it up I can see it out there, you know And so I don't know if it's the real thing or what somebody's it's aftermarket.
[00:54:20] Will Sanchez: So if Someone that's listening to the show is seeing a bpc, you know bbc 157 somewhere You What is your warning to anyone out there besides the fact that this hasn't been approved?
[00:54:32] Dr. Reza Jazayeri: So it's being utilized. It's been used for probably over a million people have used it now. Okay. Um, so it's the, the, the, the LD 50, which is the lethal dose on this is extremely high.
[00:54:43] Dr. Reza Jazayeri: You really can't hurt yourself on. That's why it's been utilized for so long. It started out in Europe, but in the States now it's extremely common. You know, like I said, half my patients here who come already, you know, are on it or asking me about it. And we're just modifying it with some of the other docs.
[00:54:58] Dr. Reza Jazayeri: Who are providing it. So [00:55:00] I would tell you don't get it online. Do not get it online. Even though you can go to a licensed physician who has been practicing this for a long time, who understands peptides and understand your risk, I can't say yes and I can't say no. I can tell you it works okay. But we're at currently today as it stands, orthopedic surgeons.
[00:55:19] Dr. Reza Jazayeri: Don't prescribe it. Uh, it's not in our armamentarium yet, but for sure it works. And so it's just a matter of time. And this is where, you know, when you see something that works by the time the FDA actually approves it, uh, it's going to be further down the line. So I'll tell you, here's the future. It involves immediate weight bearing after injury.
[00:55:40] Dr. Reza Jazayeri: I can't stress that enough. How important weight bearing is. Okay. Starting the, starting the amino acid supplementation at the time of injury and getting into the prehab intra op amino acid supplementation as soon as you can, weight bearing and actually safely BFR pre op and
[00:56:00] post op. And then these peptides I think are promising for, you know, for the immediate post op period for the six to eight weeks.
[00:56:08] Dr. Reza Jazayeri: Some people live on them. You know, um, but I would say from a safety perspective, um, 68 weeks is not unreasonable.
[00:56:17] Dr. Grant Garcia: That's going to be an awesome quote. I love it again. Remember everybody peptides orthopedic surgeons can't prescribe them But there's other doctors that can that know them better. So go to those people for that last piece Everything else we can safely do and it's fda approved.
[00:56:31] Dr. Grant Garcia: Uh, and so this is going to be awesome
[00:56:32] Dr. Reza Jazayeri: You guys there's a lot of information. So I work with a lot of residents and stuff So there's a lot of clinical studies that we put on so if you go to xr science, um This is essentially an organization of, um, you know, providers and athletic trainers and surgeons who've come together
[00:56:51] Dr. Grant Garcia: on the screen guys.
[00:56:52] Dr. Reza Jazayeri: Yeah. So there's a lot of good. If you look under the, um, healthcare provider section, you'll see the clinical studies. Um, and so that then you guys [00:57:00] can reach out to our team out there if you have any questions, but this is really an exciting time because it's more than implants now, you know, we have, we have to be more educated on this stuff so we can better help our patients.
[00:57:09] Dr. Grant Garcia: We finally have more tools because like, I'm sick of my first few years of practice. I was sick of telling them that like, I'm just going to give them all the best implants. And then you get like, then that like gets boring. And then you're like, I have nothing left to give you. And then like, but I want to be better.
[00:57:22] Dr. Grant Garcia: And how can you beat the guy next to me? And how can you give, how can I be more enhanced and, you know, other than weird off label things and things that are inappropriate that I would never want to offer now, I have these things. You know, this is one of those things I'm not gonna be able to offer.
[00:57:35] Dr. Reza Jazayeri: Yeah.
[00:57:35] Dr. Reza Jazayeri: And I'll tell you of the things that I told you, the amino acid is so elementary actually, in my mind, now that I've seen what's out there and what we're using, like, so when people are like, Oh no, these amino, and I'm like, Oh my God, this is like, so elementary. I'm not even going to explain it. tell you the other stuff that we're already doing, you know, because it's just too much, you know, you have to, yeah, no, no
[00:57:54] Dr. Grant Garcia: baby, baby steps for everybody.
[00:57:56] Dr. Grant Garcia: But to be honest with you, as we know with orthopedic surgeons, it, everything takes a [00:58:00] little bit of time and you have, you get stuck in your ways. Um, but the one last thing that's really cool about this company too, is that it was started by you as an orthopedic surgeon. I think that people, when we offer things, Like PRP and things like that and they come to us they like it because we're the orthopedic surgeons offering it It's not someone who doesn't have expertise in the surgical and the non surgical route and so this is really important for us because it's just there's so many of these random companies that offer things that are not approved or they're They're in a run by just businessmen and there's not any background to science on it, right?
[00:58:30] Dr. Grant Garcia: And there's not the certifications and those things so it's really nice to have that you've done all the work You're a clinician, you're a good guy, you've done the research, you've got the certifications, the safety things, it's all important for our patients to know that, that, that the surgeons like myself, I can confidently go in tomorrow and I had a patient Yesterday I said I got this guy on a podcast.
[00:58:48] Dr. Grant Garcia: You're gonna love it. You're gonna get some amino acids for your post op recovery. Just wait till it pops up and they're like, when is it coming? When is it coming? I'm like, listen, we'll see how fast it gets edited and things like that.
[00:58:57] Dr. Reza Jazayeri: Yeah,
[00:58:57] Dr. Grant Garcia: but you know, this is I feel totally comfortable [00:59:00] tomorrow Offering this and this is good for everyone to listen to and hear
[00:59:03] Dr. Reza Jazayeri: You know, we've been using this for over a couple of years now, and I'll tell you, I'm still learning so much.
[00:59:10]
Dr. Reza Jazayeri: And these, these conversations that we're having are, I'm just excited to kind of share this with you because I learned through the process and, you know, maybe we can study some of your patients. And I'm always interested in research and learning more. By no means is this the end. I think this is actually the beginning.
[00:59:23] Will Sanchez: Thank you so much, uh, xrscience. org Guys, thank you so much for having
[00:59:29] Dr. Reza Jazayeri: me. This is exciting. And, uh, you know, we'll keep this going. And, uh, look forward
[00:59:37] Will Sanchez: to, you know, pushing this together. very
[00:59:40] much. Appreciate it. Audio Transcript
Dr. Andre Shaffer: Spine surgeon and cutting edge technology in spine
Will Sanchez: [00:00:00] Dr. Garcia, welcome. That's my jam right there. It got a little like, you know, you guys did such a good job. We did such a good job. Anyway. Hey, thank you everyone. And thanks for listening to sports doc. Talk. Be sure to check us out on your favorite listening platforms. We're on Apple. We're on Spotify. I heart you name it.
Will Sanchez: And now with our videos, please check out our YouTube page. Dr. Garcia, we're really excited about our guests, but before we bring on our guests, how are you? I know I was having some issues. I didn't know if we would get the show going today because I was having internet issues and I was scrambling, but I'm hoping that your day was a little bit better than mine.
Dr. Grant Garcia: I was scrambling, but not from internet issues. Uh, it was [00:01:00] good, busy, you know, as usual. Uh, but yeah, I'm excited we can do this show. I mean, we just put on one last week, but this is, A really important guest that I'm excited for people to share. And, you know, we have breaks coming up and everything. So I was hoping we could get this on.
Dr. Grant Garcia: And I'm so excited, uh, to introduce this. As you guys know, I ranted for about five minutes introducing this show about a week ago. Uh, so hopefully anybody heard that. If not, you will hear the update today. Um, I don't know if you want to kick it off and we'll go from there.
Will Sanchez: Yeah. Let's bring on a, he's in our green room.
Will Sanchez: All right. We're going to send somebody to go get them. No, it's not that, not that complicated. Let's bring on a Dr. Schaefer there. Dr. Schaefer. Welcome. Thanks for hanging out with us. Uh, Dr. Schaefer, I, I, I bothered Dr. Schaefer there and I was like, uh, are you still in the operating room? You got your scrubs going on, but I love how he said, you know, you, you gotta be ready to stay ready.
Will Sanchez: So, uh, welcome to the show. Dr. Schaefer.
Dr. Andre Shaffer: Thank you. Thank you. Pleasure to be on really. Uh, it's a privilege.
Will Sanchez: Go ahead, Dr. Garcia.
Dr. Grant Garcia: Yeah. [00:02:00] Schaefer. This is Dr. Andre Schaefer. He's a spine surgeon actually in my group, which is awesome. And we actually know each other really well. I've been friends for way too long.
Dr. Grant Garcia: Uh, we went to hospital surgery, special surgery together, and he had the privilege of taking care of some pretty amazing athletes as well. Uh, while he was there with me. Um, and we've got along working together in residency. Yeah. Um, he actually went to Cornell, uh, undergrad as well, so he's kind of a slacker.
Dr. Grant Garcia: And then now you have him having triple fellowship training, uh, as he did one, uh, in Harvard for trauma, uh, two at, um, in two in Seattle, he did hip preservation, but really the big thing in one of his real passions, again, with some minimally invasive stuff coming out with spine. And so he just, He finished his spine fellowship.
Dr. Grant Garcia: He's been in prior practice for a little while and now he's joined us and we are so happy to have him. I can tell you right now that I have way too many partners coming up to me telling me how [00:03:00] excited they are to have Dr. Schaefer as part of the group. Um, and for me it's near and dear because it's really been nice to have somebody like that that takes things by the reins and he's doing so many cutting edge things in Seattle.
Dr. Grant Garcia: Uh, I don't want to brag too much about you, Andre, cause you have to speak at some point. Um, but he is, he was the first, uh, person in all of Washington state, uh, to perform endoscopic spine. And I think I'm an endoscopic spine outpatient, especially with the new Arthrex system, which. We know we like to talk about that and it was no internal brace will, but he still did it with just a regular scope.
Dr. Grant Garcia: So we're going to talk about this procedure. It's really important, near and dear to me as well. Um, but enough of that, let's talk about how Dr. Schaffer is doing.
Dr. Andre Shaffer: Ooh, I got three kids and my wife's putting them to bed. So I'm, I'm happy to be up here talking about spine.
Will Sanchez: That is great. In fact, you know, let's, let's, let's take a quick look at the beautiful family. I mean, your resume [00:04:00] is legit, you know, as you know, Dr. Garcia tongue in cheek over here saying you're a slacker. But, uh, I mean, your, your journey has been a very interesting one. You know, can you just give us a, just a brief look in insight into, you know, how you went from firefighter to now just say a renowned surgeon, you know, just, uh, a little bit of that journey.
Dr. Andre Shaffer: Yeah, absolutely. Yeah. You know, so, um, I was born and raised here in Seattle. I was a Seattle firefighter for seven years. Um, and it was really a colleague of mine who, uh, fell about 45, 50 feet. Um, while training that even got me to go to college. Um, and so, uh, you know, went to the university of Washington, a proud Husky.
Dr. Andre Shaffer: Um, and while I was in college, I kind of found my footing academically and decided, you know, maybe I should shoot for something a little bit more. Uh, [00:05:00] Um, sort of rigorous than just being a firefighter. Loved being a firefighter, nothing
Will Sanchez: rigorous than a firefighter. That's a, that's something that you don't always hear.
Dr. Andre Shaffer: Yeah.
Will Sanchez: Being just a firefighter. That's amazing.
Dr. Andre Shaffer: Yeah. So, you know, I, I, I, I went to, I guess I went to undergrad did well. And then, yeah, I got to go to Cornell. I applied. Um, and got in. And so then, you know, sort of like the dog that caught the car, you know, so I got, I got into medical school. So I should, I should probably go.
Dr. Andre Shaffer: Uh, so went to medical school, um, at Cornell. And then me and Grant met, uh, first day of sub eyes actually, uh, in Seattle at University of Washington. And then we ended up matching at HSS together
Dr. Grant Garcia: on the other side of the country. Yeah. And so it is history. You can't make that up dude. We literally worked together for a whole month in Seattle at University of Washington doing trauma, which by [00:06:00] the way, everybody knows I'm not a huge fan of that.
Dr. Grant Garcia: I like sports. Uh, but nonetheless I did it because I was interested in going to U Dub and then we ended up together in New York, which was crazy because we didn't really know until We showed up, I saw your picture and I was like, dude, I know that guy.
Dr. Andre Shaffer: Yeah. Yeah. It was a good time. So, so yeah. So now, yeah, now I'm here.
Dr. Andre Shaffer: And I, you know, I, uh, you know, when I was in residency, I wasn't, um, you know, a lot of our spine was open. I was, I was interested in spine, you know, from biomechanics and sort of, it's, it's, it's, it's, it's, it's important, right. Spine connects your head to your torso. And so, uh, Very important stuff, but just, it was so open that I wasn't really as much of a fan of that.
Dr. Andre Shaffer: And, and, you know, the patients had a hard time kind of bouncing back from some of the bigger surgeries that we were doing. And so it wasn't until I was in my trauma fellowship and I'm, um, and you know, I'm seeing some of the, some of the work that people like Andrew Simpson was doing up at [00:07:00] Harvard, you know, big MIS proponent, um, and watching them do tubular micro decompressions and seeing like, Oh wow, there's, there's an alternative.
Dr. Andre Shaffer: And so that was what got me interested in spine. Um, and then when I was doing my hip preservation fellowship as well, seeing how much overlap there was between the hip and the spine and how many patients would come in with hip problems that we would send off for their spine. And vice versa. Um, and so, you know, that, that kind of primed the pump and then I went off and did trauma and hit for a while.
Dr. Andre Shaffer: And then, you know, finally, when I started hearing about, you know, spine endoscopy or endoscopic spine surgery, that was the thing that kind of told me, Hey man, we gotta, I gotta, I gotta go back. I gotta circle back and figure that out. And so I got to work with, uh, Some, uh, really great neurosurgeons and orthopedic surgeons in my spine fellowship, uh, down in Phoenix, Arizona.
Dr. Andre Shaffer: And, you know, they, they enabled me to kind of go to whatever classes and courses I wanted and kind of check [00:08:00] stuff out. And, you know, my program director was interested in endoscopy as well. And so we, we did, you know, uh, a handful of them. during the year. And then I, that kind of, I kind of took that, um, that basis or that, that, that foundation and said, Hey, let's run with it.
Dr. Andre Shaffer: So
Dr. Grant Garcia: this is a good segue. So we'll see this. You saw this with, uh, Dr. Acevedo. Um, you went from open spine surgeon to minimally invasive spine surgeon to if patients don't know what this is, you are essentially scoping their spine. And you took this to the next level because people, we talked about this in the surgeries I do.
Dr. Grant Garcia: You see the surgery. You practice, you practice, you practice, and then you do it on a patient. I've seen where you, I know what you've done behind the scenes, obviously, because we chat about it all the time, but maybe tell the audience, like, how did you get this level? Like, it's not, everyone can say, like, this is, this is like going from, like, making cereal to A filet [00:09:00] mignon.
Dr. Grant Garcia: Like this is next level stuff. Like he went to, he's going to, you can't see anything that's going on until you put that scope in. So you're finding it localized. And this is this incision, this looks massive, but you know, I'm an arthroscopist. This is, this is my wheelhouse in terms of these scopes, that incision on the screen is like this big.
Dr. Grant Garcia: So tell the audience like what it takes to get this level. So people need to know that, you know, this is not something that just straight over simple, easy to do.
Dr. Andre Shaffer: Yeah, no. So, I mean, you have to have a number of, um, skills. And I think. You know, this is where some of my other experience doing trauma, you know, kind of kind of comes in because a lot of the first portion of your case is localization with an x ray.
Dr. Andre Shaffer: And that's something that if you do trauma, you're really comfortable, you know, steering needles, steering, you know, dilators to specific place using an x ray and doing it safely. Right. So, you know, the first thing is understanding the anatomy, understanding what you're trying to actually accomplish with your tools.
Dr. Andre Shaffer: So that you can use an x ray [00:10:00] machine to get there safely. Um, and so that, and that, that, that, that's tricky, right? Because you have to, you have to find out where you make your incision. You have to find the trajectory and there's a lot of planning and work that goes into it. You know, you know, the patients, you know, get, Onto the table and, you know, I'm taking x rays and measuring things and being really careful and they almost look like a blueprint, you know, because there's so many markings, but that's, you know, because I'm trying to make sure that we make one incision that we're being as minimally invasive, but also as safe as possible in the process.
Dr. Andre Shaffer: Um, and so, you know, you make an incision, you take x rays that are, you know, AP lateral, which are different types of views, you take some oblique views, um, and you kind of combine them so that you get a sort of a three dimensional representation of what you're looking at in your mind. And then it just, you know, it's, you know, you know, sports grant, it's, it's, it's, uh, triangulation and, and just, you know, kind of having the hands to, to say, this is the angle that I'm going to go for.
Dr. Andre Shaffer: And this is, this is where it's at. Um, and so what that took for me was, you [00:11:00] know, going to, you know, cadaver courses and then beyond that, you know, practicing on cadavers and, you know, practicing, you know, in the lab a number of times so that we, you know, so we felt like we were ready for, For primetime. And so at this point, I've probably done 40, 50 levels in the lab, just making sure that I can, you know, consistently target that I can consistently get access to the, to the foramen or consistently get access to the interlaminar space so that we can be safe and effective.
Dr. Grant Garcia: And I think it's important for people to know, like, this is not a skill that's, easy. Uh, I everyday scope, right? I'm doing five scopes, six scopes and UC residents to try to do it or fellows as they start and they struggle the triangulation. So Dr. Schaefer went from a spine surgeon. He had the hip arthroscopy skills.
Dr. Grant Garcia: He has the skills he learned at HSS. He has this trauma trauma skills, but he had to put all those together to do this. The result [00:12:00] is A significant improvement for patients, but also it shows dedication, right? Like there's a lot of people that don't want to do this. Not only is it challenging to get this product in a surgery center outpatient, which we will talk about in a minute.
Dr. Grant Garcia: But on top of that, getting an outpatient and doing it safely and doing it well is no feat. It is very, very challenging. This is, this is no, there's no joke here. And the fact that he's able to do it consistently is really impressive. And I think that I really want patients to know about this option because we've seen it.
Dr. Grant Garcia: And this is basically where sports was. About probably 15 years ago, and I think that we're literally at the cusp and I feel like will and I could have this conversation with you in two years and you'll be like, dude, I'm way beyond that. Like we're already like on this trajectory. And what do you think about endoscopy?
Dr. Grant Garcia: Um, and spine surgery? And where do you think this is going? I mean, I
Dr. Andre Shaffer: think it's I think it's it's it's at its infancy. You know, it's been good. It's what's crazy is it's not It's not new. It's been happening for 20 years, but it just hasn't gotten [00:13:00] the acceptance right in the United States. You know, people were doing it out in South Korea and Japan, but not as much in the United States.
Dr. Andre Shaffer: And so, um, you know, I'm kind of happy to be one of the one of the few people locally that, you know, doing it and, and, and being able to, um, being able to do it in the ASC and get people home right away. Right. You know, I, I, uh, I tend to call my patients, you know, two, three days later. And I had a, I had a guy a couple of weeks ago who I operated on and I called him, you know, on a Friday and I hear all this commotion in the background.
Dr. Andre Shaffer: And I'm like, Where are you? And he's like, I'm at work. I'm like, dude, two days
Dr. Grant Garcia: post op. What are you doing? He did his surgery on the Wednesday. So people need to hear this is two days later.
Dr. Andre Shaffer: I called him on Friday. He's like, I'm at work. And I was like, why? And he's like, I feel too good not to work. And I was like, are you taking it?
Dr. Andre Shaffer: He's like, I'm taking Tylenol, you know? And so that's, that's just, that's, you know. And what do
Dr. Grant Garcia: you think this guy with, with an open discectomy, what do you think would have happened for him?
Dr. Andre Shaffer: Again, it's different, hard to tell
Dr. Grant Garcia: per patient. Yeah,
Dr. Andre Shaffer: no, he probably [00:14:00] wouldn't have gone to work for three weeks or so.
Dr. Andre Shaffer: Yeah. Just because, you know, you have all, you have, you have so much more soft tissue dissection with an open discectomy, right? And even a tubular discectomy, you're taking bone, there's, there's more that you're doing. you know, getting there just to just so that you can see the just that you can see the tissues.
Dr. Andre Shaffer: Um, you know, there's a lot more that you do. And so this and this is one of the this is kind of one of the cool things is that you can make these really small incisions and they're powerful because you can see so much more because of the the magnification of the scope. Um, and one of the other, you know, large benefits of this is that When you, um, when you do this, because you're, because sort of the, the, the, the approach is so small, you have more muscle that's working and working.
Dr. Andre Shaffer: right away. And, you know, the people who love that as patients for sure, but you know, who else loves it as physical therapists, [00:15:00] right? At the end of the day, they're the ones that are spending, you know, hours and hours and hours with these patients afterwards, trying to get them back, you know, into the game, trying to get them back to where they're going.
Dr. Andre Shaffer: So this is one of my favorite slides, right? Orthopedic surgeons, we love what we do. We're pretty happy, but you know, it's, it's ultimately the physical therapist that kind of, you know, Kind of flushes that, you know, dunce the ball, right? We, we pass it off to the, to the, to the PTs and we do, we do a great job, but what we do essentially is we fix anatomy and then the physical therapists will sort of help rehab these patients.
Dr. Andre Shaffer: you know, across the finish line. And so that's, that's, I think that's one of my big reasons for, you know, spine endoscopy and minimally invasive spine surgery in, in all is just, you know, taking these, taking sort of what spine used to be, which was this open morbid, you know, difficult recovery. And, you know, hearing these amazing patient stories where they're like, I have no pain.
Dr. Andre Shaffer: I didn't take any medications. I feel great. I [00:16:00] mean, I think that's that to me is like one of the most, um, satisfying things about it. And that's why I'm so passionate about it. Right? I get to, I get to, I get to, I get to scope the spine. It's great.
Will Sanchez: Dr Schaefer. Um, I just wanted to kind of follow up there with, uh, from the patient's point of view when you say, and I've had friends have surgery and we'll kind of maybe we'll get into that in a second here.
Will Sanchez: I'm going in for back surgery. And you go, Oh, shit, you know, it was there for the young ins, but it is, you know, that that stigma of Oh my, you're going in for back surgery. What does that entail? How debilitating it is. I had a friend and this was probably about 12, 13 years ago, went in for major back surgery from the back and then cervical in the front, about eight years.
Will Sanchez: eight hours, took him. He didn't feel right for almost a year and to the point where he was like, I wish I didn't [00:17:00] have surgery. In about a year time, he started to feel better. It was like, okay, I'm, I'm finally better. I can walk. He's a, he's a chef. So standing up long hours, everything like that. But you know, that stigma about back surgery, you know, now with this new technology, instead of maybe being fearful, maybe we get excited because.
Will Sanchez: There's hope and relief for people that are suffering through this type of debilitating pain. And if you, if anyone's had back issues, you can't walk, you can't sleep, you can't move. It is
Dr. Andre Shaffer: by far the worst. Yeah, you know, these patients with, with, with radiculopathy, you know, you have a disc herniation and you essentially get in through a minute, you know, eight millimeter incision, you find it, you localize it, you find it and you start pulling that disc out and then.
Dr. Andre Shaffer: You close, you know, it takes two sutures to close. You, you know, glue the skin close [00:18:00] and put a little Band Aid on the Band Aid.
Dr. Grant Garcia: I saw his patient, they literally this tiniest little.
Dr. Andre Shaffer: And they go home and they're showering and they're, they're out of pain, you know, like you go see him in the recovery room after surgery and they're moving their foot and they're just looking at it.
Dr. Andre Shaffer: Like. This is amazing work. It works, you know, the pain's gone. And that's, I mean, it's just, and then, you know, well,
Dr. Grant Garcia: you can, you can see the Dr. Schaefer is pretty low key, low enthusiasm for this procedure.
Will Sanchez: Yeah, no, it's important. And obviously he, you know, he made a mention at the beginning of the show that he was inspired from what he saw, you know, that kind of, you know, it's, it's Always wonderful when our paths go down a certain certain route that especially if we're not expected, but, uh, to to give people an option to be pain free.
Will Sanchez: You're giving quality of life, right? That's I mean, I've had piriformis flare up and I'm like, I can't [00:19:00] move. I'm picking up my leg to swing it over the bed, you know, different issues at different times that that that's happened. And I can't imagine anything worse than that. Yeah. Um, maybe I'll stick with that right there.
Will Sanchez: Why is something like piriformis, um, happened so frequently? Is that something that's just body or, you know, over time or stress from playing ball or, or anything like that? Is there anything that you can pinpoint or is it just, just a matter of time as, uh, you get older, maybe a little arthritis, just wear and tear, what, what's, what's a normal cause because I know so many people suffer through piriformis or something similar like that.
Dr. Andre Shaffer: You know what I think it is? So, your nerves don't like being touched. Nerves, in the human body, is something that, you know, Grant knows, if you, to find a nerve, you find fat. And that's because the body puts fat around nerves so that nerves don't get touched. And so, [00:20:00] if you are touching a nerve, it's going to irritate it.
Dr. Andre Shaffer: If you're touching a nerve in two places, it's going to irritate it even more. It's called double crush syndrome, okay? And so, you may have some tightness, you may have some spasm in your piriformis muscle, but I think what happens is as your, as our backs start to, Degenerate a little bit, right? A little bit of degeneration.
Dr. Andre Shaffer: That's that's that second hit, right? That's that that's the second place that that nerves being touched. And so, you know, if you if you have a little bit of degeneration in 1 place and a little bit of, you know, in the other place. It's, it's not like they're adding, they're multiplying, right? Cause nerves, nerves just, they don't take a joke.
Dr. Andre Shaffer: They don't like being touched at all. And so, um, that's, I think part of what it is, right? You know, you, you, you push a nerve around a little bit too much. It'll let you know. And that, that's why, that's why it's so debilitating. That's why it's so painful for folks.
Dr. Grant Garcia: So I want to go, I love the piriformis syndrome, but I want to go back to endoscopy.
Dr. Grant Garcia: I love talking about it. So the, uh, so [00:21:00] what makes this so difficult outpatient? Like, why are we not seeing this more frequently? You know, again. Yeah. Dr. Schaeffer Proliance first one, like this is not easy. And I think there was a number of things that collided here. Um, but maybe you could tell a little bit of a story.
Dr. Grant Garcia: 'cause I think that's important for the listeners to hear too. You know, doing your surgery at hospitals sounds all great. The problem you have is you can hit with a massive bill. I know I've had spine surgery to hospital. I can show you how big the bill is. Hmm. And I've seen, I know surgeries at the surgery center and how much they cost too.
Dr. Grant Garcia: So there's differences just in that component. And then the other thing is finding a provider that even can do it. I mean, we see it all the time. I see it all the time. I didn't even know this was an option. No one told me about this. And Will and I talked about this. How do you find innovative people? And so what, what is the journey that you did briefly to get to this level?
Dr. Grant Garcia: You know, you're doing now things outpatient arthro, uh, anoscopy, and still no one's figured out how to do it yet.
Dr. Andre Shaffer: Yeah. So, so when I was. You know, like I said, this is the [00:22:00] reason I went back to do a spine fellowship, right? I was practicing, I was happy doing, you know, drama and, and, and, and hip stuff. Um, but saw this technology and said, Hey, I gotta, I gotta get on with this.
Dr. Andre Shaffer: I gotta, this is something I gotta do. Um, and so right from the start, when I was in my fellowship, I was, you know, talking to companies about, Hey, like, How do we get, you know, how can I do this, you know, after I finished this fellowship and, you know, they all, they all want you to buy a very expensive tower and they want you to buy very expensive equipment and, you know, the outlays.
Dr. Andre Shaffer: 250, 000 at least, right? Just just to get it. Um, and so, you know, that was kind of a thought like, all right, we'll build a practice and, you know, slowly but surely we'll get the equipment. Um, but one of the cool things about our our surgery centers, we have essentially, you know, half of the equipment that you would have to buy already [00:23:00] because it's used for arthroscopy, right?
Dr. Andre Shaffer: And so if you're, you know, if you're part of a big hospital, the big hospital, you know, if they don't have, um, you know, a certain tower, like an Arthrex tower, if they have a different company tower, they're not gonna, um, they're not going to buy a tower just for you to do spine endoscopy or very few will.
Dr. Andre Shaffer: Um, and so it can be difficult just to get the equipment, just to get the basic equipment in. Um, and so, you know, I kind of got on in on the ground floor with, uh, with a company Arthrex that's, you know, really trying to revolutionize spine endoscopy. Um, they're doing a lot of development work and they're, you know, taking off.
Dr. Andre Shaffer: And so I got in. Really early with them and, you know, got to go to one of their first labs. And I've been, you know, going to a lot of lab, you know, a lot of lab time. Like I said, probably 40, 50 levels at this point, um, and, you know, helping develop, you know, helping, helping develop, you know, tooling and evaluating things and things like that.
Dr. Andre Shaffer: Um, [00:24:00] so that, you know, we know what we can use, we know what's safe, so we know what's efficacious. Um, so there's that. So that, so I think the cost is one is one aspect of it. I think, you know, a lot of the spine surgeons who are out there, I think are Our good surgeons and are very capable surgeons. But this is essentially arthroscopy.
Dr. Andre Shaffer: This is a different skillset. It's a different way of looking at something when you try to do, you know, an open ACL, which I know no one does that anymore. Right. Especially not, not, I'm gonna, I'm gonna, I'm gonna shake
Dr. Grant Garcia: on the camera a little bit. She
Dr. Andre Shaffer: not in Grant Garcia's neighborhood. Right. But you know, if you, when you go from open to trying to do it through.
Dr. Andre Shaffer: You know, a small incision with, you know, that's, that's, that's, and you're in an instruments that are 15 centimeters away from where. the pathology is that's that's difficult. That's a different set of hand skills. And so, you know, I had the benefit, I had the benefit of doing, you know, [00:25:00] 150 hip scopes in fellowship and doing, you know, knee scopes and, and, and, and, and percutaneous access, uh, for some of these, you know, for some of the nails and other, you know, intramedullary things that I did as part of trauma.
Dr. Andre Shaffer: And so I just had, I had the benefit. It's not like I'm, The greatest thing since sliced bread. It's just, I had the benefit of being able to have some of these skills already from different equipment. Right. So if you have those skills and you're saying, Hey, I want to do something smaller, well, there it is right there for you.
Dr. Andre Shaffer: Right. And if you have those skills, then it's not going to be, you know, for our ordeal to take a disc out. Right. It's going to be, and I
Dr. Grant Garcia: think that's also a big thing, right? I mean, we've had, you had a lot of pushback before you came, not just, not for me, but in general from. Everybody because you know, before the Arthrex system came out, it was a very expensive.
Dr. Grant Garcia: The cost will probably heard that cost. That's pretty high, even for a medical facilities. And so you [00:26:00] basically have complete barrier. We talked about this before. Well, right. This is a perfect example of tech and blocking, right? No one pays for that equipment except for the surgeons. And then it. Gets reimbursed over time and pays itself back.
Dr. Grant Garcia: But going in the black that much is usually not a really good benefit. And it's hard to get everybody on board when, you know, open disks do fine, but they're not great. And so as a result, it's hard to really convert. And that's why that's one of the reasons. And the other thing is the skill set and the other thing is like taking a long time.
Dr. Grant Garcia: Like if Dr. Schaefer starts doing these and instead of it taking one hour, it's taking four hours and patients are doing worse. That's another problem too. So we'll, we've talked about this. Like the surgeries that I do for some of my crazy surgeries are more memes. We're still efficient. And if we're not, that's when problems happen.
Dr. Grant Garcia: So when people dabble, and I always tell people, if you're seeing somebody, you don't want to dabble her, right? It's okay if people are a little slower. There's not about different timing and, you know, being 10 minutes faster. Like you don't want to time yourself in the OR and things like that. That's not appropriate.
Dr. Grant Garcia: But if you are proficient, you should be efficient in the operating room. And efficient in the operating room is actually [00:27:00] important. And some of the best surgeons are the most efficient. It doesn't mean they're the fastest because there's not the fastest. I'm saying it's efficiency. I told Will before, it's like a You know, like you're in an orchestra, right?
Dr. Grant Garcia: You're doing it. But the fact that, you know, Dr. Schaeffer's first endoscopy was what, like an hour and 15 minutes. And it was a really tough case and your second one was like an hour or something like that. I mean, we're talking about, this is not much added time and all those benefits we see there. And honestly, The drawbacks are really, you know, that's again, just, those are standard risks.
Dr. Grant Garcia: Uh, and I think we've talked about all the different things, but I don't think most of those will eventually kind of go away. Right. I mean, most of those things are minimal.
Dr. Andre Shaffer: I think, I think it's, you know, I think a lot of it is, you know, like the operative time, it depends just, again, it depends on the pathology, it depends on the patient.
Dr. Andre Shaffer: Um, and you're, and honestly, I think a lot of it is your surgeon's comfort level, right. With the equipment and with the technique. Um, um, So, you know, yeah, my first, my first one took, what, I think it was an hour and 45, I don't think it was an hour and [00:28:00] 15, I think it was an hour and 45 minutes, but it was a really difficult case, you know, and then my next one was an hour.
Dr. Andre Shaffer: It was just under an hour, you know? And so it's, it's, it's. You know, there is, there is a learning curve there, but it's, I think it's a pretty steep one. I think it's pretty rapid in terms of the progress that, um, that you can make, especially if you have some, you know, other skills that are applicable to what you're doing.
Dr. Grant Garcia: Well, I think also Will sees now, we talked about this many times, Will, with all the other surgeons we've had on. Practice, practice, practice, practice a little more, think about it, get better. And so that's, for the viewers, that's the most important thing in your surgeon, in my opinion. And Will probably, I don't know if Will agrees with this, but like, you know, the mentality of like, you know, getting better each time, right?
Dr. Grant Garcia: What did I do? What do I need to make notes on? What I need better? Like, until you got it. And then once you got it, don't get complacent. Right. Six months later,
Dr. Andre Shaffer: keep
Dr. Grant Garcia: going, keep getting better. It's better for the
Will Sanchez: patient, right? You know, access that certain doctors have compared to [00:29:00] others, right. You know, whether if they're working at a hospital, what equipment is available to them.
Will Sanchez: Um, so I, there, there's a lot of levels, uh, to all of this, just from the prior discussions that we've had, uh, with folks, you know, where, you know, maybe not privy to some of this stuff, right? And you know, and that's why we always tell the patient, you know, please go get a second opinion, right? And obviously with insurance, that can make things pretty complicated.
Will Sanchez: You know, and so we start to go down a slippery slope here with a lot of the discussions, right? So, you know, whether it's, do you have the option to have a fusion or a dis replacement? Maybe you don't have it, you know, why would insurance then say, well, you're better off to have a dis replacement, but we're going to approve the fusion where I'm not sure what the percentages are, but you may have to reoperate on those.
Will Sanchez: So it's a, it's a, I guess a gray area and you guys would know better than I would. But just from [00:30:00] listening to these, the conversations, there's a, there's a back and forth dance that kind of happens between patient, the doctor and insurance. Uh, so that's always an interesting, uh, dilemma.
Dr. Grant Garcia: Well, well, you, you, you, you had to go there now it's time to talk about disc replacements.
Dr. Grant Garcia: Sorry. It's okay. No, no. I love it. So this is important. So I want to talk shape around here because this is stuff is this stuff is really new as well. And so I want him to talk about, you know, I think let's start with the one that's more common, which is the cervical disc replacement, kind of tell about the differences in that and really why it's better for younger patients and what's the benefit.
Dr. Grant Garcia: And then let's talk about lumbar because lumbar to me is valuable, but I also have a personal interest in this. So, you know, this, this to me at first, obviously cervical. So, you know, tell us what's the cervical disc replacement and we'll maybe throw up a slide there so people can see. Um, and then, yeah, there you go.
Dr. Andre Shaffer: So one of the, one of the ways that you can help patients. So generally [00:31:00] when you're doing. Surgery in someone's neck. It's for nerve compression. Okay. And it's for nerve compression from a disc that's herniated, that's squeezed out the back and pushing on the nerves, right? Like we said earlier, nerves don't like being touched.
Dr. Andre Shaffer: by anything, including pieces of your own body. So one of the, one of the most powerful ways of getting that compression off is by taking that disc out from the front generally, which believe it or not is easier for patients and is less invasive than going from the back. Um, But going through the front, finding the disc and pulling it off, decompressing the nerves.
Dr. Andre Shaffer: And once you've done that, you have a space that's open. Um, and that can be, uh, that's a lumbar disc replacement there. Um,
Dr. Grant Garcia: we'll go back to the
Dr. Andre Shaffer: cervical one. But yeah, once you, once you, uh, once, once you get that space open, you can do, you have to put a spacer in there to sort of hold the bones apart and keep, you know, keep all of the anatomy in the right, Place that [00:32:00] it's supposed to be in.
Dr. Andre Shaffer: You can do that one or two ways. You can do that with a fusion and with, uh, uh, a static spacer that doesn't move, or you can do that with one of these, you know, uh, disc arthroplasties that you see here. And what those do is those have in plates and a little core that allows the end plates to move and flex and bend.
Dr. Grant Garcia: So more natural, right?
Dr. Andre Shaffer: Much more natural. You don't lose as much, you don't lose as much motion. Um, and what we're, what we're finding is, you know, there's a risk of something called adjacent segment degeneration, right?
Dr. Grant Garcia: Well, this is what you were talking about.
Dr. Andre Shaffer: Where, where when you have one segment that's fused, all of the, the patients still move, right?
Dr. Andre Shaffer: Just because you fuse one level doesn't mean your neck is going to be rigid. You're going to move. You're just going to put more stress on the other discs. Uh, while you're doing that, if you're young, that means you have a longer lifetime of more stress being put on the desks. Also, you think about your 30 year old patient, your 35 year old patient, [00:33:00] they're doing more intense things, right?
Dr. Andre Shaffer: They're doing CrossFit, they're running marathons, they're doing things. They're really using their neck as opposed or their spine, as opposed to maybe a, you know, It's a, it's 65 year old, you know, uh, do a workout of the days. Right. Um, and so, you know, younger patients put a lot more stress on their neck and if they have a level that moves, that's a lot better for them.
Dr. Andre Shaffer: Um, ultimately, because the lower, because there's a lower risk of adjacent segment degeneration. But there's also better outcomes. You know, patient reported outcomes are far superior with a disc arthroplasty. Um, you know, my brother had a disc herniation and I made sure he got a disc arthroplasty as opposed to a fusion because he's younger than me.
Dr. Andre Shaffer: You know, he's in his thirties. And so it's, it's really important to, it's really, really important to. Um, I think to preserve motion in the spine as [00:34:00] much as you can. And so I'm, I'm, you know, maybe a hair less passionate about, uh, cervical disc arthroplasty and lumbar disc arthroplasty than I am about. Um, about, you know, endoscopy, right?
Dr. Andre Shaffer: I like endoscopy, but I love, I love, I love disc arthroplasty as well. There are some, there are some times when you shouldn't use a disc arthroplasty. And a lot of that is based on, you know, how much arthritis you have in your facet joints. And those are the joints in the back of your spine, behind your spinal cord.
Dr. Andre Shaffer: And so some people disc arthroplasty still aren't, uh, or aren't, aren't a good option in. Um, but
Will Sanchez: arthritis affect that just so we can have a better understanding. If you have arthritis buildup back there, why wouldn't you want to do something like that?
Dr. Andre Shaffer: So if you have arthritis in your neck and the facet joints in the back, they still move when you have a disc arthroplasty.
Dr. Andre Shaffer: So you can still have residual pain in the back of your [00:35:00] neck. It may be something that's, It may be something that you can tolerate. So that's why it's always a conversation with your, with your physician. I always talk about what the goals are, but it may be something that you need that, that, that, that if your, if neck pain is a big part of what's going on, as opposed to arm pain.
Dr. Andre Shaffer: Then sometimes, sometimes you, you say, yeah, well, maybe we should do a fusion, but you know, foreign, you know, generally most patients, especially younger patients do a lot better with disc arthroplasty as opposed to fusions.
Will Sanchez: So, I'm sorry, your evaluation, then it goes across multiple levels, right? Um, the age, what's happening to them physically, what needs to be done, maybe if they have an arthritis.
Will Sanchez: So, you're, you're taking all of this. You know, wealth of information. And then coming up with what's the best course, uh, to treat this particular ex patient, uh, moving forward for what's happening now and, you know, maybe how it [00:36:00] affects them in the future.
Dr. Andre Shaffer: What do you, you know, occupation, uh, are you, are you hyper mobile?
Dr. Andre Shaffer: Are you, you know, what do you do things where you need overhead? We need to be able to do things overhead. Absolutely. Picking up three kids at
Will Sanchez: home,
Dr. Andre Shaffer: right? Exactly. You know, we'll, we'll put different, we'll put different, we will put different disc types into different patients based on, you know, how their, how their body is, right?
Dr. Andre Shaffer: Some, some discs move less. They're more constrained. Uh, other discs are less constrained. And if you have a patient who's hypermobile, you're going to put a more constrained disc in generally.
Dr. Grant Garcia: Well, that's interesting to hear. You'll first off to comment, Will, you heard about the dreaded back surgery, right?
Dr. Grant Garcia: Well, one of the other things people worry about is with back surgery, you get recurrence. Like a lot of these back surgeons patients are for life, right? You know, every five years you come back and get your next level fused. So the idea behind, I think this is not only is it, It's a one time surgery or, you know, last a lot longer [00:37:00] and you're having less issues above and beyond.
Dr. Grant Garcia: So the goal is, I think, long term, right? Would you say this, Andre, that you had to have the patients are not coming back all the time, right? It's all the goal is to reduce the number of long term surgeries for these patients because a lifer of spine is never a good outcome. for at least for what I've seen and will seen.
Dr. Andre Shaffer: So there, there's a number of reasons. I think that, you know, disc arthroplasty is, is the future of spine surgery, right? One, you get better patient outcomes to fewer, you know, neat, fewer, you know, less need for operations. You know, they're supposed to be, I was just seeing something the other day that says there's supposed to be a 1, 500, 1, 200, uh, spine surgeon shortage in the next like 10, 15 years.
Dr. Andre Shaffer: And, you know, if I've got patients who keep coming back, cause they need That's so many patients that, you know, don't get care, right? And if you and the longer you delay spine care, you know, it tends, it tends to constrain your options to things like fusions, right? Um, you need patients who've [00:38:00] ignored their neck, ignored their back for 20 years and it's harder, right?
Dr. Andre Shaffer: So I always tell people, Hey, you know, make sure you're doing your physical therapy exercises. And I say, Hey, but if you're having issues, don't ignore them. Come back. You know, the sooner you come, the sooner you come to see me, the sooner that I can do something small. As opposed to having to do something big, you know, and if I can do something small and get you kind of back on the way, that's so much better than if I have to do, you know, big multilevel fusion.
Dr. Andre Shaffer: I'll do them if I have to. I'll do them through MIS techniques so that we get people back up and moving quickly, you know, more quickly. My preference is to do something small that, you know, preserves motion and, you know, You know, has people, you know, extremely happy right away. And that, that's it. That's that's cause that's, that's what I, that's what I ultimately want to do.
Dr. Grant Garcia: And I think for this is important. Will, we have said it before. This is why second opinions are so valuable. You know, even today I saw six second opinions and three of them had heard opinions that were completely different than what I told them. Right. And you're getting an opinion saying you need to have a fusion of your neck and [00:39:00] you're below 60 years old or 65 years old.
Dr. Grant Garcia: And you're like, it's only been bothering me for a little while. You know, that's someone you should maybe think about it because sometimes if there's not a lot of arthritis, the fusion sometimes is the easier option, right? It's easier to get approved by insurance. It's cheaper for the surgery, but it's not the right answer.
Dr. Grant Garcia: It sure as heck is not the right answer. So you got to make sure. If you're a patient you really go to the people if the person does I tell someone If they tell you cervical arthroplasty or they tell you something doesn't work They better be the one that also does those surgeries. Cause when someone says it doesn't work, and there were people I've seen that have said my, some of my surgeries don't work cause they don't, they don't, they never seen him before.
Dr. Grant Garcia: I'm like, that's not very helpful. Like you want someone with experience that has all options. And so that's why it's great to have someone like you on here to talk to the patients, to hear about this, especially the younger patients who want to get back to sports. They want to get back to things. So you don't want your neck fused.
Dr. Andre Shaffer: So one of the things that's interesting, uh, Grant is that, you know, disc arthroplasty is actually cheaper. [00:40:00] dis arthroplasty is actually cheaper than when you start, when you start adding up all of the, all of the fusion, the fusions, right? Than fusions. Yeah. Fusions. There's, there's, you know, I hate to say it, there's a, there's a, there can be a financial motive, you know, that that exists for, you know, people saying fusion
Will Sanchez: is, is the fusion something that, um, I'm not trying to throw insurances out there.
Will Sanchez: the bus. But, um, is this something that they kind of defer to? It's kind of like, uh, you go to the doctors and they say, well, we're going to take an x ray first. And you go, I don't have a broken bone. Like, I know I need an MRI. Well, we got to go through the x ray first. Is that just part of the, the process when it comes to something, uh, like this in your field, when it says, well, we're going to explore this route first before we go to the next?
Dr. Andre Shaffer: I think the reason that, uh, insurance companies, uh, like to steer patients away from arthroplasty is because, um, arthroplasty [00:41:00] doesn't have the same volumes. And so there aren't the same discounts on, uh, on implants. Now that said, the amount of implant that you put in is generally greater, right? So if I do it, if I do a disc arthroplasty, that's the one implant that I put in, right?
Dr. Andre Shaffer: So that's the one implant that your insurance company pays for. But if I do a fusion, I'm putting a static spacer in, I'm putting a biologic in, I'm putting his plate and screws in, right? There's a lot more that goes into it. Um, and again, sometimes a fusion is the right thing. It's not, you know, again, I don't want to come off as dogmatic and say it has to be an arthroplasty because I tell page, I tell plenty, plenty of patients.
Dr. Andre Shaffer: Um, and I do plenty of fusions, you know, um, if I can avoid it, I like to, right. If, if, if it's safe to do it, if it, if it looks like it's going to work for the patient, Then I'm then for me, I'm looking to do a fusion or I'm sorry, I'm looking to do an arthroplasty as [00:42:00] my default and I have to have a reason to not do the arthroplasty first option.
Dr. Grant Garcia: That's that's 100%.
Dr. Andre Shaffer: Yeah,
Dr. Grant Garcia: that's that's a listen. Everybody hear that. We're going to repeat that on the next thing. That is the number one thing you need to hear your surgeon. What is your default? Yeah. Okay. You're a spine restoration surgeon basically at this standpoint. And when people, it's the same thing with mine, you come into my office, the default is to save your knee.
Dr. Grant Garcia: The secondary third tertiary or fourth option is to do a knee replacement. Right. Right. Or do a shoulder replacement. Right. So this is what I'm talking about. This is really important. I think Will would appreciate this. The best outcome for the patient is to save as much as possible of the person's body.
Dr. Grant Garcia: That's not the default. If that's not the default, then you should be concerned. Okay. Now again, you say the default is that, but that doesn't mean you can't jump. Um, I don't want to get too sidetracked. I want to jump to the lumbar spine because that's that, even though these seem like they're the same, [00:43:00] they're not.
Dr. Grant Garcia: And for insurance authorizations and getting approved, and we've heard about the tech, the roadblocks, the lumbar spine, would you agree has more roadblocks and the cervical spine?
Dr. Andre Shaffer: Absolutely. You know, I think insurance companies are more, uh, Um, more reticent to approve lumbar disc arthroplasties than they are, you know, lumbar fusions.
Dr. Andre Shaffer: And I think, I think it's probably one of the more, um, I think it's probably one of the more, uh, unfortunate things that are, that's kind of happening right now. Um, this is actually a newer, this is a, this is an investigational device, uh, that's having some pretty good, uh, you know, kind of reports initially.
Dr. Andre Shaffer: Um, it's doing, they're, they're going through their ID. They're already enrolled. Um, but this is, this is a most, most lumbar disc arthroplasty is you have to put in from the front. So you have to have an incision on the front of your abdomen. You have to have a vascular surgeon, you know, move some of the structures so that you, so we can get access to that, to the, to the spine.
Dr. Andre Shaffer: [00:44:00] And then we have to take the disc out and put the, put the arthroplasty in that way. But this is actually something that you can put in from the back. And what's really cool about it is you can put it in through minimally invasive Uh, incisions and with a minimally invasive approaches so that you're not, uh, devitalizing a lot of the muscles alongside the spinous processes.
Dr. Andre Shaffer: And I think that's one of the reasons, uh, to get back to that. You know, we'll talk about adjacent segment degeneration and people taking such a long time to bounce back from spine surgery. I think it's because of. the traditional approaches where it's a big incision and you essentially, you know, make a midline approach and you just reflect or move a bunch of muscle off of the bone.
Dr. Andre Shaffer: Well, when you do that, that muscle doesn't work the same way. And if you ever have to come back and look at that muscle, it's scar afterwards versus if you can do it through a minimally invasive approach where you're going through a small incision and you're spreading muscles opposed to. stripping muscle that ends up with patients who, you know, have dramatically less pain.
Dr. Andre Shaffer: That's why that's, I [00:45:00] think one of the reasons why endoscopy is so powerful is because you're spreading muscle, you're not stripping muscle. The other reason is the fluid, you know, whenever you're washing away all that, all that inflammatory, uh, sort of the inflammatory chemicals that happen as a result of surgery, you just have less inflammation postoperatively.
Dr. Andre Shaffer: To get back to discard to plasticity, um, that modus is going to, I think, going to be a really, I think that's going to be a game changer when it, when it comes out and get approved.
Dr. Grant Garcia: And again, we like new tech. So this is important for patients. This is a young person's surgery, right? You fuse their, you, you don't fuse their back.
Dr. Grant Garcia: You give them this replacement. And the nice thing is if you can do it to the front, the back, you don't have to stay over house, right? Usually those patients, that could potentially be someone that goes home
Dr. Andre Shaffer: and
Dr. Grant Garcia: potentially a surgery that's done at the surgery center for outpatient purposes. Is that correct?
Dr. Andre Shaffer: Versus
Dr. Grant Garcia: when you get it from the front. You're going to the hospital for that. Yeah. Um, and that's more challenging and you're already fighting with insurances and as soon as you get a hospital stay and insurance doesn't want to cover it and you have to pay out of pocket, you're looking at. you know, [00:46:00] 57 times cost to the patient, right?
Dr. Grant Garcia: Because it doesn't get doesn't go to anybody but the patient when it's not covered, which stinks. Um, so I think this is really important for patients. I think the one last part we're going to, we're going to get close.
Will Sanchez: Looks like we lost him, but we'll, we'll just kind of keep that going as, as he comes back.
Will Sanchez: Um, I saw today on a good morning America. Um, something that they had determined at the Mayo Clinic and let's bring Dr Garcia back. It's okay. I'll just finish my thought and then we'll get you back in there. Dr Garcia. Um, saw no good morning America today. They had done a paralysis stem cell study at the Mayo Clinic.
Will Sanchez: They had 10 patients, 7 of them had really great results. 3 didn't have bad results, but pretty much stayed as is. So my question to you is, the, the role that something like stem cells, uh, will play a part in, In surgery, back surgery [00:47:00] going forward, uh, especially with something like this that, you know, they were talking about this, uh, just today on, uh, good Morning America.
Dr. Andre Shaffer: Yeah, I think I, I, I'm, I'm a big believer in stem cells. Um, but I'm, but I, I'm measured about their use in the back, especially right now. Um, you. You have to know why something works in order to use it appropriately and have patients get good benefit from it. I think, you know, are there patients that get benefit from stem cell injections into their back?
Dr. Andre Shaffer: Well, it depends on what the cells are. Right. Are they, you know, it depends on who the patients are, right? Are these young patients or these old patients? How bad is their back
Will Sanchez: paralysis? I mean, that was the study. So it really bad, right? I mean, they're, they're pretty much dire the lowest.
Dr. Andre Shaffer: That's probably their nerves, right?
Dr. Andre Shaffer: I think a lot of, a lot of patients. Come and ask me about, you know, disc herniations and well, can I just put [00:48:00] stem cells into it? Okay. That's yeah. You can put stem cells into it, but if your disc is already degenerated to the point that it's not, you know, that the, that the mechanical environment isn't going to let the stem cells make.
Dr. Andre Shaffer: uh, cartilage or make, you know, um, make type, you know, type one and type two collagen, then it probably isn't necessarily going to work. And so you got to be, I think you got to be careful. I think in 20 years, we're going to be a lot closer to, to that kind of Holy grail of, you know, saying, Hey, you have a problem with the disc and we're going to do an injection of stem cells and
Will Sanchez: fat out of you and put it in your lumbar.
Dr. Grant Garcia: Right. Yeah. I'm telling you, Dr. Schaefer is coming back on in a year or two. We're going to hear about the, The modus spine happening all the time. We're going to hear about him scoping everything in the back, front, who knows. And then we're going to hear about, we get to hear about biologics and spine.
Will Sanchez: Yeah. I wanted to bring it, bring it up because I'm pretty sure that people will, you know, approach you about that without having the information, the knowledge. So I think it's important to at least discuss [00:49:00] it. So it's great. for talking. And,
Dr. Grant Garcia: and obviously interested time, but I do got to ask this question.
Dr. Grant Garcia: Do you ever do. Oh, is there ever a reason to ever consider doing PRP in the back? Like I know people get it done as a guy that has a lot of PRP in the knee and occasionally the shoulder. I get a lot of patients asking about it for the lumbar spine or for the cervical spine. Is there any data that's out there or what's the, what's the top?
Dr. Andre Shaffer: I think it's, I think it's actually, so there's data that says it's as effective as a, um, as an epidural steroid injection. Um, yeah. So would you consider
Dr. Grant Garcia: doing that? Like, let's say someone failed, like, you know, you have one epidural, two epidurals and they're just okay. Would you ever say someone's like, dude, I don't want my disc done.
Dr. Grant Garcia: Would you say, Hey, listen, they're like, I want to do a PRP. Yeah. Would you consider that? Is that something that time we would kind of think about it?
Dr. Andre Shaffer: Absolutely. Yeah. I think if you've, I think if you've done, if you've, and so, so the, the interesting thing about the disc injections is that, or a spine injections is that epidurals are helpful.[00:50:00]
Dr. Andre Shaffer: Diagnostically for us as well as therapeutically for patients. And so, you know, I want to see that you're getting some improvement from the epidural injection, at least temporary right now, if it doesn't work, I can always do another one. And if that works, but doesn't really get it done, you know, if you don't have anything that's compressing.
Dr. Andre Shaffer: On nerves, then I'm, I'm inclined to say, Hey, yeah, let's do some PRP at that point. Right. And that, that's, I think the stem cells, right. That, that I think are that, that we kind of have a good sense of, okay, it may work for us. Right. As opposed to some of the, you know, Taking fat out of somebody's, you know, thigh and say, you got a little lipo and you got a little disc injection, you know?
Dr. Andre Shaffer: Um, I mean, look at,
Dr. Grant Garcia: look at Dr. Schaefer. He's a plastic surgeon and spine surgeon, all mixed in one.
Dr. Andre Shaffer: I wish, I wish. No, but yeah, I think, I think, you know, it's, it's, uh, I think PRP is something that's a little bit different, right? There's a lot of data [00:51:00] behind PRP that shows that it's effective and shows that it's safe.
Dr. Andre Shaffer: Um, and now there's data that's shown that it's essentially got, you know, similar efficacy to, uh, to the, you know, to epidural steroid injections. And so, you know, I'd consider it for a disc that's, that's, that's really bad, but not that bad, right? I might consider it for a desiccated disc as opposed to a completely degenerated disc.
Dr. Andre Shaffer: Awesome.
Will Sanchez: All right. Well, we wrap it up. I just, I just wanted to just show this here and I didn't show it to Dr. Schaefer. And if, if you're listening on, um, on a podcast, check us out on our YouTube page so you can see the slides and see our beautiful faces. So please check us out. Um, we always talk about patient relationships and how important it is.
Will Sanchez: And I just wanted to share. a few things from the patients. Uh, just recently from the last month or so. If you go to patient reviews, um, please check it out. I'm just going to highlight a couple of things. [00:52:00] He fielded all my issues fully in a manner that made sense to me, even if he probably felt like he was drawing a crayon, just making it really, uh, uh, visually and, uh, just breaking it down so they can understand, you know, Dr.
Will Sanchez: Schaefer exceeds far beyond standard care. It's another review. I appreciate that he starts with the least invasive treatments and continues from there, depending on results. And by the way, I had this all set up before we even talked about it. So that is a great, uh, way to just showcase what we've done.
Will Sanchez: When you have this feedback from patients, when they walk out of your office and they're happy with not only the treatment, but the doctor patient relationship leading up to the treatment and post, what, what does that, what does that mean for you as, as someone that does this, you know, in their profession, but you know, that helps so many.
Dr. Andre Shaffer: Yeah, you know, I mean, it's doing doing what we [00:53:00] do is a gift. It's an honor, right? It's a privilege to be able to help people in the way that we that we do, right? You think about, you know, how, how privileged you are to be able to help somebody get back to their life. And so, you know, that's, that's what I want, right?
Dr. Andre Shaffer: I want people to, you know, I want people to understand what their options are. I want people to feel comfortable with the options. I want people to feel comfortable with which options they're choosing. And then I want them to feel like, you know, the experience is as, as least traumatic as it can. Right.
Dr. Andre Shaffer: Cause if you think about how scary it is to go to a doctor's office and how scary it is to have them talk about, you know, procedures and surgery and things like that, that's That's not really an enjoyable, you know, that's just, it's just not enjoyable. Right. And so I don't, I don't really want to be somebody who's just sort of, you know, slogging through patients and then you take it or leave it.
Dr. Andre Shaffer: That's just not really, that's, that's not my personality. Um, and so I want people to, I want people to feel like they're, you know, [00:54:00] like they play a meaningful role in their care because they do play a meaningful role in their care. Right? If they're, I think if people are happy that they're going to, they're going to do better if they feel like they got the best shot at, you know, getting what they wanted and, and it helps, they're going to do better.
Dr. Andre Shaffer: And that's, that's all that, that, that's what matters is people doing, you know, people having excellent outcomes, um, you know, through, you know, minimally invasive, you know, means and, you know, Helping them out.
Dr. Grant Garcia: So I think that's important for the listeners to hear. You've heard dr. Schaefer talk You've seen his innovative stuff, but also the personality is important And I find that when people come and they get extra opinions again another reason just get another opinion because sometimes you got a gel With the surgeon.
Dr. Grant Garcia: I mean like we've we've Dr. Schaffer can mention this, but if a patient doesn't feel comfortable with you, I don't want them doing surgery with me. Right? No, I want it to be. Everyone's got to be comfortable. As soon as I had a patient [00:55:00] today that was terrified of the other surgeon and she wants to go to him because she knows the person and I'm like, that's the silliest thing I've ever heard in my whole life.
Dr. Grant Garcia: I was like, you should feel comfortable. If you're afraid of the person that's operating on you or you're nervous about it or something, unless you absolutely have something that's the only person in the world, which is pretty much never the case. Get another opinion. See someone that you, that you like, that, you know, and that's why we do these videos.
Dr. Grant Garcia: You know, this podcast with someone like Dr. Schaffer so people can, can meet him and understand that, you know, we just talked for an hour. That was pretty easy. Uh, and we talked about some pretty intense stuff. And so you're in there, you're nervous, you're getting your first back surgery, just, just reach out.
Dr. Grant Garcia: So, you know, you've got, this is, this is a good option for patients. And then think, if you don't feel comfortable about the situation, there's something you think, there's something else you're missing. That gut feeling you have inside when you meet somebody and you're like, I think there's more to this. I think it can be done differently.
Dr. Grant Garcia: There's got to be another way. Just look it up on your own and find the right person for it, but I think it's really important I think we'll know this back surgery is terrifying especially big stuff [00:56:00] and sometimes it might not be necessary Or the key is just to get the right stuff, right? Well
Will Sanchez: 100 percent Doctor Schaffer.
Will Sanchez: Thank you so much for being our guest and just sharing your knowledge and just kind of hanging with us. We'd like to thank all of our listeners and viewers. Check us out at sports dot talk dot com and we're on sports dot com. Sports Talk podcast and on YouTube, Ben iHeart and Spotify. Dr. Garcia. Stop me, I'm gonna keep rambling.
Dr. Grant Garcia: Oh, you keep going. I'm listening. And check us out our website, ww@sports.talk.com. You can see everything. You'll see transcripts of the show. You'll see video podcasts, you'll see split video podcasts and on all the social media we posting. And you're gonna be seeing Dr. Schafer's beautiful face pop up a few times in the next month or so.
Dr. Grant Garcia: So check it out. I'm excited to show you guys off and show this stuff off. Patients need to know about this. This is not common surgery in the Washington state area. You need to hear this, consider it, think about it. This is, I can't tell you guys anymore. I've done my best. Okay. That's it. There's no [00:57:00] more I can do.
Will Sanchez: All right. Dr. Schaffer, go back to being dad. Now, out of, out of any roles that you have. Thank you so much for hanging with us. Take care.
Dr. Andre Shaffer: Thanks for having me. Take care guys. Audio Transcript
Tech and Innovation: Roadblocks to Success

Will Sanchez: [00:00:00] Dr. Garcia, welcome once again, and we want to thank everyone for listening to sports doc talk. Um, we're just ecstatic with everybody listening to the show and commenting. So we always love to hear from everyone. Uh, that Garcia, as you see, I'm excited. It is the start of the 2024 baseball season. You Mariners fans relax.
It's okay. I can be a Yankee fan. Don't be upset about everything in 80s and 90s. You should be upset about the Dodgers and everybody else at this point. Get over it. Anyway, this is not the way to start with the fan base. Dr. Garcia, I apologize. Welcome to the show. How are you? What's going on?
Dr. Grant Garcia: I'm good. It's been a little hiatus, but, uh, now we have some good shows coming up, so this'll be excellent. Yeah, things are good. We're busy. Ski season, as we talked about before, is very busy. So, uh, I'm good. There's no rest for me at this point.
Will Sanchez: Are you excited, excited about [00:01:00] baseball? Are you, you know, I know you're a huge football fan and you know, it's one of the things that, uh, we always get a chance to talk about, but what's your, uh, your fandom when it comes to, uh, baseball here?
Dr. Grant Garcia: I like baseball. I'm not like a, I'm not a massive fan in terms of like watch it every day. Um, but you know, be taking care of so many baseball players. I mean, things have really picked up. We have so many more baseball players coming in because you know, the weather's getting nicer. Uh, and so. That connection with my love of the hate to say to the fans, the Yankees, um, you know, it's exciting to get excited for, for everything.
Will Sanchez: Let's get into this, uh, this new tech in the roadblocks and challenges. We spoke a little bit before we started the show. So let's kind of catch, uh, folks up on, you know, some of these tech that you've been working on and that you're excited about, whether it's Misha and bear balloon and things like that. So let's kind of jump into it right away.
Dr. Grant Garcia: Yeah. So this episode. I think I thought was important because I wanted people to see [00:02:00] behind the scenes and I want people, you know, unfortunately, and we're not doing advertisement, but you know, we're promoting really cool products that help patients and that sounds really glamorous and glitzy. And unfortunately, not everything is free, and unfortunately, not everything can happen for everybody. And so I think that the understanding that what roadblocks there are to tech for the average patient, for certain patients with certain, you know, providers, uh, and the new roadblocks also for just providers to actually use it, and depends on where you work. So this is a pretty complicated topic. We're not going to go deep into it. Too crazy on this because I obviously don't want to overload the audience with, you know, minutiae and nerdy details about the technical aspect of getting this new product because it's already, that's, I know, I know, I know it is, but I don't want to overdo this one because, but this is sort of like the, it's a little bit more of the business side of things, which is interesting.
And as a surgeon who's private practice, You know, every cost I see. And so I understand the [00:03:00] numbers game about this and how it works. But also I'm someone who likes to offer the latest, the newest stuff because. I think it's going to help the patients, right? I at least offer what I think is going to help the patients and what is going to get them better And most of the time thankfully i've been correct in terms of it being an improvement Um, but the reason we're doing this is so to keep people more informed, right? We talk about all sports all orthopedics all the time. Well, how does that happen? Well that happens from innovation and how does innovation happen? Well, it doesn't happen for everybody It doesn't happen overnight and there's a there's a continual attack To get these things done and some things are easy and some things are not so, you know We'll we can we're not going to go through each product individually, but you know, you got the misha You have agility.
You have all these really nice new cartilage products coming out autocart. Um, The there's other ones for other different companies. There's the balloon we've talked about before there's prochondrics, which we've used before There's an extensive list of products. There's acl repair [00:04:00] Right. Two types balloon and preservation technique.
We've talked about, you know, how do these matter? What do these matter for getting them into the into the operating room? Can every patient get it? You know, not everybody is a qualified. I had an ACL repair that I was supposed to do last week and the patient was all set up to go and he was excited. I was excited and two days before the insurance said it's not indicated.
Will Sanchez: Oh my God.
Dr. Grant Garcia: And had to change the surgery and do a reconstruction. So it happens. It's not often actually, it was the first one I've had in a while, but the insurance carriers make a, add a big part. So we don't want to go, we'll, we'll, we'll do it piecemeal right now, but that's the, that's the gist of this topic.
And hopefully people get informed and honestly, it might even inform some doctors and surgeons because you know, if you're looking at adding something new and you kind of haven't thought about this, it's important. And again, it matters where you work as well. So we'll go into that.
Will Sanchez: Yeah. And utilizing the, you know, the technologies to promote, um, improve outcomes. Um, maybe the, the [00:05:00] speed of the surgery, the patient recovery, right? There's so many different aspects of it. And then you're adding the insurance part of it. And, you know, I'm, I'm not privy to that information, how it works, but, um, Is there a typical time frame when you're dealing with something like that and you're looking into someone's insurance that you can kind of get that information, you know, upfront instead of so close to a surgical date or it all depends depending on the insurance and you know, everything else.
I'm really feel like I'm going into the deep woods right now. Uh, you're going a
Dr. Grant Garcia: little deep.
Will Sanchez: For
Dr. Grant Garcia: the first time ever on this show, I'm going to try to go less deep. Okay. All right. Yeah,
Will Sanchez: I'm good. I caught myself.
Dr. Grant Garcia: So no, so it's totally normal. So most of the time these surgeries, you try to preauthorize them. So the patients are, you know, make sure that the insurance is going to get, is going to pay for the procedure and the patients aren't left with a big bill because that's never good for anybody. Right. It's not good for us and it's not good for the patients. Um, and so we try to preauthorize things, but you know, and then again, [00:06:00] that's also what can delay people getting surgery.
So they come into the office, right? They hear about the product. They're super excited. They're like, I want that. You know, that's the one I want. I trust you. I've seen the data. I've seen the shows. Like I know about this. I've done my research. And then we go, okay. So they walk over to the surgical desk and they sign up for surgery.
The problem is. That when you have someone like my practice that has a lot of innovative products, sometimes I have to say, Hey, listen, I know you're in pain. I know you want this surgery, but we can't schedule you yet until we confirm that they're going to allow us to do it because I don't want to give you, or I don't want you to get a big bill in the mail. That's never good. You've heard stories of that all the time, right? You've seen on the news. It's not surprise billing because we give information if they need it, but it doesn't look good for anybody. And so that's hard. Now it doesn't happen that often. Thankfully, most of these things before I offer them, you know, there's, I'm strategic about this. Like, you know, I put it on my website, I've done the research. I've already practiced in the lab. [00:07:00] I've seen the product plenty of times. And then I go live, right? So when I go out, it doesn't happen with everybody, but when I go out, I've done more than enough information in the background. So you feel, so the patient will feel comfortable and I feel comfortable, like adding that stuff is not technically challenging for the most part.
Um, but at the same point, and I've done the background research on the insurance, but I can't do so much, right? Like sometimes I get out there, I offer it. And all of a sudden I get one, one of the company's switches. They're like, well, as of yesterday, we don't pay for I'm like, how is that possible? But it's just the world we live in.
Um, and when you have a middleman, like the insurance company, uh, you're going to have to, um, make sure that you, you know, work the system to allow this, to get patients, to have it be offered to them.
Will Sanchez: And there's a lot of variables also, um, when it comes to, geez, here we go again, uh, from state to state, uh, state to state, um, the different types of insurance, the levels of insurance.
copays and you know, things like that, that plays a part, [00:08:00] um, in assessing, um, how the patient is going to be able to, you know, pay for this type of surgery. Besides all that, when you have, and you, it was perfect, you know, uh, example that you mentioned that you had to pivot, um, Is that part of the options that when you're talking to a patient and you're offering this, you know, maybe this technological advancement that can help and speed up and then something happens that you're not able to do that process and you have to pivot and re explain and kind of go through all that.
Are those options up front that you kind of focus on and say, we can do this or we can do that? I know when I got my Achilles, they said, well, we can do the speed bridge or we can put a cast on, you know, and we can do it this way. So I, I got my options up front. So let's say something happened with my insurance.
At least I wasn't blindsided. I knew in the back of my head that there were other options to do.
Dr. Grant Garcia: Yes. So the one thing I'll step back and for your [00:09:00] example is there are some of the products we offered are called imp. They're implants and they're not much different in cost than the older ones, right? Mm-Hmm. . Okay. Maybe a little bit more. Okay. And so those are really easy to bring in. And like for instance, like the ACL or para from arthrex, right? It actually is better for certain respects because I'm using less of something else for a reconstruction. So it may actually be less expensive. But it's newer and better.
So that's a really good one versus bear, which is a good surgery as well. But that's, you still have to do the repair and then you have to add that on top. So it's like buying a car and they're like, well, you don't get the cruise control and you don't get the new headlights. So if you want those two things, that's added.
Now it's not charged to the patient, but the insurance company says, we're not going to pay you extra for that. And so we've already given you your lump sum of your insurance. And if it doesn't cover the rest, you're on the hook. And you know, it's not usually the doctors paying the extra amount. It's usually dealt with through the hospitals or the surgery [00:10:00] center.
And unfortunately, it goes on to the patients. And so the important part is to make sure that doesn't happen or that the surgery center is not eating the costs. And then you're doing surgeries that are below cost. We know how that works. If you have a store and you sell products, About you sell products and it costs more than the actual product. That's never good Um, and so, you know, we want to make sure that we're those things are important But it just changes right like your speed bridge and doing another technique. There really isn't a significant cost difference Uh, and so that's a good one. But like you talk about a misha implant. Yeah misha amazing It's really interesting, but it's very difficult to get approved right now because There is no particular, and this is another, we can jump to this, there's no particular, and so people might want to know about the code. Do you have any questions about that before we jump into that section?
Will Sanchez: No, go ahead. Yeah, let's, let's jump into that because you're talking about the, the Misha, right? And, you know, it's, it's really interesting when you, you see, you know, and we've talked about it with other, uh, um, advancements, but this is their fifth [00:11:00] iteration before it was approved by the FDA, so there's all these back and forth and kind of tweaking, you know, this technology and this advancement. So kind of, does that play a part in it also, you know, how many, how many times did things kind of go in front of the FDA, maybe get read, you know, just did and go back and forth. Am I touching upon something here that can, uh, add to it?
Dr. Grant Garcia: Yes. So the, we'll try to make it really brief. We talked about the F the five, five, 10, the five, 10 K pathway. So some of these implants and surgeries, they just go right through the next one, like Arthrex and they'll like update an acre, right. Or they'll do the tight rope. And like, it's a lot faster to get approved, but like the Misha, that's like all brand new, right. They're going to try to find something when you have like a hip replacement and you tweak it. You can easily get a new one approved for the most part. I got you. And some of these cartilage procedures, they can just kind of like navigate. you know, it depends on Macy's difference of pharmaceutical thing. It's like a lot more complicated, but overall [00:12:00] these, the FDA approval, like the bear implant took 10 years to get approved.
Wow. Right. And on top of that, it's the other thing that's that you have to understand is like usually who's selling the product did not design it like bear, like Micah did not design the bear. It was designed at Harvard. And then these companies wait until it's really good. And then they buy it out.
Right. So they bought out that new implant and now they have to make money on it, but they just paid a lot of money for it. And so they have to figure it out. Um, and the same thing is can also think of it as like a drug, right? The drugs come out, they're really expensive at first. Um, and insurance sometimes says, well, I don't really know if you need that. There's not enough studies on it. And so you've got to be strategic. The good thing is. And again, I'm not touting my own horn as an orthopedic surgeon, but doctors are, some doctors are pretty smart and we end up being, figuring out things pretty quickly. So I have little tricks and ways of getting most of these things done or making sure we say the right things to the insurance company to make sure that you get it approved.
Cause obviously what I care more about, [00:13:00] I don't, I don't care about the insurance company. I only care about the patients. I mean, that's the only reason I spend all this time. I mean, being on the cutting edge stuff. Is a lot more time. Like if I just did regular ACLs and regular rotator cuffs all day, I would have an extra 10 hours of my week back.
Right. But that'd be, that's not what I want to do. I like those things, but I also want to be able to offer these innovative things.
Will Sanchez: Yeah. You mentioned that, um, insurance companies often rely on specific codes to determine reimbursement for, uh, surgical procedures. Can you explain that a little bit?
Dr. Grant Garcia: Yeah, that's a perfect example. So in surgery, we have a code book and the code book is like, you know, let's say you have an meniscus. They're each separate codes. And the code is how much the code is set by the insurance company or whomever. And it's a negotiated rate. And so, you know, that code is not only goes like the code is like what I get reimbursed, but also that code is important for the hospital or the surgery center because it's how much they're getting paid, which is actually the more important part of the implants, right?
[00:14:00] If I use all these fancy things, like I don't. Make any more from it like there's no code as a matter of fact a lot of times It's a net loss for everybody because I'm it's a more expensive thing, right? But it's better for the patients which has been in the end was way more important for me But what's but for the hospital or the a surgery center these fancy things are a big bright and they're expensive and so If there's not a code for it, it basically has to get eaten out of another code.
So imagine, let's say I gave you 10, right? And you're all the codes out to 10. Um, if there was another code, it'd be 15 and then you could pay for that more expensive thing and then add it together. So sometimes those two codes are enough to pay for everything. And you can add this fancy implant on top of it. And sometimes it's not. So, so how do they navigate,
Will Sanchez: how do they navigate this? If they don't have, if. They don't have an existing code. Who determines what code to select in order to apply certain costs? Are we getting ourselves in trouble here? But like, [00:15:00] that's, you're knocking yourself
Dr. Grant Garcia: in trouble. This is, this is the, this is the most frustrating thing of innovation. So sometimes. You can use, they have outlets of like unlisted, right? Like this doesn't, this code doesn't fit anything like this. Me champagne doesn't fit anything that currently exists, which is why it's so cool and so innovative, but at the same point, there's nothing like it. So there's never been a surgery like it.
There's never been a procedure like it. And so the insurance company has no marker for what they did, what it's worth. So they're like, you know, what's number, what's number one priority of the insurance company. No, right. So then we got to be like, okay, well, this is kind of like this and it's more like this.
And then that's where the team of the company, my, my group of people, you know, me as a surgeon writing letters and saying, it's actually really beneficial. Here are some studies. And then at some point, eventually things get. easier, but in the beginning it's tough. And sometimes that can be the barrier. I mean, companies go under even with a really good product because of the cost.
And so it's important for us as surgeons to understand, is this [00:16:00] worth it for us to push it? And why would he push it? For me, I push it because there's a niche that it needed to fill and. It's a benefit to patients and patients want it and it's going to be, it's going to do better things for them just like a lot of the other products I've talked about, right?
Like two years ago, I didn't even two or three years ago, we didn't even have really good ACL repair instrumentation. We had some, but not as good as the newer stuff. And now patients are rocking these surgeries. And so it's like, if I never, we never did that for patients, imagine all those people that have had to get reconstructions unnecessarily, or wouldn't have had to keep their own ACL. So it's just, you know, just think about those things, but it's also hindsight's 2020.
Will Sanchez: So is it up to you and maybe the hospital to push? for fair compensation for the medical teams and patients. Do you have to do the legwork after that, after being denied and then say, well, this is, let me explain to you why we should be doing this or X, Y, and Z. Do you even have a, if that's the case, do you even have [00:17:00] a team that solely has to focus on that? Because knowing that they're going to get a pushback based on what you may be doing in the future.
Dr. Grant Garcia: Yeah, I don't mean to smirk during these comments, but it's just because I'm, I'm, I like hearing your response because nobody hears about this side of the thing. And so seeing someone who's lame in terms understand what goes on behind the scenes is really interesting because that's the way I would expect you to respond. Um, but yeah, so. I have a team, you know, I do some of the work, uh, obviously I deal with the headache, right? Cause I'm the one, I'm the one in the front, right? I'm the one that showed the patient the product. I'm the one that talks on the
Will Sanchez: podcast. You're the doctor name that's attached to the surgery.
Dr. Grant Garcia: So I deal with the brunt of frustration half the time, but my staff does too, right? They're the ones getting calls being like, can I schedule it? Can I schedule it? Can I schedule it? Um, but it's like, it's a, it's a group effort here. Yeah. Most of the time it's actually not the hospital. You'd be surprised. They're the ones saying no, no, no. And until it's approved by the insurance company, they don't really do much, [00:18:00]
Will Sanchez: which is kind of
Dr. Grant Garcia: crazy. It's the onus is on the doctor because their incentive for something really expensive and new is very little. Why would they do that? Right? Like why would they offer it? Yeah. Um, unless they're going to bring them more business and so one of the number one questions they have is can you bring more business as a result of this, which is kind of crazy, but that's just the way it works at the surgery center. It's a lot different, which is where I actually do most of my stuff. You know, they're that's a little different because. I'm significantly involved in that. And so as a result, I make a lot more decisions there so I can get things pushed way faster, which is why we're able to do a lot of the fancier, newer procedures at the surgery center outpatient. But I'm also privy to way more of the costs. You know, a lot of doctors not in private practice, they don't see any of this stuff. So like this, this may be brand new to them. They're like, I didn't know it was more expensive. I just do it. It's not a big deal.
Will Sanchez: Right.
Dr. Grant Garcia: But as me, I have to be conscientious about that. But I also have to, you know, deal with the pushback. Um, and you know, they'll, they'll hear the pushback, but they won't know why. Right. Like they're not going to be told from the hospital. It's this much [00:19:00] X more or less. And you're not going to, we're not going to get reimbursed. So we're not letting you do it. Um, but, but the code thing is important part, right?
Like some of the things when something's so far out there and so new, just like a new drug, It's really difficult to get approved at first. And this is talking about like amazingly renovated, revolutionary product, right? Like the speed bridge, amazing product, the tweaks that Arthrex does amazing products, but they're not revolutionary to the point where they need to have their own separate new surgery type, right? It's just a modified modification of a current surgery. And when you modify a current surgery, that's a lot easier to get the coding done. Right. Because most of the time it's like, Oh, it's like the code for ACL repair and the code for ACL reconstruction is the same and it's actually already listed. And so the nice thing is when I start doing repairs, I didn't have to add any, there was no coding issue and the costs were fine. Um, and it's not an issue, um, but it did become a problem with the bear implant because I had to still do all that surgery and add the bear on top and the bear is not inexpensive. [00:20:00] Um, and so that's important for, you know, people to understand because. As soon as it came out and I started doing it, I had floods of people coming and asking for the bear. Um, and we had to be understanding of saying, hey, how is this going to work? Can we offer this to patients? Because the hospital wasn't doing it. They're not allowing it. because it's too expensive.
Will Sanchez: So here's the million dollar question. Ready? Stand by. Here we go.
Dr. Grant Garcia: I know this is where this is going.
Will Sanchez: How do we get hospitals to get on board for technological advancement while still surviving and having financial stability and then getting approval with insurance where it could be one happy pond between doctors, hospitals and insurance and the beneficiary out of all this is the patient. The show's not that long.
Dr. Grant Garcia: I, I am not even sure I'm gonna fully answer this question for you out of, out of, uh, the fact this is gonna go live at some point. Um, so it's not, I don't know if it's gonna happen for a [00:21:00] long time. It depends. But with Covid, um, and Okay, it depends on the place. Yeah. With Covid it depends place.
There were a lot of cuts in things and a lot of hospitals lost a lot of money and so they were more strictly evaluating things. So like basic surgeries, they love those right. Basic surgeries, they love them or, you know, a hospital based surgery is loved, but when it's a quick, easy outpatient surgery, and then it's super expensive, they get no money from, you know, the most expensive thing they make off of like is spine surgery or a surgery where you're in the, you're in the hospital for multiple days. Right. Because then you get like, it's the, the charges. Like, you know, I had surgery, I had to go to the hospital. It's like, you know, you see your bill. I won't you
Will Sanchez: there that long too. So it's kind of a, really a cash 22. Now they're like, you're saying they want, they, they get, they make money by keeping you there, but they really don't want you there as well. They're, they're kind of pushing you out the door.
Dr. Grant Garcia: Nobody knows what they want at the hospital sometimes. So I'm also very biased because I do 99 percent of my surgeries outpatient surgery center. But the reason that that's beneficial to patients [00:22:00] is that when I do a surgery, We do the highest level surgeries in the area pretty much. Um, we're doing really complex surgeries, but we're doing them outpatient and the insurance company is paying a lot less for those surgeries because they're not paying for the other things that are involved in the hospital and the patients are paying less to, you know, even patients that end up paying out of pocket sometimes, which happens, we have patients from Canada or overseas, or they don't have insurance and they want to pay for a surgery. Still, it's much less than going to a hospital, like four or five times less sometimes it's crazy.
Will Sanchez: And.
Dr. Grant Garcia: You still get the same amount of care plus the efficiency of the surgery center and you know, the cleanliness and everything else and the ease of getting implants in like when I have these conversations, like I'll be, you know, once every two or three weeks, I'll call one of these new companies and I'll say, you know, let's talk about the implant and they're like, well, how fast can you get it improved? I'm like, how fast can you make it economical for the patients and everything else? Because that's not hard for me to get it approved at the surgery center. You know, I get. new products. And in like two weeks, we're using one of the first renditions of a live [00:23:00] surgery in like a couple of days or a week. And, you know, we didn't need approval for it. You know, as long as the patient's okay with it, I can wear a head camera and navigate and teach other surgeons how to do this surgery. You know, it's not hard to get new products involved. Um, it's really more of, is it the, it's more of the cost. You know, is this going to make, is it going to be good for everybody? Is it going to be something where like we actually can do this and make it fair and even and not have a situation where, you know, if everybody's just, if the surgery center is just making no money or no, it's just all above cost. That's a big problem.
Will Sanchez: All right. It's 2024. Um, I just did, uh, an event, you know, I do a lot of events and I just did one from Microsoft with, uh, Satya introducing now, uh, Mustafa, which is now part of the AI team that they pretty much got from Google and the long way that I'm pretty much getting to is how is AI going forward can maximize, [00:24:00] um, the little things to maybe ensure that we could get closer to that middle ground where we can save money financially for the hospitals, right? Um, implement maybe faster procedures because we're spending less time on certain things. So there's money saving their costs there, and then the patients can get what they want. Um, so pretty much identifying cost Effective alternatives as AI ensures like groundbreaking treatments that's accessible to patients. Can you see a world now where AI is working on all of these aspects and speeding up the process where you're saying, you know, we can save money here because we're changing it, but it's still the same. Can we see that implemented possibly? where all of a sudden we get closer to that middle ground of everyone's a little bit happier.
Dr. Grant Garcia: We can, but you got to think about this. You got to change the [00:25:00] mentality. It's not no first, then yes, right? It's, It's, you know, there's certain, there's a com, I'm not going to bring up an insurance company, but they review every single chart now. And they never used to do that. If there's a certain code, you just get it approved and they trust the doctor. Now, every single surgery needs to be approved specially. So it takes an extra three months for the patients and it's torture for them, right? And so if they program the AI to say, we're going to deny this surgery first. And then make them do a secondary review and that's built into the AI, there's no way it's going to work, right? If it's, if it's like, okay, these guys have been to medical school for four years, five years of residency, one year of fellowship. They've taken care of thousands of patients and they want to do a surgery on a patient because they think it's the right thing for them. How is that the, not the person that should be dictating whether or not it's the right thing to do? I understand, you know, evaluating big fancy things or really expensive surgeries. Should we relook at them? But for the basic stuff, it's, it's absolutely absurd. So they're, they're wasting so much [00:26:00] time trying to cut costs and trying to roadblock things. And you've seen it so many times in the news, right? Of people who had these surgeries and they wanted to get the newest thing. You got friends.
Will Sanchez: Yeah. Yeah. So
Dr. Grant Garcia: they need to, they need to get. Right. So for the simple stuff. They need to just get rid of that stuff completely. Maybe the
Will Sanchez: stuff that AI is using the algorithm that reads the correct codes, right? We go back to codes or the correct
Dr. Grant Garcia: notes, the correct notes. That's really the key. So they can see like, okay, Dr Garcia
Will Sanchez: codes or notes. If you match that, then we can push that along. And then the more, the complicated stuff, we spend a little bit more time dissecting or something like that, but instead of a hundred percent kind of deep diving and really kind of, um, dissected it all. You know, some of the stuff that hits all the codes, hits all the notes, reads it, and then it gives it a thumbs up automatically. And then maybe that gets pushed and speeds things up. I don't know. We're just making stuff up.
Dr. Grant Garcia: No, I think we should talk about this. Another topic. It's a, this is a fantastic, this is not where [00:27:00] I thought this would go, but this is awesome. So the way the AI can help in the way I see this doing is if first off, the insurance companies are not priority is not denial. It's it's approved, right? You know, you have raising premiums and higher denials. Like that's never good. Right. So if the priority is approve and I, and I trust the surgeons, so, you know, 75 percent of the stuff they do, we're going to trust them. Right. And if they, if, if there's a surgeon that's got a bad track record and trust me, not everybody's great. We know how this works. Then maybe they're, their stuff's being more scrupulous, but for the ones that every day come to work and work 80 or 90 hours to help people, you know, for, uh, for these causes or try to get these new things approved, you know, most of the things we do should just be, we're done. You're good. And the AI sees like, you know, ACL tear, pain, more than a couple days, all the, you know, risks and benefits were discussed. Like, just do it. Go get it done. Get done for the patient, right? Okay. Super fancy cartilage procedure. You're going to realign their knee and like, just wait a second. Let's just take a, [00:28:00] let's take a look at what you've done so far because that's a lot of surgery. But what they can do is the AI can have all of the data. that we already know built in. They can see the, you know, the 1500 studies on cartilage transplants and know that like they work because I still get insurance companies after transplants and cartilage transplants been out for almost 15 years, if not more. I'm probably even probably incorrect on that. And there's over 1500 studies that are really good. And I had, I have really good insurance companies that say it's still experimental. I was like, I don't know what,
Will Sanchez: yeah, that's, that's
Dr. Grant Garcia: great. That's crazy. As a matter of fact, there's been like multiple versions of cartilage transplants and how they get better over the last 15 years. It's just, it's, that's impossible to say, right? Like if a car was 15 years old, you would say, you would say it's beyond experimental. You're like, it's time to refresh. Yeah. Yeah. It's just like, so the, that's the biggest thing we, the AI can be like, yeah. Here's all the studies, you know, because a lot of times people don't know when we do [00:29:00] insurance approvals, I get on the insurance call and the person on the other call is an anesthesiologist and no offense to the anesthesiologist, but that does not orthopedic surgeon. And half the time I get on the call, they just want me to talk to them. So they'll give me approval. So I'll be like, hi, here's what I'm doing. And they're like, I'm not even sure what surgery you're doing. And I'm like, excuse me, but you're the one denying the surgery right now. Yeah. And so like we need, we just need it to be where the AI is so smart. It says, okay, 1500 studies and cartilage transplants. They've done alignment. They've checked all this stuff. Everything's good. Boom. You're done. You're approved. The surgery center
Will Sanchez: utilization that the patient. Um, you know, whatever is happening with them, finding the cost effective pathway that I can maybe utilize that as well. That makes insurance feel a certain way about it. Um, but I think I can possibly bridge a big gap right now that's happening, um, and maybe get us a little bit closer because if if they can help plan and assess [00:30:00] these strategic. Um, accessibility and deniability and kind of reduce some of that, then maybe we get closer to some of these goals. And then, like you said, if it's something that's really complex and I think you, you illustrated it perfectly saying, hey, wait a minute, hold on before we go that route, you know, let's go this route, let's explore this route before we do something that's complicated. But if you have the data, you have the notes, um, You know, it, it would be great just to, you know, click on the button. You know, this is what I'm doing. And I'm, I'm, what are you doing? Well, there's between start to finish. I'm inputting six codes and I'm, these, these are the six codes I'm putting in. It reads it, it understands what's happening and what's the diagnosis and goes, yeah, that sounds good. Check approved next, you know, and if we could get to something like that, that would be just ideal. And, um,
Dr. Grant Garcia: And it would also on the costs, you're really appointed because you asked me, how do I get all these things done? Well, I have an ex, a lot of staff that [00:31:00] helps me and that's not inexpensive, right? And so people ask, why is the United States so expensive for healthcare? Well, it's expensive because the healthcare costs in, in Canada. and they have lower healthcare costs. They have a lot more rationing of costs, which is why I see a lot more patients coming down for cartilage transplants or some of the fancier surgeries cause they're not a practitioner. So they ration or sorry, rationing of care. And so, you know, total knee replacement, I'm sorry, you know, regular, regular surgeries, ACLs. Those are, those are easy. It's a long wait, but you get them done. Right. But when it's a fancier surgery, they just say, we just don't pay for it. Right. It's too expensive for the healthcare. I gotcha. For the whole thing. Um, and so that's, that's how you keep the costs down, but also, you know, there's less insurance authorizations, right? It's because all through the government, so you're not having multiple companies changing their policies and you're not having for profit, right? I mean, look at, look at the Yankees stadium, how many insurance companies are on the back [00:32:00] of that wall? Yeah. You know, like how many insurance companies we can talk about insurance all day. We've taught this. We don't want to go too much detail, but insurance, anything right there, but they're pretty much run all sports. And they run all the advertisements. How do they have so much money to do that? You know, that's interesting to me and then I have we have this conversation about how people can't Um get the things that they want and we're not talking about, you know, it's it's money it's they're expensive but not as much as a the name on a stadium costs So, you know, it's unfortunate, but you know what I mean? The thing is also we're not going to be Debbie Downers here. I think what people need to understand is that,
Will Sanchez: no, I think this is good. I, I mean, I'm not sure how people feel about, I mean, I think this is really good topic. I mean, something that it's something that it's, Something that we don't always talk about, right? We're usually talking with technology and we're having our guests and things like that. I think having this topic to have these discussions and having real discussions, right? There's a real conversation that we're having, uh, that is concerning to every single patient, [00:33:00] doctor and hospital provider. They all are dealing with this in some way, shape or form. And then, um, and. I love hearing about how the pandemic, you know, added to this and made this even more difficult because of what was happening to the medical, uh, field during that time. So I think this is, I think this is great topic. So
Dr. Grant Garcia: yeah,
Will Sanchez: and then one
Dr. Grant Garcia: thing I'll tell, no, I, I think it's good and that's why I wanted to bring it up, but I think what I think the patients should take away from this, and we have a couple of little things I think we still want to chat about, but, um, Is that I, as a physician or orthopedic surgeon, and there are a lot of us out there, and if you're listening, most of the time we can get this new technology done, okay?
I'm very, I'm always thinking of creative ways to get it paid for for you, so that you can get it done, and I'm always thinking about, not only do, I mean, It's great to have something that's so new and awesome and works so well, but that's, I'm [00:34:00] also want to figure out how it's going to be able to happen for you.
And so by the time I'm offering it, most of the time I figured it out. Um, and most of the time, a lot of the doctors have figured it out. So the good news is that this is not that common. It's just good for the patients. If hopefully someone listens to this, that comes in my office and says, yeah, I know that that's going to be tough to get approved. But like, I really want it. And honestly, a lot of the, like, I have a guy waiting for the Misha implant and he's like, I know it's going to take a couple months for the insurance company. I know it's going to be a fight back and forth. I'm okay with it. And like, that's why I want something like this, right?
Like I want someone to understand that like, when you want like the newest, fanciest, shiniest thing, and it's going to be better for you because it's avoiding knee replacement. That you're okay with being a little bit patient, right? Cause we know in the United States that the word patience is not the best thing. And listen, I am probably one of the worst people of that, but nonetheless, it's important for people to understand that most of the time that these things aren't out of reach. And thankfully, if you live in the United States and you go to good physicians or surgeons that have been trained well, and they really care, [00:35:00] you know, you can get these things done.
Um, it's just, it's all about access and it's not access. That you, if you have an insurance company, you're not going to get access. It's more like finding the people that are willing to offer it for you. And that's what we keep talking about. Innovation, sports, orthopedics all the time.
Will Sanchez: Yep. And there you go with innovation and AI. You know, we, we're going to get to these AI capabilities and, uh, we're going to help navigate the complex landscape of medical technology by prioritizing patient outcomes and financial sustainability. That's the goal.
Dr. Grant Garcia: All right. So this, so just to remark this, this is going to be AI in orthopedics is going to be a topic. Will and I have way too many pending topics, so this will be on the docket maybe towards the summer. Um, the one thing I wanted to bring up with people, uh, is that we've talked a lot about the costs. But the other balance in the roadblocks is, you know, there's a, there are a handful of people that [00:36:00] like these new texts, but not everybody's willing to jump on it right away.
And some people want to see the long term data. And so there's a lot of naysayers too. And so that's also hard for people. I see a lot of second, third, fourth opinions. And sometimes I get opinions that are also reverse opinions. They've seen me. They've seen someone else and then they come back and see me and they're said, the doctor said that the surgery you do, it doesn't work.
And I said, okay, well then we have to work this out. Now again, I'm not offering things that are experimental. My things have been studied. Sometimes it's because it's a competitive nature, right? You know, if that surgery is not offered by the other person and they're upset because they know they're not going to be able to take care of you. They may say it, right? And that's something people need to be aware of as well. It's important, but it's also why I always tell people to get at least one other opinion.
Will Sanchez: Yes.
Dr. Grant Garcia: Because you never know what you're going to find out. And honestly, we joke all the time about Dr. Google, but I will tell you that Dr. Google, in some [00:37:00] cases, if the appropriate search terms are used, can actually be really helpful for patients. I've had so many patients be like, I didn't even know that you could fix that. Because my doctor said it wasn't possible.
Will Sanchez: And
Dr. Grant Garcia: then they come into that and go, wow, actually that's really possible. And so that's important, but it's also important to understand why some doctors may be hesitant, right? If you're, we're all risk avers like I'm not the type of person that's going to have a bungee cord and have a little bit of frame in it and just jump off the bridge. Right. Like I know that I'm, I'm, I need that. I need two bungee cords.
Will Sanchez: I want nothing to do with bungee cords. Let me stop you right here. Right. I've jumped out of a plane. I've done, I've done a lot of stuff. There's no way you're strapping me to a rubber band and having me jump off at anything. I digress right here, but I just want to stop you right there. There's that, that exact, there's no way I'm doing a bungee cord. Anyway, go ahead.
Dr. Grant Garcia: All right. So you know what? Let's, let's do like, uh, like lottery. You know, they're not, a lot of our friends aren't going to play the lottery. They want to have, they want to have a [00:38:00] guarantee, right? They want to make sure that what they're doing is going to work. I don't want to go in the OR and say there's a one in five chance that I'm not coming out with any type of good outcome, right? That's never, that's never my goal. My, I go in there feeling like this is 99, a hundred percent. Right. Even if it's not always that case, um, but some in a lot of surgeons want more long term data. You know, I'm willing to push the envelope a little earlier, but also my patients know that. And so I've had that balance. I built that practice to do that, but it's totally fine that surgeons aren't ready for that. You know, that doesn't, you don't have, and especially if you're new in practice, it's really gutsy. If you're new in practice and you're ready to feel like the patients are concerned about your age, your abilities, because you're new, In practice, and I know because that was me a little while ago, right? And it's okay to be nervous to try something new, and it's okay to wait longer to have more information, right? You're not going to miss the boat on this. And I think that's important for people to understand. And just because you see someone online [00:39:00] promoting some really cool new product, it doesn't mean you have to do it. Um, but at the same point, you should have an open mind because that's what I've started to do is have an open mind. When I first, when I first started practice, if you asked me if I would repair an ACL, I'd tell you absolutely not. I'd say that's, I don't think it's a good idea.
Will Sanchez: Gotcha.
Dr. Grant Garcia: And now look at me, I'm going down to talk about, to talk to all these surgeons through Arthrex about how ACL repair is so amazing. So you have to just have an open mind. And the best way that innovation happens is cautious optimism. And so my first patient I did an ACL repair on, I told them this might not work. Here's the data. It's a higher chance of retear. And all of a sudden, you know what? It worked really well. And then the second one, I told them this might not work.
And I've done one of these. And the next patient told they've done a few of these next patient, you know, and then now I'm now I'm at like 35 patients and I can say, okay, my last 35 I've done really, really well, you know, for the most part, we're [00:40:00] talking about a very successful procedure, still short term follow up, but successful. So you build upon those things or you build upon experience, you know, someone coming in saying, I saw Dr Garcia's lecture on ACL repairs. He's done this many and they've done that. Well, I feel good. That I do it the same way or the same technique that's online or that that's available that I'll do that.
They will do well as well. So it's just it's important for people to understand that though. Um, and, and then, and that this is the way it works. This is the way innovation happens. It also happens from us being willing to share, you know, I'm constantly texting on my phone. I've got texts from different people.
Like, how do you do this surgery? How do you do this surgery or vice versa? I'm asking them like, Hey, You know, we did a really unusual surgery today that you see once every two or three years Um really uncommon and I used a a special tight rope fixation. Oh yeah. Will will like, um, and the old surgery for this was a huge reconstruction passing tendons. You have to be non wavering. I did the surgery [00:41:00] in 30 minutes. It used to take about an hour and a half, which just trying some new technique with new implants and new innovation. So it's important to understand that you want to take the risks sometimes. And it can really help, but it doesn't, it's not always that case. And just to understand, like you want to make sure you look at the data before you do this and that everybody's a little bit different.
Will Sanchez: Yeah. And I think the highlight for those listeners is pretty much to, you know, you're engaging the patients in this decision making right. And, and having that informed decision. And we, I think we mentioned it every other show. to always get a second opinion, right? We talk about I'm doing this and I'm doing that, but we always encouraged to get that opinion to get that information. Um, and, and making sure that you're comfortable with that process because more importantly, the patient is the one that's kind of going through this and having being informed on what they're about to get into is, is really important. So they're not surprised or caught off guard. You want to be [00:42:00] happily surprised, not the other way around. So I think communicating that and, and sharing, uh, that information is really, really important, uh, for the patient. So once again, we always encourage, especially when you have these procedures to, it's fine to talk to multiple people, you know, and even my friends, they're like, I have a doctor. I say, great, go for it. Get all the information. I recommend just because you're doing something big. You know, I had a friend that had hip surgery. Um, you know, after an accident, it just does not hurt to talk to somebody else. You have to wait anyway before, you know, you're going to have the surgery, go talk to someone else and hopefully they're going to tell you the exact same thing and you're going to feel really comfortable about this decision making and you go with whoever's you're most comfortable with. So I think that's the, the big picture. Get your information. Be informed. So your decision making process, you feel comfortable going into it.
Dr. Grant Garcia: Yeah. So two points to that one. Yeah. [00:43:00] And a lot of times I see second, third opinions. They just came in. I go, I totally agree with that. He said, you know, I think that that's awesome. I think you go with whoever you want to go with. We feel most comfortable with and about 75 percent of the time. That's what happens. 25%. I might have a differing opinion, but that's also my experience. Um, and so, and that's the way I feel again, I'm never knocking another doctor. That is the last thing you want to be that type of person. So I say, here's what I would recommend and you choose what works for you. And I've told you this before, I, and I have a, I kind of have a running joke with my patients and obviously, you know, if patients in pain, I'm not, we're not joking around by different options, but nonetheless, I give people a book, like a menu of surgery options, and they're not used to that.
Sometimes they're told this is the way it is. I'm, I'm the surgeon. I'm going to do this. Dude, this thing for you and I had a patient last week. I gave them six ICL options and they said, Oh my God, I wasn't expecting to have so many choices. I said, well, I want you to decide because this is comes to starting a new tech. When you offer something like that, you have to [00:44:00] give them an out. If they don't feel comfortable with it after they do some research, right? And I, and most of the time for some of these procedures, they're all in, but sometimes they get nervous. You know, I've had patients that have been scheduled for the bare ACL and they've backed out and the patients have been scheduled for ACL repair and they've backed out and that patient has been scheduled for any of these types of procedures and they backed out cause they were nervous.
And that gets to your point on, do I have alternatives? 95 percent of the time I tell them, here is what we used to do. Here's what we do. And you used to use like. six months ago. And I just have the luxury that patients come in asking for the new tech because of my website, my social media, my reputation for having some of the new tech referral for my partner saying this guy's got the new tech.
And so I get, I'm, it's, I am, it's easier for me to have these conversations. The problem, the hardest part is when you have the patient come in and this is, I keep bringing up ACL repair because this is the best example. You have a patient come in, they've seen three doctors. All of them said they need a reconstruction [00:45:00] and I think I can fix it.
And that's where things are like, you know, you give yourself an extra 10 minutes, you close the door, you sit down, you lower your voice, and you're about to tell them something that they did not hear before. And that's going to be a little bit of a shock. Right. And those are the hard ones. And for people that are just starting out to offer new tech, that's by far really daunting.
Right. It's really daunting to say, you know, I'm going to do something that's a little bit new, right? Because if you've just gone through a few years of practice and you've now established yourself and you're no longer, people no longer looking at you as a baby face surgeon, that's maybe learning how to do these surgeries.
And now you're offering a new procedure. It's important to come with some confidence, but also it's important to understand, you know, where the patient's coming from too, because. Some patients I tell them, I'm like this. I told them the first person did a lower trapezius transfer on, which is where you transfer this.
And we've talked about this very briefly. Yeah. I said, listen, I've gone to the conferences, I've learned about this, but this is the first one I've done. I feel very confident that I'm going to do well and for you, but they have to know that, right? And then when, and then [00:46:00] they didn't end up doing amazing and then the next one and the next one and the next one, but you know, it's, what's your reaction
Will Sanchez: when, when you have a patient that, that, I'm sorry. What's your reaction when you have a patient that you can tell is intimidated by maybe the situation or, uh, the procedure, but you can tell, right? That, that there, there, there's maybe there's some doubt or they're intimidated where they may just, you know, just say yes to anything, you know, because I'm pretty sure you have. you know, people, because that's just natural reaction. You know, is that a red flag for you? Is there something there where you kind of notice what's going on and say, well, wait a minute, I, I kind of want, I want them to have this procedure, but at the same time, I don't want them to just go along with this, um, feeling a certain way.
Dr. Grant Garcia: Yes. So to answer your question, there are two types of those types of patients. The first one is the one where there are these, you know, patients that are [00:47:00] just so trusting of the surgeon and they're not doing any research and they just want you to tell them what to do, right? Most of the time that's good, but sometimes I'm like, okay, wait a second.
Like, you know, you came in like ready to sign up for surgery and I don't think you need it. Right. Or I'm not sure you're ready for this. Like, do you understand? Like, I've just told you I was going to break your leg, straighten it out. I was going to replace your meniscus. There's complications. And they just said yes right away.
Like, that's never normal in my opinion. And I love when I went, sometimes they come in, they're like, you know, some of my engineers from Boeing, they're like, Oh, I got it. Like, here's the alignment you're going to correct. And like, I get it. I get it. Like, that's not that person I'm worried about. Yeah. Yeah.
Yeah. So yes, occasionally I will be honest with you. This happens every single day in my office. You have heard about the procedures that I do. I have a patient coming in, they say they have anterior knee pain, and I tell them they have a cartilage defect, we're going to need to do some realignment. When you do really complicated, fancy procedures, and you do big combinations of them, I mean, we do some of the most complex procedures in Washington State.
There is no way that you don't get patients in the office. I have [00:48:00] patients that start off the visit crying, because they're so upset. They've had 10 years of pain. I've had patients coming in, So angry because they've seen three doctors and no one said they could help them. I get to see every variation.
And honestly, 10 percent of my patients, I have a patient that I had to see five visits before her ACL reconstruction because the first time she had ACL surgery, it was such an atrocious experience. She had PTSD and did not want a surgeon to touch her. But she was so miserable, I had to basically earn her trust for five visits straight.
And you know what's really cool? I just did her surgery and I just got a, we got a big hug. So that was awesome. So we're back on track, but you, you have to adapt to each person. I mean, this is another show topic. It'd be the personality. The personalities needed or how you have to adapt in the office to each patient because that's really important. I tell people with the first visit when I throw out, and you know me, I talk fast and I have lots of information I want to say. And that's not always the best idea, uh, with some patients that are a little bit nervous, but it's just my personality type. [00:49:00] So, I tell them it's okay to feel like a deer in headlights.
Okay, this is normal for the first visits. You are not required to do anything today and I don't want you to. Now most of the time those big surgeries that I do require initial simple scope and so that's pretty easy to conceptualize, right? Well, like I'm going to take you to the operating room, we're going to put two poke holes in and we're just going to go look and figure out what's going on.
We do that for a number of reasons. One, because I can tell me more information in the MRI and two, because I might be able to get a little bit of benefit and three for the insurance company. So they can see, like, look at that hole. Like you can't not get, let us do the surgery on them. Right. And then, so once they do that, then they go to my website and they do all the review of the stuff. And then all of a sudden the second visit. Third visit.
Will Sanchez: Yeah,
Dr. Grant Garcia: and then I feel ready and then when they start repeating and telling me what surgery they're getting and they're like I'm getting MPFL TTO Macy cartilage transplant. I go you're ready. You're ready. No now you're informed And so yes, [00:50:00] most of my patients for the really complex stuff Which is probably about 30 percent or 40 30 percent of my practice is really really complex.
They're always like that well And they're most of the time completely shell shocked by the options. Very, very rarely are they shell shocked the day before surgery. So that is, that's what I pride myself on. That is the hardest but most fun part of my practice. Yeah. Is taking something super crazy complicated and super intense And making it them feel completely comfortable with it and understanding.
And that's why I spent so much time on the surgical videos and so much time on the podcast and so much time, all this. So my patients can see all of that and they go, Oh, that makes sense. It doesn't look fun. But it makes sense.
Will Sanchez: It doesn't look fun. Nope. All right. We should wrap it up soon. Let's talk about our next guest here. Why don't you talk about, uh, about Dr. Schaefer here?
Dr. Grant Garcia: All right. I'm super excited about this one. You know, I, when I asked him to come on, I'm, I'm really excited. So [00:51:00] Dr. Uh, Andre Schaefer is probably one of my best friends as well. We both went to hospital special surgery together in New York. Um, both taking care of all the professional sports teams, which we've talked about. Um, and he is now back in Seattle and we're actually both from Seattle. He's originally a firefighter, but what's really cool about him is he's triple fellowship trained, but he is now our newest spine surgeon. By new, I don't mean new to practice, just new with us. And he is, has some of the most cutting edge, innovative spine surgeries you can imagine. And we have a lot of good spine surgeons in the area, but the stuff that he's offering, he's going to talk to us about scoping people's backs. And I just saw one of the patients in the operating room. He, the next, the patient called the next day to ask if he had actually had surgery, you know, and, and spine surgery is not supposed to be fun.
And he is, he has made this into, he is on the edge. And again, he's just, you know, he's just building a Seattle practice, but the, the, the, The stuff that he is doing [00:52:00] is next level. And people need to know about this because very few people in the area are doing this. He's doing disc replacements of your neck, disc replacements of your lumbar spine.
We never used to do those. Everyone was told fuse, fuse, fuse, fuse, fuse, which means. That something's going to happen to the next disc below and you're a repetitive spine patient, you know, and he's doing these scopes where he's taking these discs out and it's just these mini tiny incisions. As a matter of fact, he was teasing me. He goes, my incisions are smaller than yours now. And I was like, dude, come on. And you can see they're smaller than the pinky.
Will Sanchez: He's talking
Dr. Grant Garcia: smack. I like it. You're going to see, you're going to hear so many cool things, and this is near and dear to my heart because I've had a herniated disc, and I almost had to have surgery for it, um, and it was nothing fun about it, and I looked, and I had a lot of trouble trying to find someone, and I am an orthopedic surgeon in Seattle to do the surgeries that he's doing, and so one of the reasons that it was really near and dear to me when he was available to be taken and come to our group was that he [00:53:00] offered endoscopic spine because that's the only way I was going to get my disc done.
And it literally took me three months to find somebody that I could even consider doing this surgery on me. And so that's no joke when you're a surgeon trying to look for that. I was willing to have to fly out of the hospital. Out of the out of the state to do it now. I don't have to if I have it. He's gonna do it.
Trust me Um, but you know what to have this opportunity to offer this technology to patients. They need to see they've already seen. Dr Ye They've seen dr. Weil there's so many other good partners in my group that offer these type of things But this spine stuff is in infancy This is what sports was 10 years ago.
You have people scoping spines doing many, many, many incisions and patients doing really, really well and doing much better than they used to do. And so I'm getting too excited, but I want everybody to understand that you are going to be blown away by what is capable of happening in spine surgery because people are terrified of spine surgery, right?
Will Sanchez: Oh yeah. It's terrifying. It's something that we talk about. Like, I don't [00:54:00] want nobody to touch my back and screwing something up. And no, and fearful about it. And, uh, a buddy of mine had back surgery major where he, uh, also he, they, they cut them in the back and then did a C section in the front. He was under for like eight hours repairing this back of his. That was just so messed up. This was a while ago. It was major, major surgery, uh, that eventually brought him relief. But maybe the first nine months he was like, I regret having surgery. And then finally he started to feel better. Anyway, I don't want to scare people here, but no, no, that's it. No,
Dr. Grant Garcia: leave that thought for everybody because one of the surgeries is going to talk about, used to have to be done with the back and the front. And as a matter of fact, in the next six months, he's going to be able to offer the surgery from a mini little incision just in the back.
Will Sanchez: That's probably
Dr. Grant Garcia: so much what your, what your friend had. And I tell you right now, one of the potential surgeries and maybe the longterm future for me is something you're talking about where maybe the back and the front needs to be done.
And [00:55:00] just talking to Andre a few weeks ago saying, no, dude, you just wait a couple of years. It'll just gonna do it from the back. It'll be a little mini guy. Like, as if like I'm going to be wait for the next upgrade. Uh, to come. So, you know, I think we're going to see something. I think people are going to learn so much and understand what's available out there because, you know, he did the first scope of someone's back in Washington in ProLiance. Like six, eight weeks ago in pro liance, that's huge. And so you're going to see, this is like, this is innovative. This is cutting edge stuff that you've never heard of. Your friends have never heard of this and maybe they have, but the ability now that Washington state and Seattle has this opportunity to have a guy like him there. Who's also, by the way, super nice. So this will be really, this'll be a really good talk. So
Will Sanchez: let's get out to the nitty gritty. All right. And what kind of fan fan he's going
Dr. Grant Garcia: to be as he's a Seattle guy, man. He's lived here. He's not going to jump ship with us on the
Will Sanchez: Yankees. We'll see. We'll see what happens. How that [00:56:00] conversation goes. What we might have to, but we'll, we'll find out. Figure it out, we'll figure it out. A fun fact, uh, I broke my wrist playing football and I had surgery at the hospital for special surgery. So we always kind of find a way to kind of bring it back around. And as we do that, we wrap it up. We want to thank everyone, all of our listeners and viewers. Check us out at sports doc, talk, uh, dot com, and also our Gmail sports doc, talk podcast at gmail. com. But you can go to sports doc, talk. com and get all our information. We have transcripts, we have our shows, we have videos. You can request topics. Uh, we have links to Dr. Garcia's website and a whole bunch of fun stuff. I don't know what else am I leaving out? Dr. Garcia.
Dr. Grant Garcia: You're not leaving out much. And we got stuff for each one of those. We got a, we had a really good one today for, uh. Hot topic. We got a really great guest that's requested, you know, do all those things, go to the website, check it out. And then it links to my site too. If you want to see how the procedures are done or learn more about them. If you [00:57:00] want to see a great video, well on there, you should also go on there. Uh, you can see all those different things. So, you know, learn about it. The website's awesome. It's been really, we've had a lot of lists. I mean, we've had people from all around the world that take a look at it. I get to see the, uh, the information. Um, but we're just here for you guys. We're here to teach. We're here to give information. And again, a lot of it's information that is likely is true, but again, take some of it for his opinion as well. So hopefully you enjoyed it and we're really looking forward to our guests next week.
Will Sanchez: You're here. Thanks for joining us. Audio Transcript
A Year in Review: Newest Ortho Sports Tech Update

Will Sanchez: [00:00:00] Dr. Garcia is unbelievable. We've found a technology. Welcome everyone. Welcome to sports doc talk. I'm Will Sanchez along with our orthopedic surgeon and sports medicine specialist, Dr. Garcia, man. What a great show. We're really excited about this show. Because we're celebrating it's an anniversary.
Will Sanchez: We're celebrating 2023 as a full year has gone by with our incredible guests. Amazing topics and you, the listeners, we appreciate everyone. Dr. Garcia, can you believe it? You dealt with me for the entire year for this anniversary. And now we are celebrating by scaring people. I apologize, everyone, because now we're on video.
Will Sanchez: We're on [00:01:00] YouTube besides your favorite listening platform, Spotify, Apple, iHeart, Amazon. We are now bringing. The noise to you too. How you doing Dr Garcia? I
Dr. Grant Garcia: know I'm excited. Happy anniversary. So one year ago from today we decided to do something different. Mix up our the old NYSE podcast, you remember?
Dr. Grant Garcia: And we came up with the idea of Sports Doc Talk. A lot of time building that logo. That logo seems simple, but it's not. It's a lot of conditions to figure out what was most important was whether it looked like Will or not. I didn't really care about my part, but I really cared more about that. We made sure it looked, it looked, will look good in the picture.
Dr. Grant Garcia: So that was,
Will Sanchez: I think you would need a lot more Photoshop to make me look good. So we're just happy. We eventually just gave up and like, it ain't getting better than this brother. And I,
Dr. Grant Garcia: and I get, we can say this on the podcast, since we're going to have a little bit of fun too. I think it's good for us to mix it up, but the microphone wasn't easy to do and not make it appropriate.
Dr. Grant Garcia: So we so we did a lot of. [00:02:00] stuff on that logo, but we're really excited about it and it was good commissioned work. So, and you know, we've come a long ways. I mean, this has been a really awesome experience. And again, the, we've had people requesting to be guests. We've had people from all around the country.
Dr. Grant Garcia: I mean, I texted will just a little while ago about, you know, I had my med school friends. There's about 20 of them, all different surgeons from throughout the country, not just locally. As a matter of fact, no one's even from the Washington state area. And they asked me about the Q collar. And they're like, you know, but this guy, Dr.
Dr. Grant Garcia: David Smith, the Q collar. And I was like, dude, I put it on my podcast. And the first response was I had no idea you had a podcast, but the second response was that's pretty cool. So it's just to give you an example of like who we've been all the interview. It's been awesome. And then on top of the topics, you know, patients coming in all the time asking about these different topics.
Dr. Grant Garcia: So, I mean, we've got over 1500 listens in 10 countries. We've had six renowned guests at least. We've had 15 episodes. It's been awesome. So thank you guys.
Will Sanchez: Yeah, definitely. And I [00:03:00] remember when Dr. David Smith reached out or, or his, his peoples, his peeps reached out to us and, you know, we had the conversation like, Hey, this is real.
Will Sanchez: Then what do you think? And he's like, yeah, no, this is legit. And, you know the, the season prior, we saw a couple of guys in the NFL level wearing this Q collar, right. Is, you know, this This design that goes around your neck and for you football fans out there and maybe some soccer. I'm not sure if they're utilizing soccer, but definitely football.
Will Sanchez: You might see this band that kind of goes behind the neck and this is what this cue collar is. It's to mitigate the absorption of slosh. Right. That sloshing that's supposed to be woodpecker around in your brain. And, and Dr. David Smith gave that great example of the woodpecker, right. And how the tongue goes out and wraps around the head and protects it.
Will Sanchez: And I'm probably saying it all wrong. I apologize, Dr. David Smith, but. You are a great guest. It was a great topic and we saw it all season, right? As we wrap up the football season, [00:04:00] we're getting ready for Super Bowl Sunday. We'll get into that a little bit later because you know, we might have to have a pick here or there before the show wraps.
Will Sanchez: So I, if you could see Dr. Garcia holding his
Dr. Grant Garcia: face going, Oh God, what are we doing now? They could just see my face. Before they weren't seeing it.
Will Sanchez: So, yeah, no, just some great guests. Recently Dr. Acevedo and Dr. Bashay the shoulder surgeons we had a really good time with them. They like to keep it light and fun and which makes them fantastic guests.
Will Sanchez: So we really appreciate those guests coming on. Who else stands
Dr. Grant Garcia: out for you, Dr. Garcia? I mean, we had Leah winters, obviously starting the napkin to reality. That was pretty amazing. She was absolutely amazing. All the guests have been awesome. I mean, everyone's different, right? Each person's different.
Dr. Grant Garcia: And the nice thing is it builds in a little flavor. You know, you don't have to hear me talking about all the orthopedic stuff. You get people doing different things. And. What's interesting, I think, is like when we started off the podcast, we had some vision for it and it kind of morphed. I mean like literally [00:05:00] some of these guests came out of nowhere, like we, these weren't planned.
Dr. Grant Garcia: And all these different topics, some of these topics weren't planned either. You know, we have a topic plan. All of a sudden someone reached out to us and we're like, we'll enter like scrap that topic for this week. We're going to do something different. About the, the podcast is like we have our, our main goal is orthopedics, sports medicine, teaching you guys cutting edge techniques and things that are real and happening.
Dr. Grant Garcia: But at the same point we pivot because something's cooler and more interesting that we know the viewers are going to like, but it has to do with the sports medicine world. You know, you see Aaron Rogers, Nick Chubb. Lonzo ball with a cartilage transplant. All these crazy things that people are like, what's the surgery?
Dr. Grant Garcia: I don't know anything about this. I've never heard about it. And all of a sudden, well, they're like, boom, we have something for you. You know, we've been talking about it the whole time, but no one's listening. So now they're listening because it hits the new
Will Sanchez: and it's funny because the two people that you mentioned, right?
Will Sanchez: Aaron Rodgers and Nick Chubb, yeah. Those were really spur of the moment shows because normally we do our show, we kind of plan it out about three weeks, a month, we come up [00:06:00] with a show. We already have the plan, but due to time and, and and really kind of doing what we want to do and being specific about it.
Will Sanchez: But when, you know, the biggest news to start the 2023 season to kick off, right? Monday Night Football, the New York Jets sold out stadium. They come out the lights off, you know, people have their cameras on and Aaron Rogers run now with the American flag. And it's just like, what a way to kick off the season jets fans are going.
Will Sanchez: We're finally gonna win. It's going to happen and three plays in the Achilles rupture and what a story to tell and that's one of the reasons why we love sports, right? Sports is my reality show. I'm not watching the Kardashians. I'm not watching anything like that. My reality TV is sports. So it, you know, that when that happened in Nick Chubb, we jumped on it because we thought it was important to share.
Will Sanchez: I, I remember when I texted you and you were [00:07:00] like,
Dr. Grant Garcia: Oh my God, right. You know, they were all talked about how this is going to be a single surgery. It's going to be so simple. And I'm like, dude, I've done this before. I know that I know we're not going that route. And then all of a sudden, you know, they get in there.
Dr. Grant Garcia: There's more damage than they expected. But again, it's also media hype. You know, we know how this works. It's like, you know, it's fun. I can say whatever they say, but it's also, you know, that they're not talking about the surgeon didn't say that. Like that's what the media wants. Cause they want people to think, oh, there's like this hope.
Dr. Grant Garcia: It's going to be super fast. And he's going to be back in two months. You know, Aaron Rogers is going to lead the jets to the, to the super bowl.
Will Sanchez: Yeah, that was, that was a lot, a lot of hope there, but there was a lot of conversation. It was like, Hey, do you, do you think this actually can happen? And you're like, yeah, now, bro, that's not, that's not happening.
Dr. Grant Garcia: I think it's a valiant effort though, for publicity. So anyhow, so, but we pivot. We pivot. You see us here now we're on video and so you're like, what's going on? Well, I mean, we had a lot of, we had a lot of requests. We had my friends who wanted to talk about the Iron Man. We had different requests from [00:08:00] guests.
Dr. Grant Garcia: Yeah, that was a good one. One request we kept getting is video. And he said, you don't, we don't see you got your funny faces on the video enough. So, and again, for the stuff that we're talking about, you know, the hands, the hand signals you can hear. The voice inflections are important, but people want to watch the video.
Dr. Grant Garcia: And so we listened and I think, you know, from now on, you're going to be seeing video podcasts of sports stock talk. So it's going to be awesome. And not just that same rendition of the logo over and over again. You're going to get to see some, a little bit of freshness. And I mean, we do have a master producer here with Will Sanchez, so I
Will Sanchez: don't know about that.
Will Sanchez: Now, this is all going to get screwed up here. So we'll apologize there. Another great guest guest, Dr. I'm sorry, Dr. Zach Smith, physical therapist, high def P. T. He was Dr. Amazing. The plethora of information that was, that was, he was talking about and the innovative techniques and technologies. And he had the app that Theracentric app.
Will Sanchez: I know I missed [00:09:00] this, a blood flow restriction and how they utilize in that. I'm just sitting there. He was gone. I was like, we're going to go four hours on this show. I mean, he will
Dr. Grant Garcia: doesn't know is my goal. The show is to always get him excited. So I bring on the most exciting things I can. And then I surprise him with something even more exciting.
Dr. Grant Garcia: So by the end, I mean, at this point, he's got his honorary medical degree. I mean, he's had what we had like 40 episodes of this. You're essentially trained once you get that internal brace degree, we're gonna be set.
Will Sanchez: All right. If it was only that easy. Anything else that stands out for you? I know we've Done so many and we could talk about so many different things.
Will Sanchez: And, and I'm, you mentioned Leah winter, right? And that was also, I feel like it was part two of the napkin to reality show that we had that you absolutely love. And I believe it was one of our most listened shows, everything that we're talking about right now, please go back and check out the podcast and our amazing guests, because we're not just.
Will Sanchez: You know, coming up with this, these are [00:10:00] shows that we had and we are definitely not doing justice right now, just with a little quick synopsis here. So please go back and listen to these shows and amazing guests that talk about what they do. But going back to Leah Wintour and that napkin of reality, I mean, tell me about that show and the response that you got from that show.
Dr. Grant Garcia: I mean, a lot of people, obviously Leah was happy to be a part of that, but it's just, you know, the idea of hearing about someone like her with a, you know, again, we talk about big companies, Arthrex. Macy, we're gonna talk about a few more. These are massive companies. This is a single person who with behind the scenes is using other you know, help people to help her along the way and, and doing something great.
Dr. Grant Garcia: I mean, she's on LinkedIn, she's got her own corporation. She flying around the country doing stuff with this. You know, innovative, but simple, but innovative idea and it's impressive. So it was really fun to have someone like that on there and hear the story. And honestly, like you heard before, but the reason she came, one of the reasons that she was so excited about this is she listened to the [00:11:00] napkin reality podcast, and then we had her on to talk about the napkin reality that she has occurred and that she went through.
Dr. Grant Garcia: So it was just full circle. You know, and again, I know we could talk all night about this, but that's obviously, this is just the we're just the taster of the podcast. But again, the website to check it out, www. sports. talk. com. It's got everything on it. And again, we spent a lot of time on this, you know, video podcasts, transcripts, and we know we track everything.
Dr. Grant Garcia: So we know people are watching these. We know people are watching, they like the transcripts, which is great. You know, our averaging about a hundred views a month on just the, on just the website itself. And then what's cool is if you able to link to my website and some of my, a lot of my patients know this, but we've got a ton of surgical videos, pretty much all these fun and interesting surges you hear about, we've got a video on it and it's, it's myself doing it and seeing the technique.
Dr. Grant Garcia: So if you want to see, like, how do you do an ACL repair with internal brace, how you do an MCL repair with internal brace. You know, again, all these things we talk about, all these funky, crazy surgeries, they're on there. [00:12:00] So, you know, visit the website. You can see right there, GrantGarciaMD. com. But again, all the links are built in there.
Dr. Grant Garcia: And if you want to learn a little bit about Will and I too, it's all on there. There's tons of information and people have really enjoyed it. So again, it's just been, we just want to kind of overview everything that's gone on and how it's been. And I'm pretty excited. I think this is going to be even more a more productive year because we just have more, we have more experience now.
Dr. Grant Garcia: So.
Will Sanchez: Yeah, before we started talking about the other topics which is future horizons, right? And, you know, when we talked about this show, we said, okay, this show can be three hours. I mean, there's so much information. So we said, okay, let's kind of, you know, pay our respects to 2023 and all of our great guests and talk a little bit about them.
Will Sanchez: And we'll dibble dabble a little bit on the future horizons. But really, this is a this is a teaser for everyone, because throughout this 2024 year, we're We're going to go back to some of this stuff that we're talking about right now. We're going to go in depth. We'll have other guests coming on and speaking about it.
Will Sanchez: So we're really excited about all of it, but [00:13:00] before we move on, right, we were talking about innovations and technology and the one that cracked me up and I'm laughing right now. So if you're looking at my face, I'm pretty much smiling. And I was like, Dr. Garcia, I'm going to bring it up. He's like, what are you talking about?
Will Sanchez: All right, I'm gonna bring it up. He's like, ah, really? Okay. Yeah, it was the hydration sensors in the Jacksonville Jaguars
Dr. Grant Garcia: You're hoping you weren't gonna bring that
Will Sanchez: up. Yes Where we talk about things that we're talking about and in the stories in the show I was like, you know what I have to bring it up again because That was amazing.
Will Sanchez: You got sensors in your urinals to tell the players if they're not
Dr. Grant Garcia: sure it's the best tech we talked about, but it's definitely the most interesting. And I'm investing. I'm investing. That's my, that's my goal now to get invested in Jacksonville Jaguar urinal hydration sensors. I
Will Sanchez: need one in the house.
Will Sanchez: So I know when I haven't had enough. water. It's going to turn a certain color. It's going to yell at me. It's like, once again, you're not [00:14:00] getting enough water. You're getting dehydrated. Do something about it. It's just, it's just a sensor to shame me into doing what I need to do. So we'll see if there'll be a home product coming soon to everyone anyway.
Dr. Grant Garcia: Awesome. All right. I think we probably should go into the cutting edge. Cause again, like you said, we're going to go brief on this. So you guys have, may have questions. You may hear about this again. This is these topics. I had two people come in today for the, for the asking about these particular innovative surgeries and they did.
Dr. Grant Garcia: I want this. I heard about it on the internet. And so today is a day just to go very briefly through it because this stuff that people do, people have entire presentations on this. So we're going to go briefly kind of see how things went. And we'll go from there.
Will Sanchez: All right. Let's start with this. Misha implant.
Will Sanchez: Am I saying it right? Misha? Misha? Yeah. Misha's
Dr. Grant Garcia: right. Misha's right. Misha, right? Yeah. All right. So this, this is cool. So I'm glad we got the audio. So this looks like, this looks wild. This looks like, you know, [00:15:00] 2, 200 year we're implanting this. But what's, what's really cool about this in the background to this is there's patients that have these, That have that have issues with their arthritis and I see a lot of them.
Dr. Grant Garcia: I saw two people today that were potentially candidates for this and when they come in, they have arthritis and a lot of times the arthritis on the inside of the knee or the medial portion of the knee. And that's the most common one. And a lot of those patients nowadays, if they're in their late forties, fifties, their doctors say, Hey, listen, I don't have any other options for you.
Dr. Grant Garcia: We're going to do a knee replacement. The knee replacement is a partial, but nonetheless, that's not ideal. I mean, if you're 40 to 50 and you have a knee replacement like that, it's not your last. It's going to wear out. And the other issue is that you have restrictions. You know, you got to take antibiotics when you go to the dentist, you have, you have other issues where that can last only a year you're restricted in terms of high impact activities, and so that's really kind of one of the reasons that this came about.
Dr. Grant Garcia: The second reason is, there's a procedure which we have talked about and we are going to [00:16:00] talk about called the high tibial osteotomy, and so this is something that not that many surgeons do, it's kind of a lost art. I do a fair number of these, and what happens is people that have that, that issue with arthritis, they start to fall in.
Dr. Grant Garcia: If they fall too much, then they only can get the osteotomy where we actually straighten their leg out is pretty wild and people do really well from it. You can see on our website testimonials, but the people that are just a little bit or the people that are people that just a little bit, those people may, you know, right now we have the osteotomy or we have a partial knee replacement, but the osteotomy is a big surgery and the knee replacements.
Dr. Grant Garcia: You know, a decent sized surgery. So this option is basically this little spring. It takes away 30 percent of the pressure. It actually acts as a sort of knee brace and we've seen awesome results. Again, there's a lot of European data in there. They have up to seven year data on this. This is the second generation.
Dr. Grant Garcia: I think the hardest part is just getting approval for it, but we're working on it and again, this is, this is a, it's a, it's a pretty easy surgery and pretty easy recovery and the patients are doing great and there's no restrictions. And again, you know, absolutely worst case in this scenario. [00:17:00] We never want to have a, an issue, but you know, removal of it.
Dr. Grant Garcia: If you have to have it done is pretty easy as well. So this is sort of the newest cutting edge thing that's coming out. And this is a really good bridge for patients that want to buy some more time and keep up their activities. And again, Will and I know we're in Seattle, you know, every time you look down the street, there's like 15 people running with each other, you know, biking, climbing, bouldering, it's just nonstop sports.
Dr. Grant Garcia: I mean, I had a patient, two patients today, they're 50s and they're like, you know, I'm really active. I'm like, dude, this is Seattle. I get it, you know, 60 being like, you know, I like to run marathons. I'm like, I get it. I get it. I get it. So yeah, so this, this, we're going to go more into this later. As this hits more mainstream again, this is, this is something that people have really not heard about.
Dr. Grant Garcia: They're getting now I talked to the company, they're getting, I think they're getting over 2000 inquiries a week for it and waiting to find surgeons that are going to be trained in this, that are going to do this. And so we're going to be right there with you telling you kind of our experience, but we're really excited on the pipeline and this is coming really soon.
Dr. Grant Garcia: Really sick ands, FDA approved. Is this [00:18:00] something
Will Sanchez: that you, I I, is this Well, that's great. Is this something that you can utilize, even if you've already had knee surgery and maybe it's not taking, or you're not being supportive, I'm not sure if I'm saying the right words here, but is this something that you can utilize to for lack of better word, kind of go back and fix maybe some of the stuff that didn't work the first time and, and put this in?
Dr. Grant Garcia: Yeah, so this is a good example. The guy that we're doing it on shortly. You know, he had his meniscus cleaned up and people don't see this. They don't realize it. Maybe he had a little bit of that, you know, kind of bowleggedness. But on top of it, the people that the biggest people you worry about is a straight leg.
Dr. Grant Garcia: So they have completely perfect legs. He had his meniscus cleaned up. Didn't do too hot. Six months later or a year later, he comes in now for me to second pinion. And I'm like, what about trying this? He's 50. He wants to run. And so that's really what it is. It just basically takes enough. It's crazy. 30 percent of the pressure gets rid of all that pain.
Dr. Grant Garcia: And that's really what we do with the osteotomies and the braces. It's just that those are more invasive and the braces are hard to wear. So this is that middle ground. And as soon as I heard about [00:19:00] this, I was like, listen, I've got these people. I don't know what to do with them. They don't want an ear placement.
Dr. Grant Garcia: We can't do injections anymore. And boom, we got this. And you keep seeing this. There's all these, these companies are finding niches. And there's a niche for all these things we're going to talk about. And again, like I said, we, we're going to talk about it for two minutes and we're about six minutes in but this is what happens on this show, but I'll stop there.
Dr. Grant Garcia: Learn about it on my website. We'll move on to the
Will Sanchez: NEP talk. All right. Well, I'll hold my my questions when we focus on that topic. Anyway, let's talk about anchors, right? You know, another great guest that we've had, Anthony Yee. You know, I felt like everything that we talked about went around, you know, anchors and the fibulox and the push lock and the, you know, the anchors and I don't know, any lock that you could think of.
Will Sanchez: So this is another lock. Let's let's get into this a little bit here.
Dr. Grant Garcia: All right, so this is pretty cool. So this company is separate from a lot of the companies we talked about and what they did is you can see this anchor. So the [00:20:00] anchor itself is not anything crazy innovative. I mean, this is a this is a very similar copy to a lot of other anchors that are out there.
Dr. Grant Garcia: But what the issue is, is the materials it's made out of. And that's the game changer. So the way it is, is we have three main type of anchors. implants. The first one is the biocomposite. So those are the ones that turn into bone, but they're super soft. And so they can crack sometimes, especially in hard legs or hard bone.
Dr. Grant Garcia: And those are the ones that people, patients want those because they turn into bone, but they're not very useful in a lot of different cases. I use them in the shoulder more, but in the knee because the leg is bones are so much stronger that can actually crack them. And so we don't use those devices as often.
Dr. Grant Garcia: Then you have peak, which is a plastic. That's what I use a lot of. So those are invisible to MRI, but they're inert, so they don't go away. And so patients don't like that. It doesn't go away. They want it to go away. But the issue you have is you have to have a harder anchor because you don't want it to break during the surgery or your surgery won't work.
Dr. Grant Garcia: And then the third step, [00:21:00] Well, everyone knows is the metal, trust me, one of the reasons that I get some of my patients come to me just because I don't use metal in certain cases. And so can we get an anchor that has the properties of metal or peak but turn into a biocomposite? Well, these guys figured it out.
Dr. Grant Garcia: And the first time I put one of these in. I like freaked out because I was like, this is awesome. I'm putting it in. And instead of the normal crack, crack, crack, which I've used plenty of companies before, this went straight through and it was, it's stronger than the plastic, but is biocomposite. So it turns into bone and it doesn't.
Dr. Grant Garcia: Some of these biocomposites also, they're so soft, they actually turn into cysts. So they're not exactly doing what you tell them they're going to do. And so this product material they've designed and found a way that it turned. And actually, they're actually competing with metal now. So it's amazing to imagine like a bone material that's as strong as metal.
Dr. Grant Garcia: And so the future and this is a lot of foot and ankle and they're now working towards they're doing some sports medicine and I use these in the [00:22:00] surgeries.
Will Sanchez: And you said and you like to use them in the shoulder area, right? Because you mentioned the foot and ankle, but you're also using no. So I like to use them.
Dr. Grant Garcia: The shoulder, it's not as, it's not as concerning in terms of the strength, but the, the, the knee is a problem. So my knee anchors break a lot of times if they're soft, and so that's why I use almost exclusively the plastic anchors and I don't use biocomposite. And my patients are like, why don't you use biocomposite?
Dr. Grant Garcia: I'm like, they're softer, they break. Well, these don't. And so I use these now more frequently because they don't break, but they turn into bone. And so that's really the winner. The future is like everything that we use to fix bone with, like my tubercle osteotomies, or we use metal to fix with. They're coming out potentially with some screws that are, but the only weird thing with the screws is they're invisible.
Dr. Grant Garcia: So when you do them, What do you mean invisible? They're invisible on x ray. So they look cool to me when I'm putting them in, but when you get an x ray, it looks like nothing's there. Because they're completely invisible. And so there's some strategies they're doing. And then the next step is to make these [00:23:00] bigger, right?
Dr. Grant Garcia: Because when we fix an ACL, we fix them with big screws, you know, like. Nine, 10 millimeter screws and they can right now they only have up to like five millimeter. So they're not there yet with their sports line. But this is once those things happen, which I'm expecting in the next year, this is going to explode.
Dr. Grant Garcia: And it's, this is the next generation of anchors. I think everyone's going to be competing for this material. And again, I, I was, it took me a little bit to believe in it. And when I tried it for the first time, I was really impressed. So yeah. You know, we'll see where they go. But you know, this is pretty cool and we definitely have to have an update on this in the near future.
Will Sanchez: Yeah. Do you feel like there'll be a jump even within a year or so that you know, as far as them having maybe something bigger, stronger that you can utilize for other parts of the body that you feel that needs, you know, more
Dr. Grant Garcia: support? Yeah. I mean, the biggest thing here is people just, it's just conversion.
Dr. Grant Garcia: It's like you're, it's a dogma is that if you have a screw, it should be metal. Right. Because that's strongest. And like, we don't, the last thing I want to do is put [00:24:00] one of these in and have it break off at like two days. And then my surgery failed. Like, right. Like I talk about all these cool innovations on this podcast, but if, if, if my innovation fails right away, that's a failure of myself.
Dr. Grant Garcia: Like I feel badly. And obviously that's terrible for the patient. I'm very fortunate that I spend. Lots of time preparing and thinking about this and being like, listen, like I'm talking the company. I'm like, I'm not using your screws until I know for sure that they're not going to break off. And if I do it, maybe I do one of these and two of the metals.
Dr. Grant Garcia: And so I'm like, Oh, this didn't break. Okay, now two of them at two of these and one of the metals. So I'm trying to if I'm integrating this and it's slowly. But obviously faster than still a lot of people do because, you know, we just, we did the first in the state of one of these anchors in the miniscule route, just, you know, four months ago or something like that.
Dr. Grant Garcia: So, you know, it's not, this is coming quickly and it's innovating quickly.
Will Sanchez: I got a quick question. I apologize, but we said we were gonna do this for two minutes, but here we are. Do they tell you what the torque is for lack of a better word is like, you know, there's a pound per pressure [00:25:00] per millimeter of screw going into this type of tissue or bone.
Will Sanchez: This is your kind of your, your sweet spot. Anything more than this is going to
Dr. Grant Garcia: fail. So The answer is sort of, but really it's also like a test, you know, we're doing it in the surgery and they're like, they're like, okay, well, don't tap it this time. You know, you tap screws. They're like, don't tap it this time.
Dr. Grant Garcia: Let's see if it breaks or not. So we're doing it. And I'm like, this isn't breaking. It's making a lot of noise, but it's not breaking. You put a screw in, it's really tight squeaking. Yes. That's what happened with this one. And I told, I looked over the rep and I said, yeah, If this doesn't break, I'm going to buy lunch.
Dr. Grant Garcia: I was like, this is crazy and it made it the whole way and it didn't break. I was shocked. So I had to buy lunch, obviously. But the but you know what? This is again, this all safe environment. We're not you again. This anchor breaks. You can easily pull it out. And the nice thing too about these is if the anchor does break, you can just drill it right out because it's just.
Dr. Grant Garcia: This material at time zero, you can actually get rid of you if you have a metal anchor break in [00:26:00] there. It's a big problem, right? You can't get it out. So that's what's cool about this. You can reuse that hole over again. It's just this is another topic. Like we said, we're ready. We're already past our timeline.
Dr. Grant Garcia: We should have a counter on here for me and it should beep at me and tell me I got to get it move on.
Will Sanchez: Well, I should stop asking you stuff also. So we'll just move on. All right, let's, let's talk about this. This implant here, which I was like, what is this thumbnail? When I first saw it, I got
Dr. Grant Garcia: around. So the thumbnail, so the thing here, you can see, so this is for, we're, we're switching topics.
Dr. Grant Garcia: So we just talked about knee knee. Now we're on the shoulder. Yeah. So again, the key here is cutting edge. So when we put in a shoulder replacement right now, we put in a shoulder replacement, we put a metal ball. And we put a plastic socket. Okay. Sometimes we don't do that, but most of the time that's what we do.
Dr. Grant Garcia: The problem you have is there's a lot of crazy weightlifter guys or guys that had surgery because they had lots of dislocations or whatever. And so I get these like. 40 year olds to early 50 year olds coming in there like I need my shoulder place. [00:27:00] Everything again is restorative. How do we prolong the person's shoulder and avoid needing a replacement just like the Misha or other things?
Dr. Grant Garcia: Well, in a shoulder arthritis, it's really hard to prolong it too long. So how do we have implants that last longer? So this is really cool. And I actually got to see the guys in France. Are a part of this team that designed this. And this has been out for a little while in Europe, but we just got this FDA approved in the United States a few years ago.
Dr. Grant Garcia: So it's a pyro carbon. So it's a way softer metal. It's actually pretty funny. So when you normally put one of these metal ones in, you know, you're hit it decently hard to get it in with this one. It's got like a doink, doink, doink, like a, like a pinball machine. Cause it's so soft, the metal that you can actually damage the metal when you hit it in.
Dr. Grant Garcia: So it's got its own special thing, but what's cool about this. And you can see here, there's a little reversion of technology and for FDA approval. So normally we do this actually without a stem. But with these type of implant, you can't do that yet. That's not fully FDA approved, but hopefully soon.
Dr. Grant Garcia: So we usually, we do our normally stemless shoulder replacements with a socket. So what the cool part [00:28:00] about this is, is you don't put the socket on, the plastic part, and you just have this soft metal, and it's made for patients and they're like, Late thirties forties to early fifties and they've found that the where properties are very low.
Dr. Grant Garcia: So these patients who normally would go on and have like really bad problems after like five or ten years because Trust me, none of these 35, 40 year olds, once you make them feel better with their shoulder replacement, they go crazy with the lifting. You can imagine like Jim, I mean, I'm 38 and if I had to get a shoulder place, I can tell you right now, I don't know if I would listen and I'd probably be doing all my weights still.
Dr. Grant Garcia: And so these are, you know, I get these mentality, these guys, so I have to protect myself when I do these. And so this way you don't do the socket replacement because one of the number one reasons for Having a failure of a shoulder replacement is that you wear out the socket and these active like kind of crazy athlete mostly are men.
Dr. Grant Garcia: I'll be honest. The women listen, which is good. The men are the ones that don't follow the rules as we know. So they you know, they can wear out that socket a lot faster. So you don't. Replace [00:29:00] the socket. And if you have a softer metal, it doesn't wear down whatever's left over. So imagine like a it's like a softer tire on the on the road.
Dr. Grant Garcia: So you just have less damage, but it's just as strong.
Will Sanchez: You mentioned the age. Is there a certain age where you wouldn't utilize this? This polycarbon? Yeah, because
Dr. Grant Garcia: you're not, it's not FDA approved to put the socket in. So a lot of people have like really bad sockets by the time they're in their 60s.
Dr. Grant Garcia: And so if you have a really bad socket, it's imagine like imagine like a P a ground in the putting green, but there's like a hole in it. So the putty, the ball will never go through that. Does that make sense? Yeah,
Will Sanchez: there's already been significant amount of wear and tear in the shoulder. Yeah. At this point, that's, it's not going to be, you know, at that point, if you're doing that repair, you're doing, you're utilizing something else.
Will Sanchez: You're not using, utilizing this. So this is more for younger
Dr. Grant Garcia: patients. Yeah. And if you get into your mid sixties, then I do a good shoulder replacement on you with a regular metal and a plastic piece. It might never need [00:30:00] anything else again. So, I mean, I've done tons of these and I, my patients haven't come back and been like, I'm loose and I'm have a problem, you know, most of them do really well.
Dr. Grant Garcia: So if you balance it well, we, again, you can always hear my voice and you can see this. What are we missing currently on the market? And this is what they figured out. They found a way to fill that niche. That niche was, what do you do for the patient that's 35 that comes in, who can't lift his arm because he has so much arthritis?
Dr. Grant Garcia: That's a bad problem. Those guys usually see like six surgeons. You know, I'm usually one of those guys they're seeing. They're like, listen, how do you fix me? And everyone's like, dude, I don't want, this is, this is not a good scenario. And so now we have this option. I think 35 is a little bit too young for this situation even, but maybe when that those 40 year old patients that we initially were saying, let's just pray and do a regular shoulder replacement, we're not doing that now.
Dr. Grant Garcia: And we have this option. So it's so cool and I'm excited for the patients that have the opportunity to have this because I think this is we're going to see in the next 10 years. These patients really were saved and we bought them more time. My office is half time. I'm going to buy you more time. That's what I [00:31:00] need.
Will Sanchez: That's perfect. I mean, I think I'm getting to the age now where I don't think that's going to apply to me, but for all the young folks out there and then hopefully with, we're always talking about innovation and technology, hopefully it'll be something along the lines for someone as we get older and, and even better, hopefully I won't even need a shoulder surgery because I've had enough surgeries already.
Will Sanchez: I'm kind of done with that. I need a break.
Dr. Grant Garcia: Well, it's interesting. You know, before we jump on this, I had a patient that came in and she needed something and she said, have I, did I wait long enough for the next thing? And I was like, you made it. I was like, you finally made it. You know, she was trying to, she actually, I think she was coming in for the, the Misha and she was asking, you know, like I told, you know, 10 years ago, I need an ear placement and I held out, I held out or the coming for the shoulder.
Dr. Grant Garcia: You've talked about that lower trapezius and they're like, you know, they told me no one can fix me. Yeah. And I need a shoulder replacement, but they're 55 and I'm like, well, we finally have it. So there is. There is this, this lag that actually is important, but it's also finding the right people, right?
Dr. Grant Garcia: Like [00:32:00] some people go, they might go, they might call their surgeon tomorrow and be like, I want the Misha. And he's going to be like, dude, I don't know what you're talking about. Like, what is this thing? Pyrocarbon? Like, get out of here. Osteofiber? I got none of
Will Sanchez: those things. We don't. Well, I got this episode of sports doc talk.
Will Sanchez: So why don't we play this for you? Yeah, that's going to go really well in the office. You're going to get a phone call like can I speak to Dr. Garcia here? Can you please not talk about stuff like this? No, not at all. All right, let's, let's move on. Let's talk about this from this new clip techniques here.
Will Sanchez: Yes. So
Dr. Grant Garcia: this is one of the two companies. There's this one in called body cat as well. So this is so cool. So, you know, and again, Will likes this full circle. So those people that are eligible for the Misha implant, but people that have more of this bowleggedness. Yeah, they need to have certain, we need to straighten them out.
Dr. Grant Garcia: And so what we used to do is, and again, I still can do a lot of this. Like, you know, it's like, imagine like, imagine I build like an entire structure of Legos without ever seeing the [00:33:00] instructions. That does pretty well. But imagine you at, you give me a really good instructions and I do it exactly as planned.
Dr. Grant Garcia: It's gonna be perfect every time. Right. So what this is, is actually we get a CT scan of the person's, and again, most of the ones, you did a lot of different implants here, but the ones we're talking about mainly are on the right side. Those two that the femur and the tibia. You can see I, I
Will Sanchez: grabbed all the pictures I could get, you know, I got You did.
Will Sanchez: And, and I, I love it too. 'cause it's like red and black and they add this whole
Dr. Grant Garcia: kind of, some of this has nothing to do with this, which is great. I love it. Yeah. This is perfect . So, so. We straighten them out. We use these plates to straighten out their legs and we can save people like I mean, I've done I last this week.
Dr. Grant Garcia: I've done three of these. They were 35, 40, 35 years old, 49 and 24. And all these people had problems where they needed. They were told they needed knee replacements. So we do this to straighten out their leg to buy them more time. But then there's some fancier stuff, which we're not going to go into too much today.
Dr. Grant Garcia: But you know, one of the girls I did, she had her A. C. Heard in, actually dogs have this [00:34:00] when they have a slope. So like there's slopes like this. Imagine your knee just keeps sliding forward, right? It just too much slope. So what I do is with this and with this surgery, I'm able to 3D model the entire knee and then they as engineers and we calculate where the cut's gonna go.
Dr. Grant Garcia: And it's literally like the most amazing puzzle you've ever done. And it tells me where to cut, how much to take off. And it's like, you know, like you like your torque numbers. I mean, this is four, I do nine degrees, three on the right, two on the left. And I can calculate all this stuff. And I'm on the Google with that got Canadian grump company.
Dr. Grant Garcia: And I'm saying, Hey, take off one more on this side. And they're showing me all this. And then they send me this printout now on this case. We didn't have this technology at that day, but a lot of times when we have it, I send, I think it can be a 3d model where it's printed cut guides and you cut it and you literally can follow the paint by numbers.
Dr. Grant Garcia: Now, again, there's still a lot of nuances to this, so this isn't as easy as I'm making it sound, but it gives when you already know what you're doing, it makes you that much better. And if you [00:35:00] don't, and if you're learning, it's a lot safer. So it's actually better for both levels. So there's people who do 10 to 15 a year or more, which is what I do.
Dr. Grant Garcia: And there's people that are just getting out of fellowship and they're doing one or two of these a year, maybe, or they're really nervous because they've never done one of these in practice. And this technology makes it so that that person gets the same quality as a 15 or 20 surgeon. And which is really important because again, everybody is.
Dr. Grant Garcia: In their early stages of learning, and we want to make sure everybody gets a good, like the same parameters, because when you mess, if you mess something up, it is a big problem. If you don't do these correctly, there can be issues. So this, this technology is awesome. And this 3D planning, we've talked about this before.
Dr. Grant Garcia: This is a repeated process. Innovation line custom everything for patients. It does much better.
Will Sanchez: So what do you need to do? You have the situation with the patient, right? How are we going to repair this? Right? And you're this is for, you know, getting 2D and [00:36:00] 3D planning for this procedure. What measurements?
Will Sanchez: What do you have to take? Just kind of give me a really simple overview so we don't get into minutia of it and go three hours on it. But. Are you taking measurements? Are you send this out to the company? Now they're taking your measurements, creating this 2D, 3D, and then they're shipping it back to you.
Will Sanchez: So what do you send them? How long does it take in order for you to make these plans for the surgery?
Dr. Grant Garcia: So measurements two types of measurements, x rays and CT scans. So x rays, I do those all in the office. Like the one I did today, I did it in about 30 seconds. So I can do all the measurements and calculations.
Dr. Grant Garcia: The CT scan takes once you get it done, two weeks to get to the company. They process it with their engineers about, you know, 20 minutes for the meeting and then two months, two to three weeks to print it. They all use the 3d printers. So six week turnaround ish, sometimes even faster. So again, that's pretty normal.
Dr. Grant Garcia: So we usually plan six to eight weeks for our surgeries [00:37:00] for the most part, especially on the complicated ones. And I just tell the patients, you know, if we somehow can sneak them in earlier, I'm like, it's not worth it. Like, you want to get the custom one if needed again, a lot of times I don't need this, but when you're like, when there's tougher cases, and again, like I said before, I'm taking care of people with three or four failed ACLs, terrible alignment, really wacky, unusual injuries that are really uncommon.
Dr. Grant Garcia: Like that's when you got to step in and use this stuff. And so for me to have these tools at my disposal. It's awesome. And then we have, we can talk a whole other story about this. Yeah,
Will Sanchez: I'll wrap it up, but you know, I'm not going to wrap it up. So what's the communication process once they have that information?
Will Sanchez: Do they go back and forth with you a few times? Is there something that they can make sure before you receive this, that they can compare it to you? Yeah. What, what, is there anything like that before they just ship it out to you and you open up the box and say, okay, I got a new toy and we're going to fix this.
Will Sanchez: And here we go. Yeah.
Dr. Grant Garcia: Well, they all know that I'm pretty OCD. So I almost always fix something that [00:38:00] they did. And I'm watching every number. So, so many times, usually it's a quick call. It depends on the situation, but it's really complicated. Like I said before, like I had this big surgery I did on last Wednesday.
Dr. Grant Garcia: It was that that was one of these really complex ones. So on Tuesday I got on the phone with Canada. For 15 minutes on a Google drive between case on Google. Whatever the zoom, the Google device call is, and I talked to them for 15 minutes and I was like, titrate this up this and again, we were just planning and trying out the software so they can do that pretty quickly.
Dr. Grant Garcia: And then I'm like, send me the approval. They sent it to me that night. And then I, I emailed them back the next morning being like, we're good to go. So it's actually pretty quick and they've gotten it. So they've gotten really, really fast at doing this. So. I think this will be a great topic for a major topic is I want it.
Dr. Grant Garcia: I can throw up one of the plans and show on the video podcast like how I do it. And that would be awesome because like I do this for this for shoulder placements. We do custom ones. We've had some awesome results so I can do episodes on 3D planning so people can see how we do it because I think [00:39:00] people would love that because everyone always asked me like how do you do it?
Dr. Grant Garcia: But I've you know, I don't have time in the office to go through one of these. I mean, I usually torture them with all this information, but nonetheless, You know, it's good for us to see how we do it. So that's a great idea. So we'll do this as one of our new technology episodes. This
Will Sanchez: is the way this is kind of the way my wife tells me to move on as well.
Will Sanchez: She kind of gets, she compliments the situation and then kind of pushes me in a direction. That's what Dr. Garcia is doing right now. It's like, yeah, let's say this for another time. This is great. I love it, but let's move on. So let's move on. We've got some goodies here, Dr. Garcia, let's let's talk about this bear implant.
Will Sanchez: And it's something that we talked about in 2023, but as we constantly know that technology is changing. So why don't you give us an update on this?
Dr. Grant Garcia: Yeah. So I'm going to be brief on this because I've had like four requests for separate podcasts and I've already just did one with Cairo. So we're going to, that'll be posted soon so they can hear the whole details.
Dr. Grant Garcia: But basically, you know, the update on this is it's doing well. It's the, [00:40:00] the, what we do is instead of taking away the ACL and doing a reconstruction, we can repair it. So you can see here we're repairing the ACL and then there's just this collagen implant that's. That you put in the knee, and this is a really dumbed down version, this is actually not the technique that most of us use now, but this is the technique from the website, and actually it's on my website, and you can watch my videos on how we, how the newer stuff we're doing, but basically you shuttle this implant in with the tear.
Dr. Grant Garcia: And again, you can see the tears of the femur side, which is more important. So you repair the ACL back, and then you have this clot, and the clot allows it to heal. And what we've seen is, again, re tear rates equivalent to ACL reconstructions. You know, again, we're still, I, I'm still, the data is still out whether it's the same, but there's been some decent, the newer data is looking pretty good.
Dr. Grant Garcia: The patients ACLs feel really good. So they actually feel like they're healed and they're back to sports. I mean, has had a patient on a video testimonial. She's back to skiing after one of these and we saved her ACL. So the right patient, right timing. [00:41:00] All this stuff is really important for it. Listen to our previous podcast on it.
Dr. Grant Garcia: You're gonna learn a lot. But again, this is. This is probably one of the biggest innovations in surgery we've had and definitely of all the things I talked to you about, it's the most common it's the most advertised, most marketed. It's one of the hottest topics. Like everybody wants to talk about the bear ACL.
Dr. Grant Garcia: And honestly, it's working. I mean, there's definitely downfalls of it. You get a little bit stiffer. There's some other little things here or there, which we can go into in the main, if we want to do another episode on it, which you probably will. But for some new technology to have that few setbacks is pretty impressive.
Dr. Grant Garcia: And congratulations to the company, but honestly, congratulations to Martha Murray. She's the doctor that invented it because they just, they just rolled with it. And she's the, really the one that came up with the idea. So Martha, shout
Will Sanchez: out to Martha Murray. Thank you, Martha. So we all want to there.
Will Sanchez: All right, let's move on here because like you said, we'll be talking about that bear. in 2024 and we've already discussed in 2023. So if you need more information please check out our [00:42:00] episodes and check out grantgarciamd. com. So there's a lot of information. All right. We've got the tight rope.
Will Sanchez: We're not just walking the tight rope, but talk about this tight rope here.
Dr. Grant Garcia: I'm obviously I lecture for this with the company. So all that is disclosure. But this is probably one of my favorite innovations. And why? Because the bear is sexy, right? There's lots of marketing of it. This doesn't have a name.
Dr. Grant Garcia: And so that's the problem that like people don't haven't heard about the second repair. So this is repair is where we repair it back as well. We don't have to add any special collagen, but this new, this technique you can see here with the button is the reason I started doing these. And I started them about a year and a half ago.
Dr. Grant Garcia: We started doing this before ACL repairs didn't do that great. And now we're at the situation where we have this tensioning device and the biomechanics of it are incredible. And you can see Will's favorite devices right through the middle of that's called the internal brace.
Will Sanchez: Oh yeah, baby. I was smiling.
Will Sanchez: I will tell you, you can see I was smiling, right? I was like, yeah, I know this. I know this [00:43:00] technique.
Dr. Grant Garcia: So I will tell you this. I have been shocked with my results. It has been awesome. I mean, I've indicated probably six people for it in the last few weeks. This, they get back faster, which is really difference between, you know, the bare ACL is really sexy patients do well.
Dr. Grant Garcia: But it's the same timeline, and so it's 9 10 months. So people have trouble. It's hard to sell a new product when you don't get any better other than saving your ACL. And that's kind of a hard sell when I sell this product. And I try to be careful because I make sure it's someone that's definitely gonna do well.
Dr. Grant Garcia: It's 100 percent of people want it like everybody wants this. And so I'm really careful. I mean, I had a guy last week or two weeks ago came in from the podcast. He's like, I want the tightrope ACL repair. I was like, okay, well, shut out. Do you do you do you know what that is? And so I was like, let me explain it to you and see if you're a candidate first.
Dr. Grant Garcia: But he was very adamant about it. So anyway, so he's going to get it and he actually was a candidate, which was awesome. But basically we do is repair it and the patients came back in five months and again, Okay. You know, I had a guy that I got a guy [00:44:00] that's now six months out. He came in with from the podcast.
Dr. Grant Garcia: Another one he wanted. He came in. He only wanted that done. I did it. He's back to everything. And he was so happy, even found the podcast cause he hadn't heard about it. And we have this, keep having this. I mean, I've done, I did one of the, I did one of the doctors that works at Pro Alliance. That was not an easy sell because the other orthopedic surgeons in her group were going to probably thought I was crazy doing a repair.
Dr. Grant Garcia: And she ended up getting back to everything she wants to do. You know, I did a guy that works that, that the beach club that I'm members of, that was a really risky one because if he didn't do well, all the people in the club are going to find out. So it turns out
Will Sanchez: that they were going to take a membership away.
Dr. Grant Garcia: Well, and, and he, and he's an, he's a nice guy, but he's very chatty. And so as a result, this was a really risky move. I should have probably thought about it better. So I did it. It did awesome. He was back in five months. So you want to hear what happened? Will everyone kept. Everyone kept getting mad because they wish they had had that surgery done and they were mad that didn't go to me and have the surgery done.
Dr. Grant Garcia: I'm like, listen, that's not for everybody. So of course it was like bad [00:45:00] advertisement because all the patients, like someone who had, who had, who knew me, but didn't want to do me to go with me because it was her friend or whatever wasn't offered an ACL repair. And so they ended up getting the reconstruction and they're ticked.
Dr. Grant Garcia: So they're coming up to me being like, why didn't you tell me about this? And I'm like, dude, I'm not even, I didn't even know your toy or ACL. You know, and getting that at the, at the club. So it was it was a good and bad thing. But it's been pretty cool.
Will Sanchez: I tell all my friends, man, did they get hurt?
Will Sanchez: Something like that was like, Hey, let me know. Let, let me know. We, we, at this point we have a plethora of talented people in our basket. And it just, you know, when I, when I ruptured my Achilles, you know, we. You probably heard in another podcast. And I joke around, my first phone call was not to my wife.
Will Sanchez: It was Dr. Garcia on the treadmill on Thanksgiving morning going, Oh shit. Let me pick this up. This fool doesn't call me normally like this. And sure enough. And he was like, and then I called my wife, but she was like, I was, she was like, are you going to hospital? I was like, Nope. I already called Garrett Garcia.
Will Sanchez: It makes no [00:46:00] sense to go to the hospital. I know exactly what I'm doing. I just got to hold tight. Eat some you know, eat some Thanksgiving dinner, watch some football, be pissed off, and then get in for surgery the following week. So, you know, if, if you've got a friend in me. And you've got some issues, reach out to your peoples because they know what they're doing.
Dr. Grant Garcia: Still, that's still going to be one of the best stories. We're going to have to do that every year, talk about your Achilles. And I don't even, I don't usually stop the treadmill for somebody. But when Will calls, I was like, something's wrong. I was like, no one calls me on Thanksgiving. And then all of a sudden it's like, boom.
Dr. Grant Garcia: And you know what, we, we got your surgeon on the phone pretty quickly to end up fixing you. Yeah. Yeah.
Will Sanchez: Spoke to him and Dr. Yi, Dr. Anthony Yi. And I was like it's okay. I'm not going to play NFL football, but we've talked about the speed bridge. And, you know, this is something that we're going to do.
Will Sanchez: And obviously there's different ways to tackle these Achilles ruptures. You know, you can throw a cast on it and immobilize it. And, you know, [00:47:00] that's one route. And I was like, no, I, I think I want something a little bit more sturdy. So this is the route I chose to go. The incision is tiny. You can't even imagine.
Will Sanchez: I've got a tiny incision in my calf and then two at the bottom of my heel. And you wouldn't even realize that, you know, you had sutures and pulling in and anchoring it down. And it's just. Absolutely amazing. I'm sidetracked right now because we started talking about it, but it's absolutely amazing. You look at my leg and I can imagine even six months or a year from now, you'll be lucky to see a scar.
Will Sanchez: My scabs off, everything is healing. There's no way if I've got a sneaker on, you're not going to see the seal decisions in the heel and you'll barely see it on my calf. It's, it's absolutely amazing. Anyway, I digress. I hijacked the show.
Dr. Grant Garcia: My bad. No, it's good. It's good. But you know what I did? I did call Dr.
Dr. Grant Garcia: Yi on, [00:48:00] I did call Anthony on Thanksgiving too. And I said, you don't have a choice. You're fixing Will on Monday. So it was it was, I had to get a little aggressive, but he's my man. So he's not, it's not the first time.
Will Sanchez: He's great people. And we have another friend, Now, now we're going down to deep end. We have another friend, shout out to Dory that she's come to see Dr.
Will Sanchez: Garcia and she's seeing Dr. Ye. He's helped her to recover. She's finally out of her boot because she had broken her ankle. She went somewhere else. I was, and then she was like, And I'm going for a second opinion. I was like, why don't you tell me? I was like, Dr. Yee. And then sure enough, she goes, Dr.
Will Sanchez: Yee, sure enough. She's, she's better now. Things are working. And then she told me, and I swear, this is a true story. She says what are they doing over there at orthopedic specialists of Seattle there? Do they just hire. All good looking. Oh my god. I was like, Dory, Dory, park yourself, but she's great.
Will Sanchez: I love Dory. She's so funny. She's, you know, she's, she's a teacher and she's a tennis [00:49:00] coach and she has great humor, but she was like, what is the criteria besides having talent? Do they just hire attractive doctors there? I was like, it may be, but it just works out that way. So shout out to
Dr. Grant Garcia: meet all of them yet.
Dr. Grant Garcia: So,
Will Sanchez: well, hopefully she doesn't break anything else. Anyway, we talked about the ACL and you've done this surgery at this point. And then for us, the next step, which this is our segue here is into the Rebless and using this type of device. Talk about the Rebless.
Dr. Grant Garcia: So I think this is kind of the grand finale final thing.
Dr. Grant Garcia: So we've had a lot of topics we've talked about again. You've shared some really good updates. This one spent about a year and a half. We've had it. It's been awesome. You know, this is really this is my post operative complex knee device. You know, I probably did seven complex knees this month. And all those people are going to get this and we've got a new system in place, which we'll talk about at some point where we can get this to your patients.
Dr. Grant Garcia: We deliver it to the [00:50:00] house and we're able to use it. But the reason it's so great is it works on passive bending, which is kind of the older version. You maybe have heard about these machines. People used to sit in. They kind of bent their knee back and forth, back and forth. And that's they've had those for years.
Dr. Grant Garcia: This one's portable. It can be programmed. It's got remote technology. So the company I work with the company actually that helps with this. So I help advise them on what to do and how to get it better, which is pretty cool. And on top of that, it can do active assist, which that's really the game changer.
Dr. Grant Garcia: It does PT for you. So it does active, which means instead of you passively bending your knee back and forth, actively, it will actually help you up and help you down if you're weak. And the best part about this is the third piece of it, it does, it does resistance. So it's actually like a weight machine.
Dr. Grant Garcia: And I've done this on level 10. And it is awesome. You know, and this will work for the knee. We have ankle. You can see here, elbow and wrist. And this is the older version, which we again, older year and a half old will knows that on our show. Things are old when they're over a year. So, you know, now we're on [00:51:00] to.
Dr. Grant Garcia: The new company is designing something again. I can't say much more than that, but it's going to be a little more innovative than this using the same technology. So, you know, this is this is really great for my patients and we're really lucky. You know, in Washington state, we're one of the few people that can get this right now because again, these are startups and patients have loved it again.
Dr. Grant Garcia: New technology cutting edge. I think the problem we have almost in our practice at OSS As you've seen, it's just there's so much technology patients are just like overwhelmed, right? They come in there like my knee hurts and all of a sudden they like leave being like I might need to have like I don't even told me they could fix it and now you're talking about alignment and this rebless and You're not even gonna go into the nice machine, but you know, that thing is that thing is rocking too We got to talk about that at some point.
Will Sanchez: Oh, yeah, I'm using I'm still utilizing the the nice machine It's absolutely amazing I don't even know, except for me draining it one time. I don't even know if I filled it up with [00:52:00] water more than the one time and then drink. It's absolutely amazing. This thing wraps around is wrapping around my ankle.
Will Sanchez: It's pumping this cold into it. I time it. I could put the compression. I could put how cold it is from scale of one to five. There's some straps so I can get, I can really kind of focus on certain areas. And that's just the ankle. They have all these other parts that you can utilize depending. And it's just plugs in.
Will Sanchez: I have a little chair. I have a little recliner recline. I grabbed my remote control. I wrap it over my ankle. I turn it on, I program it. And it's, I'm not running for ice. I'm not running out of ice cubes. I'm not dealing with any of that stuff, especially since I was in mobile, luckily, and now I'm moving around, but being a mobile and having that.
Will Sanchez: That nice And I feel like it's like, it's like an 80s term is nice, this nice machine that you can utilize and and it was just so [00:53:00] convenient and I, I used it so much, especially the first two months of this rehab and I, I can't, I can't say enough good things about this machine.
Dr. Grant Garcia: Yeah. So we won't go too much details, but Will is probably one of the first in the state to get this.
Dr. Grant Garcia: I trialed it. With the company and I was like, we got it. We got to have this for our patients. So we'll got it. He loved it to signed up to get it for more patients is definitely looking ahead. And now patients are getting exclusively. So they're getting our practice. It's awesome. So all my knees get it.
Dr. Grant Garcia: My shoulders get it. Dr. Weil just signed up. He's going to start using it for hand stuff, which is crazy. There's no machine out there like that. So we can have little mitts for the hand, little mitts for the wrist. Oh, check out his podcast too. He did an awesome job. Ankle, Dr. Yi's signing up too, doing it soon.
Dr. Grant Garcia: So we have the opportunities to do this and more to come. You know, we're going to be working with the company to get the word out because this was designed by professional athletes for professional athletes. And we're giving that same care to our patients. And again, this is not. You know, [00:54:00] you've seen the technology far and superior.
Dr. Grant Garcia: I mean, I've had surgery. I had to use the ice man. It's not very good. Like my wife was like, my wife was like, if you get surgery again, I'm never using the ice man. And so as soon as, and she's like, I'm never doing it for you again. Cause she was tired of filling up the ice. It's a lot of work. You can't get it up and go.
Dr. Grant Garcia: So when she saw this nice machine, I showed it to her and I was like, what do you think? She's like, first off, it just takes my white when she gives me a thumbs up. I'm like, I'm all good. Like, I'm happy. So no,
Will Sanchez: we're going to, no, no, we passed that. We can forget about it. We're at that point. We're going to wrap it up.
Will Sanchez: And you know, and that was our segue to looking ahead. That's one of the shows that we're going to have in 2024. I'm talking about this type of technology because we are yeah. We definitely want to always talk about innovation technology along with the things that are out there, but things that are coming which provides information and gives patients hope, right?
Will Sanchez: Because Dr Garcia is here to provide this information. I'm here to ask questions and [00:55:00] also to make sure that we're, we're really focusing on. Our listening group, and usually our listening group are patients or potential patients. And as Dr. Garcia always says, Hey, you don't have to come here. You don't have to always get a second opinion, but have the information, right?
Will Sanchez: You can't have enough information so you can ask questions, whoever you decide to go to. And that's what we want to provide. So, you know, looking ahead, we have, we're going to have some great guests. We're going to have some great topics. And more importantly, we want to say thank you. I mean, Dr. Garcia, you know.
Will Sanchez: All of our listeners, you know, family, friends, loved ones, people that just walked in saying, I've heard the podcast and I want, you know, I want this, which is great. So at least more information, we just want to thank you. We're trying to have a good time with this and provide, things that we think will benefit everyone.
Will Sanchez: Dr. Garcia.
Dr. Grant Garcia: Yeah. I mean, I second that. I mean, I want to thank all the listeners. I know there's a lot of [00:56:00] patients. There's a lot of potential patients, also a lot of doctors and orthopedic surgeons and reps that are on this that listen, but really the patients and again, not even the ones that come to see me, the ones that just hear about it and they go to their doctor and the doctor goes, that's a really good idea.
Dr. Grant Garcia: I should do that. I mean, that's if I, if I had no patients from the podcast, yeah. And I just heard from periphery that someone heard that and they went and did a surgery and they, they had the, they had the option they thought was better for them. That would be important to me. I'm just trying to give information, right?
Dr. Grant Garcia: Like in clinic, that's where I get my patients. I show up, I do my job. This is fun. I like talking about this stuff cause I, I totally nerd out. I mean, and this is, this is the way I'm in the office too. But you know, we'll tell you behind the scenes on the same way I get, I get totally jacked about this stuff and I want to make sure people know about it.
Dr. Grant Garcia: Because if they know about it, they're better. And for someone that has to do a lot of revision surgeries and a lot of surgeries, third, fourth time issues, it probably would have been good if someone knew about it the first time. And so it doesn't have to be me. It could be anybody. And again, second opinions are really important.
Dr. Grant Garcia: You know, people always say to me, they're like, [00:57:00] Hey, I don't you know, my surgeon didn't want me to get a second opinion. I'm like, well, that doesn't make any sense. Like if you get a second opinion on my patient, I'm okay with it. It doesn't bother me. You go whoever works best for you. The one final line I always say to people is if you're not feeling comfortable with the surgeon.
Dr. Grant Garcia: Then you shouldn't do surgery with me. One hundred percent. Like you got it. You got to be all on board. You got to enjoy the experience as much as it's not always fun. But again, thank you to all the listeners. This has been a lot of fun. This turned out this podcast went in a different direction. That was great.
Dr. Grant Garcia: And we have so much future stuff for you for the most part. You know, but the but it's good. I mean, we have all this, you've heard of this technology. There's going to be a lot of questions about it. And we're going to go into each one of these again. And as Will knows, I'm going to throw some curve balls and I'm going to give him more technology throughout the year.
Dr. Grant Garcia: But for now, this is what we have and it's pretty cool. And again, this is just sports knee and shoulder. I mean, I'm not even touching on the ankle. I'm not even touching on the hand. Not even touching on the spine. More to come, guys. Some awesome guests coming up. Some things you've never heard about or you want to [00:58:00] know about.
Dr. Grant Garcia: So, thank you. All
Will Sanchez: right. We just wanna thank everybody. Please check us out@sports.talk.com. We, we talk sports, we talk orthopedics. Okay? Apparently we talk all the time, so it's kind of what we do here. So we just wanna thank everyone and if whether you check out sports.talk.com, we have our transcripts.
Will Sanchez: We have a lot of information. Also check out Dr. Garcia's website @ grantgarciamd.com. Thank you very much, Dr. Garcia. You ready for 2024? Let's do it. Take care everyone.Audio Transcript
Shoulder Experts Dr. Acevedo and Dr. Shariff

Will Sanchez: [00:00:00] Welcome everyone, and thank you for listening to Sports Doc Talk. Check us out@sports.talk.com, all sports, all orthopedics, all the time. Except for today. We've got two great guests. I'm Will Sanchez, along with our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia, our guest today. You have to listen to their podcast.
Will Sanchez: : It's absolutely amazing. What incredible guests is the name of the podcast is called. I'm a pod star, not a doctor. Check them out on your favorite listening platforms. Check them out on YouTube. They've got their shows. They've got snippets of great moments. Let's bring them in. Dr. Daniel, Danny Acevedo. A. K.
Will Sanchez: A. Cuff Daddy, I know it's like a rap star here, and Dr. Sharif Bashay, A. K. A. the American Gangster. Oh, fellas, thank you so much for taking time. I'm a huge fan of the show. I've been watching it. I love the snippets. I think it's [00:01:00] genius, right? The little two minute, three minute snippets just gives you that nice little taste and flavor if you're not listening to the whole show, and really gives an example of the creativity and the diversity of your show from, you know, golf and surgeons and you name it.
Will Sanchez: And I've seen interviews with you guys. Anyway, I'm yip yapping along the way. Thank you very much for being here. Dr. Garcia, how excited are you to have these two gentlemen on the show?
Dr. Grant Garcia: I'm super excited. This is, this is going to be a good mix. You have guys that are incredibly well known on the internet and throughout their world for their techniques, their cutting edge, they're teaching everything, but they're also super funny.
Dr. Grant Garcia: Chill and their podcast is awesome. You know, it's a completely different vibe than. Honestly, what our podcast is like or some of the other ones out there. AndBishai you know, you may hear from them, you know, the goal is for them, if you learn something by accident, that's awesome. But otherwise just here to have fun.
Dr. Grant Garcia: I'm
Will Sanchez: really excited. [00:02:00] Excuse me. I'll start real quick. You know, every time we have doctors on the show, I have to, you know, it's, it's respectful, right? And you have to say, you know, Dr. Bishai, Dr. Acevedo. But with these two, it doesn't feel that way. Dr. Bishai, this sounds funny saying it. Bishaithank you so much for being here.
Will Sanchez: How has the show been, doing this podcast? How's this experience been, been for you?
Dr. Shariff Bishai: Man, I love it. It'sBishai I'm, I'm hanging out with my boy. And so whenBishai Danny and I are on the mic, it's like, I'm to picked up the phone to hang out. And our DJ producer, Bobby, he's the creativity. He's the one who comes up with all that stuff you love.
Dr. Shariff Bishai: And so we got to throw him a shout out. And so that's Bobby digital. And we just have a good time. And so for me, if anyone's listening, great. If no one's listening, I'm still having a good time.
Dr. Shariff Bishai: And so we got to throw him a shout out. And so that's Bobby digital. And we just have a good time. And so for me, if anyone's listening, great. If no one's listening, I'm still having a good time.
Will Sanchez: Dr. Acevedo, Danny, the cuff daddy., once again, thank you so much for being on the show. [00:03:00] Bishaitell me about the idea of this podcast and how this got started.
Will Sanchez: Bishai who was the creative genius, you know, putting this together? Obviously we got a shout out from Bobby, but as far as the concept of putting this show together, explain that a little to me.
Dr. Daniel Acevedo : Well, the name, I came up with the name.
Dr. Shariff Bishai : So
Dr. Daniel Acevedo: no, so, you know, I met, I met SharifBishai at one of, at the ASCS meetings. And I see him at meetings, you know, we're both like lecturing and teaching and, and we kind of clicked, we got a similar vibe and, and I was trying to find somebody to, to have a podcast with.
Dr. Daniel Acevedo: And, and I didn't really want to do like. You know, I wanted to do a fun podcast. I mean, obviously we all ever, there's a place for every podcast. You guys have a place. We do sports. Very cool. I don't want to copy anybody. I just wanted a place where I could showcase like my normal self and, and just how normal and cool, like some of my doctor friends are and some of my other friends are.
Dr. Daniel Acevedo: And then, so Sharif hit me up and, and then he's like, [00:04:00] HeyBishai would you be interested in having a podcast? And I was like, Oh, yeah, I've actually been thinking about a podcast. I'm like, who could I do it with? And then he texted me back and he's like, me. And I was like, oh, okay. So that's kind of
Dr. Shariff Bishai: how it came up.
Dr. Shariff Bishai: Yeah, that's where it goes back even further. So a couple of years ago, Bobby reached out to me and he was like, Hey, we have a great idea. Why don't we have you on? Bishaiwe'll make you the host. So we'll interview all these other kinds of doctors. And I'm like, orthopedist is like, no, no, no. Like family practice and urology.
Dr. Shariff Bishai: I'm like, that sounds terrible. And so it kind of died. And then when Danny and I started, you know, getting to know each other and I call, I was thinking to Bobby, I was like, you know what, I think I got a guy. So I called Danny and then Danny's like, well, let's have a meeting and. We can figure out if this will work.
Dr. Shariff Bishai: And he like essentially going to interview us to see if we were cool enough to hang out with them. But then
Dr. Grant Garcia: obviously we passed that. Gangster dude. He's cuffed daddy. It takes a lot.
Dr. Daniel Acevedo: Bishai yeah. It's all about the [00:05:00] vibe. You guys, you know, you guys have good chemistry. You know, I know me and SharifBishai have good chemistry, so that's huge.
Dr. Daniel Acevedo: Right? Like I was thinking of some other people, but it actually worked out great. And I'm having a good time. Bishaiyou know, we're having fun on our podcast and we're just kind of doing the thing.
Dr. Shariff Bishai: The hardest part about our podcast is LA internet period.
Dr. Grant Garcia: I can see Danny's shut down a few times with his LA internet.
Dr. Daniel Acevedo: : Dude, it's the LA internet. Like the LA internet sucks. Like, like at five o'clock everybody's home and there's like probably like a million people like where I live, like alone.
Dr. Shariff Bishai: I thought people went outside and exercised and ate avocados and shit. No dude, you're playing Fortnite
Dr. Daniel Acevedo: and whatever they're doing at night.
Dr. Shariff Bishai: When we first met he goes, you're a Gemini. And I was like, okay, I didn't realize that you could figure that out, but that's cool. And he was absolutely right. And so the Gemini, you know, it means there's the, the yin and the yang kind of thing. And so it kind of makes sense why I'm American Pharaoh and Dr.
Dr. Shariff Bishai: Bishai. So it kind of all fits. [00:06:00]
Dr. Daniel Acevedo: That's awesome. It's like residency grant. Didn't you have a nickname in residency? I'm sure you did. I think
Dr. Grant Garcia: I probably had a few of them. Yeah. Yeah. TBishaih, they're all over the place. Depends. I'm usually pretty hyper, so I get like the, you know, like in the, I'm always like full speed everywhere.
Dr. Daniel Acevedo: Yeah. It's funny. Cause like when, you know, when I was thinking I wanted to do a podcast a while back, I saw that you guys had a podcast. I was like, oh, that's cool. And then I liked, you guys talked about sports and ortho and I was like, oh, that's really cool. So I like that. And then, you knowBishai Scott Sigmund has his podcast and.
Dr. Daniel Acevedo: And at the time I was like, dude, I really want to have a podcast, but you know, I don't follow sports like that. Like I'm more of like a, like a, I go to meetings and then I'm crazy on the side. So like, where, where do I fit in? And thenBishai it's funnyBishai when me and Sharif Bishai kind of metBishai at a meeting, we kind of started talking and, and we both were like looking for a podcast partner.
Dr. Daniel Acevedo: And then he kind of hit me up. He's like, Hey, do you want to do a podcast? I was like, Oh yeah. I [00:07:00] was like, I've been totally thinking about when I was like, who can I do one with? And he's like me.
Dr. Grant Garcia: Anybody, anybody but you know,
Dr. Shariff Bishai: it was like, it's like, no, you really, you know, but Bobby, who is our producer and DJ, he was great because he reached out to me a while back and he's like, Hey, I want to do a podcast with you and you could be the host.
Dr. Shariff Bishai: And each week we'll bring on a different type of doc and blah, blah, blah. And I was like, Hey, that sounds terrible. I mean, I have no interest to do anything but orthopedics and preferably just sports. Bishaiand then so it kind of died. And then when I, when Danny and I started talking, he calls, he's like, why don't we meet?
Dr. Shariff Bishai: And if this sounds like it may work, then we can move forward. So he's like, essentially, we're, he's interviewing us. It's like, cause he's got options.
Dr. Daniel Acevedo: No, dude, it's not even that. It's like, like your podcast is awesome. You guys do sports. Like I'm not into sports like that. Right. And I'm already, we're already into orthopedics.
Dr. Daniel Acevedo: You're into orthopedics. I see some of your videos, Grant. They're [00:08:00] awesome. BishaiSharif has videos. We all teach. We're all a part of this, but I just, I wanted an outlet where I was like, look, a lot of people that meet me are like, you're a doctor. Like, you're really cool. Like, I really like your vibe, your, your.
Dr. Daniel Acevedo: different. You're down to earth. And then I just wanted to be like, you know what? There's a lot of people that I hang out with that are actually like me. And I wanted just a platform just to kind of showcase that, you know, I mentor students. I mentor my own children to try to get people to be doctors, to be like us.
Dr. Daniel Acevedo: And I think the best way. To kind of get people to know who we really are. Like it's just to kind of show it right. And obviously not to be too crazy, but that's kind of where the idea came from is I just wanted to kind of show like other stuff that I'm into, like the friends that we talk to stuff we talk about,
Dr. Grant Garcia: you know, I love that.
Dr. Grant Garcia: I love that idea. I mean, it's just like the, I think that's, that's what in my office, like the same sort of thing. It's like, I'm, they're so used to someone either like rigid, quick, just want to go, go, go and to get out of the office or they're not used to like the [00:09:00] personality type. So if you have a little personality, it can really connect with the patients, especially, you know, you guys are super fun.
Dr. Grant Garcia: And so like, if you already have, you already have all the skills. Right. And so then now you're just the fun person. So you can, the doctor, it just eases their stuff. Cause I mean, I see what you guys are doing. Like these aren't, some of these aren't straightforward cases. I'm sure your patients aren't coming in just giggling before they meet you.
Dr. Grant Garcia: So, you know, you don't talk to you about, so yeah. So it's like you're decompressing. Difficult situations with all the stuff you do. And honestly, the stuff that you guys are doing is the stuff that I've always look forward to doing at some point and just getting, breaking out and showing your true personality.
Dr. Grant Garcia: Cause most of us have personalities that people want to hang out with. You know, we have 95 percent of my 99 percent of my friends are not doctors. So, you know, that doctor persona that you have to have in the office sometimes is not, you know, where you're always are and you guys are kind of. Letting loose and showing people the other side, which is what people think is fun and entertaining.
Dr. Grant Garcia: You're like, Hey, listen, this person could be, you can have a beer. You always think, I always tell people, like, if you feel like you could have a beer with your surgeon or like [00:10:00] chill with your surgeon, you think they're a good person and on top of the fact, they're going to do a good job, that's the best type of personality to deal with.
Dr. Grant Garcia: Because it's just, it's a, it's a different level of care. I thinkBishai when they're, cause that, that personality persona you guys are showing, you know, it's just something that's like a connection.
Dr. Shariff Bishai: Yeah. I thinkBishai Danny and I vibed the second we met. And I think it's important, like you said, I think the first thing's first we're docs and we have to be good to our patients, offer a product that is.
Dr. Shariff Bishai: Going to make them better, but at the same time you got to be human and I think you definitely see our human side I think there's this this need from people to think that doctors have to be a certain way They have to be that rigid person and and then at the same time while they want us to be that way then they say well That doctor doesn't have a good bedside manner.
Dr. Shariff Bishai: It's like well, you can't have it both ways so I think you got you got to straddle that line a little bit and kind of Come in and out. I don't think you [00:11:00] necessarily need to be friends with every one of your patients But you need to have that respect for them as they'll have for you And I think what comes of that is a nice doctor patient relationship But at least for our pod whoever's listening because now I have patients coming in saying oh, I listen to your show And I'm like, oh shit what I say, you know careful You just
Dr. Grant Garcia: mentioned, you went to HarvardBishai to hang out with your buddy.
Dr. Grant Garcia: You guys are all over the internet on your non podcast stuff. And all the, all the really prestigious things that you guys do. How, I've talked about like what I do to try to stay cutting edge for my patients in Washington and Seattle area. What do you guys do? Like, what is it that you can do that, that allows you to keep doing those things?
Dr. Grant Garcia: I mean, you're teaching about arthroscopic. DTAs, arthroscopic latergies, and for some of the patients, they'll look those things up. They've talked about those before. So like, how do you guys do it? What, what's your, what's the trick? What's the
Dr. Shariff Bishai: flavor? What's the magic? For me, it was my patient population and I kept on seeing these things that I just didn't have.[00:12:00]
Dr. Shariff Bishai: An answer for, I knew there was an answer out there. And so I said, well, how do I task myself and challenge myself? And I said, I'm going to just go learn. So I went to Europe and I went to Lafaz. I went to Ravenscroft in Manchester, England, and then I went to Paul Favarito in Cincinnati and George Athwell and Hamilton, Ontario.
Dr. Shariff Bishai: And, you know, bounced around, did a couple other labs and it took me. From the day that I said I wanted to learn arthroscopic glottis A to my first case was almost two years and I don't think it takes that long now because there's a lot more opportunities than there were back in 2013 to 15 when I did this.
Dr. Shariff Bishai: So I think it was. The, the shift in the way I thought about things. And I thought we were, why are we seeing so many failures with bank cards? So I need to figure that out. And then I did the same thing with like lower trapezius transfers. What are we going to do? SCR doesn't work and you know, we don't know what the balloon's going to be.
Dr. Shariff Bishai: And not everybody at a young age needs a reverse. So I got to have. [00:13:00] I have to find something and that's when that whole thing started and Basim taught me that as well. So for me, it was the patient population I was seeing, giving them an answer and making sure that I could do it with my hands. And if I couldn't, then I needed to get them to somebody who could.
Dr. Daniel Acevedo: Yeah, that's kind of what I do. Like I always joke with my, my colleagues. I always tell them, I'm like, you got to stay ready to be ready. And they look at me like I'm crazy, but that's kind of how I am. Right? Like if I see new techniques come out, I go to meetings, people talk about these techniques. I try to learn them.
Dr. Daniel Acevedo: I'll set up a labBishai or I'll either do it. Sometimes I don't need to do a lab and I'll just like do it on the patient. And just kind of tell them, Oh, this is the first time I'm doing it, but it's not a big deal because you know, we're all. Technically gifted after like a certain point. And I think after like six, seven years of getting my reps in and I finished my fellowship and I, I kind of knew what I could do and what I couldn't do.
Dr. Daniel Acevedo: I tried to do the stuff that I couldn't do. And I challenged myself, you know, arthroscopic Latter day was always something I wanted to do. And once I got my scope skills up, I learned how to do it. [00:14:00] You know, I talked to LaFoss, I talked to Boileau and then, and then I figured it out. And then, and then as far as the videos go, like, I just like teaching, you know, I like, I like.
Dr. Daniel Acevedo: Videos and the social media type thing so I would make Vumedi videos if I did a good case And I thought that I had something to offer somebody else trying to learn how to do something Like I did a SCR video early on I did an arthroscopic later J video early on in a trap transfer You know because I know a lot of people want to learn how to do it, and I think for me.
Dr. Daniel Acevedo: I'm like People know me. I'm like, here, this is what I did. Check this video out. And then it kind of helps people. And it's, it's always nice because people will text me. It's like, Hey, I watched your video before the surgery really helped. And, and for me, that helped, that helps me want to continue to teach other people just how to help patients, man.
Dr. Daniel Acevedo: Like it's, we're all in the game. You know, I watched stuff that you do and like how you teach patients and, and stuff that you're, we're all learning from each other, which is great. So for me, I think just, I just follow other like minded people. And then I just try to push myself to, to continue to be
Dr. Shariff Bishai:better.
Dr. Shariff Bishai: And if they think that I can do it, then they're [00:15:00] usually like, Oh, I can do it. If Bashay can do it, I can do
Will Sanchez: it.
Dr. Grant Garcia: No, I, I love it that, I mean, this isBishai Will's heard me talk about this before, but it's good to, that's why I wanted, it's good to have you guys on here for him to see sort of, this is, this is not just one person doing something, trying to get better or whatever, it's all different ways to do things.
Dr. Grant Garcia: And this is what, you know, listen, he's traveling, you're traveling out to outside of country to France. Bishaiyou're going to Canada to learn these new techniques. You know, it's good for the patients to hear this stuff because they don't, you know, they don't always understand that some of these more complex things sometimes take that stuff.
Dr. Grant Garcia: You know, not all the time, you knowBishai what Daniel said is true too. I mean, I hate to say it. Sometimes you watch a YouTube video. If you, if you know the steps, if you got everything else, I just tell them, it's just combination. You're just changing the order, right? It's like for the lower trap transferBishai for me, it was just the dissection.
Dr. Grant Garcia: So I did that in the lab a couple of times just to kind of get that feel. And then the trance I did SCRs before. So that wasn't the hard part. BishaiIn terms of the conversion rate. So for it's interesting to see what you're saying. And what you mentioned about [00:16:00] the videos is exactly what early on. I was like, I'm putting out these videos.
Dr. Grant Garcia: I'm like, I don't know if anybody cares. I think it's cool. Actually, it helps me. It helps me a lot, actually, though. I like having the video. I'm like, I haven't done a surgery in like a year. I'm like, how do I do it? I'm like, Oh, it's on my video. So
Dr. Shariff Bishai: it's helpful. I think videos are so important. AndBishai I'm the chair of the orthopedic video theater for the academy right now.
Dr. Shariff Bishai: And so for us, we want as many videos as we can get, because we will review those peer review those and make sure that they're to the standard of the academy and then make sure that when they get out there. Everybody can use them. And it's not something that, oh, you got to pay for this or you can only do this if you're not.
Dr. Shariff Bishai: We want people to see these because these are experts that are putting it out there. They're reviewed by a contact a context expert. And then at that point, anybody can watch him. So it's great for residents and fellows and even people in practice. So I think video is the new way. And then once I starts kicking in and we can layer those [00:17:00] with the papers that we discussed within our videos, I think it's gonna be amazing.
Dr. Grant Garcia: it. Go for it. Tell me your journey. I want to hear your journey. And I might chime in on some things, but you know, I do a little bit of IP. Again, I'm a surgeon by most of the time. You are the expert.
Will Sanchez: Have you ever gotten anyBishai videos where you goBishai yeah, man, we can't, we can't put that out there. That is justBishai just something. Is there any video that's ever stood out there? You're like, yeah, nope, that's, that's not going to work. And makes you question about that, doctor.
Will Sanchez: We don't have to say names. We don't have to say names. Oh, gosh. Will, you did do it. You did it,
Dr. Daniel Acevedo: didn't you? Let's just say it's a Maybe a style difference, right? Like, it's just like people, some people dress better than others, but you know, they're still wearing clothes.
Dr. Shariff Bishai: That's fair. That's nice. I like that.
Dr. Shariff Bishai: That was very diplomatic. You know
Dr. Daniel Acevedo: what I want to do? And I don't even care if I give this idea to all these listeners that you have. BishaiI want to do this thing called the cuff cloud. And then basically like, it would be like this. Stop it, stop it, stop it. It's coming up. Stop it.
Dr. Shariff Bishai: Now we just tease the listeners. [00:18:00] I like it.
Dr. Grant Garcia: They're going to be all, they're going to type it out. Cuff cloud
Dr. Shariff Bishai: now. Yeah. End of Q1, it'll be out.
Will Sanchez: Can, can you get some scrubs made with like really big cuffs and then walk in to the operating room? Can you get something like that? So they, you know, cuff daddy's walking in with these big cuffs.
Dr. Daniel Acevedo: Dude, no, I need to get a chain though with like a big C on it. That would be super cool. Bishaibut there's a, there's a doctor in Beverly Hills. I don't want to say his name, but he's, he has these special scrubs where they're cut off. And like, he's, he's always like showing his cutoff scrubs. And I was going to DM him cause I wanted to see where he got those.
Dr. Shariff Bishai: He got them at the store and then he got scissors. That's where he got it.
Dr. Daniel Acevedo: Hey, I was going to ask you, Grant, I think it's pretty cool. Like, I like what you do. I don't think I could do that. I like how you were doing on your podcast. Bishaiand you talk about like you sports and, and so do you, do you use your podcast to kind of like help the community with these topics and stuff?
Dr. Daniel Acevedo: And like, how are you promoting it in your community?
Dr. Grant Garcia: So [00:19:00] I, I just do like, if I get something crazy, like our patients are confused about something, I'll do a podcast for it or to promote the actual like thing, like ACL repair or, you know, other things. And then I'll, I'll use it and publicize it on, you know, all the social media things I can, but it's actually funny.
Dr. Grant Garcia: I get people coming in asking for the surgeries on a podcast. BishaiI mean, I very frequently patients come in, I mean, and I, some like device companies I work with, like for like rehab stuff, people come in asking for that stuff after the rest of the podcast. So it's really interesting how you really, you have to be careful, obviously, because whatever you're putting out there, I realized really quickly, like if you, as long as you make sure it's real information, you could see you're talking about, you knowBishai you guys talking about like vetting the videos.
Dr. Grant Garcia: We're, we're known surgeons now. So you start putting something out that's not accurate. That's a big problem as well. Bishaiso that's good. Like I found out really quickly that if you promote the right things and the things that are fair and reasonable, people want to listen to it. So I kind of swerve around and I'll, I'll hit up to Will.
Dr. Grant Garcia: : I'll be like, well, what do you think about this topic? Cause obviously he [00:20:00] knows more of the layman term stuff and he's like, that's super cool. Let's talk about it. Bishaiand I try to promote mostly cutting edge stuff because I think. For me, I'm super excited about like the next cool thing, the next cool thing, the next cool thing.
Dr. Grant Garcia: And so for me, I'm like, I want to get that up to date. I'm like telling people about how to fix a rotator cuff to me is boring. Bishaiyou know, I want to talk about like how I'm going to make it better. I'm going to do some crazy patch or do some, some other type of thing that there's out there. So that'sBishai that's kind of the way I think about it.
Dr. Grant Garcia: I'm not that answered your question. Yeah,
Will Sanchez: and Bishai and just to piggyback on thatBishai I've worked with a lot of coaches between high school, middle school, youth coaches. My background is a producer at master square garden. I used to work with the high school Rangers Knicks. SoBishai when we still have texts and conversations and we want to make sure that we communicate these things and, you know, and, and try to get some information like.
Will Sanchez: This is what we're seeing on the field. This is what's happening. So then when Garcia and I [00:21:00] talkBishai you know, that's where I go. Yeah. That, that sounds really good. And that's something that's important. Bishaiyou know, talking about, you know, the Q collar, knowing how concussions Yeah. Playing a big part ofBishai just the, the conversation right now.
Will Sanchez: Right. I just saw that California is now trying to make a movement here to banBishai football. tacklingBishai and football. I don't know when it's 2028, whatever that is. I don't have the information in front of me. So, so it's a big topic. So when we could talk about these things and address them and speak with great guests like yourselves, it's just, I think people resonate to the conversations.
Will Sanchez: So that's how we kind of come up with some of these topics here. Well,
Dr. Shariff Bishai: well, I'm going to jump on that. You know how you get rid of concussions in football? Tell me, take off the
Will Sanchez: helmet. You're not the first person to say that. Or I've also heard, take the face mask off.
Dr. Shariff Bishai: Yeah, because if you, if you look back at the statistics, it's as technology gets better, the concussion rate gets higher, the, [00:22:00] there, there's certain things.
Dr. Shariff Bishai: I mean, yes, we've changed rules. You can't target, you can't do, they can't lead with the crown of the helmet, but it's a weapon. Just like when you put a kid in a cast, the first thing I tell 'em is like, this is not a weapon. You can't get the crap outta your little brother and sister.
Dr. Daniel Acevedo: That's why you, that's why you can't get a cast in jail,
Dr. Shariff Bishai: right?
Dr. Shariff Bishai: You go, we learned
Dr. Grant Garcia: some. See you were gonna learn something
Dr. Daniel Acevedo: on this today. Well, we used to have a jail at the USCBishai at the USC county. We go to jail and like they wouldn't like us to put cast on 'cause the, the inmates would use them as weapons.
Will Sanchez: There you
Dr. Shariff Bishai: go. It
Will Sanchez: totally makes sense too. So what do you do?
Will Sanchez: Just soft cast, ace band?
Dr. Daniel Acevedo: Or we like cast them and then they like keep them there or they put them in isolation or something. I don't remember. I hated going up there. It was scary.
Dr. Grant Garcia: I did. I saw that. I went to my USC interview. I saw the prison there. I was like, this is interesting. That was scary.
Will Sanchez: This is interesting.
Will Sanchez: That's
Dr. Grant Garcia: where you learned all your cutting edge techniques, I thought.
Dr. Daniel Acevedo: Yeah, dude, it [00:23:00] is. I mean, it was a great place to train, you know. I don't want to say we practiced on these people, but yeah, we practiced on these people. But, you know. Everyone's practicing. I don't know. You can't sugarcoat it. I mean, what are you going to do?
Dr. Daniel Acevedo: Just, you know, Isn't
Dr. Grant Garcia: that where we're in? We're in practice. I was, I spread that to people. They're like, listen, I try to tell even the new fellows that people call me, they're like, I saw your video. Tell me about this. And I'm like, dude, if you're doing the same thing you learned in fellowship. In your first few years, you're not doing it right.
Dr. Grant Garcia: I was like, I remember I did like 20 surgeries. I never learned in fellowship and I thought like Cole and everybody knew everything and they're awesome, but like, you know, my third case, I did a glenoid fracture and I'd never seen one done arthroscopically. And I'm like, oh my God, how do I do this? And they're like,
Dr. Grant Garcia: smoothly. This is so important. I think the listeners should this is going to be our longest podcast ever, this is so exciting.
Dr. Daniel Acevedo: you, you Mills video.
Dr. Daniel Acevedo: That's what I did. And then I did it. I,
Dr. Grant Garcia: I, that's what I did actually, but I, it actually worked, so I was like, this is pretty cool. Yeah. So yeah.
Dr. Daniel Acevedo: So for everyone listening, yeah, everyone listening, if you're a doctor, you got to keep putting these videos out because we're all watching. We're all looking
Dr. Grant Garcia: for sure.
Dr. Grant Garcia: It's weird. It's so weird to hear. It's so great to hear it. Like it [00:24:00] took a little while before we started hearing it. But people were like, I was down like giving a talk or something else. And then people were like, some from random, you know, private practice docs, like I watched your video on that. That's really cool.
Dr. Grant Garcia: And I'm like, what? You know, that's it. It makes you feel good to be helping and teaching. Obviously, like, I think the good thing is like the open forum. Like, I like YouMedi a lot because it's super chill. Like, every once you get a thumbs up, you know, you know, someone thinks it was okay. You get a weird comment every once in a while that you don't respond to.
Dr. Grant Garcia: But outside of that, you know, my biggest concern with the videos was like, someone's gonna be like, that's not right at all. They're trolling. They're
Dr. Shariff Bishai: trolling the trollers. But how many times have you watched a video and you're like, that's not right. No, no, that's or at least the narration that you say the wrong thing.
Dr. Shariff Bishai: So I went to Memphis to teach a course two weeks ago and one of the guys is a buddy of mine that I was teaching and he said, Hey, I watched your artscopic letter J video andBishai yes, 53 minutes. You didn't edit it. Thanks for doing that because it was made it really [00:25:00] nice to be like every step of where you struggled.
Dr. Shariff Bishai: I'm like, well, that was the point. Bishaiand he goes, but, but you called theBishai you called it. The coracle chromium ligament. And you were talking about the coracle clavicular ligament. So I'm like, bro, if, okay, you know, but dude,
Dr. Grant Garcia: the guy, you should give the guy luck. I would never watch 53 minute video that he should give him.
Dr. Grant Garcia: So he can say whatever he wants about your video. He sat there for 53 minutes and watched it. That's fair.
Dr. Shariff Bishai: That's impressive. I want to shoot him a text.
Will Sanchez: Right now. Do you think he's watching the video as he's in surgery and just hitting pause on the button and then kind of doing the procedure and then, dude, there you go.
Will Sanchez: You know, is that, is that why, you know, he's like, yeah, I sat through the whole video because this is exactly what I did in the
Dr. Shariff Bishai: operating room. So funny story, Danny did that, but on a cadaver. So when he watched my video while practicing it, so they had it on a screen for him here and a screen over here where he was working on and he was watching back and forth.
Dr. Shariff Bishai: And that's the skillset Danny has. Yeah. Is like, I
Dr. Grant Garcia: wanted
Dr. Daniel Acevedo: to play with the screws. Cause I was doing, I'm doing arthroscopic later days with the button. And I'm like, let me [00:26:00] check this screw game out. So I set up a lab. And I saw Sharif's video and I was like, Hey, can I put this video up on the screen? And the Dubuque techs are like, yeah, why?
Dr. Daniel Acevedo: I'm like, I'm going to race it. And they're like, what? I was like, yeah, just put it on. So then I was like, go. And we played and I just kind of like did it. And I was looking at his video to make sure I did the steps. And then I finished it in like 45 minutes. And then I took a picture.
Dr. Grant Garcia: That's like the Ridge race.
Dr. Grant Garcia: Remember like the Ridge racer with like the shadow car. Yeah, trying to, but
Dr. Daniel Acevedo: the cadaver doesn't bleed to be fair. Right. It doesn't bleed. And you know, I wasn't really worried about nerve damage, so I'm just kind of going in there doing it. ,
Dr. Grant Garcia: I think. I think Will's jaw's about to drop
Will Sanchez: to the ground here, here and all.
Will Sanchez: No, I go like this. La, la, la, la, la la la. I didn't hear anything. The cadaver. I know, but you know
Dr. Grant Garcia: what though? This is, well this is the good part about what you guys do. You bring out like the real stuff. 'cause like this is all anybody that tells you, they just like know how to do it. And then on top of that, there is a certain skillset.
Dr. Grant Garcia: I mean, Danny, your skillset is not common, right? Like [00:27:00] people always say, like, like say to the holiday Inn, it's like, no, I watched the YouTube video and I did it. Like, that's not like, not everybody does
Dr. Daniel Acevedo: : that. I do stay in my lane. You know, I have a nice. Practice now, I get to do shoulder elbow, a little bit of knee, but like, you know, I'm not doing everything right.
Dr. Daniel Acevedo: Like I have, I do cuffs, arthroplasty and instability. Those are my top three, but I'm not in fractures, but I'm not like a general ortho, right? So it's, it's really tough for these general ortho guys, man, that are like doing a lot of different stuff. Right. I mean, I think that's, there's still a role for that, but like you're a sports guy, right?
Dr. Daniel Acevedo: So you're doing a lot of sport shoulder. So you're kind of in your lane. You know, so you could be really good.
Dr. Grant Garcia: Yeah. No. And that's the, that's the point. It's hard for people to understand. Cause they see like some guys, like the guys that were talking about my videos, they're like, I saw your TTO, Macy MPFL.
Dr. Grant Garcia: It looked really cool. I'm like, dude, you shouldn't try that for your first one. I was like, you know, they're like talking about meniscus transplants. I'm like, dude, it's the, it------------------------------'s a, it's not like a see one, do one, teach one type of thing. But your point is, your point is well taken. Right. Cause it's hard for people to [00:28:00] process that every, not everybody knows that.
Dr. Grant Garcia: Even you see the word sports surgeon, or you see the word shoulder surgeon, it's not always the same. Or, you know, the word surgeon, right? Orthopedic surgeon could mean many different things. Bishaiso it's, that's important indication as well for people that, you know, we're talking about like, this is high level, like we stay in line, but you don't want to see me do an ankle.
Dr. Daniel Acevedo: Yeah. I mean, I'm sure you're good, right?
Dr. Grant Garcia: I just not, I just feel like I'd rather, I'd rather do a meniscus transplant to be honest with you. But yeah, so I like ankles.
Dr. Shariff Bishai: You would do a meniscus transplant over an ankle fracture.
Dr. Grant Garcia: I love meniscus transplants. So I agree with him. He's a neat guy. I'm a glutton though for punishment.
Dr. Grant Garcia: I love all the fun stuff. I'm not sweating after cases. It's not, I'm a high octane. Probably like Danny. I'm like, I'm like the Ridge Racer, you
Dr. Shariff Bishai: know, with the ghost. No, but I agree. I think, but that's what is going to make you. I mean, you're still young, but as you get older, you're going to realize how good you are.
Dr. Shariff Bishai: At what you do, because you've picked your poison and said, this is where I'm going to be. I think there's a place for the [00:29:00] general orthopod and they're needed without question. However, if you have a unique injury, I think it's important for that patient to really Interview and get a second opinion, essentially figure out, talk to your doc.
Dr. Shariff Bishai: Now they ask funny questions and say, how many have you done? And that's always interesting to me because the answer is more than one. However, I always ask them, what's the number you're looking for? Because I don't even think they know what they're asking. They just want to make sure it's not your first one.
Dr. Shariff Bishai: So I say, when they'll say, how many of these have you done? I'd be like, what's the winning answer.
Will Sanchez: Thousands, right? Exactly. I think that's the go to. Thousands. Or you could
Dr. Grant Garcia: be like Danny and just tell your patient it's always his first one.
Dr. Daniel Acevedo: No, I tell them, I tell them real numbers. You know, I'm pretty, it was nice that my old job, I had like a database, so I actually knew my real numbers and my complication rate, which was awesome.
Dr. Daniel Acevedo: No, I tell them, I tell them real numbers. You know, I'm pretty, it was nice that my old job, I had like a database, so I actually knew my real numbers and my complication rate, which was awesome.
Dr. Daniel Acevedo: And I wish some of my newBishai hospitals had that. Like I like to know what's my complication rate, revision rate, like how many did I do [00:30:00] just to be able to tell patients, right?
Dr. Grant Garcia: And I try, I keep like a track of my surgeries. I'm able to know like rough numbers, but it's, you know, at the same point, you're right.
Dr. Grant Garcia: Like, what does it matter? Right. I've seen doctors that I've seen. I know that do like 200 and I'm like, you did, there's no way you did the first one 99, you know, as proficiently. So it doesn't, you know, the number doesn't always matter either. Like you said, like, what are you looking
Dr. Shariff Bishai: for? Exactly. Because I think there's also the person that's done a thousand but has done a thousand, maybe not the best way.
Dr. Shariff Bishai: So that's their way and there's new techniques or whatever. Right. And. So I think that number is arbitrary. I think it's about being proficient and knowing the data. And I think personally, I mean, I keep all my own data and I still, you know, publish. And we looked at the complications of the arthroscopic clatter Jay to make sure that I was doing a service to the community and not a disservice.
Dr. Shariff Bishai: And we found that after 25 is the year learning curve and it matched the other articles that were already out. So I was like, cool, there's five other articles that all said [00:31:00] 25 and that's where mine was. And. And we went from there. So I'm at 92 now, and it's, I feel like as though I'm in a, in a, in a nice space to help the area people in the area.
Dr. Shariff Bishai: I mean, I had a guy, you know, that was sent to me from Dallas to have it done all the way to Detroit. And I explained to him, I'm like, you flew over four dudes that could have done this for you arthroscopically. But somehow he got to me, but I was happy to have
Dr. Daniel Acevedo: it. I haven't had that yet. I thought about that the other day.
Dr. Daniel Acevedo: I had someone drive like a few hours and I was like, Oh shoot, that's cool, man. But like, I feel like if someone flew to see me, I might cry. I might like tear up a little and then
Will Sanchez: Would they get like a little gift basket or something like that? A little memory? Yeah, I'm gonna call my
Dr. Daniel Acevedo: mom. I'm like, Mom, I made it.
Dr. Grant Garcia: It's different depending on market to like I get a lot of people flying like from Alaska, Idaho and like other places, but they, it's also different in like Seattle. It's different market than you guys, LA. I mean, where you're at is crazy. And in Detroit too,
Dr. Shariff Bishai: it's just different. There's a lot of dogs here.
Dr. Shariff Bishai: And I [00:32:00] think the, the key is with, with those, I call them my mail orders. And so when the mail order comes in at my scheduler, they'll see me on a Monday, they'll have surgery on a Tuesday. So me post up day one. So they'll be in town for two nights, three days with me, and then they're off. And if they want to come back, happy to do it, or else I'll help them facilitate care wherever they're from.
Dr. Shariff Bishai: So I think what's cool about it is they feel that individualized, like, concierge type medicine. I don't love it because I want my data. I want to know how they're doing. And if I feel like I can't get to them, I feel like I'm not I'm not where I want to be, but at the same time, if that's the only place where, how we can do it, then, then, you know, you just do it.
Dr. Shariff Bishai: Yeah. I got a
Will Sanchez: question regarding the show of a pod star, not a doctor. Okay. So there's a segment on your show. There's lots of segments on your show and it's called keeping it gangster. Gangster. Now, who came up with this idea? How did this idea come to [00:33:00] fruition?
Dr. Daniel Acevedo: That was my idea, so, I, you know, even in residency, like, everyone would, I would be kind of up with the slang, and then I would just say words, and nobody knew what the vernacular was, and so it happened.
Dr. Daniel Acevedo: to me at meetings, I'll be at meetings and I'll be like, Oh yeah, low key or I'll be like, yeah, bruh. Or I'll say Riz or something. And then one of my friends, Melissa was like, I don't understand half of the shit that you're saying. I was like, I'm going to have a segment to teach people how to speak slang.
Dr. Daniel Acevedo: Right. So that's kind of how that came up. Sharif,
Will Sanchez: what were your thoughts when you were like, All right, we're going to roll with this. What were yourBishai initial thoughts
Dr. Shariff Bishai: on that? I thought this was amazing just because it's like listening to my 16, myBishai 13, and my 11 year old speak. So I was like, this is perfect.
Dr. Shariff Bishai: Now I can have a conversation. Yeah. I mean, we helped, we
Will Sanchez: helped so many dads. Now, do they think you're cool or they're like, Dad, come on now. Please just, just don't, don't say those words to me. Come on. What's the reaction you get?
Dr. Shariff Bishai: So if you look at my Instagram, the first thing it says is hashtag manchild.
Dr. Shariff Bishai: [00:34:00] So they know I'm a kid. So to me, they were like, that's fine. We will accept it.
Will Sanchez: All right. This is, this question is for both of you. What's your favorite Keeping a gangster episode because obviously that's going to tie around a guest, maybe a reaction, maybe some of the words that you used. What's your favorite?
Dr. Shariff Bishai: I would say it was our first episode and it was with Kamran Hamid out of Chicago who is also rapping. He's great for you. Danny's cracking up already. Bishaiyeah, he was great. He's awesome. We were showing, so I, I made up the words and I was showing them and Danny and Cameron had to read them and he wrote one back, but he put your instead of like you are.
Dr. Shariff Bishai: He wrote it. Why? Oh, you are apostrophe. So I'm like, and he kind of put it up and he brought it down. It was like, no, no, no, no, no, no, no, no. Pull that back up. Where did you put that [00:35:00] apostrophe? Bishai
Dr. Daniel Acevedo: I don't know. I had fun with my friend, Jessica Mina. She, she, she was giving us some new words. We never heard about like shooketh and stuff.
Dr. Daniel Acevedo: Bishaiit's, you know, it's just fun. It's just, like I said, just trying to loosen people up and, and just kind of show like, look, we all have kids, you know, we're around this stuff too. You're not the only one. And just kind of like making light of it. And just. Like I said, just having fun. I think it really, it loosens the guests up and it kind of catches them by surprise because they're like, wait, what?
Dr. Shariff Bishai: Yeah, we have one coming out inBishai I think like a couple of weeks where he plays the game. What am I sitting on? We'll just leave it at that.
Will Sanchez: Well, that's, that's a teaser right there.
Dr. Grant Garcia: The audience is dying to see this now. This in the cuff cloud. Everyone wants to know about
Dr. Daniel Acevedo: it. Dude, we're just, we're just having, we're just having I mean, you know, I worked all day, like tomorrow I got like three big cases.
Dr. Daniel Acevedo: And so like, it's fun to just, to just come, like come in and like hang out with Sharif and [00:36:00] whoever, I guess is like, we're talking to you guys. Like we're just chilling. Like, so it's, it's fun to decompress and just be silly. So I have a lot of fun. It's it's,
Will Sanchez: it's good. It's great. BishaiI saw a couple of them and.
Will Sanchez: I forgot, I should have wrote it down Bishai but you were speaking to someone and you, you had a keepin it gangsta with golf terms. Oh yeah.
Dr. Shariff Bishai: And I
Will Sanchez: was dying. I thought it was hysterical. I've never, some of those I've never heard before. So that's a teaser for anyone that's listening. Please go check out Emmy pod star, not a doctor.
Will Sanchez: They have so many great shows and there's so many great segments. And one of my favorite is keeping a gangster because most of the time, Danny can't keep a straight face. He's just dying throughout the whole thing. AndBishai and just like Sharif said, he's, he's got the card. He's holding them up. like the word and flips around.
Will Sanchez: If you get it right or wrong, it's just whole great segment. And obviously it's well produced. So congratulations to the both of you for, you know, one having fun, right? Let's just start right there. Just the way you alluded to that. [00:37:00] This is kind of a break into your normal daily life. And now all of a sudden this has turned into something that people resonating because they could tell you having a good time.
Will Sanchez: You're having fun with, with what you're doing and you're entertaining and you have incredible guests that are coming on. Just like you mentioned that, you know, you have a golfer and you have someone from the Pistons and you have a doctor and there's just, it's great. It's, it's really, really fun and I really enjoy it.
Will Sanchez: So I just want to personally say congratulations on the podcast and Bishai I look forward toBishai listening and watching
Dr. Shariff Bishai: it. Well, the good news is you guys are going to be guests on our show soon. So that's going to be a lot of fun. Cause I'm going to, I'm going to break Grant out of his Dr. Garcia. We're going to come up with Something for
Will Sanchez: G money.
Will Sanchez: I'm
Dr. Grant Garcia: ready for it. I'm gonna have to, I'm gonna do some calisthenics beforehand. I'm ready.
Dr. Shariff Bishai: We might, you know, you don't know if you're keeping a gangster or might be in like a pushup contest with us. Who [00:38:00] knows ,
Will Sanchez: that's, oh, I, I, I saw that one. I, I, Danny, didn't you have an issue there? You got challenged to a pushup contest at what was at a conference or something like that?
Will Sanchez: Yeah, it was like
Dr. Daniel Acevedo: two in the morning out. It was two in the morning and we were coming back from, we were hanging out all night. And then like, Paul's like, push up contest, like it's down. So then I was doing push ups and I was like, watch me do these plyos. And I just kind of like missed and hit my
Dr. Grant Garcia: face.
Will Sanchez: I saw that one.
Will Sanchez: Sharif went at you pretty good with that one. I was like, Oh man. So yeah. SoBishai push up contest that, thatBishai that'll be a good one. So we got to find a great nickname for Dr. Garcia, double G something along. G Money. Yep.
Dr. Grant Garcia: I like that one too.
Will Sanchez: So we got, we got a couple of good ones. Listen, I know it's getting late.
Will Sanchez: We really appreciate your time, especially being on the East Coast. And SharifBishai real quick, I see Detroit Lions helmet in the back. We got some stuff going on. We got a big matchup. [00:39:00] Matthew Stafford is coming. I don't know, I would say coming homeBishai to go against the lions. So this, I find it extremely, there it goes.
Will Sanchez: We were seeing an autographed helmet from, from Stafford. AndBishai what, you know, what are your thoughts? I mean, he's coming back, they made the trade. We thought it was kind of, you know, maybe one sided. And now both teams have really benefited from this trade. And now it comes down to this playoff game where whoever wins or loses, it's.
Will Sanchez: The conversation is going to be extremely
Dr. Shariff Bishai: interesting. Yeah, I think Detroit's begging for this. I mean, it's been 30 years since we hosted a playoff game, which is insane. I mean, I remember back in the nineties when that happened andBishai where that was, was that the Pontiac Silverdome, which is now an Amazon fulfillment center.
Dr. Shariff Bishai: Bishaithey knocked down that building and built that. So you can tell that it's been a while now from the standpoint of these lines, I think, first of all, Decker reported. So [00:40:00] we'll just leave that. Okay. And then I'll say that. So we should have won a Dallas. However, I think it was good that thing lost because they, this Dan Campbell team is really interesting.
Dr. Shariff Bishai: I mean, when he came out originally and he showed up in Detroit and said, we're going to bite kneecaps and we're going to claw and appeal to the press conference. Yeah. He's like, what the hell? But now you realize what he was talking about. It's like, we're going to be blue collar. We're going to just, you know, We're going to work hard and that's what they've done.
Dr. Shariff Bishai: I mean, when he came out originally and he showed up in Detroit and said, we're going to bite kneecaps and we're going to claw and appeal to the press conference. Yeah. He's like, what the hell? But now you realize what he was talking about. It's like, we're going to be blue collar. We're going to just, you know, We're going to work hard and that's what they've done.
Dr. Shariff Bishai: So I think with Stafford coming back, who is great in this community, I got to know him when he was here. I did a lot of work with one of the rehab places here. And so he's just a good dude. His wife is great and just a great family. And he still comes through Detroit whenever he gets a chance. So the problem is he's the enemy this time.
Dr. Shariff Bishai: So it's going to be weird to, to, to see him like that. And they've actually banned people from wearing Detroit lions, Stafford jerseys for the game. So you can't, if you're wearing it, they won't let you in, which is crazy. Bishaibut I think it's going to be great when loser draw, I think. [00:41:00] The Lions have turned the corner.
Dr. Shariff Bishai: They're going to be a presence in the NFL for a while, at least in the NFC North, and we'll see.
Will Sanchez: Bishaiit's going to be a, it's going to be a great game. It's one of thoseBishai if you're a Lions fan, I would think that you want to see Stafford play well because he meant so much, but still go home with an L. So that would be my thought on that
Dr. Shariff Bishai: one.
Dr. Shariff Bishai: And so Danny and I got to figure out what our bet's going to be because he's in LA and I'm in Detroit. And here we go.
Will Sanchez: Danny, what's, what's the bet here? Push ups?
Dr. Daniel Acevedo: I don't know, I don't like betting money, I'm cheap. I would rather do push ups.
Dr. Shariff Bishai: Late night push ups. I got it, I got it. If I win, so if the Lions win, Danny has to eat red meat.
Dr. Shariff Bishai: And then if, and if he wins, then I'll go vegan for a week. What? No,
Will Sanchez: I don't
Dr. Daniel Acevedo: want to eat
Will Sanchez: meat.
Will Sanchez: Sounds like a little kid. I don't want it. No, I don't want that. [00:42:00] Dr. Garcia, any final words before we let this gentleman go?
Dr. Grant Garcia: Dude, thank you guys so much for being on here. This is awesome. Hopefully the listeners really enjoy this. I'm looking forward to letting loose at the next one. It'll be
Dr. Shariff Bishai: good. Yes. Grab your favorite drink, sit down, enjoy.
Dr. Shariff Bishai: Just to remind
Will Sanchez: everyone, it's Dr. Daniel Danny Acevedo, aka Cuff Daddy, Dr. Sharif Bashe, aka the American Gangster, and check him out, I'm a pod star, not a doctor. Please everyone, check him out. Thank you for listening to the show.Audio Transcript
Guest Lia Winters: Easy Whip Inventor

Will Sanchez: [00:00:00] Welcome, everyone, and thank you for listening to Sports Doc Talk. Please check us out at SportsDocTalk. com. It's a great website. We have a lot of information. Dr. Garcia has some great references. You can check out transcripts from our shows. So, really, we want you to go there and check out our website.
Will Sanchez: And, once again, I always remind our listeners, We are on every platform that you can think of, Apple, Spotify, Amazon, you name it. So please, whatever's your favorite listening platform, go check us out. I'm Will Sanchez, along with Dr. Grant Garcia, you know how we like to do. We talk all sports, all orthopedics, all the time.
Will Sanchez: We have a great guest with us today. The Leah Winter from Winter Innovations, co founder and CEO. We're going to get to her in a moment. But before we do that, let's bring in our orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia. Happy [00:01:00] holidays. How are you? And maybe the kids aren't listening.
Will Sanchez: Have we taken care of, you know, some of the holiday goodies for the kids?
Dr. Grant Garcia: So I'm doing good. Happy holidays to you as well. You know, always orthopedic surgery end of the year is busy, but we're looking forward to the holidays and If the kids aren't listening, yes, everything is good so far, and I think Santa's gonna come in hot this year, so we'll see.
Will Sanchez: That is great. , Dr. Garcia, please bring in Leah Winters, as you introduce her, tell, tell me, what really excites you about this conversation about this guest for our show today?
Dr. Grant Garcia :So, you know, Leah Winter, we're gonna talk to in a second, and she's, again, the CEO and co founder of Winter Innovations.
Dr. Grant Garcia : And you can hear the word winter is in her name. So obviously she's the founder and I think you know, we had our most popular episodes are so far has been napkin to reality We had so many listeners on that and we talked about taking the napkin idea And taking it all the way to the product line and I talked about a few companies [00:02:00] that took large products on a large scale and that takes a lot of people.
Dr. Grant Garcia : This is somebody who did this with basically 1 person working their way up and very impressive person, but also she's going to give us more details that we miss because we're always open to correction. So this will be great, but I thought it was an excellent option. And again, an innovation orthopedics.
Dr. Grant Garcia : What the listeners should understand is that it's easy to tweak something small or to tweak a, you know, go up to a brand new product, but she, she found a way to make a stitching unit smarter, faster, better, which is incredible to find a niche in a product line, such as that. So she took a very innovative approach, excited to talk about her journey, her product and the future.
Dr. Grant Garcia : So with that, with that, I'd like to introduce Leah Winter.
Lia Winter: Thank you so much, Dr. Garcia. You're so kind. Really appreciate you giving me the opportunity to be here. Excited to dive in.
Will Sanchez: Leah, you know, we, I was listening at your [00:03:00] story and please go check out Leah's website I was on your LinkedIn page snooping around and I saw a great little piece that they put together. And I see that some of that inspiration and I want you to kind of talk about this was you mentioned that when you were 16 years old, your mom.
Will Sanchez: tore her ACL, and unfortunately, she had to have revision surgery 10 days later. And a surgery and a recovery that should have been a lot shorter took her almost two years. How did something like that become so impactful and lead to where you came up with this idea for your technology?
Lia Winter: I love to talk about this because for so many entrepreneurs, their family and experiences that their families have lived or experiences that they have lived themselves end up being the passion and drive behind the new products and innovations that come out.
Lia Winter: So exactly like you said, my mom tore her [00:04:00] ACL while she was at the gym playing volleyball with her friends. This was when I was about 16 years old. She had a world class surgeon do her ACL surgery. But there, as a lot of the listeners know, there are a lot of steps, a lot of technical details in the surgery.
Lia Winter: And unfortunately her surgery had to be revised 10 days later, which meant she went under the knife again. So what typically is a six month recovery. Recovery for ACL surgery became two years for her. So, I, I kind of knew from that experience, and again, I was young, younger here, but knew that if a surgery doesn't go right the first time, what happens to a patient and how difficult that journey could be because I saw my mom live it herself.
Lia Winter: So, fast forward a few years, I was an athlete in high school and everything, and like many orthopedics industry. Went through my own orthopedic injuries, had treatments, and that inspired me to become a biomedical engineer. And during my [00:05:00] biomedical engineering training, I had the opportunity to do research and development.
Lia Winter: I was always drawn to sports medicine. So there was a day in the lab where I was doing an R and D project on ACL grafts and how they were stitched. I had to sit there for six hours with products that were currently out there and figuring out. out how to stitch the grass and then biomechanically test them.
Lia Winter: And I know Dr. Garcia talked about this a little bit on NAPKIN to reality. So during this testing, there was a moment where it really stuck with me about The needle products that were used to stitch were very tedious for me to use. Then as my my R& D project continued on I started watching surgeons come into the lab and and Saw that stitching really was a bottleneck in the surgery So this experience helped me realize that from a technical side There was an opportunity to improve and then from the personal side my mom and her experience really stuck with me So those two things really were were my inspiration behind Starting my company and coming up with the [00:06:00] idea for my product.
Dr. Grant Garcia: I think this is an excellent point, which he's bringing up. I think from an orthopedic standpoint, it's important to hear this. Cause the listeners are like, well, you know, stitching, tell me more about it. You know, what happened to your mom is incredibly unfortunate. And when the stitching, you know, we, a lot of things we do and how most of my ACLs, at least half of them.
Dr. Grant Garcia: There's a stitching component that's not built into the system that we're stitching and sometimes you can see when you're stitching the way the tissue is the way that the biomechanics of it are done is there can be a little bit of cut out and what cut out for the The listeners and again, we're not going to go into the engineering component is that you can kind of split the tissue.
Dr. Grant Garcia: Again, you want to keep the goal is you want a stiff construct and you want the sutures to be built into the tissue. But sometimes the needle itself you guys can think about it like imagine you're, you know, you're trying to you're passing something you have to make a hole in it. And so if you make the whole inappropriate direction, or you make a certain type of stitch, you can actually cut through the middle, and that can [00:07:00] cause those problems you're talking about again, it's not common.
Dr. Grant Garcia: For that particular issue that your mother dealt with, but it's obviously catastrophic and enough to someone like you to change the way you're doing your course and your path. And so it's really important to have this down because again, I've heard on my podcast before, but our margin for error should be zero.
Dr. Grant Garcia: And so that's why innovations. It's so important.
Lia Winter: Absolutely, yes, Dr. Garcia. And if it might be helpful for the listeners, I'd love to share a little bit of background and context on ligament and tendon surgeries, because I know that you do have a pretty wide range of listeners. So just a little bit of background.
Lia Winter: These ligaments and tendons are the soft tissue structures that are either connecting bone to bone in the case of a ligament. Or muscle to bone in the case of a tendon. And unfortunately these tendons can tear when too much force is put on a joint. And a lot of people are familiar with these things from sports and they can happen in many different areas of the body, but it's not just athletes.
Lia Winter: Every day, [00:08:00] people can experience these injuries, the weekend warrior. These are things like ACL tears. biceps tears, Achilles tendon tears. And I think these are hot topics, especially for sports medicine surgeons. I mean, this is your bread and butter, Dr. Garcia. And I know a lot of your listeners have heard of some of these from your recent segments.
Lia Winter: So like, for example, Nick Chubb and Aaron Rogers but. For the most part, severe tears require surgery, and most of these ligament and tendon surgeries actually require stitching of the tissue. The surgeon is taking sutures, which is a fancy word for medical grade string, and passing them through the tissue with a needle.
Lia Winter:So, for example, for, we talked, I mentioned Achilles. For Achilles tendon surgery, a common approach is repairing. Where the native tissue is sewn back together for something like an ACL surgery. The common approach here is to reconstruct it. And this is where [00:09:00] tissue is taken from another part of the body.
Lia Winter:A lot of times this is called a graft and the graft is stitched before this construct is implanted into the knee to replace the old torn ACL. And that's the kind of surgery that that my mom had. So I think before we talk about stitching. It's important to understand the overall context of the surgery because it, it is quite a simple thing, but it does have a big impact on the overall steps, especially in ligament and tendon surgery.
Lia Winter:So, Dr. Garcia, would you like to weigh in on that at all?
Dr. Grant Garcia: Yeah, I mean, if the part, if the listeners want to hear how important this is, this week, I will probably do this stitching technique and I'll probably do stitching overall, probably 10 times. So, that's ten times in one week, multiply that by 52 weeks, and again, you know, this, it changes sometimes, sometimes it's four times, but I don't think I'd go a week without doing stitching like this.
Dr. Grant Garcia: So this is an everyday thing that we deal with. And and again, I'm a sports surgeon, so I probably see a higher volume of things that require to be [00:10:00] stitched, but flexor tendons for hand, you can talk about other knee ligament tendons, a lot of ankle tendons we can talk about. I mean, again, Leah is making this as simplified as possible, but there are more tendons that we fix with these types of stitches than we had fingers on her.
Dr. Grant Garcia :Fingers and toes. So it's really important to understand that.
Will Sanchez: Yeah, I'm sorry, go ahead. Go ahead, Leah. No, go ahead, Will. No, I was just going to say, just to let the listeners know, as I'm listening to all this tendons and sutures and everything else, and I've kind of gone through my ruptured tendon. So I have a cast on right now, and luckily I had a great surgeon.
Will Sanchez: One of the surgeons that was actually on one of our shows. Dr. Anthony Yee performed that. So when we're talking about the sutures and the stitching and everything else, I am the example. You two are the doctors, and I'm the example here. So if we were in a room, I could just show up my leg and just talk about really the importance of it and having that [00:11:00] assurance of of that.
Will Sanchez: that suture to really kind of hold things in place so these, tendons can unite and start to heal. And all of a sudden, you know, for us weekend warriors, go out there and have some normality as we were joking before we started the show so my wife could get some peace because right now she's holding down the fort at home and it makes it very difficult.
Will Sanchez: And I was thinking about your mom where you mentioned. what she went through, not only the strain that it puts on her physically, but what it does to her emotionally, mentally, and what it does to the rest of the family, just because she had such a difficult complication, how that can be inspiring for something that you have created here.
Lia Winter: Exactly. Yes. That's definitely my story and inspiration. What keeps me going forward and Why I love doing what I do with Winter Innovations.
Lia Winter: So if I may, I would [00:12:00] love to share a little bit more specifically about what Easy Whip is and how it solves some of the problems that I observed through, one, my mom's patient story, but two, the technical things that I observed as a biomedical engineer. So Easy Whip really is the first and only two part needle for stitching in orthopedic surgery.
Lia Winter: We have some really good graphics and videos on our website if anyone's interested to see how the product works. But for listeners, think a needle within a needle, that's what a two-part needle means. So these two portions are attached to opposite ends of a length of suture. So again, medical grade string.
Lia Winter: So when they're connected, the suture is a loop. But when they're separated, it's straight. This is a really simple change to conventional needles, but it drastically changes how stitching can be done. With Easy Whip, it can be used to create a traditional whip stitch, and this is where the product gets its name, Easy Whip.
Lia Winter: And we also have a new patented stitch method, which we call the [00:13:00] Whiplock. This adds additional strength to the stitch, and surgeons can create hybrid patterns based on the needs of each patient and surgery. So really, a more custom approach. And then in addition to the versatility and strength benefits, it can also save time from avoiding extra movements and reducing the number of needle holes through the tissue, which Dr.
Lia Winter: Garcia was talking about how important the placement of the holes and making sure the tissue integrity stays intact, how important that can be. And I would add
Dr. Grant Garcia: to that, again, I whip stuff all the time. The contracts we currently have are a fixed loop, so they imagine a fixed loop. So if you want to pass it through, you gotta have another assistant that uses, that releases their hand and passes it through.
Dr. Grant Garcia: It's a, it's an art. It's like a ballet in the operating room. And sometimes it's challenging. And you have a needle flying around all the place. So it becomes challenging. With this technique, you don't have to ever do that. The, the tendon stays straight. And [00:14:00] as you release it, I've never seen a double needle like this before until I got to see yours.
Dr. Grant Garcia: So it was really, really cool. And the idea that it works so functionally well and the way it stitches, but that hybrid thing she was talking about is really, you know, the whip is amazing. But the hybrid technique is honestly the game changer in my opinion, because you can really do this special locking stitch with it.
Dr. Grant Garcia: And so that reduces, if you pull hard enough on these other, some of these other techniques, you will see the tendon get cut. Again, it doesn't happen all the time or we'd have a lot bigger problems, but enough to cause traumatic things such as your mom's issue and so this sort of lock stitch is really what excited me the most about the product and it's really cool that you can do this and it's basically technically, technically dependent, right?
Dr. Grant Garcia: Because, you know, we could do all different things with the same stitch. Is that correct?
Lia Winter : Yes, yes, the same product. So the surgeon can decide based on the needs of each patient in each case when they are about to create each individual stitch, what is most needed, a locking [00:15:00] stitch or just a simple traditional whip stitch.
Lia Winter : And overall, that kind of depends on the case. And The overall context of the surgery, but really a lot more versatility. And I exactly like you said, Dr. Garcia, that's what's resonating with surgeons the most and getting them really excited about using our product.
Dr. Grant Garcia: And it's good for the, I want the listeners to hear this again.
Dr. Grant Garcia: It's just really impressive. You know, this is a, this is like she reinvented the wheel. Like the stitch is so common and this stick technique we used to use before is like everywhere. And she found a way to have an innovative product on something that is time tested for so long and have it be, make it better.
Dr. Grant Garcia: And as soon as you see this, you're like, wow, that is a lot better, but you don't realize it until you see it. So this is one of those things that I just, that's why I'm so excited about having her on here. Because I just, I want everybody to hear the brains behind this. And honestly, too, the, you know, the personality type of you is, is going to be great for the listeners to hear how this happened.
Dr. Grant Garcia: Because it's, this is not [00:16:00] often that we get to meet someone like this. Yeah.
Will Sanchez: So Leah, we talked about your mom being inspiration,
Will Sanchez: but who was your inspiration for you to say, Hey, you're on the right path. You're doing a great job. pretty sure like anything , doubt kind of may creep in or am I heading in the right direction? But that person that motivated you because I can see that you're in a position now where you can motivate our young folk and young people that are involved in the medicine field.
Will Sanchez: So what are your thoughts on that? There are a
Lia Winter:lot of people who have helped me along this journey. And I would say being an entrepreneur is very hard. So a strong support system of people encouraging you, helping you find the right resources is so critical to the success. So I, a little bit more context.
Lia Winter:I my background is in biomedical engineering and I started my company when I was in graduate school at the university of Tennessee, pursuing an MBA and a [00:17:00] master's of science and biomedical engineering. I, I. engineering foundation, but realized that in order to understand how the products I was researching were actually impacting patients and the business overall it would help to add business skills to my engineering foundation.
Lia Winter:So it started out when I was in graduate school and I wouldn't say I really set out to start a company from the beginning. I Looked at the resources provided by the University of Tennessee and was, became aware of the entrepreneurship program at the university and kind of said, well entrepreneurship would be a good thing to combine business and engineering exactly the way I say I want to.
Lia Winter:So I decided to start getting involved in the Entrepreneurship Club on campus. And I had a friend and a mentor who said, you know what, it would be great if you pitched your idea for EasyWik. So EasyWik had started out as a Class project at one of my engineering classes. And they said, if you, it would be great [00:18:00] if you pitch this in a competition, kind of like shark tank and started preparing your kind of business skills, but putting the legs underneath of this idea to actually make it become a reality.
Lia Winter:And I, I said, I'm an engineer. I don't like talking in front of people. And it was just that I hadn't learned or practice those skills and decided really to rise to the occasion, enrolled in my. First pitch competition, which was 90 seconds. So I think shark tank, if anyone has seen the the show but basically you get up there, talk about the idea and I won first place and 1, 500.
Lia Winter:And the next day I took that money and got a business license and officially. It was started off as a sole proprietorship, but that really was the beginning. And continue to do pitch competition. So ended up winning about 30, 000 from the university of Tennessee, and then looked at the broader resources and realized there was this thing called the pitch competition circuit with a bunch of universities that host pitch competitions and.[00:19:00]
Lia Winter:Traveled around the country my last semester of graduate school to the University of Louisville, the University of Georgia, and kept winning all of these pitch competitions. So I had about a hundred grand in funding by the time I graduated. And that's when, again, some family and mentors said, you have something here.
Lia Winter:You really should go ahead, try this see if we can make it into an actual commercialized product and company.
Dr. Grant Garcia: That's amazing. I do want to chime in here. So I got to tell listeners his background on Leah because this is, this is going to be awesome. So Leah is saying she's, you know, shy engineer trying to work on her pitch competition.
Dr. Grant Garcia: So Will can tell you this because Will was one of the. You people I responded to on LinkedIn who asked me to do podcasts and now we're at three plus years later. We're doing this awesome show But I get probably five messages a day From about products for people either from an investment side to try my new product out and pretty much delete all of them So we're talking about over a [00:20:00] thousand messages Leah is the only message I've ever seen and I still am surprised how she did it.
Dr. Grant Garcia: So she sent me a personal video Telling me that about the product and ask and with my name on it and everything else I've never seen that before in like the last five years and I I showed to my partners I was like check this out and immediately responded back to her The first thing I think I said to you leo was i've never seen someone Now again I'm not telling anybody else on LinkedIn, I'm not going to respond to your messages just because you do this video now, but I've never seen that before and her pitch was awesome, so I'm she had me at that.
Dr. Grant Garcia: And so that's why again, it's also, I just remember that as we're talking. And so I think she, I think she's gone a pretty good ways from an engineer just behind the scenes. Well,
Lia Winter: Like everything you guys were talking about was so true. So research Dr. Garcia [00:21:00] on LinkedIn, sent him that video, flew across the country to meet him in person and do a demo with easy whip. And now here I am. So I love that this story has come full circle.
Will Sanchez: It's awesome. That is amazing.
Dr. Grant Garcia: So let's tell us what we got wrong with Map into Reality. Again, in the nicest way possible, obviously. No, no, no.
Will Sanchez: Go for
Dr. Grant Garcia: it. Go for it. Tell me your journey. I want to hear your journey. And I might chime in on some things, but you know, I do a little bit of IP. Again, I'm a surgeon by most of the time. You are the expert.
Dr. Grant Garcia: You are the, this is the reason you're on this show is you've gone the whole way, and you know more behind the scenes than anybody I know. So tell us what you had to do to do this. I want the listeners to hear this. This is what it takes, guys. So this is going to be interesting. So go.
Lia Winter: Of course. Yeah. So just a really high level overview of our company.
Lia Winter: So graduated from the University of Tennessee in 2019 and officially founded the [00:22:00] company, became a full time entrepreneur. The first thing we did when we graduated, so I teamed up with my co founder, this is when I start talking about WE. We did an accelerator program so an amazing resource for startups that are actually trying to go forward with the next steps of their company.
Lia Winter: It's called Zero to 510, and it's in Memphis, and it's a play off the name of the 510 and the 510 K, which was discussed a lot in Napkin to Reality and the pathway that WE took, so we'll talk about that a little bit. So did that accelerator help set us up really well to prepare for fundraising? So we got tired of living big check to big check and pitch competition to pitch competition.
Lia Winter: So raised our first round of investment funding in 2020. Use that to put towards all of the testing necessary to get clearance from the FDA through the 510k. And that went through in 2021. And then had our first surgery in the very end of 2022. So that's just kind of a high level of where we've been and what it's been [00:23:00] like, and a lot of work and steps have gone into that.
Lia Winter: So I kind of mentioned that for me, what made this a reasonable journey and gave the motivation and inspiration was just breaking it up into individual steps. And so one of the things very early on, someone said, after I won a pitch competition was. You need to get a patent to protect your idea. Dr.
Lia Winter: Garcia talked about a lot of different pathways You can partner with a larger big company or take the path that I took and start your own company regardless protecting the invention is the key first step So I, I really remember it was again, we were just winning pitch competitions and scraping together the first capital.
Lia Winter: I was on the phone with our patent attorney who had just finished the application and it was ready to submit, which means the fees hit and everything. And I remember our patent attorney telling me. Patents are like potato chips. You can't have just one and I was on a call, but I kind of like I made a face He couldn't see me, but that's [00:24:00] crazy.
Lia Winter: I we barely have enough money for one. Well fast forward We now have a patent portfolio that has three u. s. Patents 13 international patents across the country. So this, that advice that I got really early on has been critical to building value from the earliest stages for our company.
Dr. Grant Garcia: I think that's important for listeners to, you know, there's two routes.
Dr. Grant Garcia: Leah took the higher risk. But higher reward and harder work, right? There is partnering with companies where you have a smaller chunk of ownership of the patent, you know, maybe, you know, hopefully some ownership and that's what a lot of the orthopedic surgeons do initially on but what Leah did is a different animal.
Dr. Grant Garcia: And so it's good for you guys to hear this because that's really neat. That's a less common route especially to get all the way to the success level she did. I mean, each one of these, she could fail and she found a way not to. So sorry, keep going.
Lia Winter: So true. And again, it goes back [00:25:00] to some amazing people that we worked with and, and we'll talk about that a little bit more when we specifically get to maybe the FDA and five 10 K, but before we could even get to that right.
Lia Winter: We had a, a patent to protect the idea, the innovation. And the next thing was how do we go about even making the product? And I, I always laugh, the first versions of Easy Whipp were hand-built prototypes. I was ordering things off of eBay, finding other sutures on the market that I could find that were maybe expired or, or things, purchasing those, ordering needles, and hand milling them on a, a mill, and drilling, and just to have feasibility prototypes that we put in the hands of surgeons, like, Family friends that we knew other surgeons in our network and said, Hey, how's the size of this?
Lia Winter: What materials does it have to be made out of? And that was a big step to start actually talking about the device and Not being so proud that it had to be perfect to get it in the hands of a surgeon. I think that was a really [00:26:00] good step that we took early on was to just get what we call a minimum viable prototype or product and get it in the hands of a potential customer to really get feedback early on and make sure how the device is being designed.
Lia Winter: Is built for the surgeon and something that, that can bring value and benefit. So those early prototypes really were important. And then it was getting the attention of a manufacturer and being a startup and asking about their capabilities. And when we said, Oh, our first run, we're thinking maybe a thousand and manufacturers laughing and saying, we heat the machine up, it warms up and it makes a thousand thousand sutures.
Lia Winter: So. Finding a manufacturer that had the capabilities. We just tapped into our network and started pitching not as much the business case, but also the inspiration behind it. And then we found an amazing manufacturer that just makes surgical needles, a really specialty niche in the market, if you will, that was a critical step early on to making sure we [00:27:00] succeeded and passed all of these tests and necessary steps like.
Lia Winter: Dr. Garcia mentioned is so important.
Will Sanchez: Absolutely amazing. Just because it sounds like you've been slacking for the last couple years what are the future goals for the company? What, what's your vision down the line or at least hopefulness for winter innovations? Yes.
Lia Winter: Yes. So right now, I would say a lot of the focus is on growing our customer base, getting new, innovative surgeons who are excited about new technology, looking for partnerships to get easy, efficiently into the hands of as many surgeons as possible and doing that at a nationwide scale.
Lia Winter: So those are kind of the long term business goals, and I'd say on the research side of things. We recently won a grant from the government. It's called a small business innovation research grant. It's a million dollar grant from the National Science Foundation, and that will fund product expansion as well as cadaver studies and biomechanical testing, which I know was also a big [00:28:00] topic in the napkin to reality.
Dr. Grant Garcia: Yes. Will you go, will you go through your, you know, again, briefly your 510k you had to go through so that the listeners can hear this again. Again, this was our most popular episode. So hearing this from someone who's gone through it is going to be excellent. And then maybe, you know, shoot down to some surgeries that weren't the first surgeries like
Lia Winter: Yes, yes.
Lia Winter: So the 510k pathway, again, just a quick summary. This is the expedited pathway for products that are currently out there, but might have a different tweak. So sutures are products that have been on the market. So we were able to use this 510k pathway. I think you talked a lot about biomechanics testing, which was a really big part of it.
Lia Winter: We did have to present that data to the FDA, but even before that just everything, I think additional context that goes into making sure a device is safe and effective. We had to do sterilization testing, make sure the product was sterile and clean for it to be open in the OR. [00:29:00] We had to do Testing on the packaging to make sure that even after it was shipped halfway across the country, the packaging still stayed intact and the product was still sterile.
Lia Winter: We had to do biocompatibility testing. We had to do manufacturing process validation. And then once all of that was finished and proven, we did additional biomechanical testing. So looking at the different stitch patterns. Pulling them apart, looking at the ultimate strength, all of those things that Dr.
Lia Winter: Garcia talked about in Napkin to Reality. We took all of that work and put it into a 510K, which really is your case to the FDA for why this product is safe and effective. And our 510K, and this is a pretty simple product, it's again a suture, was 1000 pages long. So it's a lot of work that goes into this preparation.
Lia Winter: And this is also a fun fact is that in order to actually get this submitted to the FDA, we had, you have to mail them. The submission on a flash [00:30:00] drive. So that was something that was funny when we were ready to submit and our our regulatory expert told us that's how it's actually done. So our 510k went through the FDA in less than two months, which is, which is really fast, especially for a startup.
Lia Winter: Most take about six months. So that's a metric that we're really proud of. And again, we worked with some great testing partners and manufacturers to help make that
Dr. Grant Garcia happen.
Will Sanchez: Awesome. Absolutely.
Dr. Grant Garcia: Go ahead. Yeah. So again, And for listeners, this is a, this is really impressive. So I think, you know, but you hear all these steps, right?
Dr. Grant Garcia: So she's gotten all the way to the FDA, but all your products can be great, but how do you present it to the surgeon? You know, I may seem like a chill guy, but sometimes if I'm, you know, not interested in something, I'm not always going to look at it. And there's a lot of other different personalities in the operating room, which we'll be able to tell you.
Dr. Grant Garcia: And so you got to work with all these different surgeons who may have their own personality types, or you got to have these surgeries that go [00:31:00] perfectly. And sometimes you get one shot. And so, you know, those first surgeries are important for your testing, but also just for your confidence. And so, so how did that go?
Dr. Grant Garcia: And then obviously we'll get to the next level, which is, you know, trying to talk to other surgeons and how did that approach go and, you know, your, your future stuff.
Lia Winter: You are so right about the different personalities of surgeons and all are so busy. So getting their attention, we were fortunate to have a very excited surgeon to be the first user of our product.
Lia Winter: So the approval process, getting it in, it all went very smoothly. I almost say we were spoiled for the first case, but I will say being in the OR for that first surgery was honestly the proudest moment of my life. I was able to see a product that I, I came up with this idea and it was being used for the very first time to help not only a surgeon, but most importantly, a patient and have been really fortunate to be in a lot of cases with easy whip now and every time, again, it's that same feeling.
Lia Winter: And when I hear a surgeon utter the value [00:32:00] proposition that I've pitched so many times or in my sales pitch, when I, I hear either the surgeon or the PA, whoever's stitching utter those words out of their own mouth, like, wow, this really was easier. I felt like it was a stronger repair. I'm not worrying as much about the tissue ripping.
Lia Winter: That's what makes all of the hard work and steps worth it. So we do have to work really hard to get the product in front of other surgeons. Some of those creative things, like I said, Dr. Garcia's example of Doing personalized videos one by one, researching our surgeons, social media has been really important for us, we've started going to conferences like the American Academy of Orthopedic Surgeons or sports medicine conferences, things like that and, but I would say the thing that's The best is referrals and testimonials from our, our happy surgeon customers that definitely goes the furthest.
Lia Winter: And so we try to really make sure those first cases go well. Like Dr. Garcia said, you have to make sure it goes right. And so I will a lot of times travel and go to the first [00:33:00] cases and help build the relationships with the surgeons and make sure it goes
Dr. Grant Garcia: smoothly. This is so important. I think the listeners should this is going to be our longest podcast ever, this is so exciting.
Dr. Grant Garcia: So the This is really important. I mean, this is something I do on it for all the, a lot of these companies I work with, you know, and again, I'm different than Lia. I'm a surgeon. She's trying to show her product off. Surgeons are skeptical and some, and there's some that want to do innovation, but there's a lot of people that want to be careful and it's fair enough.
Dr. Grant Garcia: Again, you don't, when something goes wrong, it's not good. Or if you're doing something and it, it ends up being not the result you wanted with the new product, it's stressful. And there's, there's previous history of products like that. Again, this is different, but there's still that concern that some surgeons have.
Dr. Grant Garcia: And so, you know, when a testimonial of another surgeon is like, this is amazing, you know, that goes a long ways, like she said, and you know, the fact is that she's excited about it. She's smart. She could talk all these things. Those are all really important because that's not the commonality. And that's [00:34:00] why she's gone so far, because I'm sure there are a lot of smart people out there.
Dr. Grant Garcia: I'm sure there are a lot of engineers out there. But you have to have the full combination. And again, it shouldn't deter you if you don't have those. Check all those boxes. But it is interesting for the listeners to see. This is not, this is a full package thing. It's like, you know, these athletes we talked about, right?
Dr. Grant Garcia: They're not just good at one little thing. They have all these things going for them. And the one thing that Leah said that she was worried about initially was her ability to pitch and talk in front of doctors or talk in front of people, and she's clearly mastered that. And so, the point I'm saying is that you don't have to have everything to start.
Dr. Grant Garcia: But you should, it's good for you to listen to mentors and be humble and understand like what it takes. You know, I came out of medical school, my comfort level is not nearly what it's like now. And talking in front of people or talking to, you know, I was just at a teaching event and half the people were older than me by 5 to 10 years in terms of surgeons.
Dr. Grant Garcia: And so that takes a lot of guts for me to try to go out there and try to teach somebody else. And so it's the same type of thing. And so it's really important to understand that like, you have a [00:35:00] purpose here, you know, you're not, and this is not threatening, you're trying to help everybody. And if that's your intent, things are going to go a lot better.
Dr. Grant Garcia: And that's the way that Lia presents herself. Yeah,
Will Sanchez: Lia would have had me if she would have had on subject title I had this great in invention called Easy Whip. Just the name alone, I would have like, I gotta check this out. Because it's like a cool 80s music video from Devo. So I love the name.
Will Sanchez: Easy Whip is awesome. Well sold
Dr. Grant Garcia: already. You don't even need to
Will Sanchez: do any product testing. No, no, I'm sold. I'm sold. The name of my invention is called Easy Whip. I was like, okay, this is awesome. So great job on the name. . I know we're going to wrap it up soon. I, I want to do a quick little rapid fire thing with you.
Will Sanchez: We're going to call this, you know this, that, or, we'll send it to the rack here. All right. And you're from the university of Tennessee. So tell me Peyton Manning, Pat Summit, or someone else when you think about the The Vols. Oh, [00:36:00]
Lia Winter: that's a tough one. I'm going to have to go with Peyton Manning.
Lia Winter: Or Dolly Parton.
Will Sanchez: Oh, there you go. Country singer. Did Dolly go to Tennessee, to University of Tennessee, or just because she is Tennessee?
Lia Winter: She is Tennessee. The last UT game that I was at, she came and performed. Peyton Manning walked her out on the field, so it
Will Sanchez: was quite fun. There we go. Okay. So dry or wet ribs?
Will Sanchez: What are we doing here? Dry. Okay, we're going with the dry rub. Alright, last one and, you know, sticking with the food theme. Goo Goo Clusters or banana pudding? I know it's big in Tennessee. What are we doing here? Banana pudding. There we go. There it is. Thank you so much, Lia. Any last words for Lia Dr.
Will Sanchez: Garcia as we we wrap it up? Because if I don't stop you, we're going to keep Lia on right through the night for another three hours. I know [00:37:00] you're so excited to talk to her and she's got some great things. She teased it already, so I'm hoping that she's going to come back to the show in the future and discuss where, where the company is going and all the other great things that are happening with.
Will Sanchez: Easy whip and her company.
Dr. Grant Garcia: Absolutely. Well, guys first off, thank you so much for being on here. I'm really excited about this product. You guys, hopefully we'll get a chance to try it out in the next month or so. Just, you know, obviously things are, things are crazy over everywhere in the end of the year.
Dr. Grant Garcia: So, you know, this is a really innovative option. And you guys will be hearing from me report on it soon. And I really appreciate you continuing on efforts and telling us your story. Cause this is it's good for the listeners to hear this and they get to see the real napkin to reality.
Lia Winter: Thank you, Dr.
Lia Winter: Garcia. It's been such a pleasure. Appreciate you giving me this platform and supporting entrepreneurs like myself.
Will Sanchez: That's Leah Winter from Winter Innovations Co-founder and CEO. What a great name. [00:38:00] Easy whip. I can't wait to see where this all goes. And you know, big Dolly Parton fan there. We want to thank everybody for listening to Sports Doc Talk.
Will Sanchez: Please check, check us out@sports.talk.com. I would like to wish both of you Happy Holidays. Merry Christmas, happy new Year, however you celebrate. I hope you're having a great time with your family, friends throughout this holiday season as we get ready for a spectacular 2024.
Dr. Grant Garcia: Happy holidays, everyone.
Dr. Grant Garcia:Thank you guys.Audio Transcript
Deshaun Watson Injury: Glenoid Fracture Surgery

Will Sanchez: [00:00:00] Welcome everyone, and thank you once again for listening to Sports Doc Talk. I'm Will Sanchez, along with Dr. Garcia. First off, this show is kind of coming out of the blue. Literally, it was put together in the last hour, and less than that Dr. Garcia reaches out to me and says, Hey. I'm really excited about this injury and just to let you know, only an orthopedic surgeon would be really excited about talking about someone's injury.
So we were like, yes, we have to do it. Let me set it up real quick before we bring in Dr. Garcia. I'm going to admit, I have a fantasy football team. And I get this notification this morning, saying Deshaun Watson out for the season being selfish. First and foremost, I go, Oh man, I'm out of a quarterback.
What am I going to do? Right. That's the first and foremost. I know you fancy football players out there fans. They know exactly what I'm talking about But more importantly it was about this injury and then dr. Garcia chimes in so dr Garcia when you heard about Deshaun Watson's [00:01:00] injury And the fact that he's out for the year the star quarterback player for the Cleveland Browns that they spent a lot of money Draft picks to get what was your first initial thoughts before we talk about the injury
Dr. Grant Garcia: itself?
I mean, obviously going out for the season is a big deal and his contract was a big deal. I mean a significantly guaranteed contract after kind of a lot of dilemmas that he went through you're kind of expecting only the best. But we know how it works in the NFL, especially with high pay contracts, but you know that, and then getting injured now for the season.
I mean. You know, this is not looking like a good for the Cleveland Browns with their trade. So this is, this is pretty frustrating if you were a Browns fan. And then not to mention the uniqueness of this injury.
Will Sanchez:Yeah. And I, and I can't wait to get your take on this injury. Especially how common or.
Maybe not so common of an injury it is just so just to give the audience some context. Deshaun Watson was playing against the Baltimore Ravens had a fantastic game and [00:02:00] actually came back and won the game and beat the favorite Baltimore Ravens in that game. He injured as we found out now after an MRI on Monday.
And then make an announcement on Wednesday that watch Watson sustained a shoulder fracture during the first half of the game and continue to play before we get into the injury by him. Continue to play with that injury in the first half. Does it have any bearing on how severe it became or it didn't matter?
And before you answer that, why don't you tell the audience what exactly, actually the injury that he sustained?
Dr. Grant Garcia:The only clarification I want to ask before I answer this is this is his throwing shoulder or non throwing shoulder? This is his throwing shoulder. Yeah. First off, I am shocked that he played through the rest of the game with this injury.
So to kind of go over it with the audience, and the reason I want to talk about this is something called a glenoid fracture. There's also another name for it, which is a bony [00:03:00] Bankart fracture based off of the description by Dr. Bankart. But when you dislocate your shoulder, Or have a direct blow to it.
You can dislocate the shoulder where the ball comes out of the socket. We hear about that all the time in the NFL. And those players come back in a few weeks. You know, usually they get rehabbed or something like that. And they get a labral tear. So, usually that will heal. And maybe that goes on to mean something surgical, but not always right away what he must have done.
And again, I don't know, don't obviously know the x rays or the, any type of other imaging he had done, but he may have partially dislocated his shoulder. He may have had a previous injury that we don't know about, and he broke off a piece of the golf tee. So imagine you've got your socket, which is the golf tee, and then you've got your ball.
That's the humerus. And when you break off the golf tee, that's really bad. For a number of reasons, one, it makes your shoulder incredibly unstable. And to be honest with you, this is one of the few times I've heard about someone able to keep playing through. So he may not have had as [00:04:00] big of a fracture as I was thinking initially.
But then the fact that piece of bone broke off with it, that if you miss that. And that he goes on to keep playing for another couple weeks. This is a big problem because the shoulder has such good healing potential that basically what'll happen is if you break off a piece of the golf tee and it falls down, you can't get it back up once it heals.
Because it'll heal and turn into it in the wrong spot. That's called a malunion. So even if he is stable but the golf tee's gone, then he's at a much higher risk of re injury.
Will Sanchez:So he mentioned that you know, he quote unquote said the whole second half that he was throwing, it was extremely painful to throw the football.
And and just talked about, you know, the severity of the playing. By the way, he completed all 14 of his passes in the second half and led them to a winning field goal to beat Baltimore 33 31. If you, just in case. So, I, like you said, I can't imagine. Having the injury, let [00:05:00] alone with my throwing arm and for any football fans out there, the amount of velocity that you have to put into that ball so it doesn't get intercepted or knocked down or however far that ball travels I can't imagine what are your initial thoughts about with him playing?
I know you mentioned that maybe the fracture wasn't as severe, but still having a fracture in your throwing shoulder to compete at the NFL level, let alone, I don't know if he got hit. took any sacks, ran with the ball, hit the ground, or anything like that. What are your thoughts on just, you know, we talk about these superhumans all the time.
What's your
Dr. Grant Garcia: thought? This is a perfect example of superhuman. I don't care if it was even a small fracture. I mean, that's, this is, most of the patients that I see with this injury, there's absolutely no fracture. I mean, the last two patients I've seen with that have been almost many back in to the area.
They come in with their arm completely locked at their sides. And this is not a, this is not an injury that you see someone come in and you're finding it [00:06:00] randomly. You know, again, If it was a very small shell of piece of bone but usually they don't say this is definitely has to have surgery. So it probably was a pretty decent injury.
And he, what happened is it may have worsened from him playing, right? It could have been a small fracture that hadn't moved. And then he played through it and then it broke off more as he played through it. And that's very well could have happened with the type of forces that he's putting on his shoulder.
So yes, I mean, he's a superhuman, right? He's incredibly good athlete. And you know, be it what it may, you can think about him whatever way you want. But his ability to play through this is, just shows his level of you know, athleticism, his pain tolerance. I mean, this is, this is incredible that he's able to go on to win The game with the, with this injury.
And then, you know, we can always, I love to go into sort of the injury itself. So the, so the, my patients and people listening will understand it a little bit better because it is, it's a little different animal. But again, we talked about the golf key, but the problem is, is not the injury. [00:07:00] The problem is not that he played through it.
It's the problem is that the surgery, so this is one of the hardest things to fix. And the issue with this type of injury is we see labral tears all the time. We can talk about, I'm sure we have a laundry list of players that have torn their labrum and had it fixed. That is a technically not very challenging surgery.
You know, it's still a surgery. We take it seriously, but that's not a technically challenging surgery. When you fracture a piece of bone, that's where things go awry and in a lot of groups There's usually like one or two people even that even know how to fix this thing and even that that that's still tough You know, I've seen these types of surgeries take three four hours now again We've got newer techniques and I'll go over some stuff that we're doing now Yeah But the older version of this was to do a big open incision to find it and put screws in it The problem you have is a really small piece of bone.
It doesn't work And sometimes you damage things and a lot of people still do it that way and they struggle. And this is one of the, one of the hardest shoulder injuries [00:08:00] to fix. And so the fact is that he got this is not ideal. And then with newer techniques, we're much faster. And in the last few patients I've done of this have done quite well, but it's a bad injury.
And the number one thing I'm worried about in him is this. Again, I've had lots of wrong predictions on these players because they're superhuman, but he's going to have to have the bone fixed and the labrum, imagine like it's all going to have to be rebuilt. And I'm assuming he's going to get a surgeon that can do it arthroscopically because that's really the way to go.
I mean, doing this open, the results are just, they're not the same. You know, my patients, now I do it all arthroscopically through scopes. It's a lot more technical. But I can do it more efficiently and I get good results and keep that bone up, but I just don't know how he's going to get it done. And I'm assuming he's going to go to someone incredibly good surgeon because he's obviously getting opinions about this, but the problem is stiffness.
And a stiff shoulder in a thrower is a career ender. So I don't know if that's going to be the case. Again, I [00:09:00] don't know how bad this was. But this is really concerning because I worry a lot about a thrower when I have to do a labral repair like this. Okay,
Will Sanchez: so let's go back to what you said, right? So...
I'll start with the last thing you said. Stiff shoulder. Now are we talking about just stiff shoulder after the after the surgery? Or are we talking about something that can stay with that person, athlete, whoever it is, to have a stiff shoulder and not regain the mobility that they had in that shoulder at one point?
Dr. Grant Garcia: That is a hundred percent correct. So it's, the answer is it's not, it's, this could be more of a permanent situation. This bone heals very well. I mean, it'll heal in the wrong zip code. I've never seen one of these not heal, whether it's healed inappropriately and they come to see me at two or three months or whether, you know, once, if you wait six weeks or more on this, the person doesn't get a repair anymore.
They have to get another procedure where we actually move a piece of bone to the front of the shoulder. So it tells you how quickly you need to act on this type of [00:10:00] injury. And then at that point, if you fix them, there is a chance cause you have to, you have to take tissue and fix it back up. You can stiffen the shoulder up.
And one of my number one concerns with this injury is the stiff shoulder. A regular labral repair is different, but generally if you have to do something urgently. surgery urgently. That's never ideal in a situation with any knee or, or shoulder, right? If we have ACL tears, we usually want to wait. There's a lot of data that shows we should wait between eight and 11 weeks after an ACL tear because of the fact the knee is really stiff, unless it's an emergency, like a piece of meniscus is stuck or something else, but those patients are at much higher risk of getting a stiff knee.
This is the same way with the shoulder. And on top of that. You have a massive healing response because the bone in the shoulder is so well, so much blood supply and it's a really high risk of instability, a really high risk of your shoulder getting stiff. The good news is This type of injuries, patients have a much lower chance of re dislocating their shoulder [00:11:00] or re injuring it.
But the stiffness is much more of a concern with a guy that's, you know, what is it, 230 million contract? Yeah. So I'm pretty concerned about that.
Will Sanchez: So, some, just some, the cliff note version is this is gonna heal real fast for the most part because of the location, the blood flow. The biggest concern besides the...
is where it heals in that placement, right? And, and if it heals, starts healing in the wrong place, is that something that if it doesn't heal correctly, you have to go back in and then do a different procedure to try to put it back where it belongs?
Dr. Grant Garcia: Yes, but that's usually if you don't fix it, like the surgeon that he's going to have to do it will likely fix it back to the right spot and keep it in there, and now it doesn't always hold perfectly because these are really tough.
I mean, imagine you're trying to hold, imagine you have the side of a deck, I'll try my best, and there's a, you have a little tiny post on that deck, but it's really loose, and you can only fix it with a few little, you can't fix it [00:12:00] with a screw. You can't fix it with a big mount. You can only fix it with a few toothpicks, and that's essentially what you're doing here.
You've got to fix it the most delicate way possible so you don't break the piece of bone because it's so thin, but you want to get it to hold up in the pedestal. So we have new technology using Arthrex technology and other technology that we actually use that we now can fix it without using any, any screws or anything like that.
So I can do this all minimally invasive. I'll give you a picture of one of my One of these patients, you'd never know they did surgery on them because everything is hidden. It's all these really minimally invasive, really low profile, brand new sort of anchor constructs, but it's still the concern is the stiffness that we talked about.
Will Sanchez: What is something that a surgeon would have to look for when you're putting, let's say, these suture anchors in if, most likely doing orthoscopic? Is it the amount of tightness, or putting it in the right place, or am I just kind of overthinking this at this
Dr. Grant Garcia: point? You are not overthinking, but the hardest part is just getting this piece fixed back.[00:13:00]
Because this is gonna, it moves around, it's very challenging. You know, this is one of those ones that we if... The listeners want to check out the website. I just posted a brand new video on actually how to fix this Which is why I was so interested in talking about this Yeah, because I was just talking about this topic and showing some people the new technique we use But you know you want to see how you fix one of these arthroscopic glenoid fractures I will when we do this post I will post about my website link so you could take a look at it but it's just a really interesting injury pattern because it's also, it's really uncommon.
You know, I see a very high volume of shoulders instability. Maybe I see over 100 to 150 patients that have unstable shoulders a year and probably have to operate on 75 of them a year, 80 of them. I see probably two or three of these a year and I have to get referrals from them from all around the area.
So if you imagine how uncommon this is in comparison to regular injuries, it's pretty low. Some surgeons who, you know, a lot of my patients come for second opinions for these and when they see another surgeon, [00:14:00] some surgeons that, some of these surgeons say, I haven't seen one of these in three or four years.
So if it just shows you how uncommon, how difficult, it's kind of a, It's kind of a nasty combo. Now again, if you know what you're doing, you can get good results. So I don't think that Deshaun Watson is going to have a poor result. I hope he doesn't. But nonetheless, it's something that people should be aware of because this is not just a standard injury.
Will Sanchez: What's normally the injury or... The action that the patient is involved in when you normally see these type of injuries in the shoulders is something that's like, if you do this, this is a common injury for that, whether it's a sport or falling on your shoulder, skiing or what, is there anything that's common or it's just kind of random because it is a random injury as, as it is.
Well
Dr. Grant Garcia: this injury usually comes with a shoulder dislocation. So the person arms outstretched all the way back, like a cocky motion, like a throwing motion. And that's when it could come out. The last two though, randomly I had one guy was in the middle of a. Was in the middle of a park, got his [00:15:00] arm caught on a bush, 10 miles out, and had to, had to limp home and drive for 4 hours into my office.
Oh my lord. So that just gives you an example of, and that gives you an example of it just comes randomly. You know, I had one person that fell on their bike, one person got hit by a Amazon delivery truck. So, you know, I, there, the, the, the, the the injuries are different all over.
Will Sanchez: I'm sorry, I'm sorry for laughing.
Dr. Grant Garcia: They're doing fine. They're all doing fine. But nonetheless, for just for the, for the listeners, really just to understand the injury and the differences in it. And again, maybe we'll look back in a year and Deshaun Watson will go on to win the MVP next year. And I'll be wrong again. But even though it heals fast, we're still looking at a solid five, six month recovery for him.
So this is not something that is going to be quick fix. And he's gonna be back. I mean, hopefully next season but we'll see throwing shoulder is not ideal.
Will Sanchez: : If everything goes right, is there still any concern, right, I'm thinking about a quarterback here, and throwing a football, of a range of motion, is there any [00:16:00] concern, or because it's in the throwing shoulder, it automatically becomes a concern, no matter what the results of the surgery is?
Dr. Grant Garcia: : I would be very concerned if I were the Cleveland Browns, because of the range of motion. I mean, that's the only thing I'm concerned about, like we had mentioned before, when you fix labrums labral tears, just the one he probably has, he has a labral tear and a piece of bone that broke off. They come together, kind of stuck together.
So just the labrum repair it alone, even throwers do well, but those are still concerning. This is a piece of bone and that, and it's at a much higher risk, it's got to get fixed so quickly. It's not like he tried to play through the season. It's not like he got his motion back. I mean, we're talking about this.
He's probably getting surgery in the next week and if he's not, I'm surprised. But once they made the announcement, I'll be getting surgery in the next week. I mean, you want to fix these within the first two to three weeks.
Will Sanchez: : Yeah. If you can. You know, I, I think about football players and I think about football pads working out, throwing a ball, getting hit by 300 pound men, [00:17:00] multiple 300 pound men.
Are we, is there concern with continuous pain with a, with an injury like this, or if everything heals right, it's just going to be the normal pain of getting hit by a 300 pound man?
Dr. Grant Garcia: :Yeah. So the there's not a lot of good long term data on an injury like this because there's so uncommon, but what we could tell you is at any time you break that joint surface, your knee like a fracture of the knee or a fracture of the elbow or a fracture of the wrist.
You, no matter how good the surgeon is, they don't always put it back exactly right. And hopefully they do. And even if you get it perfect, they're still damaged the cartilage and the cartilage doesn't like to be damaged. It doesn't like to be separated, beaten up, pulled back. It just doesn't like it. So his risk of arthritis in that shoulder is significantly higher as a result of this injury.
He won't feel that pain for a long time. And he may not ever feel it, but nonetheless, that is what his risk is. Short term pain [00:18:00] with this, it tends to be very minimal. You know, my, my patients are happy with the result, but my patients aren't Deshaun Watson. Yeah. When, with this injury, I mean, I don't, can't think of the last athlete I've had with an injury.
I've had football players with a small bony bank cart. But if he took off a bigger piece of bone, that is concerning. But again, I wasn't there. I don't have the x rays that are on the CT scan. Yeah. But I think it's good for the, for the listeners to hear the different levels of this injury and what this means.
But the, you can imagine, this went from like, Oh, we don't know. This is okay. He played through the thing. Now he gets surgery. It's done. You know, there's not even a question,
Will Sanchez: :man. Obviously we know he's going to rehab the hell out of it because they're just programmed to just kind of work all the time.
That's usually that, you know, we've had these discussions on many shows that that's the main component after you've, you know, rebuilt and fixed the patient. And we had the discussion with our physical therapist that the next step is the rehab just [00:19:00] to kind of give. Some context, if it was just kind of like a regular, you know, John Doe walking into your office and they had this type of surgery.
What is a similar kind of rehab or exercises that you're now looking to do to fix the shoulder, stabilize the shoulder, strengthen the shoulder, and trying to get back to some normality?
Dr. Grant Garcia: : Yeah, so the, the problem with this injury is if you have a regular labral repair, you can move someone pretty quickly.
Yeah. You know. Sling for a week or two come out of it really quickly get motion back and we're getting more and more aggressive the better Technology we have they've got to fix a piece of bone and the bone takes about six weeks to heal So if you imagine he doesn't want to overstress his shoulder so quickly Yeah, but you want to get the motion back?
But if you get the motion back too quickly, you can pull that piece of bone and break the entire fix It's a catch 22 and so, you know, he may get repeated x rays, he may get CT scans and check and make sure he's not moving it. I don't know what level of overkill [00:20:00] they're going to do to check them. Or they may say, Hey, listen, we'll get it good enough.
Even if it moves a little bit, you're going to be stable. You're not going to have pain. So I'd rather you not get too tight and you can throw again. So I don't know what they're thinking. Per se, if I was, if I was taking care of him, I'd probably give him a little bit more accelerated protocol than my regular patients.
He's also really, he's still a young man, so he's going to heal really fast. I mean, I would tell you half these injuries are, are usually in patients over 30 years old and so they tend not to heal as fast. They still heal well, but they're not as fast. He's younger. And he's a super athlete. And so, probably better to get him going sooner.
Is it enter risk is this place pulling off and not healing and having further issues is a pretty low risk him getting stiff is a pretty high risk. So if you're thinking about how we determine what someone should do for their rehab, we try to, yeah, well, that's the way it works in life. You know, not all my surgeries are, they're, they're custom approaches.
You can't just, every person's [00:21:00] different. And so he's going to hopefully get a custom approach. You know, so he's going to start strengthening at six weeks. Like, our goal is hopefully that four, you know, five to six month mark, but he may get, he may start throwing sooner. Who knows? I mean, there's no way to do an internal brace in him, but who knows if they'll try it.
You know, for just to make you happy. Well but the but nonetheless, you know, we've seen freak and we've already seen freak recoveries with Aaron Rodgers thrown out of the field. So maybe he'll prove me wrong.
Will Sanchez: Everyone should get an internal brace. I'm just saying it's everyone, you get an internal brace and you get an internal brace is like Oprah, like just giving out internal braces everywhere.
Looking ahead. Right. And obviously there's no way for you to determine, because obviously you're not, you're not going to be with Deshaun Watson with their team. You haven't seen you know whether it's. MRI results and going forward because pretty much you're telling me they're going to get in there, they're going to fix it, try to do a great job and then monitor and then try to maybe fast track it without injuring it so we could, you know, be aware of stiffness, try to get some mobility and [00:22:00] then work your way up.
So there's, this seems like there's all these different levels. And the only way to do that is to monitor the situation constantly, which obviously they're going to have the best doctors and try to. Tech, their monstrous investment of a player going forward, but training cap, it's in seven months. I know this is crazy.
I know we're in football season right now. We're kind of holidays are coming along and everything else, you know, you're throwing the ball, you know, June is one of the things we saw Daniel Jones get injured and how long he's going to be out seven months from now, throwing an NFL ball, is it? There's, is it really no way to determine what the result's going to be and, or I guess maybe the better question is, what would be a concern for you if in, let's say, four months from now, Deshaun Watson is not doing what?
And then that might determine whether they're going to be ready for the next season or not.
Dr. Grant Garcia: I just [00:23:00] think if he's not throwing the ball yet, I mean, you, the thing is he's going to probably have to wait. I mean, it's, this is, a thrower is different than any other athlete we deal with. This is the hardest of all the things we do when it comes to a shoulder injury.
For me, my hardest thing in the, in my office is dealing with a pitcher or a quarterback that injures their shoulder with a labral injury. So this is the hardest thing in terms of surgical outcome. Because you just don't know what they're going to do. And we've seen better and better results. And our, our results are getting better.
Our data is getting better. But you just don't know. And so I, you know, I'd like to see him consider start throwing at four months and hopefully that seven month mark he's rocking it and whipping it and accuracy is there and everything else. Yeah. But if you're five months out and you're not seeing him try any throwing, you should be really concerned because they're clearly trying to figure something out now again.
I don't know. We'll see how it goes and maybe he'll be on the field throwing balls at two months and everyone will say, Dr. Garcia has no idea what he's talking about, but we'll see. [00:24:00]
Will Sanchez: Hey, we say that already jokingly. lIsten, everybody get an internal brace. Ask, ask Santa for it and put in your stocking stuffer, whoever you're asking for.
Everybody stuffers. It's just going to make life a lot easier. Anything else as we wrap it up, br>
Dr. Grant Garcia: Dr. Garcia? Now I just want to make sure the listeners learned about this injury. It's very interesting and really when you see that you're saying Oh, what the heck happened? He broke his shoulder, but the good news is it's not as bad as what we a lot of other injuries We see people that fall off ladders, etc Yeah but it's a unique injury to an athlete such as this and people should know what the outcome is and the surgery and this is Not gonna be a chip shot.
So they get him back next year on the field Kudos to those
Will Sanchez:surgeons remind everyone to check us out at sportsdoctalk. com. We've got some great content there. And we always remind our listeners, there's transcripts of our shows. So if you don't want to listen to, to us, then please read up [00:25:00] on us. We've got some great information.
Remember we're talking all sports, all orthopedics, all the time. I'm Will Sanchez and Dr. Grant. Garcia that gets extremely excited sending me text messages when people get hurt. Only, only Dr. Garcia can love you a certain way. So Dr. Garcia, thank you so much for your time and everybody out there. Thank you for listening.
Dr. Grant Garcia:Thank you guys.Audio Transcript
Football Injuries and Innovation: Grass vs Turf and 5G Heads Up Display Helmets

Will Sanchez: [00:00:00] Listening to Sports Doc Talk. I'm Will Sanchez along with Dr. Grant Garcia. Like always, sports, orthopedics, all the time. This is what we do. This is what we love. And we love talking with you and just talking about the things that we really care about. Before we get into our show topic, let's welcome in Dr.
Will Sanchez: Grant Garcia, our orthopedic surgeon and sports medicine specialist. And just a reminder, check us out at sports. talk. com. Dr. Garcia. How are you this, this beautiful fall as we get ready for the holidays. Is everyone excited? I know you got some little ones running around the house. Are they starting to get the excitement of the holidays coming around or is this a little too, still too soon?
Dr. Grant Garcia: They're excited. You know, the. It's my daughter's birthday before the holidays, so she's, she's way more into that than the holidays yet. So once that passes in early December, then the holiday rush will come. Once the, you know, once we get the tree up [00:01:00] and everything else, people tend to get, the kids tend to get more excited.
Dr. Grant Garcia: But we're good. Yeah, no. End of the year is crazy though for orthopedics, so it's hard to Get super excited about the holidays. Yes.
Will Sanchez: Now, I'm going off topic right now for what we're about to talk about. But do you tend to see some of that uptick, one, because people are starting to do activities that they haven't done since maybe last winter?
Will Sanchez: Or two, they're trying to get some things done, you know, whether it's insurances or trying to get certain things at the end of the year. Or is it a combination? What has been the pattern for you that you've noticed with patients coming in?
Dr. Grant Garcia: So some patients may know this, but basically the worst time to get surgery by North Peak Surgery is in December because it's the busiest because everyone has their ductible.
Dr. Grant Garcia: And so they meet their ductible and then they decide to like, okay, I'm going to get my knee done. I've been waiting two months and waiting six months and waiting a year. So December is the busiest time of the year for pretty much all my partners, um, right before the holidays and up to basically patients will be, you know, they'll be asking for [00:02:00] surgery all the way till I've done surgeries as New Year's Eve.
Dr. Grant Garcia: Oh my God. I want to get done before the end of the year. So the yeah, the end of the year is a big deal. As a sports surgeon, unfortunately, as we know, ski season's coming up and so that's a. That's a different level of busyness, but the end of the year is always the busiest time of the year. You know, we all prepare and staff prepare for a higher amount of cases.
Dr. Grant Garcia: It's just busier. All right, so let's all
Will Sanchez: insurance related. Yeah, you know, it sounds like it and I know personally for myself I used to snowboard a lot and you know, I've been far enough removed where I'm going Yeah, you're starting to get a little too old for that. Not so much getting too old for that But the fact that I've haven't Snowboard in over a decade and now I'm just like I feel like I'm gonna go out there.
Will Sanchez: Something's gonna happen utilizing muscles and I'm not used to doing and used to carving and things like that, but Like I said, we're getting way off topic about what we're going to talk about today, because what we're going to talk about today is really an underlying [00:03:00] theme that's been around for a long time, and it finally seems to be at a heightened state, especially the last year in football, and that's been the argument between turf and grass, and that's the topic that we're going to get into today.
Will Sanchez: We're going to talk about the differences of the turf, Turf, grass, and maybe what kind of roles it plays when it comes to injuries, non contact injuries, and so on, so on and so forth when it comes to that. So, real quick, Dr. Garcia, what are your thoughts for someone that is an orthopedic surgeon that has been a part of professional teams and high school teams and seeing all these different, from the professional player field to just, you know, the high school field.
Will Sanchez: What are your thoughts initially when you hear the topic of turf versus
Dr. Grant Garcia: grass? I mean, the first, the first thing you're thinking of with this is, you know, this is [00:04:00] a, this is one of those ones where this is a open box and it's, it's kind of, it's an underlying theme, obviously, I think in football, if you look at it, because It's really the debate is grass versus turf, but it's also players versus owners And there's a huge cost factor in here that I am not saying is related to why the decision is to do grass versus turf but we're preparing for this episode.
Dr. Grant Garcia: I mean it really opened my eyes to sort of the differences and You know, what what are these sort of conundrums and you know, you hear the players, right? Someone gets hurt on the field, a non contact injury. You know, Odell Beckham Jr., a couple years ago, you've got, you know, there's just a plethora of players that have gotten hurt, and they all say it's a result of the turf, right?
Dr. Grant Garcia: And the Players Union is talking about that. But then you have some studies that show, you know, there's maybe no difference, and maybe those were earlier studies. And you always have to be careful in like, who's the bias here? And understand all these different things. But I think the audience is going to just enjoy hearing about...
Dr. Grant Garcia: You know, what goes on with that debate and then the [00:05:00] preparation, right? Because, you know, I didn't even know anything about that there was, there was, they were looking at the quality of the turf and they have to have a certain criteria in order to meet that in order for the game to be allowed to be played.
Dr. Grant Garcia: And the same thing with grass. So, you know, this is a really interesting topic and it's, you know, we're not going to solve it today, but hopefully we get more information. And there may be a little bit of bias opinion here, but again, I'm also somebody who doesn't, as much as I, as much as I make my living off of injuries I have no interest in people having more injuries.
Dr. Grant Garcia: And so I do think it's important for people to understand the differences.
Will Sanchez: 100%. Just to give context, there are 32 NFL teams in the NFL which means that there's 30 stadiums, two teams share. the stadium. You know, we're fans of the Giants. They share the stadium with the Jets and the Chargers and the Rams share their stadium in L. A. So there's 30 NFL stadiums and right down the middle, 15 of them [00:06:00] use grass fields.
Will Sanchez: The other 15 use some kind of synthetic turf. And last year, the NFL P. A. president, J. C. Tretter, called for a ban on specific turfs, especially what's called slit film turf. It's citing safety concerns. And this type of turf has statistically have had higher in game injury rates compared to other surfaces for each of the following, right?
Will Sanchez: The non contact, missed time, lower extremities, foot and ankle injuries. So let's start right there. When it comes to non contact injuries, that is something that As a surgeon, that piques your interest right away, right, because those usually tend to be, and correct me if I'm wrong, the more serious type of injuries that you can sustain.
Dr. Grant Garcia: I think it probably depends on what you're thinking of, but I think that yes, I mean, you see those non contact injuries, you know ankle sprains. You know, ACL tears, I mean, there was [00:07:00] a number of times when you see a player run on the field, usually wide receiver someone open field, you know, it's pretty hard to get a non contact injury if you're kind of in the center of the line and you'll see them twist and grab their knee.
Dr. Grant Garcia: So it's a kind of a, it's kind of a combination of those things, you know, the, the contact injuries like Nick Chubb suffered. You know, that was pretty gruesome and that's a totally different animal. So you know, they tend to be just a different, they just a different look to them. They're just more worrisome to me because.
Dr. Grant Garcia: You're trying to figure out what happened, right? You're just, you know, when you see someone just get clobbered and then he goes in another direction, or their hip goes a different direction, or their arm goes a different direction, or whatever, we don't want to, you know, go into too many details, you know, you kind of know what happened.
Dr. Grant Garcia: But when someone just tweaks, runs on the field, twists, and then all of a sudden go down, you're trying to figure out, you know, that's a, that's a, that's kind of a conundrum. You're trying to go, immediately go look into what's going on.
Will Sanchez: This might be a stretch here, but... Have you noticed or in your profession, a higher tick of [00:08:00] injuries from turf to grass, or it's just, is that just too hard to really kind of realize or, you know, having asked that question with your patient From what you've seen from, you know, players coming in, whether it's soccer, football, lacrosse, you know, because especially I guess at the high school age, they're probably going to play more on turf fields because of the cost savings for these stadiums compared to maybe some of the other fields that are happening, you know, at the You know, the city park or something like that,
Dr. Grant Garcia: I think that's important point.
Dr. Grant Garcia: So, you know, I'm not asking him. Unfortunately, when you're in the office, you know, did you plan grass or into yourself on turf? But it makes more sense to me, right? The idea of grass more give, right? It can rip apart, it can pull, and if you have these thick cleats on, you're still going to kind of make some turns.
Dr. Grant Garcia: The turf, as much as we always try to have the word synthetic and more natural, it's not going to rip. It's supposed to be [00:09:00] longevity. I mean, you can't design, grass is not high longevity. But turf is, that's why it looks so good all year round, no matter how much they try to make it and put, you know, tire chunks in it and all other fancy stuff.
Dr. Grant Garcia: And again, I don't even know all the different types of turf, I'm not a turf expert, but, you know, it makes sense to me that there would be more injuries on it. And especially injuries that require very, you know, precise movements or these sort of small tweaks. I mean, we've seen this already in the sense that more recently there are, they are a higher number of foot and ankle injuries found.
Dr. Grant Garcia: And there's been a couple of studies which we'll talk about but with I think the point you brought up That's really important for everybody to understand and say, you know, why does this matter? Why is this not being fixed? Well, the word cost is real. Yeah I mean I was hearing about this and I think it's well, I mean we may talk about this or not But you're talking about you know turf field to maintain to put in It's moderately expensive, but it's not very hard to maintain.
Dr. Grant Garcia: The grass can be, you know, upwards of two to 3 [00:10:00] million. And, you know, you have these owners who don't want to spend more money and would rather have the money be profits versus using all grass. But what the interesting statement is when we were doing some research on this is that the grass now and all the technology grass can be done at any level.
Dr. Grant Garcia: Right. And I think, I think a few of the places like green Bay, who you'd imagine would not be able to handle grass or places like. Miami or whatever that can't have grass because of the heat, they both maintain them. So the weather is not a factor anymore. And so there's really, really the reason I think is because it's harder to maintain and more expensive.
Dr. Grant Garcia: But then again, you're, this is my own opinion.
Will Sanchez: No, let's keep it real. That's exactly what it is. I mean, let me, let me, let me grab a quote from Tiki Barber. He he mentioned this on his his radio show about two weeks ago. And this is his quote. He said, Whatever the cost is, isn't that worth the maybe 500 million of salary on your team?
Will Sanchez:[00:11:00] You are putting that investment in each player at risk every time they play on this terrible surface. Barbara explained on that Monday, every single week, I feel like someone is getting hurt on this turf. If the giants and the jets are serious about player safety and the NFL, they have to change that turf to grass.
Will Sanchez: : I don't care how much it costs. It's worth it in the last player's salaries, paying guys to be on injured reserve and just. For the non football fan out there, Tiki Barber is a former running back, great from the New York Giants. He has affiliations with the Giants, he works with the Giants, he works on their flagship store, he has relationships with the owner, John Mara.
Will Sanchez: So he is really kind of putting himself out there, this is not coming out of left field from someone that's not, that... It doesn't have insight. So this seems really, really personal and, and kind of a reach out there to the owner [00:12:00] to say, Hey, you have to get this done no matter what the cost, because the cost of losing these franchise players are going to cost you more.
Will Sanchez: What do you think about when you hear that quote from Tiki Barber?
Dr. Grant Garcia: I think that's an incredibly good point. And it also makes the question, you know, why have we not done this? And I know that. The problem you have and we've talked about studies on this. This this show and how they can be really, you know, challenging and they're always a little bit biased one direction or the other.
Dr. Grant Garcia: And there's statistics we have to look at, you know, if you have the same study being done multiple times, which we can talk about that 1 we were mentioning previously, you know, recently showing a significant uptick in foot and ankle injuries with artificial turf. They're not lying. And you have players arguing for it and you're absolutely right.
Dr. Grant Garcia:: I mean, we all talk about this, you know, why do I do certain treatments on a professional player? That's different than I do on a regular natural athlete there. Unfortunately they are paid more [00:13:00] money. And so as a result, even if they miss getting back one game earlier, it's worth the more expensive treatment or the out of pocket expense.
Dr. Grant Garcia:Because I want to get them back. But if I get back one week earlier, or you get back one week earlier to your, you know, our day jobs, it's not the same financial difference. And so, you know, these, these guys being out and being paid on injury reserve. You're absolutely right. It's not that expensive to put grass in and maintain it compared to one of your best players or a combination of players.
Dr. Grant Garcia: I mean, even one or two players that are making two to three million dollars a year, which is probably, it's considered low for the NFL. You know, if they are an injured reserve, that already pays for the grass. And so it's, it's, it's kind of a silly thing. It's almost at this point now, an ego thing, I think.
Dr. Grant Garcia: And just sort of like, that's the way it's been done. Right. And these, and obviously it makes it easier for them. It is a lot of hassle. They have to change it over all the time. But at the same point, it's not like there's only one or two teams doing it. Half the teams already have graphs. And so I, I, and I, I think that his [00:14:00] quote is excellent.
Dr. Grant Garcia: He's got good insight. Again, he's not a statistician, he's not a grass master, he's not a turf master but nonetheless you know, he's done this enough that I would really trust his opinion and he cares for his players, but he also cares for the Giants. So for him to say that, it's a, that's a big
Will Sanchez: deal.
Will Sanchez: yeAh. And we're talking about a player, like I said, for, for the, the listeners that don't know who he is. He retired at... The height of his football career, he led the NFL or was the second leading rush in the NFL when he retired and he retired because of the fatigue that he felt that, you know, it's getting beaten, beaten up on Sundays by players, but also landing on turf and for anyone that's ever played right now, I'm not just saying football, soccer, anything.
Will Sanchez: When you fall down, we look at, we look at them, they fall, they get up. Yeah. That hurts. Those fields, those turf fields hurt. It's like it's [00:15:00] just falling down on something hard, and it's just it makes a big, big difference. I want to put in context because. If you're looking on a grand scale around the world, the biggest game around the world is soccer.
Will Sanchez: And the biggest league is the Premier League. And just to give you context, their football, they call them football pitches, you know, as far as their field. And stadiums opt for a high quality, hybrid, grass. system in that hybrid grass system, which the NFL does have for their grass fields, especially in Arizona, right?
Will Sanchez: We go back to these weather you know, hot weathered states or cold weather states. They using this hybrid grass. They use about 95 percent of this hybrid grass with then it's reinforced with like this artificial turf fibers like the other 5 to 10 percent depending on the quality of grass. So if you If the premier league, [00:16:00] which is at, like I said, at the highest level with the biggest sport in the world, this is what they're doing for their players because they pay them a lot of money.
Will Sanchez: Maybe the NFL should take a page out of that. and put that into their stadiums because these players have been asking for grass fields for quite a long time. Dr. Garcia, when it comes to high schoolers playing that have no choice and they're playing on turf fields, what are some of the concerns or have you noticed concerns besides injuries?
Will Sanchez: Is there uptake in concussion or anything like that from hitting these hard turfs? Or once again, is this something that You know, if you don't ask the turf when you have the communication with the patient, it's hard for you to really know.
Dr. Grant Garcia:I mean, I think this is a challenging and sort of loaded question, but I'm used to it on this show.
Will Sanchez: Yeah, yeah, yeah. I know, I know.
Dr. Grant Garcia: My bad, my bad. No, it's okay. [00:17:00] So basically, you know, we're talking about costs again. So you did Premier League and the NFL. These are where money's no matter, and the word multiple millions of dollars get thrown around like it's just candy. Yep. Right? This is different than the high school team.
Dr. Grant Garcia:And you know, again, I take care of Marshall High School. We have, you know, reasonable funding, but we do not have NFL level funding. And so to have a grass field, especially in Seattle, would be a disaster. And so the artificial turf is nice because even if it rains, it doesn't, it's not very slick. Yeah. But I do worry.
Dr. Grant Garcia:I mean... There's, we know there's an uptick in concussions. We know there's an uptick in injuries in general because players are getting faster and you have these mismatches, especially in high school. I mean, it's almost more of a risk, right? Because the, some kids haven't gone through full puberty yet, et cetera.
Dr. Grant Garcia: But I do think that, you know, when I see those players hit those the turf. Field, it looks harder. It looks more comfortable. You know, I myself have played on fields like this before. And it feels different. Now again, it [00:18:00] depends on the weather, whether you like it or not. But, you know, it's but again, in the lower levels, there's no choice.
Dr. Grant Garcia: It's just, it's just without a doubt, the upkeep. The ability to keep it good quality, because again, we're talking about good maintained grass, but we're not talking about poorly maintained grass versus turf, because I imagine a poorly maintained grass is probably a much higher injury rate than turf.
Will Sanchez: Yeah, and some of these turf fields are as you say, not in great shape.
Will Sanchez: They're kind of coming off at the seams. I know Magnuson Park, which is in Seattle, it's a big park out here. They have a couple of fields. One of them is in excellent shape. They changed it about two years ago. And they have another one where I've seen rugby games being played. It's coming apart, and I think they finally closed it up.
Will Sanchez: So I'm assuming that they're going to start working on it. So even some of the turf fields, it makes it even worse if they're not in great conditions, but you know, like you said, those are the situations. There's only but so many fields out here and [00:19:00] you know, you just kind of wish that you know, things could be a little bit better, but it is what it is.
Will Sanchez: As we wrap up the turf versus grass conversation, I'm going to be a little cynical here, but I'm feeling kind of that way. I'm, this is the week I'm kind of having. So I'm going to go, I'm going to go a little cynical here and say that. I think also you take it with a grain of salt when I think about these owners, maybe being hesitant to change right away and give the players what they want.
Will Sanchez: I start to think about negotiations and give a little and take a little and we'll give you this, but we want that. And you know, we got 17 weeks. We will love 18 weeks and we can do this if you could do that. Like I said, I have no idea, no justification, but we know. This is a business and businesses with owners and players is a give and take type of situation.
Will Sanchez: So I'm not saying that that's what the case is, but there's always that little voice in the back of my [00:20:00] head because I'm playing cynical this week that that possibility may be there.
Dr. Grant Garcia: I think that's an excellent point. I I think you I think you may find out sooner or later you may be more correct than you think.
Dr. Grant Garcia: Well,
Will Sanchez: I'm hoping nobody comes knocking on my door. I'm not that, you know, let's, let's make sure we don't have Goodell's goons coming after
Dr. Grant Garcia: me. Well, you, you know, you've hit it, you know, you've hit it big on the podcast start knocking on
Will Sanchez:your door. Alright, let's, let's make sure we don't hashtag the NFL when we release this.
Will Sanchez: All right, let's go to a great story. I was really excited about this. I saw this a few months ago, and then I'm watching Sunday Night Football, and there it is. There's a commercial by AT& T, and I was like, this is amazing. I was talking with Dr. Garcia about this. We said, next show, we're going to talk about it.
Will Sanchez: Sure enough, commercial on Sunday Night Football, and this is their AT& T 5G helmet with which is, which has been AT& T logo. Used this year on October 7th at [00:21:00] the Gallaudet University, This school is for the deaf. And they have a football team. AT& T created this helmet that they can utilize and it has a screen in front of their helmet, a clear screen, where the coach can put this information, the play call, the quarterback can see it, and the rest of the players, and they know exactly what's going on.
Will Sanchez: So this is really a game changer. Before we get into all that, what are your initial thoughts on this type of technology that's out there and how do you think that can benefit you?
Will Sanchez: Because we always talk about technology in your field and what can you see as a next level for this type of technology?
Dr. Grant Garcia: Well, in the interest of time, I won't get too excited about this, but... They know this when I saw this and you showed it to me. This is a this is pretty impressive technology I think it's good for the audience to hear about it I mean the ability for these deaf players to be able to see the heads up display screen And see it in [00:22:00] action plus the idea of the 5g helmet having all the communication signals I mean remember the old shows when people were trying to tap on their helmet because they couldn't hear the play call Yeah, it sounds like this is completely new technology And so this is really interesting to see because we always talk about concussions and helmets But not really what else that can be brought into them and the ability of this to sort of run new plays or especially for some of these players that go you know even in the nfl level but college, you know high school when you're learning the place To have one of these heads up displays, especially for some of the wide receivers, et cetera especially if you, you know, you just started on the team and you haven't been able to chance to learn them all.
Dr. Grant Garcia: That's pretty awesome. You know, a lot of times we use, you know, in our high school, we use signs and things like that to show them, but to have this sort of technology with this helmet built in I think it'd be a game changer in terms of just being able to do more plethora of things and keeping everybody organized.
Dr. Grant Garcia: : For my work, we already do some of this stuff, and this is pretty awesome. You know, this heads up technology slash virtual reality is kind of a coalescence together. You know, when I do some of my surgical [00:23:00] videos, I have some of this, I have this 4D or 4K head camera that I wear, and I actually have a heads up display in my eye when I'm operating, and I can see what I'm doing, so I know whether the picture is going to be good quality.
Dr. Grant Garcia: So I already do some of this stuff. And the new features we're talking about are You know, you get 3D mapping of the patient for shoulder replacement, and then you can actually see if you put the implant in and you can actually virtually put it in with your hands. Now, again, that technology is limited and there's different things, and this is going to be, I think, one of the next generations of technology for surgeons, because what we could do is get an MRI or a 3D, a 3D CT scan, so what it is is like a CAT scan.
Dr. Grant Garcia: And then it can, and then it basically will show someone's bones or anything in three dimensions, and you can spin it around in your helmet, essentially like having a computer right there that's sterile. And then it can also have part of your surgical plan. So as you're putting things in, it will show you if you're doing the right orientation.
Dr. Grant Garcia: They already do a lot of this guidance, sort of 3D modeling and spine surgery. And we're doing it in a [00:24:00] lot of other places because we've noticed that the precision that we can do things is even better. So you have a highly trained, skilled surgeon. With incredibly high technology, it's just gonna, it's gonna make your surgeries better, more precise and faster.
Dr. Grant Garcia: And the less time you're under surgery, the better you do. It's just, there's no doubt about it. You do a good surgery, but you're also efficient. That is the best case. And I've seen in surgeries when I have really efficient surgeries over time as I've gotten better and better, I've seen that my patients are doing better and better.
Dr. Grant Garcia: And I'm doing maybe the same surgery, you know, the exact same thing from the year or two before that. But as you get more efficient and you have less time under anesthesia, it just makes more sense. And so, you know, this, all this technology is only going to help patients, which is pretty awesome. And yeah.
Dr. Grant Garcia: I think that you see technology in the higher level for the for football.
Will Sanchez: How do you see this as a teaching tool? Let's say Dr. Garcia, you know you know, a few years from now where maybe he's now teaching the young bucks, the young men and women of the [00:25:00] future surgeons, and you. sitting there as a proud papa and having some kind of technology like this that you can sit there almost kind of like a coach and guide them through something like this or maybe something beyond even our thought process.
Will Sanchez: You know, this is stuff I think about. I'm like, just besides what you're doing right now, but how can you use this as a guidance or a teaching tool going forward? What are your thoughts on something like that?
Dr. Grant Garcia: Well, I hate to tell you that there's actually more reality than you know right now. So, you know, I do some of this stuff, again, we used to do it with the avail system we had talked about previously, where the camera system was in there, we went live and I'd done a few of these from my operating room, where I would teach people how I'd do something and show them it.
Dr. Grant Garcia: And there are certain companies that if you need to learn a new procedure, the surgeon will actually bring in, you'll have a camera come in and do a sort of video live for you so you can, they can help you walk through or you can watch them in the operating room through this type of situation. But the newer technology, which is really not there yet, it's hard.
Dr. Grant Garcia:Even the camera system I use is quite [00:26:00] technically challenging and it's not the best system out there. It's just pretty good. There's just nothing like it. Yeah. But really the next step I think is. You have a head camera on it's a great camera. It's really you don't really have to think about it Because you don't want to have distractions in the operating room.
Dr. Grant Garcia: That's never a good thing but you have the ability to have this camera on and watch you It's guided by your head, so it sees your bird's eye perspective, which is really, that's the part that people can't see usually in the operating room, right? There's, in certain cases, there's only one person, even though there's a few people operating that can actually see exactly what's going on, that's usually me, the surgeon.
Dr. Grant Garcia: And so then I can do that huddled together with this, or a heads up display to see what I'm showing them, and then they can actually ask questions and you can teach. And so the answer is yes, this is a very early market for this type of technology, and this is going to be a game changer. Even in the last few years since, you know, residency fellowship and now surgery and then starting to build, you know, build a repertoire teaching other surgeons about certain techniques that we do in the complex [00:27:00] stuff that we do over here in Seattle now.
Dr. Grant Garcia: You know, this technology like this is incredibly helpful. It also saves a lot of time. I mean, it's a lot of effort for me to fly out to someplace to teach where I could teach directly from my operating room where I normally work anyways. Yeah. And so it's, it's really, it's better for all parties involved, lower costs too, because you're not paying for someone to fly out in hotels, et cetera.
Dr. Grant Garcia: It's just, it's overall better quality for everybody. And so that's really what's important. But you're also utilizing technology. It's like Zoom. But for surgeons,
Will Sanchez: which is pretty cool. You think besides whether it's the cameras or the technology getting better, but outfitting the operating rooms, whether it's having, , 25 mini cameras from different angles
Dr. Grant Garcia: It will. And it's also the push. It's the push for the companies who want to teach. It's the push for the surgeons who want to have that better perspective. I mean, hospital social surgery, where I trained, we had cameras, we had one camera and the lights. And so you could bring it over to right where you want it to be.
Dr. Grant Garcia: And so we have so many people that would come from all over the world to watch our surgeons operate because obviously it's one of the best hospitals in the world for orthopedics. Yeah. And we had so many visitors all the time from international that they would sit in the back and they could watch the whole surgery and ask the surgeon questions.
Dr. Grant Garcia: So you know that and that's that's what a lot of these new operating rooms and technologists do. We're more of a private practice so it's a different teaching facility but a lot of facilities nowadays they're starting to do more outfitting that right because you want to be able to see and people want to come in if they're going to shadow you.
Dr. Grant Garcia: : And watch, they don't want to see someone turned around talking and kind of mumbling. They want to be able to see the whole thing, you know. It makes the experience better, and [00:29:00] as we all know, you know, what you hear, you hear about 20%. But when you see it, it's a whole other animal. You're like, that makes perfect sense to me.
Will Sanchez: It's funny. I was thinking of like some old movie where the surgeon turns around and looks at, you know, the young surgeons that are coming up , , all dressed in white, I am now going to do this and, you know, turn back around. They've got a little you know, pencil and notepad and taking notes and things like that so thanks for that, that visual.
Will Sanchez: What do you think about the university and the football players? This university for education for the deaf
Dr. Grant Garcia: I Saw a video when they introduced the helmet, they introduced the technology. To them saying this is going to be available to you and said, man, I'm really happy for the kids that are going to college and playing football and, and having something like this. And I'm looking forward to the technology that's going to keep expanding and who knows where this kind of goes.
Will Sanchez: What are your [00:30:00] last thoughts on on this technology and just, you know, this 5G helmet that Gallaudet was able to use?
Dr. Grant Garcia: Well, I'm just really excited. You know, hopefully we can do another episode like this in a year or two and talk about, Hey, remember that episode we had on the 5G helmet from the, from the prestigious university in DC?
Dr. Grant Garcia: Yeah. Now look at it being used more. You know, these, we get, it's so fun that we've done this for so long now. You know, with the new rebranding of the show, but even our old episodes, you know, we've done this for almost what now? Three years? And we can now look back on episodes and be like, Oh, look how wrong we were, but also every once in a while we can say, look at all the cool technology we're talking about.
Dr. Grant Garcia: Look what it is now. I think this is going to be a good segue to the next few episodes, which hopefully our listeners will enjoy. The next episode, we have an excellent entrepreneur we're going to talk about. Talk about some new technology and napkin to reality, which everyone will really enjoy that.
Dr. Grant Garcia: It was extremely hot on our podcast. And then the end of the year episode, which I know Will and I are really excited about is [00:31:00] I talk and we'll talk about a lot of fancy things that we do in orthopedics and sports. But you know, I talk about like, Hey, check this new thing out. We're going to be doing, but that thing we talk about doing is only six months old.
Dr. Grant Garcia: Well, now it's been about a year or two. So where are we at? What were you right about? What were you wrong about? And, you know, hopefully we get more rights than wrongs, and, you know, we're pretty happy with the new technology, but I think that the listeners want to hear about it. This is the most cutting edge stuff, and there's some new things, too.
Dr. Grant Garcia: And again, I tell everyone in my patients that if you come back to my office or my PAs, if you come to my office in a year or two and I'm doing exactly what I did before, then I'm not getting better. And that's something you should be worried about. And so every year we're advancing. And so I'm really excited to have listeners here about all this new technology that I can offer them, and how we continue to push the envelope in the future.
Dr. Grant Garcia: So that'll be our sort of Christmas episode. So we're excited. Thank you all for listening and follow us on our all the platforms we've talked about. And Will, [00:32:00] I hope you feel better. And obviously, you know, many thanks for coming on tonight. I know you weren't feeling up to it, but I think that...
Dr. Grant Garcia: I think that the listeners will be really happy to hear our turf discussion and our 5g helmet. So
Will Sanchez: Before we go You know, I got some trivia for you.
Will Sanchez: You're trying to sneak on out of here. You were like, all right people, thanks for coming. Good night, y'all. No, no, no, no. Hold on a second. Hold on a second. All right. We were talking about the 5G helmets and all these wonderful deaf and blind athletes. Well, it's a deaf and blind school. So that's why I mentioned the deaf and blind athletes, but they're deaf athletes.
Will Sanchez: So, and I think you got this here. All right, so Some of the hearing, you know, impaired players was Bonnie Sloan and Larry Brown and Kenny Walker and even Flozel Adams, he played with Pittsburgh and the Cowboys, some really well known kind of players if you're a football fan, right? But the first [00:33:00] legally deaf person in the NFL, do you know who that player was?
Dr. Grant Garcia: Oh my gosh, no, I have no idea.
Will Sanchez: He was a Super Bowl champ and he played for the Seattle Seahawks.
Dr. Grant Garcia: Not Jim, not Jim Zorn, no he's not deaf. Who,
Will Sanchez: no, who is it? Derrick Coleman. Derrick Coleman was on the football team really with the Legion of Boom. He he won the Super Bowl with them. He was, he is recognized as the first legally deaf person. The other players I mentioned before. They had some hearing issues and loss of hearing, and I think some of the loss of hearing is probably getting smacked upside the head by Too Tall Jones and some other players, but that's a whole other story.
Will Sanchez: But the first legally deaf person in the NFL was Derek Coleman from the Seattle Seahawks, and he won himself a Super Bowl. So just tying all of that [00:34:00] there together. So imagine how difficult it was for him to play in the NFL. NFL at the NFL speed and still be able to be a player. And he was, he was a player five, six years, at least, you know, I don't have the numbers in front of me, but he played and he made it.
Will Sanchez: So kudos to Derek and everyone else out there that are playing and doing their things, whatever the challenges are just a little information. And, you know, I know Dr. Garcia was trying to get out of here before we got to the trivia. So we just want to thank everyone. Thank you for listening to SportsDocTalk.
Will Sanchez: Check us out at SportsDocTalk. com. We've got our shows. We've got transcripts of the shows, right? We're talking about you know, this is a great episode, right, for Deaf, right? We, we're, we're there. We, we have this information on our website. You can read. All the mumble jumble that I'm talking about right now.
Will Sanchez: You can read it in our scripts and our transcripts. So please check out the website. There's a lot of great information. Dr. Garcia [00:35:00] always has some really cool stuff and talk about cool toys and all the other stuff that we talk about. So please check it out. Dr. Garcia, before we go, any last words? No,
Dr. Grant Garcia: thanks to all those listeners.
Dr. Grant Garcia: Always fun. Thanks Will. And I'm looking forward to the next episode. All
Will Sanchez: right. Thank you everyone. Thank you, Dr. Garcia. Take care.
Dr. Grant Garcia: Take care.Audio Transcript
Innovations in Physical Therapy with Hidef Co-Owner Zach Smith

Will Sanchez: [00:00:00] Welcome everyone and thanks for listening to Sports Doc Talk. Be sure to check us out at SportsDocTalk. com I'm Will Sanchez and once again we are so thankful and grateful for everyone listening and checking out our websites and I think Dr. Garcia promised the next 1, 000 fans to listen to our show A Miniature Pony but we'll bring him on in a second to confirm that.
Will Sanchez: So we are just so excited about it. We have a great guest today, but before we get to that guest, Dr. Garcia, can you confirm, are you giving out miniature ponies for our 1000 listeners ?
Dr. Grant Garcia: Oh, yeah. I, I wish I had a thousand miniature ponies, so I can't confirm that, but it's a, it is a good idea.
Will Sanchez: Listen, we're really excited about today.
Will Sanchez: We have a big component of what you talk about, seems like every single show, and that is the work that you do, getting to the patient, repairing them, um, getting them [00:01:00] back to where they need to go. But really the next step is your handoff to someone that really does the work as far as physical therapy.
Will Sanchez: putting in all the work that has to go into recovery so they could get back to normality. And we have an exciting guest today, Dr. Garcia, please introduce our guests. And before you do, please explain a little bit more why it's so important to have a physical therapist to get you on your road to recovery.
Dr. Grant Garcia: So you know, we thought about this show and you guys all hear the fancy stuff that we do. We're cutting edge procedures. We do, you know how we're trying to push the envelope. Yeah, that's all well and good. But, you know, my, my surgery is hopefully anywhere between an hour to two hours worth of work, you know, there's some pre discussion, but really that's it, you know, most of that's handoff and the handoff is to physical therapists.
Dr. Grant Garcia: And if you don't have a good team, you'll see pretty quickly. That despite how good a surgery you do or whatever you do in the operating room, it really doesn't matter if you don't have a good team. And [00:02:00] so, you know, being now in Seattle for a little while and getting to meet a lot of good physical therapists, there's just some really high quality places, um, that I think Really will help things and also when you those difficult situations where you need to have second opinions second opinions for physical therapy Because the things not going the way you want, you know, I've got my go to's Tonight, I'm really excited to introduce Zach this is he's one of the co owners of high death And you've really been instrumental in helping me take care of my patients.
Dr. Grant Garcia: I know I've sent Plenty of patients his way, um, even for second opinions on top of my standard surgical patients. So some of my patients will drive an extra distance just to see him and his team. Um, and they take care of anything. You know, there's, there's sometimes you have in physical therapy, the procedures that we do are unique.
Dr. Grant Garcia: And they're not commonly done. So you see a meniscus transplant, you see a Carlos transplant, um, and that can, that can make people nervous as they rehab, but this team does not falter and I've never had any issues before and they've taken care of plenty of those patients of mine. So, [00:03:00] um, it's a pleasure to have them on.
Dr. Grant Garcia: And I really want to talk about. What cutting edge stuff that they're doing to help our patients get ahead and with our better outcomes, because again, all these athletes are seen online, Aaron Rodgers, Nick Chubbs, you name it. Lonzo Ball is going to come back from his Carlos transplant. Most of that work is being done by amazing physical therapists.
Dr. Grant Garcia: So thank you Zach for being on here and love to
Zach Smith: hear more about your stuff you're doing. Well, thanks for having me on and I appreciate you guys taking the time, uh, to bring me on here and, and I've had nothing but positive experiences with you and your team and, and never hesitate to send people over. I know you guys are the best in the business over there.
Zach Smith: So we've enjoyed being able to be on the cutting edge of. of medicine with you and bringing some of the passion that we have for sports medicine and recovery of some of these complex surgeries. And so it's been a, it's been a really fun thing to work with you and your team. I was actually just online yesterday watching a bunch of your surgeries that you're doing.
Zach Smith: So I've been, I've been loving what you've been doing with taping the surgeries. Sometimes I'll [00:04:00] be at parties and I'll be watching your surgeries and people will look over at me and they'll see that I'm on a phone looking at surgeries and they're like, what are you doing? And I'm like, Hey, come over here.
Zach Smith: You got to see this. This is what This is Dr. Garcia. He's got these surgeries that he records and it's really well explained. And so, yeah, I'm even bringing some of the people that are not in the medical field into the fold on some of the stuff that you're doing. And so, so, uh, thank you so much for having me on and, you know, I'm looking forward to it.
Will Sanchez: Awesome. It sounds like Zach's hanging out with a bunch of guys like myself, just kind of randomly looking at these, uh, surgeries, these internal braces, you know, that's my thing right there. So Zach, I can relate Zach Smith. He's a physical therapist and co owner. Sure. Like. Garcia mentioned at hi-def pt, that's H i d E F p t.com.
Will Sanchez: So you could check out, check him out and check more information out there, at his website, uh, de Garcia, uh, please, can you continue?
Dr. Grant Garcia: So, I mean, I think. I want to know more and I kind of talked to Zach about this and [00:05:00] I'd like to know more about like, what do you guys do? How do you guys do it? You know, I've told everyone kind of my backflow and my secrets to sort of how I try to stay on top.
Dr. Grant Garcia: But you know, I'm not, I'm not as experienced in the PT world. I know I send them to you. You do an awesome job and the patients come back looking really good. But what does it take? You know, what does it take for you guys to stay on top? And, uh, you kind of explain your methods and what you're doing that's new.
Zach Smith: Yeah, I mean, the first thing is, I think what it takes is consistent team effort on education and keeping up with the latest in what's going on with surgical techniques with rehab and performance and all of that. So I think in the Pacific Northwest, like you said, there's so many great clinics and so we're just happy to be a part of, of the community of PT here up in the Pacific Northwest because there are so many good physical therapists up here.
Zach Smith: And, and really what, what I think is, has led to us being one of the leaders in sports rehab and performance, um, has just been our, our attention to education. So, like [00:06:00] this upcoming week, we're, we're bringing in a course, um, from a guy named Tim Gavitt, which is all about load management. Um, you know, he's a, he's a legend in the, in the field coming out from Australia.
Zach Smith: We host a lot of courses on a, on a variety of different topics. And then on top of that, our team stays up to date by. Um, a bi monthly full company wide meetings where we review, uh, journal articles relating to new stuff that's coming out, maybe some old stuff as well. We go through case studies and case reviews, so some of these, uh, more difficult surgical procedures, uh, some of the harder rehabs and the more complex patients, what we'll do is someone will present that case at our, at our bi monthly meeting, and, uh, and we'll get weigh in from, from all 11 of our physical therapists, um, and plus, you know, we bring people in.
Zach Smith: Like yourself, uh, to help educate our physical therapists on these procedures and help make sure that, you know, we do right by the patients because, you know, there, there are the simple straightforward procedures like, you know, metastatic needs, total knee replacement, [00:07:00] total hip. Like some of those are kind of, you know, like they're, they're fairly simple, they're fairly routine.
Zach Smith: We kind of know what to expect unless we get a curve ball, um, with some of the healing processes, but with things like, uh, you know, complex, even like a simple ACL, that's a complex rehab. And if you don't know how to test and make sure that you're loading the knee correctly through that rehab process, there could be a lot left on the table as far as like return to sport timelines.
Zach Smith: And you're seeing guys like Jordan Brooks returning to practice at six or seven months, um, returning to, I think, full play at eight months and. I think a lot of that, that type of faster return to sport, not that it's always advised early on like that early, right. But a lot of that is, is because of dedication and time spent and diligence with physical therapy, not just on our side, though, from the physical therapy and clinic side, but also helping to make sure that our patients are also ACL,[00:08:00]
Zach Smith: you know, That takes a lot of effort, right? That's, you know, I've got, I've got patients who are professional athletes where it's their full time job is now an ACL recovery. And so when we have patients that take that sports mindset that like they attack the recovery, we see really good results. And so we really try to bring that level of energy and effort into the clinic.
Zach Smith: And everyone who comes through our doors is treated like an athlete and that mindset. helps us to propel these people forward. You know, they're in three of our four locations are inside of gyms. One of them is is a standalone but looks like a gym. And when people come in, they don't necessarily feel like they're in a medical center.
Zach Smith: They feel like they're in a training facility, which for a lot of these injuries, right? We don't want to push people too early. We're always safe. We make sure we respect all the protocols and and all of that. But when the time comes to load and make sure we have adequate load for adaptation, um, You've just got to really understand how to do that and how to do that safely.
Dr. Grant Garcia: I [00:09:00] think that's a great point. I mean, I think we made a number of excellent points. You know, I think the one thing is education is really important. And I find that you have groups that are maybe not as up to date and you have some groups that are. I mean, the reason you guys will get a weird, you know, they'll get a Bay Area ACL, or you'll get a meniscus transplant, or you'll get a Carlos transplant, you'll get an NPFL, or you'll get a revision ACL of mine.
Dr. Grant Garcia: And there's really not many questions. You can follow the protocols and you do your education. And I think that's really nice. Like, you know, I love that. I love being able to teach those sort of more complex things, but it is nice to, when there's some breadth of knowledge, you know, even the fact you're joking about the videos, you clearly care enough to watch them, to learn about it.
Dr. Grant Garcia: And so that's really important. I, I think for me when I'm handing off my patients, you know, I want to know I, you, we've all heard the stories before. I have them plenty of patients come back and said that the person they worked with didn't have any idea what type of surgery they had done. Um, even though we had sent them with operative notes and you know, it's not to knock anybody.
Dr. Grant Garcia: It's just that that that's hard for me when I do a lot of work and I'm spending a lot of difficult, uh, you know, time [00:10:00] doing this. And so it's good for me to know people that Really care about the education. It's good for the patients. You know that too. You know, we you know this there is a difference between good PT and bad PT And if your therapist on board if you care about it, you read literature, you understand how things are adapting That's good.
Dr. Grant Garcia: And so, you know, you know me like I'm okay with feedback to you're like you listen, you know, dr Garcia, you're not really there's some newer things that we're doing like have you thought about this and that's really good idea Thank you, right? Like I can't read every paper I just like you can't read every paper.
Dr. Grant Garcia: So we're here as a team. Um, and I think we drop our egos cause all we care about is the patients. Um, so that's really important. And the ACL thing is like, you're dead on on that. I mean, there's patients that don't get the athletic mindset early on and it's a long recovery. And when you have that athletic mindset, you know, you can do big things.
Dr. Grant Garcia: You know, the one thing, you know, you probably heard me ask the patients before, it's like, how is your testing? And they'll be like, what are you talking about? You know, and if I get them from someplace like yours, You know, they got their testing with them as a sheet, you know, they've had everything done and they know they're ready or they know they're not ready and that's really important [00:11:00] too.
Dr. Grant Garcia: And so that's just the basics of just ACL in general, so I don't mean to interrupt
Zach Smith: you too much, but yeah, that's important. No, no, that's, that's perfect. And really that, that points to like one of, one of the things that we try to stay on top of, which is, you know, you mentioned the testing and when we talk about testing, we talk about the main one for, for ACL is quad.
Zach Smith: Testing with dynamometry, isokinetic strength, um, isometric strength. So we test at 60 degrees and we try to take more of a criterion based measurement of progress, right? There's, there's constraints from, from, from, uh, the physiological healing side. And then there's constraints from a strength and Performance side.
Zach Smith: And so what we try to do is try to marry both of those concepts and make sure that, hey, we're not stressing the graph too much in certain ways or like a meniscus repair, right? We can't load it in certain ways. But we want to make sure that if we can load something that we're not just fearful of, hey, we can't load, you know, anything, right?
Zach Smith: So someone that [00:12:00] comes in with a meniscus injury and they've got a brace locked There's no reason they can't do hip and core work. There's no reason they can't do upper body strength work. All of that helps to simulate their body and keep them from, from astro sitting elsewhere. So one of our big focuses on is on hitting other areas, right?
Zach Smith: So they come in with a knee injury. We could still potentially work ankle, definitely hip. Definitely core, um, and upper body. And so that's one of the things we work on. And then with the, with the testing, we've also got a very, uh, stringent return to sport testing that we utilize. So there's, you know, there's a lot of testing out there.
Zach Smith: They have sport court tests, which test basically muscle, uh, endurance and strength. Um, we'll do some, some one on one numbers, but there's really, and some single hops and double hop numbers, but really the big one is like you said, it's. The strength number, right? So there's certain things that we want to hit.
Zach Smith: And if someone doesn't hit those numbers, it's going to be really hard to progress them in their program. You know, if someone comes in and they want to start running [00:13:00] at 12 weeks, but they only have a 50 percent limb symmetry on quad strength, that's going to be very difficult from my perspective. But, but very easy to explain to the patient also.
Zach Smith: And most people understand that because we set these goals and expectations up front. Hey, this is what I would like you to be at eight weeks. I'd like you to hit 70%. Limb symmetry with your quad. And so this is the stuff that's going to take to get there. And if you don't do it, it's like a math test, right?
Zach Smith: You come in, we know that you haven't really done the work or we haven't helped to guide you in that work to get you to that 70 percent or there's something else going on and we need to reevaluate our approach as a physical therapist and a physical therapy clinic of why we're, you know, we're sitting at 50%.
Zach Smith: Um. At eight weeks, and you know, maybe there's a pain issue that we need to deal with, you know, maybe there's some manual therapies or something else we can do, or maybe we need to do some more blood flow restriction therapy to help boost that strength in the early phases, and so all of [00:14:00] that we try to take into account with the testing, but the testing really guides us and tells us, because there's been a lot of cases, you know, on both sides where I get someone, and I test, and I anticipate that they're going to be very strong, and then we test them, and And they're not strong.
Zach Smith: And then we have to look and say, Hey, why is this happening? Hey, we need to refocus. And sometimes it's a little bit of a reality check for patients, but in a good way, it helps them refocus. Because if I wouldn't have had those objective tests that can't, that just cannot, those numbers don't lie. And, and if I didn't have that test, I could have gone through six months of rehab, not knowing that, Hey, the quad actually is not getting stronger.
Zach Smith: We're just working on, you know, compensation methods through the hip and through, through the calf. And so there's a lot of things that we could do to help to, to guide them in the right direction. But we have to know these problems are happening. Um, and so like, obviously the easiest stuff is like range of motion measurements, everyone takes that.
Zach Smith: But really this, like most phases of the rehab, the [00:15:00] strength and the ability to accept and, and, uh, load eccentrically, that's going to be the most important piece of, of this rehab process.
Will Sanchez: Hey, Zach, is this something that you're measuring day one? So let's say, you know, someone like Dr. Garcia sends you a patient, they walk in through the door and you're doing this, you know, whatever it is, dyno meters kind of measurement, you know, that you're measuring the force and the power and what's.
Will Sanchez: the muscular strength. , are you doing that day one? And then how often, I guess, depending on the injury, how often are you going back to this test to see what the measurements are for the patient as for you to figure out you and your team to figure out that they're progressing in the right direction or you have to change course?
Zach Smith: Yeah, for something simple like a meniscus, uh, uh, Like a metastectomy where we don't, where Dr. Garcia doesn't go in and repair the meniscus. So we're not worried about tensile load on that meniscus. We can test them a lot earlier on, depending on the patient, usually like second or third visit. Um, for [00:16:00] ACL, we really don't want to test it.
Zach Smith: There's really no reason to test until about eight weeks. And so there's this period of time where we have to really motivate these patients within this early phase of rehab, because we're not even going to do that test. The knee is already, it's swollen. It's inflamed. The quad probably isn't even activating.
Zach Smith: The quad muscle isn't activating for the first few weeks very well. So we're using a lot of electrical stimulation and blood flow restriction therapy to try to maintain size of the quad. And so there's really not a whole lot of benefit to testing it that early on for us, as far as like the numbers that we see, because a lot of it's going to be inhibited by pain and fear.
Zach Smith: And so at about eight weeks, if we've worked them out correctly, we can get a very good, accurate number. Um, I've seen numbers as early as six weeks, uh, on an ACL and it's all going to depend on the, on the protocol, right? So like a, a meniscus repair or a root repair, and Dr. Garcia, you might be able to speak a little bit more on this.
Zach Smith: Um, we're not going to test those nearly as early because we can't load them into flexion. [00:17:00] And so it's going to be a lot more difficult for that. And so there's other metrics that we can take though, quad, quad girth. Like making sure that they're not getting so much actually in the quad that, you know, we know that muscle cross sectional area is directly related to strength.
Zach Smith: And so we know if we have those metrics, uh, you know, we've got some idea of what's going on. Um, and then after we take the initial test, it's every two to four weeks and we're doing a serial testing, right? Because strength testing can go up and down by anywhere, you know, like on a max effort day. Plus or minus 20%.
Zach Smith: And so sometimes we'll test somebody and then test them two weeks later and they're actually down a little bit or we test them in four weeks and then they've had a good restful night's sleep the day before and they haven't taxed their sexual nervous system. And then all of a sudden they've got a massive improvement.
Zach Smith: So we try to take regular tests throughout the process so we just can track it a little bit more Uh, like a linear progression and we can really see what's going on, like every few weeks, but really like every week, we [00:18:00] probably wouldn't get that much result with testing it week to week for the time, uh, sacrifice of it just because adaptation of strength takes a while to gain, um, especially in the later stages of rehab, but earlier, definitely closer together helps us gain some valuable information.
Zach Smith: Um,
Dr. Grant Garcia: yeah, I mean, that's a, those are important points you brought up, you know, the dynamometry is important. You'd be surprised some people don't do that, and, uh, I don't really get it. That's how I get the best test for me in terms of how people are doing. You know, cause they complain, they'll say, I've got some anterior knee pain, you know, I feel weak.
Dr. Grant Garcia: And I'm like, what's your dynometry? And they just don't know cause they haven't been tested for it. So it's really important. And I'm obviously not, I don't get that from your group, but that's an important thing to be part of. I think for Will, if he's heard this, he brought up this, this term a few times called blood flow restriction.
Dr. Grant Garcia: Oh baby. This is a really hot topic. And, uh, this might be the internal brace of, physical therapy. So if you don't want to listen up, but tell him a little bit about what your blood flow restrictions like. What do you guys like to use it for? You know, [00:19:00] it's a, it's a kind of sometimes controversial topic.
Dr. Grant Garcia: I'm obsessed with it. I love it. I would do it for all my patients if I can. Um, I do think it makes a difference. I tried it myself a few times. Uh, but maybe tell the listeners and, uh, maybe do, uh, help Will out too so he can do his prescription for blood flow now.
Zach Smith: Yeah. Yeah. Uh, so blood flow restriction therapy is basically, um, it's, it's a class of tourniquet, but unlike in surgery where we fully occlude the blood flow to the extremity, um, we occlude a certain amount.
Zach Smith: So basically how it's done is there's a cuff that's placed up at the Very top of the thigh right by the kind of in the groin area, um, and it wraps around the thigh and the, the customer we have are very smart. They have a built in Doppler and they have a built in pump. And so they're completely wireless and they run the Bluetooth to our phones.
Zach Smith: And what we first do is we take your what's called limb occlusion pressure. And we figure out how much pressure does it take on this cuff to include all of the blood flow in your leg. [00:20:00] And then the maximum at which we work is that 80 percent of occlusion. So we're not including full arterial, uh, blood flow, but we are including most of the venous, uh, flow.
Zach Smith: And so there's not a lot of return of blood from the limb. And so the science behind this is now very good. It's been mostly done in ACL cases. And we've shown that we can, um, we can really slow down the rate, and if not even pause the rate of atrophy, if done early. In rehab for post op cases such as knee, post op ankle, post op foot, we usually use it.
Zach Smith: Our clinic is mostly using it in the lower extremity. We use it a bunch in the upper extremity though to elbow, hand, wrist. Um, there's even some good, some good literature that shows that even though the cuff on the arm is placed at the armpit, it still has some effect. Because of the backflowing of the arterial system into the rotator cuff.
Zach Smith: And so basically what this does is it tricks your body [00:21:00] into a muscle hypertrophy. So there's three different ways that our muscles grow in size and grow a muscle growing in size is called muscle hypertrophy. And basically there's three different ways. One way is by eccentric loading. So that's the slow lowering on a squat or a bench press.
Zach Smith: So we overload that phase of exercise and we under load the concentric phase or the up phase. That's one way. Uh, another way is progressive overload. This is like the standard way that. Weightlifters get strong and big. They just progressively increase the weight at which they lift over time, right? Today, I lift 200 pounds on bench press.
Zach Smith: In six months, I lift 250. I will gain size and muscle by doing that. The third way is what's called metabolic overload. And that's basically where the muscle produces a byproduct during exercise. Usually it's, it's hydrogen ions and lactate and, and those are a signaling mechanism for your body to [00:22:00] increase muscle mass because your body is under stress.
Zach Smith: And so what these BFR cuffs do, the blood flow restriction is they block the blood flow from going back up into the body. And so it pulls those hydrogen ions and lactate and all of the other metabolic byproducts in. Muscle activation and physical exercise. And so it stimulates this massive response where your body thinks you're doing a lot more exercise than you are, which helps you to maintain and activate your mTOR pathway, which is the pathway for increasing muscle size and strength.
Zach Smith: And so. This is the basic mechanism. There's a lot of ways to do it. Um, there's some rules around it, right? There's some contraindications. There's certain people that can't do it, uh, because of like things like, you know, uh, having a blood clotting disorder, being on blood thinners, things like that. There's, there's a few things that, you know, would preclude you from being able to do this, but most, most healthy people can do blood flow restriction.
Zach Smith: Um, there's really not a whole [00:23:00] lot of downside. There are some, um, cases of, of a few injuries that have occurred with, with probably improper use and non high tech cuffs. But the cuffs that we use are, are very, are very high tech, very easy to operate and they're, they're, they're fairly user friendly and are very user friendly.
Zach Smith: And so, um, some of the protocols that we do for blood flow restriction therapy is we do a little bit higher reps and lower weights. So some of the studies are showing. That at about 30 to 40 percent of your one repetition max. So the maximum amount of weight you can lift you with BFR, you can get the same amount of muscle hypertrophy at early phase rehab, as if you're lifting.
Zach Smith: 80 percent of your one repetition max and about 80 percent of your one repetition max. And so the good thing is, is for things like ACL with like people that have anterior knee pain, uh, people who have had a meniscus transplant or a cartilage surgery that can't take a lot of Mechanical load [00:24:00] or a lot of weight load.
Zach Smith: We could do exercises with much less weight and get similar result in maintaining, uh, muscle hypertrophy. And so that's been a huge piece of our postoperative rehab for both the upper extremity and lower extremity. Unfortunately, you can't do it for like core injuries and back injuries, things like that.
Zach Smith: Although I did have an interesting case of a guy who had a, a, uh, radiculopathy, an injury to the nerve that came from his lower back, and he had almost no calf strength, and we did BFR for six months, and he was able to produce, uh, body weight strength of that calf. By the end of six months, which was very cool because, because previous to that, uh, he just couldn't physically load his calf enough because of the lack of nerve, uh, reception to the calf.
Zach Smith: So, um, we've seen really good results with it and it's just, you know, another tool in our bag that we use early on, especially in post op cases to help people get back to a hundred percent. [00:25:00] Hey,
v Will Sanchez: Zach. Um, yeah, I know. I love it. Yeah. Are there any restrictions? I, you, you mentioned certain restrictions when it comes to maybe the type of medicine you're on and blood thinners, things like that.
Will Sanchez: And, and, uh, I know Dr. Garcia and I talked about, , B F R before and, , and kind of going back to this KATSU training. , but. Is there an age restriction? Is this for all ages or is there a ideal age group that this would benefit?
Zach Smith: No, that's, that's a great question. Um, it really could benefit from people from all ages.
Zach Smith: So I've, I've used it up to people age 75. Uh, you know, obviously, and unfortunately, as, as we age, people, people tend to gain comorbidities and they tend to have You know, things like elevated blood pressure, they're on statin drugs, they're, uh, maybe they've had a stroke in their history or TIA, and they start to gather these, these, these contraindications to blood flow restriction.
Zach Smith:[00:26:00] So I think, you know, like, as the population ages, you become a little bit less of a candidate for blood flow restriction therapy, but you're not necessarily precluded because of age. The younger ages, that's kind of an interesting topic right now going around and I talked to a couple surgeons recently who say, you know, Hey, as long as someone, um, is, you know, 12, 13 years old, basically hitting puberty.
Zach Smith: I've got absolutely no problem with them doing blood flow restriction therapy. Um, It's all about tolerance though, right? Cause these cuffs at 80 percent occlusion of your, of your lower extremity. Um, we usually don't start at 80. We start to get them comfortable at 60. Then we worked up to 80 percent at 80%.
Zach Smith: Those cuffs are tight and maybe, you know, Dr. Garcia, I'm sure you felt this too. It's not the most comfortable thing in the world when pressurized or around your thigh and squeezing. And so, you know, some younger kids [00:27:00] don't have as. wouldn't have as good of tolerance to it. And some people in general don't have as good of tolerance to it.
Zach Smith: But I'm always surprised when I'm like, Hey, you know, I warn people, I say, Hey, this is uncomfortable. Let me know if it bothers you too much. It's not a hundred percent essential to your care, but it will definitely help you. And most people are able to just, Hey, I got used to it and now I love it. And we have a lot of patients that actually end up buying the cuffs for themselves to continue to do their workouts.
Zach Smith: Uh, Because, you know, they love, they love the results so much. And that's
Dr. Grant Garcia: a, that's a big thing, Will. The people do that all the time. I hear that they come in, they say, I bought my own because I was so happy with the results. Yeah. It's a big deal. And for me, it's one of the, you know, if I've got go to PT's, I really want to make sure blood flow restriction is an option, uh, for the patients.
Dr. Grant Garcia: You know, especially with some of those patients, you know, they're four months out, you know, Zach, and they're, Quads don't look great and they're ACL and you're like, are you doing blood flow? And they said no, I never tried it before and to me that's a concern, right? I'm also concerned if they say they are doing it and they look they look [00:28:00] weak But that's I don't tend to see that as often again Antidotal one surgeon, but I think it's important and it's a real thing I have a couple videos of me doing it and there's a burn Well, you you feel like you you feel very weak within a couple within a couple sessions
Zach Smith: And I actually do it a lot myself.
Zach Smith: Yeah, I do it a lot myself. I've had, I've had knee surgery on both my, uh, on both my knees. I've had, uh, posterior patellar surface cartilage injuries, osteochondral defects. Um, and so, so like injury to the cartilage behind my kneecap. And, uh, one of my, one of my training tools. When I'm doing knee load to maintain quad size, especially of my right knee is, is blood flow restriction and, uh, and, and yeah, even just bicycling, cycling for 15 minutes with blood flow restriction cuffs on is even on light resistance, it is a massive feel of workout.
Zach Smith: Like you're, you're like, you're on fire by the end of it. [00:29:00] And, uh, and the great thing is you don't have to load the knee. So my knee never hurts after I do BFR. But my muscles are always sore, and that's a sign to me of something that I need to be doing for my own personal need. And I know that a lot of my patients experience the same thing where they say, Hey, yeah, my knee didn't bother me at all.
Zach Smith: But my glutes and my, and my quads and my hamstrings are really sore, but like in a, in a good muscle way that I haven't gotten to feel for a while.
Will Sanchez: Yeah, it sounds amazing. I mean, , it sounds like we should do an experiment, but, , that'll be a conversation for another day. For my birthday, my buddy, , sent me a,
Will Sanchez: I'm looking at it right now. MetaQuest 2, uh, VR,, you know, going into, 2023 and beyond, right? We're seeing Apple jumping on it. We, you know, obviously we know about MetaQuest and I know that virtual reality is something that, uh, you're dabbling in. Can you explain a little bit about that?
Will Sanchez: Because virtual reality is just, you know, it's the future and it's here and I can't imagine where it's going to be [00:30:00] 5, years from now.
Zach Smith: Yeah, so we're using, using, uh, via, uh, VR and, um, kind of in a way that you probably wouldn't expect. So I think there, there's a lot of cool applications. Um, some of the stuff that we don't do, which, which I think we, we will now that we actually have a, uh, someone who's specializes in working with amputees is, is working on limb reintegration of like sensory stuff.
Zach Smith: So, you know, like phantom limb pains that people have. There's, there's some stuff coming out with via VR technology and. And using VR to reduce those phantom limb sensations. What we like to use it for right now currently is what we call sensory reweighting. And so basically when you get one of these lower extremity surgeries, like an ankle, uh, an ankle surgery, a knee surgery, hip surgery.
Zach Smith: You lose something called proprioception, or you diminish your proprioception, you don't lose it fully. But what happens is, because you've had some disruption to the [00:31:00] mechanoreceptors, or the things that recept, uh, information from your leg, like sensation, um, that's disrupted, you start to re weight. your sensation or your, your balance system to the other two systems.
Zach Smith: So there's three ways that we maintain our balance. There's your vestibular system or your inner ear, which basically helps you to a sense the, the, the horizon. And so, you know, some people get vertigo, they have a disruption of their vestibular system. You've got your, uh, proprioceptive system and your proprioceptive system basically senses.
Zach Smith: where your position is in space, right? So you've got, you've got your feet on the ground, your skin is in contact with the ground, you know your foot is flat because you can feel that. Your knee knows that it's slightly bent because you've got mechanoreceptors in your knee. And then the last system is visual.
Zach Smith: And the visual system is obviously like, if anyone's ever tried to balance and close their eyes, it automatically becomes harder because you've removed one system of [00:32:00] balance. And so what we do is we put people on hard surface, with a barefoot and we start to try to reweight the system back to the proprioceptive system.
Zach Smith: So after you've gotten one of these injuries or surgeries, your body is relying heavily on your vision and on your vestibular system. And so, uh, especially, you know, like for older adults who have vestibular dysfunction, but even like in dark situations, you'll notice that people are more likely to fall and get injured in the dark because.
Zach Smith: They don't have good proprioception and now it's dark. So they've eliminated their vestibular or their visual system. And then maybe they're turning their head. So their vestibular system has changed and they're more likely to get injured. And so what we want to do is we want to try to start to get that sensation back into the proprioception so that person can sense what position their knee, their foot and their ankle are in, in relative to themselves so that their injuries are less likely.
Zach Smith: So what we do is we. We put someone in a VR headset, and we have them do [00:33:00] things like riding roller coasters, or we have them do, um, like, like mazes and courses, or we'll have, uh, you know, like, they'll be watching gymnastics, and people will be flipping, so, basically, we're removing the visual system, or the actual visual feedback that's happening, and then, that change in movement from the, uh, roller coaster also helps to disorient the vestibular system, and it makes them rely very heavily on the sensory.
Zach Smith: Okay. On the proprioceptive system and what type of feedback they're getting from the floor through their foot, through their ankle, through their knee, through their hip. And so that's a lot of what we're doing right now, as far as balance training in VR. And it's incredibly difficult. I've ridden a lot of roller coasters now with a VR headset on, uh, standing on one leg.
Zach Smith: And, and it's incredible how much of a deficit you will pick up in someone like, like my right knee versus my left knee because of my surgeries. My right knee when I first started this, uh, was incredibly [00:34:00] diminished with proprioception, which led me to understand that, hey, my quad strength. And my lack of proprioception is leading to continuous injuries in this leg.
Zach Smith: And so if I want to try to prevent continuous injuries in my knee and my ankle on my right side, I gotta make sure that my proprioception is, is up to, up to par, and that I re weight a lot of my balance from my visual and my vestibular system. And so there's a lot of ways to do that without having VR.
Zach Smith: It's just a really cool and fun and engaging way to do balance, rather than just having someone stand on there. foot eyes closed and turn their head, right? So it becomes a lot more, um, engaging and fun for patients to gain back their proprioception. That's a great point. I hadn't
Dr. Grant Garcia:heard that before. I know a lot of stuff you're talking about, but that technology sounds incredible and it's a nice option.
Dr. Grant Garcia: And I, I, you know, I've been injured before too. And I've noticed that when my eyes closed, one of my legs is not as strong as the other in terms of balance. And Uh, I might have to [00:35:00] watch some more roller coasters to get stronger now that I hear this.
Will Sanchez: It sounds like a trip to Busch Gardens. Let's just go and do it for real. Anyway, , I know you've got a lot of stuff going on, with PT and you have some other technology, you've partnered with, , Theracentric, , and it seems like this is, an app for exercising for patients at home. If you want to talk about that a little bit and describe kind of like what, what is the benefits of patients having access to something that they can do at home?
Will Sanchez: Yeah.
Zach Smith: Yeah. I mean. Like Dr Garcia said about his surgeries of like, you know, two hours to three hours of work when he's doing surgery with physical therapy. The maximum amount that I'm going to have somebody in is three times a week, you know, for 45 to 60 minutes depending. But the typical person is really only going to be able to make time for one or two appointments.
Zach Smith: And so out of your entire [00:36:00] week and the amount of workouts that you have, one to two times a week is just not enough. And so if you really want to get the results and you have a high level goal, right? Like you have an activity goal. Hey, I want to be able to, I want to be able to hike up, um, poopoo point on tiger mountain, or I want to be able to jog a 5k, or I want to be, go back to basketball or tennis.
Zach Smith: Then, you know, you've got to, you've got to work outside of the clinic. It's not just about what you do inside the clinic, because if you rely on just what you do inside the clinic, you're definitely not going to achieve the result. And so we have partnered with several physical therapy exercise apps in the past, and this one is probably, is definitely the best that we've had.
Zach Smith: Um, and it's great. It gives access to patients, um, anywhere they go. Everyone takes their phone, right? Like if you give someone a printout. Or even yet, like, you know, some, some PT clinics are still drawing stick figures, um, which is fine, right? Like if that gets the job, if it actually gets the job done, that's fine.
Zach Smith: But the nice thing is with our [00:37:00] app, you've got videos of every, every exercise. It'll time your rest breaks. It'll help you count your sets and reps. Um, it's very smart how it'll guide you through. It'll help you motivate gamifies. You know, streaks of getting into physical therapy, exercise in your home exercises.
Zach Smith: Um, and so all of that combined helps people be more successful. And the cool thing is that I love about this exercise is that I can on the spot. With HIPAA compliance. So I can, I can be compliant with the medical laws. I can shoot a video of you doing your exercises and put them into your own exercise app, and so you could see me or you could see yourself doing your actual exercise.
Zach Smith: Um, so instead of a patient. Taking these videos on their phone and then trying to figure out how many reps and sets we can actually integrate these videos right into the app where they see the reps and the sets and the rest breaks and all that. And then when they pull up the video at the video of them inside of our clinic, doing that very specific exercise.
Zach Smith: And so that's the great thing is like, if we come up with a unique, very, um, [00:38:00] customized exercise for somebody, then we could say, Hey, this is like. This is exactly how you do it and when I voice over the, the, the video as I'm, as I'm shooting the video, they get the very specific instructions. So every time they're at home, they hear me coaching them through the exercise or they can hear me coach them through the exercise that they want and we found that our compliance rate with home exercise program has, has over doubled.
Zach Smith: Since we switched to this, to this technology based, um, home exercise program with higher tech, uh, app. And so like, if I can get somebody at 70%, 80 percent compliance with home exercises, um, we know we can do a great job versus industry average of 30%. It's just, it's really not enough load to get the adaptation that people are going to go for, especially, um, if you're trying to get back to an activity.
Dr. Grant Garcia: No, and I think that's a good point. Go ahead. I think it's a good point that the, you know, the on the number of patients I see that, you know, they kind of forgot about the home [00:39:00] stuff and then just do the PT at home, PT. And then as you know, as your insurance starts to run out toward the end of the year or by the end of your surgery recovery, you know, the home stuff is really important.
Dr. Grant Garcia: So I think it's good for listeners to hear that. There's a better option out there than just stick figures or print offs. I mean, I've seen the same thing, you know, my family members have gone to other PT places just cause it was closer. Um, not that they shouldn't have gone to high def, you know, uh, but nonetheless, when they go there, we get printouts and they're going to lose those things.
Dr. Grant Garcia: I mean, I, first time my mother in law brought home printouts, they were lost within 24 hours. And so the, the, the, the online ability, don't
Will Sanchez: get yourself in trouble. Dr. Garcia.
Dr. Grant Garcia: They may be listening. I'm not getting myself in trouble. Okay. I'm not getting myself in trouble. I'm good. I'm always in trouble though.
Dr. Grant Garcia: Let's be honest. So the, uh, so, but it's important. It's important. And that's a really good thing for the patients to know that there's a high quality app out there that'll make their lives easier and get them back faster, which is again, that's the whole point of our show. That's the whole point of what we do.
Dr. Grant Garcia: That's the whole point of what you do [00:40:00] and what I do. We try to find a way to get our patients back faster, be more compliant, do well and look good. Because honestly, if they do their homework, it's going to make you look good. And it's going to make me look good. And let's be honest, those are all important things.
Dr. Grant Garcia: So the key here is all patient compliance is important.
Zach Smith: Yeah. And there's like one more thing on that printout thing. The thing that always got me with those printouts is that you have a picture of the start and you have a picture of the finish, but you miss everything in between those two pictures. And that's really where the money is, is, is in execution of the exercise and knowing that you are, Executing it correctly and people also feel more confident when they can see the exercise and they also hear the Explanation of the exercise and we go.
Zach Smith: Oh, yeah. I remember when he said that to me in clinic This makes all the sense in the world versus back back You know four or five years ago when I was giving out printouts people come in and they'd like yeah They're doing this right the whole time and I'd recheck it and it's just completely off And, [00:41:00] and not that there's not variation to exercise, but it's like some of this stuff would be completely, uh, you know, like this wasn't even close.
Zach Smith: Um, and so that's really what, what, what I've loved. And then also on our end, we get to see when patients log in, how many exercises they've done, how many sets they've done, and I can see how many minutes they've spent in the app. And so I can really help to hold people accountable, which is kind of. The way that I think physical therapy should be going is into not just rehab and the clinic, but health coaching somebody through their entire journey of physical therapy and helping them to stay motivated because, because I know I like to work out and I like to get in the gym, but I always train better.
Zach Smith: When I've got a coach or someone looking out for me, or I've got a workout buddy. And so that's what I think that this helps us to bring is, is the accountability side and people feeling like, Hey, this person's in it with me versus, you know, Hey, I see this person once a week. And then when I'm not in there, it's kind of out of [00:42:00] sight, out of mind.
Zach Smith: Exactly.
Will Sanchez: This is Zach Smith, physical therapist and co owner of HiDefPT. Check him out at H I D E F P T dot com. Zach said it earlier in the show. If you go to his Instagram and check everything out that he's posted, some really cool stuff. But he mentioned in the beginning. It's walking into a gym.
Will Sanchez: It looks like a gym. It feels like a gym and they're getting to work like a gym. Zach, thank you for your time. We really appreciate everything and please check out his website. Reach out to him. We need to get into a bunch of other stuff and dry needling and God knows we could have gone on and on but please check out his website.
Will Sanchez: Reach out to Zach and his team. They've got a lot of great benefits. Obviously, Dr. Garcia loves dealing with him, sending his patients over there because they know they're in great care. Zach, thank you so much for your time. Thank you for being with us today.
Zach Smith: Will, Dr. Garcia, thank you guys [00:43:00] so much. I appreciate you having me on.
Zach Smith: It was a fun conversation. We'll have to run it back again. I've got some questions, uh, for Dr. Garcia. Um, and so I think we could jump into some cool stuff. I appreciate you guys though. Thank you.
Dr. Grant Garcia: Awesome. Yeah, no, thank you. I know we always, every time we do this, Zach, we always have like a million things afterwards, a question.
Dr. Grant Garcia: So let's do
Zach Smith: it again for sure. Yeah. Yeah. Let's
Will Sanchez: do it. Okay. Take care, Zach. Dr. Garcia, great show. , most important thing that I want to kind of, you know, relate to the audience and you talk about it, Zach's talked about it, is the physical therapy part of what it is. we need to do, right? When I had, I tore my Achilles, I've had injuries, I've had surgeries.
Will Sanchez: The only reason I've gotten back is because I went to physical therapy and I was diligent about it, right? And I went home and did my homework that was put out there for me. And now, like, my left leg that I had Achilles, my [00:44:00] Achilles injury, my rupture is stronger than my right leg because I worked so hard at it and I did ladder drills and, and did balancing acts.
Will Sanchez: and single leg, , exercise and all these other things. So I just want to reiterate to everyone out there, you get what you put into it. And if you put the work in post surgery, you're going to have great results. Dr. Garcia, as we wrap it up, last thoughts, , on this show.
Dr. Grant Garcia: Well, it was just, it's incredible to hear all the technology coming out there.
Dr. Grant Garcia: And again, I completely second and third what Zach and you said. about compliance. It's really important. It's good for our patients to hear. Listen, there are if you have something that you're dealing with some problem or either non surgical surgical, um, and you're feeling like you're not getting what you need.
Dr. Grant Garcia: You know, there are places out there that can do it for you. Or if you are certain things that you're missing, there might be, you know, pay people or we know our bodies and it's important understand that there's technology out [00:45:00] there. That's why I do all the marketing. Um, for myself, because patients don't understand what's out there.
Dr. Grant Garcia: I mean, I've saw multiple patients even today that had, that we had technology we've been doing for the last few years and they had no idea they could have saved their knee with this, this opportunity. So it's just more information gathering for patients to teach them. So they're not, they're learning better and they're understanding what gets them back in the game.
Dr. Grant Garcia: And in the end, like we've said before. Patients first, getting them back to things they love, because when that patient comes back and they say they're back to everything, that smile on their face, it's worth everything. For Will
Will Sanchez: Sanchez and Dr. Garcia, special thanks to Zach out there, and I promise Dr.
Will Sanchez: Garcia is going to work on getting that miniature pony out there for our listeners, don't blame me, blame Dr. Garcia. We appreciate you listening. Thank you for listening to Sports Doc Talk. Dr. Garcia, have a great night.
Dr. Grant Garcia: Take care.Audio Transcript
Highlight Episode: Nick Chubb Injury and Aaron Rodgers Surgery

Will Sanchez: [00:00:00] Welcome
everyone and thanks for listening to Sports Doc Talk. I'm Will Sanchez along with our orthopedic surgeon and sports medicine specialist, Dr. Garcia. Dr. Garcia, I had everything planned out for this show, right? We were like, we're going to do a show on Aaron Rodgers. We're going to talk about his Achilles and the procedure and who he went and how he went into the darkness is going to come back and, you know, in three days and rise again for the New York Jets.
But we'll get into all of that. Unfortunately, we've got some really bad news and we know how difficult, how beautiful the sport of football is, but at the same time, how difficult it is. Nick Chubb had an injury tonight and we're doing the show Monday night, Dr. Garcia, when you saw the injury, you heard about what happened to Nick Chubb, what was the first thing that you thought about and let's get [00:01:00] into what type of injury this is.
Dr. Grant Garcia: So I'm, you know, I had my usual friend group and I saw this and get texts blowing up saying, you know, do you see what happened? You see what happened? And looking at the injury footage and then hearing from most people, I mean, it's only been injured for less than an hour. And I've heard from about six people asking what happened.
So obviously this is a pretty hot topic and people want to know because he's a very high profile player with a pretty bad injury. So basically had a knee dislocation and in isolation, this is really not a good thing. You know, for me as a sports surgeon that is the last thing I want to see on the field.
You know, there's obviously severe neck injury with paralysis. We don't want to see that or, you know, the Demir Hamlin injury, but those are really rare. This one's not as rare, but fairly rare. We've seen a few players with it, but having knee dislocation is just awful. It's one of the worst things we can think of.
And there's been a few players that have had this, but unfortunately for Nick Chubb, this is actually the second injury of knee dislocation on that same knee, which just makes this a whole [00:02:00] other level of. But basically if you look at it, and again, I'm not there examining under MRI, but if you see it in slow motion, it's pretty obvious what happened.
You can see he tears his MCL, which is the ligament on the outside. Almost definitely tears his PCL, which is the ligament on the inside. That's the one you hear about less, probably tore his ACL. His posterior corner, or LCL, which he had reconstructed in Georgia in 2015, may be okay, but this is considered a grade 3 or 3 ligament dislocation, and the other concerning thing is an injury to his artery, which I know there was a Bears player, or one of the players, about last year, that had to get rushed emergently to the operating room because he had an injury to his artery, so this is This is a bad combination of things and we'll obviously see how it unfolds and I just hope that this obviously is not the end of his career, but also that he can, you know, there's no major arterial damage and they can protect him and they will again with NFL.
We've seen them. They can do things that most places if you got injured on a field, you wouldn't be able to do. So I do have faith [00:03:00] that they're going to get that done.
Will Sanchez: All right, I have a question here. So just kind of going back to let the listeners know you mentioned in 2015 as a sophomore when he was still attending University of Georgia, he dislocated his knee toward the MCL PCL LCL in the same left knee that he had the injury tonight.
If you're in a physician, if you're running out in the field to treat him what is the one of the first things that you need to do? Because obviously there's Some besides the the physical trauma what's happening emotionally because it's such a serious injury So you have a team go out there What are the some some of the first things that you have to concern yourself with the player and the injury at the same time?
Dr. Grant Garcia: Well, let's assume they saw the footage before they went out there or they saw them the injury itself And they might not have and they ran out right because he goes down Says he's injured and then now you're seeing the game footage on the screen or on ESPN P. N. But that was the zoomed in one. Let's say they saw the footage.
The first [00:04:00] thing I'm worried about is his state of his leg. Because you know, I've seen in residency and things like that, injuries like this where they go on attended and you have a major problem because you've lost arterial or a supply of the blood to the leg. So the first thing I'm running out there doing is obviously making sure that it's relocated so that it needs an appropriate position.
But the other important thing is making sure that there's a pulse in the leg and you see that people check their pulse in their neck, their arm, you know but you can also check in your feet and that doesn't give you the whole story of whether this is a real injury. There's some other tests you have to do, but just checking for that initially is something that's important and making sure that the foot looks like it's got some normal perfusion and not like all of a sudden it's becoming, you know, pink or a different color.
And again, really quickly it just happened. So it might not have happened at that moment. Yeah, but that's the first thing I'm checking and then I'm getting him off the field as soon as possible.
Will Sanchez: When it comes down to this type of traumatic injury, right, and whether it's the femur, the tibia, whatever that's no longer connected to the knee, and it's, [00:05:00] for lack of a better word, it's not funny, but it's one of those words that is used, dislocated knee.
It doesn't sound bad, but then obviously when you describe what the injury is, it's really bad. What is the concern and how do you check for possible nerve damage in that immediate situation? Or is that something that you have to do when you get back to the locker room? What's what's that concern like and how do you recognize it immediately?
Dr. Grant Garcia: So damage to the nerve is usually on the outside of the knee, there's a nerve. You can have damage to the other nerve on the inside of the knee, but that's a lot less common. Okay. But damage to the outside of the nerve was with someone, you've probably seen someone that wears a brace called a, it's like an AFO or something where it keeps the foot from slapping.
So the nerve, the nerve that lets your foot lift up can be injured in this type of injury. Probably, Nick Chubb probably didn't have it at the initial time, because obviously he wouldn't be the level he is right now. But that can happen and that's a big deal. I've seen that before a number of times.
With these massive meatus locations, so you can have a nerve injury and you can have an artery injury. The [00:06:00] nerve injury is A bigger problem in the long run, right? Because sometimes it doesn't come back. But the artery injury, the nerve injury, if it happens and you notice it, there's nothing you can do at that moment.
As long as you've relocated the knee. The biggest thing is to get the patient's knee, or to get the player's knee in alignment, and get them checked out to make sure it's not an injury to the artery. That's the number one thing to do right now.
Will Sanchez: All right. And the last thing before we move on just because I'm just fascinated by this type of injury and I just, I can't imagine going through something like that.
How do you deal with the dislocation? Is that something that you're going to deal with before you go to the hospital that you have to pop it back in place or move it into place? I'm not, I'm probably not saying it correctly as far as you saying the word. Those are good questions. But you know, how do you deal with that?
Because this knee is. out of place, and I'm assuming that this is extremely painful.
Dr. Grant Garcia: So, the answer to that last question is yes. [00:07:00] But the the problem is this is the second knee dislocation, right? Yeah. Because when you tear three ligaments, usually the whole knee dislocates. Now, this is quite bad. It went backwards.
You could see it just completely go in a different orientation. Ugh. And bend in a way it's not supposed to go. And so he's gone through this before. And this may be one of the reasons that dislocated like this, because the ligaments you make in theory, they're stronger, but they're always a little bit higher risk.
And once you got damaged to your ligaments and things like that, you're at a higher risk. Now, again. He hasn't gotten injured or had significant injury like this since 2015, so he's done fairly well since his Georgia injury. So that's impressive, and I didn't realize he had dislocated his knee before until this happened.
Because you wouldn't expect a player of that caliber with this injury. So he's already proven he can do it, but revision surgery, we've seen with Odell Beckham Jr. with an isolated ACL revision. much longer recovery. And this is a bad, bad one. I mean, this is the second injury of this caliber. I don't, we have to probably look it up.
But I don't know of anybody that had a second one in the same [00:08:00] knee and made it back. But again, I have to do my research, but this is not the one that I would wish upon anybody. And again, we don't have the actual, you know, maybe his ACL is okay. Maybe it's his PCL but to dislocate your knee that far back, usually you have to take advantage of a number of ligaments.
And it's going to be also tricky, I think, again, this is, we don't want to get this podcast too long for the listeners. Too late. But the other problem you have to think about, yes, too late. So, well, this is complicated, but this is super interesting, people that want to know about it. It is. So basically, this is a whole nother level of injury, if you want to talk about complex, like the guy getting this injury right now, and I don't know if they're in the Cleveland Brown Stadium, if they are because a few of my friends are actually
Will Sanchez: team docs.
No, they're at the Steelers. facility, in fact, the fans did a good job and cheered for him, so it was nice.
Dr. Grant Garcia: Yeah, so there's some really good surgeons there at University of Pittsburgh, and I imagine that the surgeons for Cleveland are there also for the game, and so they're both going to go right now to figure out what we need to do for him.
He won't operate on everything right away, because you don't want to do that, because there's a lot of... This is a whole [00:09:00] nother lecture we could do and talk on this. We may want to add this as a talk later on. But basically they want to stabilize him. The same thing as trauma. This is like a trauma to the knee.
It's like a car accident, right? Like you're not going to fix everything right away. Yeah. You're going to figure out, like, let's calm everything down and do the big stuff later. So let's not worry about the major stuff. But the problem you have is he's had reconstructions already of his PCL. Probably his LCL and probably his MCL.
So he already has new tissue either used from his own knee or from cadaver, but probably a combination of both. And so now where are you going to get it from? So he can't use his own tissue because a lot of it's been taken already. And maybe from the other leg, but do you want to do that in a running back like him?
Yeah. And will he, can he, can a cadaver ligaments hold up in an NFL player? Don't know. So, you know, this is a, and now he's got tunnels and probably hardware in there. So this is not like, this is a straight up simple, let's go reconstruct everything. They're going to have to figure out things to avoid.
Because he's took him, he's done some wear and tear on these ligaments over time. And it's not the same as your own natural ligaments. So this is going to be and there are some really good [00:10:00] surgeons at both those places. And he's probably going to get some second opinions very quickly. But this one is going to be this
Will Sanchez: is going to be a dizzy.
All right, I'm apologize right now because I have another follow up question, and I'm really sorry, but this is I've got so many thoughts on this Will they consult the original surgeon? I don't know who it was right from Georgia or whoever they wherever he had a surgery When it comes down to something like this that they're going back in to Refix something that was already broken and fixed would they make a phone call or hey?
You know like consult at all or go back and look at some of the old film To, to see what they're dealing with, you know, before they jump in.
Dr. Grant Garcia: This is a great question. This is a revision question. So I do a lot of revision ACLs and revisions such as this level. I mean, this is a pretty unusual injury. But whenever you're doing a revision, you want to get data from before, right?
Because let's say they use something that's metal. You don't know how to take it out. Right. It's there's hundreds of metal implants out there, and they're all required different [00:11:00] screwdrivers and different removal devices. So if he's got a bunch of metal in his knee, and I don't know, I've never seen the inside, but he's got multiple screws that are different sizes.
It's like you go into a car and you don't read the instruction manual. How do you take out the engine appropriately? If you don't have all the right, the right ratchets and the right wrenches, et cetera. So if this is something where it has that, this could be a whole nother level. Again, these guys are good.
This is not something, you know, you're used to going into the operating room, and if you have to kind of audible things, you will but they're definitely going to consult previous notes. I don't know if calling the surgeon is something that they would always do, because, you know, how are they going to remember from 2015?
Obviously, he's a big deal, so maybe they do remember that surgery. But overall, you know, it's But you, we all use somewhat similar techniques. We have different variations, but you know, there's some, there's good ways to do an a c l. There's good ways to do a posterial corner. There's good ways to do an MCL l.
Yeah. So if you do it relatively a good way, you know, kind of what's going on. And a guy like him who was checked out a number of times during the draft and each time he's gotten through physicals. Yeah. You know, his knee was checked out for quality. And so, you know, I don't, I'm not super worried about that [00:12:00] part.
But yeah, they're gonna do some homework tonight for sure. This is gonna be an all night event. At least preparing if they have to do anything for him. So this is behind the scenes. This is a whole nother animal. We had a lot of these giants players that had these severe urgent injuries and not even this level.
And it was, you know, this is going to go into the wee hours, probably. Man,
Will Sanchez: that wow. All right, we're gonna move on. I, I, I'm telling you, I could, I could ask a bunch of other things. And, you know, we, we've done so many shows with new tech and everything else, and we're 2023, and this, this procedure happened in 2015, so I could imagine the changes from Then to now and going back and you know, whether they have to, like you said, finding the right screws and you see him, I, whatever I'm going down to rabbit hole.
Let me, let me move on. He's going
Dr. Grant Garcia: to have a few internal braces. If I have to make a comment
Will Sanchez: about that. Oh man. You know, you just, you, you just like, you just like saying the term brace because it gets, it gives me a hype, man. I get so high. Let's, let's get right into it. You know, Aaron Rogers, man, traded to the jets on April [00:13:00] 24th, 2023.
I mean, Every JET fan, and I have a lot of friends that are JET fans, they ran out and they got, they bought tickets. In fact, my buddy's going with, with his son and his grandkids to the JETS Kansas City game. They got tickets because it was the kid, the kid's birthday and everyone's excited. And HBO is like, we're going to put them on hard knocks.
And the NFL is like, well, opening night, we're going to have them play Buffalo Bills division rivals. on September 11th. And that night, you know, it's packed stadium. Aaron Rogers comes out by himself running out of the tunnel with the American flag and it's waving and the crowd is just rambunctious and just Absolutely rock star atmosphere.
The place is jumping. The savior is here. We're finally going to win a Super Bowl after 54 years, going back to 1969 and Willie Joe, name it. And four [00:14:00] plays later, Aaron Rodgers gets sacked. He stands up and he sits back down. And something is wrong before we get into a real quick when you heard about what had happened when I heard about when I saw it was unbelievable.
I couldn't believe it. But when you heard about what had happened, what was the first thought? Because you're a Giants fan. You're a football fan as a fan. What was your thought
Dr. Grant Garcia: as a fan? It was horrible. You know, that's the last thing you want to do for a team that really needs the motivational boost. And, you know.
You think about what you, what you want about Aaron Rodgers and other things he's done, etc. But you know that what he's brought to the team and what he's brought to the fans in New York Jets, you know, and the fact that this happened so quickly after the first game. I mean, it's just, it's just frustrating as a fan of any team and just you feel badly for those, the Jets fans, you know, and you feel badly [00:15:00] for him.
Too because this is not an easy injury to recover for and I think you'll get back but That's not why we're doing this show is because whether or not we think you'll get back. We're doing it for the The innovative tech that he was supposedly given.
Will Sanchez: Yeah, get into this orthopedic surgeon that had performed this surgery.
He has a history of working on athletes and some notable ones, so can you talk a little bit about this specific doctor and the type of work that, and the type of players that he's already done some of these surgeries on? Yeah,
Dr. Grant Garcia: so I think the more important part of this talk is the behind the scenes. because this
Dr. Grant Garcia: is, this is no cakewalk to take care of Aaron Rodgers. And you probably heard that he texted the doctor right after he got injured, you know, telling him, get ready. I'm getting operated on tomorrow type of thing. So this is a guy with a speed dial to professional athletes at that level.
Wow. So this is Dr. Neil Elitrosh. He's the team physician for the Los Angeles Rams. He is the Grand Master of Curl and Jobe, which is a extremely prestigious [00:16:00] LA fellowship. I actually had the pleasure of interviewing with him. He's a really nice guy and obviously, you know, really well known. You know, my most memorable post I saw of him was him with having operatable Sylvester Stallone and Arnold Schwarzenegger in the same day.
So this is the type of guy that we're talking about. He's on Saquon Barkley, you know, Joe Burrows, Tom Brady you know, and he's, he always is pushing the envelope too. You can see, you know, he mentioned the word internal brace a lot, you know, with he talks about Tom Brady, how he internally braces MCL to get him back when he had that MCL injury.
And he does a lot of behind the scenes celebrities as well. But, you know, if you look up at so many professional athletes and he's. He's always been a high level player in terms of you know, one of the cutting edge leaders, one of the leaders for the celebrities and for the athletes. But over the last like five to six years, he's really taken off and, you know, he's really good friends with the CEO of Arthrex.
And so he's done a lot of innovative things through Arthrex. Obviously that's, we've talked about them as an innovator. And so he's, he's well known throughout the world. You know, he's the Tommy John guy. He's [00:17:00] the now knee guy. He's the shoulder guy, you know For Jacksonville, he's the one that did the eight anchors on the quarterback for, he's the one that said that was the worst tear I've ever done and, you know, ended up putting, you know, eight anchors in the shoulder of a normal human being is a lot.
So, you know, he's a, he's, he's done every one you name. I mean, if you look up his type of injuries he's done extremely prestigious. So, Dr. Neal Eltrage is the physician, and you'll probably, you know, he may get consulted on this one. You know McGregor?
Will Sanchez: Yeah. McGregor went down. Conor McGregor from
Dr. Grant Garcia: UFC.
Yeah, look him up. So my friend did the, my friend is a trauma surgeon at UCLA, did the surgery, but Neil Alatrosh was, was required to be in the operating room to do it as well. So Neil Alatrosh, I'm not sure he is an expert at tibial shaft fractures, but he was in the surgery because he's a celebrity surgeon.
Yeah. So that gives you an example of how big a deal he is that McGregor wants you in the operating room.
Will Sanchez: All right, let's talk about this procedure, right? And you know, I, I was excited not about the injury, but the fact that they did this internal brace and [00:18:00] I went to look at it because I'm just, I'm fascinated.
You know, I'm, I'm dying to do it on, on a patient and we got to find a way. I might have to go to a different country to get away with it, but they showed where they, they drilled in and placed internal brace and how they pulled it. The Achilles together to hold it in place. So just talk about that procedure.
And I don't know, what are they calling this? The speed bridge for this torn Achilles? Yes.
Dr. Grant Garcia: So I will burst the bubble a little bit that this is not new. This has been around for a little while. Yep. The idea, the word internal brace, which we've talked about, and please listen to our previous episodes about internal brace, internal brace is where you do a bone to bone.
So in this situation, he technically wasn't internally braced, but everyone loves that idea. And so now everyone's using it for anything. It's now a catchphrase. It should be your catchphrase, but nonetheless... I'm gonna get a
Will Sanchez: t shirt that says, I love internal brace.
Dr. Grant Garcia: I'll get you one. I need to get you one.
There you go. So the so basically he wasn't [00:19:00] technically internally braced because remember the word brace is to sort of make it rigid. And you don't want to make the Achilles rigid because the Achilles has to stretch so far. Yeah, you need that flexion, right? Yep. Yeah, and again, you don't internally brace tendons, you internally brace ligaments.
So ligament is the UCL. A ligament could be the A C L that you internally brace. The M C L is a ligament, but the a achilles is a tendon, and so by bracing the tendon that would be very bad. So he technically wasn't internally braced. So the procedure that he had is called a speed bridge. We do it in the shoulder as well.
I've done this in the Achilles before. It's a really slick way of doing it, and the thought process is that when you tear your Achilles, You split it mid substance. Initially, the older way of doing it was to do it open and then they came up with percutaneous techniques where you can do it through a small little incision, maybe like, you know, a little bit longer than your thumb.
And then you can connect them together and sew them. Well, the third way of doing it is the way that Aaron Rodgers had it, where you kind of say the bottom [00:20:00] part's like pretty good, so you maybe put a stitch in that, but the top part's where the big part of the Achilles is. And so you sew that directly into the bone, so the fixation is much more rigid and you can move people faster, and there's a lower chance that they're gonna tear out.
So they dumped it into his heel bone, which is what you probably saw. And the speed bridges, that means it's a lot faster with no knots or anything, because the knots can cause injuries. Because one of the biggest complications of Achilles is to get an infection. And so that's why these percutaneous techniques have been invented, because Achilles were known for having problems with having wound infections.
With these new percutaneous techniques, it's extremely low, and now you have this newer technique, the speed bridge technique, which fixes it into the bone, so it's much more rigid fixation. You never want to really be repairing tendon to tendon together, that's why this newer technique is so impressive.
Will Sanchez: Your tendon snaps, right? So, there's a part of it that's up and there's a part of it that's low and they're not connected. So, when they did this procedure and they're bringing them close together, are they just bringing it close [00:21:00] together and letting the body heal itself because now they're next to each other?
Or do they have to, at that point kind of connect them?
Dr. Grant Garcia: So that's, that's the best question you could, you've asked tonight and you've asked some good ones. So that one is the trick that people do that. Even when I was learning this and we learned about this, it doesn't make any sense. So it's a lot of people can be treated without surgery with an Achilles injury.
If you keep the person in the elevation, eventually the tendon will grow back together in some cases. So there is some data that you can do non operative treatment, especially in patients as they get older. So the idea is that it doesn't have to be in the same, the same zip code, right? Or maybe this is the same household.
And so. We used to tie them together either with a big open incision or this percutaneous technique. But what I was saying before is they really don't care about that bottom tendon, and they just pull the thing down as close as possible and keep it rigid. And then the idea is that by keeping that part rigid and stretched out, you don't have a likely chance it's going to pull off.
You can start moving faster, and the little leftover tendon We'll heal back there [00:22:00] and eventually it'll be fine. And the first couple of times I did this, it was really weird because you're used to like repairing everything back together. Like you want to make things look perfect, right? Yeah. I'm an OCD perfectionist and you have to tell them, no, don't worry about it.
It's not a big deal. It'll be fine. And that's what these newer surgeries, you have to kind of come to the comfort level. And it's always these. Really big innovators that cutting edge that understand this and learn this and teach this and invent these techniques understand ahead of time, and then you slowly pick up on them, but that's exactly the point.
So this is it is a partial repair, but really, it's just basically putting in the same household and then the body will heal it because it's not moving, right? Because it's been braced down to the ground.
Will Sanchez: Are you, are you doing anything or are you adding anything to that area to speed up the healing process besides, I'm, I'm assuming that they're going to put them in a boot, but is there anything else that they can do to kind of, yeah, we're in the same neighborhood, but we want you guys to be a little bit friendlier, quicker, and not just kind of you know, bumpy to each other in the street, [00:23:00] you'd be like, hey, no, you're, we're, we're putting you in the same in the same place.
Dr. Grant Garcia: So they're probably using, you know, they may have used. And again, the data is kind of mixed and whether any of those type of biologics help them, but it's Aaron Rogers. So why not throw everything at him, right? The other thing is you don't want to give him too much stuff in there and then causing infection, right?
Cause you give him too much things. You're not really, you're kind of experimenting with and trying new things. You want to be careful, right? It's just a fine balance. Now, if you're in Dr. Neal Alatrosh doing this. You're not super worried about your reputation because you've got such a big deal. So you want to try something that's going to get them back faster, that's going to look better, right?
Yeah. And then they're going to use that special dressing I think they had talked about that's an antimicrobial because again, we don't want an infection because the most common place to get an infection is right here where you had it. Now again, probably had it done percutaneously if Dr. Neal Eltrash did it.
Yeah. But nonetheless, you know, that's something to be aware of as well. So. They're, they're attacking the healing process from rigid, solid, incredibly good fixation so you can start moving early, because remember we've talked about [00:24:00] this, the faster you can move our patients, the better they're going to get back to, that's why internal brace works so well, because you can move them faster and test the ligament faster.
That's the whole, that's the whole reason why it's so effective. And things don't stretch out. Two, you know, you want to make sure you don't get an infection. So you have a special dressing and three potentially biologics. So you've done everything right in the body to make it go better. And I think this is be a great topic at some point for one of our, our show is to kind of say.
What makes things better, right? And this is this, this device, this technique has made better. And, you know, where it came from, Arthrex, which we talked about before. So this is, this is a combination of, and you could see they jumped right on. I mean, there have been multiple Arthrex posts about this new technique in the speed bridge and really bringing light to it because it's done a little less frequently than the side to side repair.
And it's just surgeon preference, but I've done it before and I've been extremely happy and that's sort of the way I now fix these because of the fixations are rigid in the bone. But also I'm a proponent of rigid fixation as it is. I'm an internal brace guy. You know that. Oh baby. [00:25:00]
Will Sanchez: And also having a smaller incision also helps with the healing process, right?
I mean, I had my Achilles done years ago and you know, I have a. Six inch scar right down my Achilles compared to the, you know, the small incisions that Aaron Rodgers had for
Dr. Grant Garcia: this procedure. Yeah, and that's 100%. I mean, that's why we started doing it. It was helping with healing because the other thing is when you get your whole Achilles opened up and I don't want to gross out the viewers but there's, there's a tendon sheet around that that has blood supply into it and that can get damaged as you open it up and try to repair it.
So, you know, I think we go for smaller and smaller decisions, not because the idea of it's sexy that you can do minimally invasive, but it's actually better for the patients and the less trauma that your body has, the faster it can heal. Okay. And so that's why minimally invasive works if obviously there's certain areas where we can't be minimally invasive if you shatter your heel.
You know, you're not getting a minimally invasive repair because you have to open it up and get all the pieces back together and etc. But we are getting better and better at [00:26:00] minimally invasive surgery and this is one of the reasons why so we can get you back faster.
Will Sanchez: Okay, he's talking about recovery and getting back by the end of the season he's 39 years old.
He just had this procedure. He wants to get out there by the time you know, playoff start, which I don't think the Jets will be in the playoffs, but that's a whole other conversation. We're just talking about the timeline. If you had to, if you were a gambling man for 39 year old, after this procedure for him to get back on a professional football field with 300 pound men chasing after you, What would the odds be of that?
Dr. Grant Garcia: So we've been wrong on gambling many times on this show. I will tell you absolutely not. But I will tell you absolutely not. This is, this is ludicrous that he was told he was four months. But you know what? Everybody's talking about it. We hit ESPN. I saw a big huge article on ESPN talking about he's going to get back in four months.[00:27:00]
But again... You know, my primary surgeries that I do are, you know, shoulder, knee, and elbow. I do do Achilles, and I do the innovative technique, but four and a half months seems is just a little, it's a little bit too. But again, it's Aaron Rodgers. He loves to get people excited about things he says. He also was talking about things he does with, listens to dolphin noises to get his healing better.
So we have to talk about, there's, there's different things that, that he said that we don't know the credibility of. But listen. More power to him if he's motivated to get back, and he will get back, and like I said before at the very beginning of the conversation, I think he'll be back, but he's not coming back this year.
Will Sanchez: Anything that works, if it puts you in a great mental space for you to deal with your injury and think that you're recovering faster by listening to Dolphins, then I'm all for it, right? Whatever gets us to our happy spot. Dr. Garcia, you know, this was supposed to be a 10 minute show, and then we started yippity yapping, and I've got, you know, 85 questions, so let's wrap it [00:28:00] up.
I just want to remind everybody, please check us out at sports. talk. com. Our shows are there, transcripts are there, just cool information. Dr. Garcia has tons of stuff on the website, so please check us out. Dr. Grant Garcia, orthopedic surgeon and sports medicine specialist. If you haven't figured it out, he knows what the hell he's talking about.
Dr. Garcia. We didn't even get a chance to talk about our boy getting hurt. Our, our Saquon Barkley with that ankle sprain, which is probably going to be out three, four, maybe longer weeks. Very concerning, but Hey, this is a tough sport. Thank you for your time tonight. And let's do it again.
Dr. Grant Garcia: And again, yeah, thank you so much for having me on.
And again, hope both these athletes recover quickly. Check us out on our website. And again, also, you know, on our website, we have posts. You can post questions. We are happy to go through a show where we answer questions from our listeners. You know, again, it's, it's always nice to hear the questions from Will, but you know, the listeners as well [00:29:00] would be great.
Will Sanchez: So. Yeah. Less of me and more of you. That should be the motto. That's another t shirt. Take care, Dr. Garcia. Thank you for your time.
Dr. Grant Garcia: Thank you very much. Bye.Audio Transcript
NFL Kickoff 2023: Predictions, Injuries, Data and Tech
Will Sanchez: [00:00:00] This is the most exciting part of the year for myself. I know for Dr. Garcia, what do I smell? I smell pigskin. I know that sounds a little nasty, but it's football season 2023. We're about to kick off. I'm Will Sanchez. This is Sports. Talk. Check us out at Sports. Talk. com. You can find our shows. You can find our gmail, please send us your request for show topics, all sports, all orthopedics all the time.
Will Sanchez: And we once again have our favorite orthopedic surgeon and sports medicine specialist, Dr. Grant Garcia. Dr. Garcia, it's football season. Welcome to the show. It's so good to talk with you once again.
Dr. Grant Garcia: Yeah, it's good to be back. I've had a little summer hiatus, but I'm extremely excited. We have the first Giants game coming up, got a brand new looking team, faster [00:01:00] team and so far healthy team.
Dr. Grant Garcia: So this is really exciting. And I'm excited about the show today because it's football season and everyone loves to talk about football.
Will Sanchez: Oh, yeah, once again, man, it's football season for those fans that haven't listened to our previous shows I'm from new york now in seattle. We have dr. Garcia here in seattle We're both giants fans.
Will Sanchez: So that is the common thread. This is how we we meet and conclude in the middle of this beautiful relationship friendship partnership It's the New York Giants that have tied us all together. So that's where our allegiance lies. How excited are you for this Giants season? After a 10 8 1 season last year, Coach Brian Dable, Coach of the Year, led the Giants to the playoffs.
Will Sanchez: They demolished Minnesota and finally get knocked out by the Eagles. How excited are you for this upcoming season as a Giants fan?
Dr. Grant Garcia: I'm extremely excited. I [00:02:00] mean, we have a lot of speed. I was just reading recently. It's going to now the fat or the fastest teams as opposed to one of the slowest teams, which is just, you know, speed kills now in the NFL.
Dr. Grant Garcia: Darren Waller, what can I say? I am really excited about watching him play. I hope he stays healthy. And I think that it's going to be good for Dan Jones to no longer have the criticism of. Getting new contract, et cetera. And you can just play as hard out and feeling more comfortable with Dave Hall.
Dr. Grant Garcia: So, I mean, there's, there's a lot to look forward to. I'm only, the only thing I'm worried about is, you know, the, the giants worked best last year of being an underdog and now they're no longer a secret. So, you know, how is that going to affect them? I don't want them to turn into a cowboy, as you know, or have lots of high expectations that doesn't
Will Sanchez: perform.
Will Sanchez: Yeah. I'm not, I'm not worried about the expectations. I'm worried about the Philadelphia Eagles and the rest of the division and the NFC conference. But as we get ready to kick off the 20 23 season. It's a perfect segue to talk about the kickoff rule change on concussions, right? So there's a paper there [00:03:00] that you had sent to me.
Will Sanchez: It's the effect of the 2018 NCAA kickoff rule change on concussion rates in college football. And in fact, the investigation performed was at the University of Washington here in Seattle, Washington. Let's talk about that. When you read the paper, what was your findings and what was really interesting about this paper that you could share with the audience?
Dr. Grant Garcia: Well, I think what's interesting is, you know, again, we're shifting now to college versus NFL. But, you know, you always keep hearing, and I think people sometimes, you know, people complain about football and they're saying they change the rules to protect the players, right? Yeah. And that's always the goal.
Dr. Grant Garcia: Change the rules, protect the players. We don't want to see concussions. We don't want to see players having traumatic brain injuries or whatever else. If we talked about Dr. David Smith from the Q caller telling us it's not concussions. We're talking about looking for more traumatic injuries in terms of the definition.
Dr. Grant Garcia: But basically by changing this college rule, they try to change it. So you no longer have kickoffs. You do fair catches and touchbacks [00:04:00] and trading trading when you start on this, it's automatic, no longer kickoffs. Or a significant decrease in that. And the thought process is by having less, this high impact, because this is the most high impact of all the, of all you're doing, right?
Dr. Grant Garcia: You have full speed, almost the entire field, coming at another player from the other side. You don't, you don't get to wind up like that in the other option, other than, you know, a kickoff or a punt return or something else. So, what they found was the thought process was, is going to reduce concussions by fixing the rule.
Dr. Grant Garcia: And what's interesting is it made no difference. And the overall amount of concussions was stable. The only thing you always want to, you know, question with these papers is how are they determining that? You know, whether the test, as we know, the tests are not always great. But nonetheless, it's interesting to bring up because we always think about real changes.
Dr. Grant Garcia: We're talking about another real change or another change in the NFL. And whether that led to improvements or decreased injury rates. But, you know, we keep talking about these interventions that are going on. And we're saying, Hey, I hope this is going to make it better. I hope this is going to be better for the [00:05:00] players.
Dr. Grant Garcia: And right now we're not seeing that. So, you know, I think people are worried. Are they going to start getting rid of touchbacks or can you start getting rid of kickoffs for the NFL? And at this point it doesn't show to be a big difference. And so maybe they're going to keep it the same. But it's interesting to have that data because I think a lot of people don't understand that, don't think that.
Dr. Grant Garcia: They're thinking, okay, a lot of these real changes, clearly there's data to show it's effective. In this case it
Will Sanchez: wasn't. Yeah. It's really interesting. And, and this is a very debatable topic, right? Because there's an aspect of it that I'm not sure if the paper. concludes is the amount of kickoffs that are not being returned.
Will Sanchez: So if you had a thousand kickoffs and now because you have a touchback rule that automatically puts the ball at the 25 and they decide not to run it back. So instead of a thousand returns, you only have 700 returns and the concussion number. Are, or the percentages are still the same. Are we still getting a decrease because we have less returns?
Will Sanchez: So, [00:06:00] I think that's where it becomes an interesting conversation because the amount of plays that are being used compared to the amount of plays that are no longer being played. So, it's an interesting dynamic in how that plays a part with these conversations.
Dr. Grant Garcia: Will, are you sure you're not an MD?
Dr. Grant Garcia: You have so much knowledge of these papers, I love it.
Dr. Grant Garcia: So funny. Anyhow, well, this is a great, it's great to know, you know, we talk about sports all the time, but we never talk about data. So it's just interesting to show this, you know, I don't want to bog the audience down with the data, but you know, the fact that people know, like, this is where NFL and, you know, us as team positions, we see this stuff, you know, this is important to us.
Dr. Grant Garcia: Right. When you're coming up with plays or working with the NFL Players Association or you're, you know, there were definitely, there were definitely neurologists and neurosurgeons and stuff probably involved in the rule change. And so they want to show, is this worth it? Right. Cause it's changing things.
Dr. Grant Garcia: I mean, the excitement decreases when you have touchbacks, right? Is there going to be a run back today? Is there going to be a [00:07:00] touchdown, you know? And so is it worth it? And maybe it's not, who knows? We still have more things to do, but your percentage information. The top, the, what you brought up is really, really an important point.
Dr. Grant Garcia: And again, it's always good to kind of criticize the paper and look at it in detail. Yeah. But I thought the audience would like to at least know that, so.
Will Sanchez: Yeah, it's, it's really interesting and it's concerning also because the numbers can be swayed different ways, right? And then do we take into consideration And we've discussed this, right?
Will Sanchez: We, we talk about the, you know, and, and the most lovingly way that we can say it, the freak athlete, right? And we'll probably touch upon some of these incredible athletes, these specimens throughout this show, especially when it comes to recovery. But then we talk about the size and the speed. I remember the joke was, well, you know, the smaller guy was the fast guy.
Will Sanchez: The bigger guy was just the bulkier guy. But now you've got guys that are 230, 240 pounds running a four or five. And you put them on a kickoff line and they're running down flying at you, you know, [00:08:00] those are also considerations thinking about how big these players are getting as the faster that they get.
Will Sanchez: And these fields are still staying the same, right? You know, CFL, right? The field's a little bit bigger, it's a little bit different. So there's so much that goes into it. And like I said, we can go on and on with this. So, you know, for For the purpose of the show, we'll kind of move on, but this is really just kind of tidbits and things for people to think about, you know, when we start to see some of these datas.
Will Sanchez: Totally agree. You know we talk about concussions, right? And this is the way we kind of kicked off this show with the kickoff rule and the change on concussion rates for, for college football. But one of the players that was most recognizable for concussions, and there were many concussions last year, but normally the quarterback gets the most attention, right?
Will Sanchez: And for Tua Tagovaiola, the Miami quarterback, I mean the spotlight couldn't have been brighter. He suffered numerous concussions last year, including one that was as [00:09:00] serious as can be when he played the Cincinnati Bengals and got flung to the ground and his head hit the ground and bounced off the ground and laid there pretty much motionless.
Will Sanchez: with his his hands in that cramped position. First off, before I move on with my question, can you once again say what was happening to that player when his extremities were tightening up that way?
Dr. Grant Garcia: Well, it was, remember, we and by the way, guys, look back on our Sports Talk podcast. We had a sort of...
Dr. Grant Garcia: Full section on that. So it'll be good if the audience is interested in refreshing the entire episode and that can be found on all of our different podcast areas. But nonetheless, it's called fencing. And it was likely from a second hit. So he had. You know, again, I don't know how the testing was done then, but there was a lot of staff changes after that, but basically not probably fully recovered from the first concussion, got the second concussion, essentially a second hit syndrome, which is not good.
Dr. Grant Garcia: And this caused a severe reaction that you see in traumatic brain injuries [00:10:00] where you can have this sort of position, it's actually kind of an innate neonatal or sort of infant response that people have. And when they fall, they kind of do this whole thing where they lift their arms up and that's exactly what he had, if I remember correctly, so not ideal.
Dr. Grant Garcia: So, I mean, it's really important with a guy like this that he's healthy, obviously with ESPN recently showing them making it potentially to the finals. Or the championships, you know, it's important that we have him at top condition, so.
Will Sanchez: Yeah, and it's going to as you said, be impactful for the team, for the league, because I think as a fan, I'm pretty sure as an owner, as a coach, as a player, and, you know, the league itself, they have to be really concerned that Tua doesn't get, You know, hit and have something like that happen to him again, because not only, most importantly, it can be so detrimental to the player and what his long term outcome is, people are already scared [00:11:00] about what happens in the NFL and what, you know, what can possibly happen.
Will Sanchez: It is something that I'm pretty sure the league have already discussed with the Miami Dolphins. I am... just guessing here, but I'm pretty sure that that was the case that they would have reached out and said something. So there's a lot of concern. And one of the things that they said he's doing is Brazilian jujitsu training to learn how to fall.
Will Sanchez: I'm not sure how that helps when a 300 pound man is flinging you, but you know, we'll, we'll see how that all works out. But you know, you mentioned at the top of the show, Dr. David Smith and his biomedical engineering and develop developing design the Q collar which is supposed to mitigate the absorption of slosh or sloshing energy by the soft tissue of the brain.
Will Sanchez: And he described so eloquently. the the inspiration of looking at a woodpecker and how the tongue wraps around the cranium and protects the brain and that's where kind of that thought process, the beginning of that thought [00:12:00] process was for the Q collar. Why aren't players, and I know, you know, there's still discussions about the Q collar even though it's already FDA approved, why are players maybe hesitant to use something like the Q collar, or is it, is it something just uncomfortableness, or just lack of information, or just going based on what maybe medical doctors are telling them?
Dr. Grant Garcia: So, I, I think you know, it's always hard to see with new tech for lots of people. Yeah. I think it's interesting the way, the point you brought up, so, Yeah, it's probably the device of medical physicians who say, Hey, I don't read the data on this. I've never heard of something that can prevent it because we know about how this works.
Dr. Grant Garcia: There was just a post about a helmet that reduces concussion rate by 25 percent in the NFL. And there are a number of comments, even on LinkedIn, people saying that's not true. You know, the helmets have not shown that just like Dr. David Smith said. And so, you know, you've got to be careful that people are always judging, like, how good is this, right?
Dr. Grant Garcia: Because this is a very, if you find the [00:13:00] holy grail to reduce concussions, I mean, that's, you're not working ever again. Yeah. You know what I mean? Yeah. So, you know, we've got to be careful with the right thing. If I was finding this, like, huge... Area that we're looking for this huge need. And so him being hesitant to use it, it makes perfect sense.
Dr. Grant Garcia: It also seems almost too simple to work, but we've heard Dr. David Smith and we've seen, you know, since we've been working with him, we've seen a lot more information from professional athletes that are using it. I would actually say the flip side that at freshman athletes tend to be more likely to use the new tech.
Dr. Grant Garcia: This situation is different. Okay, because they're always looking for get to the edge, right? Like I, I don't consider myself a professional athlete, but I try to keep myself on the edge in terms of trying new technology, innovation, etc. And I'm more willing to try some new things based off the sort of patient population I have and what I'm looking for in the Seattle area and these athletes are always looking to find an edge.
Dr. Grant Garcia: How can they? Be a little better. How can they up their game? And they're lucky enough in their situation to have unlimited funds and to have the NFL, you know, their teams back in there, I mean, you [00:14:00] see, there's all this new biotech and we can jump into one topic, you know, you want to talk about but there's always, there's always new tech.
Dr. Grant Garcia: They're always trying new things. I mean, it's interesting because most of these companies use the NFL and professional teams as a marketing tool, right? So if they get, they get into the NFL or they get into Sounders locker room, they say, Hey, listen, the Sounders use them. But it's funny because it's actually easier to get into professional teams than it is to get into like a regular doctor's office.
Dr. Grant Garcia: Because professional teams are like, Hey, we'd love to use this. This is brand new. It's not going to hurt our players. It's like a, it's a. peptide evaluator or a blood tester or a massage gun or something really kind of minute. And so they're always willing to try it because they're looking for the edge.
Dr. Grant Garcia: I mean, we're always trying to beat the next person in the NFL and it's a huge multi million, probably billion dollar industry. And so if you can find a way to give your players a day faster or 10 days faster, you know, it makes a big difference. And so you'll see like when you go in the locker rooms, they have tech all over the place and they're always trying something new.
Dr. Grant Garcia: You know, they're trying these. Yeah, we the copper or the, or the the armbands for [00:15:00] the players, you know, if they're overthrowing, you know, there's, we talked about the tech on the, these players wear all the time. So it's interesting that there is certain hesitancy with some things, but again, the other concern is constraint, right?
Dr. Grant Garcia: Like, is the cue call going to constrain him that he can't focus even though it's a very light amount of pressure? And so you don't see a lot of players with braces or other things to protect their... Our body part is easily because if it does slow them down and they lose speed, right? So you want tech, but you don't want to be lost.
Dr. Grant Garcia: You, the tech should only improve you. And if it slows you down at all, they're not going to use it. Right. Cause they don't want to get caught or they don't want to get injured or they don't want to get taken off the field. You know, the NFL is very competitive.
Will Sanchez: Yeah, that's really interesting. And for the people that are listening, there are numerous NFL players using this Q collar right now.
Will Sanchez: I know right off the top of my head starting running back for the Dallas Cowboys, Pollard, he's, he's always using the Q collar. He's using it for protection. And some of the things that Dr. Garcia just mentioned, so I just want to elaborate on that. It's, it's a pressure that's, it [00:16:00] goes on the back of the neck.
Will Sanchez: It causes a slight... increase of blood volume in the head and it helps reduce the brain's movement when there's impact. So the extra infusion of blood creates kind of, you know, using, you know, Dr. Smith's words, an airbag effect that restrains the ability to move inside the cranial fluid and that's where the thought of the woodpecker or the ram becomes that inspiration because when you You know, let's say if you were to take an x-ray, you would see this protection that's happening around their brain to reduce the movement.
Will Sanchez: And maybe if you've seen the movie concussion or something like that, you, you see, there's a part in the movie where you see that the brain is shifting back and forth and rattling inside the cranium, which is causing this concussion. I don't know if I described that as well. Dr. Garcia, please help out if I didn't do it as
Dr. Grant Garcia: well.
Dr. Grant Garcia: I told you, you need to get your M. D. You're an expert.
Will Sanchez: So... Just to give everyone an idea what [00:17:00] this sloshing of the soft tissue of the brain and what this Q collar is. So it's just, once again, we just want to bring stuff up. Also, it ties into some of our other shows. In fact, that show was on June 27th.
Will Sanchez: So, it is an incredible show with Dr. Smith talking about the Q collar and the biomedical engineering that kind of went into all of this and is part of our tech and football kickoff. So, Dr. Garcia got jokes. You know, he's taking a shot at me a little bit earlier talking about getting into this biotech and what I really want to talk about.
Will Sanchez: So just to give everyone some insight, I'm reading this article and it's on the Jacksonville Jaguars, right? So I'm like, all right, cool. And oh, they got this new biotech. And it's in the urinals and I'm like, Oh, this, I got to read this. Right. So I send a picture to Dr. Garcia and I said, Hey, they have sensors in the urinals.
Will Sanchez: And when the players use the urinals, the sensors will turn either green, yellow, or red based on the [00:18:00] player's hydration levels. And I was like, This is really cool. This is biotech. I don't know, Dr. Garcino's like, okay, we're talking about urinals. I said, I'm gonna bring it up for the show. We get this biotech.
Will Sanchez: So, listen, even though it's hysterical, but it tells, the fact that it can tell the player how, how well you're staying hydrated. There has to be some benefit to that, right?
Dr. Grant Garcia: Listen, I think that the thing is, you've seen, you know, on Instagram, they have the glucose monitors and you have It's all about knowing your body.
Dr. Grant Garcia: And we've, we've talked about this extensively on the show. And our last episode, you look back on, you know, what athletes do to get the edge or get better and the tech they're using, you know, we have smartwatches tells us when to sleep, tells us our blood pressure, tells us. EKG tells us heart rate then you have, you know, this thing tells you whether you're hydrated or not.
Dr. Grant Garcia: If you're telling your glucose levels, we just want to know everything about our bodies so we can be more in tune. You know, am I feeling crummy because I'm tired? Am I feeling crummy because my [00:19:00] blood sugar is low? Am I feeling crummy because I'm dehydrated? Is my, is my urinal hydration system showing green, yellow, or red?
Dr. Grant Garcia: You know, I think. It's important for us to understand that all this tech is important, and it's just another way for them to be aware of it, right? You know, these guys, they're super athletes. A lot of times they're not even thinking about their athleticism. They're not thinking about hydrating the body. I mean, you've seen all the movies and shows where they go out to dinner, and I've seen them back and...
Dr. Grant Garcia: You know, working in the locker rooms with these professional athletes, they have huge meals. They're not talking about very healthy food they're eating, you know, they're not really watching some of the things they're doing because they're just these super athletes constantly exercising, working out all the time.
Dr. Grant Garcia: But there are certain ones that take their, their health really seriously. And I think this is a, this is an important point that they're saying, you listen, I mean, Jacksonville is not cold right now, you know, so it's important to figure out a way to stay hydrated. It is super hot in Florida. Players.
Dr. Grant Garcia: Yeah. We've seen full players that have gotten really injured over the last bit. So while I can laugh all I want on your, at [00:20:00] your urinal center post you sent to me or you text you sent to me it is important and especially for Jacksonville. You know, I don't know if the Seattle Seahawks right now are worried about hydration, when it's like 64 degrees outside.
Dr. Grant Garcia: But in Jacksonville, I could see the reason
Will Sanchez: for it. Listen, if they they, they're one of these teams that there's a lot of expectations. They expect them to get to the playoffs and, you know, possibly win the South. And, and go kind of far away, you know, far into the playoffs. So, they want to make sure that if they have any playoff games in Jacksonville.
Will Sanchez: That everyone's nice and hydrated, so these urinal sensors, you know, they might get a Super Bowl trophy at the end. They'll put like a little star next to the urinal, so who knows where this is all gonna go. So, I think we've gone awry, but listen, we hope that you're getting some information on it because the reality is...
Will Sanchez: If you listen to our shows, Dr. Garcia is always talking about tech, right? This is, you know, he loves it. You know, lovingly I say, he's a nerd about it, right? [00:21:00] And it's great for us, the patients, because he's always staying on top of technology and innovation. And this is... Even though it's, it's a little bit of a funny topic, but it just shows that the biotech is such an important part of everything that we do, whether you're a doctor or you're a patient or you're an athlete.
Will Sanchez: So having these biotechs be a part of our lives. is so important, and to see where it may go, and I'm kind of teasing a future show as we talk about future tech, as we see where we're eventually going to go, it should be really exciting to everyone.
Dr. Grant Garcia: I couldn't agree more. I don't want to change your topic, but I definitely think you guys are going to see in the up and coming months, we've got a lot of good shows planned for you, and I think one of them will be, sort of, what are the new cutting innovations, you know.
Dr. Grant Garcia: Last year's old news. Yeah. Let's figure about the new year. What are we, what are we doing? How did we do last year? How did, how was our, how was this stuff I talked to you about from the [00:22:00] new innovative procedures or how is it new at the N F L? You know, there's been rule changes even in the N F L or things that have changed.
Dr. Grant Garcia: N F L, like how did that affect him? You know, we talked about recently on major League Baseball. Yeah. With the change in the pitch timing. You know, we don't know anything yet about how it's gonna cause injury, but I know we talked on the episode a few years ago with our old podcast. That's been molded now into this new one the game of numbers.
Dr. Grant Garcia: And I think you remember, I remember it was a while ago that we brought it up and how does the expansion of the NFL game time increase injury rates? And we said, there's, there's no way it doesn't hurt, it increased injuries. But yeah. You know, I sent you that recent paper. I don't know if you want to tell everyone about kind of what you thought.
Dr. Grant Garcia: I don't mean to segue, but it's actually super interesting topic. But I know that was a huge, that was a huge discussion in the NFL, whether we should add it, you know, we know why the NFL players, the NFL owners want to do it. There's a lot of money involved in any other game in the NFL. Right. But for the players, are they going to get injured?
Dr. Grant Garcia: Because we don't want that.
Will Sanchez: Yeah. No, it's a perfect segue [00:23:00] because that's where I was leading because the Jacksonville Jaguars are, are going to play in London twice this year. And for your Seattle Seahawks fans, by the way, you guys lead the league in total mileage for this upcoming season. And I believe you led the league last year, this upcoming season, they will travel almost 32, 000 miles over 36.
Will Sanchez: Time zones. In one NFL season, by far and away the most, San Francisco 49ers are next on that. So this segues right into this this paper that you're talking about is the Association of Injury Rates Among Players in the NFL with Playoff qualification, travel distance, the timing of the game, and the addition of another game.
Will Sanchez: So, Dr. Garcia, talk a little bit more about the findings that they had, this investigation that was performed at Northwestern University.
Dr. Grant Garcia: So, it's really interesting. So, basically, they, and [00:24:00] again, a lot of these Articles that use like NFL player data or a lot of there's a lot of Major League Baseball because there's a lot of good player data out there.
Dr. Grant Garcia: Yeah. That I've done actually my own papers on using the Major League Baseball database. So this one's really interesting. So basically it looked at five NFL seasons 2017 to 2018 and then through 2021, 2022. Yeah. And when they expanded to the from the 16 game to 17 game schedule, they looked at whether or not, There were more injuries during that time, and then they also looked at they looked at whether or not they're more likely to make the playoffs and all those other things, injury rates for based off distance and what's really interesting.
Dr. Grant Garcia: And again, this is one paper, but they're looking at a lot of accumulative data. And again, you. You can only look at so many injuries, right? You're looking at basically news, like if someone tweaks their toe and it's not listed as an injury report, you're not going to ever see that in the NFL data. So it's just something for people to understand.
Dr. Grant Garcia: What's interesting is they found no difference in the injury rate or the number of injuries by adding another game, [00:25:00] which I find kind of fascinating. And it's kind of hard to wrap my My brain around that. But it's interesting that people saying for these kind of argument for the players associate or not fair session, the owners that this new increase did not increase rates.
Dr. Grant Garcia: It gave the players potentially more options to work for something or get to the playoffs and also to showcase their talents. And hopefully there was some bump in, in income as a result of it for the players. But you know, it sounds like this was a good, this was still a good thing. It's we, everyone loves more NFL.
Dr. Grant Garcia: If I have to, you know, I'd love to see the Giants play an extra regular season game. So I'm not complaining about it. But it's important to see that. But what's interesting, this is actually super, this makes the most sense is that the play, the teams that are the least likely to qualify at the playoffs had the highest injury rate and the highest amount of players on injured reserve.
Dr. Grant Garcia: Which makes perfect sense, right? Like we didn't know when your team starts getting decimated with injuries. Your team's success drops significantly, but this actually makes this is actually documented now and this paper is helpful for that So, I don't know if you have anything else to take away from [00:26:00] that, but I thought that was really interesting I know our listeners were gonna love that because they don't have access to these papers and I'm sending you Yeah, so it's nice that we're able to get that information out to the public No
Will Sanchez: I think it was a great paper and just kind of reiterate, you know The purpose of the paper was to determine whether they're higher Cumulative travel distances or, you know, overseas played, like when I mentioned Jacksonville going up, played at London twice.
Will Sanchez: In fact, I think they're gonna stay there both weeks. I think they're gonna do back to back you know, early season, bye week. Right. And for me, as a fan, that always stood out. It's like, oh man, the, the, the bye week. This week is week four. And then they have, you know 13 more games to play without a bi-week.
Will Sanchez: So as a fan, you're concerned for your team like they getting in that bi-week early. They added an extra game. I've always thought that they should add a second bye week, but you know, this paper is now saying that it's not, you know, it's not making much of a difference, right? Because the conclusion over the five NFL seasons, with the distance, the play, the bye week timing, the added, like, was not associated with [00:27:00] increased injury rates in NFL players.
Will Sanchez: So, it'll be interesting to see, I would love to see this paper five years from now, right, and to see if that stays consistent, because there will be so many other variables, once again, like, kind of, we mentioned, right, the size, the speed, the biotech, right, you know, from 2017.
Dr. Grant Garcia: Well, and more international games.
Dr. Grant Garcia: More and more
Will Sanchez: international games, but it's, it's, it's going to happen, right? And how do they handle that? How do they talk to the doctors? Maybe, maybe that's a conversation that you can you know, help with, you know, when they talk about travel and especially as, you know, we decide to play more games overseas.
Will Sanchez: Do they talk to, do they consult with the doctors, or do they just consult with, you know, the, the banks, you know, bank stub here saying, hey, we just made extra money, when it comes to, hey, this is the best way to take care of our athletes, you know, if we're gonna go overseas, this is the way we should do [00:28:00] it, I, I know people like Richard C. Oh my God, what's this guy, anyway, the player from Thursday Night Football complained about Thursday Night Football saying, you know, about the injuries, you know, going up on Thursday Night Football, shorter weeks, you know, what, what is all of that data? So I think there's still some added data that needs to be inputted into you know, some of these papers.
Dr. Grant Garcia: And again, you know, we don't usually drop papers on our show, but these were two super interesting topics that I thought people would like to say, and this one especially when I sent it to you. And, you know, I immediately thought of making sure that the audience heard this. And again, remember, most people listening to the show, You know, not like Will Sanchez that has an MD from his podcast but the but understanding the epidemiology and understand how these papers are done.
Dr. Grant Garcia: You got to take it as a grain of salt, right? Like this is important. This information is interesting. It's a topic. And if anything, it's great for your, it's great. It's great for parties, party conversation. You know, I mean, people talk about the NFL all the time and be like, Hey, that's your game. Do that cause more injuries? [00:29:00]
Dr. Grant Garcia: Well, no, I heard about this, this situation where it didn't but what's, I think more important about it is it just gives some more food for thought and saying, okay, maybe our, maybe our indications or maybe our concerns about this were not perfect or not correct and, and, or how can we make this topic better or more intro, how can we look more into this and find ways to really think about this better because it doesn't really make sense, right?
Dr. Grant Garcia: Shouldn't there be more injuries? So maybe there's something we're missing. Okay. Yeah, I
Will Sanchez: agree. And if that 100%, which you should always do, right? And by the way, that was Richard Sherman that was drawn a blank on, I was like, I can see his face, and I can't say his name, and I was thinking about it, I was like, oh, it's Richard Sherman.
Will Sanchez: Because obviously he's talked about it, and it's funny, he complained about Thursday Night Football, but now he works for Thursday Night Football. But I digress, let's kind of move on. Let's talk about some key injuries for some players, let's make some predictions sure to go wrong. As we get ready to wrap up our 2023 NFL kickoff season if you're a Cincinnati Bengals fan, you know, one of the most exciting quarterbacks in the league, you know, [00:30:00] arguably the tops, you know, top two, top three quarterbacks, you know, in NFL, Joe Burrow has his calf injury.
Will Sanchez: Obviously the show is before week one. Commences this weekend what are your concerns for an injury, that calf injury for Joe Burrow? Do you have any concerns? Has there been enough time or are there any concerns starting week one and hopefully playing the entire season? So that's 18 weeks of football after this injury.
Dr. Grant Garcia: I think you've heard this before, but this is one of my least favorite injuries to deal with. You know, these are so nagging. I think Aaron Rodgers had this a while ago. There's been a couple other players with this. But these calf injuries, they come with two muscles, the soleus and the gastrocs muscles.
Dr. Grant Garcia: And when you get these tears, usually it's a tear of the muscle, not an Achilles tear. That's a different animal. And I know you you know, we've heard of players that had the calf injuries and then got Achilles injuries. I don't think that's what he's going to turn into. But they can nag. And then you come back and I've had plenty of, [00:31:00] you know, athletes, non athletes come back with these and you know, they're better for six weeks and all of a sudden they re injured again.
Dr. Grant Garcia: Now you can sure as heck know he's done everything possible to get ready for week one and he's, you know, he's doing PRP, he's doing other stem cell options, he's probably doing anything else and things I haven't even heard about yet to get him back because he's very important for the team. But watch out, you know, I do worry, is he going to get it re injured?
Dr. Grant Garcia: And so, you know, that's just, it's just a stressful injury to deal with because it's just so you really can't fix it, right? You just got to let it time be and you got to give it treatment. And so that's hard, especially when you're a big surgeon and you're trying to get an athlete back faster.
Will Sanchez: Is there any benefit for them saying, you know what, the first two weeks, three weeks, four weeks of the NFL season, we're just going to rest you, or is this just too hard to answer because you really don't know the severity of that calf injury for Joe Burrow?
Dr. Grant Garcia: You know what, say that to, say that to the Mahomes and the Kansas City Chiefs. Now again, it was a Super Bowl. Yeah. But you know, this is the NFL, you know, you had, you had all this time to, [00:32:00] to rest up And you lose two or three games at the beginning and you're iced, you know, it's really hard to come back.
Dr. Grant Garcia: We've seen the statistics. If you're 0 3, your playoff chances drop significantly. Especially
Will Sanchez: in the AFC this year. Correct, yes. Yeah, yeah, absolutely right. And then hopefully hopefully Joe Burrow will stay healthy. Hopefully you know, maybe he's not taking off running, you know, as he's done before and kind of says, hey, you know, I can only push it, which I doubt because when you get out there, you're such a competitor, you're still going to do it.
Will Sanchez: And then the last thing that we want to see... is kind of, and you kind of alluded to it, was kind of like the Kevin Durant injury where he had a calf injury and then obviously in the playoffs you know, we saw that pop and that was the Achilles. Well, on that happy note, we'll move on because there's just no way to do it and as a football fan you just kind of want to see everybody out there.
Will Sanchez: He's one of those more, you know, exciting players that you love to see play week in and week out. So hopefully... That calf injury has healed up nicely. [00:33:00] Staying in the leg, Cooper Cupp, wide receiver for the Rams, has had a nagging hamstring injury. Apparently he flew to Minnesota to talk to a specialist.
Will Sanchez: Who knows? Do you know that specialist in Minnesota? What are the concerns when you have a wide receiver, like Cooper Cupp, that's had some injuries in the past? And at a speed position, when you're having a hamstring injury, what are the, I guess, the varieties of injuries that are most concerning, or least concerning to most concerning?
Will Sanchez: Well,
Dr. Grant Garcia: you touched on my two least favorite injuries now. I'm on number two. So these hamstring muscle injuries are a pain in the butt. I mean, you've seen them. I think when Oda Beckham Jr. first started with the Giants, he had this injury, and it was just waiting for him to give his debut. And these are, again, The calf injury is a muscle injury.
Dr. Grant Garcia: This is a muscle injury usually. And what it is, is you get a little muscle tear. You want it to heal as quickly as possible, it doesn't heal as fast as you want, then you re injure it. So, he's probably going to a specialist, [00:34:00] I don't know who he's going to over there in Minnesota. But nonetheless, probably going to one of the Vikings team physicians up there, those guys are really good.
Dr. Grant Garcia: But regardless, the, you know, he's probably considering treatment options, maybe even considering surgery. But probably not, you know, I would imagine you wouldn't want to do it, but he's also probably getting different opinions to see whether fixing this is going to get him back if they don't think he can get back on his own.
Dr. Grant Garcia: So I'm sure he's talking to a bunch of people. When you're flying out to see a specialist there is definitely a thought of surgery on the plate, in my
Will Sanchez: opinion. So that's the red flag. When you see, hey, he flew out to see a specialist, that's one of the things that cross your mind saying, okay, this is maybe a little bit more severe there than, you know, just a slight pull and there might be surgery, you know, that's on the board because of the severity of this injury.
Dr. Grant Garcia: And also, I mean, again, the NFL players. Are different, you know, usually a normal person wouldn't go fly out if it was a non operative treatment. Like, if they're like, oh, I want to, I just, I might tell you this can be treated with three weeks or four weeks of rest. Yeah. Most people aren't going to fly and see another person. [00:35:00]
Dr. Grant Garcia: to double check on that outcome, right? If I tell you, you need a massive big surgery, or you need a surgery that's going to cut away half your season or your entire season, you might be like, whoa, I want to get another check. You see that all the time. So, you know, to me, that's a red flag for how bad this is.
Dr. Grant Garcia: But again, I'm not in the, I'm not in the clubhouse. I don't know what's going on so I can't actually see the injury itself, but I get a little bit worried when I hear that.
Will Sanchez: Yeah, by the way, he's already been ruled out for week one. They, you know, they had it on the table. There you go. He may or may not play, but he's, he's been ruled out already.
Will Sanchez: So we'll see how that kind of goes. And then You know, we talk about these, and this is kind of why I'm using these guys right here which I think would have been the offensive rookie of the year Brees Hall tore his ACL meniscus in week seven. One of our favorites Sterling Shepard had a very, You know, bad injury himself when we hear about a c l and meniscus and the type of injuries that [00:36:00] both these players have had and the fact that they are ready to go week one of 2023 season, first off, the type of injury and also the recovery in the work that has to go into it and for, in order for you to get ready to, to be able to play at this high level for week one.
Dr. Grant Garcia: So first off, I think the hard part of this is that. It's not that it's impressive that they're getting back, but it's what it shows. And you know, as a, as a surgeon, and I do a lot of ACL injuries, you know, players, my, my patients, athletes, et cetera, that aren't professional athletes come in and they see this and they say, Hey, why can't I get back in seven months?
Dr. Grant Garcia: Why can't I get back in eight months? You know, every, these players are doing it. I should be able to do it too. Well, the average return to playing is between nine to 10 months and maybe even longer than that. If you look at the data. That's in general in all commerce. Now, again, these aren't professional athletes.
Dr. Grant Garcia: But I think you get this sort of warped perception of what normal return is. We always talk about the Adrian Peterson ACL, where he came back [00:37:00] stronger, had an amazing year, ran for over 2, 000 yards, if I remember correctly. Yeah, he's not human. Everyone talks about that. He's not human. No, he's not human. I totally get it.
Dr. Grant Garcia: We've talked about that before as well, but nonetheless, you know, it's a lot of work. They're doing, like I said before, they're using tons of biotech. They're using rehab tricks that we haven't even heard of. They're flying around to get treatments. They're working six days a week, things that we can't do with normal jobs.
Dr. Grant Garcia: I mean, their job is to get better and play football. And so they have to do that all the time. They're putting in five hours. I mean, you hear their, you hear their workout regimens, like five hours of exercise a day. I mean, well, we wouldn't be sleeping if we had five hours, five hours of exercise a day with our jobs.
Dr. Grant Garcia: So, you know, at this point they can get, they can do things we can't do in our normal life. So that's why they're able to get back a lot of times. And they're also, they're still fairly young. I mean, these players are still young. They consider them old at 31 years old. You know, so it's, it's, they have young bodies and they're adapted to this.
Dr. Grant Garcia: And also. These players play through different things. I mean, we have patients that recover [00:38:00] from ACLs. They say their knee feels some stiffness at six months, or they have a little bit of discomfort. You know, these guys are feeling the same thing, but they don't. They don't really care, right? These are players.
Dr. Grant Garcia: They're used to getting hit, they're used to getting damaged, they're used to getting beaten up. You know, they play with pain. We could talk about that topic as a whole other section. But, you know, I could tell you if you asked 90% of the NFL players on the field if they have any pain, most of them would say yes.
Dr. Grant Garcia: Yeah.
Will Sanchez: Yeah, you know, it's funny, you know, now, now that we know some some more information and some of the technology, and we think about Adrian Peterson and how fast he came back from his injury, and he didn't even use an internal brace. I mean, come on now. I mean, that's, that's absolutely ridiculous. By the way, check out our show on Internal Brace.
Will Sanchez: It's a great show. I think, I think we mentioned it every show because it's my favorite. I'm going to perform it. I'm not sure. I'm going to walk in. I got to steal some credentials and I'm going to work on, or maybe I shouldn't shout myself out like that. We'll just move on. Let's wrap up the show. Let's wrap up this show here and let's let's get some predictions sure to go [00:39:00] wrong.
Will Sanchez: Who, who are you liking to come out of the AFC to be the representative in the Super Bowl for this 2023 into the 24 season?
Dr. Grant Garcia: I'm thinking, I don't know. It's hard to, it's hard to decide. I think the Chiefs, man, I'm still
Will Sanchez: thinking. You think the Chiefs are still the team to beat?
Dr. Grant Garcia: They're just, they're, they just always surprise me.
Dr. Grant Garcia: And they still got Patrick Mahomes. Yeah. And that's the big thing. So I, I'm, I think that there, I think there's still, there's still the team to beat.
Will Sanchez: I like it. I'm gonna go with a wild card just to be different. I was thinking Jacksonville. I'm gonna go with the Ravens. Lamar Jackson, if he could stay healthy.
Will Sanchez: You know, they have a new offensive coordinator. It's something different. And if that happens, that means that, you know, Joe Burrow didn't get through the season unscathed because that's the same division of the Bengals. So, you know, I hope I'm not putting the [00:40:00] kibosh on Joe Burrow. All right, the NFC, who do you like to be the representative in the NFC?
Will Sanchez: There's you know, there's some interesting teams there. I don't
Dr. Grant Garcia: know. I mean, I think the Eagles are still so strong. But I mean, it's not a very strong. Division right now with a lot of the teams. I don't think the giants are going to be close. No, I think giants can be close behind. I mean, if they don't get injured, if Darren Waller stays healthy, the giants have a close back.
Will Sanchez: Yeah, it'll be interesting. I think the Eagles are just head and shoulders above everyone else. But to be different I'm sorry Seahawks fans. I, I will, I'm going to go with the 49ers to represent. I think the 49ers could get the Eagles with a healthy quarterback. They just gave Nick Bosa about a billion dollars.
Will Sanchez: With his new five year contract I'm pretty sure they're gonna be like, hey, you know, remember last year when you whooped on us [00:41:00] and we had no quarterback playing? Revenge is sweet. So I would love that. That would be ideal. I would love to see that matchup to send one of those teams into the Super Bowl.
Will Sanchez: So that would be fantastic. So, ladies and gentlemen, these are our predictions, surely to go wrong. Let's wrap it up as we always do. I like to bust your chops. So we're going to have a little trivia. We're going to send it right down your lane as a Giants fan. By the way, the Giants were they've been around since 1925.
Will Sanchez: So in two seasons, it would be a hundred years. They're one of the first of one of five teams when they first started the NFL. And I don't even think it was called the NFL at the time, but then when they started the football league. So Saquon Barkley is fifth on the rushing list with 4, 249 yards. If he stays healthy and gets another thousand yards, he's gonna pass Joe Morris and be in that third spot.
Will Sanchez: Can you name the running [00:42:00] back that has the franchise's rushing record?
Will Sanchez: Is it Tiki Barber? Tiki Barber has 10, 449 yards and maybe one day will be in the Hall of Fame. That is the correct answer. Tiki Barber. I never get those. This is awesome. Number 21 in your program, ladies and gentlemen. This has been great. It's a great show. This is always a lot of fun. It's always good to talk some sports and talk a little tech and talk urinal sensors.
Will Sanchez: So, that really made my day. So, just want to remind everybody, check us out, sportsdoctalk. com. We're talking sports, we're talking orthopedics, and we're talking all the time, obviously, because I'm still rambling on. I'm Will Sanchez, Dr. Grant Garcia. Dr. Garcia, thank you so much for your time. Any last thoughts as we wrap up the show?
Dr. Grant Garcia: Well, first off, thanks again for this show is always fun and I'm [00:43:00] glad that we talked about all those various topics and I think the listeners will enjoy it. And we want to mix it up a little bit. We've had a lot of guests on recently and we're gonna have some guests in the future. I think we're going to start hitting on maybe some of these non surgical options like rehab.
Dr. Grant Garcia: We have some great rehab facilities that we work with and I'm sure you'll love to hear about their cutting edge technology they're using. And then we're going to have a great episode coming up, which I'm really excited about. And so stay tuned for it in the next few months. It's going to be sort of.
Dr. Grant Garcia: Things we predicted in terms of new surgery that we were doing, and how we're being, how we're pushing the envelope even more, and how our previous sort of new tech that's now old tech is doing. And so it'll be really interesting to talk about some things and If Will's lucky, I'll even add some more internal brace stuff for
Will Sanchez: him.
Will Sanchez: Oh, baby. Woo! Sweet music to my ears. Don't tease me like that. I'm getting excited. It's just kickoff time. Dr. Garcia, thank you so much for your time. You have a great evening. I'd like to thank everyone out there, the listeners. We love you guys. Please check out our website. Feel free to email us. We'd love to hear some of the [00:44:00] topics that you want to get some more information or just hear us ramble them on.
Will Sanchez: So, but listen, we cannot do a whole show on urinals, so please stay away from that. Once again, thank you very much. Thank you, Dr. Garcia.
Dr. Grant Garcia: Have a good night, guys. Thank you all.Audio Transcript
Dr. Wayne Weil: Hand and Elbow Surgeon

Will Sanchez: [00:00:00] Welcome everyone, and thanks for listening to Sports Doc Talk. Be sure to check us out at SportsDocTalk.com. All sports, all orthopedics. All the time. I'm Will Sanchez and we are really excited about today's guest, Dr. Wayne w, board certified orthopedic surgeon with subspecialty and training hand and elbow surgery.
Will Sanchez: He's recognized as Seattle's Top Doctors and one of the our own Seattle's top doctors. Dr. Grant Garcia is with us. Dr. Garcia. Welcome. How excited are you about our guest today?
Dr. Grant Garcia: I'm very excited. I was excited to invite him. You know, Dr. Uh, Weill is a fantastic hand surgeon, does lots of sports, uh, hand surgeries, and it's as one of my partners, I get to see him do them every day and be impressed by the technology that he is using.
Dr. Grant Garcia: Uh, you know, he takes, helps me with Mercer Island, uh, teams that we take care of and does all the hand stuff for us. Uh, you know, he's a [00:01:00] fantastic, uh, partner and friend. Uh, in addition, you know, you may have seen our segments recently on the dual surgeon approach, and we just posted another one, episode five of 10.
Dr. Grant Garcia: Uh, and so for these really complex elbow cases I tell you about, he's really the my go-to and it's been really helpful for that. So I'm really excited to have him on the show. Hopefully we can pick his brain and, uh, hear more about sort of the cutting edge tools. And really it's nice to have one of the top, uh, hand and, uh, elbow surgeons in the, uh, Washington state with me.
Dr. Grant Garcia: So it's really excellent. So thank you Dr. Wel for being on here.
Dr. Wayne Weil: Uh, pleasure to be here with you guys today. Really excited. So I
Dr. Grant Garcia: think, you know, we can go in all, we can go so many different topics today, but the one we always hear about, and I know you, we see it pretty much always in the news or ESPN, is the sort of gamekeeper skier thumb.
Dr. Grant Garcia: Will you tell us a little bit about this, sort of, the treatments you're doing for it and maybe some athletes you can think of, you know, off the top of your head that, uh, have been treated
Dr. Wayne Weil: with this? Yeah, uh, I think that's a great place to start. Uh, Gamekeeper's [00:02:00] thumb or skier's thumb, it's a super common injury, uh, at the, um, thumb metacarpal phlange joint, which is kind of that big knuckle on your thumb.
Dr. Wayne Weil: And, uh, basically, uh, you can think of that, uh, ligament as the a c l. You know, you have all heard about the a c l on the knee. Uh, this is the. Uh, basically the ACL of the thumb and, and, uh, so it's a common injury in ball sports, uh, or in any sport, uh, where the, uh, hand is outstretched a and people are falling.
Dr. Wayne Weil: So, mountain biking, skiing, skateboarding, um, and again, uh, ball sports, uh, especially basketball. And, uh, then, uh, baseball as well. So, And basically what happens is, um, let's say in baseball, um, couple of, uh, this is probably now [00:03:00] five or six years ago, Bryce Harper sliding into third base, uh, and, uh, his thumb got caught on the base and, uh, wrenched his thumb back and, and tore the ulnar collateral ligament.
Dr. Wayne Weil: Uh, Basically what happens with that is you lose the stability in the thumb for power, pitch and grip. And obviously, uh, somebody who's, uh, holding a baseball bat, uh, uh, needs that power pitch and grip. Or, uh, somebody who's, uh, riding a mountain bike or holding a ski pole. Or even our, our weekend warriors who are, uh, just, uh, you know, trying to hold a golf club or, or, or somebody in the kitchen trying to open up the pickle jar if, uh, if you've torn your ulnar collateral ligament.
Dr. Wayne Weil: Really affects your, your power pinch and your grip. Uh, and so in athletes, uh, this, uh, typically, uh, was a, uh, fairly [00:04:00] debilitating injury in that, uh, it would, uh, oftentimes be a season ending injury. Uh, Um, because after, uh, a repair of the owner collateral ligament, typically I, uh, we'd need to put you in a cast for six to eight weeks.
Dr. Wayne Weil: Then there'd be a long rehab time afterwards. And so the full recovery was roughly six months, which was, was basically a season ending injury. And over the last, uh, really about the last five, six years. Uh, hand certains, uh, we've borrowed a bit from the foot and ankle docs and, and from the knee docs. And, and I've started, uh, using a technique called an internal brace.
Dr. Wayne Weil: Uh, and with that internal brace, we can, uh, augment our ligament repairs and then, uh, instead of a six month recovery, We can get folks, [00:05:00] uh, especially pro athletes, uh, back to sport in about six weeks. Wow. Uh, and it's, it's been really gratifying to, to treat our athletes, uh, and even our weekend warriors, uh, with this technique cuz we can get people back to doing the things they love doing in, in, in such a, a faster fashion.
Dr. Grant Garcia: That's awesome. Well, thank you for that update. I know that Will is very excited. This is probably the internal brace is probably his favorite topic ever. So we've gone through the round of internal braces all over the body and now you know we have another reason for Will to get excited. You can do internal braces.
Dr. Grant Garcia: The thumb. Oh, I love it. On the ucl. I, I love it.
Will Sanchez: Yeah, I think it's absolutely incredible the, the internal brace and, and hearing about the recovery from, athletes and just everyone in general. Just, uh, just a quick follow up. You mentioned golf. Um, you know, we think about the, the golf grip. How many injuries do you see from golfers?
Will Sanchez: You know, I, I'm not a great golfer, so [00:06:00] sometimes I take a swing and I'm slamming right into the grass, and all of a sudden I'm, I'm feeling that reverberation kind of shooting through my hand and my wrist. So what kind of injuries are you seeing when it comes to, golfers? Because believe it or not, one is seven Americans play golf, in 2022.
Will Sanchez: And a follow up to that is, Is there a grip that may prevent less injuries? , open or closed grip?
Dr. Wayne Weil: Yeah, that's a great question. Uh, you know, in terms of the actual grip itself, uh, not really aware of any one, uh, being better than the other. I think really it's all about, you know, uh, the mechanics of the ball striking and really I think a lot of the injuries are, are coming from.
Dr. Wayne Weil: Essentially what, what you described earlier is, is, is sort of those swings that, uh, uh, don't end up being as sweet as, uh, we'd like 'em to be. And, uh, you know, you take a shot really fat and you [00:07:00] hit the ground really hard and that can cause a, a number of different, uh, injuries. Um, you know, number one, uh, wrist injuries, uh, there's a area of the wrist.
Dr. Wayne Weil: Kinda, uh, but on the pinky side of the wrist, uh, called the t f ccc, it's one of the ligaments of the wrist that helps stabilize the, what we call the ulnar side of the wrist. Mm-hmm. Or the pinky side. And, and that acts, uh, kind of like a meniscus in a knee. It's a bit of a shock absorber. And, and that can be, uh, torn, uh, with a pretty violent, uh, impact into the ground.
Dr. Wayne Weil: Uh, other things that, uh, can happen is, uh, you can, uh, have, uh, it's a rare fracture, but it's a, uh, somewhat common fracture in golfers and actually baseball players as well. It's called a handmaid fracture, a hook of the handmaid. Um, and then, uh, other [00:08:00] injuries. Uh, Or, uh, can be a lot more of a chronic nature.
Dr. Wayne Weil: People can develop a golfer elbow, which is, uh, similar to tennis elbow, but golfer's elbow happens on the inside of your elbow as opposed to the outside of your elbow. I think will
Dr. Grant Garcia: you, you got a perfect segue for your Mike Trout
Dr. Wayne Weil: question. Well, I, Will Sanchez: yeah, I didn't want to jump in here, but I mean, you, you mentioned the Hammed bone and um Yeah.
Will Sanchez: You know, for all you baseball fans out there, uh, the loss of superstar Mike Trout, he suffered that fractured, um, and. I mean, correct me if I'm wrong, first off, if you could describe the Hammed bone injury. Uh, they're saying that he's gonna be out four to eight weeks. He has a cast from his hand up to his elbow.
Will Sanchez: So that seems like a pretty serious injury. But is that injury common or uncommon? And then following up, what does that mean? The fact that his hand all the way up to his elbow is ha is donning the cast.
Dr. Wayne Weil: Yeah. [00:09:00] So, you know, it is one of those injuries that, that, that I like to call uncommon, but common for me, uh, as a hands, um, and in, in the general population, fairly rare, um, in, in my practice, you know, seeing a lot of baseball players, a lot of golfers, Um, I see it fairly often.
Dr. Wayne Weil: It's often, uh, misdiagnosed and, and, and missed in general. But, uh, essentially the hammock bone, if, if you're looking at your hand a and you push on the, uh, pinky side of the heel of your hand, you can feel a little tiny protuberances in there. Mm-hmm. And, and. That is what we call the hook and the handmaid.
Dr. Wayne Weil: And, and the hook and the handmaid is important in that it acts as almost like a pulley or a lever so that [00:10:00] your, uh, flexor tendons to the ring and the small fingers, which are, will give you your, your power grip strength. They, they key right off of the hook of the handmaid and so. If you have a fracture, uh, off of the hook of the handmade, those jagged edges of bone can, um, cause the tendons to tear as the tendons ride o back and forth over that, uh, fractured area.
Dr. Wayne Weil: And the other big problem with the hook of the hand. It has a pretty poor blood supply, so it's a tricky, uh, bone to, to, to get, to heal. And so the reason Mike Trout is now in a giant cast for this tiny little bone, which is less smaller than the size of a peanut, it that the, the goal is to just completely immobilize everything in the.
Dr. Wayne Weil: Uh, hand [00:11:00] and the way to do that is with this giant cast that goes above his elbow. Cause you need the cast to go above the elbow to prevent rotation of the wrist. So, um, moving your palm from the palm up to the palm down position. As well as just the, the flexion and extension of the wrist. Um, and there, you know, they're, the doctors treating him are, are really trying to keep him outta the operating room cuz the next step if the bone doesn't heal, is an operation.
Dr. Wayne Weil: Hmm. Alright. So,
Dr. Grant Garcia: Talking about more of the sort of hand bones, et cetera, but also kind of moving on different topic. I've seen some sort of crazy stuff you're doing now with, uh, you know, as we, as we know, as we get older or people do a lot of pinch grip, you get a lot of, you get some arthritis in sort of the base of your thumb.
Dr. Grant Garcia: We call it cmc. Yeah. And you're doing some things now. You know, we used to see, remove it, put extensor [00:12:00] tendons. In there. And I think you probably still do that, but there's some other ways you're trying to, you basically are doing the similar stuff that I'm doing in the knee, sort of cartilage restoration, uh, and other options for people that are younger.
Dr. Grant Garcia: Cuz those procedures aren't really as good if the other older procedures aren't really as good for young patients. So what are you doing that sort of more innovative in that area? And are you doing arthroscopy? Are you any other implants you're using?
Dr. Wayne Weil: Tell us about that. Yeah, that's a great question. You.
Dr. Wayne Weil: Uh, it is a, it is a big interest of mine in, in terms of, um, solving this problem of a base of the thumb joint arthritis. And, and traditionally the, the operation of, of choice, uh, was to remove the arthritic bone called the trapezium, and then, Uh, put in a spacer, uh, typically a portion of, uh, one of the forearm flexor tendons or, or one of the thumb extensor, uh, tendons.
Dr. Wayne Weil: Um, and, and this operation works [00:13:00] really well if you're 70 years old. Um, but in somebody who's maybe in their mid forties or fifties who has kind of early onset of this problem, Um, it's been a big, uh, uh, problem for us to solve in terms of, well, what do we do for these folks? And like I mentioned with kind of with the internal brace that we sort of stole the, the idea from the foot and ankle docs, um, for basally thumb arthritis, we're, we're, we're sort of borrowing from our, our, our knee colleagues in terms of, um, Uh, techniques like arthroscopy.
Dr. Wayne Weil: Uh, so now we can do, uh, now that the cameras and the, the instruments from the knees have been miniaturized, uh, we can now, uh, work in the smaller joints and the wrist and the hand, and, and so arthroscopic surgery, the base of the thumb is something that I enjoy doing and [00:14:00] oftentimes in, in young folks.
Dr. Wayne Weil: This is my, my first, uh, step in terms of treating this issue. Uh, we can, uh, debride, um, different cartilage lesions, um, and we can, uh, debride any inflammatory tissue that's in the joint and hopefully by, uh, folks, uh, uh, uh, significant amount of time before having to do any major operations. Um, and then kind of next up the line, uh, from our surgery is, is, um, surgery to try and.
Dr. Wayne Weil: Um, basically put a, a spacer in between the two, uh, bones, the trapezium and the thumb metacarpal. Uh, and by doing that, oftentimes, um, we can preserve the, the normal anatomy. Um, you know, there's a reason why that trapezium and, and that thumb metacarpal are there to [00:15:00] begin with. And, and so, uh, trying to keep them there for as long as possible just makes intuitive sense to me.
Dr. Wayne Weil: And so, um, we have different implants that we're now using, uh, that work as spacers. Uh, and then, um, Once we go beyond that, uh, there, there's also a lot of interest in, uh, um, a technique that we're using called the tightrope technique. Uh, where, um, instead of having to sacrifice, uh, some of the tendons of the forearm to recreate some ligaments that are required for thumb stability, uh, we'll use a, a tightrope uh, implant.
Dr. Wayne Weil: Uh, and again, that that's something that's been miniaturized and, and kind of stolen from our, our foot and ankle colleagues. So there's a lot of new, um, uh, surgical procedures that, that we're performing now that, uh, I think really [00:16:00] will, will, um, be incredibly beneficial to, to my younger patients, um, where we don't see that the traditional.
Dr. Wayne Weil: Surgery that we do for a 70 year old is, is gonna hold up in a, in an active 40 or 50 year old. I
Dr. Grant Garcia: think that's a great comment. I think it's important for listeners to hear this cuz I think, as Dr. Wild knows, I do a lot of knee stuff and I get a lot of patients even in their fifties that come in and they were only told the only options are replacement.
Dr. Grant Garcia: Right? Or the only option is this sort of extensor tendon, salami technique that's really for 70 year olds, right? And so it's important for the patients to know that there's other options out there and these are innovative. They're still cutting edge. They're, you know, we don't have 20 years of data on them, but they work really well.
Dr. Grant Garcia: You know, things I do did a couple surgeries today that they're only about a couple years old, but nonetheless, they work very well. And so it's important to understand that those techniques are offered and the second opinion's very important. [00:17:00] So if you've seen somebody and you're not exactly sure, you know, get another opinion.
Dr. Grant Garcia: Always good to get another opinion, especially when you're younger and you don't wanna have an end stage procedure. You know, once you get that trapezium removed, there's no going back. Right. Yeah. So it's
Dr. Wayne Weil: important to have those options and, and, and that's one of the things that I, I think is, is really important in our younger patients is, is trying to find solutions that fit.
Dr. Wayne Weil: Younger active patients. You know, an operation that's really good for a 70 or 80 year old is not necessarily good for a 30 year old. And, and really what we're trying to do here is, is tailor our treatment, uh, to, to the individual patient. And again, a 30 year old is not an 80 year old, and so we gotta have.
Dr. Wayne Weil: Uh, techniques that we can, uh, use for our, our young active patients. That's awesome.
Dr. Grant Garcia: Well, I [00:18:00] know we, uh, for, for a hand surgeon you see a lot of hand fractures. So are there any sort of and wrist fractures. So are there any sort of innovations that have come up for you
Dr. Wayne Weil: and, uh, there are ways
Dr. Grant Garcia: to make your patients do better?
Dr. Grant Garcia: You know, the old school way is you. Break something in the wrist or you break something in the hand, you're immobilize for a long time, you're stiff and you know, you complain for six months that you're getting over it. Uh, and I know there's newer things out there that you're doing. You know, your patients are not, I don't see hundreds of cast in the office when we're in clinic together.
Dr. Grant Garcia: So you're doing something different. So tell us what you're doing and, uh, tell the
Dr. Wayne Weil: audience a little bit more about that. Yeah. You know, that's also, uh, I think we're in a really exciting age in orthopedics in general, uh, over the last, uh, 20 years. Um, there's just been a huge wholesale change in how, how we think about things in general in orthopedics.
Dr. Wayne Weil: Um, and I'm lucky enough to have gained, uh, [00:19:00] in the early, um, Early two thousands. I finished med school in 99, and so I've been kind of witness to this whole transformation in orthopedics. Uh, you know, when I was a resident, uh, uh, a hip replacement, uh, patient stayed in the hospital for four or five days and now they go home after an hour and a half in the surgery center and, and similar in, in the world of hand surgery.
Dr. Wayne Weil: Um, with wrist fractures. Um, for, for many years, people were treated in, in awful casts, and then their wrists came out of the cast and they were crooked and looked horrible and, and worked even, even worse than they looked. Uh, and then, uh, there was an interest in external fixators, which, uh, Basically, uh, looked like an erector set that was pinned to your arm, and, uh, nobody like those either, and they, they worked maybe [00:20:00] marginally better than a cast.
Dr. Wayne Weil: Um, and then there was an interest in, in, instead of doing these erector sets to maybe, uh, putting in some plates and screws. Uh, and that was really began the evolution of, of how we treat wrist fractures and, and especially just the radius fractures in general, uh, to the point where now we've got, uh, Uh, what's called the voler plate, which is the voler side of the hand is the palm side of the hand, so voler plate, uh, and, and fixed angle devices, which basically means the, the, the screws lock into the plate and it creates, uh, really stable fixation of fractures.
Dr. Wayne Weil: Uh, and, and, Think of it kind of like an internal cast, uh, to the point where at this point after, uh, an internal fixation, uh, of a distal radius fracture. Uh, I don't use a cast anymore. There's no cast. Uh, it's just a soft bandage. After surgery, folks, [00:21:00] uh, start their physical therapy three to five days after surgery.
Dr. Wayne Weil: Uh, so they start their physical therapy before I even see them in the office, which I, I see them in the office at two weeks after surgery to take out stitches. But they've already had a week of physical therapy before they've even seen me postoperatively. Uh, which just basically. Uh, like any other surgery, I'm sure like all, all your operations, Dr.
Dr. Wayne Weil: Garcia, you know, as, as soon as patients hit physical therapy and, and they can get hit the ground running, it just speeds up their recovery so much faster. So they're, you know, back to work, they're back to sports, uh, back to regular life, you know, months and months, uh, ahead of where they would, if, if, if they weren't, uh, uh, engaged in that, that PT right away.
Dr. Wayne Weil: So, Um, the voler plate has been a huge advancement in, in the world of hand surgery, uh, and, and it's really gratifying to be a part of [00:22:00] that, uh, Um, kind of wholesale change in, in how we, uh, uh, treat these fractures. And these fractures represent one sixth of all fractures seen in an emergency room. So one of the most common fractures, uh, that we see in.
Dr. Wayne Weil: And I see, uh, you know, 10 or 15 a week. So, uh, it is super common and, and it's great that we have a great solution for it. Well, that's amazing to hear.
Dr. Grant Garcia: Well, I think. And I think it's excellent to hear that we have such a good, um, person to take care of those in the area. So thank you again for that information.
Dr. Grant Garcia: I think there's something, uh, I'd like you to kinda share cause I know that we've all talked about this special rehab. Uh, devices we use and things like that. I know you just recently started doing, you did a couple patients with your fractures and this new machine, the relists, which you've also had done with your elbow, uh, patients.
Dr. Grant Garcia: Again, still working on, you know, outlets for it and insurance things and everything else. Yeah. But will you tell the, the viewers, you know, they've [00:23:00] probably seen your, um, insane surgery you did on the elbow of that kid, that every, every part of their body was stuck and you've been able to find ways. To offer probably one of the only ones.
Dr. Grant Garcia: You're one of the only ones in Washington I know that's hand surgeon that has this opportunity. So it's pretty amazing to have this device. Uh, tell us little bit about your sort of experience with it and what it's, how it's helping your patients. Again,
Dr. Wayne Weil: you know, I, I'm a huge believer in motion and if we can fix
Dr. Grant Garcia: fractures and,
Dr. Wayne Weil: and.
Dr. Wayne Weil: And fixed ligaments, uh, in a way that we can get them moving as quickly as possible. Uh, then we have the opportunity, I think to, to really get outta the gates running quickly and, and, and with this new relist device, I, I think it's awesome. It is just, again, it's all about movement, moving people quicker, and the great thing about it is that, Um, because we can monitor [00:24:00] our patients remotely now, um, it just makes us be a able to really dial in people's therapy protocols basically on a personalized level.
Dr. Wayne Weil: Uh, you know, it used to be, uh, that we would, um, you know, make physical therapy prescriptions and it would be. You know, one size fits all and, and sort of like our pump surgeries, uh, that we're trying to really individualize to the patient. Um, this device allows us to individualize, uh, patient's rehab protocols right from the get go.
Dr. Wayne Weil: And, and it's, it's, it's so scalable in that there's so many, uh, variations that we can tweak with this device, whether it's, you know, just simple, um, passive range of motion. Versus active and active assist range motion, which the, uh, means, you know, just moving the, the joint versus actually [00:25:00] having the patients fire the muscles and start their strengthening protocols.
Dr. Wayne Weil: Um, and it's so adaptive. I mean, you can use it in the knee, you can use it in the elbow, you can, uh, we've used it in the wrist now. Um, so, uh, it's really, I think, again, very exciting, uh, to be an orthopedic surgeon, uh, in this day and age. Cause we have so many. Better tools that we can provide to our patients and, and we're getting such better outcomes than we did 20 years ago.
Dr. Grant Garcia: Well, and I think the important thing that the listeners need to hear is that, you know, you see, we talk about all sports, orthopedics, all sports all the time, but it's more than just the surgeries. Right. And I think Will's seen this before where there's lots of things that we are non-surgical treat, but also in the surgery is not just the surgery.
Dr. Grant Garcia: You know, that's the, that's the. That's the part that everyone finds is sort of the sexy, glamorous, technology driven, but really it's, the postoperative is very important. And as you heard from Dr. L, he does an amazing surgery, but if that patient doesn't move, [00:26:00] they don't look good. Yeah. And so he's, he's talking about ways to accelerate everything.
Dr. Wayne Weil: And so when you
Dr. Grant Garcia: do that, that's when you have patients rocking it in the office at six weeks. And so having the device plus the good surgery plus. Accelerated rehab. It's a combination and so, you know, will hears us talk about this all the time, but it's not, you know, we're orthopedic surgeons, but we also specialize in.
Dr. Grant Garcia: Orthopedic postoperative care. We specialize in preoperative evaluation. You know, it's not just doing the surgery. We love the surgery part, but I also love good outcomes. And so the key here is with seeing with Dr. Wild is same thing. It's just continuing. How can we fix it at every level? It's a supply chain, you know, kind of machine sit system we have to have, but you gotta make sure that every part's working correctly or you're not gonna
Dr. Wayne Weil: get
Dr. Grant Garcia: a good outcome.
Dr. Grant Garcia: But if you do it correctly, you get good outcomes appropriately. So. Yeah.
Will Sanchez: And it's a, it's a good reminder also, we had talked about this on one of our other shows about technology and, [00:27:00] biofeedback. And, uh, you're talking about this rebless, right? That was the, a robotics one that we talked about.
Will Sanchez: Yes. How
Dr. Grant Garcia: it please look at our previous episode to learn
Will Sanchez: about it, you know, the, the physical therapy device for both upper and lower extremities , and Dr. Weil, uh, said it perfectly, right? The elbow, the wrist, the ankle, knee joints. , so As a patient, right? As someone that's gonna come into your office, and have something done.
Will Sanchez: And knowing that, okay, that was just, that's step one. But now what's the next step to get back to having some normalcy, right? To get back to doing the things that we want to do, whether it's, you know, grabbing my coffee mug because my, my. Thumb is now fixed and I'm, you know, getting treatment or, you know, going for a run because now my knee is fixed.
Will Sanchez: So from the surgery through the rehab and having technology, that's really exciting for, for us. But I know for you guys too, cuz it's like new toys. So it's, uh, it's really exciting.
Dr. Wayne Weil: Yeah, it's, it's, it's, like I said, it's [00:28:00] really, I think the golden age of orthopedics is, is upon us and, and we are having this huge, um, uh, merger of, of, you know, high tech computer electronics and, and, and, you know, old school anatomy and surgery.
Dr. Wayne Weil: You know, my kids ask me all the time, uh, about, you know, the, you know, Bionics and the, the $6 million Man and all that. I think forget books, I mean, we're, we're, it is, it's closer than we think. Um, and it's really exciting, especially with inflation.
Dr. Grant Garcia: You may be six mile, mile man
Dr. Wayne Weil: sooner or later. Oh yeah.
Dr. Grant Garcia: Uh, I think we're gonna have to wrap up soon, but, uh, Dr.
Dr. Grant Garcia: Wahl, can you tell us anything sort of, you know, hand, wrist, what are you most excited about in the future? Anything you've heard about that you're looking forward to kind of read about? I know you're da dabbling, you know, you talked about the tightrope, you [00:29:00] talked about the, some implants you're using for the thumb.
Dr. Grant Garcia: Is there anything else you're kind of thinking about in the future that may be coming? You gotta learn a little bit more about it, uh, for the listeners. So they kinda get excited and. Maybe check you out in the future and find out if there's something you can offer for them.
Dr. Wayne Weil: Yeah, I mean, you know, from a, a sci-fi perspective, uh, a lot of interest in, in just robotics and biofeedback and, and, you know, for our severely traumatized patients, uh, one day being able to provide them with, with, uh, a real.
Dr. Wayne Weil: Uh, useful and working robotic hand as opposed to just a, a hook, but that, that's pretty far out there. Hmm. I think more, uh, closer on the horizon, uh, is, uh, the continued sort of miniaturization of, uh, our implants that we use, uh, and, and tools that we use in other body parts. Uh, the fact that, uh, we're [00:30:00] now able to get, uh, cameras that are small enough to, to fit into the small joints of the, the wrist and the hand, um, really allows us to kinda move hand surgery forward.
Dr. Wayne Weil: Uh, kind of like the knee and shoulder docs have been able to do over the last 10, 15 years. Um, we're gonna be able to do all the stuff that they do. Um, just on a much smaller scale. Uh, so that I think is quite exciting. Um, and then, um, the other, uh, one that I, I think is, is really important is, um, sort of nerve recovery and nerve regeneration.
Dr. Wayne Weil: Uh, so you slice your hand and you lose feeling into your fingers. Um, when you're taking out that avocado pit or, uh, uh, slicing the, the bagel and you slice open your hand, um, really getting nerves to regenerate quicker, uh, so we can, uh, repair your nerve and, and you [00:31:00] get sensation back into your fingers faster.
Dr. Wayne Weil: Uh, all that I think is, is really exciting.
Dr. Grant Garcia: Oh, we just opened up in another Pandora's box, so we're gonna hold off on that until the next time we have Dr. We on, but the, ive got one more question ballgame.
Will Sanchez: I got one more question before we let
Dr. Wayne Weil: him go. Yeah. We, we can talk about kitchen, uh, kitchen knife injuries, uh, next time.
Dr. Wayne Weil: Oh,
Will Sanchez: no, no. One last question before I let you go. As a, as a parent, and I know everyone on the call as a parent, we have our little ones and they fall and sometimes they're like, oh, ouchie or something like that. But is there a, Hmm. Lack of better word. A simple sign where you need to, as a parent, say, you know what?
Will Sanchez: You should go get your, uh, child checked
Dr. Wayne Weil: out as
Will Sanchez: far as a wrist. I, I had a friend that their, daughter fell. You know, they, they complained a little bit here and there, but didn't complain much because just to remind everybody, there's eight bones in the wrist and 27 to hand. Yeah. So you might have an injury that doesn't hurt that much, but something is wrong.
Will Sanchez: Is there a sign? As a parent listening that if [00:32:00] your young child that may be having a trouble communicating displays or exhibits this, you should go have them check it out.
Dr. Wayne Weil: Yeah. You know, I, I tell this to, to my patients and friends all the time, you know, kids are smarter than adults, right? Adults, you know, always are trying to play through the pain.
Dr. Wayne Weil: Whereas a kid, if something hurts, they're not gonna use it. And so if all of a sudden. No, you notice that your, your, your kid isn't, you know, grabbing stuff, with their, uh, hands normally again, or they don't wanna ride their bike or they don't wanna go out and climb trees cuz uh, you know, their wrist or their hand.
Dr. Wayne Weil: , you know, it seems to be bothering them. Those, those I think are telltale signs that, um, you know, something's wrong when there's sort of this immediate change in behavior. Mm-hmm. Um, where you, where, you know, you had a kid running around yesterday. Now they're, they're, [00:33:00] they're kind of mopey and, and, and not wanting to do, uh, the normal stuff that they, they usually do.
Will Sanchez: Great. Thank you so much, Dr. Weil, please everyone, orthopedic specialist of Seattle. Check out Dr. Wayne Weil at Seattle Hand Doc as well. I mean, you've got, you gotta read his bio, I mean, from where he is been, where he is
Dr. Wayne Weil: graduated, and
Will Sanchez: nyu, I know you're a Maryland guy. I mean, marathons, triathlons, Ironman, we ain't even get into that.
Will Sanchez: I had a whole other thing for you there, but we don't want to keep you up. Dr. Wilde, thank you so much for your time this evening.
Dr. Wayne Weil: Thank you. Thanks you guys. It was great chatting with you and hope to do this again with you. Okay, thank you. Thank you very much for being on
Will Sanchez: Dr. Garcia once again. Great. Guest, initial thoughts on what we just heard?
Dr. Grant Garcia: I just. I just love hearing innovation. You know, you guys always get to hear me talk about all the fun, fancy stuff I like to do, but you know, I only do three joints and there are a lot more in the [00:34:00] body and there are a lot of other bones and other things that we do. And I think what you're seeing is that we're in a day and age, especially in uh, Seattle practice that we have, or in a downtown city practice, you have to be super specialized.
Dr. Grant Garcia: And there's so much to keep track of. You really wanna make sure that you're getting the person that does the most of this. Yeah. And understands the most of this. So that's really what this our practice has turned into. Um, and patients expect that, you know, there, the days of going into somebody that does everything is just, it's important.
Dr. Grant Garcia: But really that subspecialist super specialist can really help out and pick up on things. You know, you, like you talked about for the hand, you're 40 years old, you're not gonna get a seven year old procedure. Yeah. You know? Now we have procedures that are set for each age limit. Um, so it's, it's really important for us to understand how this works.
Dr. Grant Garcia: It's important for patients to be informed too. You know, the number of patients that come in, they're like, I had no idea that was an option. You know, that's why we do this. Yeah. Right. We teach them about what's out there, what can be done to get them to do, uh, better. And so really it's, it's important for us to make sure that we educate the [00:35:00] patient population, you know, from the Seattle area to.
Dr. Grant Garcia: Uh, throughout the Washington State, et cetera, and or people that listen to our podcasts from elsewhere, we've got people from outside the country listen to this. Yeah. Hopefully they can have those options where they are. So that's really what our goal is, is to inform patients and just to show 'em how excited we are for n New technology.
Dr. Grant Garcia: And, you know, it'll be exciting in a year or two to update on this and find out what we heard, what happened, what didn't happen. Um, and that's the way technology works. So we wanna keep people updated. Again, all sports, all orthopedics really. Maybe all innovation would be another thing
Dr. Wayne Weil: we could add to our title at some point.
Dr. Wayne Weil: I like it.
Will Sanchez: I like it. No, definitely. It was great to, uh, kind of circle back to, uh, the technology we've talked about before with Redless. I was like, oh, atrial robotics, redless. I know exactly what you guys are talking about. So it is really exciting to hear that, uh, the different ways that all of this is being utilized.
Will Sanchez: From, you know, the knees to the wrist and you know, hands and so on and so forth. So, I,
Dr. Grant Garcia: I need to remind the listeners that despite, while everyone thinks that Will Sanchez is a doctor, he's still in [00:36:00] training. We're still working on this, but you may think he's a, a physician from this podcast. So I've been impressed.
Dr. Grant Garcia: Uh,
Will Sanchez: thank you. I'm work, I'm working on it hitting, you know, you know, secretly I'm gonna, I'm just gonna walk in with scrubs one day and say, all right, Dr. Garcia, move over. I got x I'm doing this in total bracing, you know, so that, that'll be great. Yeah. But Dr. Wild's absolutely incredible., Check out his resume, you know, from NYU Hospital and, you know, shock trauma hospitals and, you know, I, I wanted to ask him, I said, listen, you're, you're from Maryland.
Will Sanchez: Um, are you excited about your Baltimore Orioles that are playing so well? Or, you know, you've been here, what I believe 18, 19 years, something like that. You correct me if I'm wrong, is he a Marylanders fan? Yeah., so, uh, you know what, what gives
Dr. Wayne Weil: here, but I didn't wanna,
Dr. Grant Garcia: I didn't wanna start off.
Dr. Grant Garcia: I think he's a true Seattle guy now. Oh really? He's coast up, but, True Seattle guy now. Yeah. We're all, we, you, we live in Seattle. You know, you become more of a Seattle except for me. I'm, I'm a I'm still the New York guy. That's right baby. I still like giants. We know this. Yeah, but that's just you and me we're [00:37:00] different.
Will Sanchez: Uh, his Orioles are doing well this year, so I didn't know, so I wanted to ask him. But we'll save that for another time when you bump. Next time when you bump into 'em, ask them. That'll be a around the round table when you guys are hanging out and say, Hey, by the way, you still Orioles fan, or you on the Mariners
Dr. Wayne Weil: bandwagon?
Dr. Wayne Weil: But Dr.
Dr. Grant Garcia: Gar, oh, maybe I'll give you update next
Will Sanchez: talk. That'll be great. Dr. Garcia. Thank you for your time. Check us out, sports.talk.com. All sports, all orthopedics, all the time. Maul Sanchez, Dr. Grant Garcia, thank you and very much Dr. Garcia for your time today. Thank you
Dr. Grant Garcia: so much. Looking forward to it.
Dr. Grant Garcia: Check us out and uh, check out our previous guests and, uh, check out what's coming up. Audio Transcript
Dr. David Smith, inventor of the Q-Collar

Will Sanchez: [00:00:00] Welcome everyone, and thanks for listening to Sports Doc Talk. Check us out@sportsdoctalk.com. Remember all sports, all orthopedics all the time except for today, but we are really excited about our guests. We've got Dr. David Smith. He is an inventor. He's an. Author, he's been on podcast, television news, you name it.
Will Sanchez: So we're really excited about having Dr. Smith on to talk about the Q collar. But before we get to that, let's get to our Dr, dr. Grant Garcia, Dr. Garcia, before we welcome in. Dr. Smith, how are you? Are you excited? It's almost summertime. You know, got some good plans for the summer for you.
Dr. Grant Garcia: Yes. Well, again, thanks for having me and we're really excited about having Dr.
Dr. Grant Garcia: David Smith today. You know summer's looking good and you know, we've had so many episodes with Tua and concussions and we've talked about concussions [00:01:00] before. And we've talked about the napkin to reality inventions, and we've brought up lots of examples, but we haven't had an opportunity to have someone as esteemed as him on the show.
Dr. Grant Garcia: So this will be excellent to kind of teach everybody what it takes. Well, where we came from and a really, a really challenging topic to deal with is concussions. And so we have one of the experts here, so I want to kind of take it off from there. And Dr. David Smith, if you don't mind kind of telling us a little bit about your product and people can learn about it and kind of what you got you into this and sort of what the dilemma is you're dealing with.
Dr. Grant Garcia: Yeah, sure thing.
Dr. David Smith: You know, my background, believe it or not, kind of mirrors yours, Dr. Garcia. I actually was an all-American swimmer like yourself. I went into chemistry and then came into medicine after sort of having some life-saving events as lifeguarding in swimming, and made a huge life change and decided that I.
Dr. David Smith: Had to move into medicine, but taking a chemical brain, a chemistry brain, and the logic train that goes with it all the way through to [00:02:00] Case Western Reserve in Cleveland which is sort of a detective world internal medicine is I left the case Western area after I got trained and actually acquired the assets from Pfizer's.
Dr. David Smith: A development team to make advanced wound dressings. And I ended up going out into the world and manufacturing these wound dressings and trying to make them smart and trying to invent them into something new and different that, believe it or not, led me to stand in front of the Army Research Lab, showing them how to not have our soldiers bleed out on the battlefield.
Dr. David Smith: And after I was done, the project coordinator happily walked up, put his arm around me and said, wow, really clever doc. He says, but you know, We really are struggling with traumatic brain injury here. We've got a hundred billion dollars a hundred years and we're having trouble moving the needle. Wouldn't it be great if clever people could just solve this TBI problem?
Dr. David Smith: And one of the guys in the room raises his hand and says, you know, I think if someone could figure out how [00:03:00] woodpeckers can smack their heads into a tree 80 million times and fly away. Maybe we'd have this whole thing solved. Everybody cracked up but me. But believe it or not, six months later, we did figure out how all of the creatures of the forest actually can tolerate unbelievable G-forces, like head ramming, sheep diving birds, giraffes, or headbutting animals.
Dr. David Smith: And of course, The woodpecker as well, and they utilize mechanisms to raise the volume of blood in the brain so the brain's not able to slosh around within the confines. And we all understand how important that is because if we get in a car and we put our seatbelts on and our, our pretensioners and the airbags go off, even the National Highway Transit Authority says, You reduced brain injury by 80%.
Dr. David Smith: Well, believe it or not, I did come up with about 15 years of research into this, 25 publications, 43 patents. And finally [00:04:00] last 2021, the FDA came out and authorized the first and only medical device to be able to make claims against traumatic brain injury, and that's called the Q collar. So to answer your question, it puts a slight amount of pressure on your jugular veins.
Dr. David Smith: It's a very, very tiny amount. If you reach down on the back of your hand and push on the back of one of your hand veins, that's 30 millimeters of mercury of pressure to collapse that vein. That's all we needed to divert a tiny amount of blood over into the venous capacitance vessels. And guess what?
Dr. David Smith: Your brain locks in place. It's as simple as that. Huh. Well, that's
Dr. Grant Garcia: a fascinating I think for all the listeners, you know, to hear kind of your story and how you went from, you know, this idea to the product, and I guess we can get into that in a little bit. But you know, And hearing, hearing this sort of, I hate to say simple idea, but pretty impressive, you know, looking at the way the animals [00:05:00] work and I understand, you know, how the juggler anatomy works and how you're adding that extra blood supply in the brain to try to stabilize it better.
Dr. Grant Garcia: I. For all the listeners out there, can you kind of tell, so that's important, but how does this sort of convert into the nfl? Like where, where did your path go with that? You know, again, N F NFL we've talked about before and all these sports shows, they wanna be on the cutting edge, but they obviously wanna keep their players safe.
Dr. Grant Garcia: So what's your sort of experience with that level?
Dr. David Smith: Well, we were very fortunate. We had. 350 million social media hits in 48 hours after the F D A released that press release. Hmm. So we got a lot of action out there and excitement, but unfortunately it's a medical device. We still had to get every advertisement okayed by the F D A.
Dr. David Smith: So it took almost an entire year still. And then we launched in 2022 and we now have 13,500 athletes. We have 150 professional athletes from. All across the spectrum, 45 N F L players. We had eight [00:06:00] people in the playoffs. We had one in the Super Bowl, Boston, Scott actually got a touchdown with a Q collar on.
Dr. David Smith: Mm-hmm. So we, we've really had an enormous amount of success in people that actually start using this device. It's been well received. We have over a million head impacts. Now think about that. A million, and these were studied by some of the best institutions in the world. This was not done in my garage.
Dr. David Smith: I'm really proud to tell you that just today, Cincinnati Children's Hospital got awarded the number one children's hospital in the United States by U S A today. That's where more than half of my studies were done. We also have Harvard researchers. We have university, or excuse me, Mayo Clinic, university of Toronto, West Virginia University, Chicago North Shores.
Dr. David Smith: My point being is, is this is not a cute seed device. This is literally $20 million worth of research in 15 years of my life. Yeah, trying to make sure that we [00:07:00] made sure that this was safe. And after a million head impacts, we didn't have a single unusual occurrence. None. Wow. Wow.
Will Sanchez: Yeah, and, and we're seeing that across.
Will Sanchez: That's
Dr. Grant Garcia: not a small feat. Do you know? No. Could you tell the listeners, could you tell the listeners off? I don't know if you seem to have a lot of knowledge off the top of your head, which is impressive. I like it. Do you know what the average occurrence is for normal head injuries? And is that to give them example of what the difference is from what you're telling them to the sort of the, the norm without
Dr. David Smith: your collar?
Dr. David Smith: Yeah, I'd be happy to kind of you know, one of the little pet peeves that I have from an academic is the, is most people do not understand the difference between a concussion and a traumatic. Brain injury. Yes. A concussion doesn't necessarily cause an injury, at least per most people's understanding, but repetitive head impacts are becoming the most obvious source to look for chronic traumatic encephalopathy.
Dr. David Smith: Our most recent study at Harvard actually used in animal model, and we were actually able with [00:08:00] jugular compression, which is how the device works. We demonstrated a reduction in phosphorylated tau in neurofibrillary tangles. These are the precursors to chronic traumatic encephalopathy, C T E. The dreaded thing that no one's been able to really get a handle on and what are we going to do?
Dr. David Smith: And yet there's not, I'm not saying that this is gonna block it, it's just the first study that suggested that something might actually be able to put a dent and what is happening to some of our traumatized to soldiers as well as. As, as well as athletes. I'll take this opportunity to tell you.
Dr. David Smith: We've already gotten complete acceptance by the Army. We just had the best Ranger competition down in Fort Benning, Georgia, just two weeks ago. 39th annual and every single one of the hundred and 30 Rangers had two colors on. Wow. How cool was that?
Dr. Grant Garcia: That was very cool. So for the, for the listeners, let's go back to that topic you had about the concussion [00:09:00] versus traumatic brain injury.
Dr. Grant Garcia: You know, from, sure. Like you said, for most of us, we hear the word TBI and I, you know, you think, you know, traumatic brain injury. We think, you know, a massive, you know, Massive issue where you have long term permanent damage and that's, that is a lot of times the issue and the word concussion, like, oh, I got a concussion, I have a headache.
Dr. Grant Garcia: Or if we hear from sort of the, in more layman terms, you know, football, that's considered more of a concussion thing and then otherwise it just kind of bon your head. Can you, with the cue collar, is the end, is the thought process that you're reducing concussions or you're reducing the concussions that could go onto a tbi?
Dr. Grant Garcia: Is that correct? Or what is, what's the, what's your pathway you're talking
Dr. David Smith: about? Sure. So as you're aware, in one season of, say, a sports team of say 50 50 kids, high school kids, there may be one, if not two concussions on the team over an entire season. Mm-hmm. But what we did was, and, and we can measure and we can study concussions by computer programs.
Dr. David Smith: It's an expensive, we can have that, like trainers go out there and question people. I mean, in the old [00:10:00] days they just said, Hey, what day of the week is it? Right? I mean, it's come a long way. From that, we ended up going a massively more detailed and expensive route. We used tensor mri. This is one of the most sophisticated imaging methods of looking down into the micro structure of your brain.
Dr. David Smith: We did a tensor r i at the beginning of the season, and then we did another one at the end of the season. And using digital subtraction angiography, we were able to superimpose these images onto each other. And if there was, Any change at all in those two images, then you get little red dots that appear on your picture, your image of the screen.
Dr. David Smith: And on the kids that did not wear a Q collar, I'm sad to tell you there were hundreds of these micro structural changes, but on the kids that wore the Q collar there were next to none. It's absolutely sobering to see these pictures, which I'd be honored to pass these studies on. They're published and they're available to any and all that are [00:11:00] interested When you use the word concussion, sadly it, it can come about from a lot of very subjective.
Dr. David Smith: Nebulous data that's put in. In fact, at Cincinnati Children's and other institutions and headache clinics, they can enter into a concussion protocol because the parent calls and says, I think my kid had a concussion yesterday. Okay. Now that's not quite as objective as being able to look down into the mechanics of the brain and objectively see a difference in their actual brain structure.
Dr. David Smith: So that's the frustration of using the word concussion. There aren't as many of them, and so when you power your studies, we analyze that we would have to do around 10,000 kids if the only thing endpoint that we were looking for. Was a concussion. Now it turns out our data did show a reduction in concussions, but one of the critiques that people have had with the Q collar is we didn't even try [00:12:00] to power our studies for concussion.
Dr. David Smith: Now that there's tens of thousands of people wearing these Q collars, I think you're gonna find that we are gonna be able to have the data for people, and we're gonna be able to demonstrate those reduced numbers of concussions out there on the field.
Dr. Grant Garcia: I think that's an excellent point for the, for the listeners, we just had a napkin to reality kind of talking about what you're, what you did, which is taking a product idea and turn into the big picture.
Dr. Grant Garcia: And I think we didn't talk about the clinical side of things. It's nice to have someone such as you with the academic background, you know, people don't understand that, you know, they want these clinical studies to have. Thousands or hundred thousands of people in them, but it's just not possible. It's too expensive, et cetera.
Dr. Grant Garcia: And so to hear that you know that that word power is really important for us to understand from an epidemiological standpoint is that. When we have these new products we're you can't get studies that big without multiple, multiple millions of dollars. And initially in the run of things, it's just hard to do it, as you would probably agree.
Dr. Grant Garcia: [00:13:00] But the fact that you got enough information and you were able to find a better way, and again, I've always thought the word concussion is very vague. It's like shoulder pain, right? Right. And so there's not a subjective way. I mean, we, when if Will asked me before, you know, how do you know from concussion?
Dr. Grant Garcia: You do an scat, you do a test, you ask what day of the week it is. You know, we've got some more sophisticated things, but in the high school level, we're not able to get those MRIs you have unless we have a big study on it. You know, I can't tell my high school kids, I'm gonna go send you for an MRI after they hit their head and they're walking and talking.
Dr. Grant Garcia: Normally it's just not something we can do in real life. But you know, there has to be better subjective information and it's good to, it's good that you were able to. Elicit that clearly. It's obviously your specialty. But it's good for the listeners to hear that, you know, that doesn't always mean they have concussion or the word concussion can be thrown out more easily and to the point where the doc, where the doctor gets a call or the trainer gets a called and be like, the parents said, my kid had a concussion without any real basis on what that
Dr. David Smith: means.
Dr. David Smith: Right, and they're in a concussion protocol all of a sudden. I mean, it's very frustrating. You use the word cost and, and yeah, you're right. It's [00:14:00] tough to cough up the kind of dollars that was put into this. And we didn't take any individual's money. This was privately found dollars so that we did not have to answer to anybody, whether it be the NFL or a professional out outfit or.
Dr. David Smith: Anything. We wanted to make sure that we had the best data we could have and people may somehow scrutinize the studies that were done. There were 25 of them, not one or two done by literally the most powerful, brilliant people that we could find in the planet Earth in brain injury today. So if, if it could be done better, we certainly don't know how, and I would love to hear how somebody could come up with somebody better than the list of our research partners that did the work for us.
Dr. David Smith: Now, mind you, I was on those articles, but I never touched a single subject patient or touched the data. I just helped people understand the physiology of what we were bringing to the table to help prevent these injuries. [00:15:00] And.
Dr. Grant Garcia: This session, I know we're gonna get sidetracked, but the science of, it's really interesting.
Dr. Grant Garcia: So the thought process of this jugular vein compression is you get enough, enough brain swelling to prevent it. So basically it's more sloshing and less likely to hit on the sides with this, this sort of impact, I hate to use the word concussion now that we've talked about. It's such a vague term. Is that the, is that the physiology behind it? D
r. Grant Garcia: And is there any, are there any concerns with, you know, more blood in the brain? We know in general if in blood, in the brain, in other areas is not good. But in this case that jugular blood is different, right? Or how is that different than sort of a traumatic brain injury where you get hit and then you bleed into your brain?
Dr. Grant Garcia: Obviously it's a different pressure, but I'm just curious sort of what's the difference in your ideas or your thoughts on that?
Dr. David Smith: Just an absolutely excellent question actually. So think about it. When you stand up, gravity is going to pull the fluids out of your cranial space, and in reality it's about four milliliters.
Dr. David Smith: Drop out of the cranial space and 20 milliliters drop out of your [00:16:00] spinal column, and that allows the brain to suddenly move around. Well, guess what? If you just lie back down, the volume and pressure inside your cranial space is about 20% higher than RQ color. So think about this. Wow. If you fear putting on this cue collar, for God's sakes, don't ever lie down again.
Dr. David Smith: Right. I mean, the physiological mechanism we're imparting is within the norms of what the body does every single day. Now, what the collar does in jugular compression actually mimics the actions of the omohyoid muscles in your neck. So you ready for this? Prior to our work, nobody knew what that damn little muscle did in your neck.
Dr. David Smith: Our orthopedic, and I see it, but I know
Dr. Grant Garcia: what it does.
Dr. Grant Garcia: Yeah. Well. Well, they didn't know.
Dr. David Smith: That's what's so exciting. Neurosurgeons actually cursed its name because every time they would go in to operate on [00:17:00] the neck in some way, shape and form, it took 20 minutes to dissect that muscle off the jugular vein. It wasn't close. It's literally affix. To the jugular vein, and it's that crazy woodpecker that made me realize the anatomy of that woodpecker's tongue is bizarre.
Dr. David Smith: It attaches to the top of the beak, goes up over the top of the skull, separates, goes around, attaches to both jugular veins, and then goes, forms the tongue, and goes in and out every time it blows into a tree. I mean, seriously. That's crazy stuff. Well, you have to have a
Dr. Grant Garcia: comment on this.
Will Sanchez: Oh, yeah. I mean, we've, we've covered a lot of topics.
Will Sanchez: I, I think Dr. Smith just a question. You know, how could you Make this even better is that putting more information or some kind of chip in the Q collar so you can have some kind of readings of you know, what the activity is before, during, throughout the entire process, whether it's soccer or [00:18:00] whether the army or football, anything like that.
Will Sanchez: Is there, like, what's the next step now to kind of keep pushing this forward and even gathering more information?
Dr. David Smith: So the, the you know, I've gotta give you a distinction. I do not own nor did I invest into the q 30 company that's actually out there commercializing. I'm the inventor. I created the patents.
Dr. David Smith: Yeah. I do get a royalty back, but I, I cannot speak to exactly what they're going to do. I do know from the last discussion with the team that they are putting monitoring devices, they'll be able to measure concussive forces and rotational impartation. And the thing that you guys probably know, sometimes you don't know where the impact is coming from.
Dr. David Smith: Yeah. Whether it's on a football field or if you're out there in the military and. Bomb goes off. You don't know if it's in the front, the back, the right, the left. You could impart a linear force into your brain or what's even more devastating, a rotational force into your brain, and it can come at any time.[00:19:00]
Dr. David Smith: That's the beauty of the cue collar. We mimic a yawn. So did you know that We now know why we all yawn. We didn't know that before we started down this path. When you yawn, you have actually four places in your jugular veins that completely collapse. Now you can, again, not believe me, Cincinnati Children's Hospitals, radiology and neuroradiology department demonstrated that and demonstrated that there's a back filling of the venous structures called the venous capacitance vessels.
Dr. David Smith: Big word, but it just simply means that the bubble wrap. Expands ever so slightly, only 5% per vessel. But all of a sudden, brain can't move around and it's just like bubble wrap. It's just like a, a airbag in your car. That's what you're gonna wanna pack around any package that you're gonna send across the country and you want it to get there safely.
Dr. David Smith: You don't put it in a steel container that's empty, you put it in a [00:20:00] cardboard box and you stuff bubble wrap all the way around it. Nature's been doing this for 20 million years, guys. All we did was mimic it.
Dr. Grant Garcia: Got it. On a, on a topic like that, you know, I, we all talk about, is there any role you think in sort of a collaborative effort, you have this now, this collar, And again, I think you made a great point for these people to understand this sort of conceptual idea.
Dr. Grant Garcia: You take an idea, you get a patent, and a lot of times you eventually sell the patent to the company and then the company runs with it. And it doesn't, you know, it doesn't mean you're fully involved with the company itself, which is what you mentioned. It's important for the people to understand how that process works too.
Dr. Grant Garcia: Cuz if people are always asking you like how you take an idea, bring it to reality, just like what you did and be wildly successful. But the question I have for you is, You know, they said, you know, these, they have these new expensive helmets. You know, my, my high school has like two or three of 'em.
Dr. Grant Garcia: They're like $2,000 a pump. And the NFL has 'em. You've seen these crazy looking helmets. Is there any role in the, in looking at, you know, a lot of times these studies, you wanna start with baseline, right? Like [00:21:00] regular helmet and versus the Q collar. But are there ideas in the future of like, how about more advanced helmets, more advanced technology with the Q collar?
Dr. Grant Garcia: Because the idea, and what I'm, what I'm thinking of is, is there any way that we can get these even better? Right. You've clearly shown a reduction from your studies, but can the collaborative effort be a combination of things, right? Because this is probably not gonna be a one size fits all or one answer to everything.
Dr. Grant Garcia: So is there any thoughts on that or what's the plan?
Dr. David Smith: Sure. Well, I, I hope you're not inferring that I don't think helmets are necessary. I mean, they do Exactly. No, no, no. They're design, I'm not inferring that. Yeah, they, they will stop you from getting a skull fracture. They will stop you from getting your eye gouged out.
Dr. David Smith: You must wear a helmet. But unfortunately helmets are not able to stop the movement of the brain from within the confines of its skull. Most traumatic brain injury researchers are now acknowledging that that is actually the true pathophysiology of an injury. You have to absorb the energy that's [00:22:00] coming, and I'm afraid that if you.
Dr. David Smith: Just make better, better and stronger helmets, you're just not changing the amount of movement of the brain within the skull confines. So you know, there's a lot of helmets that come and go. They've continued to make these improvements and there's not. Been any change in brain injury. So from my research and Dr.
Dr. David Smith: Julian Bales, who is one of the colleagues that worked with me, you are hard pressed to find a one, two, or 3% reduction in brain injury on any study. We blocked 83% of brain injury in the studies that we submitted to the FDA 83.
Dr. Grant Garcia: You know, I, I think that's an important point. You know, you, you have me, I follow this stuff pretty well, and that's still kind of, you know, I know that the helmets have had trouble with really producing the results, but it's also the idea similar to what we have in orthopedics and will understand this.
Dr. Grant Garcia: Essentially you are. You internally? It's an internal, I don't wanna get well too excited, but it's an internal [00:23:00] brace of the, of the of the the brain versus this external device and the word externally. When we do things externally and try to do external fixtures or things like that, they just don't have the.
Dr. Grant Garcia: It's also that torque and moment arm, and when you internally are able to kind of cushion the brain, it seems like that would be more powerful. So it all makes sense to me. And you know, unfortunately, as we know with the NFL or any of these concussion things, it's a multimillion dollar business. And so these helmets are always trying to one up each other and find what the best option is.
Dr. Grant Garcia: You know, they got the sensors as you know, you know, my, my high school and the teams I've taken care of, you know, they have the thing go off and it shows who got hit harder. It doesn't always mean anything and a lot of times it can do some malfunctions, but nonetheless, you know, it's interesting to hear your thoughts on that and that point is really important.
Dr. Grant Garcia: Cause I think that there is this misconception that that is the reason to stop concussions and it's for other reasons. And it, you know, again, we want players to be safe and we don't wanna give misnomers that homeless are not effective. But it's important to hear that there's still a lot more room that needs
Dr. David Smith: to be done.
Dr. David Smith: Well, in 2016, one of the lead articles in the [00:24:00] San Francisco Chronicle was that helmets protect skulls. They do not protect brains, and that's a powerful statement all by itself. But then when you find out who made the statement, that was a joint statement by the chairman and chairwoman of the Federal Trade Commission.
Dr. David Smith: US safety protective services. One of those, I can't remember which one it was, but at the end of the day they pointed out that you cannot make a claim that helmets reduced concussions and brain injury and that. That statement in 2016 came out right before they took every single helmet off the shelf worldwide that made the claim that they were anticon concussive because there's just no data showing that we have 25 articles by the best researchers in the world showing not a reduction in justice, nebulous term of concussion, but also actual physical.
Dr. David Smith: Damage to the brain structures, and that's what I think is, has just [00:25:00] got to be heard by most people. Yes. We didn't really go after that name in word concussion. We went 10 levels higher than that to try to help people demonstrate that we really were able to do statistical analysis. We were able to do all of these unbelievable methods in prospective studies.
Dr. David Smith: Best studies you can possibly do to demonstrate that this product is safe and effective.
Dr. Grant Garcia: Yeah, and for the listeners prospective is best option because basically you're not, you're not looking back at things where people can say, oh, I think I had it. I think I didn't. Cause if they get a concussion, they're gonna wanna remember one thing versus the other.
Dr. Grant Garcia: Prospective is like, you ready? You set it all up ahead of time and they don't know what's gonna happen. And so it's a lot less likely to be biased
Dr. David Smith: for the listeners. Yes, you gotta remove variables. You make sure that the. Two study groups are identical in absolutely every way except that that you can, except that one of the group has a collar on and one does not.
Dr. David Smith: And if you go backwards retrospectively in [00:26:00] time, you don't really know if the situations were identical. And so, yeah, you're right from a scientific standpoint, you just cannot provide more pristine and more powerful data that we did than what we did without sacrificing our subjects, which of course, were high school students and we're not gonna do that.
Dr. David Smith: Right, and so yeah, this is incredible levels of data I, you can probably hear in my voice. I'm really excited about it and very proud to literally be with some of the brightest researchers in the world and then have this kind of result pop out. Unbelievable.
Will Sanchez: Dr. Smith. Will, do you, yeah, yeah. I just have a, a question here.
Will Sanchez: You mentioned Dr. Julian Bales. And real quick, for those that don't know who Dr. Bales is, if you saw the movie Concussion about Dr. Omalu Dr. Ben Omalu, Julian Bales was the team physician or team doc, head team doctor for the Pittsburgh Steelers in that movie. So [00:27:00] having someone like him, Being a part of this discovery, this, this, this journey that you're embarking on when it comes to the invention of the Q collar, what kind of credence did that lead and what kind of, conversations allowed, you to have to say, Hey, this is something we are on the right path here when it comes to this.
Dr. David Smith: Well, you're absolutely right. I mean, he opened so many doors I can't even begin to tell you. And I think you'll find that Bennett O'Malley attributes Julian, for having an open mind. Yeah. When he came with the idea and concepts of what was happening to our football players and to be Quite blunt, I had just as big of a hurdle to get over with him.
Dr. David Smith: So not many people have the physics in the background to understand the, the impact levels that are involved. And I'll tell you what, it wasn't easy getting past his secretary when I had to teller that I wanted to talk to the chief of neurosurgery about woodpeckers. It really put me in a bad [00:28:00] way, guys.
Dr. David Smith: It was not a pretty sight, but at the end of the day, I'm really proud to tell you that I actually had three of my visual props in that movie. Concussion. I actually had to sign away a release because they used woodpeckers in there. Mm. They used Newton's cradle, if you remember. Yes. Those steel ball balls that are descended from twine and you lift the one out and drop it and it crashes into the middle balls.
Dr. David Smith: Yep. But nothing happens in the middle balls. The energy impact goes all the way through them, and then out the other side goes the other ball. That's what our device does. Yeah. It creates what are called elastic collisions, which means no energy gets transferred into the brain, and you're gonna love this.
Dr. David Smith: I actually was able to convince my team to spend $400,000 on a hearing study where we actually impact with an I E D level blast wave into little tiny laboratory animals. Half of them had jugular compression collars on, and [00:29:00] half did not. We preserved 93% of the hair cells of their hearing apparatus.
Dr. David Smith: When the Q call is on we block. Hearing damage on the battlefield, I shoot regularly. I get ringing in my ears every time, even though I have an ear muff and an earplug in. You put the cue collar on, the energy of that blast goes right through you and is not absorbed. It's so cool. So that's
Dr. Grant Garcia: essentially like the idea what people think of electricity.
Dr. Grant Garcia: If you can kind of pass it through without having it go into you too, you know, it's sort of like, or a ground or sort of like a grounding thing. So it kind of
Dr. David Smith: avoids it. You're you're quite right. I mean, and, and that's exactly what Newton's cradle ball depicts is those center balls. The energy doesn't, if you took that center ball, that steel ball and put a soft, gushy, pliable, grape, In there, all the energy of the impact will go right into that middle ball and that grape explodes.
Dr. David Smith: And if you have room [00:30:00] inside your brain, and I have tons of visuals I mean, I hate to give you, you know, to sit here and chill my websites and whatnot, but if you go to David Smith md.com, we have visuals, what we'll actually show you where we took eggs and put them into these unbelievable antique paint shakers.
Dr. David Smith: And they were in these mason jars partially filled with water and fully. Filled with water and within the partially filled mason jar with a fresh egg at the bottom, within five seconds, that becomes meringue. It just explodes the egg. But on the other side where there is a completely filled mason jar, meaning your skull, that that egg never breaks, doesn't matter how long you leave the machine on, it never breaks.
Dr. David Smith: The energy does not absorb by that egg. Awesome. It's actually relatively straightforward physics, but physics isn't easy for people to conceptualize, which is why I made all these visuals for people to get an idea. Yeah. Of what. [00:31:00] Amazing science is actually going on when you put that simple color on.
Dr. David Smith: That's
Will Sanchez: awesome. Before we wrap it up here yeah cuz I feel like we could talk about this forever and this is, this is perfect because we should be talking about this cuz it's really exciting, especially for every parent, every coach every person that has experienced this. And that kind of leads to my question is what's been I.
Will Sanchez: I don't know the greatest comment or compliment that you've gotten from someone. You've had players. If, if you look it up, there's N F L players wearing it now you can see every Sunday you could see the Q collar on soccer players like you, like you say. You mentioned the, the military. What is the one thing that stands out that, when you heard that you went home and you were like, man,
Will Sanchez: I feel really good about this. This really kind of made my day,
Dr. David Smith: well. I was here in Cincinnati, Ohio when we were playing the New England Revolution Revelation, and Omar Gonzalez was wearing his cue collar and a buddy of mine grabbed [00:32:00] my collar, went running towards the field, held it up in the air, and.
Dr. David Smith: Omar Gonzalez sees the cue caller and he points at it and he puts a thumbs up in the air and my buddy yells, Hey, the inventor's up here wanna meet him? He ran all the way through. All the fan came up to me, hugged me, and said, doc, I will never take this caller off. I'm a completely different player. I have a spatial awareness and reaction.
Dr. David Smith: Time is improved. And remember, We mimic a yawn. So physiologically we're identical to a yawn. And guess what? A yawn does it actually. Activates your attentional network. You're more aware when you yawn. So we've patented it for this. Oh, by the way, we just got another patent a couple weeks ago. We prevent vibrational forces from entering into your brain.
Dr. David Smith: Well, guess how cool that is for people going over the, in the what do you call it? The Play [00:33:00] field for many of the NASCAR that are rumbling down the field and you've got a cobblestone down in Atlanta, Georgia, and they're just exhausted after, you know, playing or running one or two or five laps around that.
Dr. David Smith: We block all of that. They, these, these racers just cannot believe how little energy is being absorbed into their brain. And you're right, the, the, the one thing that you can say about Dr. Dave, I hope to God it's on my tombstone, is that I was clever. Anyone can get these letters after their name. I've got letters after my name that go on and on.
Dr. David Smith: But you know what? You just cannot teach clever. And this technology is just clever. It's just standing on the shoulders of nature. Nature figured out how to do this and protect its little creatures. We are finally giving that same protection to mankind, and it's working in spades.
Will Sanchez: Awesome. Absolutely.
Will Sanchez: [00:34:00] Great. Dr. Smith, thank you so much. Please check out his book When Heads come together. You know, his tagline is Nature's My Mentor. So it was perfect that he ends this show on talking about nature and what it's meant to him and the inspiration to all of this. Please check out the Q Collar, the first and only device.
Will Sanchez: Authorized by the FDA for claims of prevention against T B I, which is traumatic brain injury. There, there's so much information. Thank you so much. Dr. Garcia, last words as we say goodbye to Dr. David Smith.
Dr. Grant Garcia: Well, I have to correct you will. You said we weren't gonna be talking about sports, but that's all we've been talking about is how we're protecting these athletes.
Dr. Grant Garcia: Yeah,
Will Sanchez: It's my trick to, to get you onboard. See, this is all my grand scheme as we get ready for the NFL season where I saw someone post, there's 12 Sundays before N F L starts, so it was extremely a, his. Hysterical. When I, when I read that there was like, it's 12 Sunday. It was on father's day. 12 Sundays.[00:35:00]
Will Sanchez: That's wonderful. To the start of the nfl. So what a way to kind of bring this in, and I'm so glad that Dr. Smith was able to be with us. Dr. Garcia, last words.
Dr. Grant Garcia: Well, Dr. David Smith, thank you so much for being on this show. This has been excellent. And you know, honestly I love to hear stuff like this in innovation.
Dr. Grant Garcia: I love to hear success and the future advances and that's what we're all about here. And I'm looking forward to telling my colleagues about this. This is really fun information and I really appreciate your time and your excellent speaker. And I think that all of our listeners are really gonna enjoy hearing this.
Dr. Grant Garcia: And thank
Dr. David Smith: you again. Well, I would like to make a personal offer to you, sir. If you'd like give me an email, I would be more than honored. I have a 20 minute full presentation of the science and everybody I've given it to, I've actually given it to the number two in the chain of command for the US Army, and she.
Dr. David Smith: Aid it up, and so I would be more than honored to give that talk to you or anyone in your department division or otherwise, just to help people understand just exactly what science went into all [00:36:00] of this.
Dr. Grant Garcia: Awesome. We'll likely take you up on that. Thank you
Dr. David Smith: so much, and thank you.
Will Sanchez: Thank you,
Will Sanchez: Dr. Smith. Audio Transcript
Dr Anthony Yi

Will Sanchez: [00:00:00] Welcome everyone, and thank you for listening to us at sportsdoctalk. Check us out at sportsdoctalk.com. I'm Will Sanchez, along with Dr. Grant Garcia. We're really excited. About today's show because we have a great guest, Dr. Anthony Yi. But before we bring him on, let's bring in our orthopedic surgeon and sports medicine specialist, Dr.
Will Sanchez: Garcia. I know you have a lot on your plate right now. You've got moving going on, family, friends, everything else going on. But first and foremost, how are you? And like always, it's great to speak with you.
Dr. Grant Garcia: I am good. Thanks for having me and I'm really excited about this episode. I think, you know, we spend so much time talking about knee, shoulder, and elbow stuff that I specialize in and we've been really waiting to have, you know, top notch foot and ankle surgeon on this show to talk about the ankle sports stuff cuz [00:01:00] it's so hot right now.
Dr. Grant Garcia: I mean, every article you see about. You know, we talked about Mahomes with the high ankle sprain and you know, there's other recent athletes that have shown getting back with some crazy surgeries, and I know we're gonna talk about your favorite topic, internal bracing. Oh, baby. And I thought, what better?
Dr. Grant Garcia: What better way to have it than the one of the, one of the Seattle experts, Dr. Anthony Yi. So we're really excited about that. I'm doing well, it's keeping busy, but I'm really excited about this show tonight. This will be our very first guest for sports doc talk. You can check us out at, you know, all the different platforms and this will be posted hopefully in the next few days so people can hear it and enjoy it.
Will Sanchez: Well, let's get right to it. We have Dr. Anthony Yi, he's with the orthopedic specialist of Seattle, and as you mentioned, he is a foot and ankle specialist. And listen, Dr. Yi, first off, we're really happy that you're here. You have all these accolades and all this training and university of Washington and Harvard and us.
Will Sanchez: And all of these experiences and awards, Dr. David, I mean David Award for best original [00:02:00] research paper and your dean's list and all this stuff. But listen, let's get past all of that. What I wanna know is if the Dr. Garcia and I come over the house because you say that you enjoy cooking, if we're coming over to Dr.
Will Sanchez: Yi's House, what are you making us?
Dr. Anthony Yi: Well, first of all, thanks for having me. I'm super excited to be here as well. Some of the cooking that I've been into recently, if you've heard of Doug Pearlman, she has an awesome little book called Smitten Kitchen. Some fairly simple stuff that can make a average guy like me make some pretty, really good dishes.
Dr. Anthony Yi: So I'd probably have you choose something from there and we could probably whip something. Sounds
Will Sanchez: good. Dr. Garcia. I know there's a lot to talk about. Why don't you just jump in right here?
Dr. Grant Garcia: Well Dr. Yi, you know, we're really excited to have you. I think one of the biggest things I keep seeing, and, you know, I, full [00:03:00] disclosure, I work with Dr.
Dr. Grant Garcia: Yi, I get to see is amazing results. And he's taking care of my family members. So this is a, this is a really special episode for me. But, you know, ankle fractures, You know, we think of ankle fractures. We used to think of 'em as sort of like, Yiah, it's a trauma injury. You know, you lots of motor vehicle accidents or people doing silly things, but high level athletes get this too.
Dr. Grant Garcia: And you know, we saw it with the Giants and other plaYirs when I was over in New York and some of these wide receivers getting in. We've seen 'em on football fields, but there's been a lot of press about some of the newer technology with these ankle fractures. And I've seen you do some of this newer stuff that I honestly, and I'm not that old in practice, had never seen before.
Dr. Grant Garcia: So will you tell us a little bit about what's going on with ankle fractures and what you're doing for
Dr. Anthony Yi: these athletes? Yiah, absolutely. So as you mentioned, you know, ankle fractures are common and we're seeing them a lot in high level athletes as well. And and. The key to treating these high level athletes is, you know, making sure you have a good solid plan for them.
Dr. Anthony Yi: You're taking good care of them, but also [00:04:00] balancing that with a timeline. Often in terms of getting them back to rehab, getting them back to the field, and sometimes maybe they may have an important. Playoff game coming up. So oftentimes there's that added pressure of a timeline and, but of course, making sure that first and foremost, you know, giving them sound care and, and proper rehab.
Dr. Anthony Yi: But one of the new tools in our toolbox is sort of a play borrowed out of another playbook that we use elsewhere in the body. And it's a, it's a nail. That we used to fix, fix def, fibula or one of the bones that make up the ankle joint. And so this is not necessarily a new concept. If you look into how we treat, for example, hip fractures or other long bone fractures like femurs or tibia, we often use nails.
Dr. Anthony Yi: And some smart people thought, why not? Let's try that for, [00:05:00] for the, for the ankle. And that has emerged as a newer method of, of treating ankle fractures. That has been great. In terms of some of the benefits of doing this oftentimes it means that we're making a much smaller incision instead of making a really big incision to fit a plate and screw along it.
Dr. Anthony Yi: Instead, this nail basically goes in through the very end or tip of the fibula bone and goes up the canal or the center of the bone and holds it in place. So one major advantage is, for example, that smaller incision that I mentioned not worrying as much about things like wound complications or infections.
Dr. Anthony Yi: Which is always on our mind as surgeons. And then the other major benefit of this is that you can get people starting to weight bear very quickly. It really depends on your comfort level in terms of how fast [00:06:00] you want patients to start walking on this. Some patients you can get going right out the gate.
Dr. Anthony Yi: Some patients you may want to wait till their wound heals up, which on average 10 takes, you know, about two weeks or so before you're comfortable enough to take sutures or stitches out. Mm-hmm. And let them get going. And this is, you know, that's a pretty signi still thing of difference for, for.
Dr. Anthony Yi: Professional athletes or high level athletes that have a timeline getting them going almost immediately, if not immediately, with, with their
Dr. Grant Garcia: rehab. And that's awesome. You know, we and will's here. You know, I remember even, you know, before Dr. Yi came to our practice, I would do a lot of ankle fractures and I always learned, and we used to do a wire with Dr.
Dr. Grant Garcia: Dean Lurch, and it was kind of crazy. We started doing these things and seeing that they would do it for the fib. Heads and fibular fractures. But most of the stuff is plating and people have other issues with, you know, problems in the back of their ankle and bigger incisions. And when I saw, I saw a few [00:07:00] of my friends get a fibular nail like a Yiar or two ago, and I seen it before.
Dr. Grant Garcia: And then Dr. Yi start. You know, I really don't do it anymore. Cause I have Dr. Ne so good at it, so I don't, I don't need to worry about that, which is nice. Will when we have a practice and we all do some super specialist work. But you fbri is, is really impressive. Have an example of a recent so brief,
Dr. Anthony Yi: briefly.
Dr. Anthony Yi: Yiah. So there was an NHL plaYir Alex killorn that. Recently had an ankle fracture. He was in the midst of the, the layoffs, I believe, and trying to get back as soon as.
Dr. Anthony Yi: Happened because of, because they got eliminated, well, I believe, but but basically, you know, he was, he had a fibula fracture. It was one that may not have necessarily required surgery if he was not on a [00:08:00] timeline, but in order to stabilize it and to try to get 'em back onto the ice. He made the decision with his surgeons to go ahead and have a flock placed.
Dr. Anthony Yi: And he was back practicing pretty quickly. But, but again I think, you know, he, he Didn't and ultimately get back into the games, but, you know, sort of a testament to how much, how fast you can get back at a high level.
Dr. Grant Garcia: Well, and you think, you know, I mean this technology, will, we talk about technology, these professional athletes treated differently, right?
Dr. Grant Garcia: You know, everything's different with
Will Sanchez: them. Yiah. One, 100%. Yiah. You know, and, and just kind of go back to what Alex Killorn, I, I remember the plaYir he plaYid with the 2021 Tampa Lightning that Yiar. They wind up winning the Stanley Cup and he got hurt game once. So imagine as a defender this plaYir is taking a slap shot.
Will Sanchez: And, and you know, any, anyone that's a hockey fan, especially the Seattle [00:09:00] Kraken craze that's happening right now, slap shot. His, you know, high nineties, you know, maybe up to a hundred miles per hour. And he got in front of this shot and it hit his leg, and that's how he broke his leg in two places.
Will Sanchez: And as Dr. Yi mentioned, he did his best to get back. He couldn't get back in time, but the beautiful part about it was he was on the ice. In skate when they won the Stanley Cup and he was able to hoist that trophy right then and there. So he didn't, he wasn't able to get back on the ice in time to compete, but he was there in time to be there with his teammates and to participate in the trophy ceremony.
Will Sanchez: Lift up that, you know, that trophy's about 35 pounds to be on ice skates, to do all those things, just games after that fracture had happened. Is incredibly impressive to think about what this fibular nail or this fac that they used for this. Dr. [00:10:00] Yi, just before we move on I know they use a radiolucent targeting guide.
Will Sanchez: What does that mean and how does that help you as a surgeon when it comes to you know, putting this fib fibular nail into a patient?
Dr. Anthony Yi: Yiah, so great question. So what that is is basically it's a device that attaches to the end of the nail. So as you're inserting the nail there there are screws that you put in at the very bottom.
Dr. Anthony Yi: And this adds sort of rotational control the nail so that it doesn't spin. And so there's a targeting guide that attaches to it so that you can accurately. Insert these screws without, and then that takes the guesswork out of it. And the other thing that I didn't mention about it is that they also have.
Dr. Anthony Yi: Holes or screw holes in the nail towards the bottom. Okay. That were engineered to be able to put in [00:11:00] another device such as a screw or something called a tight rope, which I think we'll probably touch on a little bit later. To address any additional injuries on top of the fibula fracture such as.
Dr. Anthony Yi: The assmosis injury or what we talk about as a high ankle sprain. And that can be all done through this, this targeting jig or guide that you mentioned.
Dr. Grant Garcia: Thank you. Well, Anthony, I wanted that segways right into, and we're not gonna get too excited with Will here, but Will's gonna have to control himself.
Dr. Grant Garcia: But it's time, I think, to talk about some of the intern, some of the you know, the ligament repairs and the tight ropes and the internal braces. But talk about this in this sort of repair, you're talking about this tight rope fixation because when I started. We were, you know, I started doing some of this stuff early on but obviously not nearly as advanced as you, but really avoiding that screws, you know, we used to put screws across the synosis and they could break people had hardware issues and then we had these sort of [00:12:00] invent of this sort of tightrope fixation to tighten it down.
Dr. Grant Garcia: Everyone's trying to copy you know, different technology out there, but now you can have a updated, you can get a flock nail. Where it's minimally invasive. You've got nothing on the outside really. And then you have this tight rope that can go to the middle, which you've showed me a few of your patients in, in the office.
Dr. Grant Garcia: And that doesn't need to be removed. And it's much more right. It's, it's, it's more freedom to movement. So it's more natural. Isn't that, isn't that correct? And it's also lower profile.
Dr. Anthony Yi: Will you give us a little information on that? Yiah, I agree completely. So in terms of the, you know, the sysm, there's, there're a series of ligaments that connect the tibia to the fibula together.
Dr. Anthony Yi: And that can tear if the energy is high enough or the injury is bad enough at the same time that there's a fibular fracture. And when it's unstable, those are situations where we repair it or fix it. And you, I'll be honest, it, it's can be quite controversial amongst surgeons, what the best way to fix this is.
Dr. Anthony Yi: Hmm. But I'm, I'm, you know, I'm with you Grant. [00:13:00] Dr. Garcia, you know, tend to lean towards using this device called Tight Rope, which is, Basically, if you imagine two metal buttons and a very, very strong suture in between, and basically what this is used to do is to cinch down the space between the tibia and def fibula so that they're in the correct alignment and to offer some stability to hold those two bones together in the correct position relative to one another.
Dr. Anthony Yi: And what Dr. Garcia mentioned is absolutely correct. You know, there is supposed to be some level of. Normal or what we call physiologic motion between the two bugs in our bodies. So traditionally we've, we use screws that pass through the tibia and, excuse me, th through the fibula and into the tibia and to, to hold those two bones in the correct [00:14:00] position while, while they heal together.
Dr. Anthony Yi: But that does. Eliminate motion, which we originally have some degree of motion in that. So you know, just from a, sort of a conceptual or philosophical standpoint, I, I completely agree with Dr. Garcia. I, I love the idea of putting in what we call flexible fixation. With this tightrope that adds enough stability to let things heal correctly, but also at the same time allows for some motion.
Dr. Anthony Yi: And I think, you know, the. Literature studies also support this in, in showing that we do a better job at getting the alignment of the fibula and the tibia or the sysm when we use the tightrope device. Yiah, and also there can be less complications with it as well. Much less likely to have to take it out than a screw.
Dr. Anthony Yi: For example, Dr. Garcia mentioned screw's breaking. That can happen just because another [00:15:00] testament to the fact that there is supposed to be some motion in between those two bonds. And what if that motion gets if is restricted with a screw, then the stress goes through that screw and it can break.
Dr. Anthony Yi: So, you know, there's a higher chance of need to take screws out. So Yiah, that's, those are my general thoughts with regards to the type of device which, which I heavily lean, encourage using my patients.
Dr. Grant Garcia: And then for the, and for the viewers this is a device that we use a lot in the acl. And for a lot of other ligaments that we do, there's sort of, it's a self-locking device, so as you pull it, it pulls it up and it locks it in there.
Dr. Grant Garcia: But then you can adjust it, which is really nice. So if you fix one side on like an ACL l you can tighten the other side and you can titrate things up and we can go over the implants another time on the ACL side of things for the tightrope. But nonetheless, this is just another, another great piece of advice that
Dr. Anthony Yi: sort of was, it's,
Dr. Grant Garcia: it's the same technology, but it's another way of using it.
Dr. Grant Garcia: Which is always great, especially, you know, this is another there's different type of proprietary places that make this, but this device is [00:16:00] pretty impressive. So, on this topic, obviously high ankle sprains are a huge discussion topic and we're gonna skip a little bit ahead, but I kind of wanna keep on with this tight rope synosis.
Dr. Grant Garcia: So the viewers can understand it cuz the idea of the sym is confusing to people. And everyone hears high ankle sprains are here. Listen, that's the one you don't want. You wanna have a regular ankle sprain. And for, you know, layman hearing this, you know, we've heard of, you know, you have a couple big athletes that have this, obviously one didn't have surgery with Mahomes.
Dr. Grant Garcia: But you know what happens These, through these patients
Dr. Anthony Yi: with high ankles sprains, they're a lot different than a regular ankle sprain, right? Yiah, absolutely. So that's a great question. So you can, you know, think of it at one area of the sprain being a high ankle sprain, another area being a low ankle sprain.
Dr. Anthony Yi: No, a low ankle sprain is that classic twist of the ankle. And you know, by and large, people don't necessarily need surgery for it. You know, take it easy for a few days up to a few weeks, and largely starting to ease back into the swing of things [00:17:00] thereafter. And that's, That's lower down. So at the tip of the fibula bone, that bump on the outside part of your ankle on the pinky to side so that there's a ligament that runs right along that region.
Dr. Anthony Yi: And that ligament can get injured or there can be a partial tear, which is, which is the lower ankle sprain. And then the high ankle sprain is more of the injury that I mentioned. Before, so there's a series of several ligaments that attach between the tibia and the fibula and hold those two bones in the correct position.
Dr. Anthony Yi: And this is often due to a pretty violent, twisting type injury with the energy sort of traveling all the way up through that space between the tibia and fibula. And there can be a lot of different variations in terms of which li, which of those ligaments are injured and how severely those ligaments are injured.
Dr. Anthony Yi: And so the, the key to treating this [00:18:00] and determining if a patient might need surgery or not, is to determine if it's a stable injury, meaning that there's not abnormal motion that the relationship between the bones are, is, is, is still preserved or. Is it an unstable injury? Meaning is there too much motion going on between those two bones now and which which is gonna lead to problems in terms of pain, not being able to use that ankle as well as you'd like to be.
Dr. Anthony Yi: And also, Concerns in the long term about developing arthritis or wearing away the cartilage in the, in, in the long term. And so, you know, some famous athletes, for example, in the nfl like Tua and you know, Tony Pilar had recently had unstable high ankle sprains for which they underwent surgery.
Dr. Anthony Yi: And, and for these, you can use that same device that I mentioned, the, the tightrope to basically [00:19:00] restore the relationship between those two bones and to restore the stability between those get those, get those, and get that high ankle strain to, to heal properly. And again, this is a little,
Dr. Grant Garcia: you know, is a better alternative, right to the old school screws in doing them.
Dr. Grant Garcia: And then, you know, sometimes, right, you add, you can add more than one if you really need to, which is nice. You can it without having to add more screws or other
Dr. Anthony Yi: fixations. Is that correct? Absolutely. So oftentimes, you know, again, this can vary from surgeon to to surgeon, but in the case of, you know, an isolated high ankle sprain you know, there's a lot of different variations of injuries that this can happen in.
Dr. Anthony Yi: But oftentimes I'm, I'm using two. Two of these devices to have to have enough stability between those two bones and to get those, get, if you heal properly.
Dr. Grant Garcia: I, I know Will's thinking this, but would you ever consider this in a high level [00:20:00] athlete that's in the playoffs that wants to get back?
Dr. Grant Garcia: Or what is the timeline? You know, someone's on the fence like ma, like Mahomes, he pushed through this. Right? But let's say you can't push through it. Would you ever consider doing this? Like unless they first round the playoffs knowing I'm gonna get em ready for the Super Bowl? Or is that not
Dr. Anthony Yi: realistic?
Dr. Anthony Yi: It, it can happen. So I mean, I might, no one's
Dr. Grant Garcia: gonna, no one's gonna hold you to, no one's gonna hold you to this. I'm
Dr. Anthony Yi: just curious. It's, it's certainly possible, I think in, in that timeline. So I may be wrong about this, but I believe Terrell Owens actually had this injury. And came back.
Dr. Anthony Yi: He, I think it happened in the playoffs and he was able to get back for their run.
Will Sanchez: Yiah, that's why he plaYid with the Philadelphia Eagles. Wikipedia. Yiah. He plaYid he plaYid in the Super Bowl with that injury with the Philadelphia Eagles, in fact plaYid really, really well. I have a quick question here.
Will Sanchez: Is this something that, this procedure, since you're, you're pretty much, you know, [00:21:00] Putting, putting a hold through the fibula to the tibia with that, you know, with this tightrope cord and you're using your suture. And first off, just for the listening audience, a couple questions. One, is this a quick procedure?
Will Sanchez: So we'll start there.
Dr. Anthony Yi: In, in terms of the actual insertion of the tightrope, actually very quick. Yiah. So basically I use an x-ray machine in the operating room at the same time to make sure that I'm happy with exactly where I'm putting this device. And then I, I, I drill across, Yip. Using a, a appropriate drill bit, and then I put the D device across and sync it down.
Dr. Anthony Yi: It's, it's very quick. Very
Will Sanchez: quick. And then is this something that you can Do you have to connect to another piece of equipment? Like let's say if you had a metal piece on the fibula side or something like that, or is this something that you can attach to the fibula to the tibia at the same [00:22:00] time?
Will Sanchez: Or does this require another piece of equipment to hold it in place?
Dr. Anthony Yi: Great question. You can use this device in isolation. Okay. Or you can use it for example, with through a plate so that button can sit directly on bone or you know, there are different plates that can accommodate that.
Dr. Anthony Yi: That button as well, so it fits nicely in a hole on the plate as well. So, for example, if you're fixing a fracture with a plate and screws and you, you leave one of those screw holes open to be able to put this tightrope through it, you can do that as well. Yiah.
Dr. Grant Garcia: So, I'm gonna segue you cuz this is a great talk, but I will not be missing Will's favorite topic here.
Dr. Grant Garcia: So we are going to, I want to talk to you about something that probably, I think that I, I think all of us see this more than anybody. I mean, you all have a friend that [00:23:00] sprained their ankle. We've all seen ankle sprains. We talked about high ankle sprain. But the low ankle sprains, I think are a lot more common.
Dr. Grant Garcia: You know, any, if you, if you don't have any friends, if you don't know a single person here that's had an ankle spraining. So it's really important for us to learn about this cuz we see tons of these, but you know, we've, we've heard about Bross and Bristow and others sort of ways to sort of fix this in brostrom procedures, et cetera.
Dr. Grant Garcia: But there's this newer procedure, which I love talking about and I know Will does too with internal brace. And really, you know, we do a lot. We talked about this in the knee, we talked about this in the elbow, but, so how does the internal brace help with instability? And is how is this a game changer for you in your practice?
Dr. Grant Garcia: Anthony, especially with athletes and young kids. And I've sent you some few patients you've done it on that were some of my Mercer Island athletes. So tell me a
Dr. Anthony Yi: little bit more. Yiah, so this absolutely is a game changer. So the internal brace, as you know is made by a specific company. No, I don't have any affiliation with them, but Arthrex.
Dr. Anthony Yi: So they [00:24:00] have come up with this awesome device that is made of a very, very heavy suture, and it's. Basically something that can augment or protect your repair of a ligament so that you can get patients going very quickly. So with the low ankle sprain or just the traditional ankle sprain, vast majority of patients will make a nice full recovery and get back to doing what they need to or want to do.
Dr. Anthony Yi: But there is a small percentage of patients. That unfortunately develop what we call chronic ankle instability, where they can't trust their ankle. They're constantly twisting and turning their pa their ankles. I just had a patient last week who a very young athlete who unfortunately even just walking on flat, even surfaces and twist their ankle because their ankle is so, so loose from having had so many ankle sprains in the [00:25:00] past.
Dr. Anthony Yi: So in patients like this I love using this internal brace because it protects the ligament repair and I can get them going very quickly. So I generally have them start walking at two weeks after surgery and starting PT right away.
Dr. Grant Garcia: So And how is that different than
Dr. Anthony Yi: before? So, Yiah, traditionally, oftentimes not, you know, keeping patients off of it for four, even six weeks.
Dr. Anthony Yi: So it's a, it's a full month. You know, earlier there was a recent study in foot and Ankle International that looked at a military population and and looked at these patients with chronic ankle and stability using the internal brace, and they found that they could get them back to activity a full month after.
Dr. Anthony Yi: And if you're talking about an in season athlete, that's a, that's a. And I think
Dr. Grant Garcia: I've heard you do this, some [00:26:00] of this with scope stuff. I mean, I've never seen someone do that before. Tell me about that and, you know, what's the, how does that add the benefit of what you can do with these sort of, these things and what other, what
Dr. Anthony Yi: things are associated with this too?
Dr. Anthony Yi: Absolutely. So one of the techniques I learned from one of my mentors, Chris Miller out in Boston was doing this procedure or was called the Brostrom procedure, which is a reconstruction. Of the lateral ligaments that are injured that can lead to this type of chronic instability. What's to do, learned how I learned how to do it through the scope.
Dr. Anthony Yi: So arthroscopy, as you know, is using small cameras through very, very small incisions to look inside an ankle joint. And you can put, use small instruments to do all sorts of things including this procedure through the scope. So oftentimes when someone has ankle instability, They're constantly turning their ankle.
Dr. Anthony Yi: There can be a lot of [00:27:00] issues in the ankle joint itself. So it's fairly standard to also do an ankle out of thoroscopy procedure at the same time to make sure that we're not missing anything like a cartilage injury that needs to be treated. And through the same incisions you can do a, a brost procedure or an arthroscopic brost procedure.
Dr. Anthony Yi: And. You know, one of the, you know, really cool Things about being able to do it this way is that avoiding a larger incision where you're worrying about the wound not healing and then it just gives you that much more confidence in getting patients going, going sooner
Dr. Grant Garcia: and, and will, I'm gonna chime in there.
Dr. Grant Garcia: You're, you know, you heard a lot of Anthony or Dr. Yi mentioned a lot of times the word incision, so you don't hear me mention that very often, and that's because I do knee, shoulder, and elbow. And those patients tend to have very little wound issues,
Dr. Anthony Yi: but, but what, what
Dr. Grant Garcia: Dr. Yi has to deal with on a daily basis is that when you have foot stuff, it doesn't heal as [00:28:00] well and it's a much higher risk of not healing.
Dr. Grant Garcia: So everything they're doing is not only can I get the athlete back faster, can I get my standard recreational back faster? Can I do it more minimally invasive? It's can I make the incisions as small as possible so I have the highest chance of them healing perfectly? Would you agree with
Dr. Anthony Yi: that, Dr. Yi? Yiah, absolutely.
Dr. Anthony Yi: You know, I. You know, the foot and ankle surgeons have somewhat of a disa disadvantage in terms of the fact that, you know, the foot and ankle is the furthest thing away from the heart. So we, you know, blood flow. Tho those are all very real considerations. We need good blood flow to be able to heal.
Dr. Anthony Yi: Wounds to prevent infections. So definitely, definitely a very, very important thing to consider.
Will Sanchez: Dr. Yuri. Is there any determining factors where you say, you know, this individual is maybe too young, or there's a certain situation there where you're, you have to make a determination that at this moment this course of action is [00:29:00] not appropriate for this patient.
Will Sanchez: Is there anything. Along those lines that you can
Dr. Anthony Yi: speak to? Yiah, absolutely. That's a great question. So in terms of age, one of the things that we always keep in mind is, Orthopedic surgeons is we, we have something called skeletal maturity. Each of our bones in the body have a different time at which they start, you know, developing and when they ossify and when they, when they mature.
Dr. Anthony Yi: And so we have growth plates at the ends of bones usually. And one consideration is if that growth plate is still open, or if it's closed, if it's still open, you know, we generally do not want to try to disturb that growth plate or do a procedure that might injure it because it can prematurely injure it or shut it down, which can cause things like.
Dr. Anthony Yi: Slowing of the growth of that bone or [00:30:00] even complete stopping of the growth of that bone, which can lead to, you know, discrepancies in the length of different bones or even what we call angular deformities. Where, for example, down, down by the ankle there's both the tibia or the shin bone and that side skinny bone and def fibula.
Dr. Anthony Yi: And let's say that the fibula bone growth plate got injured and the tibia wasn't. Mm-hmm. And the tibia continues growing. You can have this. Unnatural angle or, or turn to your ankle. So Yiah, absolutely. So these are all, all considerations. In terms of, you know, so you may want, you may need to alter your technique or consider a different procedure or just as you mentioned, holding off on a procedure if, if in certain situations.
Dr. Grant Garcia: Great. Great. Well, Dr. Yi, in essence of time, I wanna ask you one more thing. I know Will wants to chime in a few more. But what do you see sort of as the sort of [00:31:00] future for foot and ankle? I mean, we've already heard about some things you're doing that are really unique to the area and that, you know, you're bringing arthroscopy in more levels of the foot and ankle in the level that I've never seen before, which is awesome.
Dr. Grant Garcia: And you're treating arthroscopy with ankle fractures and. With, you know, ankle sprains now and other different levels of arthroscopy and minimally invasive procedures. But so what's on the, what do you kind of see as the future? What is the sort of the couple main things you're, that you're looking forward to seeing in the future for our audience and they can
Dr. Anthony Yi: hear about it?
Dr. Anthony Yi: So, I think one of the really exciting things I'm passionate about and things I'm really excited about in terms of foot ankle surgery is seeing how far we can take this concept of minimally invasive surgery. So far I feel like we're just at the tip of the iceberg. So, you know, as you know, the concept of minimally invasive surgery is performing, you know, safe, effective surgery through incisions that are as small as possible.
Dr. Anthony Yi: So whether that means for, you know, the ankle fractures we talked about, using [00:32:00] that. Then figure their nail through smaller incisions or doing the bro procedure through the scope or fixing a bunion through tiny incisions that, you know, just need a single one or two stitches using a spec special burr or, you know, repairing an Achilles through a very small.
Dr. Anthony Yi: One and a half or to two centimeter incision so that we can really, really try to minimize complications like wound complications or infections, decreased pain, and get athletes and or for all patients for that matter back on their feet as soon as possible. That, that's one thing that I'm personally really excited about in terms of the future.
Dr. Anthony Yi: And then some, some another area within foot and ankle that I'm also looking forward to seeing developments in cartilage restoration. So I briefly mentioned, you know, cartilage injuries earlier. You know, we have some [00:33:00] techniques in our toolbox that have worked fairly well so far, but I think there are some other techniques.
Dr. Anthony Yi: I know Dr. Garcia is, is our you know, expert here in Seattle on, on doing the Macy procedure. And, and that's been very successful around an knee. And that's starting to become a tool in our toolbox for the ankle as well. It has not Yit been approved by the fda, specifically for the ankle, but my thoughts are that it probably will in the very near future based on, you know, the studies that I see and then also colleagues that do this a lot.
Dr. Anthony Yi: For example, I have a colleague in the, in the Army who they have less restrictions when it comes to, you know, getting things approved that are difficult to get approved through you know, private, private or civilian insurance. So, you know, you know it's one of the other areas that I'm, I'm, I'm very looking very much [00:34:00] forward to seeing our develop.
Dr. Grant Garcia: Awesome. Well, thank you so much Dr. Yi. This is, I'm looking forward to seeing more of your cartilage stuff. As you know, I do a lot of it for the knee, but there's just less. Of it approved for the ankle. And so it's good you're pushing the envelope and I know you're working with Macy team to try to figure out ways to do more of that and other cartilage things.
Dr. Grant Garcia: So hopefully our patients, well I know our patients are gonna benefit, benefit already from your minimum invasive impressive techniques. So thank you for joining us and I'm sure Will has a few more things to add, but this has been fantastic and I think all the patients Seattle are happy to have you here.
Dr. Grant Garcia: So, and I know I am, so thank you.
Dr. Anthony Yi: Well, thanks for having me. Yiah,
Will Sanchez: I'll wrap it up. I know we're going a little bit long. I, I couldn't agree more. As far as, you know, hearing a doctor saying that we want to have smaller incisions and less invasive and things like that, so those are all key words that every patient wants to hear, right?
Will Sanchez: Because we want you to, Have, do less [00:35:00] to our body, but fix us faster and get us up and going. So these are all key things that people want to hear from our side of the of the table. So that's a great thing. And before I let you go, Dr. Yi, just to remind everybody, Dr. Yi he's the orthopedic surgeon, foot ankle specialist.
Will Sanchez: Out of orthopedic specialists of Seattle. So please look him up. There's, you can check him out on his website. He has a great LinkedIn page. And I know if I'm having foot and ankle issues, I definitely want to reach out to Dr. Yi before we let you go. I know I have a Harvard man on one end and a Penn man on the other.
Will Sanchez: So let's just get right to it and just have a little fun here. Dr. Yi, do you know who won the football game this past season between the two of you
Dr. Anthony Yi: guys? Oh man.
Dr. Grant Garcia: This is not good. This is not good. I would, I would,
Dr. Anthony Yi: I would assume Harvard, I would assume Harvard. [00:36:00]
Will Sanchez: Harvard won 37 to 14 ruin Penn's chances at a Ivy League.
Will Sanchez: Title at the end of the Yiar. That is my gift to you, Dr. Yi, for spending some time with us. Thank you very much. We really appreciate it. Dr. Garcia, I apologize for that. You know, we will find a way for you to take a shot at me somewhere else. I'm still waiting for, for me to perform internal brace. Maybe Dr.
Will Sanchez: Yi let me come in and, and and take care of that. So, Once again, Dr. Yi, we really appreciate your time. We appreciate your knowledge on all the subject matters that we talked about today. You have a great night.
Dr. Anthony Yi: Hey, thank you so much. I really appreciate it. Had a lot of fun tonight. Thank you. Take care.
Dr. Anthony Yi: Dr.
Will Sanchez: Garcia, man. Awesome. That, that was a lot of fun. It was great to have Dr. Yi on. What are your last thoughts on the evening as we wrap up our show and just having someone like Dr. Yi on?
Dr. Grant Garcia: Well, I'm just excited that we have this [00:37:00] platform now that patients can. Get more of what they ask for. You know, it is more sports, but now we can expand it.
Dr. Grant Garcia: You know, we have so much more we're gonna be doing with this show. We're getting requests, we're getting people messaging me. I'm hearing from my own patients that they love hearing the type of topics we're talking about. And again, if you have any patient, if any patients have any requests, anybody has any requests, let us know.
Dr. Grant Garcia: We're, I mean, we have a lot of things in store. We have a lot more guests. We're gonna have company stuff. We may even get a chance to have some of the arthrex and other company teams on here to learn more stuff. And I know Will's gonna ask a lot of good questions, as he always does. So I'm really excited about it.
Dr. Grant Garcia: Subscribe to us. We have another special guest coming up in a few months, a few weeks with some potential NFL ties. So I think it'll be really exciting and there's a lot more in store. We're not even, we haven't even touched the tip of the iceberg with this show, so we're really excited.
Will Sanchez: Yiah, it was a great show.
Will Sanchez: I mean, the fact that we were able to talk about the Fibular nail and obviously minimally invasive and the targeting guide and the push lock. Anchors and how that has you know, [00:38:00] resulted on you know, different athletes and different people. And obviously my favorite internal brace and just kinda speeding up the process and getting you out there and rehabbing four weeks earlier and, you know, and just kind of dealing with all that stuff.
Will Sanchez: We talked about the tight rope and how it's affected high profile athletes and, you know, the, the. The cool kind of part of that from drilling a hole through your fibula to the tibia. And it's great information for us, right, because we can talk about this, but the patients are the ones that are gonna benefit from the new technology, everything that that's kind of happening.
Will Sanchez: So as we wrap it up, My little question to you is, who has more Ivy League titles when it comes to football? Is it Penn or Harvard? Dr. Garcia?
Dr. Grant Garcia: I think it's Penn, actually. Penn needs to be really good at football, if I remember correctly. Maybe I'm wrong though, mostly.
Will Sanchez: Harvard has 17 Ivy League championships.
Will Sanchez: Penn has 18, 18 Ivy [00:39:00] League championships. So see, look. Oh, finally got one. Right. There you go, baby. Okay, so just because you lost this this past winter, don't worry about it. You can still hold. Hold over Dr. Yi's. Had the extra championship. Let's go Penn. Let's go Quakers. And once again, remind everybody, check out Dr.
Will Sanchez: Grant Garcia. He's. Our orthopedic surgeon is sports medicine specialist. Check us out at sportsdoctalk.com. Email us sports doc talk podcast gmail.com. You can find all that stuff on our website. Just go to sports.talk.com. You'll find all that stuff. Dr. Garcia, it's always a pleasure. Thank you for taking some time to be with us this evening to lend great information for bringing Dr.
Will Sanchez: Yi on. I had a great time. Me too. Thanks
Dr. Grant Garcia: so much. It's always fun. Audio Transcript
The New Aging Athlete

Will Sanchez: [00:00:00] Welcome everyone, and thank you for listening to sports.talk. I'm Will Sanchez, along with Dr. Grant Garcia. Check him out@grantgarciamd.com. Please, please, please, please, we want to hear from you, so reach out to us at sportsdoctalk. Podcast gmail.com and the reason I'm kind of jumping into the whole Gmail and you know, having you guys reach out to us and we love this communication.
Will Sanchez: Before we get into that, Dr. Garcia, welcome to the show and really you presented this show because someone came up to you. And requested it. Tell us a little bit more about that.
Dr. Grant Garcia: So you know, we also have the ww sportsdoctalk dot com as well, so you can, there's a whole link you can add in what you wanna talk to Doctor or will about and as well add to your episode.
Dr. Grant Garcia: So it's a pretty easy interface. And so Gmail or that interface works out great. We actually have another request, which eventually we're gonna get [00:01:00] to. But this topic is a good friend of mine Nina Thatcher. I wanna give her a big shout out. But so she is a former Iron Man, or Iron Woman, you could say.
Dr. Grant Garcia: And she is an extremely athletic individual, a great person. One of my good friends and she had heard the podcast and seen some of my posts on LinkedIn, et cetera, and was asking, you know, what can we. Do. As you know, as we get older and as we age to keep doing the things that we want to do, and we've talked about this a little bit for professional athletes, but not in the respect of sort of a recreational athlete.
Dr. Grant Garcia: And so this brought up a good topic of not only Ironman event. And a lot of her friends are iron ironmen contenders or qualifiers or finishers. But really how do we keep athletes going? How do we keep the aging athlete at the level we want them to be? And, you know, there's certain tricks that I've talked about in my surgical aspects, but there's a whole nother gamut of technology.
Dr. Grant Garcia: And we're gonna try to do our best to get into that today. So,[00:02:00]
Will Sanchez: Real quick for our listening audience, if you don't know what this event is, this Ironman event no disrespect, but you have to be a little bit of a lunatic to do this stuff. It's a 2.4 mile swim, 112 mile bike ride, and then you have a 26.2 mile run.
Will Sanchez: So you're running a marathon and then you have to. Complete it within the 17 hours and there's cutoff times for each leg. So if you've taken too long on the swim or the bike ride, you don't even get to compete on the mile run. So there's all of these different obstacles. I remember I did a. AIDS ride event from New York up to Boston and that first day I rode 120 miles.
Will Sanchez: I stopped about four or five times to go into the medic tent to get my back check. I swear I'm not even joking. And this is Young Will Sanchez feeling groovy and training and I couldn't even move. I got there, it was pitch black dark [00:03:00] at our first leg, 120 miles later, and I just felt. Awful. I was like, I would never do this again.
Will Sanchez: It was a great cause raising money for aids, but what I did to my body, I don't, I still don't think I've recovered. Dr. Garcia, when you think of something this enormous, what's the first thing that goes through your head?
Dr. Grant Garcia: Pain. Lots of pain and per perseverance. But you know what, you know these, you know my friend people I know that do this, it's a different mindset.
Dr. Grant Garcia: They're different. They're different level. Of sort of both mental and physical. I mean, these are the people that are in the water swimming at six in the morning consistently, even as they're in their twenties, thirties, et cetera. You know, they don't give up when they were done in college. Like they just keep going.
Dr. Grant Garcia: Or some people find their new passion. You know, you hear all these stories of somebody that goes and starts doing these in their late thirties to forties. And it. And being a former athlete, taking care of athletes, taking care of Ironman, taking care of professional athletes, you name it, [00:04:00] you know they, there's a mental aspect to it that is unteachable and you either have or you don't, or you develop and you don't.
Dr. Grant Garcia: But it's really hard to tell someone to have that mindset. But my job and our job obviously today is to talk about the things that you can't, that you can help with. What are the additives to help with this, you know, the standard injuries you have with Ironman athletes, you have the standard sort of tendonitis.
Dr. Grant Garcia: You have stress fractures a lot of times of defeat. And we know a lot of iron men that have gotten these injuries plantar fasciitis. And we're gonna be hopefully in for a treat next month with my partner, Dr. Anthony. Ye's. Gonna talk a little bit about some of these lower extremity injuries. But these overuse injuries are really important to understand.
Dr. Grant Garcia: And how can we as. Physicians or as the population better understand the treatments available and what is the future. Because really we're, we're on this cutting edge of regenerative medicine, and I think that's really important for us to understand like what's the next step. And obviously be careful because.
Dr. Grant Garcia: You know, [00:05:00] there's, there's different levels and the word regenerative is always something you gotta be cautious of. But how can we have this aging athlete? How can we can keep them going? And that's really important.
Will Sanchez: You know, when we talk about the aging athlete for you, you know, sports fans out there, we know a couple right off the top of the hits, right?
Will Sanchez: LeBron James at 38 years old, it is a specimen, right? Tom Brady just retired. We'll figure out if he's gonna stay retired, but he's an amazing specimen. But a lot of these athletes that are performing at a high level that have been in the pro, in the pros for so long, usually have some kind of routine that's helping them along with that.
Will Sanchez: Right? So for LeBron, it's the weight training, the yoga, the Pilates. He has the. The, his core workout is this, is all of this effort to keep that, that body fine tuned and ready. Right? Tom Brady talks about, you know, he has a pre-workout [00:06:00] pliability then he has functional strength conditioning, then he goes back to pliability.
Will Sanchez: So there's all of these things that we are, we're learning more more and more each day that we need to do certain things to kind of, Give our body a chance to even perform. As you get older, what are some of the things that you think about that as you get older, some of the things that we should be keying in not only to perform and to, whether it's, you know, play tennis or doing anything else and just kind of enjoy life, but to really kind of keep the body going and be functional in your day in and day out activities.
Dr. Grant Garcia: I think you hit on it a few times. I mean, you brought it up with every athlete you just mentioned. It's adaptability. They were doing different things at the end of their careers than they were at the beginning, but they're performing at the same level. They've adapted to their age, they've adapted to their athleticism.
Dr. Grant Garcia: They've adapted the level, you know, You [00:07:00] can't be fif, you know, you've seen these videos on Instagram or other things. People lifting it appropriately and injuring themselves and they're like in their young, you know, early fif, early teens, late twenties, you know, those guys aren't doing that. You know, they're not just going up and lifting as much weight as possible.
Dr. Grant Garcia: They're doing everything in their possibility to try to maximize their athletic ability, but in a different way. You know, we've seen the evolution of fitness, right? It was before it used to be sort of all a, you know, constantly lift, lift, lift, lift, lift. Heavy weights, protein, protein, creatine, you name it, to the point now where it's like lean muscle mass, high intensity training.
Dr. Grant Garcia: Plyometrics with a combination of yoga, flexibility, aquatics training, you know, those things are all really important and constantly keeping your body, you know, you want, the things that are in, are in bad shape to get a break and you want the things that are in good shape to take the brunt and be able to get back you know, be able to get more exercise in those areas.
Dr. Grant Garcia: And so I think that's really important for these athletes and that's really [00:08:00] the major thing. And then, you know, I think it's time for us to kind of jump into the next topics. You know, I think we've talked about this before and you guys can see on our previous podcast earlier on, you know, the aging athlete, at least from that standpoint, from the professional athletes, important.
Dr. Grant Garcia: But what about the recreation athletes? What about the technology coming out? You know, this is really important. I think one of the biggest. Advances is regenerative medicine. I don't know if you have any comments on this and what you've heard. Cause it's always good to hear, you know, both sides of the story as to what's sort of the, the next thing up there because regenerative medicine is a hot topic and that everyone is talking about it.
Will Sanchez: Well, I do have a question because I'm hoping that. This is something that's going to help me in the future because I've had issues in the past and I, knock on wood, it hasn't been as bad the last year, but I was getting these, this injury about every. Two to three to four months. And that was with my perforance.
Will Sanchez: And I went to a doctor and at the time he was like, yep, man, you've got some arthritis, [00:09:00] you've got some injuries. You know, things had piled up over the years. I, you know, I played this, that, and everything else. And he was, and at the time he was like, we just, we gotta get to a point where we could get some stem cells and do some things and, you know, maybe we can help your, help the way you're feeling.
Will Sanchez: Well, I have still not had that treatment yet. You know, so when it comes to something like that, will that be beneficial to me or apply? And if so, what is the timeline that that can happen? Because I'm gonna make an appointment tomorrow.
Dr. Grant Garcia: So, you know, I think obviously we get into a broad spectrum. So regenerative medicine is the idea.
Dr. Grant Garcia: Can we find a way with medical technology to regenerate parts of the body? Or to protect the body. Yeah. And from an orthopedic standpoint, it's really important. You know, we're looking for the holy grill. We've talked about this before. You know, we are starting to, to try different stem cells for tr treatments of, you know, early arthritic [00:10:00] changes.
Dr. Grant Garcia: But we don't have a lot of data yet. You know, do we use, there's fat stem cells, we have stem cells from synovial joints, we have stem cells from amniotic fluid again. We're not selling these things right now as an orthopedic group. Yeah. Cause we're still on the verge of trying to figure them out. They're still in sort of testing phases.
Dr. Grant Garcia: Obviously you gotta be careful when people are selling stem cells at, you know, five, $10,000 a pop telling you it's gonna change your life. And so we gotta be careful about that. But there are other fields where it's, they're testing it. I mean there multiple sclerosis is a big one. ALS brain injuries.
Dr. Grant Garcia: Yeah. A big one for us is orthopedics is spinal cord injuries. And they're trying to look at ways that we can find a way to regenerate stem cells to get people back to what they're doing. And can we do that with a combination of other medicines? You know, you've seen these impressive gene splicing options.
Dr. Grant Garcia: You know, I just was reading about Dechen Muscular Dystrophy, which is a really horrible disease Yeah. Where you heard about sickle cell and they've spliced genes to get people better again. I mean, they're treating all sorts of genes with this sort of [00:11:00] regenerative medicine. Awesome. And looking at aging, I mean, Not only are we treating diseases or treating injuries, but can we reduce or turn around aging with these things called tel.
Dr. Grant Garcia: It's sort of the end of your chromosomes. That's sort of as the longer you have that maybe you have more time in this planet or not. And finding ways to reduce ways to have those be damaged. And so, You know, I think we're, we're not there yet. But that idea of regenerative medicine is a very hot topic.
Dr. Grant Garcia: And I think that this plus AI in the next 10 years is gonna be one of the, you know, the cutting edge fields to treat diseases that are really bad and to treat diseases that are not as bad. You know, no offense to your hip arthritis, but obviously it's very important. They wanna treat that, but can we also save people's lives?
Dr. Grant Garcia: And I think that we're gonna see that this, this stem cell thing, it may not be what we think it is now. You know, we think of stem cells as like you take some juice outta your body, just mix it around and get the new stem cells or something that we have to develop in the lab, you know, with other techniques.
Dr. Grant Garcia: Or is there gonna be an epiphany where it's designed by computers and computers [00:12:00] figured out? We're, we're, we're getting there and we're confident. It's one of the hottest fields. Everyone wants it happen. We all want a magic shot. I have patients all the time that ask for this, and we're getting closer each day, but it's just gonna take more time and unfortunately Will, there's no appointment for you at this point?
Dr. Grant Garcia: Oh darn. As soon as there is, you know, I'll be, you know, I'll be telling you right away. Yeah. I mean,
Will Sanchez: because really the, the paraform is pain. I thought it was in my hip and everything that was going on, and then I had some tests done and really it's coming from my spine, so I'm getting this. Arthritis in, when it gets inflamed in my spine and it's making me feel like I'm having the pain and the perforance and I'm stretching, I'm doing all this stuff, which obviously is, is beneficial, but when this flares up, I mean, I can't move.
Will Sanchez: I pretty much amusing my hands. To lift up my thigh. To swing my leg around. Right. And I'm not the only one. Everyone's kind of going through it. You, you mentioned sickle cell. My niece and nephew were born with sickle cell and they've gone through, as little kids have gone through, just, [00:13:00] you know, the worst as if, you know, if you know what sickle cell is, you know, it, it is something that is just, it's really, really difficult to deal with.
Will Sanchez: And My nephew already had to have surgery. Normally they want their surgery at five years old, but he was having so many issues that he had to have it early on. And now the, the younger sister is now showing complications from it as well. So without, you know, getting into all the. Extra details.
Will Sanchez: Really, this is something that when you say regenerative medicine and the goals and things like that for everyone, Ms. Als and everyone else, I mean, this is, this has gotta be a big one. And I, you know, the, you're on the clock, brother. You, you better go figure this out. You go everywhere and you do all these tests, so you're no pressure, but you're on the clock.
Will Sanchez: Listen, let's move on. Because it really is, it's a, it's a. Topic that we can really kind of keep on and discussing because there's so many different aspects of it. We talk about, and I'm wearing it right now. So I [00:14:00] got up this morning, I, I did some stretching, I grabbed some kettlebells, I did some, some swings, some snatches, things like that.
Will Sanchez: I did a timer and then I put in my average heart rate what was the highest heart rate. I have this information now on my wrist, so when we talk about. All of these different technologies, these wearable technologies that we've already done a show on, but how it plays a part for these athletes, especially the Asian athlete, what is something that they should particularly pay attention to if you have a, a wearable technology as far as, you know, maybe keeping themselves healthy or not, you know, trying to avoid injury.
Dr. Grant Garcia: Well, I think, you know, think about back this like 10 years ago, you wanted an heart rate monitor, you strapped it on your chest, you got very little readings. I hated those
Will Sanchez: things. Heart, by the way. Those things were so annoying. I know. And they're shaved,
Dr. Grant Garcia: they're not fun. No. So they, so now we have, [00:15:00] you know, all of these different monitors and we'll talk about a couple we didn't talk about before.
Dr. Grant Garcia: Yeah. Let's go through kind of each aspect of it, right? So you have. The simplest thing with is the Apple Watch. And I hate to say simple, but you know, it's a pretty common piece of technology. You kind of put it on your wrist and that's it, and it could do most of the stuff you want. And they keep advancing in every version, you know, soon they're just gonna tell us what we need to do.
Dr. Grant Garcia: They're like, work out harder, you know, they're gonna be able to advance all those things. Great. And so Mac now? Yes, precisely. So basically now, you know, as an athlete, You can see, you know, before when I didn't have an Apple Watch, I had no idea what my high heart rate was. Hmm. And I was like, used to say as a, as a younger person, why does that matter?
Dr. Grant Garcia: But now I know, you know, if I do a hit workout and I only get to one 30, I'm like, did I really work that hard today? If I go for a run and I get to one 60 and I feel pretty good, I'm like, I feel like I got my, my level at. But if I get to one 70 and start feeling not feeling very good, I maybe pushed it too hard and so I can adjust my workouts based off that level as someone who really likes.
Dr. Grant Garcia: I'm an analytical guy, [00:16:00] obviously we know a little dorky being a doctor, but nonetheless, you know, I find it important for me and people who, you know, these athletes, like I talked about, these ironmen. These people that are doing all the time, like they're calculating. They have all their stats. They know what they do.
Dr. Grant Garcia: You know, we talked about Verlander before, you know, he knows his, he knows each speed pitch he has, you know, they have an encyclopedia in their heads for their bodies. Yeah. And that helps him get, that's helps these, some of these players as Verlander is a great example. Of being at the top of their game for so long.
Dr. Grant Garcia: You know, I can tell you right now, I can show you. I can tell you right now, if you ask LeBron James what his top bench press was, his speed, his vertical, and everything else, and every year he would know with without a doubt. Yeah. He would've all the numbers in his head because that's what he does. And same with Tom Brady.
Dr. Grant Garcia: You know, they have all their physical stats in their head and they know they go for goals and it's personal best. Not always against everybody else. We know they're competitive, but really it's personal goals that get you to the next level. And these Apple, these watches and things like that, they can monitor those and get you to that next level or protect you because you know you're overdoing it [00:17:00] because our bodies as being competitive athletes.
Dr. Grant Garcia: You know, that you can hurt yourself. And so I think that's, I think that's an incredibly important part of the wearable technology. In addition, I don't wanna jump in too much, but into sleep as well. You know, we are so focused on the daytime activities, right. We always wanna do more. I am a terrible culprit of this.
Dr. Grant Garcia: Yeah. And honestly, until about a year and a half ago, I was really bad at sleep. Maybe even two years ago, I would, my resident, I would just work, work, work, barely try to get away without sleep, try to do two or three rounds of coffee a day. Cause I was like, I'm I gotta go. I gotta, I gotta make, do a better, I gotta get better.
Dr. Grant Garcia: I gotta keep working. Yeah. And until I got the watch and realized that I was doing a very bad job of sleeping and when I slept a lot, all of a sudden my memory came back and I felt more alert and I was actually more productive. It was, I mean, I remember falling asleep in class as a kid cause I was so tired from swimming and working and getting ready for medical school and everything else.
Dr. Grant Garcia: And I've finally taken it on my own as thankfully. The life helped a lot with that, with getting back to sleeping. Yeah. But [00:18:00] as an athlete, you and as any pet professional, sleep is essential. And if you're skipping on sleep, you might as well skip your workouts cuz you're just doing yourself a disservice.
Will Sanchez: Yeah, it's a great point because when you look at all the training, right, whether it's, you know, we talked about Brady and LeBron and, you know, even Mark Wahlberg, right? They, they all talk about, you know, the rock. I've seen his training. There's like sleep, get up early. Workout, eat, supplements, nap, workout, sleep, nap.
Will Sanchez: And so the sleep is an integral part along with it. And I'm terrible with naps and usually I don't have time for them. But it's amazing to me. And I'm a, you know, a little like I. A little angry, the fact that some people could just fall asleep really nice and easily and, and get those naps in. But sleep is a big part of any training.
Will Sanchez: Anyone out there pick your favorite, you know, personal follow or to, you know Arnold Schwarzer has you know, a new app now is doing stuff. Sleep. Everybody's talking about [00:19:00] sleeps, and as we mentioned right now, supplements. As you're getting older, what are some of the key supplements that we should.
Will Sanchez: Be utilizing because maybe our body is not creating the necessarily the same amount, or if we're staying active, we need to kind of help the body along with adding some supplements.
Dr. Grant Garcia: So, you know, the biggest one is omega-3, you know, fatty acids. A lot of times, like as us, thankfully in Seattle we have a lot of fish, salmon especially.
Dr. Grant Garcia: Yeah. So that helps to sort of improve inflammation in the joints. Improve joint health in general. And so that's a, that's a really important supplement. You know, you just gotta be careful though, at the same point. You know, supplements are a great way to add more balance to you. You can have, you know, vegetable supplementation, you can have other supplementation, you know, vitamin b12, vitamin C, et cetera.
Dr. Grant Garcia: But you also can be careful cuz it's also a huge market and it's not really FDA regulated. Yeah. Similar to other things we've seen. And so supplementation's good, but. [00:20:00] People sometimes think, okay, so the recommended daily value is this. So if I have two times more, I'll be two times better. Yeah. And that doesn't work like that.
Dr. Grant Garcia: Gotcha. And the one of other thing that's really good, especially for us in Pacific Northwest is vitamin D. We are very deficient. You know, I'm a guy that likes the sun. If I could take advantage of it and my mo you know, over the last few years I've had a couple values that have been low vitamin D despite.
Dr. Grant Garcia: Being of Latin heritage. And so it was surprising to me to see vitamin D levels and talking to, you know, even my primary care doctor, they're like, this is extremely common, you know, and, and the people in the Pacific Northwest and upper Northern Regions. Tend to have low vitamin D levels. Yeah. And especially for my patients.
Dr. Grant Garcia: I'm a bone health kind of guy cuz I see breaks and fractures all the time. You know, a lady in her fifties falls, breaks her wrist. Breaks her shoulder. That's not normal. I mean, it seems normal to us, but it's not, it shouldn't happen. It's osteoporosis or osteopenia. Yeah. And so bone health is essential. So vitamin D, calcium is good.
Dr. Grant Garcia: And it's not just women, it's men too. You know, we don't, we're not [00:21:00] above the osteopenia, osteoporosis, and no one wants a fracture. And so it's important for us to make sure we take care of our bodies. And extreme athletes can be at other risks as well. And so you wanna make sure you have right supplementation if you're gonna be doing it.
Dr. Grant Garcia: If you're doing a 2.4 mile swim and 112 mile bike ride and a 26 mile marathon, you better be properly hydrated. It's not just water. Yeah. You know, we could have the joke of Gatorade, you know, but again, it's all of those things are essential for supplementation. You have to supplement in what you're coming out.
Dr. Grant Garcia: You can't also go for being perfectly fit and just, you know, eat salad all day, either. You have to have a good combination of things.
Will Sanchez: Yeah. As men, you know, I was gonna bring it up as far as, you know, the role electrolytes plays, you know, especially if you're training and competing. And so I, I think the, the, to oversimplify it is to pretty much be aware of what you're putting out so you can recognize what you need to add back in.
Will Sanchez: Right. I mean, I think that's the, the easiest, most simplest way to kind of put it Dean Car Caris. I'm [00:22:00] pretty sure you know who this guy is. He an ultra-marathon runner. He competed in the largest, nonstop run by a human being. Back in 2005, he ran 350 miles nonstop. He's not human, all right? He's just not.
Will Sanchez: So it took him 80 hours almost 81 hours, and he's 60 years old. To this day, he's averaging about 70 to 120 miles a week, and he talked about three things. One, he talked about overbuilt running shoes. Cross-training and really the one that stands out to me, and we talk about it, we recognize it, but it's something that we really need to be aware, is he says, No sitting allowed.
Will Sanchez: It just weakens the posture when it comes to, mm-hmm. Athletes and being active. What does the role of Sitting too long or sitting too much can play on the body. And maybe that's something that you've seen with patients coming in, how it affects them
Dr. Grant Garcia: sitting [00:23:00] atrocious. It's good, bad for your back. It's, you know, I, I've had back issues before and I realize I'm thankful in my job that I rarely am allowed to sit.
Dr. Grant Garcia: Yeah, so I got lucky. But I'm also tired at the end of the day because you're constantly standing. But you know, sitting is just not good for your body and unfortunately in a tech driven market and you know, with our day and age of being on computers, we all are sitting there sitting on the couch and watching shows.
Dr. Grant Garcia: Yeah. But really, you know, being active, getting up and about, you know, the kids help. Because obviously they make you sit stand all the time. There's no sitting allow when you have children. But you know, the, the sta the stand, there's a reason your watch calculates how often you stand. Yeah. You know, it's a really important function.
Dr. Grant Garcia: And I think he's also simplifying in the sense that. Don't. Don't sit around and let life go by. You know, guys like there's a reason he looks like the way he does and there's a reason he's able to continue to train. Yeah. And he's very lucky genetically hasn't, has things he can do that. You know, we talked to us before.
Dr. Grant Garcia: Not everything is just training, not everything is effort. [00:24:00] There's a lot of genetics involved. If everyone trained like the LeBron James, Not, most of them wouldn't be, almost none of them would be with LeBron
Will Sanchez: James. I still can't dunk. I still can't dunk. Even if I trade like LeBron. I know. So go what your point is.
Dr. Grant Garcia: Yeah. Yeah. So I think, I think really what the, the, you know, the important part of this is that if you wanna be an active person and you want to be active, you just gotta go. You gotta do it. You gotta think about it. And you know what? First it's gonna be hard. If you're used to sitting 12 hours a day and you go to like eight hours a day, you know, we've seen these big push for standup desks.
Dr. Grant Garcia: You know, at my office we don't, we can't sit down because everything's a podium. So we're standing constantly. Yeah. You know, I find myself leaning a couple times cause I get a little bit tired of standing and running around between patients. You know, my staff finds it funny cuz I run between different office stores and everything else and I'm constantly moving.
Dr. Grant Garcia: But, you know, it makes me feel better. At the end of the day, you find you're sitting, you think you're resting, but it's actually worse for your body. And it slows down your metabolism and all these different things. So it's, there's, I think the hardest part, I think is the combination of activity, [00:25:00] diet.
Dr. Grant Garcia: Exercise, rest, et cetera. And people don't understand how that balance works. You have people that are on one end, they're all diet, right? Diet this, diet that. You've seen all that, and that's really important. Yeah. But that's not, there's a, it's a, it's almost sort of a, I'd say a pyramid or a square. And if you only focus on one little corner, you're not gonna be successful.
Dr. Grant Garcia: You know, these are high level athletes. They're not just eating the best foods possible all the time. Only, you know, they're focused on a lot of things, the sleep aspect. The train aspect and then the recovery aspect. And all of these are essential. And I don't wanna jump back to an old topic, but you know, the one thing I forgot to mention with the wearable technology with, in terms of sort of monitoring your body, is those new glucose monitors.
Dr. Grant Garcia: Have you seen those? No. They had so basically they're really simple and anybody can have them, and it's basically put on the side. It used to be for diabetics. Okay. Patients. But basically you can just monitor your glucose with your phone and it can, it's another way that some of our athletes are using it for training or with people who do intermittent fasting.
Dr. Grant Garcia: You can [00:26:00] identify your glucose levels and that's also part of your regimen is to see what your glucose levels are like cuz you can, you can know more information. We don't have that ability yet until this thing came out. But this new technology is pretty impressive. It's pretty painless. And it just sits on the side of your arm.
Dr. Grant Garcia: You may have seen people with these little nubs on the side of their arm and you just scan your phon and it tells you what your glucose levels are and other levels as well.
Will Sanchez: For those that don't know why it's important to explain, please.
Dr. Grant Garcia: So glucose is, is the initial sugar. There's other levels of sugars and I don't want to go into sort of the Yep.
Dr. Grant Garcia: Overall details of the way our body processes energy. But glucose is essential. And if your glucose, you don't wanna have glucose. Glucose levels can come from a lot of things, but, you know, fruits and vegetables are mainly fruits. Simple sugars are really important. And you don't wanna obviously have glucose from, you know, candy and those things.
Dr. Grant Garcia: It's a different level of, it's not the same type of stuff about the high fructose corn syrup, et cetera, but you don't wanna have your glucose levels get low cause that's when you start to get hungry, you get shaky, you don't [00:27:00] feel as well. And so I think that understanding and monitoring this, you know, you've heard the rock, he talks about having five or six meals a day.
Dr. Grant Garcia: You know, that's like really the way to go. Is you're just never really that hungry. Yeah. And so you're not engorging yourself. You know, we're so used to this. There's been an article I heard that like, you know, I talked about like the three meal regimen was invented basically by like, you know, Americans, this, this like sort of these three different things.
Dr. Grant Garcia: We have to have all the time or three meals, dessert and espresso to paint on where you are. Yeah. But really it's the keeping your, your glucose levels at a, at a moderate thing. I find if during the day I just have a little stack here or there. It, it can make it so eat less during the day and that's another good opportunity.
Dr. Grant Garcia: And obviously if you're exercising, you get a massive glucose low from your exercise, you don't want to, you know, skip a meal then, and then have an issue later on. I mean, the way your body metabolizes fat, I think it's always hard people to understand. But understanding that it's not just about, The diet.
Dr. Grant Garcia: It's about everything and it's all essential. And I think the problem is if you're, if you're hy, our bodies can only, our minds can only process [00:28:00] so much. So if we're hyper-focused on one of those, those things I call the square we're missing on the other things. You have to be kind of cognizant and you gotta sacrifice.
Dr. Grant Garcia: Okay, I'm not gonna be perfect on diet now, you know? The rock always talks about cheat days. You know, it's okay to let your body, let yourself have some not so great foods every once in a while, but it's also great. It's okay to not get perfect sleep all the time, but you just don't wanna make it a habit.
Will Sanchez: Yeah, so I guess the Rock was watching me yesterday as I had a nice margarita slice of pizza. So don't, don't tell anyone. But yeah, it was delicious. But, you know, going back to your point, I had a slice of pizza. I didn't have three or four, like, you know, which is easy to do. So in, in moderation real quick, I, I, I feel like we could do, I dunno, two hours on this thing.
Will Sanchez: So I'm just trying to move it along a little bit for anyone that's trying to say, hey, I've been outta shape. I kind of wanna get back in shape. I know personally I can't do it, and so I'm gonna go look to go somewhere, try to get some training, go to a [00:29:00] facility. I'm not sure. There's a million different ones.
Will Sanchez: Everyone's saying the same thing. Is there one thing, maybe two things to focus on. If you're going to go to a place to try to, you know, get back in shape, you know, that you should recognize and say if they do this, or if this is there a part of their training, then that's a good sign for you to go there.
Will Sanchez: Is there anything that stands out for you?
Dr. Grant Garcia: Well, I think you gotta go in and I, I hate to jump back to that, but I think you gotta go in with the regimen of, I'm gonna do my best and not hurt myself. Right? Because if you're outta shape, We saw this so much, so many times during the pandemic. People didn't work out at a gym for two months.
Dr. Grant Garcia: Two years, and they come back and they get hurt and then I see them in the office. So going in, if you've been outta shape, is to focus on the things that you can do well first, making sure you're, you know, you're stretching, you're doing all your adequate thing that's not gonna burn fat, but that's gonna protect you from getting injured.
Dr. Grant Garcia: Cuz as soon as you get injured, you're back to where you were. Yep. And. The one thing that's really people don't [00:30:00] understand is, I think if you go to these gyms, you get a lot of people lifting weights and they, the, the people that are lifting the weights are usually people that look like they lift a lot of weights, right?
Dr. Grant Garcia: And then you see the people on the cardio machines trying to burn fat. But what people don't understand is that actually weightlifting is more fat burning than cardio. Yeah. And so really the focus should be on weights, especially pay for people as they're trying to gain muscle mass. But it's, again, it's cross-training.
Dr. Grant Garcia: And that's what you had mentioned before with talking about Dean. You know, cross training is essential and so I do this workout all the time. I do, you know, hit exercises, but then I'll mix it up and do con cardio and really focus on weights to try to keep the tone and try to burn that fat cuz you know that extra effort you're doing.
Dr. Grant Garcia: So don't skip on different areas in the gym or in with a trainer. And you'll see a lot of the trainers focus mostly on the weights. And the reason being is that's where they can give you the most value. It's really not helpful to have someone tell you to run on the treadmill. You know, that doesn't really add a lot of skillset but also mix up the machines.
Dr. Grant Garcia: There's so many different options and so just constantly keep [00:31:00] the body guessing. I know that's kind of some jokes they have running and keep the body guessing, but it really is essential. And that's the same thing we're talking about with all these athletes. They're constantly keeping their body guessing.
Dr. Grant Garcia: Yeah. So when one part gets tired, they focus on something else.
Will Sanchez: And, and just to put it out there and you know, I, I, everybody kind of knows this, but the reality is it doesn't matter when you start, right? So if you're 30, 40, 50 I've worked at a local gym here with kettlebell training and I've.
Will Sanchez: Seen people come in 60 seventies and even 80. And you know, and they move a little bit of weight and they're doing you know, weight training, doing different things. And if you watch 'em for six months, you watch 'em for a year, they're moving around and it's just, it's beautiful to see. And it's inspiring.
Will Sanchez: And the reason I say it is just like, Don't get stuck like, this is what I've been doing. It doesn't matter, you know, start today, get out, go for a little walk, or whatever the case may be. Anyway, that's my spiel [00:32:00] there. Anything coming up as far as, you know, there's so much right, you know, whether it's advancing cartilage and we've talked about internal brace and things like that.
Will Sanchez: Is there anything out there out of the million things that we can discuss that stands out for you, especially with the agent athlete?
Dr. Grant Garcia: So I think from an orthopedic standpoint, you know, we talked a lot about the things that do prevent injury, but it's gonna happen and sometimes it unfortunately happens when you don't want it to.
Dr. Grant Garcia: Mm-hmm. Is to understand that there are solutions and like we've said before, get other opinions. This is the most common area I see as we get to these. Arthritis or early arthritis issues, there are less and less physicians, even orthopedic surgeon, that feel comfortable with cartilage restoration or getting athletes back at that age.
Dr. Grant Garcia: Hmm. The number of patients are surprised when I tell them I have a surgery that I'm gonna do for you and I'm not gonna restrict you afterwards because my number one goal is not to replace the joint. My number one goal is to save a joint, and so you need to make sure you shop around for the right people.
Dr. Grant Garcia: Again, it's not always the [00:33:00] right. Solution for everyone. Yep. But knowing that there are advances out there, you know, you should be given multiple options. And you're, as you're younger and things that we're willing to do are more sort of, Risque or so more cutting edge as you're younger because you're just not eligible for a near place.
Dr. Grant Garcia: I mean, especially when you're below 50, 55. So there's other things that we do now. I mean, I, like I, I said before, I just, I was at a, a big national meeting teaching newer techniques to save the acl. You know, we didn't do this a few years ago. We had no technology for it. You know, people, half the surgeons there that were learning about this were blown away that we have this technology.
Dr. Grant Garcia: Wow. And so, and just, I just basically did a, I did a course teaching about cartilage restoration and how we can save the knee. And so there's all these things that I can do as a surgeon, and there's other surgeons out there as well that have these opportunities. You just need to know this. And, and the goal of my procedures, you know, is always, patients always go well, I'm not I'm not in that much pain normally.
Dr. Grant Garcia: Okay, that's fine. But can you do the sports that you want to do? And they say, no, I'm [00:34:00] unhappy. And that's why they're in the office. And I tell them, and then will, you've probably heard me say this before, I do not do surgeries for the most part, so you can just walk down the hallway. Yeah. You know that's not why you'd spend all the time doing this.
Dr. Grant Garcia: This is so you can get back to the activities you want to do. Does that mean you're gonna get back every time? No. But does that mean that we're gonna do our best and we've had good results? Yes. I mean, you've seen it on the website, you've heard about these testimonials. You know, patients do well if done for the right reason, but it, it's important for the patients to understand that there are solutions and there are ways we can avoid knee replacement with injections, cartilage restoration, and there is cutting edge.
Dr. Grant Garcia: I mean, even the next year, I'm gonna add three more cartilage options. Probably to my repertoire with the newer technology coming out. So, you know, there's just so many different things and this is really the future. Of like you heard, a can we, can we prevent these joints from happening? And if we can't, can we get them back with surgical procedures that are less invasive or faster recovery?
Dr. Grant Garcia: You know, you've heard about the Reeb list, which we're gonna talk about next week on a [00:35:00] webinar. While we take these complex knee patients and get them back for rehab. We are, we are hitting this from all angles. The pre, the, during the post. The recovery, the rehab, the long-term man monitoring with these wearable technologies and you name it.
Dr. Grant Garcia: So our goal is to continue to keep these athletes going and if something happens to you, come right back. We'll figure out a solution. That's the key.
Will Sanchez: That is the key. And that's that's perfect. Hey, listen to your body, right. Hey, listen to your body. Get out there. Keep moving. Don't be afraid of getting injured.
Will Sanchez: You know, obviously be safe and smart, but it'll be beneficial for you in the long run to move, you know, to whether it's the, the, to hinge, to squat, to just get outta bed, right? If you don't move, you know, as you get older, those things are gonna become more difficult. Dr. Garcia, I think we're going to wrap it up.
Will Sanchez: What do you think?
Dr. Grant Garcia: I think we talk all night on this, but it's probably gonna be tiring for our listeners to lis listen for the next two hours. So here's what I'll tell everybody. If you have [00:36:00] any, if you want any of these topics in more depth, please reach out to us on the gmail sports.talk podcast gmail.com or head out the, it's a really great website@wwwsports.talk uh.com.
Dr. Grant Garcia: There's a great. Way to fill out a referral and ask about what type of episode you want or if you want more information, we're happy to jump on this and then listen to different websites and learn about this, cuz there's lots of information.
Will Sanchez: I love it. And you know, you, you're so close, Sue, wrapping up the show, but, but in honor of the Kraken making the playoffs and because of the topic.
Will Sanchez: All right. Who was the oldest hockey player to play in the N H L?
Dr. Grant Garcia: Oh my gosh. I don't even think I could get, I don't even think I can get close
Will Sanchez: Gordy. How He's not even close. He played to. 52 [00:37:00] years old, one of the greatest hockey players to ever play for the Detroit Red Wings. And he also played with the Hartford Whalers. He played 26 seasons. So if he could go out there and play 52 years years old, that's amazing.
Will Sanchez: If he could play in the NHL until from 46 to 1980, if he could play that entire time where it was, I mean, he, he didn't even have a helmet when he started. And got hit and took the punishment and kept his body in shape and did what he did, you could go out there. So that was my little trivia, honoring our hockey playoffs and also our aging show.
Will Sanchez: Dr. Garcia, thank you for playing. Appreciate it. It's good to talk to you. Check him out. Grant garcia md.com. He's our orthopedic surgeon at Sports Medicine Specialist. Good job, buddy. Thanks for having me. Hey, we'd like to thank everyone out there listening. We [00:38:00] appreciate it. Keep the questions, the comments, and the suggestions coming in.
Will Sanchez: Thank you very much. Audio Transcript
New Episode: MLB New Rules and Injury Risk
[00:00:00] Welcome everyone, and thank you for listening to SportsDocTalk All sports, all orthopedics. All the time. I'm Will Sanchez, along with Dr. Grant Garcia. He's your orthopedic surgery and sports medicine specialist. Check him out@grantgarciamd.com. Dr. Garcia Spring is in the air. Flowers are blooming and the ballpark is starting to buzz as baseball seasons back around, and especially here in Seattle where the fan base is really excited about this upcoming season.
We are gonna get into that little bit, but really our show is gonna be talking about a little bit about a baseball, but pretty much some of the new rules and some of the new challenges that some of the doctors and some of these players may be facing first. And for. , Dr. Garcia. Welcome. And what kind of, fan are you?
Who's your favorite team when it comes to baseball? Well, you know, I'm, well, I live in Seattle and I know [00:01:00] that Mariners are true to heart for a lot of us. , you know, we're in New York as I know you are too, , with football, and I am. My dad grew up being a Yankees fan and my grandfather, my dad always told my sister, she said, I hope you bring home someone that's a Yankees fan.
That's what she told to her. So we are Yankees fans. , so I root for the Yankees for the most part. So how, how unusual it is that. We're both Giants fans, we're both Yankee fans. So let's go Yankees. Let's get ready to go. I've already got my ticket for one of the games when they come out here. I believe it's in May.
I think they're coming out here really early this year. Oh, okay. So, , I've got one of my tickets already, , for, for the family cuz we have to at least show up to one of the games. So we are really excited and what's really exciting about this year is that it's probably the most. Excited. I've been about a season that doesn't include wins and losses for the team I love, but for the overall game, right.
And we go back to the strike [00:02:00] season when Sosa McGuire came back and really kind of saved baseball. And I know, , when it talks about steroid use and everything else, you know, people tend to forget that these two individuals really saved baseball in the summer of baseball, which, Absolutely incredible, and I'm excited about this season on that same level because of some of the different changes, whether it's the speed of the game, , that's something that's happening now because now we have a pitch count and just to kind of, , inform our listeners if they're not baseball fans or not, know exactly what that means.
There's now a countdown, so it counts down from 30 seconds between batters. So after a batter 32nd clock comes on, starts to count. In between pit , pitches to that batter, it will be 15 seconds with nobody on in 20 seconds if there's a bass runner and then the pitcher must start its delivery before the clock expires.
The batter has to get in the in the box by a certain time. I don't wanna go through all the minutiae of these, [00:03:00] you know, all the rules, but. The, the point of context here is the game is going to speed up, right? And in the minors, they tested us and it's sped up by about 25 minutes. So they're trying to shorten the game with the, with, , the, the span of everyone's, or lack of span of, for some of the people that go to these games, it should be a little bit shorter.
So is this something that's excited for you, exciting for you with these new rules that you're looking forward to this? So, you know, as a surgeon, I've got a fairly short attention span. So for me, I'm looking forward to these shortened rules. I've always, I love baseball. I love watching baseball. , I love, you know, taking pair of baseball players.
I, I love everything about baseball, but the, the speed of the game is challenging. When you, you know, go straight from football to baseball season, , and you know, football to speed with the clock count, , or, you know, my new favorite sport is hockey since I, I'm actually a big Kraken fan now. [00:04:00] Okay. , so it's just different to watch, , the speed of those games versus baseball.
So it's nice to see a little bit of integration. I'm sure there's comments. Is people have issues all over the board with different things in terms of, you know, this is not going away from the original way the baseball was played. , but I think it's good to have sort of, it sped up in the game it is now because sometimes these games can go really long, you know, like four or five hours extra earnings, et cetera.
And having this sort of account, I think will, will change things up and make it a different strategy in the. I, I agree. And, , it, it should be really exciting and you know, we're talking about being a Yankee fan, especially the old Yankees Red Sox games. There you go. You're going four pla plus hours. And we're lucky enough that we live on the west coast, and I say if you are a sports fan and you live on the West coast, It's just absolutely beautiful because the games end early.
Mm-hmm. But on the east coast, like the national, , championship for basketball is happening and they're starting at nine [00:05:00] 20 on the East Coast. So these games really go along, especially if you're a fan, and more importantly, if you have little ones and you want to take him to the game, even if it's not that little, you know?
But they've got school the next day starting the game, so. Going home and getting home at 11, 11 30, midnight is a big deal. Anyway, we're not gonna get into all that. That could be a different show. If people want to talk sports, we're here for that because we are sports fans. But we wanted to do this show and, and the reason was was how does the pitch clock affect certain pictures?
And when I first started thinking about this, I said, we've got pictures now. They throw in the high nineties, right? They, they hit triple digits, they throw a hundred, the grom, a bunch other pitchers, right? And they had the luxury of throwing that fastball, hitting 99, a hundred, 101, and then getting the ball back, walking around the mound, you know, getting themselves ready, you know, hitter or adjust themselves, , a minute later to throw in another.[00:06:00]
You don't have that luxury now. And I was thinking, what happens to the fatigue of these pictures, especially pictures that throw hard. So just off that, just off that basis, what is something that really kind of stands out when you think about a picture that throws so hard and is really, really getting ready to throw that pitch again?
15 seconds. Well, as we know, you know, the baseball pitch is one of the most looked after, analyzed, , movements in all of sports because it's such a high torque, high acceleration, high deceleration, , force. And we see a lot of injuries as a result. You know, some of us who do care, a lot of baseball players, you know, we see so many different Tommy John injuries or shoulder.
Due to baseball, and it's because of this sort of recoil and acceleration. So to hear that, you know you're gonna have players that can go in the high nineties to. Triple digits, which happens a lot more [00:07:00] now than it used to. , you know, that is a concern in my opinion. I think that what we'll see is that there's gonna be some adaption.
You know, these pitchers who either throw this hard are not gonna be able to go as long, , and, or they're gonna have to change their pitches up. So they're gonna have to have, they can't continually throw fastballs, , or stick with a high fastball, , repertoire. , but at the same point, you know, it's gonna be interesting to see because I, I think.
Most of the things we do in baseball are based off pitch count. Yeah. And when you're younger, now again, this is major leagues, but a lot of times it's like, okay, you hit a hundred pitches and there's certain ages that we go off of, , and that the little league pitch count. And so, and players themselves have all been tracked for pitch count too.
That's what, you know, the playoffs are a little different. Yeah. And so it'll be interesting to see if this changes that number. You know, the data. We need a few years to see what happens. I do hope we don't see an increase in reconstructions or Tommy John, , u c reconstructions as a result of this, cuz it's already sort of on the rise, , with all this other stuff.
So it'll be interesting to see. [00:08:00] In the next two years, you know, hopefully we're still doing this Sports Doc Talk podcast and we can talk about this episode and go back to it and say, has there been an increase in injuries as a result of the change in the game? Cause you know, there'll be, there'll be articles on this all over the place in the next year or two if you find out that data, you know.
and it's really interesting that, that you mentioned that because. The data, right? That was the key word that you just say there, you know, how much data is there. Mm-hmm. Right. So there's data in the minor leagues, but it's different in the majors. Right. , even though we think that that's, that's the next step.
But the reality is it's multiple steps for you to be, you know, a single, a aa, triple A pitcher that then be a consistent top notch or. Everyday player, pitcher, , in the major leagues. You, you are doing something that is very different. And this is the first year that we're doing it. And we talked about the fastball, right?
Cause that was just kind of the easy thing to think about. But what about what we've talked about in previous shows with our kids or young kids, [00:09:00] and these are an adults, but they're throwing, breaking pitches. What kind of fatigue or concerns you might have when it comes to the elbow muscles or ligaments where you're doing something, you know, you're putting that strain so quickly after, you know, you've thrown a pitch.
Well, I mean, I'm, I'm worried in the majors because of how hard they throw, but these, these players have been self-selected, right? They're already the ones that didn't get injured or they got injured and they recovered. Well, they're all giant. You know, you can tell a baseball player how good they are by a pitcher.
You know, if you stand, they stand up in the office in their above your head. You know, I'm not that tall. I'm about six one. , but you know, the ones you can tell these guys are very large and strong. And so their bodies have been self-selected to be these top players. , but when younger kids are growing, it's a big difference.
I mean, again, that, that speeded , that speed, , sort of in accelerated pitch count, , information or accelerated pitch count rule. [00:10:00] Caused some more injuries, but it might not change at all. And I'm sure that MLBs done, done information on in scene in the minors that didn't change anything or they wouldn't have gone ahead with it cause it's the last thing they wanna see.
but for little kids, this is concerning to me because until your growth plates close and for an adult male can be between 16, , around 16 years old, but it can be a little bit older. If you throw too hard, you can actually change the rotation of your. Which can be something that's a little bit concerning.
You can have sort of growth plate disturbances, , and for younger kids, I mean, I see, I've seen kids now with Tommy John injuries at 13, 11, 12, and we never used to see those. , and we're seeing a lot more at 15 as a result of pitching. And so now you have a, now you have this plus a faster count. And they have to more remove more rapidly.
it does concern me, but again, with Little League, you know, they're not doing the same psych out stuff that they do in the major leagues with sort of the way they trot around and do the different things. So it's, it's part of a show as well. So it's, it's twofold, but I, I do worry that there's a chance we see with the [00:11:00] younger ones, I think the younger kids are way more susceptible injury than the adult picture.
You talk about shoulder fatigue, what are some of the, , key shoulder injuries that you'll see in whether it's a pitcher or that type of movement, whether it's baseball or something else that will impact that shoulder? So with people with mostly the ones I see, they're usually in their 15 and above. And so most of their growth plates are completed.
So if their growth plates are closed, for the most part, and number one thing is slap years. And that's a lot of. What I see in the office doesn't always need surgery, but I see a lot of slap tears and BA and high level baseball players. I probably just saw few last week, for instance. So that's one thing we see.
The other one you see is rotator cuff strains. Occasionally you see a rotator cuff tear and then bicep symptoms. , but the number one thing is a SLAP injury, , which means you, there's a tear of the top part of the labrum. , the thing is you don't need surgery. And we looked at Yankees players and we looked at the Mets and everything else, and we took care of them.
you see these in players as a result of, in [00:12:00] order to peel your arm back, you know, when you throw a baseball, you don't, you're not normally built to throw a baseball like that. Your arm goes back a certain amount. It's called external rotation. And as you learn to pitch better, you can, you find a way to get your arm out.
Externally rotate more, so therefore you can speed up your velocity. Yeah. And that's how some players get fa throw ba the ball faster, but as a result, your body's not used to that. So you peel off the labrum so that you can get your arm back farther. And then sometimes it become symptomatic. And that's called the slap tear.
I'm gonna stay with that area, right, because I'm trying to think about the arm and, and before we work our way down, I'm just gonna kind of work your way back. Would you see a back injury or somewhere along their line? Can it be, you know, anywhere it's a, a disc or a strain or something like that from, , having this, this momentum, this force as being conjured up by, by throwing a baseball like this.
You could, I mean, you heard of players with spasms, but that's [00:13:00] generally in the older kid age category. Mm-hmm. Gotcha. I don't see too many back injuries from pitching. , you see a lot more from football, et cetera, , or with, you know, like Ben Simmons with obviously the basketball, , but the, , not as much, , in the pitchers with the back, you know, you have that shoulder gerd.
Also a lot of scap. , so that's the scap is the bone, , where the socket connects in and that's where your wing bone, where people see the winging thing on the, on the back. And so pitchers get a lot of sort of, we call dyskinesis or the scapula doesn't move appropriately. And as a result, your pitching's all thrown off.
Because remember, when you lift your arm up, your arm only goes so high, then you have to use your scapula to get the rest of the way. Yeah, because your scapula is like sort of locked in or not moving appropriately. When you throw, you're not gonna throw. Well, so the thing is people always think, oh, your shoulder, you.
The main part of the throwing arm, it's way more than that. You know, there's, they use all these little sensors on people's shoulders and these baseball players to look at the mechanics of them. And we've done those in, , studies that I've been in, , a part of as well, to sort of find the biomechanics.
But it's the entire body. It's not just an [00:14:00] isolated part. If you are working with, , let's say the Mariners, right? And I know you have experience with the White Sox and, and you know, so on and so forth with all of that, , what is something that you may or you think that has been discussed, , in the room saying, okay, We have to look out for X, Y, and Z with our pitchers on the mound throwing, you know, every 15 seconds.
What, what do you think is something that might be in the, that conversation with the team doctors looking at their pitchers, not only F from game to game, but throughout the season? Well, I mean, the first thing they're gonna do is stringently watch. You know, if they start losing velocity, you have a picture that's routinely hit, throwing 95, 96 miles an hour and starts going to 93, 92, , at a much earlier stage.
You know, you, you guys would, you'd be shocked at how much da Well, you, you're a data man, so you know, but basically you'd be shocked how much data out there is out there. I mean, we basically write papers on papers. [00:15:00] That data that's com commercially available for anybody and it's free. , , and you can go on the websites and look this up, but you can see, you know, how someone pitch counts, changes and they have even more, , , impressive data behind the scenes of these of these players.
And each one can have pitch counts and it's all tracked. , so they're, you know, they're really doing a good job of trying to make sure they're watching them for. Obviously that's the number of pitches they're throwing, you know, curve balls, breaking balls, , et cetera. , but really at that speed that people are worried about, they start losing speed and losing accuracy.
that's when we say, okay, it's time for them to be pulled out, and we're watching that. And you can also see people drop their arm, certain fatigue movements. Now the high level players are pretty good. They have really good mechanics. Yeah. But no matter what you, what it is you've seen in football, you've seen in any of these sports, no matter what type athlete, athlete, you.
You still can get fatigued. And so as a result, you're watching for those signs, body movement and then the speed and then the control. Can you have some injuries from, from this? , we talked about the shoulder, obviously we talked about elbow u UCL, you know, [00:16:00] Tommy John, things like that. I'm assuming the forearm, but the hand and wrist.
how does that affect, is there anything that you know, can come. , come of this from having an injury from, you know, having this torque and, repeating this motion, so quickly. Is there something that you would look out for the hand and wrists as well? So you, you get a little, you get less hand injuries from baseball, but there you do get hand injuries usually from the baseball hitting.
So, you know, yeah. Someone gets grabs, tries to grab the ball or jams their finger or breaks their finger or sliding, you know, , into, , the plate. , so that's usually where the hand injuries come from. There's less injuries, cuz again, most of the torque you're generating is actually in your elbow, which is why the elbow is so focal.
It's also focal cause it's. Devastating of all the injuries for pitchers and pitchers are essentially the quarterback of the team. And so when a pitcher goes down, it's a big deal. Right? You know, you obviously every player's important on there, but yeah, when the pitcher is out [00:17:00] for that, that's a, that gets focal.
It's just like if a quarterback gets hurt, everybody knows about it. We know these guys train like, like there's no tomorrow. But do you think that training, and, you know, this is a tough, question to answer because it, there's such a big area, but do you think training is going to change the, do you think there's gonna be anything that, , doctors start to do with maybe their pictures or pre preventative training to help reduce injuries or in order for you to, , withstand the rigors of such a long season?
Oh, you, you can believe it. I bet they've been doing it already. You know, everyone's looking for the edge. Every single ma league baseball, whenever you work with a company. So we talked about this on the napkin innovation episode. We had two, , Two or 3, 3, 2 months ago or so. Yeah. But basically, you know, when we see new to new technology, the very first thing that technology tells us is we've already, we've already have it in all the major league baseball centers.
And so they always show the new technology to these guys, get them on board. [00:18:00] To use it to see if it works with their athletes for the most part, as long as it's safe. And wearables are a huge aspect of this. Yeah. So, you know, there's different sleeves that can track the counts. There's different baseballs, there's different other movements that, that track all the mechanics of the players.
And you, you know, they're practicing this, , during their practices and you know that they practice this, you know, they're practicing in times and you're not even thinking about it. And so they're, they're prepping for this already. , They had the whole season, you know, sort of to discuss this and seeing what's happened in the minor leagues.
You can tell they already had scouts out there doing this. So what we think they might or might not know, they're already way ahead and they've been preparing for this. You know, were the pitchers preparing for it with their standard routine? Maybe, maybe not. Yeah. , but they're also gonna adapt. Right.
You know, you've seen as soon as someone has something new way of beating the system here, they're all gonna catch on very quickly. , cause this is only a matter of. So, , Dr. Grant Garcia as a goodie bag would consist of, , wearables data, , and training. What, what, [00:19:00] what else is in that goodie bag, you know, to make sure that your guys are still, , ready to go.
Big bags of ice. They're always the, the, , baseball players, you know, you see 'em come in after the White Sox, , and they're, you know, wrapped with ice all over their body. It's just sort of, It works well. I love ice. You know, I've been injured before and I've had to use ice. It's, it works amazing. It's the, it's the cheapest, easiest thing you can do and it doesn't injure you.
but, you know, these guys are loaded with ice and wrap, , as soon as they leave, , the stadium and come, go to the locker room. , so that, you know, that's one thing you wanna put in your goodie bag too, but obviously you gotta keep it in the freezer, so that's a little bit challenging. But I think, you know, the wearables are really important, like you mentioned, , and then sort of any supplementation.
And then you're also testing sort of, you know, all their vitamins and minerals and making sure their sweat counts and they have all these different things to try to find, get these app athletes at maximum ability. And also depends on the weather too. Yeah, that's a good point. I didn't even think about the weather, how it plays a part, especially.
Early in the [00:20:00] season in, , some of these cold weather states. , and how that affects, let's just talk about it real quick since you mentioned it. How does cold weather compare to, if you're playing in, Minnesota and, instead of, , you know, Miami or something like that. How does the weather play a part?
Is it, is it a positive or negative if it's, a certain temperature. Well, I think, you know, when the low temperatures, you're concern about some tightness, right? Spasms, , you know, the arm may be warmed up, but the rest of the body may not be right. So you could have other injuries or your mechanics may be slightly off.
You know, again, a lot of these players practice in these conditions. But then again, where's most of the training? Spring trainings in warm weather climates. And so they're, they're still really adapted to this type of weather Now, A lot of the stadiums are covered, et cetera, and when you start actually playing, you know, your by temperature raises significantly.
I worry more about the extreme heat because that's when you can get fatigued. Mm-hmm. You can be dehydrated, you know, again, [00:21:00] these are professional athletes, you know, they'll only hydrate so much. You know, you have to. You know, you see them in the dugout, they're having a good time. , they're trying to have their best to try to enjoy the game.
you know, you have certain pictures that are a different animal like Verlander that probably, you know, doesn't speak and just sort of has everything that's teed up perfectly. Yeah. But that's not the way everybody is. So basically, you know, that's when you worry about hydration. Are they properly, are they properly, , setting themselves up to get it through the game because you have high temperatures, faster pitch.
You know, that's when, that's when sweat and other electrolytes are really important in understanding what the body's doing. And that's probably where they get into some of these sort of wearables. You can test the sweat, those different things. And I'm sure there, there's things that I've even heard of or seen, , that I'm sure these players are using to try to get an edge and keep themselves on top.
It'll be an exciting season. I'm looking forward to it. I'll play doctor on my couch looking for, , a, a drop in miles per hour, maybe, the ball not snapping so hard on a curve ball, and [00:22:00] I'll sit there and point to no one and say, look, he's getting fatigued. There's something going on. So I'll play Doctor on the couch as you play real Doctor in the real world.
let's talk about baseball predictions this season. Let's hear it. Who is coming out of the National League for you? What team are you picking? Hmm. You know how to do it right? I, we had to go do this, right? I know you always do this. Yeah. What you got? Come on, let's pick it. Who's your team? I'd say, you know, I don't know.
It. Maybe I would say Houston. All right. So Houston's an American league, but we'll take Houston. Right? So you think Houston will be back in the World Series and about the National League? Who do you think, let's see, I'm thinking. Dodgers. All right. That's a good one. All right. I, I'm gonna go with the Braves, even though I think San Diego is gonna give, , play really well.
I would love to say the Yankees, but I still think that the [00:23:00] Astros have, , slightly better team. But we'll see. There's so much baseball and these obviously predictions sure to go wrong. So please don't hold us to it or not do do, so we'll talk about it. , and you know what? I forgot. There's one more thing before we go and I just wanted to bring it up.
Oh, all right. Here we go. Since we're in Seattle and we're, , we're in Mariner country, we're gonna do a little trivia, and if the Mariners wanna be successful this year, they're gonna be led by their Skipper Scott's service, who was the last American League manager of the year for the Mariners. Can you pick who that coach was?
Lou Pinella. Lou Pinella, what? In 1999. In 2001. He's the only American League manager of the year for the Seattle Mariners. That answer is correct. That's unbelievable. I got that right. I never did it. Right. That's great. That is wonderful. I wanted to tie it into some Yankee [00:24:00] way. Also, I noticed Seattle Romero is fan fans to say, what are you talking about?
Yeah. Lou Pinella was in New York. Yankee, he played for the Yankees. Mm-hmm. But you know, we don't get everybody's, , Feathers ruffle. Listen, thank you for taking a little bit of time so we can talk about this show, talk a little baseball, and more importantly talk about some of the things that all of us are gonna be looking forward to, because there's so many new rules, so many different changes, whether it's, , banning the shift and, you know, getting in the box right away.
With the, the pitch, , clock and, runner of second base and so many different rules. We're really excited about this season. I hope everyone gets out to the ballpark with your friends and family. Have a good, , good time. Get your, peanuts, cracker jacks, and, you know, get your, , cold beverage and try to have some fun.
This. Summer to me, baseball is a sign that summer is around the corner and it's almost here. So we get some blue skies, some nice sun rays, and spend a lot of time outdoors. So, , I hope you're excited [00:25:00] about Summer as I am, Dr. Garcia. I'm very excited about Summer, excited about the, , the new season.
Excited about this podcast and make sure you guys, , subscribe to us. We have a brand new website, , ww SportsDocTalk.com, which has a lot of information you can learn about Will Sanchez and myself. , plus, you know, subscribe to any of the networks you want to. We're on all the major, , podcast centers and I am excited to announce we have our first listener episode coming up next.
we have a good friend that asked to learn. , how to keep our athletes who are aging back in the game, , and from a former Ironman, what does it take? And so that'll be our next episode. So everybody looking forward to doing that in the next month or so. And there's a lot more coming up. We've had a lot of requests for different things, so we're really excited.
Yeah, and please keep the request coming on. , we always put some polls in Q&A and feel free to reach out to us , in the many different forums and put in your request. [00:26:00] We want to hear about this and hear about that. So just a reminder, thank you very much for listening. Sports doc talk, all sports, all orthopedics all the time.
I'm Will Sanchez, that's Dr. Grant Garcia. Check him out. GrantGarciamd.com. He's our orthopedic surgeon in Sports Medicine specialist. Thank you for listening to the show, Dr. Garcia. Thank you for being with us and taking some time today. Thank you for having me. Take care. Audio Transcript